
Ledipasvir/sofosbuvir for 12 weeks in patients co-infected with HCV and HIV-1
22
Ledipasvir/Sofosbuvir for 12 Weeks in Patients Coinfected With HCV and HIV-1: ION-4 Curtis Cooper 1 , Susanna Naggie 2 ,Michael Saag 3 , Luisa M. Stamm 4 , Jenny C. Yang 4 , Phillip S. Pang 4 , John G. McHutchison 4 , Douglas Dieterich 5 , Mark Sulkowski 6 1 University of Ottawa, 2 Duke Clinical Research Institute, Durham, NC; The Ottawa Hospital, Ottawa, ON; 3 University of Alabama at Birmingham, Birmingham, AL, 4 Gilead Sciences, Inc., Foster City, CA; 5 Icahn School of Medicine at Mount Sinai, New York, NY; 6 Johns Hopkins University School of Medicine, Baltimore, MD IAS 2015, Vancouver
-
Upload
- -
Category
Healthcare
-
view
30 -
download
0
Transcript of Ledipasvir/sofosbuvir for 12 weeks in patients co-infected with HCV and HIV-1

Ledipasvir/Sofosbuvir for 12 Weeks in Patients Coinfected With HCV and HIV-1: ION-4
Curtis Cooper1, Susanna Naggie2,Michael Saag3, Luisa M. Stamm4, Jenny C. Yang4, Phillip S. Pang4, John G. McHutchison4, Douglas Dieterich5, Mark Sulkowski6
1 University of Ottawa, 2Duke Clinical Research Institute, Durham, NC; The Ottawa Hospital, Ottawa, ON; 3University of Alabama at Birmingham, Birmingham, AL,4Gilead Sciences, Inc., Foster City, CA; 5Icahn School of Medicine at Mount Sinai, New York, NY; 6Johns Hopkins University School of Medicine, Baltimore, MD
IAS 2015, Vancouver
2
Disclosures
Dr. Cooper received funding as a :
Speaker for Gilead Sciences, Abbvie
Consultant for Gilead Sciences, Abbvie, MK, BMS
Program Funding for Gilead Sciences, Abbvie. MK, Roche
3
Background
Ledipasvir
– Once-daily, oral, 90-mg NS5A inhibitor
Sofosbuvir
‒ Once-daily, oral, 400-mg NS5B inhibitor
Ledipasvir/Sofosbuvir FDC– Once-daily, oral, fixed-dose
(90/400 mg) combination tablet– Single-tablet regimen for
hepatitis C
FDC, fixed-dose combination.
SOF nucleotide
polymerase inhibitor
LDVNS5A
inhibitor
SOF nucleotide
polymerase inhibitor
SOF nucleotide
polymerase inhibitor
LDVNS5A inhibitor
N
NN
O
NO
O
H
H
N
O
N O
O
H
N
N
H HFF
SOF nucleotide polymerase inhibitor
LDVNS5A inhibitor
OO N
NH
O
O
P
O
HN
O
O
OH3C
H3C
CH3
HO F
CH3 SOF nucleotide polymerase inhibitor

Background and AimsHIV-HCV (ION-4)
Liver-related complications remain a leading cause of death among HIV/HCV-coinfected patients1
Safe and effective oral treatments compatible with multiple antiretrovirals are needed for the eradication of HCV in HIV/HCV-coinfected patients
Aim of this study was to evaluate the efficacy and safety of LDV/SOF for the treatment of HCV in patients coinfected with HIV-1, currently on antiretroviral therapy
41Smith, CJ et al. Lancet 2014; 384:241-8.
Study DesignHIV-HCV (ION-4))
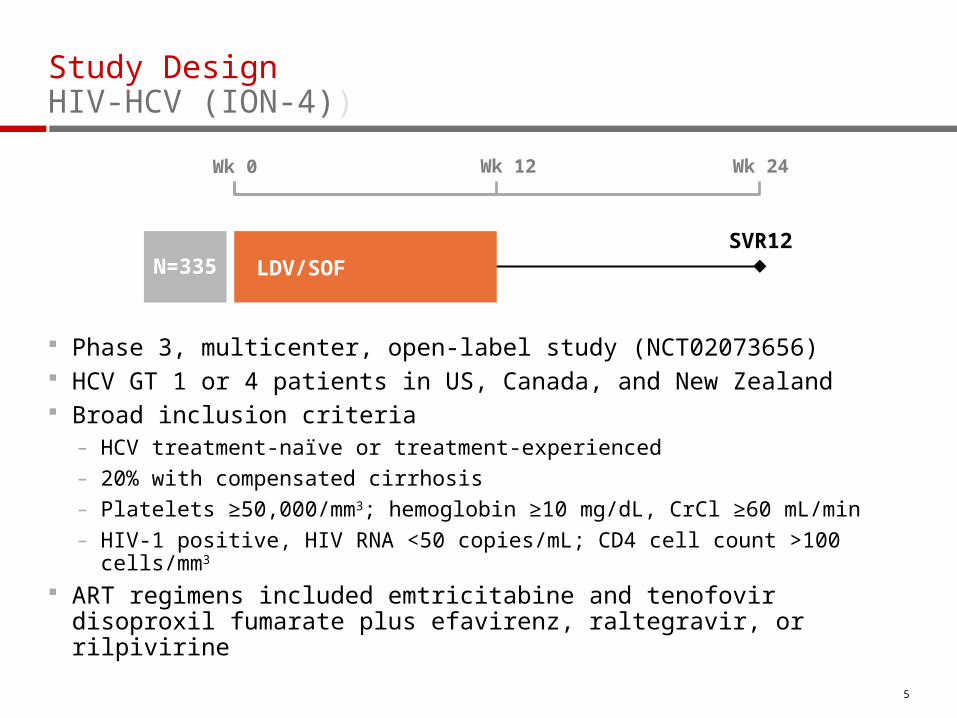
Phase 3, multicenter, open-label study (NCT02073656) HCV GT 1 or 4 patients in US, Canada, and New Zealand Broad inclusion criteria
– HCV treatment-naïve or treatment-experienced– 20% with compensated cirrhosis– Platelets ≥50,000/mm3; hemoglobin ≥10 mg/dL, CrCl ≥60 mL/min– HIV-1 positive, HIV RNA <50 copies/mL; CD4 cell count >100 cells/mm3
ART regimens included emtricitabine and tenofovir disoproxil fumarate plus efavirenz, raltegravir, or rilpivirine
5
Wk 0 Wk 12 Wk 24
SVR12 LDV/SOFN=335

EndpointsHIV-HCV (ION-4)
Primary efficacy endpoint: SVR12 – HCV RNA <LLOQ at post-treatment Week 12
HCV RNA analyzed by COBAS TaqMan HCV Test v2.0 HPS, with LLOQ of 25 IU/mL
Safety– Adverse events and discontinuations
– Maintenance of HIV-1 RNA <50 copies/mL
– Serum creatinine
6

7
Results: Demographics and Baseline CharacteristicsHIV-HCV (ION-4)
LDV/SOF 12 weeksN=335
Mean age, y (range) 52 (26-72)
Male, n (%) 276 (82)
Black, n (%) 115 (34)
Hispanic or Latino, n (%) 56 (17)
Mean BMI, kg/m2 (range) 27 (18-66)
IL28B CC, n (%) 81 (24)
GT 1 327 (98)
HCV treatment experienced, n (%) 185 (55)
Cirrhosis, n (%) 67 (20)
Mean HCV RNA, log10 IU/mL ± SD 6.7 ± 0.6
Median CD4 cell count, cells/µL (range) 628 (106-2069)
HIV ARV Regimen
Efavirenz + FTC + TDF 160 (48)
Raltegravir + FTC + TDF 146 (44)
Rilpivirine + FTC + TDF 29 (9)

0
20
40
60
80
100
Naïve vs ExperiencedOverall Cirrhosis Status
LDV/SOF 12 Weeks
ExperiencedNaïve No Cirrhosis Cirrhosis
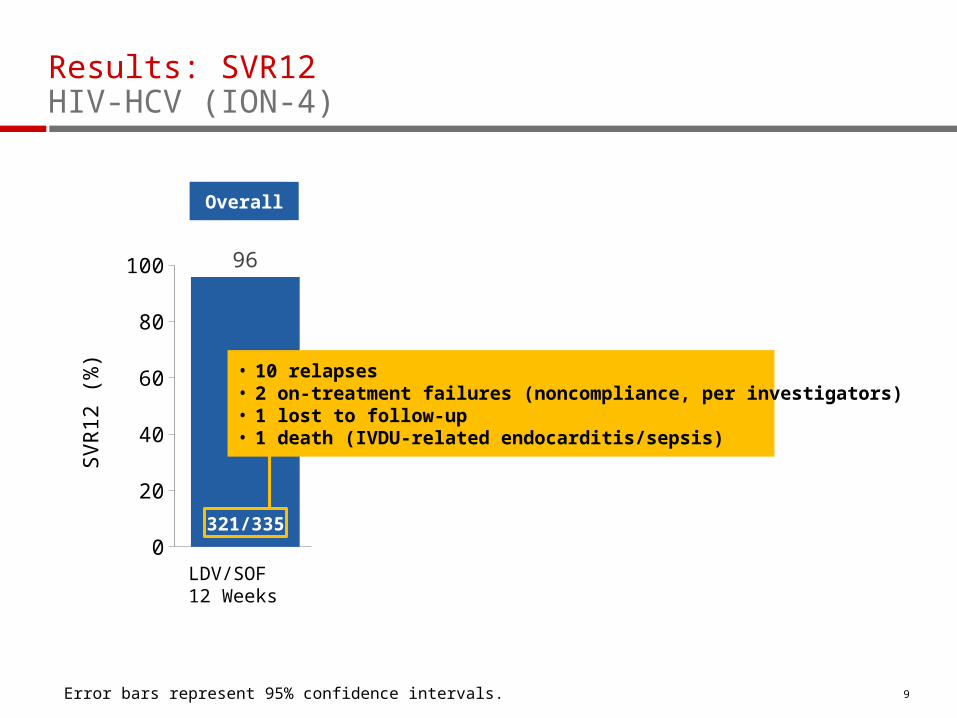
321/335 142/150 179/185 63/67258/268
SV
R12
(%
)Results: SVR12HIV-HCV (ION-4)
8Error bars represent 95% confidence intervals.
0
20
40
60
80
100
Naïve vs ExperiencedOverall Cirrhosis Status
LDV/SOF 12 Weeks
ExperiencedNaïve No Cirrhosis Cirrhosis
321/335 142/150 179/185 63/67258/268
SV
R12
(%
)Results: SVR12HIV-HCV (ION-4)
9
• 10 relapses • 2 on-treatment failures (noncompliance, per investigators)• 1 lost to follow-up• 1 death (IVDU-related endocarditis/sepsis)
Overall
Error bars represent 95% confidence intervals.

0
20
40
60
80
100 96 95 97 96 94
Naïve vs ExperiencedOverall Cirrhosis Status
LDV/SOF 12 Weeks
ExperiencedNaïve No Cirrhosis Cirrhosis
321/335 142/150 179/185 63/67258/268
SV
R12
(%
)Results: SVR12 by Prior Treatment ExperienceHIV-HCV (ION-4)
10
Overall
Error bars represent 95% confidence intervals.

0
20
40
60
80
100 96 95 97 96 94
Naïve vs ExperiencedOverall Cirrhosis Status
LDV/SOF 12 Weeks
ExperiencedNaïve No Cirrhosis Cirrhosis
321/335 142/150 179/185 63/67258/268
SV
R12
(%
)
Results: SVR12 by Prior Treatment Experience and Cirrhosis StatusHIV-HCV (ION-4)
11
Overall
Error bars represent 95% confidence intervals.

Results: SVR12 in SubgroupsHIV-HCV (ION-4)
12
LDV/SOF 12 Weeks, N=335
Overall
SexMaleFemale
RaceBlackNon-Black
HCV Genotype1a1b4
Baseline HCV RNA (IU/mL)<800,000≥800,000
Baseline BMI (kg/m2)<30≥30
IL28BCCCTTT
CirrhosisNoYes
Prior HCV TreatmentNoYes
ARV RegimenEFV + FTC + TDFRAL + FTC + TDFRPV + FTC + TDF
Baseline CD4 (cells/μL)<350≥350
60 70 80 90 100SVR12, % (95% CI)

Results: SVR12 in SubgroupsHIV-HCV (ION-4)
13
LDV/SOF 12 Weeks, N=335
Overall
SexMaleFemale
RaceBlackNon-Black
HCV Genotype1a1b4
Baseline HCV RNA (IU/mL)<800,000≥800,000
Baseline BMI (kg/m2)<30≥30
IL28BCCCTTT
CirrhosisNoYes
Prior HCV TreatmentNoYes
ARV RegimenEFV + FTC + TDFRAL + FTC + TDFRPV + FTC + TDF
Baseline CD4 (cells/μL)<350≥350
60 70 80 90 100SVR12, % (95% CI)
Statistically significantin multivariate analysis

Overall EFV/FTC/TDF RAL+FTC/TDF RPV/FTC/TDF0
20
40
60
80
10099 100 98 100
9085
9590
Non-Black Black
% S
VR
12
103/115215/217 52/6197/97 13/13 49/5042/44100/102 9/1018/18
ION-4 – LDV/SOF in HIV/HCV
SVR12 by ARV Regimen and Race
PK and Other Exploratory AnalysesHIV-HCV (ION-4)
No difference in SVR in HCV mono-infected ION program (12 weeks) for black (89/90, 99%) versus non-black (431/448, 96%)2
LDV and SOF population PK levels– Similar across the different ARV regimens
– Similar between black and non-black patients
– Similar between patients who relapsed and those who achieved SVR
GWAS and whole genome sequencing analysis underway
152Lennox et al. AASLD 2014 Oral abstract #237
Results: HCV Sequence AnalysisHIV-HCV (ION-4)
Deep sequencing of NS5A at baseline identified 59 (18%) patients with NS5A variants (RAVs)
– 55 (93%) of patients with NS5A RAVs achieved SVR12 Post-treatment NS5A RAVs were observed in 10 of the 12 patients
with virologic failure
No NS5B S282T was observed in any patient at baseline or virologic failure
16

Results: Safety SummaryHIV-HCV (ION-4)
17
*Serious AEs in >1 patient were hepatocellular carcinoma (n=2) and portal vein thrombosis (n=2) in patients with cirrhosis.
†Confirmed IV drug user developed Staphylococcus aureus sepsis, endocarditis with associated embolic brain abscesses, and multi-organ system failure.
Patients, n (%)LDV/SOF 12 Weeks
N=335
Overall safety
AEs 257 (77)
Grade 3‒4 AE 14 (4)
Serious AE 8 (2)*
Treatment D/C due to AE 0
Death 1 (<1)†
Grade 3‒4 laboratory abnormality 36 (11)
¨ Stable CD4 counts through treatment and follow-up phase
¨ No patient had confirmed HIV virologic rebound

Results: Adverse Events (≥5%)HIV-HCV (ION-4)
18
Patients, n (%)LDV/SOF 12 Weeks
N=335
Headache 83 (25)
Fatigue 71 (21)
Diarrhea 36 (11)
Nausea 33 (10)
Arthralgia 22 (7)
Upper respiratory tract infection 18 (5)

Results: Renal FunctionHIV-HCV (ION-4)
19
EFV+FTC+TDF (n=160)
RAL+FTC+TDF (n=146)
RPV+FTC+TDF (n=29)
LDV/SOF +
60
70
80
90
100
110
Cre
atin
ine
Cle
aran
ce(m
L/m
in),
mea
n ±
SD
WeekBL 1 2 4 6 8 10 12 FU-4
¨ 4 patients (1%) had change in creatinine ≥ 0.4 mg/dL– 2 completed treatment with no ART change
– 1 had dose reduction of TDF, 1 discontinued TDF

ConclusionsHIV-HCV (ION-4)
In this Phase 3 study of 335 HIV/HCV-coinfected patients, 96% achieved SVR12 after 12 weeks of a once-daily, single-tablet regimen of LDV/SOF– Prior HCV treatment status or the presence or absence of cirrhosis
did not impact outcome
– In contrast to larger studies among monoinfected patients, a lower response rate was observed among coinfected black patients treated with LDV/SOF (SVR12 90%)
LDV/SOF was well tolerated, with no treatment discontinuations due to adverse events and no adverse impact on HIV disease or its treatment
20


Acknowledgments
22
We extend our thanks to:
The patients and their families
All participating investigators throughout the US, Canada, and New Zealand
This study was funded by Gilead Sciences, Inc.
UNITED STATES: David Asmuth, Rachel Baden, Meena Bansal, Maurizio Bonacini, Norbert Brau, U. Fritz Bredeek, Raymond Chung, Calvin J. Cohen, Eric Daar, Craig Dietz, Robin Henry Dretler, Richard Elion, W.J. Fessel, Jason Flamm, Timonthy Friel, Joel E. Gallant, Joseph C. Gathe, Eliot Godofsky, Philip M. Grant, Federico Hinestrosa, Gregory Huhn, Mamta Jain, Dushyantha Jayaweera, Donald Kotler, Jay Lalezari, Charles Landis, Annie Luetkemeyer, Kristen Marks, Cynthia Mayer, Anthony Mills, Karam Mounzer, Susanna Naggie, Bruce S. Rashbaum, Jorge E. Rodriguez, Peter J. Ruane, Paul Edward Sax, Michael Saag, Kenneth Sherman, Marc Siegel, Richard Sterling, Mark Sulkowski, Karen T. Tashima, Pablo Tebas, Melanie A. Thompson, William J. Towner, Chia Wang, David A. Wheeler, David A. Wohl, Kimberly Workowski, David Wyles, Benjamin Young CANADA: Curtis Cooper, Emmanuelle Huchet, Mark Hull, Marina Klein, David Wong PUERTO RICO: Javier O. Morales-Ramirez, Jorge L. Santana-Bagur NEW ZEALAND: Edward Gane, Catherine Stedman


















