Quality Improvement Project (QIP) “Improving the Use of Psychotropic Medication
Upload
darren-ellisCategory
view
216download
3
Lessons Learned from Psychotropic Medication Monitoringfor Texas Foster Children
A joint project of
Texas Department of Family and Protective Services (DFPS)
Texas Health and Human Services Commission (HHSC)
Texas Department of State Health Services (DSHS)
All opinions are the authors and do not represent an official position or policy

BACKGROUND
Concerns were raised about psychotropic prescriptions given to fostercare children around 2004. In February 2005, DFPS, DSHS and HHSC released the Psychotropic Medication Utilization
Parameters for Foster Children, which were updated in June 2007 and most recently in December 2010. The current version can be found at:
http://www.dfps.state.tx.us/Child_Protection/Medical_Services/guide-psychotropic.asp
These Parameters use eight criteria to indicate a need for further review of the child’s medication regimen. Including such things as: Multiple drugs in the same class Five or more drugs Lack of appropriate diagnoses Dosage outside of recommendations
A system was needed to assess the degree to which these parameters were being met. I was involved in initially setting this system up and continue to work relatively closely with it.
We were very fortunate to have cross agency support and cooperation at all levels to get this project done.

RESOURCES YOU WILL NEED
Access to Medicaid data. You will need eligibility, claims/encounters and prescriptions.
Obtain reference files and decode tables to make sense of the Medicaid data.
Doctors specialty information, drug class descriptions and related information, diagnoses and procedure code descriptions.
Access to your own programs administrative data if you don’t have dedicated Medicaid program codes for foster care.
A statistical program such as SAS, SPSS or R and one (or more) persons who can serve as programmer.
A relatively high initial set up cost in time and effort but a lower ongoing cost to keep the data flowing once its set up.
One or more doctors and program experts at least on occasion for consultation.
Some consultation needed at the start and more later for specific report interpretation.

IMPORTANT QUESTIONS
Who will you keep? We keep only children age 0-17 for the time they are actually in foster care and under the state guardianship, other Medicaid time is excluded.
How often and how long will you look at the data? We look at quarterly reports, and annual reports. A rolling six month time frame is probably ideal, but people like firm time windows with clear cutoffs too.
What will be your review process, medically complex cases can have surprising medical needs?
Cases outside parameters are reviewed by the HMO administering the plan.
How will you communicate with your providers and how often?
Currently our primary communication is on a formal quarterly basis with the HMO and as needed as well. Approximately every year we review the highest providers.Children outside parameters should be flagged at any point by the HMO’s data systems.
How will you treat all the different varieties of foster care such as relatives, substitute care, residential treatment facilities?
At this point we don’t distinguish these on a regular basis.

MAJOR DRUG DECISIONSWhat drugs will you keep? We keep most antipsychotics, antidepressants,
anticonvulsants and stimulants as well as miscellaneous drugs.
Will you exclude drugs based on diagnoses? We exclude anti-convulsants based on seizure disorder diagnoses and diphenhydramine (Benadryl) based on allergy diagnoses.
How many prescriptions and how long? We look at all, but the focus is on two or more prescriptions covering 60 days. Since all we have is claims data, we use this criteria to indicate a drug is not a test, but a serious treatment.
How is polypharmacy defined? We use 60 concurrent overlapping days for two drugs to define the minimum bound of polypharmacy. One major idea is the availability of drugs to be metabolized simultaneously. Different prescriptions in different parts of a month doesn’t seem like much like polypharmacy it seems like sequential medication.
What will be your parameters for deciding what might too much, too young?
Currently five or more of any drug, and two or more in the same class. We use our own formulary classes (but AHFS or Medi-Span would work just as well). Looking at only single drugs will create enormous workloads. Some parameters change based on age.

BASIC STEPS1. Merge the Medicaid data files with their references.2. Then more merges and roll ups:
Roll up patients and flag services and diagnoses,Roll up scripts by chemical names by patients (calculate lengths of scripts),Roll the chemical names up by class by patients (calculate length and
polypharmacy), Summarize patients with flags for drug class and chemical name and length of
scripts.3. Retain merged and labeled files to run further analyses and reports.
CHALLENGES Prescriptions and diagnoses are not connected with one another.
You have to pull the diagnostic information from the claims/encounters. Diagnoses and Drugs have to be matched based on the person id.
Individual drug prescriptions have to be built up into larger groups to cover periods of time.
There will probably be a time lag in your data probably a minimum of 30 days and probably more like 90 days plus.

USEFUL REPORTS AND DATA
A big picture overview of patients A summary of prescriptions for all clients and by age, maybe by program type or facility.
Individual Patients prescriptions The individual prescription claims data for clients who are outside of parameters, which requires going back from the rolled up flag file to the original claims data.
An overview of doctors A summary of the number of patients each doctor has with the number with prescriptions in certain categories: 60 day plus, class poly pharmacy, multi drug poly pharm, and poly pharm.
A Break down by type of doc: Psych vs Others.
Basic Research/Reference Files A file that rolls up and merges both prescription information and diagnoses information by patient (one row per client).
Roll up the start and end dates for all drugs by chemical name received in a period of time and keep them as a reference for patients outside of parameters so you can see what drugs, when and how long for polypharmacy patients.
Helpful troubleshooting file for doctors Interleave the raw data lines by date of prescriptions, services with diagnoses (one row per claim).

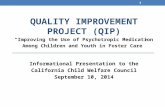
Update on the Use of Psychotropic Medications inTexas Foster Children: Fiscal Years 2002-2011
28.0%29.6% 29.9%
26.4%25.0% 24.7%
21.5% 21.2% 20.5%19.3%
3.3% 4.0%5.0%
3.4%2.5% 2.5% 2.0% 1.8% 1.6%1.8%
0.4%0.5%0.5%0.9%1.4%1.1%0.7% 0.6%0.7%0.7%0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
FY2002 FY2003 FY2004 FY2005 FY2006 FY2007 FY2008 FY2009 FY2010 FY2011
Perc
enta
ge o
f Chi
ldre
n in
Fos
ter C
are
Psychotropic Meds 60 days+ Class polypharmacy Five or more Meds polypharmacy
36% Decrease since 2004
68% Decrease since 2004
70% Decrease since 2004

CLOSING THOUGHTSOur results indicate that both the parameters (~ 05-07) and managed care
(~ 08-11) have had relatively large effects.• The parameters and provider outreach decreased a baseline (~ 02-04) of
either multi-drug or class polypharmacy of slightly over 5% to well below 4%.
• The parameters and provider outreach alone decreased either multi-drug or class polypharmacy from below 4% to slightly over 2%.
• Overall both interventions have resulted in well over a 50% reduction in either type of polypharmacy.
• We are hoping for further improvements with our participation in MEDNET and further refinements of our monitoring system.
Setting up a monitoring system and looking at your data can help you stay on top of the drugs and diagnoses in your system of care and help improve quality of care for your patients.