
Lesley Pearson, Silver Chain - “True GRIT” the Evolvement of Primary Health Nurse Practitioners
44
“True GRIT” the Evolvement of Primary Health Nurse Practitioners Lesley Pearson Primary Health Regional Manager
-
Upload
informa-australia -
Category
Health & Medicine
-
view
246 -
download
1
description
Lesley Pearson, Regional Manager, Silver Chain Group, Primary Health, Country WA delivered the presentation at the 2014 Developing the Role of the Nurse Practitioner Conference. The Developing the Role of the Nurse Practitioner Conference 2014 is for organisations and managers looking to better understand, utilise and grow the role of the nurse practitioner in their health service. For more information about the event, please visit: http://www.healthcareconferences.com.au/npconference14
Transcript of Lesley Pearson, Silver Chain - “True GRIT” the Evolvement of Primary Health Nurse Practitioners

“True GRIT” the Evolvement of
Primary Health Nurse Practitioners
Lesley Pearson Primary Health Regional Manager
Silver Chain Purpose
The Silver Chain group exists to:
Build community capacity to optimise health and
wellbeing
Community capacity can be defined as “the collection of
characteristics and resources which, when combined,
improve the ability of a community to recognise, evaluate
and address key problems” (University of Queensland).
Health can be defined as “a state of complete physical,
mental and social and not merely the absence of disease
or infirmity” (WHO).

Shark Bay
Abrolhos Islands
Mingenew
Leeman
Eneabba
Beacon
Bencubbin
Brookton Hyden
Walpole
Eucla
Lancelin
The 12 Remote Area sites
SIHI Regions

• First Point of Entry into the Health
system
• Essential to the Health and
Wellbeing of a Community
• Supports Health Promotion and
Education
• Wide service access to vulnerable
groups.
• Delivers better health outcomes at
a lower cost
Primary Health …….

• State Government
funding
• Little understanding on
what the Primary Health
nursing products are and
what the cost is to deliver
• No one size fits all
• Non Recurrent Funding
• Health Reform
Silver Chain Country Primary Health

• Recent negotiations with Country
Health around Nursing posts have
reinforced the development of this
intelligence
• Nurse Practitioner pilot programs
require lobbying and transitional
planning around sustainability
• Primary Health generally has
inadequate information which effects
planning
• Ratio GP / 10,000 WA 6.4/ 7.9
• 1.5 Billion shortfall ( $180/individual)
A brief history…….

Contract Measurables

1. Collaboration and
Engagement
2. Economics
3. Business tools
4. Research
5. Innovation
6. Marketing
Deliverables

Deliverable One : Collaboration and Engagement

• Highest risk
• Testing ground
• Communication
• Relationships
• Engagement
• Contract
deliverables
Collaboration

• Different priorities
• Contract management
• Political pressures
• Changing health
environment
Relationships

• Working within complex
systems
• Frustrations
• Timely responses
• Competing priorities
• Sharing the intelligence
• Common strategic intent
Networking and Engagement

Deliverable Two: Health Economics
• Primary Health
support team
• Access to Group
Manager Business
development
• Finance business
partner

• Identification of the 4
products
1. Primary Health – NP
2. Primary Health
Emergency – NP
3. Primary Health –
Emergency RAN
4. Primary Health RAN
• Identify components that
deliver the product
The unit cost journey – the beginning

• Cost component analysis
– Direct staff costs
– Training
– Travel
– Consumables
– IT
– Building costs
– Depreciation
– Overheads
First cut

• Value proposition assumptions
– Customers and beneficiaries
– What does the market value
– What are our products
– What are the benefits for
customers
– Alternatives to our service
– Evidence of benefits
Second cut

• Reviewed the minimum cost of a
service and an „average‟ health
centre
• To analyse minimum service we
identified
– Staff mix and FTE
– Roster – on call
– Average number of call outs
– Minimum and maximum number of
clients
– Relief required
Third Cut

• Finance Business Partner
consulted
• Reviewed the true cost of all
PHRANs and PHNP staff
• Identified that demographics and
remoteness would effect unit cost
• Realised Primary Health Remote
could not provide 1 cost as per
metro HITH ($183)
• Exemplars identified based on
ARIA
Fourth Cut

• Lancelin – Inner Regional
• Walpole – Outer Regional
• Beacon – Remote
• Shark Bay – Very Remote
• EWB Hub- Remote
Exemplars for Unit Cost

1. NP roaming Primary
Health no relief cover
and no client transfer
2. NP Primary health and
Emergency Clinic based
3. RAN Primary Health
Emergency
4. RAN Primary Health only
Established Four Models

Shark Bay Primary Health and Remote NP

• Number of occasions of services in
– Prevention and Promotion
– Diagnosis and Treatment
– Scheduled services
• Attendance during
– Business hours
– After hours
– Weekend/public holiday
• Interhospital transfers
• Assumptions such as transport
costs
NP Shark Bay Inputs for exemplar site
• Four models per exemplar site
based on volume
• Inputs
– FTE
– Attendance
– Transfers
– Direct staff expenses
– Indirect expenses
• Accommodation to very remote i.e.
Eucla (Depreciation New Building)
Price on volume

Shark Bay Very Remote ARIA 10.78 Volume FTE

Shark Bay – Very Remote, all services

Shark Bay – Triage 1-5

• Triage 1 Resuscitation
• Triage 2 Emergency
• Triage 3 Urgent
• Triage 4 Semi Urgent
• Triage 5 Non Urgent
Triage 1-5 cost assumptions

SIHI Nurse Practitioners New Frontiers
Merredin Primary Health NP SIHI RA4

Primary Health Only
• Strategic thinking
• Clinical Leadership
(MDT)
• Wound Care
• Stoma Therapy
• Mentoring
• Staff development

• Triage 3,4,5
• Scheduled Services –
Primary Health clinics
• Diagnosis and
Treatment – e.g.
immunisation, mental
health, adult chronic
disease
• Women‟s Health
• Telehealth
Primary Health Only
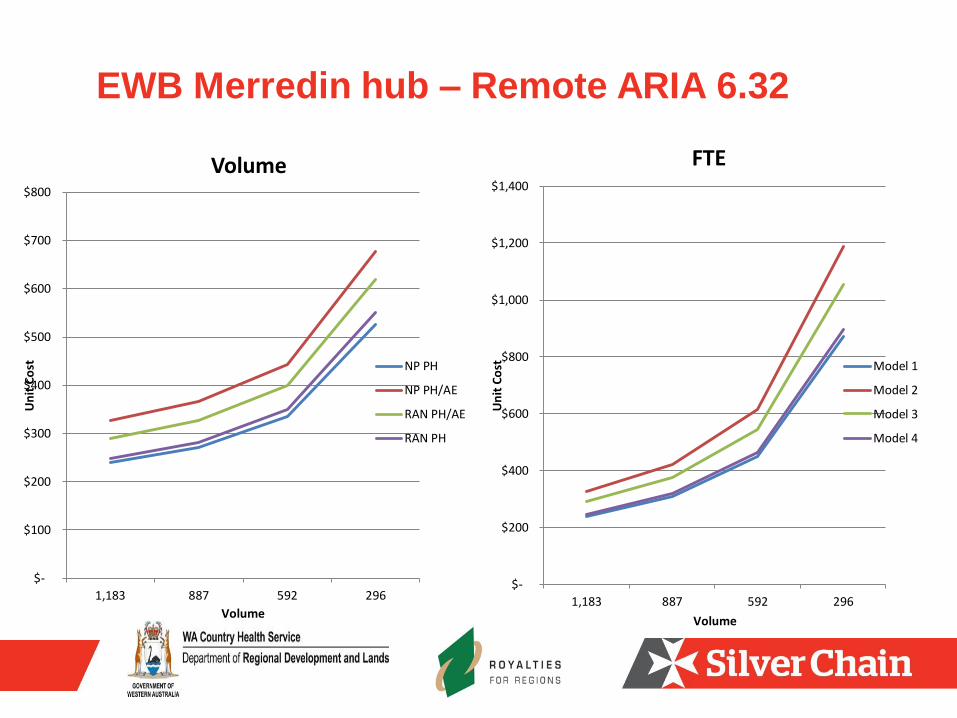
EWB Merredin hub – Remote ARIA 6.32
$-
$100
$200
$300
$400
$500
$600
$700
$800
1,183 887 592 296
Un
it C
ost
Volume
Volume
NP PH
NP PH/AE
RAN PH/AE
RAN PH
$-
$200
$400
$600
$800
$1,000
$1,200
$1,400
1,183 887 592 296
Un
it C
ost
Volume
FTE
Model 1
Model 2
Model 3
Model 4

Model EWB Merredin hub
• Medicare income 30%
• Travel 1,000km / week
• Volume 1183 increasing
• Agreed assumptions around
the product
• Political benefit for investment
• Bilateral PHC conversations
state and commonwealth
SIHI Nurse Practitioners

• Price on volume is limited in
use for remote locations
• FTE cost analysis does not
determine the product
requirements for this
modelling
• Both models have
limitations
• Business financial
modelling with Private
practice is critical
Deliverable Two findings to date

• Best Practice
• COMCARE
• Smartphones
• Flablets
• Samsung tablets
• PHCG committee
• Operational Manual
Deliverable: Three Business Tools

• Silver Chain QOL Client
feedback
• UWA/Silver Chain
• DOHA
• CRANA
• Contract and reporting
• DOH and WACHS
Deliverable Four : Research

• Improved Health Access
• Reduced client travel
• Power of story telling Case
studies ( built into to all
levels reporting)
• Poor Care coordination
Deliverable Four : Findings

• Health Navigator
• Integrated record systems
linkages Best Practice
• Business system flow
across agencies ( client
records)
• NP modelling innovating
changes to Remote Primary
Health
• Financial analysis
Deliverable Five: Innovation

Deliverable Six: Marketing

• Phone applications
• Pilot trials
• Political
• Media
• Merchandise
• Targeted to community
Marketing

• Developing Applications
for products
• Webpages
• You-tube
• On line appointments
Marketing

• Posters in ED
• Local Media
• Proposed Film series
• Story telling-Bill‟s story
• Royalties for Regions
• Logos
• Conferences
Marketing Outcomes

Contract Negotiations:
• SIHI contract ends June 2016
linkages into clinical Strategic
planning 2020
• Aged Care NP contract ends
June 2014
• Discussions with Medicare
Local re a business model with
GP practice and Primary
Health NP Aged Care/Primary
Health
Future: Sustainability

Nurse Practitioner Future
• Candidacy program
• Medicare payments
• Stronger business
acumen
• Consumer Choice
• Private Health Insurers
• Primary Health Marketing
• Value add proposition to
Government


















