
Lessons Learned: Implementing Practices to Improve CLABSI ... · Organizational learning can be...
13
magazine.nationalpatientsafetyfoundation.org http://magazine.nationalpatientsafetyfoundation.org/magazine/spring2013-lessons-learned-improve-clabsi-rates/ Lessons Learned: Implementing Practices to Improve CLABSI Rates On Jun 10, 2013 Children’s Hospital of Philadelphia Home Care invested time and focused, sustained efforts in implementing the World Health Organization’s Five Moments for Hand Hygiene as part of a safety initiative in reducing its CLABSI rate. Implementation resulted in a reduction in infection rates; lessons learned; best practices and changes in mental models, such as a redefinition of “team”; and system-level changes such as innovative, coordinated, community-level educational outreach. by Verna Cole, PhD, & Kelly Monacella-Duffy, MSN, RN Introduction Patient care is delivered by systems as well as by the individuals utilizing them; patient saf ety improvement must include individual, group, and organizational learning (Edmondson and Moingeon 1998). Few organizations share their experiences with other health care entities on recursive steps and successf ul strategies identif ied as part of their organizational learning while implementing patient saf ety initiatives. This article highlights the individual, collective, and organizational learning achieved as Children’s Hospital of Philadelphia (CHOP) Home Care implemented new initiatives f or inf ection control targeted at decreasing central line-associated bloodstream inf ections (CLABSI). Through surveys and semi-structured interviews with f ield nurses, their immediate supervisors, and department leaders, a qualitative study of home care nurses’ experiences during this implementation was conducted. Four initial surveys and 10 interviews were completed. The interviews detail staf f understanding of how f ront-line experiences were moved f rom lessons learned to best practices to system-based practice. The implementation of a practice change is a process that takes ef f ort and time. Organizational learning is particularly relevant during all stages of implementation because processes such as inf ormation transf er, skilled management of the change process in specif ic settings, and in-depth understanding of the dynamics at play are needed to ensure adequate time, f ocus, and attention to resource management in supporting continuous improvement while limiting risk, and monitoring f or unintended consequences. Background Patient saf ety is the application of saf ety science methods toward a health care delivery system to minimize saf ety incidences and adverse events (Emanuel et al. 2008). A culture of saf ety comprises numerous f actors and may include the healthcare agency’s ability to: 1) integrate individual and group learning f rom patient saf ety initiatives with current policies, processes, and practices; and 2) improve, spread, and sustain the changes (Jones et al. 2008). Essentially, the way organizational learning is managed af f ects the adoption of initiatives, the rate of improvements, and organizational perf ormance (Edmonson et al. 2006). Organizational learning can be def ined as “developing the capacity to transf er knowledge across the
-
Upload
nguyenkiet -
Category
Documents
-
view
215 -
download
0
Transcript of Lessons Learned: Implementing Practices to Improve CLABSI ... · Organizational learning can be...
magazine.nat io nalpat ient saf et yf o undat io n.o rghttp://magazine.nationalpatientsafetyfoundation.org/magazine/spring2013-lessons-learned-improve-clabsi-rates/
Lessons Learned: Implementing Practices to Improve CLABSIRates
On Jun 10, 2013
Children’s Hospital of Philadelphia Home Care invested time and focused, sustained efforts in implementing theWorld Health Organization’s Five Moments for Hand Hygiene as part of a safety initiative in reducing its CLABSIrate. Implementation resulted in a reduction in infection rates; lessons learned; best practices and changes inmental models, such as a redefinition of “team”; and system-level changes such as innovative, coordinated,community-level educational outreach.
by Verna Cole, PhD, & Kelly Monacella-Duffy, MSN, RN
Introduction
Patient care is delivered by systems as well as by the individuals utilizing them; patient saf ety improvementmust include individual, group, and organizational learning (Edmondson and Moingeon 1998). Feworganizations share their experiences with other health care entit ies on recursive steps and successf ulstrategies identif ied as part of their organizational learning while implementing patient saf ety init iatives. Thisarticle highlights the individual, collective, and organizational learning achieved as Children’s Hospital ofPhiladelphia (CHOP) Home Care implemented new init iatives f or inf ection control targeted at decreasing centralline-associated bloodstream inf ections (CLABSI).
Through surveys and semi-structured interviews with f ield nurses, their immediate supervisors, and departmentleaders, a qualitative study of home care nurses’ experiences during this implementation was conducted. Fourinit ial surveys and 10 interviews were completed. The interviews detail staf f understanding of how f ront- lineexperiences were moved f rom lessons learned to best practices to system-based practice.
The implementation of a practice change is a process that takes ef f ort and time. Organizational learning isparticularly relevant during all stages of implementation because processes such as inf ormation transf er,skilled management of the change process in specif ic settings, and in-depth understanding of the dynamics atplay are needed to ensure adequate time, f ocus, and attention to resource management in supportingcontinuous improvement while limiting risk, and monitoring f or unintended consequences.
Background
Patient saf ety is the application of saf ety science methods toward a health care delivery system to minimizesaf ety incidences and adverse events (Emanuel et al. 2008). A culture of saf ety comprises numerous f actorsand may include the healthcare agency’s ability to: 1) integrate individual and group learning f rom patient saf etyinit iatives with current policies, processes, and practices; and 2) improve, spread, and sustain the changes(Jones et al. 2008). Essentially, the way organizational learning is managed af f ects the adoption of init iatives,the rate of improvements, and organizational perf ormance (Edmonson et al. 2006).
Organizational learning can be def ined as “developing the capacity to transf er knowledge across the
mccaffertyl
Text Box
This article originally appeared in Patient Safety InSight (spring 2013) published by the American Society of Professionals in Patient Safety at the National Patient Safety Foundation. It is used here with permission.
mccaffertyl
Sticky Note
Accepted set by mccaffertyl

organization, to share expertise and inf ormation while purposef ully, continually adapting and growing together(Rowley and Poon 2010). It encompasses f ive core disciplines: systems thinking, team learning, shared vision,mental models, and personal mastery (Senge 1990).
CHOP Home Care’s Inf ection Prevention & Control Program provides surveillance and guidelines f or theprevention and control of the spread of inf ectious pathogens to patients, caregivers, and health prof essionalsin the home care setting. Since 2009, the goal f or CHOP Home Care’s CLABSI rate has been f ewer than 2inf ections/1,000 line days. CHOP Home Care’s perf ormance has shown progress and sustained improvementf or several years. Progress is attributed to standardized practices, as outlined in CHOP’s policy andprocedures, consistency in practice by all clinicians, and patient/f amily education on central- line management.
Moments for Hand Hygiene
Preventing health care associated inf ections in the home care environment presents unique challenges. Unlikeinpatient or ambulatory settings, home care relies heavily on a combination of f amily and other caregivers,potentially result ing in a complex mix of instructions and varying care philosophies. Patients and f amilies can beoverwhelmed when they are expected to manage the care of a sick child at home. Some f amilies are preparedand comf ortable, but many need round-the-clock support to ensure success. Amy Gallagher, CHOP HomeCare’s director of Clinical and Patient Care Services, describes the unique challenges that home care staf fnavigate daily:
Our clinicians have no control in the home. The home is the patient’s environment. We don’t have control overwho’s going to touch the line. Our goal in home care is to try to create a normal home environment while stilltrying to manage a central line. . . . In some f amilies, up to f our members could be involved in that child’s careand touching that line. To me, the risk of developing a CLABSI is much greater because of the unknown thathappens in the home every day.
For these very reasons, repetit ive education and consistent care at every visit and f rom each clinician areessential. Consistency in clinical practice f or sterile procedures and hand hygiene provides a clear message tof amilies that care provided in the home is a reliable extension of the excellent care CHOP delivers in theoutpatient setting.
In 2011, CHOP introduced the World Health Organization (WHO) hand hygiene guidelines and other well-researched practices to the enterprise. CHOP’s inf ection control committee implemented evidence-basedchanges to its sterile dressing change procedure with return demonstration by all clinicians across theorganization. Site scrub and dry t imes were increased, and a separate sterile cap change kit was introduced.Although f orms of these procedures were already in place, they were modif ied based on evidence supportingdecreased inf ection rates. CHOP Home Care management f ormally educated the staf f about the new inf ectionprevention init iative. This was f ollowed by an evaluation of CHOP Home Care nurses’ sterile technique andprocedural compliance by supervisors during home visits. CHOP Home Care implemented several widelyaccepted best practices combining behaviors and technology as part of their goal to decrease CLABSI f urther(Moureau 2009). The most dramatic change to care was the introduction of the WHO hand hygiene protocol.
CHOP f ocused on how hand hygiene was being delivered by all health care workers. The Home CareDepartment, along with the hospital, adopted the WHO inf ection control program tit led My Five Moments f orHand Hygiene [Figure 1]. These WHO recommendations and hand hygiene best practices are considered thegold standard f or health care worldwide. Although these best practices were developed primarily f or hospitalsettings, Sax et al. (2007) describe themas appropriate f or home care staf f in providing a user-centered f ocuson quality inf ormation and training around hand hygiene.
The WHO approach to hand hygiene requires application of three primary concepts and two strategies. The

Fig ure 1: My 5 Mo me nts o f Hand Hyg ie ne (Wo rld He alth Org anizatio n). Click to e nlarg eg rap hic
Fig ure 2: Ho w to Hand rub (Wo rld He alth Org anizatio n). Click to e nlarg e imag e .
primary concepts are moments, patient zones, and hand rubbing. The strategies are f ormalized hand hygienesteps and delineated patient zones. Home Care developed education to support and train staf f on theseconcepts and strategies.
Implementing the WHO approach requires understanding key concepts. Moments are def ined as geographicalor patient care situations indicating when hand hygiene is required.
Patient zones ref ers to thepatient and the geographicalsurroundings that contain thepatient’s normal f lora (WHO2012).
Proper hand washing meansf ollowing prescribed steps, inthe correct order and f or theproper duration recommended.An alcohol-based hand sanitizersolution is worked f rom thepalms to the back of the hands,through interlaced f ingers, toback of f ingers, then thumbs,and f inally the f ingertips. It is af ormalized process with sixdistinct steps [See Figure 2,below].
Historically, clinicians wereinstructed to use soap andwater f or 1–2 minutes bef orepatient contact with minimalf ocus on technique. In 2004,The Joint Commission added aNational Patient Saf ety Goalrequiring compliance with handhygiene guidelines f romaccredited health careorganizations. In 2005, WHOlaunched the First Global PatientSaf ety Challenge f ocusing onthe central role of hand hygienecompliance on reducinginf ections. In 2009, WHOreaf f irmed the recommendeduse of soap and water whenhands were visibly soiled andalcohol-based hand rubs whenhands were not visibly soiled.Standardization of handwashing and expectedadherence to both when and

Fig ure 3: WHO g rap hic o f aco ntaminate d hand
how hand washing occurs is relatively new.
Typical hand washing practice did not include the standardized six steps in a precise sequence and at preciseindications. In an ef f ort to promote continuous quality improvement, decrease our CLASBI rate, and promotehand hygiene compliance, our clinicians at CHOP needed to adopt the standardized practices. This required re-education f or a basic ref lexive process of hand washing, which involved a several-pronged approach in orderto impact the thought process f or this concept while delivering care autonomously in the community. Directoversight would not occur in the same manner as in the inpatient setting. A home-care-specif ic rollout wascrit ical to implementation. The unique setting of the home brought challenges that needed to be addressed f orclinicians. Our policies provide the standard f or clinicians, but the environment is not controlled by staf f .
Families are taught inf ection control principles and given education on how to prevent inf ection. They have astrong desire to keep their child healthy, but many competing priorit ies can make vigilance dif f icult at t imes. Ourexpectation is that the clinician is doing hand hygiene at the right t ime every time in the home, whether we arepresent f or direct oversight or not. In addition, clinicians are providing education to the f amilies f or handhygiene at each and every visit.
Organizat ional Learning
In high-risk environments, individual, team, and organizational learning are strategically important skill sets.Organizational learning consists of three stages: 1) knowledge acquisit ion; 2) knowledge sharing; and 3)knowledge utilization (Nevis et al. 1995).
Knowledge Acquisition
Knowledge acquisit ion f or CHOP Home Care was accomplished by interdisciplinary staf f education. DuringCHOP’s inf ection reduction init iative, department managers f or nursing, respiratory therapy, and pharmacyimplemented joint learning activit ies.
Supervisors led f ormal education sessions, in the f orm of a Skills Lab, to teach new hand hygiene techniques.The Skills Labs f ocused on perf orming all six steps, in the correct order, every time during a home visit, andstressed the moments and patient zones. Supervisors then monitored the proper implementation of these skillsduring home visit observations.
Ref erence documents were also integral to successf ul implementation.Managers provided staf f with a variety of graphics f or use as ref erence tools.Staf f described two WHO graphics, the picture of a contaminated hand [Figure3, at right] and a diagram of the 6-step hand rub [Figure 2], as extremely usef ul.Staf f ref erred repeatedly to these as “easy to carry, easy to ref er to, easy toread.”
Adopting the new practice required time and f ocused ef f ort. Fostering explicitknowledge included providing resources, meeting time, and opportunit ies f orrepetit ive, individual practice with immediate, individual f eedback during skillsvalidation and supervisory visits. Managers and supervisors required andmotivated staf f to persist in changing their practice. Staf f were individuallyengaged through strategies such as ready access to usef ul inf ormation,ongoing recognition and reinf orcement, and captivating questions. Collective communication tools—including astandardized e-mail model, using, f or example, the ISBARQ (introduction, situation, background, assessment,recommendation, Q&A) method, to reduce communication errors and increase patient saf ety, monthly e-mailreports on inf ection rates per line days with patient specif ic inf ection reports, saf ety stories at the start of

Fig ure 4: Pause fo r the Cause . Click to e nlarg e .
department meetings, and f ollow-up e-mails with meeting minutes—were consistently used to maintainheightened awareness and provide education in the moment.
For new staf f , the init iation process includes multiple opportunit ies to learn hand hygiene procedures with aqualif ied clinician, return demonstration in a controlled setting, and demonstration in the home visit during theorientation period. New staf f orientation includes skills validation and skill integration during supervised homevisits, where emphasis on repetit ive practice and application in the context of the home with immediatef eedback by a preceptor is standard practice.
Implementing the WHO hand hygiene activit ies presented staf f with two types of learning challenges. First, theyhad to unlearn their previous practice. Unlearning took more time f or staf f than anticipated. At f irst, many f eltthe steps were counter- intuit ive in their workf low. The Webster ’s dictionary def init ion of “unlearn”—“to put outof one’s knowledge or memory [or] discard the habit of ”—presents its own challenge. Unlearning meant staf fspent t ime ref raming a new understanding of hand hygiene. Previously, staf f reported “using a good amount[of alcohol rub] and ensuring hand hygiene was done of ten.” To counter this mindset, Home Care leaders usedWHO’s evidence-based guidelines coupled with standardization, to motivate staf f away f rom their f amiliarhabit, toward a consistent six-step process.
Back to top
The second learning challenge related to thedemonstration of f luency f or two very dif f erent types ofskills. Hand washing is a skills-based task and requiresless time f or thought than addressing patient zones inthe home, which is a rule-based task. Rule-based tasks,or “if - then” tasks, require a higher degree of consciouscontrol (Reason 1990). In the case of hand hygiene,clinicians must f irst observe and determine a true momentf or hand hygiene, then select a course of action, andf inally execute or def er hand hygiene. [See Figure 4, atright]
Incorporating patient zones required more time f orthought and remained a challenge f or some nurses. Theydid not distinguish between the time needed to internalizea skills-based task and that needed to internalize a rule-based task, and were puzzled by their struggle withautomating patient zones (or their practices).
One nurse commented:
Af ter 13 years of nursing, delivery of care had become a natural f low. The new process interrupted every singletask I ever learned. I was interrupted by internal ref lection: Do I have to wash? Learning patient zones hastaken more time than re- learning hand washing. When we started this [init iative] it became evident that we werewashing all the time. Now the times I’m told NOT to wash f eels dif f erent and dif f icult. —Field nurse
Historically, hand hygiene protocol dictated doing it well and often. Clinicians used individual judgment to deemwhen hand hygiene was necessary. For this init iative, clinicians now needed to “f lip the switch” to make thechange successf ul. Rapid identif ication of moments f or hand hygiene, as determined by situation and patientzones in the home, required time, f ocused attention, coaching, and ref lective practice with valid f eedback, untilnurses developed a repertoire to easily draw upon (Haskell 2001). Staf f verbalized their experience withinternalizing the process:
Hand hygiene generally doesn’t interf ere with care delivery, but if I’m working with a child with complex needs or

in a chaotic environment, I need to pause, ref lect, and f ocus, to determine if hand hygiene is indicated. –Field nurse
Patient zone identif ication was an evolving process as situations presented in the home care environment.Staf f worked with leadership as questions arose. With f ocused practice and descriptive f eedback, handhygiene became second nature, with staf f demonstrating f luency with the six steps, allowing them to f ocus ontheir environment and identif y patient zones. The outcome was decreased f requency of hand hygiene with astandardized, evidenced-based technique.
Staf f demonstrated clarity around the purpose of the changes and motivation f or persistence with the newpractice:
We have kids who are at higher risk of inf ection and lower resistance. Most of our patients on IV’s are f ragile.We have to f igure out why they’re getting inf ected and doing that means eliminating the caregiver as thesource of the inf ection. We go step-by-step, hand washing longer, but washing f ewer t imes. – Home Carenurse
Knowledge Sharing
The second step in organizational learning is knowledge sharing, which includes activit ies designed to blendknowledge (Nonaka and Takeuchi 1995) and storytelling (Hutchens 2009). Both of these strategies are anormal part of a home care nurse’s routine.
Nurses’ comments depicted home care as an environment where they openly and collectively blended explicitknowledge of hand hygiene with tacit knowledge of the patient population, the uniqueness of each home, andf amiliarity with each other as they collectively worked to ef f ect saf e patient outcomes. Sharing of tacitknowledge and experiences occurred primarily through f ormal and inf ormal clinician contact (Bransf ord et al.2000), such as meetings with peers, phone calls to each other as questions arose, and as staf f stopped in theHome Care of f ice. This collaborative process was essentially teamwork. It was also the means by whichindividual learning was transf erred to the organization and captured in enhanced procedures related to central-line management in home care.
For this init iative, CHOP added a sterile cap change kit. Previously, a sterile cap was added to the steriledressing change procedure. This new practice added another sterile set-up in the home, where the availabilityof useable surf aces can prove challenging. Staf f collaboration (teamwork) was a reoccurring theme duringtroubleshooting discussions about this change.
Nurses viewed teamwork as group review with interchanges of issues, ideas, and practice:
I make phone calls to other nurses around issues or patient concerns. As we talk, ideas are triggered. It ’simportant to talk with each other. For example, I was able to come up with a creative strategy to encourage apatient to wear her mask during dressing change. Then I shared the strategy with the next scheduled nurse toensure a unif ied approach. I f irst worked hard to get Mom on board. She needed to agree that we would allwear masks. Then together we came up with this game f or putting on the mask. – Home Care nurse
Team use of creative strategies can include distraction techniques. Most home care nurses have a comf ortbasket f ull of books, pin wheels, and other gadgets to utilize during stressf ul procedures f or the child. Manychildren will be assistive with procedures if they can take part in the process, such as being in charge of puttingthe mask on their parent bef ore they put on their mask.
A recent hire brought a dif f erent perspective:
Teamwork here is done on a level playing f ield. I always call if I have a question. With this team, not knowing will

Fig ure 5: CLABSI Line Days, CHOP Ho me Care . Click to e nlarg e .
not be held against me. So, I’m not af raid to ask. – Home Care nurse
Storytelling is a well- recognized patient saf ety practice and an ef f ective strategy f or sharing knowledge.Members of Home Care’s leadership team point readily to memorable stories that promote saf ety. One memberrecounted there are generally two types of stories: best-practice and near-miss stories:
We started sending out e-mails about best practices. They may be scenarios that we see, or something wef ind during chart reviews or during supervisory visits, or something we learn f rom being copied on an e-mail,and we put it out there. It shows how the process is being applied to patient care. When we see or hear of aninstance where we have made a posit ive dif f erence, we blast it out to the f ield.
We believe in making mistakes visible. A mistake that doesn’t reach the patient is called a “near miss” and ispublicized. We talk about and report it, which has turned the near miss into “I caught this,” which is a good thingand a powerf ul thing to be involved in. Typically, the person reporting is the person who catches it. He or shewants to help others know how important processes are.– Home Care leadership team member
CHOP Home Care’s goal, to be the saf est children’s hospital home care provider in the nation, requires ablame-f ree culture where staf f openly evaluate missteps. Clinicians are primary providers of inf ormation onsaf ety events. They share stories about what occurs in the home, which enables the care team to ef f ectivelyevaluate our educational, operational, and clinical processes.
Knowledge Utilization
The third and last step of organization learning is knowledge utilization. CHOP Home Care’s CLABSI rate hasdecreased since adoption of the hand hygiene init iative. Our ult imate goal is a continued decrease and eventualelimination of inf ections in the home care central- line population. [See Figure 5, below.]
Knowledge utilization disseminates knowledge gained f rom evidenced-based practice, including lessonslearned f rom practice.
Lessons Learned
Numerous lessons werelearned f rom implementingthis init iative.
1. Implement one init iative ata time and allowsuf f icient t ime f or f luencyin the required skills. Thehand hygiene programwas rolled out at thebeginning of the f iscalyear, which occurs in July,typically a dif f icult t ime togather staf f . The goalsf or f uture init iatives would include ensuring that all staf f are exposed to the required education prior tomoving on to next steps
2. Plan and monitor f or consistent attendance of all clinicians at learning events. Lack of consistentattendance impacts inf ormation sharing and practice. Further, sporadic attendance coupled with

misunderstood inf ormation, in an environment with a strong inf ormal communication system, can have awhisper down the lane ef f ect requiring more work to correct. Planning inf ormation sessions f or all staf fwill decrease time lost to miscommunication.
3. From inception, create an enterprise-wide or department-wide init iative and communicate the messagethat inf ection control is not just f or nurses. Reducing CLABSI includes responsibility on the part of allhome care employees. The emphasis is on points of commonality:
When you think about CLABSI itself , it ’s not just about the nurse. It ’s about the pharmacist that dispensessupplies and medications and needs to understand the entire process related to central- line care because if apatient is asking f or too many supplies, or too f ew, there may be something that the f amily is not doingcorrectly. This is a way f or the pharmacist to f ind out and disclose to the team that something is not quiteright. — Amy Gallagher, Director of Clinical and Patient Care Services
Lessons learned and the init ial outcomes f rom staf f ref lection point to actions and strategies employed insupport of department- and enterprise-wide goals. Transf orming lessons learned into usef ul organizationalknowledge is the goal of the looped learning process.
Single-Loop Learning
Argyris and Schön (1978) def ine single- loop learning as reactive problem solving, error correction, or amanagement by exception approach to issues or individual ref lection (O’Connor and Kotze 2008). Problemsolving is similar to taking corrective action to achieve the desired outcome in that it is limited in solutions andscope of action. Problem solving was an integral part of implementing the new inf ection control init iativesoverall and hand hygiene practices in particular. Individual staf f members regularly applied problem-solvingstrategies to issues f aced while implementing hand hygiene.
The home care setting requires problem solving f or application of procedures and tasks. Clinicians are wellversed in thinking bef ore acting. For example, when the nurse leaves the patient care area and accessesmedications in the home ref rigerator, that nurse is moving to a new patient zone, an action that requires handhygiene to be perf ormed. Clinicians avoided this situation by having f amily members retrieve medications f orthem.
Lessons learned are embedded into standard operating procedures and become shared best practices. Forinstance, the strategy of solicit ing f amily-member help in retrieving medications f rom the ref rigerator wasshared via e-mail as a best practice. It was discussed during clinician meetings, where the strategy was ref inedand incorporated into practice. If the lesson learned required a more signif icant change to practice, then a smallrepresentative workgroup gathered inf ormation and presented to the leadership team f or review and init iationof the process into practice. Ongoing supervisory and patient saf ety visits allow opportunity to revisit thestrategies employed and ensure they work f or clinicians and f amilies. Undoubtedly, maximizing the benef its oflessons learned begins with continual collective ref lection on practice, outcomes, and process.
Crit ical ref lection at all levels is a behavior promoted and supported by CHOP’s culture of saf ety. Ref lectingand resolving are recognized saf ety behaviors that rest on a corporate belief in “practicing with a questioningattitude.” A questioning attitude, or thinking crit ically, is def ined as detecting incorrect data and/or assumptionsthat could lead to erroneous decisions and actions. Ongoing, collective, crit ical ref lection tied to newdef init ions, changes in collective actions, and a generalization of results lies at the heart of knowledgetransf er and double- loop learning.
Back to top
Double-Loop Learning

Knowledge transf er within organizations is the process by which a group or department is af f ected by theexperience of another (Argote et al. 2000). In the simplest f orm, while single- loop learning emphasizes“knowing how” throughout the problem-solving process, double- loop learning emphasizes “knowing why” itimpacts strategies (Goh 1998). Double- loop learning means examining the organization’s design (Nevis et al.1995; Schein 1995) employee skills and competencies, and asking questions such as: Why are solutionsworking? What are our underlying assumptions around our inf ection rates? How are the rates impacted by theenvironment? These are the types of questions posed around lessons learned f rom hand hygiene. Ref lectionon these questions leads to the development of best practices: joint learning and shared leadership.
To create and maintain joint learning and understanding, the CHOP Home Care Department workscooperatively across disciplines on a daily basis. In the words of John Tamasitis, manager of ClinicalOperations and Respiratory Therapy:
We didn’t always operate this way. Right now “Opening” to Home Care service occurs together. Openings usedto occur by discipline. Now the department is scheduled as a team at one visit, and we work collaboratively.
Shared leadership is an ef f ective way of disclosing mental models, values, and assumptions.
Double- loop learning results in increased ef f ectiveness around decision making and shared acceptance ofpossible f ailures and mistakes. Ref lection on the variables that continue to impact our CLABSI rate promptscontinued work with f amilies to create the outcome we desire—f ewer central- line inf ections. CHOP Home Carehas also taken department- level action in re-examining the challenges some f amilies f ace and thinking throughhow we might do things together dif f erently:
Families are taking inf ections seriously. They are giving it t ime and thought when I am teaching. But sometimesit’s very hard. Like the mother who is f ighting an uphill battle because multiple f amily members provide care, sothere is a range of mindf ulness to the potential of risk of inf ection. That varies with f amily members. Themother ’s 16-year-old son also provides care. That’s just the reality of it.—Home Care nurse
We talk with the parents and share what works. We ask a lot of questions. We do handof f s. We take a lot ofresponsibility f or it, but we are in the home approximately two hours per week. The unknown variables arethere and are outside of our control.—Home Care supervisor
The ways in which individuals and departments exchange relevant inf ormation can make double- loop learningdif f icult (Edmondson and Moingeon 1998). However, joint learning and shared leadership minimize dif f erencesin the mental model that shapes individual speech and actions, reducing def ensiveness and increasing theef f ectiveness of the inf ormation being shared (Argyris and Schön 1978).
At CHOP double- loop learning is occurring at the enterprise level; the Inf ection Control Committee is takingaction to sustain and spread best practices around hand hygiene. Organizationally we are now reviewing thecontext within which we practice and determining if there is a need f or community education. The committee iscoordinating the enterprise approach to community education and bringing people together to connect thedots between the various settings.
Home Care provides educational in-services to inpatient and ambulatory departments about the care andservices available within the organization. Presentations at Nursing Grand Rounds and department in-servicesheighten understanding and awareness of home care practices. Residents, case managers and otherpersonnel attend home visits with nurses and respiratory therapists f or observation. They report the valuableinsight gained as they return to inpatient settings with a better understanding of what Home Care provides andwhat patients need.
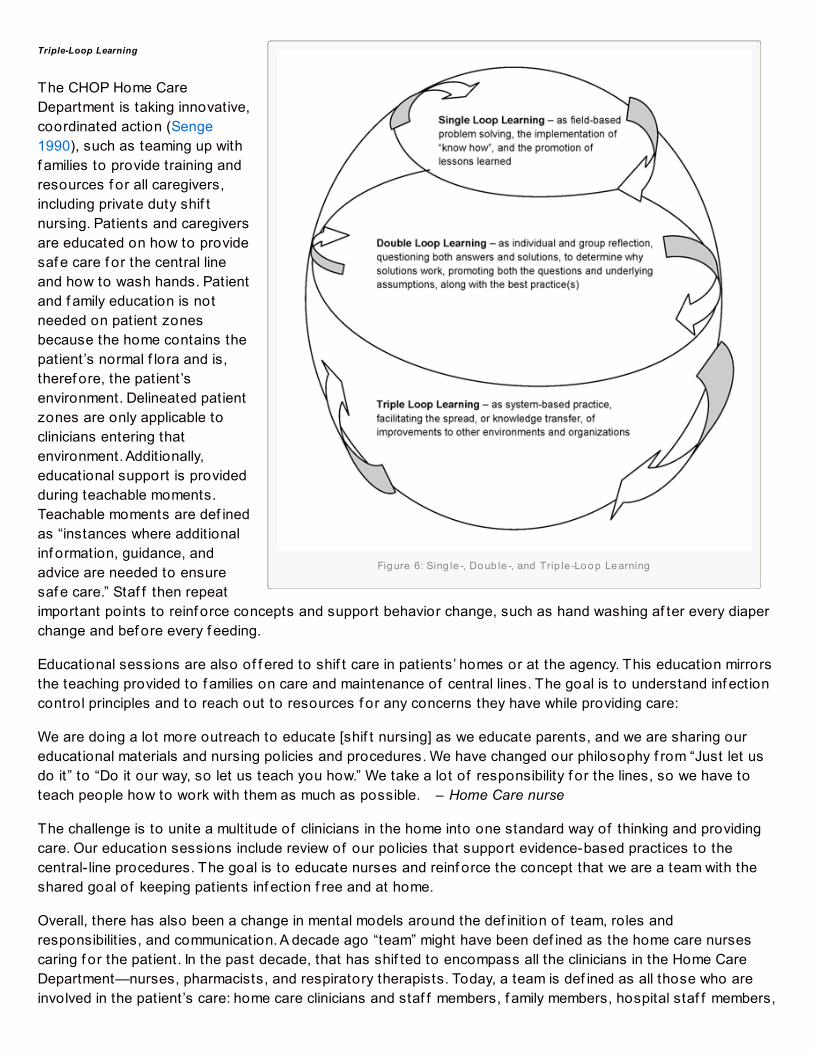
Fig ure 6: Sing le -, Do ub le -, and Trip le -Lo o p Le arning
Triple-Loop Learning
The CHOP Home CareDepartment is taking innovative,coordinated action (Senge1990), such as teaming up withf amilies to provide training andresources f or all caregivers,including private duty shif tnursing. Patients and caregiversare educated on how to providesaf e care f or the central lineand how to wash hands. Patientand f amily education is notneeded on patient zonesbecause the home contains thepatient’s normal f lora and is,theref ore, the patient’senvironment. Delineated patientzones are only applicable toclinicians entering thatenvironment. Additionally,educational support is providedduring teachable moments.Teachable moments are def inedas “instances where additionalinf ormation, guidance, andadvice are needed to ensuresaf e care.” Staf f then repeatimportant points to reinf orce concepts and support behavior change, such as hand washing af ter every diaperchange and bef ore every f eeding.
Educational sessions are also of f ered to shif t care in patients’ homes or at the agency. This education mirrorsthe teaching provided to f amilies on care and maintenance of central lines. The goal is to understand inf ectioncontrol principles and to reach out to resources f or any concerns they have while providing care:
We are doing a lot more outreach to educate [shif t nursing] as we educate parents, and we are sharing oureducational materials and nursing policies and procedures. We have changed our philosophy f rom “Just let usdo it” to “Do it our way, so let us teach you how.” We take a lot of responsibility f or the lines, so we have toteach people how to work with them as much as possible. – Home Care nurse
The challenge is to unite a multitude of clinicians in the home into one standard way of thinking and providingcare. Our education sessions include review of our policies that support evidence-based practices to thecentral- line procedures. The goal is to educate nurses and reinf orce the concept that we are a team with theshared goal of keeping patients inf ection f ree and at home.
Overall, there has also been a change in mental models around the def init ion of team, roles andresponsibilit ies, and communication. A decade ago “team” might have been def ined as the home care nursescaring f or the patient. In the past decade, that has shif ted to encompass all the clinicians in the Home CareDepartment—nurses, pharmacists, and respiratory therapists. Today, a team is def ined as all those who areinvolved in the patient’s care: home care clinicians and staf f members, f amily members, hospital staf f members,

and other community entit ies that might provide care, such as staf f nurses or school nurses.
Conclusion
Health care’s characterization of patient saf ety has changed to include a f ocus on inf ection control anddecreasing CLABSI (Starr and Torbert 2005). Roles and types of communication have also changed toaccommodate the expanding def init ion of a “team.” As described by our team at CHOP during interviews, theimplementation of a practice change is a process that takes ef f ort and time. Lessons learned were the init ialtools that propelled us f orward through a systematic learning environment based on the communication andeducational needs of our team members. Further education and collaboration are needed f or systemimprovements to occur (Schyve 2005) and to be sustained. Enterprise- level actions, as exemplif ied by theeducational goal of CHOP’s Inf ection Control Committee, are being developed to support and enhance theexpanding def init ion.
Shana Ratner (1997) def ines a learning organization as “one in which [staf f ] at all levels, individually andcollectively, are increasing their capacity to produce results they really care about”—in this case, patient saf ety.The staf f at CHOP Home Care invested time and f ocused, sustained ef f orts in implementing WHO’s FiveMoments f or Hand Hygiene as part of a saf ety init iative in reducing its CLABSI rate. Implementation resulted ina reduction in inf ection rates; lessons learned; best practices and changes in mental models, such as aredef init ion of “team”; and system-level changes such as innovative, coordinated, community- level educationaloutreach. Broadening our impact and connecting it back to posit ive patient outcomes are key activit ies f orsustaining a culture of saf ety.
Verna Cole, PhD, is the education and development liaison for Children’s Hospital of PhiladelphiaHome Care. Kelly Monacella-Duffy, MSN, RN, is the clinical operations manager for Home Health.Questions and comments about this work may be directed to Dr. Cole at [email protected] Ms. Monacella-Duffy at [email protected].
References
Argote L, Ingram P, Levine JM, Moreland RL. 2000. Knowledge transf er in organizations: learning f rom theexperience of others. Organizational Behavior and Human Decision Processes. 82(1, May):1–8, 2000.doi:10.1006/obhd.2000.2883. http://www.sciencedirect.com/science/journal/07495978/82/1. Accessed Jun 3,2013. []
Argyris C, Schön D. 1978. Organizational Learning: A Theory of Action Perspective . Reading, MA: Addison Wesley.[]
Bransf ord JD, Brown AL, Cocking RR, eds. 2000. How People Learn: Brain, Mind, Experience, and School.Washington, DC: National Academies Press. []
Edmondson A, Moingeon B. 1998. From organizational learning to the learning organization. ManagementLearning. 29(1):5–20. []
Edmondson AC, Dillon JR, Rolof f KS. 2006. Three perspectives on team learning: outcome improvement, taskmastery, and group process. Working paper. http://www.hbs.edu/f aculty/Publication%20Files/07-029.pdf .Subsequently published in Academy of Management Annals. 2008;1:269–314. []

Emanuel L, Berwick D, Conway J, et al. 2008. What exactly is patient saf ety? In Henriksen K, Battles JB, KeyesMA, Grady ML, eds. Advances in Patient Safety: New Directions and Alternative Approaches, Vol. 1: Assessment .AHRQ Publication No.: 08-0034-1. Rockville, MD: Agency f or Healthcare Research and Quality.http://www.ncbi.nlm.nih.gov/books/NBK43629/. Accessed Jun 3, 2013. []
Goh SC. 1998. Toward a learning organization: the strategic building blocks. SAM Advanced ManagementJournal. 63(2, Spring):15–22. []
Haskell R. 2001. Transfer of Learning: Cognition, Instruction and Reasoning. San Diego, CA: Academic Press. []
Hutchens D. 2009. Applications of Narrative and Storytelling as an Organizational Discipline. 2009.http://www.davidhutchens.com/Biz%20Writing/articles/organizationalst.html. Accessed Jun 3, 2013. []
Jones KJ, Skinner A, Xu L, Sun J, Mueller K. 2008. The AHRQ Hospital Survey on Patient Saf ety Culture: a toolto plan and evaluate patient saf ety programs. In Henriksen K, Battles JB, Keyes MA, Grady, M.L., eds. Advancesin Patient Safety: New Directions and Alternative Approaches, Vol. 2. Culture and Redesign. AHRQ Publication No.08-0034-2. Rockville, MD: Agency f or Healthcare Research and Quality.http://www.ncbi.nlm.nih.gov/books/NBK43709/. Accessed Jun 3, 2013. []
Moureau N. 2009. Winning the war on CLABSI: the role of education and new technology. Infection ControlToday. 13(10 Oct):np. []
Nevis EC, DiBella AJ, Gould JM. 1995. Understanding organizations as learning systems. MIT SloanManagement Review. 36(2):73–85. []
Nonaka I, Takeuchi H. 1995. The Knowledge-Creating Company: How Japanese Companies Create the Dynamicsof Innovation. New York: Oxf ord University Press. []
O’Connor N, Kotze B. 2008. ‘Learning organizations’: a clinician’s primer. Australasian Psychiatry. 16(3):173–178.[]
Ratner S. 1997. Emerging Issues in Learning Communities. St. Albans, VT: Yellow Wood Associates; 1–34. [ ]
Reason J. 1990. Human Error. New York: Cambridge University Press. []
Rowley C, Poon I. 2010. Elements in management learning: f rom individual to organizational learning.http://www.cassknowledge.com/research/article/elements-management- learning- individual-organisational-learning. Accessed Jun 3, 2013. []
Sax H, Allegranzi B, Uckay I, Larson E, Boyce J, Pittet D. 2007. ‘My f ive moments f or hand hygiene’: a user-centered design approach to understand, train, monitor and report hand hygiene. J Hosp Infect. 67:9e21. []
Schein EH. 1995. Building the learning consortium. MIT Organizational Learning Center, Working Paper 10.005. []
Schyve PM. Systems thinking and patient saf ety. 2005. In Henriksen K, Battles JB, Lewin DI, Marks ES, eds.Advances in Patient Safety: From Research to Implementation. Vol. 2: Concepts and Methodology. AHRQPublication No. 05-0021-2. Rockville, MD: Agency f or Healthcare Research and Quality; 1–4. []
Senge PM. 1990. The Fifth Discipline: The Art and Practice of the Learning Organization . New York: Doubleday. []
Starr A, Torbert B. 2005. Timely and transf orming leadership inquiry and action: toward triple- loop awareness.Integral Review. 1:85–97. []
World Health Organization (WHO). 2012. Hand Hygiene in Outpatient and Home-based Care and Long-term CareFacilities: A Guide to the Application of the WHO Multimodal Hand Hygiene Improvement Strategy and the “My

Five Moments for Hand Hygiene” Approach. Geneva: World Health Organization.http://www.who.int/gpsc/5may/hh_guide.pdf . Accessed Jun 3, 2013. []
mccaffertyl
Text Box
This article originally appeared in Patient Safety InSight (spring 2013) published by the American Society of Professionals in Patient Safety at the National Patient Safety Foundation. It is used here with permission.







![Olmsted CLABSI Bundle IFIC [Read-Only] · CLABSI Prevention Bundle Basic Interventions: – Hand hygiene – Full barrier precautions during CL insertion ... CDC/HICPAC CRBSI Prevention](https://static.fdocuments.in/doc/165x107/5b023f1c7f8b9a0c028f8446/olmsted-clabsi-bundle-ific-read-only-prevention-bundle-basic-interventions-.jpg)










