Lecture 7: Policy Design: Health Insurance & Adverse...
25
Health Insurance Spending & Health Adverse Selection Lecture 7: Policy Design: Health Insurance & Adverse Selection Johannes Spinnewijn London School of Economics Lecture Notes for Ec426 1 / 25
Transcript of Lecture 7: Policy Design: Health Insurance & Adverse...

Health Insurance Spending & Health Adverse Selection
Lecture 7: Policy Design:Health Insurance & Adverse Selection
Johannes Spinnewijn
London School of Economics
Lecture Notes for Ec426
1 / 25

Health Insurance Spending & Health Adverse Selection
Outline
1 Health Insurance & Care
2 Rise in Spending & Impact on Health
3 Adverse selection: theory & empirics
2 / 25

Health Insurance Spending & Health Adverse Selection
Health Insurance
Different from other examples of social insurance
triangle relationship between customer, insurer and providerco-existence of private and public initiativerelation between health care and health outcomessome similar issues as with social security
Health is an important field because of enormous size andrapid growth
1950: 4% of GDP devoted to health care in US2003: 15% of GDP devoted to health care in US2075: 38% of GDP devoted to health care in US
Health economics is field in itself. We will focus on publicsector interventions
3 / 25

Health Insurance Spending & Health Adverse Selection
Health Care Spending in OECD Nations in 2002
Health Care Spending in OECD Nations in 2002
0
3
6
9
12
15
Slov
ak R
epub
licKo
rea
Mex
ico
Pola
ndLu
xem
bour
gTu
rkey
Finl
and
Irela
ndC
zech
Rep
ublic
Spai
nAu
stria
Uni
ted
Kin
gdom
Hun
gary
Japa
nIta
lyN
ew Z
eala
ndN
orw
ayD
enm
ark
Aust
ralia
Belg
ium
Net
herla
nds
Swed
enPo
rtuga
lG
reec
eC
anad
aFr
ance
Icel
and
Ger
man
ySw
itzer
land
Uni
ted
Sta
tes
Heal
th C
are
Spen
ding
(% o
f GDP
)
Source: Gruber (2007)
4 / 25

Health Insurance Spending & Health Adverse Selection
UK vs. US
UK: publicly funded health care system (NHS)
largest employer in UKinsures most types of careprivate health care for top-ups, only taken by 8%
Before ‘Obama-care’US tended to have less publicintervention than other developed countries
50% compared to 75% on average elsewheremedicare vs. medicaidinsurance provided by employers, large tax subsidy - financedwith payroll taxmany types of care uninsured, many people uninsured
5 / 25

Health Insurance Spending & Health Adverse Selection
Rise in Health Spending: Reasons?
General consensus: technological progress with moreexpensive methods (supply effect)
example: angioplasty: expensive but saves lifes (of somepatients...)
Newhouse (1992): residual argument (a la growth accounting)
only 1/4 to 1/2 of rise in spending can be explained by otherfacts
demand effects: aging, increased income, subsidized bygovernment, increased insuranceother supply effects: supplier induced demand(fee-for-service), malpractice
Limited direct evidence for impact of technological change
6 / 25

Health Insurance Spending & Health Adverse Selection
Health Spending vs. Health OutcomesIs increase in health spending a problem?
optimal health share is likely to grow with incomevoluntary choice to adopt (expensive) technological progressBUT prices are distorted due to insurance
Does health insurance / higher spending improve health?margin vs. average
evidence for "flat of the curve" health careextremely high average value of health improvements in thelast decennia
young vs. oldsubstantial impact of Medicaid (Currie & Gruber 1996)insignificant impact of Medicare (Card et al. 2008)
opportunity cost of each health policy (see RDD example)
How to measure health improvements? Are healthimprovements of ‘First Order’importance for insurancepolicies?
7 / 25

Health Insurance Spending & Health Adverse Selection
Opportunity Cost: An RDD Example
Source: Almond, Doyle, Kowalski and Williams (2009)8 / 25

Health Insurance Spending & Health Adverse Selection
Opportunity Cost: An RDD Example
Source: Almond, Doyle, Kowalski and Williams (2009)9 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Market Failures and Government Interventions1 Asymmetric Information:
heterogeneity of risk types → adverse selection in insurancemarketprice subsidies, insurance mandates,...
2 Externalities/Internalities/Consumer myopiatax subsidies for health insurance, government providedinsurancesin taxes (alcohol/cigarettes), fat tax,...
3 Other reasons for government provision or regulation;1 Suppliers exploiting asymmetric info about desirable care (e.g.,licensing of doctors, fixing physician salaries)
2 Incomplete market: ex-ante risk uninsured, since we cannotcontract before birth
3 Equity concerns: health inequality may directly enter socialwelfare function (e.g., in US, white infant mortality rate is6/1000; black is 14/1000)
10 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Adverse Selection as a Motivation for SIKey paper: Akerlof (1970), Rothschild and Stiglitz (1976)
environment with asymmetric information: individuals knowrisk of becoming sick but insurer does notmarket failure: underprovision of insurance (completeunravelling in extreme case)government intervention: through mandated insurance caninduce a Pareto improvement
Renewed interest: negative correlation puzzletheory predicts that high risk types buy more insurancecoverageempirically, the exact opposite is found in many insurancemarkets
Most recently: estimate welfare cost of asymmetricinformation
structural vs. reduced-form approachesstrong assumptions on importance of preferences
11 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Simple Demand and Supply of InsuranceBased on Einav, Finkelstein & Cullen (2010)
Consumers have the choice between contract H and L.Contract H provides more insurance coverage at additionalpremium p
Assume unobserved heterogeneity ζ determines both the valueand the cost of insurance.
Additive model:
v ≡ vH (ζ)− vL (ζ) ≡ π (ζ)︸ ︷︷ ︸‘risk’-term
+ r (ζ)︸︷︷︸‘preference’-term
π (ζ) equals the insurer’s cost of providing insurancer (ζ) captures the net-value of insurancefor CARA γ and normal risk x : π (ζ) = Ex , r (ζ) = γ
2 var (x)
12 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Heterogeneity in Risks: Adverse Selection
Buy contract H iff v (ζ) ≥ p,
Demand : D (p) = 1− Fv (p)
Cost of providing insurance depends on types buying insurance
Average Cost : AC (p) = E (π|v (ζ) ≥ p)Marginal Cost : MC (p) = E (π|v (ζ) = p)
More risky types tend to value insurance more such that thecost of providing insurance is increasing in p
13 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Adverse Selection
14 / 25
Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
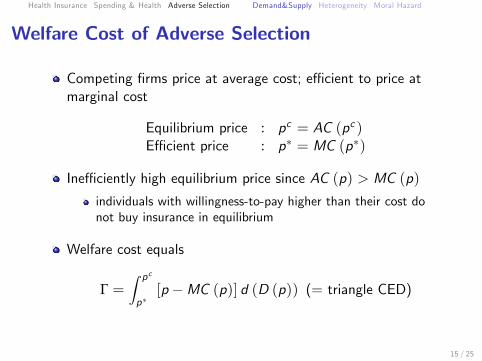
Welfare Cost of Adverse Selection
Competing firms price at average cost; effi cient to price atmarginal cost
Equilibrium price : pc = AC (pc )Effi cient price : p∗ = MC (p∗)
Ineffi ciently high equilibrium price since AC (p) > MC (p)
individuals with willingness-to-pay higher than their cost donot buy insurance in equilibrium
Welfare cost equals
Γ =∫ pc
p∗[p −MC (p)] d (D (p)) (= triangle CED)
15 / 25
Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
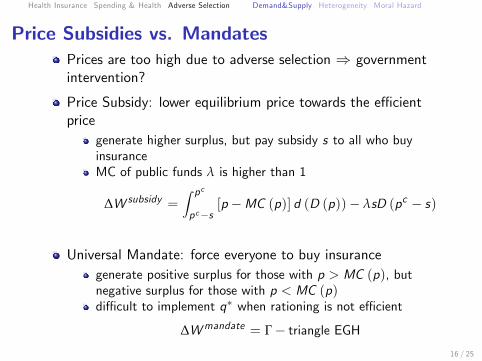
Price Subsidies vs. MandatesPrices are too high due to adverse selection ⇒ governmentintervention?
Price Subsidy: lower equilibrium price towards the effi cientprice
generate higher surplus, but pay subsidy s to all who buyinsuranceMC of public funds λ is higher than 1
∆W subsidy =∫ pcpc−s
[p −MC (p)] d (D (p))− λsD (pc − s)
Universal Mandate: force everyone to buy insurancegenerate positive surplus for those with p > MC (p), butnegative surplus for those with p < MC (p)diffi cult to implement q∗ when rationing is not effi cient
∆Wmandate = Γ− triangle EGH16 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Welfare Analysis using Suffi cient Statistics
Suffi cient to estimate demand curve and average cost curve
need information on available options, contract choices andthe medical claims for given pricesneed exogenous price variation as well
Approach allows to calculate welfare loss due to ineffi cientpricing and gain from policy interventions
Einav et al. (2010) analyze employer-provided healthinsurance
consider choice between high-deductible and low-deductiblecontractexploit variation in the premium across business unitsobserve how many buy and how much they claim
⇒ effi ciency cost is small (only 3% of total surplus), bothprice subsidy and mandate would decrease welfare!
17 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
18 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Adverse Selection: Pricing vs. ScreeningAkerlof (1970):
presence of high risk types prices lower risk types out of themarketextreme unravelling: no one buys contract (except highest risktype) - even when everyone prefers to buy at actuarially fairpricemeasure of ineffi ciency:
E (π|v (ζ) ≥ p)− E (π|v (ζ) = p)
Rothschild and Stiglitz (1976):
previous approach takes contracts as givenallow insurers to provide a menu of contracts specifying priceánd coveragescreen low risk types by providing less insurance at reducedpremium
19 / 25
Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Positive Correlation TestRobust prediction of Adverse Selection Model:
high risk types will buy more insurance ⇒ positive correlation,conditional on observables
Empirical evidence started with Chiappori and Salanié (2000),finding no significant correlation in car industry, conditional onobservables
other markets with insignificant correlation: life insurance(Cawley & Philipson 1999); health insurance (Cardon &Hendel 2001)
markets with negative correlation: long-term care insurance(Finkelstein & McGarry 2006), Medigap insurance (Fang,Keane and Silverman 2008)
Empirically, heterogeneity in risks do not play the role weexpected...
20 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Heterogeneity in PreferencesCurrent literature conjectures the importance ofheterogeneous preferences
Back to model (v = π + r) - assume normal heterogeneity
MC curve simplifies to
MC (p (q)) = µπ +cov (π, v)var (v)
[p (q)− µv ]
MC curve flattens if the variance in preferences increasesMC curve is upward sloping ifcov (π, v) (= var (π) + cov (π, r)) < 0
Suffi cient statistics approach: unnecessary to uncover theunderlying heterogeneity
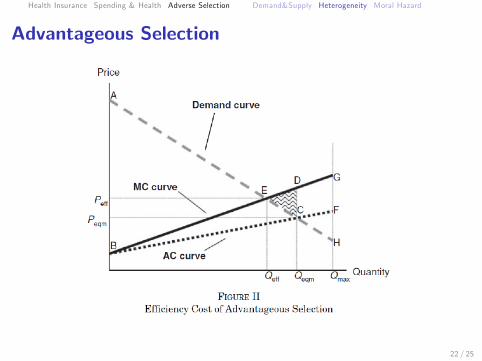
adverse selection if MC curve is decreasingadvantageous selection if MC curve is increasing
21 / 25
Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Advantageous Selection
22 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Heterogeneity in Preferences?
While current empirical approaches attribute residualheterogeneity in demand to heterogeneous preferences, directevidence is limited.
Recent work questions stability of preferences for givenindividual across domains.
Suggests importance of other drivers of the demand forinsurance (risk perceptions, inertia, cognitive ability,...),possibly unrelated to the actual value of insurance.
23 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
Adverse Selection vs. Moral HazardInsurance of medical care induces moral hazard
ex ante: less precautionary effortsex post: overconsumption of medical care
Moral hazard predicts the same positive correlation.insurers reduce insurance coverage to provide optimalincentives (either ex ante or ex post)very different from reducing insurance coverage to screen goodrisk types
How to distinguish from adverse selection?no precautionary efforts (life insurance/annuities)use experimental or quasi-experimental variationuse dynamic data
Moral hazard and heterogeneous preferences may explainnegative correlation-puzzle
people who are more risk-averse buy more insurance, but exertmore effort as well
24 / 25

Health Insurance Spending & Health Adverse Selection Demand&Supply Heterogeneity Moral Hazard
In Sum
Health insurance is a particular type of Social Insurance (careprovider, private vs. public, impact on health). Expenditureson health care are growing exponentially.
Private information about health risks may cause adverseselection; underprovision of insurance would justifygovernment interventions.
However, empirical evidence suggests minor role of people’srisk as a determinant of their insurance choice.
25 / 25