LETTERS TO THE EDITOR .XtW,:.e..,.';. · Letters tO the Editor * I N AN~~~~~(Figure 2 Swollen cell...
3
75ournal of Neurology, Neurosurgery, and Psychiatry 1995;58:756-764 LETTERS TO THE EDITOR Death after ecstasy ingestion: neuro- pathological findings Ecstasy (3,4-methylenedioxymethampheta- mine; MDMA) is a widely used recreational drug that has recently been associated with a syndrome of hyperpyrexia, restlessness, rhabdomyolysis, and acute renal and hepatic failure and at least nine deaths have been reported in the United Kingdom.' There are no neuropathological reports of patients who died after taking ecstasy. A 30 year old man attended a "rave" party where he took ecstasy, heroin, and amphetamine. The next day he drank large amounts of alcohol and was found uncon- scious in a pool of vomit some hours later. He had a convulsion and was admitted to hospital. He was pyrexial (38 5°C), and remained so until his death five weeks later. Creatine kinase was 11 178 IU/l (normal < 300 IU/1) on admission and 3468 IU/l four days later. He remained comatose and had no hypertonia, but had occasional gener- alised muscle spasms. A chest infection was treated with antibiotics. No evidence of hepatic or renal failure or diffuse intravas- cular coagulopathy was found. Brain CT showed clearly defined low densities in the globus pallidus bilaterally. Postmortem examination showed bron- chopneumonia, lung abcess, and pulmonary embolism. The brain weighed 1450 g after fixation. Coronal slices showed clearly demarcated bilateral necrosis of the globus pallidus (figure). There were small foci of necrosis in the white matter. Histological examination confirmed necrosis of the globus pallidus. There was intimal proliferation in large blood vessels without necrosis or inflammation. The sub- stantia nigra was gliotic. There was mild astrocytic gliosis in the amygdala and hypo- thalamus. The cerebral white matter showed diffuse gliosis and spongy change without myelin debris or inflammation and sparing only the subcortical zones. Well defined foci of necrosis up to 0 5 cm in diameter were identified. The cerebral cortex, hippocam- pus, brainstem, and cerebellum were nor- mal. A major problem in understanding the Coronal slice of the fixed brain showing necrosis of the globus pallidus bilaterally and foci of white matter necrosis (arrows). pathology of this case is that, like most drug abusers, the patient took a combination of drugs. Consumption of alcohol may have potentiated their effects. The most striking neuropathological change was necrosis of the globus pallidus, an area rich in sero- toninergic and dopaminergic nerve termi- nals. Pallidal blood vessels showed changes compatible with prolonged vasospasm, pos- sibly the result of local release of serotonin and other biogenic amines induced by ecstasy or amphetamine. Blood vessel changes have been noted after cocaine and amphetamine abuse.2 The pathology resem- bles that of carbon monoxide toxicity, but similar white matter changes are described in nine cases of heroin abuse.' Damage to the globus pallidus is found in hypoxic- ischaemic cerebral injury but almost always in association with damage to the hip- pocampus or other areas of the cerebral cor- tex. Although at least nine deaths after inges- tion of ecstasy have been reported,' neu- ropathological findings have not previously been described. It is important that these cases be fully studied if we are to improve our understanding of the effects of these drugs on the human brain. M V SQUIER Department of Neuropathology, Radcliffe Infirmary, Oxford OX2 6HE, UK S JALLOH Department of Pathology D HILTON-JONES Department of Neurology, Milton Keynes General Hospital H SERIES Department of Clinical Pharmacology, Radcliffe Infirmary, Oxford OX2 6HE, UK Correspondence to: Dr M V Squier. 1 O'Connor B. Hazards associated with the recreational drug "ecstasy". Br J Hosp Med 1994;52:507-14. 2 Klonoff DC, Andrews BT, Obana WG. Stroke associated with cocaine use. Arch Neurol 1989;46:989-93. 3 Wolters ECh, Stam FC, Lousberg RJ, Van Wijengaarden GK, Rengelink H, Schipper MEI, Verbeeten B. Leucoencephalopathy after inhaling "heroin" pyrolysate. Lancet 1 982:ii;1233-237. Lewy body dysphagia Swallowing disorders are encountered with increasing frequency in elderly people.' Swallowing depends on the complex inter- play of sensory pathways from the tongue, mouth, pharynx, and larynx (cranial nerves V, VII, IX, X) with coordinated autonomic, voluntary, and reflex contractions involving cranial nerves V, VII, X, XI, and XII. It is therefore not surprising that dysphagia complicates a variety of neurological disor- ders, many of which are more common in the elderly population, such as pseudobul- bar palsy due to cerebrovascular disease.' It is, however, seldom the sole presenting feature of neurological disorders.' We describe two patients with isolated painless progressive dysphagia who at neu- ropathological examination showed severe neuronal loss, Lewy bodies, and dystrophic neurites in the dorsal vagal nuclei, with only a few Lewy bodies in the substantia nigra, nucleus basalis of Meynert, and cerebral cortex. These patients represent a new pre- sentation of Lewy body-associated disease. Patient 1 was an 80 year old retired man who developed painless progressive dyspha- gia for solids, and to a lesser extent liquids, over a two month period. He described dif- ficulty initiating the swallow, with regurgita- tion of food (solids more than liquids) from the upper oesophagus or pharynx. He lost 6 kg in weight over this period. His appetite was normal and there was no vomiting or haematemesis. Five years earlier a peptic ulcer had been diagnosed at endoscopy and successfully treated with ranitidine. Two years earlier he developed a mild left oculo- motor nerve palsy of unknown cause. He took senna and fybogel for constipation, propranolol (40 mg twice daily) for long- standing paroxysmal supraventricular tachy- cardia, and temazepam as a hypnotic. Examination was unremarkable except for the presence of a partial left oculomotor palsy. In particular there was no evidence of Parkinson's disease or cognitive impair- ment. Endoscopic examination showed no abnormality in the stomach or oesophagus. A limited barium swallow showed the oesophagus to be slightly dilated with a minor hold up of barium at the oesophago- gastric junction. Computed tomography of the chest was normal. He developed fatal bronchopneumonia while in hospital. Patient 2 was an 88 year old woman who developed painless progressive dysphagia for solids more than liquids over three months. After swallowing, food was imme- diately regurgitated from the pharynx or oesophagus. There was no regurgitation after the meal was completed. Appetite was normal and she had no nausea or vomiting. She had lost 12 kg in weight over the pre- ceding three months. One month before the onset of dysphagia, she had suddenly devel- oped mild pyramidal weakness of the left arm, which was diagnosed as a stroke. She was otherwise well, took no medication, and lived an independent life. .; ,. a f A S_ > Q * . . ,.'; S.' .. .'_ ' .. .: . ' .. f' g .. ' li .. } #. W<i-. s a. N ... t.8# zi .. ,, s .. ..... r . ',j: _ .: .. i. 4 v :. ,* 9 .i t. ¢. K b. ... .. ... ... - e FJlli ir S 4k,, .jt H: .s .: .s b . # .. .. ^: .r B:. .. : Ju: s +. .: :d.::A,, .::, .XtW,:.e .. ... KrreN i. .:ffn.:, . 4, $'i Figure 1 Swollen cell in dorsal vagal nucleus from patient 2 showing Lewy body (haematoxylin and eosin). Bar = 1 00 p m. 756 on March 23, 2021 by guest. Protected by copyright. http://jnnp.bmj.com/ J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.58.6.756-a on 1 June 1995. Downloaded from
Transcript of LETTERS TO THE EDITOR .XtW,:.e..,.';. · Letters tO the Editor * I N AN~~~~~(Figure 2 Swollen cell...

75ournal of Neurology, Neurosurgery, and Psychiatry 1995;58:756-764
LETTERS TOTHE EDITOR
Death after ecstasy ingestion: neuro-pathological findings
Ecstasy (3,4-methylenedioxymethampheta-mine; MDMA) is a widely used recreationaldrug that has recently been associated witha syndrome of hyperpyrexia, restlessness,rhabdomyolysis, and acute renal andhepatic failure and at least nine deaths havebeen reported in the United Kingdom.'There are no neuropathological reports ofpatients who died after taking ecstasy.A 30 year old man attended a "rave"
party where he took ecstasy, heroin, andamphetamine. The next day he drank largeamounts of alcohol and was found uncon-scious in a pool of vomit some hours later.He had a convulsion and was admitted tohospital. He was pyrexial (38 5°C), andremained so until his death five weeks later.Creatine kinase was 11 178 IU/l (normal <300 IU/1) on admission and 3468 IU/l fourdays later. He remained comatose and hadno hypertonia, but had occasional gener-alised muscle spasms. A chest infection wastreated with antibiotics. No evidence ofhepatic or renal failure or diffuse intravas-cular coagulopathy was found. Brain CTshowed clearly defined low densities in theglobus pallidus bilaterally.
Postmortem examination showed bron-chopneumonia, lung abcess, and pulmonaryembolism. The brain weighed 1450 g afterfixation. Coronal slices showed clearlydemarcated bilateral necrosis of the globuspallidus (figure). There were small foci ofnecrosis in the white matter.
Histological examination confirmednecrosis of the globus pallidus. There wasintimal proliferation in large blood vesselswithout necrosis or inflammation. The sub-stantia nigra was gliotic. There was mildastrocytic gliosis in the amygdala and hypo-thalamus.The cerebral white matter showed diffuse
gliosis and spongy change without myelindebris or inflammation and sparing only thesubcortical zones. Well defined foci ofnecrosis up to 0 5 cm in diameter wereidentified. The cerebral cortex, hippocam-pus, brainstem, and cerebellum were nor-mal.A major problem in understanding the
Coronal slice of the fixed brain showing necrosisof the globus pallidus bilaterally andfoci ofwhite matter necrosis (arrows).
pathology of this case is that, like most drugabusers, the patient took a combination ofdrugs. Consumption of alcohol may havepotentiated their effects. The most strikingneuropathological change was necrosis ofthe globus pallidus, an area rich in sero-toninergic and dopaminergic nerve termi-nals. Pallidal blood vessels showed changescompatible with prolonged vasospasm, pos-sibly the result of local release of serotoninand other biogenic amines induced byecstasy or amphetamine. Blood vesselchanges have been noted after cocaine andamphetamine abuse.2 The pathology resem-bles that of carbon monoxide toxicity, butsimilar white matter changes are describedin nine cases of heroin abuse.' Damage tothe globus pallidus is found in hypoxic-ischaemic cerebral injury but almost alwaysin association with damage to the hip-pocampus or other areas of the cerebral cor-tex.
Although at least nine deaths after inges-tion of ecstasy have been reported,' neu-ropathological findings have not previouslybeen described. It is important that thesecases be fully studied if we are to improveour understanding of the effects of thesedrugs on the human brain.
M V SQUIERDepartment of Neuropathology,
Radcliffe Infirmary,Oxford OX2 6HE, UK
S JALLOHDepartment of PathologyD HILTON-JONES
Department of Neurology,Milton Keynes General Hospital
H SERIESDepartment of Clinical Pharmacology,
Radcliffe Infirmary,Oxford OX2 6HE, UK
Correspondence to: Dr M V Squier.
1 O'Connor B. Hazards associated with therecreational drug "ecstasy". Br J Hosp Med1994;52:507-14.
2 Klonoff DC, Andrews BT, Obana WG.Stroke associated with cocaine use. ArchNeurol 1989;46:989-93.
3 Wolters ECh, Stam FC, Lousberg RJ, VanWijengaarden GK, Rengelink H, SchipperMEI, Verbeeten B. Leucoencephalopathyafter inhaling "heroin" pyrolysate. Lancet1 982:ii;1233-237.
Lewy body dysphagia
Swallowing disorders are encountered withincreasing frequency in elderly people.'Swallowing depends on the complex inter-play of sensory pathways from the tongue,mouth, pharynx, and larynx (cranial nervesV, VII, IX, X) with coordinated autonomic,voluntary, and reflex contractions involvingcranial nerves V, VII, X, XI, and XII. It istherefore not surprising that dysphagiacomplicates a variety of neurological disor-ders, many of which are more common inthe elderly population, such as pseudobul-bar palsy due to cerebrovascular disease.' Itis, however, seldom the sole presentingfeature of neurological disorders.'We describe two patients with isolated
painless progressive dysphagia who at neu-ropathological examination showed severeneuronal loss, Lewy bodies, and dystrophicneurites in the dorsal vagal nuclei, with onlya few Lewy bodies in the substantia nigra,nucleus basalis of Meynert, and cerebralcortex. These patients represent a new pre-sentation of Lewy body-associated disease.
Patient 1 was an 80 year old retired manwho developed painless progressive dyspha-gia for solids, and to a lesser extent liquids,over a two month period. He described dif-ficulty initiating the swallow, with regurgita-tion of food (solids more than liquids) fromthe upper oesophagus or pharynx. He lost6 kg in weight over this period. His appetitewas normal and there was no vomiting orhaematemesis. Five years earlier a pepticulcer had been diagnosed at endoscopy andsuccessfully treated with ranitidine. Twoyears earlier he developed a mild left oculo-motor nerve palsy of unknown cause. Hetook senna and fybogel for constipation,propranolol (40 mg twice daily) for long-standing paroxysmal supraventricular tachy-cardia, and temazepam as a hypnotic.
Examination was unremarkable exceptfor the presence of a partial left oculomotorpalsy. In particular there was no evidence ofParkinson's disease or cognitive impair-ment.
Endoscopic examination showed noabnormality in the stomach or oesophagus.A limited barium swallow showed theoesophagus to be slightly dilated with aminor hold up of barium at the oesophago-gastric junction. Computed tomography ofthe chest was normal.He developed fatal bronchopneumonia
while in hospital.Patient 2 was an 88 year old woman who
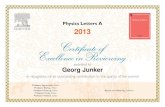
developed painless progressive dysphagiafor solids more than liquids over threemonths. After swallowing, food was imme-diately regurgitated from the pharynx oroesophagus. There was no regurgitationafter the meal was completed. Appetite wasnormal and she had no nausea or vomiting.She had lost 12 kg in weight over the pre-ceding three months. One month before theonset of dysphagia, she had suddenly devel-oped mild pyramidal weakness of the leftarm, which was diagnosed as a stroke. Shewas otherwise well, took no medication, andlived an independent life.
.; ,. a f
AS _ > Q * . .,.'; S.' . . .'_ '...: . ' .. f' g .. ' li
.. }
#. W<i-. s a.
N
... t.8# zi..
,, s ....... r .', j: _.:
.. i.4 v:.
,* 9
.i t.
¢.K
b. ...
.. ......
- e FJlli
ir S4k,, .jt
H:.s
.:.s
b. # .... ^: .r
B:... : Ju:s +.
.: :d.::A,,
.::,.XtW,:.e .. ...KrreN i..:ffn.:, . 4 ,
$'i
Figure 1 Swollen cell in dorsal vagal nucleusfrom patient 2 showing Lewy body(haematoxylin and eosin). Bar = 100 pm.
756 on M
arch 23, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.58.6.756-a on 1 June 1995. Dow
nloaded from

Letters tO the Editor
* I
N
AN~~~~~~(
Figure 2 Swollen cell in dorsal vagal nucleusfrom patient 2 showing Lewy like serpiginouseosinophilw inclusions (haematoxylin andeosin). Bar = 200ima
General examination showed a frailwoman with mild aortic sclerosis. She hadmild pyramidal weakness affecting the leftarm, but neurological examination wasotherwise normal, with no evidence ofParkinson's disease or cognitive impair-mentA barium swallow examination showed
no obstructing lesion in the oesophagus buta paucity of peristalsis, and some tertiarycontractions compatible with her age.
She died from bronchopneumonia whilein hospital.
In both brains there was severe neuronalloss with ubiquitin immunoreactive dys-trophic neurites and Lewy bodies in bothdorsal vagal nuclei (figs 1-4). Scanty Lewybodies, without appreciable cell loss, weredetected in the substantia migra, nucleusbasalis of Meynert, and the cerebral cortex.There was no pathology in the hypoglossal
nuclei and nuclei ambiguus. This dorsalvagal nuclear pathology has been describedin idiopathic Parkinson's disease and diffuseLewy body disease.3No neuropathological basis for the partial
oculomotor palsy in patient 1 was found. Asmall infarct in the right, posterior internalcapsule was found in patient 2.Lewy bodies are spherical, eosinophilic,
ubiquitin immunoreactive neuronal inclu-sions.2 They are found particularly inmonoaminergic and cholinergic neurons ofthe brainstem, diencephalon, basal fore-brain, and cerebral cortex.2 Kosaka and col-leagues were the first to draw attention tothe possibility that neurodegenerative dis-eases associated with Lewy bodies can beconsidered to form a disease range based onthe number and distribution of Lewy bod-ies.3 At one end of the range they placedpatients with Lewy bodies apparently con-fined to the substantia nigra causing idio-pathic Parkinson's disease. At the other endare patients with many and widespreadLewy bodies, including Lewy bodies in thecortex associated with a parkinsoniandementia syndrome referred to as diffuseLewy body disease or Lewy bodydementia.2 Both of our patients showedsevere neuronal loss from the dorsal vagalnucleus, with Lewy bodies in many remain-ing neurons, and dystrophic neurites.Elsewhere, scanty Lewy bodies, withoutsignificant neuronal loss were found inthe substantia nigra, nucleus basalis ofMeynert, and cerebral cortex. WhereasLewy bodies, neuronal loss, and dystrophicneurites in the dorsal vagal nucleus are welldescribed in idiopathic Parkinson's diseaseand diffuse Lewy body disease, they havenot previously been described as the princi-pal neuropathological finding in the absenceof clinical dementia or parkinsonism.2The dorsal vagal nucleus provides pre-
ganglionic parasympathetic innervation tothe oesophagus, as well as other thoracicand abdominal viscera. Although there areno reports of idiopathic Parkinson's diseasepresenting with isolated dysphagia, thissymptom is nevertheless a common featurein both idiopathic Parkinson's disease anddiffuse Lewy body disease, and patients
04..
-....'
I
s.
- . sCr
F, 4.*r e} /
.'W . 4
0 * .-3 *
I0
N,. ...4.1.
0'
Z,-.0 .t
r 41.l-
Figure 3 Abundant ubiquitin-immunoreactive neurites in(antiubiquitin haematoxylin). Bar = 40 /lm.
1410.1 IM,
I 0X
q-.f4'o it
tp %
0 01)1, (N ... '.. 0
-P
to. . *
0
.r o
fp
V" 4b
.S,
dorsal vagal nucleus from pat
Z ;.. .K;.-..
J
Figure 4 Classic Lewy bodies in nigralneuron, patient 1 (haematoxylin and eosin.Bar = SO prn.
with idiopathic Parkinson's disease com-plain of dysphagia far more often than doage matched subjects.4 There is a generalcorrelation between the severity of swallow-ing dysfunction and the severity ofthe Parkinson's disease. In idiopathicParkinson's disease, dysphagia is most com-monly clinically localised to the oropharynx,and solids cause greater difficulty thanliquids.5 A variety of motor abnormalitiesin the oesophagus have, however, beendescribed in Parkinson's disease, includingdysmotility, dilatation and pseudodi-verticula. A recent study by Edwards andcolleagues has shown that patients withidiopathic Parkinson's disease do nothave any single characteristic video-oesophagraphic abnormality.5
Several possible explanations have beenput forward in the pathogenesis of theseproblems including degeneration of thedorsal vagal nucleus, peripheral dopaminedepletion, Lewy body formation in themyenteric plexus, and disordered neuro-muscular junction transmission.5Lewy body associated diseases can there-
fore present as idiopathic Parkinson's dis-ease, a parkinsonian dementia, isolateddementia, and now dysphagia.2 In thesepatients we speculate that had pneumonianot developed, they would probably havedeveloped idiopathic Parkinson's disease asthe nigral involvement became more severe.
MATTHEW JACKSONGRAHAM LENNOXDepartment ofNeurology
MARGARET BALSITISJAMES LOWE
Department of Pathology,University Hospital,
Queen's Medical Centre,Clifton Boulevard, Nottingham NG7 2UH, UK
Correspondence to: Dr James Lowe, Departments of Pathology, University Hospital, Queen's
Medical Centre, Clifton Boulevard, NottinghamNG7 2UH, UK.
1 Wald A. Understanding the pathophysiologyof dysphagia and constipation in neurologicdisorders. Am J Gastroenterol 1994;89: 1-3.
2 Lowe J. Lewy bodies. In: Calne DB ed.tient 1 Neurodegeneration. Philadelphia: WB
Saunders and Co, 1994:51-69.
757
D.
1.:IV.,- 1. .k
qb
.ia-.j.-I
10
v.. 0, 4
Xp
on March 23, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.58.6.756-a on 1 June 1995. D
ownloaded from

Letters to the Editor
3 Kosaka K, Matsushita M, Oyanagi S,Mehraein P. A clinicopathological study ofthe "Lewy body disease". Psychiatria etNeurologiaj7aponica 1980;82:292-311.
4 Edwards LL, Pfeiffer RQ, Quigley EMM, etal. Gastrointestinal symptoms in Parkinson'sdisease. Mov Disord 1991;6:151-6.
5 Edwards LL, Quigley EMM, Hamed RK,Hofman R, Pfeiffer RF. Characterisation ofswallowing and defecation in Parkinson'sdisease. Am Jr Gastroenterol 1994;89:1525.
Local IgG production in aqueoushumour in patients with idiopathicuveitis compared with MRI findings
We have previously reported an increasedconcentration of antibody to measles in theaqueous humour of patients with multiplesclerosis related uveitis.' We further found ahigh frequency of asymptomatic multiplesclerosis-like lesions on MRI of the brain ofpatients with idiopathic uveitis.2 There wasa significant association between MRIlesions and high aqueous humour andblood concentrations of antimeasles anti-bodies.3The local production of oligoclonal IgG
in the CNF has long been considered as apathognomonic characteristic of multiplesclerosis, and also a good biological aid toits diagnosis.4 Oligoclonal production ofIgG has also been suspected in the aqueoushumour of patients with multiple sclerosis,on the basis of the ratio between albuminand IgG contents in both aqueous humourand serum.'
This study was aimed at determining ifthe presence of white matter MRI lesions inpatients with uveitis was linked to anincreased content of IgG in the aqueoushumour, and if this increase could beexplained by the high concentration ofantimeasles antibodies in the aqueoushumour.
Sixty eight patients with idiopathic uveitis(23 males, 45 females, aged 15-49), all freeof neurological symptoms, diabetes, andblood pressure problems, were submitted toboth a brain MRI examination and a sam-pling of blood and aqueous humour. Allpatients gave informed consent to their par-ticipation in this study.The presence of white matter lesions on
MRI was determined in each patient bythree independent radiologists according toPaty's multiple sclerosis diagnosis scale.6
Samples of aqueous humour and bloodwere assayed for albumin and total IgG bylaser nephelometry and measles virus, her-pes simplex virus (HSV), varicella zostervirus (VZV), and cytomegalovirus (CMV)specific IgG by enzyme linked immunosor-bent assay (ELISA). The following coeffi-cients were calculated': albumin quotient =aqueous humour albumin/serum albumin;IgG quotient = aqueous humour IgG/serum
IgG; IgG index = IgG quotient/albuminquotient.The values of these three coefficients as
well as optical densities in aqueous humourfor each of the four virus assays were com-pared in patients with lesions on MRI(MRI +) and those without (MRI -) byWilcoxon's test. Partial Spearman correla-tions were calculated to assess if the relationbetween the local IgG production coeffi-cients and MRI was related to a specificviral expression.The results showed an association
between the presence of brain lesions andhigh ocular IgG production as representedby the IgG quotient (P = 0-002; table).Albumin quotient did not differ significantlybetween the groups and the association wasdue to differences in the values of the IgGquotient (P < 0 05).
Moreover the measles optical density inaqueous humour of MRI + patients wassignificantly higher than that of MRI-patients. (P < 0 0001). We did not find adifference in VZV, HSV, or CMV opticaldensities between the groups. The values ofthe measles optical density in aqueoushumour were significantly correlated withboth IgG quotient (P < 0-01) and IgGindex (P = 0 04). Finally, when adjustingfor the effect of measles optical density inaqueous humour, the partial correlationbetween IgG index and MRI remained sig-nificant (P < 0 05).The well documented relation between
multiple sclerosis and uveitis is difficult toevaluate from a clinical point of view.Asymptomatic forms of ocular inflamma-tion have been variously described in multi-ple sclerosis. The local production of IgG inthe CSF of patients with multiple sclerosisis also well documented.4 White matterlesions on MRI of the brain are present invarious inflammatory diseases, but speciallymultiple sclerosis.The aim of this study was to check if the
IgG concentration was increased in theaqueous humour of patients with idiopathicuveitis. The albumin quotient measures themodifications of the blood ocular barriersand by comparing both albumin and IgGquotient, the local production of IgG (IgGindex) can be evaluated. The associationbetween a high IgG index in aqueoushumour and the presence of white matterlesions in patients with idiopathic uveitisand without neurological symptoms mightbe a phenomenon similar to the localincrease in the IgG index in the CSF ofpatients with multiple sclerosis.Our study is based on a quantitative mea-
sure of IgG production that is less sensitivethan the qualitative measure of oligoclonalIgG. We think, however, that the largenumber of patients studied compensates forthe lower sensitivity of our measures, com-pared with studies based on qualitativemeasures that involve a smaller number ofpatients.The common presence of measles anti-
bodies in the CSF of patients with multiplesclerosis is well known.7 After adjusting forthe values of measles optic density in aque-ous humour, the correlation between IgGindex and MRI remained significant. Thisindicates that measles optical density inaqueous humour and IgG index are posi-tively linked with MRI but the link betweenIgG index and MRI lesions is only partiallyexplained by the link between measles opti-cal density in aqueous humour and MRI. Ifmeasles has a role in the origin of multiplesclerosis and multiple sclerosis relateduveitis, it may not be the only contributingfactor.
We acknowledge the Association pour laRecherche sur le Sclerose en Plaques (ARSEP).
SERGE KOSCIELNYDipartement de statistiques midicales,
Institut Gustave Roussy,Villejuif, France
PHILIPPE THULLIEZLaboratoire de la toxoplasmose,
Institut de Puiriculture,Paris, France
EMMANUEL-AIAIN CABANISMARIE-THER.ESE IBA-ZIZEN
Service de Neuroradiologie,CHNO des quinze-vingts, Paris, France
ELISABETH DUSSAIXLaboratoire de Virologie,
CHU Bicetre,Le Kremlin Bic&tre, France
ETIENNE BLOCH-MICHELCLAUDINE TRICHET
LAURENT HELLEBOIDUniti d'immunologie oculaire,
CHU Bicitre,Le Kremlin Bicetre, France
Correspondence to: Dr E Bloch-Michel, United'immunopathologie oculaire CHU de Bicetre,Faculte de medecine Paris Sud, Le KremlinBicetre, France.
1 Bloch-Michel E, Helleboid L, Hill C,Koscielny S, Dussaix E. Measles virus anti-body in aqueous humour of patients withuveitis associated with multiple sclerosis.Lancet 1992;339:750-1.
2 Bloch-Michel E, Iba-Zizen MT, Koscielny S,et al. MRI and idiopathic uveitis in:Dernouchamps JP, Verougstraete C,Caspers-Velu L, Tassignon MS, eds. Recentadvances in uveitis. Amsterdam: Kugler,1993:459-60.
3 Helleboid L, Dussaix E, Tounzi Y, ThulliezKoscielny S, Bloch-Michel E. The role ofneurotropic viruses in the etiology of uveitis.In: Demouchamps JP, Verougstraete C,Caspers-Velu L, Tassignon MS, eds. Recentadvances in uveitis. Amsterdam: Kugler,1993:253-6.
4 Waksman BH. Multiple sclerosis. Curr OpinImmunol. 1989:1:733-9.
5 Quentin CD, Reiber H. Intraocular immuno-globulin G production in patients withperivasculitis of the retina and multiplesclerosis. In: Secchi AC, Fregona IA, eds.Modem trends in immunology and immuno-pathology of the eye. Milano: Masson,1989:214-6.
6 Paty DW, Oger JJF, Kastrokoff LF et al.MRI in the diagnosis of MS. Neurology1988;38: 185.
7 Felgenhauer K, Schadlich HJ, Ackerman R.Cerebrospinal fluid virus antibodies: adiagnosis indicator for multiple sclerosis.JNeurol Sci 1985;71:291-9.
Local production coefficients in MRI+ andMRI- patients with uveitis
MRI+ (n = 21) MRI- (n = 47) Pvalue*
Albumin quotient 0 007 (0-003-0-011) 0-006 (0-003-0013) NSIgG quotient 0-008 (0 006-024) 0-004 (0-002-0-011) 0-02IgG index 1-33 (0 72-2 67) 0 74 (0-43-1-00) 0-002
*Wilcoxon test.Results are medians (25th and 75th percentiles).
Central nervous system demyelinationafter vaccination against hepatitis Band HLA haplotype
Although very unusual, acute CNS compli-cations may occur after vaccination againsthepatitis B.' We report a patient with evi-dence of severe demyelination in the CNSafter hepatitis B vaccination.
758 on M
arch 23, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.58.6.756-a on 1 June 1995. Dow
nloaded from