Lecture positioning for spinal surgery
52
Positioning for spinal surgery Upper Chesapeake medical center spine conference Friday November 3 rd , 2017
-
Upload
spiro-antoniades -
Category
Health & Medicine
-
view
74 -
download
0
Transcript of Lecture positioning for spinal surgery

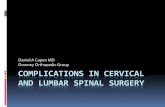
Positioning for spinal surgery
Upper Chesapeake medical center spine conference
Friday November 3rd, 2017
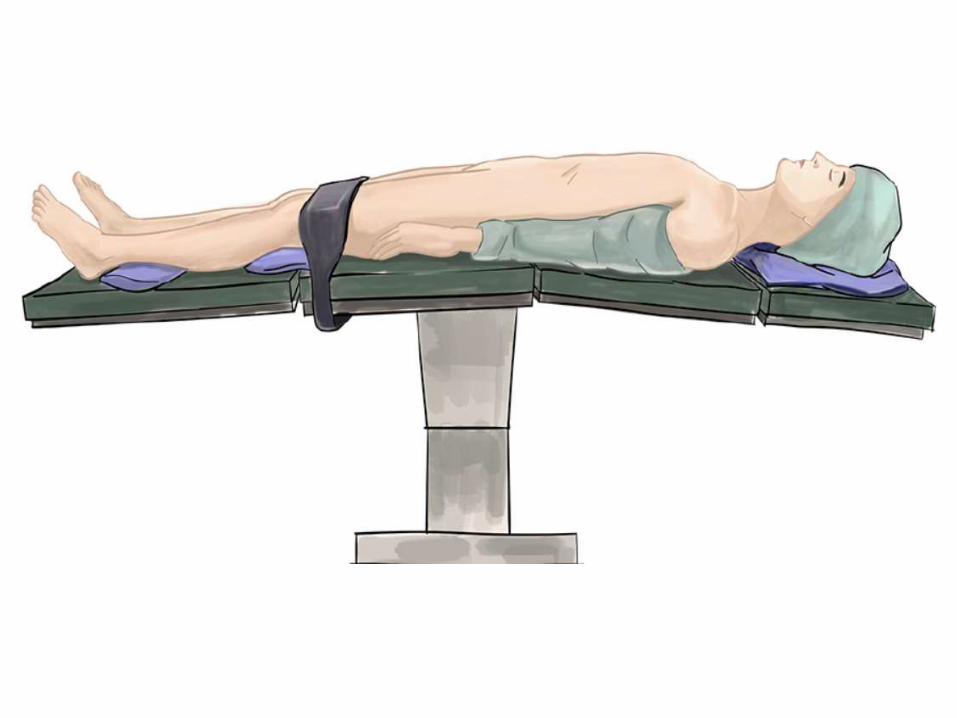
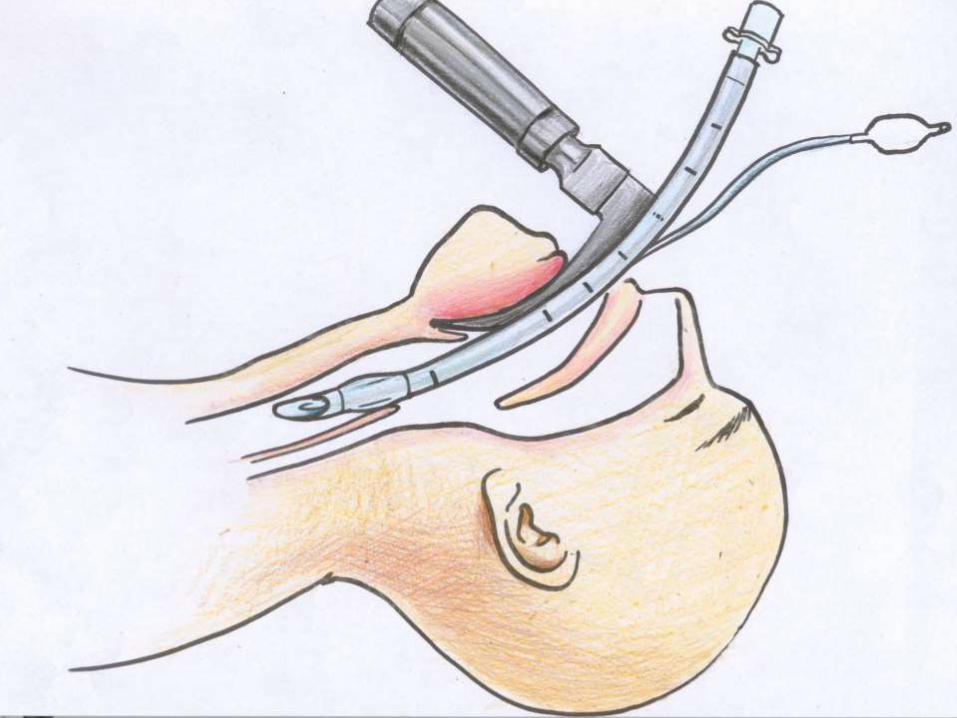
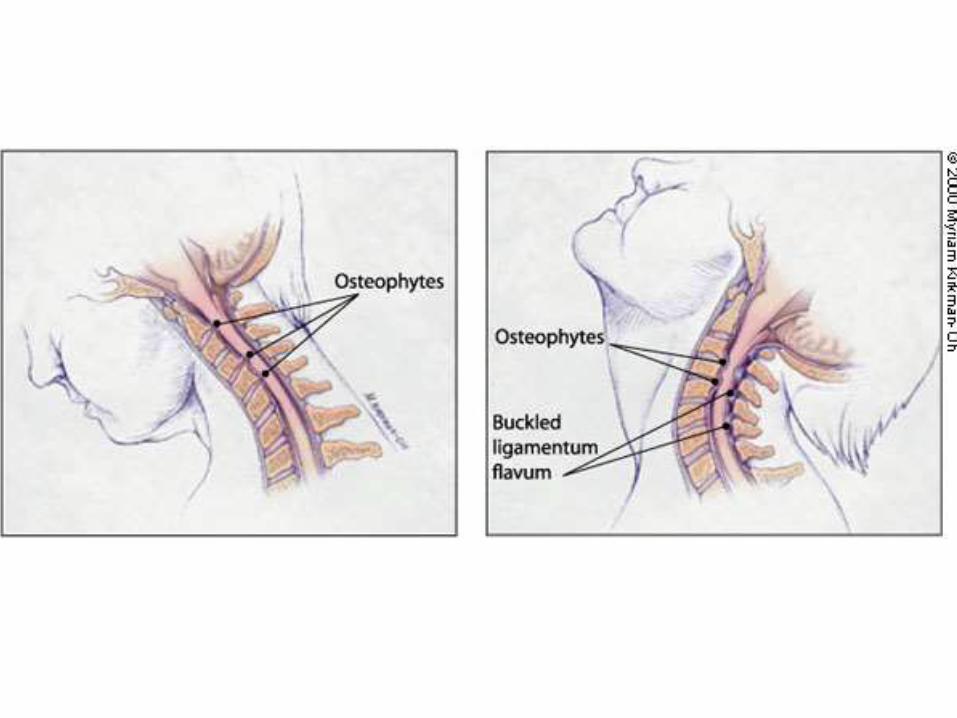
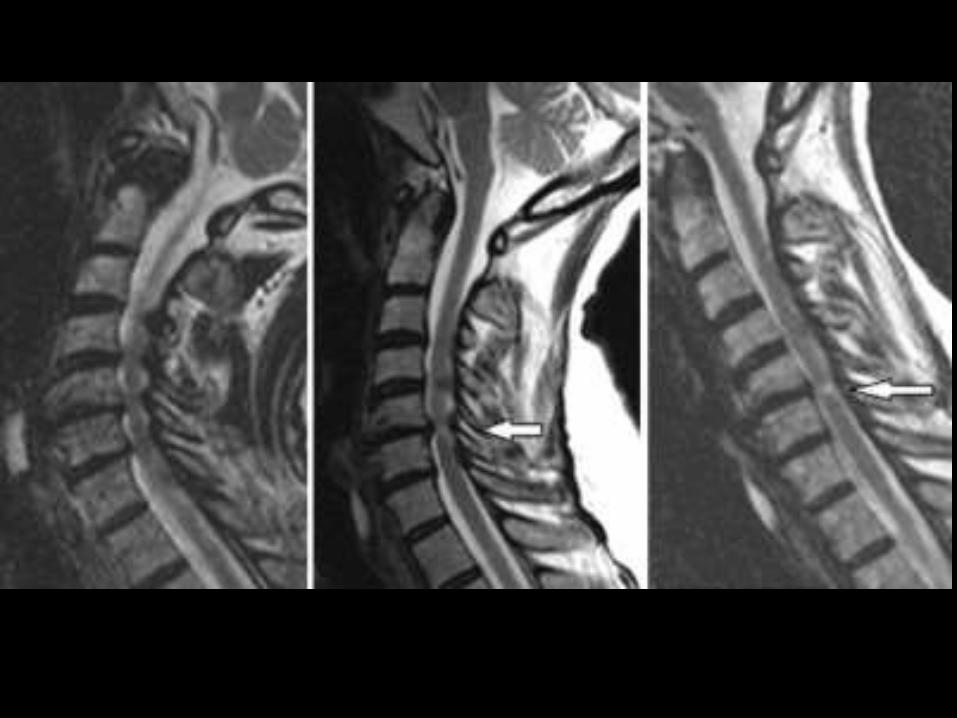
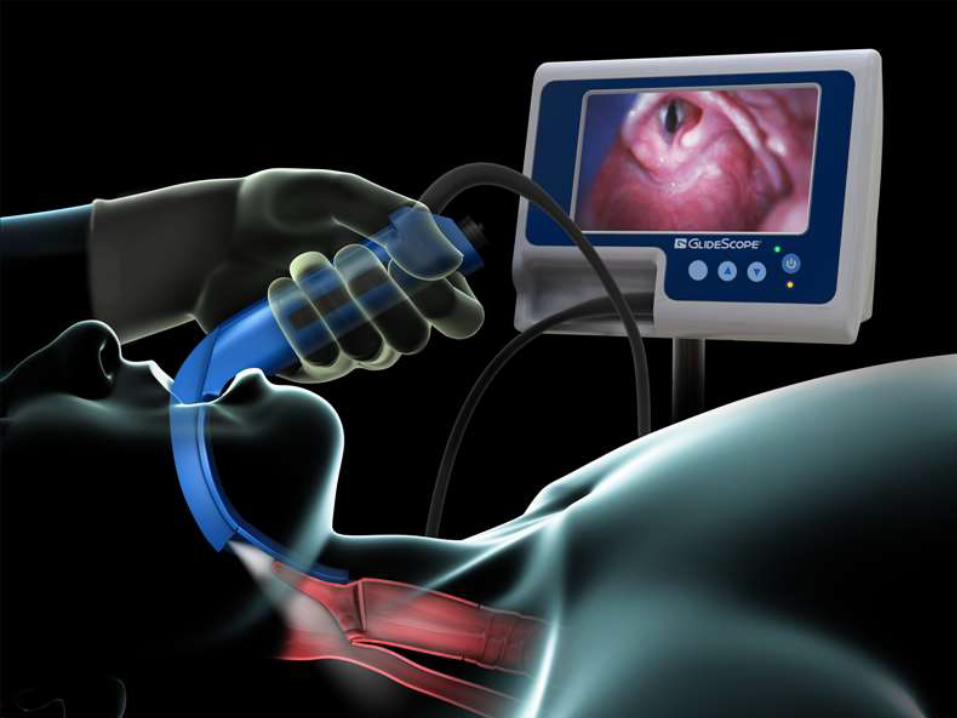
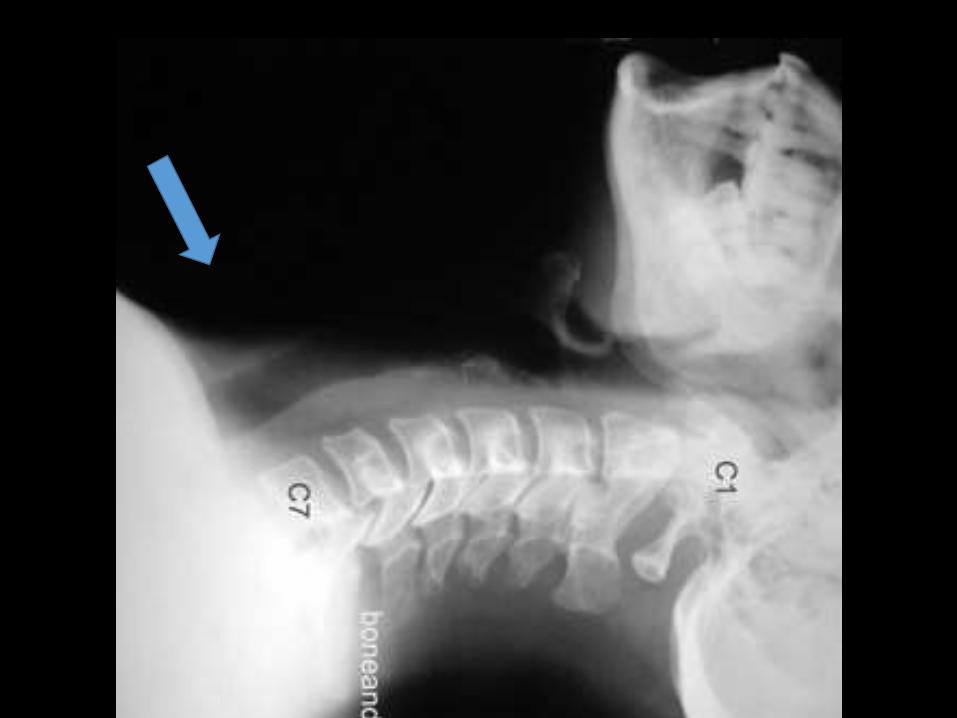
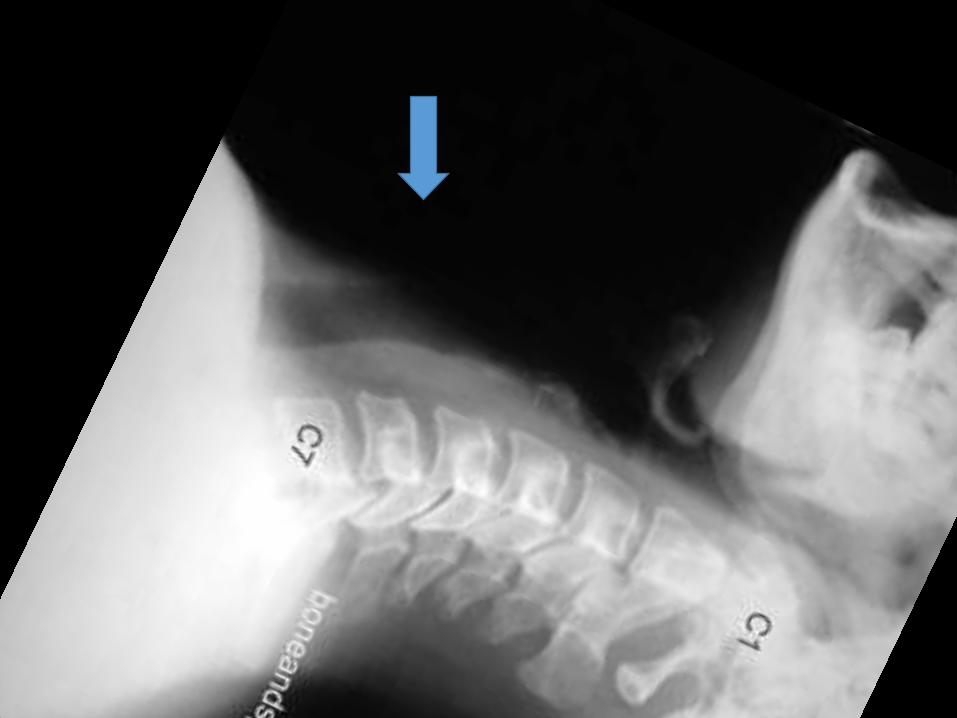
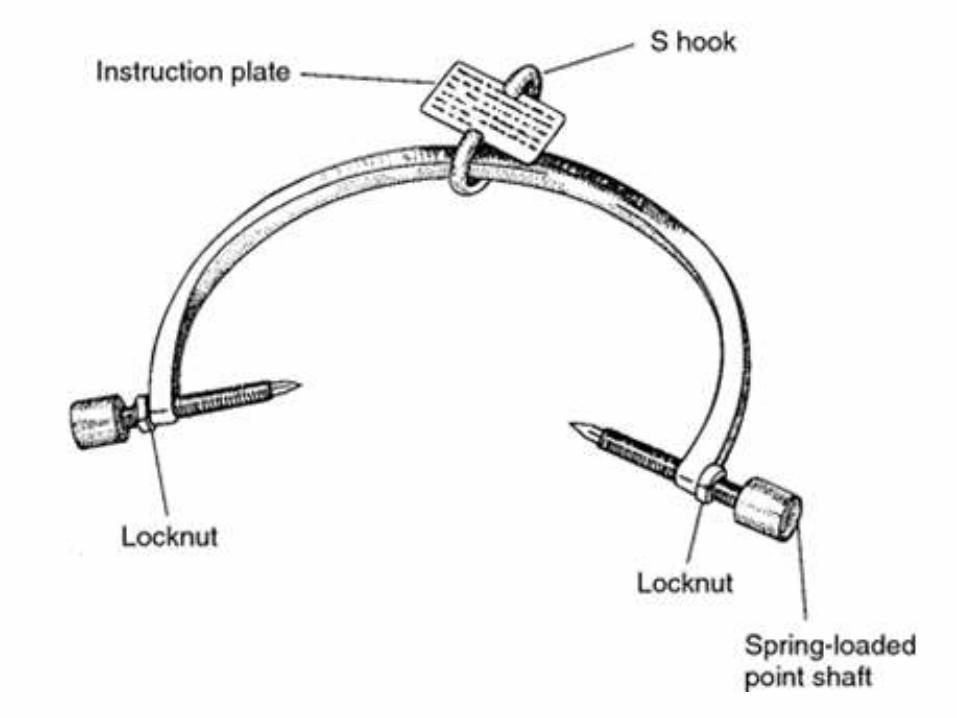
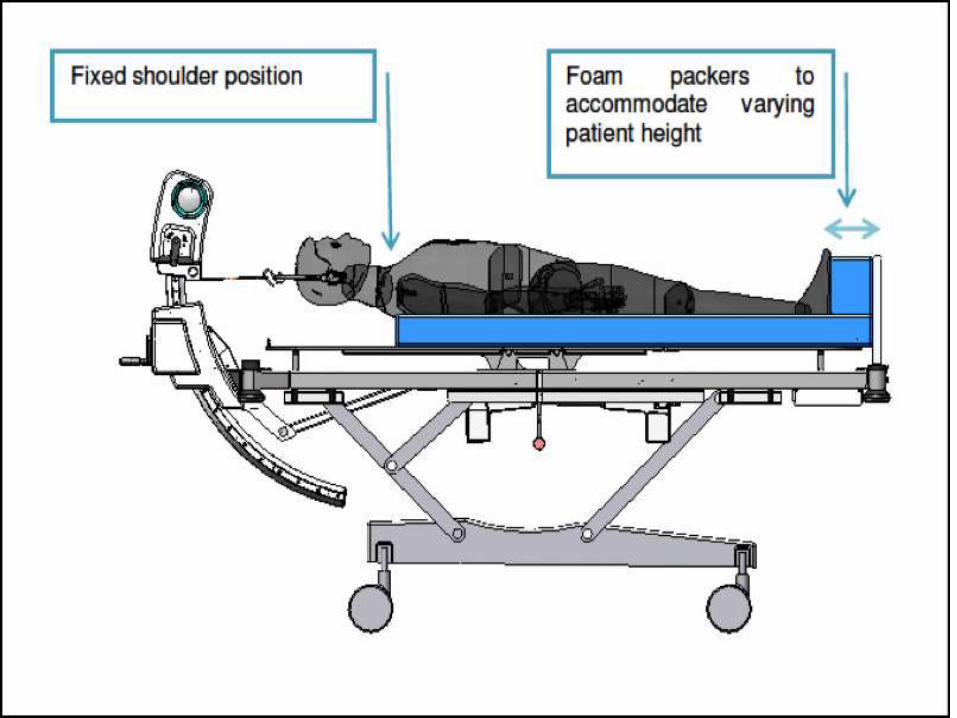
Be careful with cervical patients






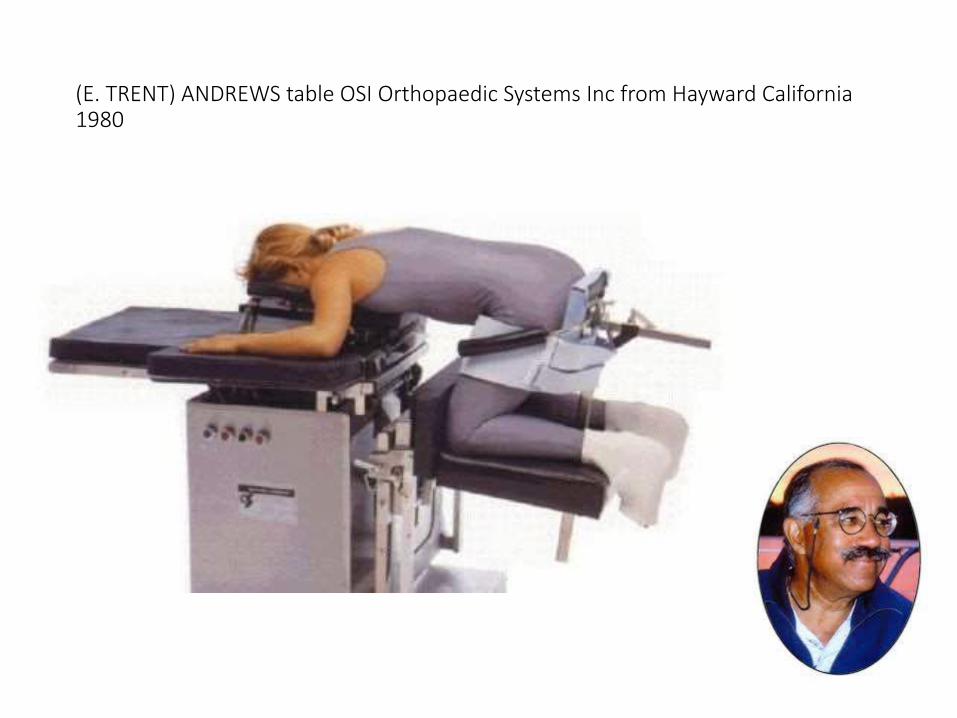
(E. TRENT) ANDREWS table OSI Orthopaedic Systems Inc from Hayward California 1980

Spinal Surgery Table 1992 OSIDr. Roger P. Jackson, has practiced at North Kansas City, Missouri late 1980’s


In 2002, OSI was acquired by Mizuho Ikakogyo Co., Ltd., in Tokyo, Japan

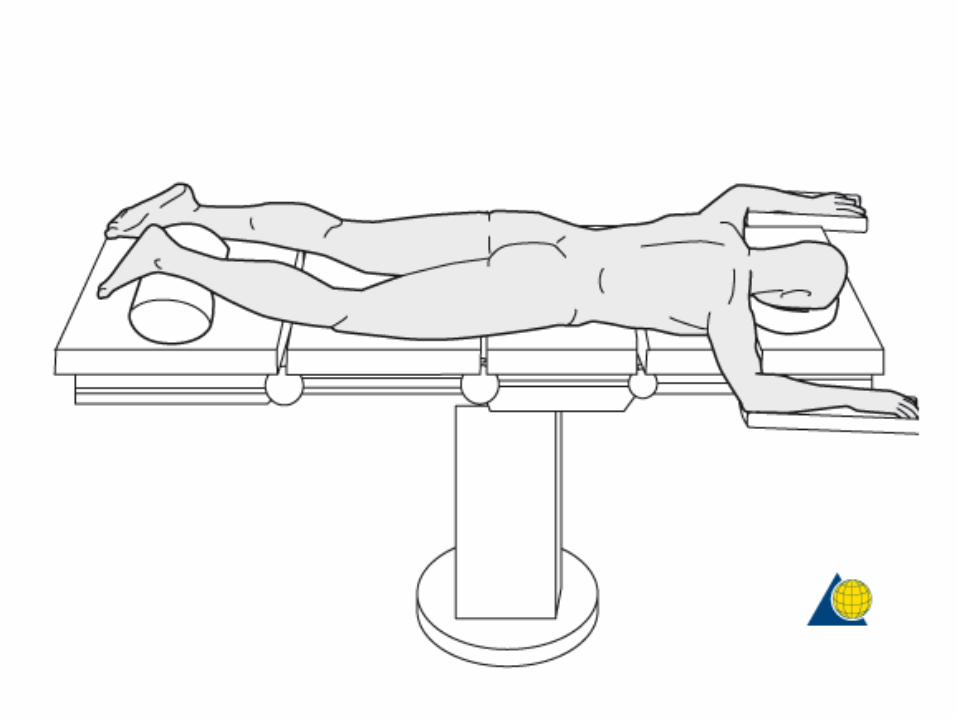
Superman prone surrender position


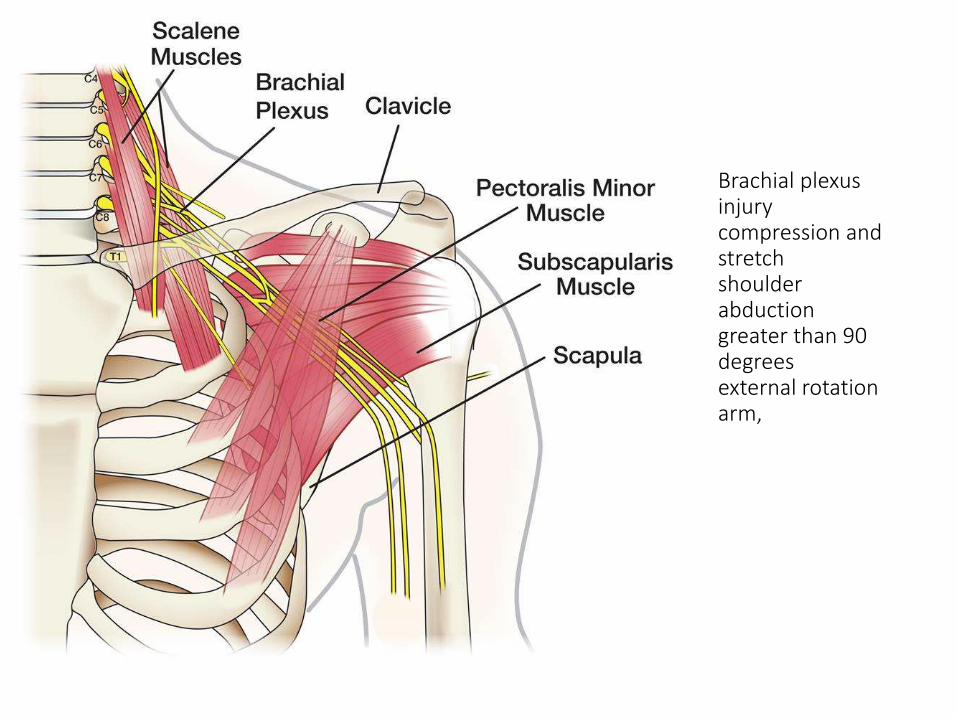
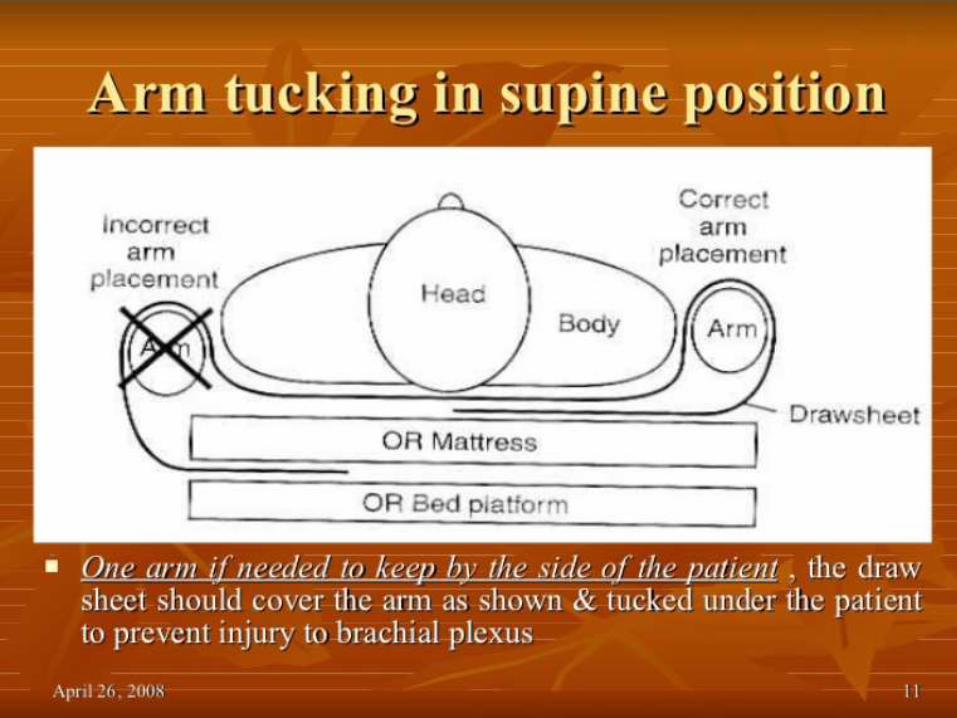
Brachial plexus injurycompression and stretchshoulder abduction greater than 90 degreesexternal rotation arm,
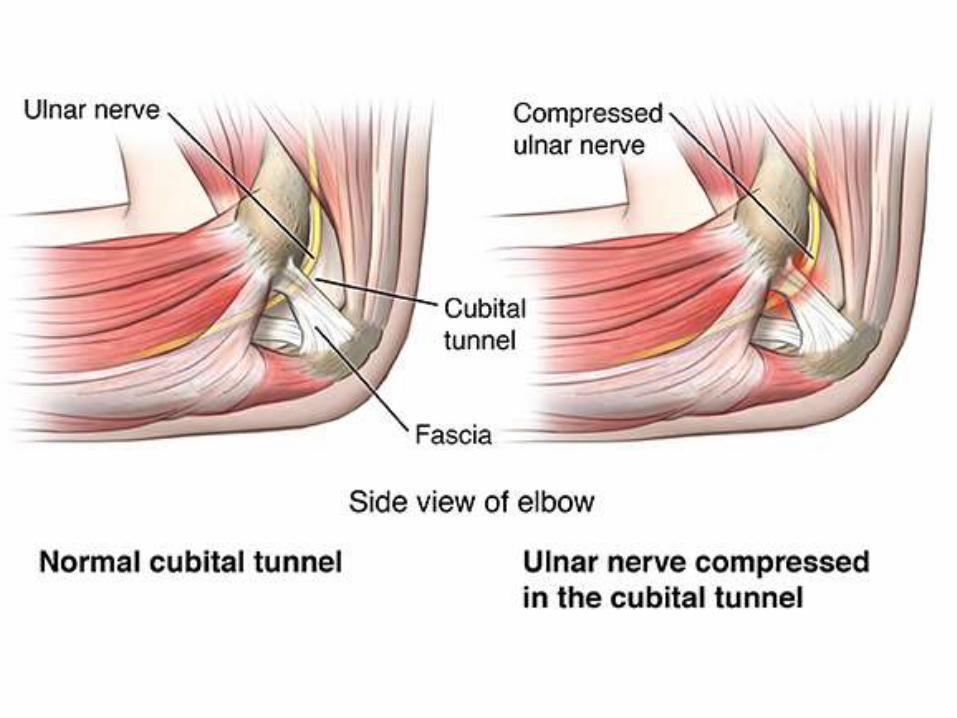
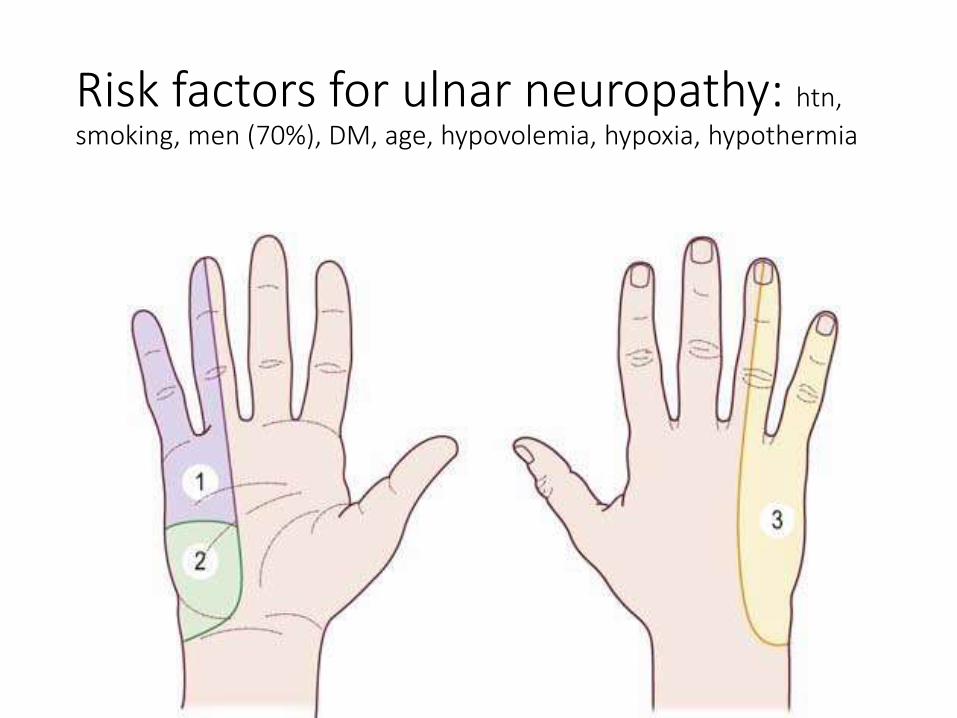
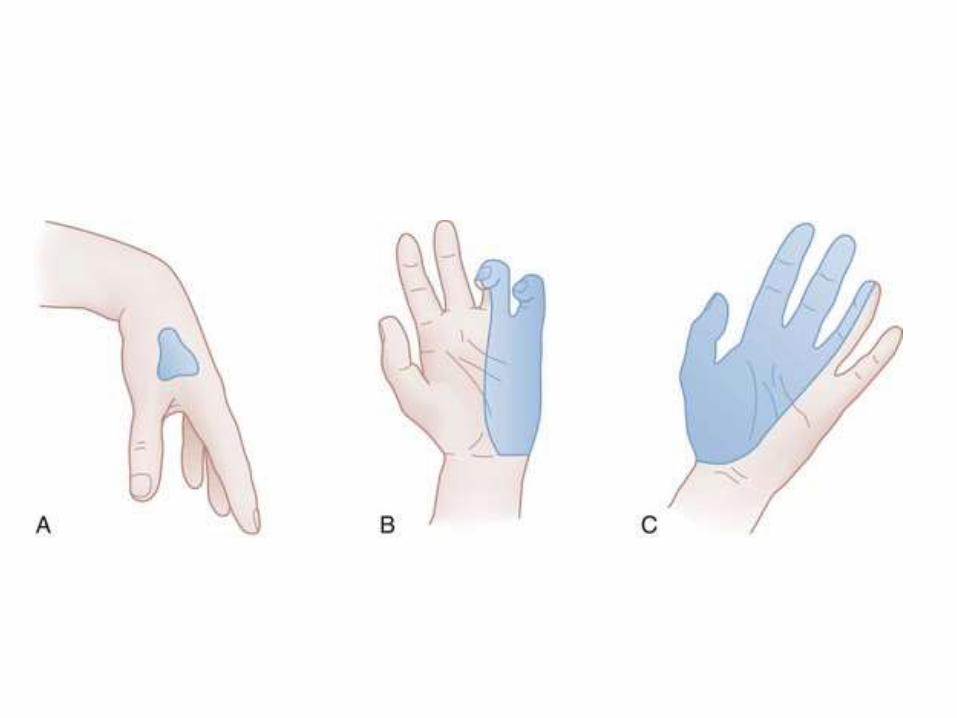
Risk factors for ulnar neuropathy: htn,
smoking, men (70%), DM, age, hypovolemia, hypoxia, hypothermia
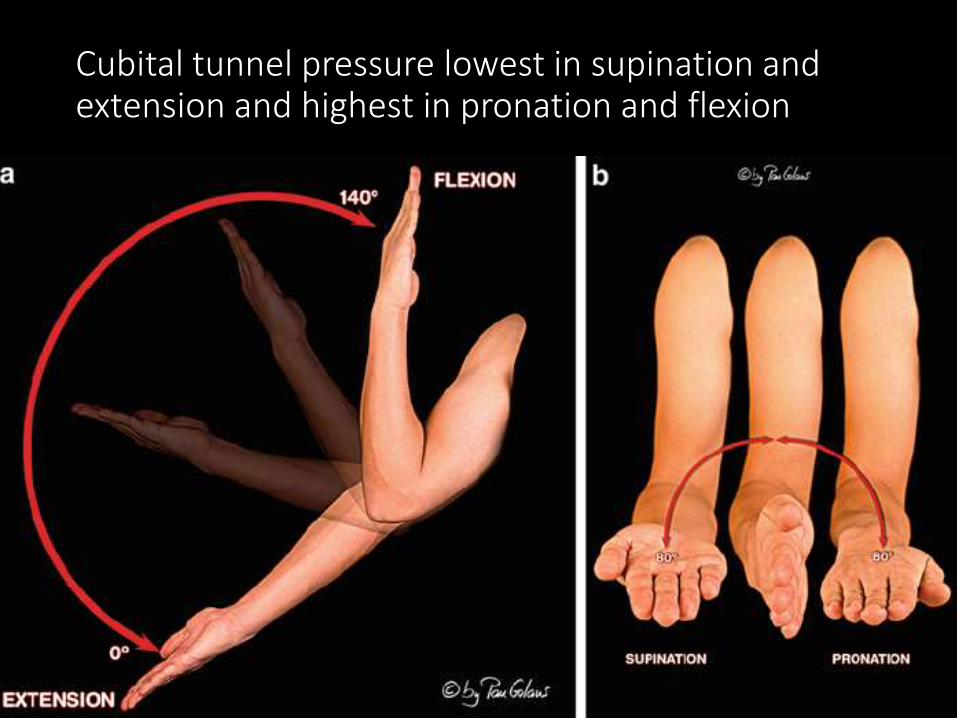
Cubital tunnel pressure lowest in supination and extension and highest in pronation and flexion
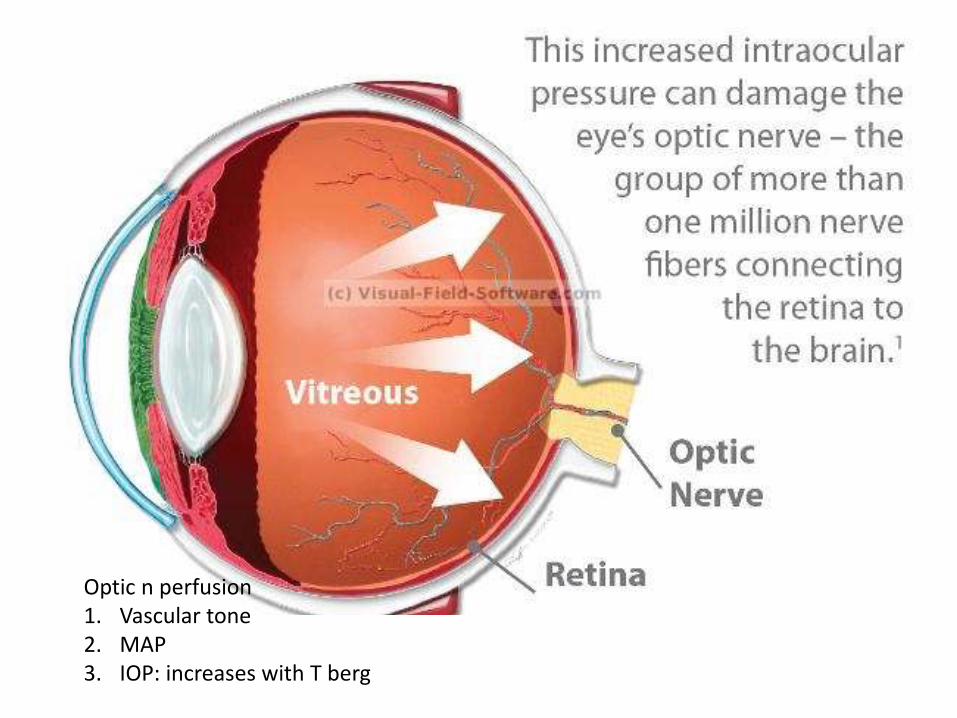
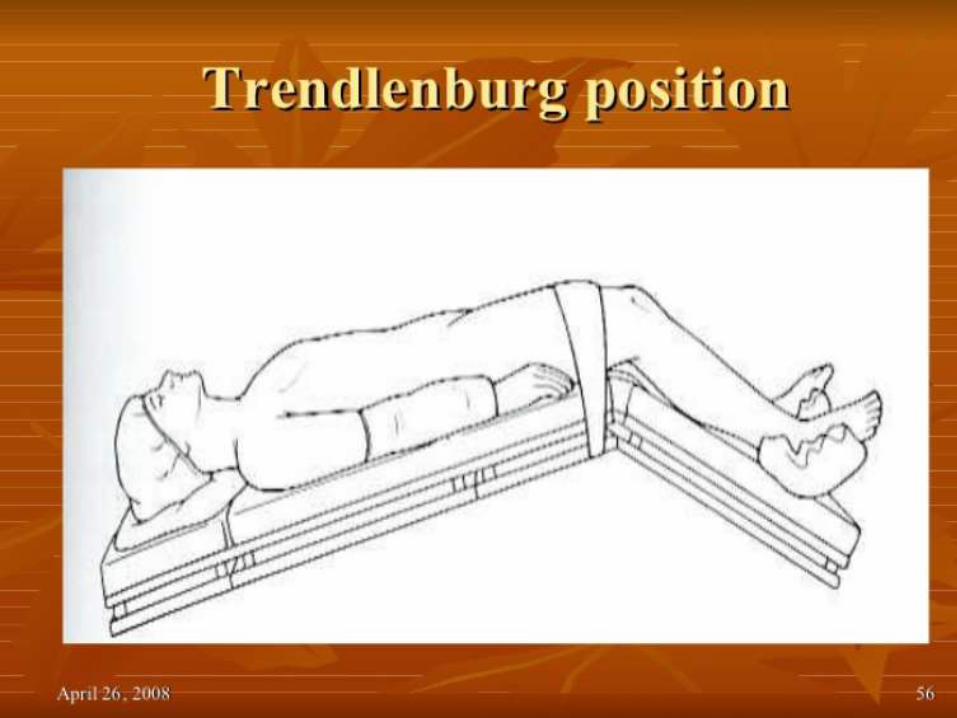
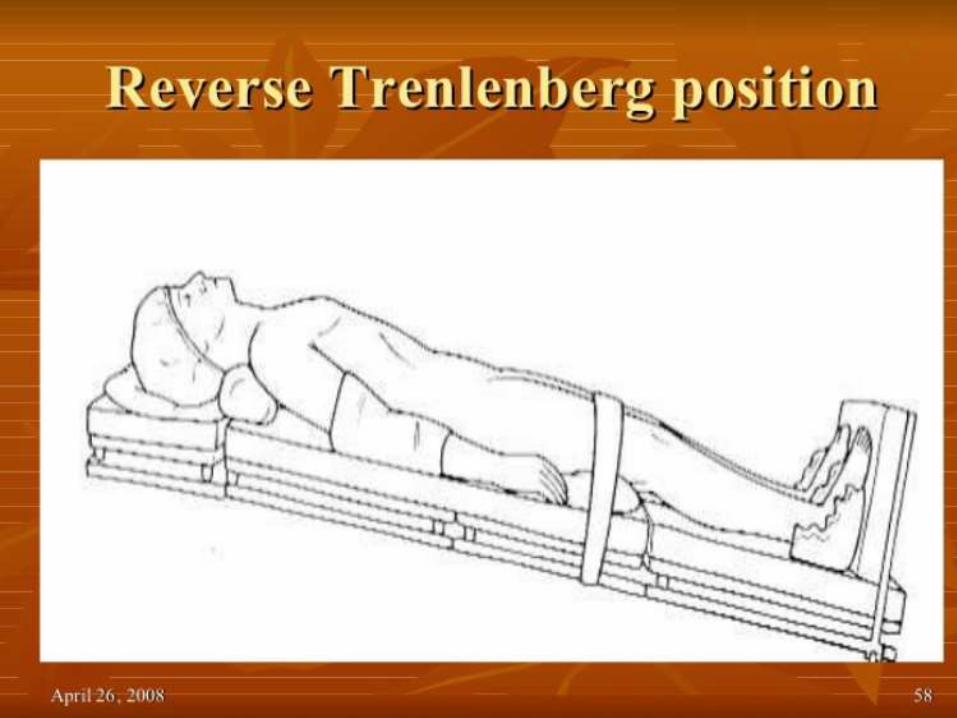
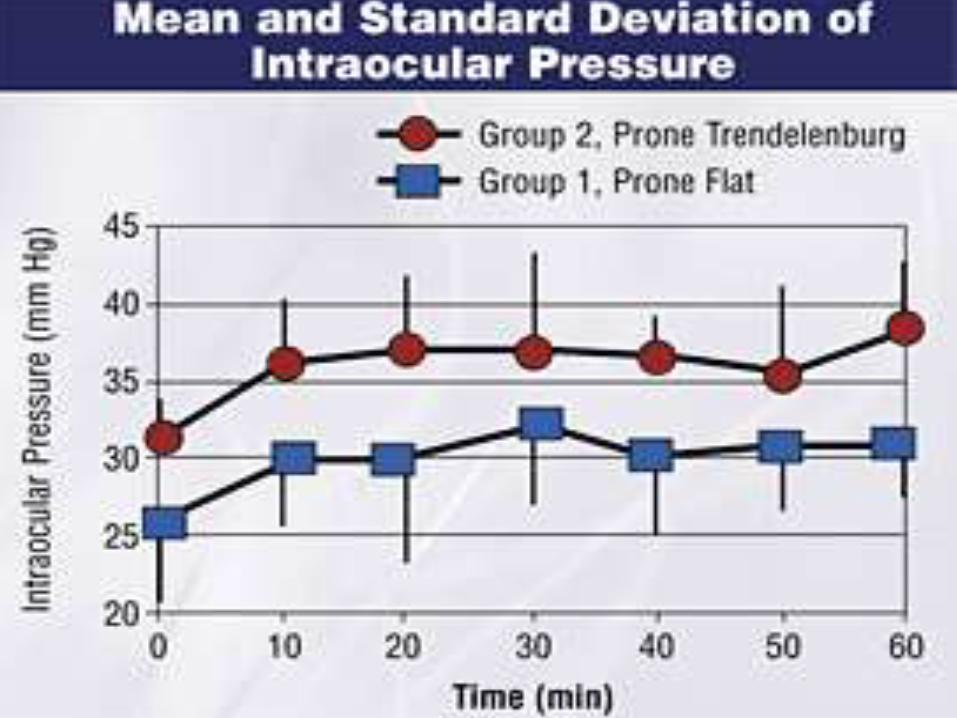
Optic n perfusion1. Vascular tone2. MAP3. IOP: increases with T berg

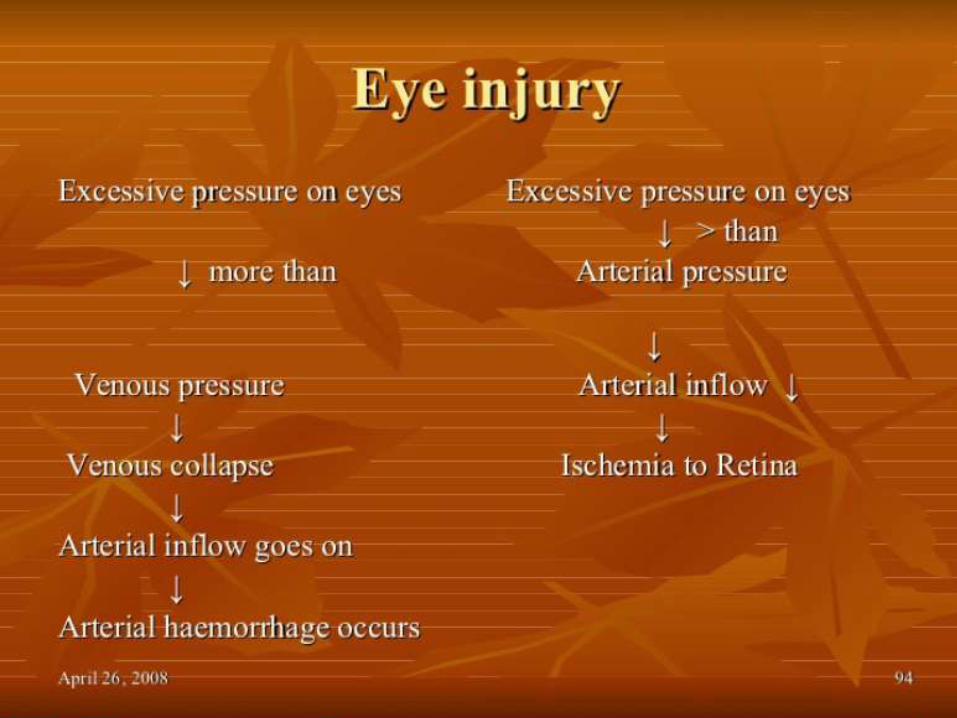
POVL: post operative visual loss
• <1:500 cases
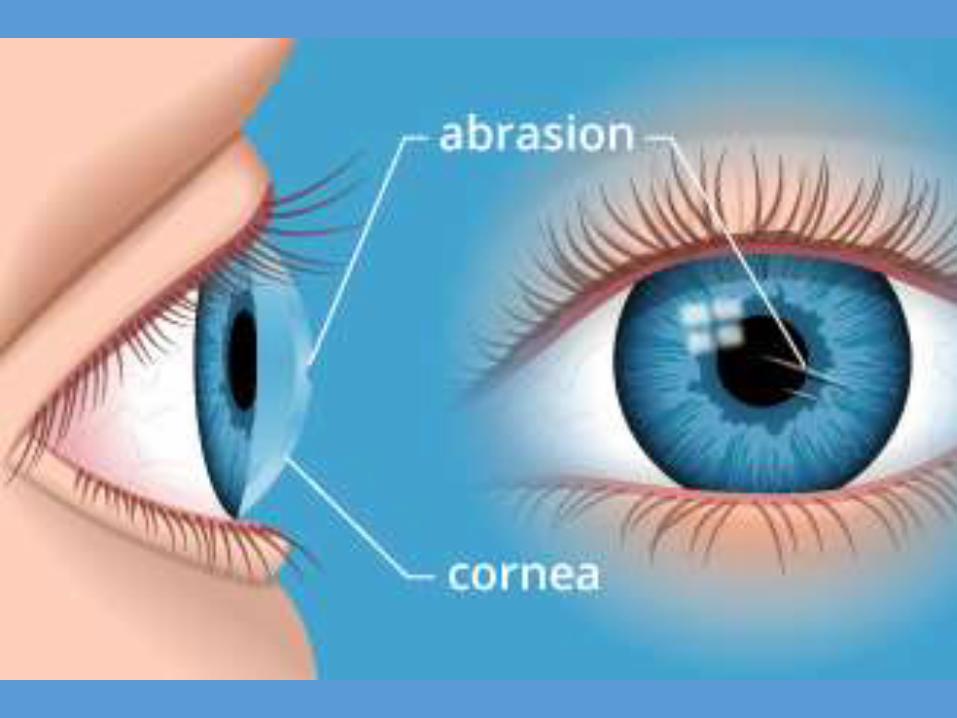
• Direct trauma
• Ischemic optic neuropathy
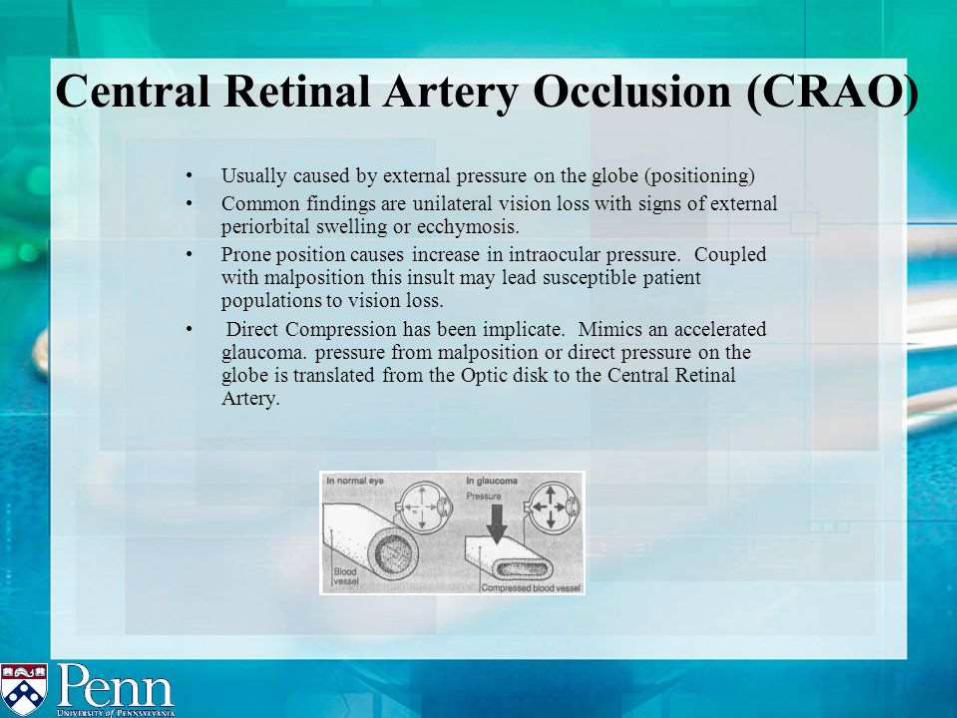
• Central retina artery occlusion
• 72% men, 84% >6 hours operative time, EBL>1 liter, mean operative time 9.8 hours *, median onset time 15 hours,
• IOP increases dramatically with trendelenberg position
*Lee LA, Roth S, Posner KL, Cheney FW, Caplan RA, Newman NJ, Domino KB. The American Society of Anesthesiologists Postoperative Visual Loss Registry: analysis of 93 spine surgery cases with postoperative visual loss. Anesthesiology. 2006;105:652–69; quiz 867-868.




thanks