PRACTICAL HEART SOUNDS Dr. Zahoor Ali Shaikh 1. PRACTICAL HEART SOUNDS Objectives 1. To understand…
Upload
mudassar-roomiCategory
view
217download
0
7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 1/15
Heart Sounds
• During each cardiac cycle, 4 heartsounds are produced.
• These can be recorded inphonocardiogram.
• By auscultation we can hear/
auscultate, 1st & 2nd heart sounds &sometimes 3rd as well.
• But 4th is Atrial heart sound, whichis never auscultated normally.
• 1st & 2nd heart sounds are called asCLASSICAL HEART SOUNDS (as theyare usually auscultated in normalsubjects).

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 2/15

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 3/15
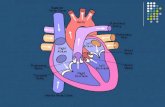
4 Auscultatory areas
• Pulmonary Area: Left 2nd intercostal space, close tosternal border.
• Aortic Area: Right 2nd intercostalspace, close to sternal border.
• Mitral Area: left 5th intercostalspace in the midclavicular line, 9cm away from the sternalborder.
•
Tricuspid Area: 4th
leftintercostal space close to sternalborder.

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 4/15
4 basic factors affecting Heart Sounds:
• Acceleration of blood: Sudden flow.
• Deceleration: Sudden stoppage of blood flow.
•
Turbulance in the flow of blood.• Thickness of chest wall.

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 5/15
1st Heart Sound
Characteristics:
• Long, soft, low pitched.
(heard as LUBB)
• Frequency: 30 –
50cycles /sec.
• Duration: 0.14 sec

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 6/15
1st Heart Sound
CAUSES:
• Vibrations due to closure of AV valves, at the beginningof ventricular systole.
• Vibrations in ventricles &large vessels whenventricular musclecontracts.
• Vibrations when bloodstarts ejecting into largeartery.

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 7/15
Physiological Splitting of 1st heart sound
Mechanism:
• Tricuspid valve may
close earlier than
mitral.

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 8/15
Intensity of 1st heart sound
Depends on:
• Force of ventricular
systole.
• Rate of increase in
ventricular pressure,
during isovolumiccontraction phase.

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 9/15
2nd Heart Sound
Characteristics:
• Short, sharp, high pitched
(heard as DUBB)
• Frequency: 50 – 200 cycles /
sec.
• Duration: 0.11 sec

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 10/15
2nd Heart Sound:
Minor causes:
• When blood flows from
ventricle to large
arteries, there may beturbulance.

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 11/15
Splitting of 2nd Heart Sound:
• PHYSIOLOGICAL
• Increases or Widens duringinspiration (0.5 sec) & decreasesduring expiration (0.02 sec ordisappear).
Cause of splitting:
• During inspiration venous returnincreasesmore blood returns toright atrium right ventricle more ejection delayed closure of pulmonary valve.
• Reverse occurs in expiration.
• PATHOLOGICAL
• In bundle branch block, mainly rightbundle branch block.
• Intensity of pulmonary component of
2nd heart sound is increased inpulmonary hypertension.
• Intensity of aortic component isincreased in systemic (aortic)hypertension

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 12/15
3rd Heart Sound:
Cause: Vibrations produced inventricular wall during Rapid InflowPhase.
Prominent sometimes in children.
Can be made prominent by increasing
venous return:i) exercise.
ii) lying position.
• Low frequency sound.
• Duration: 0.04 sec.
• Best heard at: Apex of heart, in 5th intercostal space (mid-clavicularline).

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 13/15
4th Heart Sound:
• Not normally auscultated butrecorded in phonocardiogram.
• Low frequency, low intensity sound.
• Produced just before 1st heart sound.
• Also called ATRIAL HEART SOUND.
Cause:
• Vibrations of ventricular wall, due toimpact of blood pumped from theatrium into ventricle during Atrial
Systole.
Diseases:
• In CCF, 4th Heart Sound is auscultated.

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 14/15
MURMURS:
• These are abnormal heartsounds.
Produced when:
1. Valvular stenosis.
2. Valvular incompetence.
3. Hyperdynamic circulation: Hyperthyroidism,
severe anemia (hemicmurmurs)

7/30/2019 Lecture on Heart Sounds by Dr. Roomi
http://slidepdf.com/reader/full/lecture-on-heart-sounds-by-dr-roomi 15/15
MURMURS
• Systolic murmurs:
– Aortic stenosis
– Mitral regurgitation
• Diastolic murmurs:
– Aortic regurgitation
– Mitral stenosis
• Murmur throughout
cardiac cycle:
– Patent ductus arteriosus
(PDA)- its murmur is also
called as machinary murmur.