Lesson 2 Medical Emergencies © 2009 Pearson Education Chapter 43: Assisting with Medical...
117
Lesson 2 Medical Emergencies © 2009 Pearson Education pter 43: Assisting with Medical Emergencies and Emergency Preparedn
-
Upload
gyles-rich -
Category
Documents
-
view
222 -
download
1
Transcript of Lesson 2 Medical Emergencies © 2009 Pearson Education Chapter 43: Assisting with Medical...

Lesson 2
Medical Emergencies
© 2009 Pearson Education
Chapter 43: Assisting with Medical Emergencies and Emergency Preparedness

Define and spell the terms to learn for this chapter.
Explain ABCD as it applies to CPR and obstructed airways.
List the signs and symptoms of respiratory distress and chest pain.
Explain the difference between insulin shock and diabetic coma.
© 2009 Pearson Education
Lesson Objectives
Upon completion of this lesson, students should be able to …

Identify and describe various types of soft tissue wounds.
Discuss first-, second-, and third- degree burns as well as the Rule of Nines
Identify steps to take for a patient with syncope.
© 2009 Pearson Education
Lesson Objectives
Upon completion of this lesson, students should be able to …

Causes of Respiratory and Cardiac Arrest An occluded airway Electrocution Shock Drowning Heart attack Trauma Anaphylaxis
Drugs Poisoning Traumatic head or
chest injury
General Guidelines for Emergency Care Early access to EMS is important. Access for the adult patient is initiated by calling 911 as
soon as it has been determined that the patient is unconscious and not breathing.
In general, “Phone first” for an unresponsive adult. With children and infants, EMS access is made after 2
minutes of CPR. In general, perform “CPR first” for unresponsive
children and infants. The sequence normally followed is Airway, Breathing,
Circulation, and Defibrillation (ABCD).

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Airway
Roll pt onto his/her back, using the logroll technique.
Assess the pt for responsiveness. No response check the airway. Listen for air movement, look for chest
movement, feel for air movement.
© 2007 Pearson Education
MEDA116 – First Aid and CPR
Breathing
Pinch the pt’s nose shut, seal your lips tightly around the pt’s mouth and deliver 2 breaths.
If pt’s chest rises, you have been successful.

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Circulation
Check for signs of circulation such as a defined pulse, color & warmth of the skin, and pt movement.
After breaths delivered check for the pulse. If pulse is weak, erratic, or nonexistent & no
signs of circulation are present begin compressions as appropriate to pt’s age.

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Defibrillation
AED is highly effective when provided immediately after or within minutes of an adult cardiac arrest.
AED will give verbal directions to the rescuer or rescue team that are easy and safe to follow.
Not to be used on infants.

Critical Thinking Question
In what situations do airway obstructions most frequently occur?

The Universal Choking Sign
Insert Figure 43-8 from PCMA 2eInsert Figure 43-8 from PCMA 2e
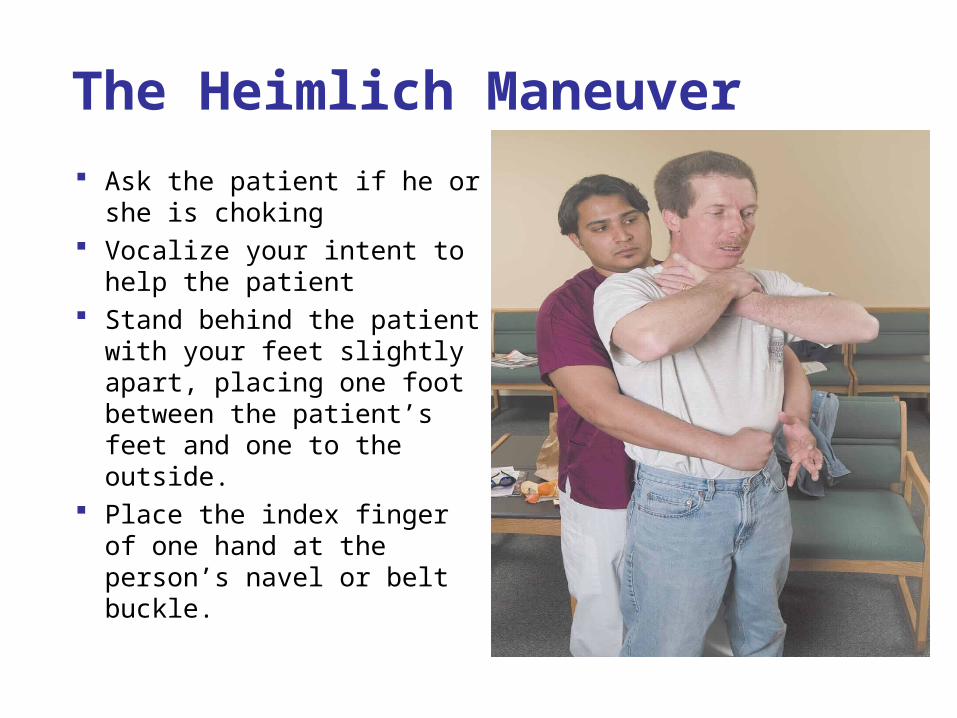
The Heimlich Maneuver
Ask the patient if he or she is choking
Vocalize your intent to help the patient
Stand behind the patient with your feet slightly apart, placing one foot between the patient’s feet and one to the outside.
Place the index finger of one hand at the person’s navel or belt buckle.
Insert Figure 43-13 from PCMA 2e
Insert Figure 43-13 from PCMA 2e
The Heimlich Maneuver
If the patient is a pregnant woman, place your finger above the enlarged uterus.
Make a fist with your other hand and place it, thumb side to patient, above your other hand.
If the person is very large or far along in pregnancy you may have to do chest compressions.
Place your marking hand over your curled fist and begin to give quick inward and upward thrusts.
There is no set number of thrusts to give to an adult who remains conscious.

The Heimlich Maneuver
Continue to give thrusts until the object is removed or the patient becomes unconscious.
If the patient becomes unconscious, gently lower him/her to the ground.
Activate EMS and put on gloves. Immediately begin CPR with 30 chest compressions
and 2 rescue breaths. Before administering the rescue breaths, open the
airway with the head-tilt chin lift and look for a foreign body in the patient’s mouth and remove if visible.

The Heimlich Maneuver
Blind finger sweeps are no longer recommended and should not be performed.
Continue with cycles of 30 compressions and 2 rescue breaths until the foreign body is expelled or advance medical personal arrive to relieve you.
Wash hands and document the event in the patient’s chart.

Chest Thrusts and Back Blows on an Infant
Insert Figure 43-15A from PCMA 2e
Insert Figure 43-15B from PCMA 2e

Steps for Adult rescue Breathing and One-Rescuer CPR Assess the patient and determine if help is needed. Shout, “Are you OK?” while gently shaking the
patient’s shoulders. If the adult patient is determined to be unresponsive,
activate EMS immediately by calling 911 and get an AED if available.
Assess the ABCs.
Insert Figure 43-9 fromPCMA 2e

Assessing the ABCs
Airway: perform a head-tilt chin lift, or, if a neck injury is suspected, a jaw thrust.
Look and feel for breath and chest movements. Attempt to get another person to call 911. If you are alone, begin the rescue sequence for 1
minute and then attempt to call 911 yourself. If gloves are available, put them on. If you have a ventilator mask, place it on the patient.

Performing Breaths
If breathing is absent, put on a mouth guard and administer two rescue breaths.
If your breaths do not cause the chest to rise, look in the patient’s mouth and remove an object if one is seen.
If no object is seen, make a second attempt to administer a rescue breath.
If the breaths cause the chest to rise, assess the patient’s circulation by feeling for a pulse at the carotid artery.

Feeling a Pulse
If you feel a pulse, begin rescue breathing.
Administer 1 breath every 5 seconds, or 10–12 every minute.
After 1 minute, reassess the patient for breathing and pulse.
Insert Figure 43-12 fromPCMA 2e

Performing Chest Compressions If you do not feel a pulse, begin chest compressions.
Kneel at the patient’s side and place your hand in
the center of the chest between the nipples. Place your other hand on top of the first hand,
making sure to lift your fingers off the chest, using only the heels of your hands to administer compressions.
Keep your shoulders directly over your hands Compress the chest 1-1/2 to 2 inches, then allow the
sternum to relax.

Performing Chest Compressions
Do not lift your hands off the chest.
Continue to compress the chest a total of 30 times, then administer 2 breaths.
Repeat this sequence for 4 total cycles. Reassess the patient.
If necessary, continue CPR until pulse and breathing return or you are relieved by more advanced medical personnel.
Insert Figure 43-5 fromPCMA 2e (middle image)
Steps for Infant or Young Child Rescue breathing and One-Rescuer CPR
Assess the patient and determine if help is needed. Shout the infant or child’s name and sharply poke at
the feet. Never shake an infant. If the infant patient is determined to be
unresponsive, perform CPR for 2 minutes prior to activating EMS immediately by calling 911 and get an AED if available.
Carefully place the patient on their back, be cautious not to move the head or allow the neck to twist, especially if a spinal cord injury is suspected.

Steps for Infant or Young Child Rescue breathing and One-Rescuer CPR
Gently, with two fingers, tilt the patients head and open the airway.
Place your ear close to the patient’s ear to listen for breathing sounds, watch to see if the chest rises or falls indicating breathing, try to feel for any breathing from the patient’s nose or mouth.
If breathing is absent, secure a mouth guard over the patient’s mouth and nose.
Administering Rescue Breaths
Administer 2 rescue breaths. If your breaths do not cause the chest to rise, look in
the patient’s mouth and remove an object if one is seen.
If no object is seen, make a second attempt to administer a rescue breath.
If the breaths cause the chest to rise, check the patient’s pulse at the brachial artery.
If you feel a pulse begin rescue breathing by administering 1 breath every 5 seconds, or 10 to12 every minute.

Administering Chest Compressions
If you do not feel a pulse, begin chest compressions.
Place two fingers in the center of the chest just below the nipple line.
Insert Figure 43-7Cfrom
PCMA 2e

Administering Chest Compressions
Compressions should be made one-third to one-half the depth of the chest. Perform quick 30 compressions.
Give 2 more rescue breaths followed by 30 more compressions. Continue the 30:2 compressions and breaths.
After 2 minutes, leave the infant and call 911 if you are still alone.
Continue compressions and breaths until the infant recovers or EMS arrives.
Automated External Defibrillation (AED) Highly effective when provided immediately
after or within minutes of an adult cardiac arrest.
Most cardiac arrests in adults are related to fatal electrical arrhythmias of the heart and are correctable with defibrillators.
Defibrillator gives verbal directions to the rescuer or rescue team that are easy and safe to follow.
AED is not applied to infants.

The Respiratory System
Body cells require constant exchange of fresh oxygen and removal of carbon dioxide.
Insert Figure 29-1 from PCMA 2eInsert Figure 29-1 from PCMA 2e

Reasons for Respiratory Distress
Reaction to a long-term debilitating disease, such as chronic pulmonary obstructive disease (COPD)
Reaction to an emergency situation, such as anaphylactic response to medication.
Due to the result of other disease processes such as obstructive conditions, such as asthma, chronic bronchitis, and emphysema, pneumonia, and acute pulmonary edema.

Symptoms of Respiratory Distress Acute anxiety with gasping breaths Bradypnea, abnormally slow breathing Cyanosis Failure of the chest to rise and fall Nasal flaring Pursing of the lips Noisy breathing Tachypnea (abnormally rapid breathing)

Steps for Administering Oxygen
Gather all needed equipment and perform hand hygiene. Identify the patient and confirm the physician’s order for
oxygen therapy. Check the pressure reading on the oxygen tank to make
sure it has enough oxygen in it. Start the flow of oxygen by opening the cylinder. Attach the cannula tubing to the flow meter. Adjust the oxygen flow to the physician’s order. Hold the cannula tips over the inside of your wrist, without
touching the skin, to determine if oxygen is flowing.
Steps for Administering Oxygen
Apply gloves, if necessary.
Place the tips of the nasal cannula into the patient’s nostrils.
Wrap the tubing behind the patient’s ears.
Instruct the patient to breathe normally through the mouth and nose.
Insert Figure 43-7 fromPCMA 2e

Steps for Administering Oxygen
Some patients instinctively hold their breath or avoid breathing through the nose when an object is placed in the nostrils.
Check the patient’s oxygen level with an oximeter. Place the probe over the index finger and record the
reading. If necessary, have the patient take a short walk to verify
that the oxygen flow rate is sufficient for activity. Wash hands and document the procedure in the
patient’s chart.

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Shortness of Breath
Patient needs immediate intervention. Patent, or unobstructed, airway is necessary in
moving in and out. Ask about the onset and what activity caused it. Patient may be gasping for air, looking pale or
cyanotic, and exhibiting nasal flaring and extreme anxiety.
Patient should be sitting in an upright position.

Hyperventilation Quick, shallow breathing or rapid, deep
breathing that results in decreasing carbon dioxide in the blood, dilation of blood vessels, and lowered blood pressure.

Symptoms and Treatment of Hyperventilation
Symptoms Light headed Chest tightness Cardiac palpitations Rapid pulse Deep sighing breaths Anxiety
Treatment Inform the physician and
encourage the patient to breathe slowly.
Have the patient breathe into an oxygen mask (not connected to any oxygen), block one nostril, or breathe into a brown paper bag. One of these methods is usually effective.

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Chronic Obstructive Pulmonary Disease
Asthma, chronic bronchitis, and emphysema are all COPD’s
Air is trapped in the lungs and carbon dioxide is unable to expel from the alveoli.
A person with COPD has sob, rapid hear rate, and experiences weakness.

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Pulmonary Edema
Fluid accumulation in the lung tissue and alveoli Pt has difficulty breathing, wheezing sounds,
cyanosis, rapid heartbeat, distended neck veins, extreme anxiety, and orthopnea.
Place pt in sitting position with feet and legs up on a bed or cart.

Chest Pain Heart attacks are the leading cause of death for
both men and women. The primary complaint will be pain in the middle
or left side of the chest, described as sharp, stabbing, crushing, squeezing, or aching.
The pain may radiate to the left arm, to the back, or up the neck.
Sometimes the pain is brought on by exertion, but other times onset is sudden and unexplained.

Chest Pain Other symptoms are nausea, weakness, SOB,
apprehension, and the feeling of impending doom.
The skin may be clammy, moist, pale, or cyanotic
Denial is common, as the individual tries to explain the pain as heartburn or indigestion.

Care of Chest Pain Have the individual stop what he or she is
doing and sit down, feet elevated if possible. Ask a coworker to stay with the patient while
you inform the physician of the situation. If instructed by the physician, or if a physician
is unavailable, call EMS. If oxygen is available, administer it according
to office protocol by nasal cannula at 6 to 8 liters per minute until the physician or emergency personnel arrive.

Care of Chest Pain If the patient has previously been diagnosed
with angina and has nitroglycerin tablets, insert one tablet under the tongue.
Tablets may be administered every 5 minutes up to three doses.
If the pain is not relieved, inform the physician or EMS on the scene.

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Telephone Call with Complaint of Chest Pain
Keep the caller on the line while asking for help from another office staff member.
Write down the caller’s name and location. Follow office protocol regarding assisting pts
with chest pain. A lot of the time offices will want all pts calling with chest pain to go to the ER (ED). If this is the case, call EMS for the pt and remain on the phone with them until EMS has arrived.
Shock
Collapse of the cardiovascular system caused by insufficient cardiac output.
Blood supply and nourishment (oxygen and nutrients, including glucose) to the tissue and perfusion to the organs are inadequate.
Untreated shock can progress very rapidly to death.

Causes of Shock Anaphylaxis Cardiac failure Hemorrhage Extreme emotional upset Respiratory distress Neurological collapse Severe metabolic insult Sepsis

General Signs of Shock
Weakness Rapid heartbeat Thirst Nausea Dizziness Restlessness Pallor Cool skin Clammy skin
Cyanosis Confusion Disorientation Unresponsiveness Shallow breathing

Anaphylactic Shock
Severe allergic reaction to a foreign substance such as medications, bug bites, and latex gloves.
Inform the physician immediately, and call EMS. The physician may order epinephrine and/or an
antihistamine. An IV may also be started. Prevention is the most important factor in anaphylactic
shock.

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Most Common Signs of Shock
Pale, gray, or bluish skin Moist, cool skin Dilated pupils Weak, rapid pulse Shallow, rapid respirations Extreme thirst

General Treatment for Shock in the Medical Office Encourage the patient to lie down with feet
elevated Cover the patient with blankets for warmth Keep the patient calm Inform the physician, contact EMS for further assessment and transport, monitor the patient’s vital signs, and provide emotional support
Critical Thinking Question
What other treatment may you give while
waiting for the patient to be transported?
Critical Thinking Question
What other treatment may you give while
waiting for the patient to be transported?

More Specific Treatment for Shock in the Medical Office
Cause Treatment
Anaphylactic Shock Epinephrine
Cardiogenic Shock IV dopamine (pacemaker), stat transport to ED
Hemorrhagic shock Stop bleeding, replace volume, stat transport
Hypovolemic shock Replace volume
Insulin shock Sugar, given to patient by any means tolerated
Neurogenic shock IV dopamine, immediate transport to the emergency room
Poisoning Consult poison center for treatment specific to the poison
Respiratory shock Intubation and immediate transport to the emergency room
Sepsis Fluids, IV dopamine and immediate transport to the emergency room
Diabetic Emergencies
HypoglycemiaHypoglycemia: Low blood sugar• Blood sugar is below 70mg/dL• May have skipped a meal, vomiting after taking diabetic
medications, excessive exercise, or an unknown reason HyperglycemiaHyperglycemia: High blood sugar
Both of these conditions cause a rapid onset of altered Both of these conditions cause a rapid onset of altered levels of consciousness, although there is a greater risk levels of consciousness, although there is a greater risk for those with hypoglycemia.for those with hypoglycemia.

Signs of Insulin Shock or Diabetic Coma Very low or very high blood sugar Vomiting Balance disturbances Uncharacteristic behavior Sweet, fruity odor to the breath Loss of consciousness Appear to be intoxicated Cold clammy skin Anxious Combative
Care for Diabetic Crisis If victim is conscious,
• Ask about the last intake of food and diabetic medication
• Glucose paste• Orange juice with added sugar
If victim is unconscious• IV glucose

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Bleeding
External• Occurs when skin is broken
Internal• Occurs with tissue damage and intact skin
Originate from 3 types of blood vessels:• Arteries• Veins• Capillaries

Arterial Bleeding
Usually copious, rapid, and bright red. Blood often spurts, echoing the heartbeat. Must be brought under control as soon as
possible. Pressure applied directly over the exit wound
may halt the flow of blood. If not successful, external pressure on the
pressure points may be. Elevating the injured part higher than the heart
may also slow the blood flow.

Bleeding from Veins and Capillaries
Venous blood flows more slowly darker in color can usually be
controlled by direct pressure.
Blood from capillaries oozes rather than
flows can be halted with
direct pressure.

Critical Thinking Question
What is the danger of persistent blood loss?
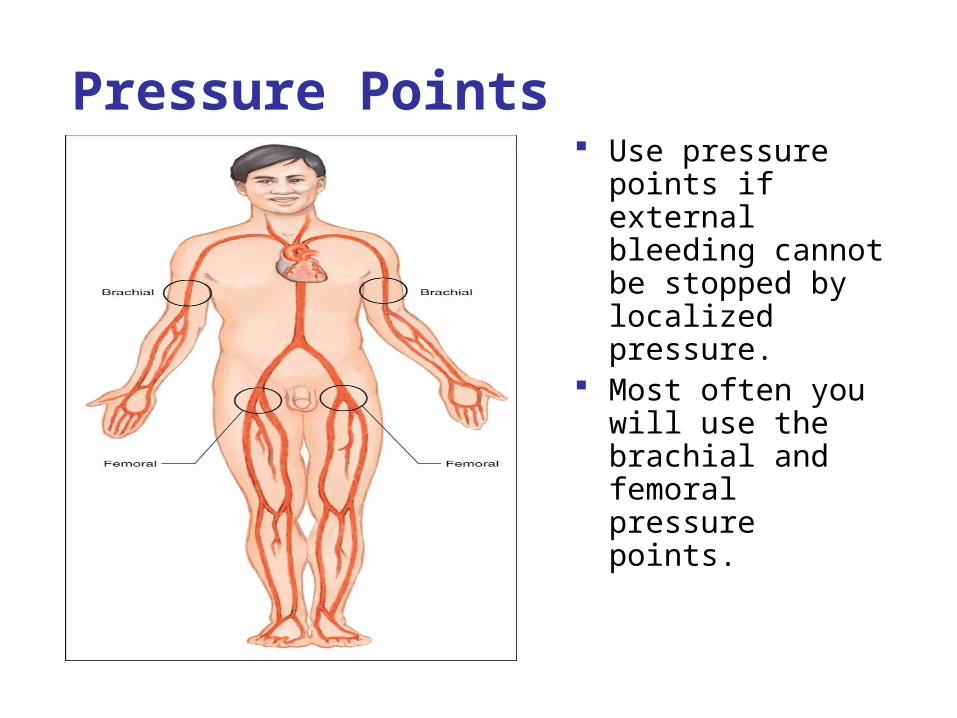
Pressure Points Use pressure
points if external bleeding cannot be stopped by localized pressure.
Most often you will use the brachial and femoral pressure points.
Insert Figure 43-21 from PCMA 2e
Insert Figure 43-21 from PCMA 2e

Open Wounds Generally not life threatening unless they penetrate
the head, chest, throat, or abdomen. Typically require irrigation, debridement, sutures,
and antibiotics. If involves nerve or muscle tissue, genitalia, eyes,
and possibly hands will require specialized care.
Critical Thinking Question
In what cases are open wounds life
threatening?
Critical Thinking Question
In what cases are open wounds life
threatening?

Classification of Open Injuries
Insert Figure 43-29 from PCMA 2eInsert Figure 43-29 from PCMA 2e

Abrasions
Occurs when the outer layer of skin is scraped away, leaving the underlying tissue exposed.
Common types of abrasions include friction burns, rug burns, road rashes, and scrapes.
Bleeding is usually in the form of oozing and the injury is quite painful because nerve endings are exposed or damaged.

Avulsions
Tearing away of skin or tissue. Usually occur on limbs and appendages, including
fingers, toes, hands, arms, feet, legs, nose, and penis.

Avulsions
Body part may become entangled in machinery or be injured in a motor vehicle accident or a confrontation with an animal.
Cleanse minor avulsion wounds with soap and water and return any skin flap to its normal position.
Apply direct pressure, then apply a dressing when bleeding is controlled.
Amputation If body part has been recovered, cleanse the
dismembered part with sterile saline. Wrap it with moist, sterile gauze, seal it in a plastic
bag, and place the plastic bag in a container on ice.
Prompt medical attention and preservation of the body part enhance the chances for successful reattachment.

Critical Thinking Question
What do you do if someone’s finger is not entirely amputated, but it is just
hanging by some skin?

Lacerations
An open wound in which the skin and underlying tissue are torn.
Usually has jagged edges that may interfere with the healing process.
Cleanse the laceration with soap and water or an antiseptic solution, remove all debris and foreign matter.
If a minor laceration, place a Band-aid, Steri-strip, or sterile butterfly.
If bleeding is severe, a physician should direct the cleansing process.
Lacerations over a joint may require joint immobilization for a few days while healing progresses.

Incisions
A cut with smooth edges made with a knife or other sharp object.
Treated in the same manner as any laceration. If the wound is deep or extensive, the physician usually
performs a surgical intervention consisting of debridement, hemostasis, and trimming away of the jagged wound edges.
If there is damage to underlying tissue, such as a tendon or ligament, further surgical intervention is required.
Puncture Wounds
Results from a pointed foreign body penetrating the skin and tissue.
Often times edges close trapping pathogens and debris in the tissue.
Cleansing may consist of simply soaking the area or may require invasive irrigation.
After cleansing, a dressing is applied. Bleeding is usually minimal.

Impaled Objects
Requires special treatment. General rule is to leave the object in place until it can be
safely removed by trained personnel. Stabilizing the object is critical to preventing further
damage. Control bleeding and stabilize the impaled object with a
bulky dressing held in place with tape or other bandages. Splint the area to prevent movement. For a small penetrating object, a small paper cup may be
used. Make a hole in the bottom of the cup, place it over the object with the lip of the cup against the skin, and secure it with bandages.

Soft Tissue Injuries
involves both the skin and underlying tissue. Avulsions, amputations, and thermal insults are
considered soft-tissue injuries because tissue as well as skin is involved.
Damage to the underlying tissue may involve blood vessels, nerves, muscles, and subcutaneous tissue.
The tearing of minute to larger blood vessels results in bleeding into the tissue and discoloration of the area.
Swelling may exert pressure on nerve endings, creating pain.

Crush Injuries
Result when force is applied to the tissue. Depending on the area involved, the crush may be
similar to pinching of tissue or it may be so severe as to involve organs and bones.
Elevating the body part above the heart and applying cold are often the only intervention needed.
With a more severe injury, the body part should be immobilized.
Monitoring vital signs and observing skin color, temperature, and moisture are essential to deciding whether more extensive intervention is needed.

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Wound Care Pointers
A dressing is a sterile covering placed directly over a wound to absorb blood and other body fluids, prevent contamination, and protect the wound from further trauma.
A bandage is a strip of binding material used to hold a dressing in place.
Simple direct pressure with a dressing will usually stop bleeding from a soft tissue injury.
Priority is to preven infection by dressing the wound properly.

Open Wounds
Open wounds can be: Superficial—penetrating only the skin Deep—penetrating the fascia, or connective layer
beneath the skin, and other structures that lie deeper still
Typically open wounds require: Irrigation Debridement (or surgical trimming) Sutures Antibiotics

Open Wound CareStop the bleedingStop the bleeding Apply direct pressure to the wound. If necessary, use a bulky dressing. Don’t remove the layers of dressing you’ve used to
stop the bleeding until a physician directs you to.

Open Wound CareClean the woundClean the wound It is very important to do this well because it is essential
to preventing infection. Cleanse the would from the center outward, beginning
with vigorous irrigation using disinfecting solution prescribed by the physician.
Wipe the edges of the wound in all directions away from the wound with sterile gauze. Critical Thinking
QuestionWhat do you do if the
wound is more serious than what you have cared for in
the past?
Critical Thinking Question
What do you do if the wound is more serious than what you have cared for in
the past?
Open Wound CareDress and bandage the woundDress and bandage the wound Cover with a sterile dressing and fasten the dressing
in place. The physician will specify whether or not to use
antibacterial ointments or creams.

Open Wound CarePost bleeding control and dressingPost bleeding control and dressing Get a good set of vitals Allow patient to remain in a comfortable position Watch for signs of shock Assist patient into a sitting position and make sure he
or she is not dizzy Make sure the patient understands home instructions Help the patient to a standing position, ensuring
stability If there are signs of shock, notify the physician
immediately; he or she may have you contact EMS

Applying a Triangular Bandage
Keep the injured arm as immobile as possible. Carefully slide the triangular bandage under the area to
be held. Two shorter sides should be pointing toward the elbow,
and the remaining longer edge should be parallel to the opposite body side.
Bring the lowest side up and over the arm. Tie the ends of the bandage behind and slightly to the
side of the neck. Tuck the peak of the bandage in toward the elbow point
of the bandage.

Applying a Figure-Eight Bandage
Place the thumb of one hand on one end of the bandage
Anchor the bandage with your other hand, then complete one circle around the extremity or body part.
Continue to alternate wrapping above and below the body joint or dressing and circling behind the joint or dressing area until the injured area is covered adequately.

Applying a Figure-Eight Bandage
If applying a bandage to a foot, ensure that toes are exposed to evaluate circulation.
Insert Figure 43-24 fromPCMA 2e

Applying a Tubular Bandage
Choose an applicator that is larger than the extremity to be bandaged.
Cut an approximate amount of tubular gauze bandage and slide the gathered bandage onto the applicator.
Insert Figure 43-25 fromPCMA 2e

Applying a Tubular Bandage
Slide the applicator over the extremity.
Insert Figure 43-26 fromPCMA 2e

Applying a Tubular Bandage
Hold the bandage against the proximal end of the extremity and pull the applicator approximately 1 inch past the distal end.
Insert Figure 43-27 fromPCMA 2e

Applying a Tubular Bandage
Twist the bandage gauze one complete turn. Next, slide the applicator toward the proximal end of the
injury.
Insert Figure 43-28 fromPCMA 2e

Applying a Tubular Bandage
Hold the proximal end of the tubular bandage gauze in place, and pull the applicator toward the distal end.
After pulling past the distal end, complete one twist.
Slide back and forth and twist the distal end of the dressing until the injured area is adequately covered.
Cut excess dressing, but remember to anchor the bandage at the proximal end.

Epistaxis (Nosebleeds)
Usually Non-life-threatening Tend to occur most commonly in dry weather
or in dusty conditions, and are usually easy to treat.
More serious if bleeding from both nostrils.
Critical Thinking Question
When should you worry about a nosebleed?
Critical Thinking Question
When should you worry about a nosebleed?

When to Worry About Persistent Nosebleeds When a nosebleed occurs after a head injury and
does not stop. If the person has high blood pressure, especially if
he or she has stopped or changed medicines for the condition.
If the person has a clotting disorder. A patient has a history of nosebleeds that have
caused shock in the past.

Caring for Nosebleeds
The physician will twist a facial tissue and pack the patient’s nose.
A chemical cold pack should be held against the bridge of the patient’s nose.
A patient may need electrocautery if the bleeding doesn’t stop.

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Burns
Occurs when an area of tissue is destroyed by the action of physical heat, chemical activity, high electrical current, or heavy exposure to radiation.
Severity depends on the amount and depth of the tissue injury.
Destruction of skin surface is important since all the skin functions are lost.
May help stop the burning and remove any metal jewelry from the burn pt.

Classification of Burns Surface area of body Depth of burn into the skin

The Rule of Nines
Insert Figure 43-30 from PCMA 2eInsert Figure 43-30 from PCMA 2e
Classification of Burns First-degree burns
• Reddening, swelling of epidermis (like a mild sunburn)• Extremely painful
Second-degree burns• Reddening, swelling of epidermis and outer dermis; blisters
noted• Extremely painful
Third-degree burns• Charring of all layers of skin and at least some deeper structures• Tend not to be painful immediately, destroys the sensory nerve
ending.

Special Considerations to Determine Seriousness Mortality is higher in:
• Elderly• Very young
Burned in enclosed area Burns of genitalia Presence of other injuries Chemical burns Electrical burns

Treatments for BurnsFirst degreeFirst degree Cool water if involves less than 10% of the body. Use analgesics and ointments, if ordered by the
physician.
Second degreeSecond degree Cool water as long as there are no broken blisters. Do not use analgesic creams and ointments. Cover with a dry sterile dressing.

Treatments for BurnsThird degreeThird degree Transport to a trauma center. Debride dead skin or damaged tissue (physician only). Cover burns with dry sterile dressing. Manage pain with injectable analgesics as ordered by a
physician.
Burns of any kind that involve broken skin may have to be debrided (removal of dead or damaged tissue.
All burn victims should be monitored for signs of shock.

Treatments for BurnsUpper Airway BurnsUpper Airway Burns Prompt intubation by the physician or EMS with the
largest tube that can be inserted. Transport to a trauma center. Listen for strider (noisy breathing). Administer oxygen as ordered by physician.
Large Surface Area BurnsLarge Surface Area Burns Dress with dry, sterile sheets Prompt transport to trauma center Monitor and treat for shock

Now You Guess!
Classify this burn.
Insert Figure 41-40 from Frazier/Malone MA, p. 896Insert Figure 41-40 from
Frazier/Malone MA, p. 896
Third-degree burn

Heat and Cold Exposure
Hyperthermia
Elevated body temperature
Results from prolonged exposure to extremely hot temperatures often
Hypothermia
Lowered body temperature (below 95 degrees)
Results from prolonged exposure to cold or cold water

Hyperthermia Heat exhaustionHeat exhaustion
• Extreme fatigue due to heat
• Occurs as the result of sodium and water depletion form the body.
• Strenuous activity often precedes heat exhaustion
Heat strokeHeat stroke• Advanced heat
exhaustion, body temperature ≥105˚
• Many patients will not sweat.
• Eventually brain cells begin to die and permanent brain damage or death may result.

Signs and Symptoms of Heat Exhaustion Dizziness Nausea and vomiting Headache Muscle cramps Diarrhea Weakness Moist, pale, cool skin

Treating Heat Exhaustion Move to a cooler environment. Encourage patient to lie down Apply cool, wet compresses and give sips of water.

Signs and Symptoms of Heat Stroke
Failure to perspire Temperature of 105˚ or higher Skin that is dry, red, and hot to the touch Headache Shortness of breath Nausea and vomiting Dizziness Weakness Dry mouth Initial rapid, strong pulse that grows weaker Drop in blood pressure Mental confusion, irritability, or hysterical behavior

Treating Heat Stroke Remove the patient from source of heat. Loosen the victim’s clothing. Cool the body as quickly as possible by pouring cool
water over the patient Contact EMS if physician is not available.

Hypothermia An unacceptable drop in body
temperature. Results from prolonged exposure to
cold or cold water

Signs and Symptoms of Hypothermia
Shivering Numbness and tingling throughout the body Skin cool to the touch and is pale with blue or
ashy tinge Shallow respirations Disorientation

Treating Hypothermia Remove cold and wet clothes. Wrap the patient in warm blankets Heat packs may be used but not directly on the
skin Sips of warm liquid Transport to treatment facility for assessment
by a physician

Convulsions (Seizures) Produced by disorganized electrical activity in
the brain. Characterized by involuntary muscle
contractions that alternate between the contraction and relaxation of muscles.
In some cases the convulsions are generalized, involving the entire body, or localized and limited to a specific area of the body.
Can result from a number of problems or combinations of problems.

Care for Convulsions (Seizures) Convulsions are not life threatening themselves Muscle spasms of full body can restrict
breathing Victims may bite tongue causing bleeding and
swelling, which can the obstruct airway Prevent injuries Pay close attention to what the patient is
experiencing so that you can describe it later.

Fainting (Syncope)
Sudden loss of consciousness. Seems to be caused by a brief interruption in the body’s
ability to control the brain’s circulation. Often occurs just after a patient has received an
emotional shock of some kind. Patient usually collapses and becomes unresponsive,
but within a minute, should awaken and return to normal function.
Patients seldom become incontinent or have seizures as a result of simple fainting, but may be injured in the course of a fall.

Caring for a Patient Who Has Fainted If the patient has fainted and there is no response,
provide oxygen if the physician orders this. Check the ABCs and call for help. If the patient is breathing well but will not wake up,
place him or her on the left side and contact the physician.
If the physician is unavailable, contact EMS Obtain a full set of vital signs and obtain a blood
sugar reading if possible.

© 2007 Pearson Education
MEDA116 – First Aid and CPR
Musculoskeletal Injuries
Involve bones, muscles, tendons, and ligaments
Includes fractures, dislocations, sprains, and strains.
Diagnosis is made by x-ray Affected part must be immobilized

Fractures Types of fractures:
• Closed (simple)—the bone is broken but does not penetrate the skin
• Open (compound)—the bone pierces the skin, or the skin is torn open by the bone or by an external force

Splinting Injuries Fractures of long bones
require immobilization by splinting to prevent joint movement above and below the fracture.
Splint also helps relieve pain and allows safe movement of the injured part.
Immobilize the bones above and below the joint (joint fracture)
Clean and cover all wounds before you splint
Never try to move or straighten a bone in a compound fracture

Sprains and Strains
Sprain Occurs when muscles,
tendons, or ligaments are torn.
It may be the result of trauma or cumulative overuse of the joint.
Strain Often called a pulled
muscle Occurs when a muscle or
tendon is overextended by stretching.
Patient may be unable to use the joint
In the lower extremities, weight-bearing is painful and sometimes impossible.

Dislocation
Bone is actually pulled away from the joint, stretching or tearing the ligaments and tendons.
A deformity is generally noted. Must be reduced and the bone reinserted into
the joint. Injured body parts should be immobilized to
prevent additional damage and reduce pain. Applications of cold also help with the pain and
slow edema.
Questions?