Lecture 2 upper respiratory tract
62
Disorders of the Upper Respiratory System Dr. Mohanad Dr. Mohanad QPT20303 QPT20303
-
Upload
mohanad-mohanad -
Category
Health & Medicine
-
view
28 -
download
2
Transcript of Lecture 2 upper respiratory tract

Disorders of the Upper Respiratory System
Dr. MohanadDr. Mohanad
QPT20303QPT20303

Objective• To learn the epidemiology and
various clinical presentation of URT• To identify the common etiological
agents causing these syndromes• To study the laboratory diagnosis of
these syndromes• To determine the antibiotic of choice
for treatment

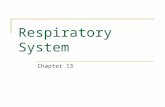
The Respiratory Tract and Its DefensesThe Respiratory Tract and Its Defenses Most common place for infectious agents to Most common place for infectious agents to
gain access to the bodygain access to the body Upper respiratory tract: mouth, nose, nasal Upper respiratory tract: mouth, nose, nasal
cavity, sinuses, pharynx, epiglottis, larynxcavity, sinuses, pharynx, epiglottis, larynx Lower respiratory tract: trachea, bronchi, Lower respiratory tract: trachea, bronchi,
bronchioles, lungs, alveolibronchioles, lungs, alveoli DefnesesDefneses
Nasal hairNasal hair CiliaCilia MucusMucus Involuntary responses such as coughing, sneezing, Involuntary responses such as coughing, sneezing,
and swallowingand swallowing MacrophagesMacrophages Secretory IgA against specific pathogensSecretory IgA against specific pathogens

Defenses of the Respiratory SystemDefenses of the Respiratory System

The classification of upper respiratory tract infections includes:
The common cold Pharyngitis Epiglotitis Acute laryngitis Acute laryngotracheobronchitis Sinusitis Otitis externa, otitis media and mastoiditis

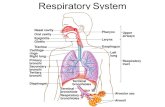
General symptoms of Respiratory Disease
Hypoxia : Decreased levels of oxygen in the tissues Hypoxemia : Decreased levels of oxygen in arterial blood Hypercapnia : Increased levels of CO2 in the blood
Hypocapnia : Decreased levels of CO2 in the blood
Dyspnea : Difficulty breathing Tachypnea : Rapid rate of breathing Cyanosis : Bluish discoloration of skin and mucous
membranes due to poor oxygenation of the blood Hemoptysis : Blood in the sputum

Respiratory infectionsInfections of the respiratory tract can occur in:1. The upper respiratory tract or 2. The lower respiratory tract, or3. Both. Organisms capable of infecting respiratory structures
include:1. Bacteria.2. Viruses: the majority of upper respiratory tract infections
are caused by viruses as rhinovirus and parainfluenza virus.
3. Fungi. Depending on the organism and extent of infection, the
manifestations can range from mild to severe and even life threatening.

FForms of Rhinitisorms of Rhinitis
Rhinoviruses,Rhinoviruses, Adenoviruses, Adenoviruses, RSVRSV Coxsackie's Viruses.Coxsackie's Viruses.
allergic rhinitis
(hay fever)
nonallergic rhinitis (common
cold) Pollen Dust mites Mold Animal
dander

Endothelialcell activation
Leukocyteinfiltration and
activation(lymphocytes, eosinophils,
basophils)
IMMEDIATE (early)RESPONSE
LATE-PHASERESPONSES
preformed &newly formed
mediators/cytokines
mast cell
SneezingPruritusRhinorrheaNasal obstructionOcular symptoms
Nasal obstructionRhinorrhea
Nasal hyperresponsivene
ss
To allergens(priming)
To irritants and to
atmospheric changes
IgEallergen
dendritic cell
T-lymphocyte
cytokineschemokines
allergen
B-lymphocyte
IgE
IL-4IL-13
The nasal allergic response
glands (mucous)

Clinical manifestationsClinical manifestations: : Fever, Fever, Rhinorrhea, Rhinorrhea, Sore throat, Sore throat, CoughCough Similar cases in the familySimilar cases in the family

Complications: Complications:
Acute otitis media,Acute otitis media,Pharyngitis,Pharyngitis,Sinusitis, Sinusitis, Conjunctivitis, Conjunctivitis, Pneumonia, Pneumonia, Adenitis.Adenitis.

Treatment (Symptomatic) :Treatment (Symptomatic) :Fever antipyretics
Nasal obstruction
decongestants
Rhinorrhea antihistamines
saline nasal drops/solution
ChlorpheniramineAcrivastine/ Claritin (loratadine)

House dust mite allergen avoidanceHouse dust mite allergen avoidance
Provide adequate ventilation to Provide adequate ventilation to decrease humiditydecrease humidity
Wash bedding regularly at 60°CWash bedding regularly at 60°C Encase pillow, mattress and quilt in Encase pillow, mattress and quilt in
allergen impermeable coversallergen impermeable covers Use vacuum cleaner with HEPA filterUse vacuum cleaner with HEPA filter Dispose of feather bedding Dispose of feather bedding Remove carpetsRemove carpets Remove curtains, pets and stuffed Remove curtains, pets and stuffed
toys from bedroomtoys from bedroom

Nonspecific Infections of The Upper Nonspecific Infections of The Upper Respiratory TractRespiratory Tract
They are identified by a variety of descriptive They are identified by a variety of descriptive names, including names, including acute infective rhinitisacute infective rhinitis, , acute acute rhinopharyngitis/nasopharyngitisrhinopharyngitis/nasopharyngitis, as well as by , as well as by the inclusive label the inclusive label Common ColdCommon Cold..

EtiologyEtiology
Influenza virus (3 immunotypes) Influenza virus (3 immunotypes) For instance, rhinoviruses (~30 to 40% of cases) consist of For instance, rhinoviruses (~30 to 40% of cases) consist of
at least 100 immunotypesat least 100 immunotypes Parainfluenza virus (4 immunotypes)Parainfluenza virus (4 immunotypes) Coronavirus (at least 3 immunotypes)Coronavirus (at least 3 immunotypes) Adenovirus (47 immunotypes)Adenovirus (47 immunotypes) Respiratory syncytial virus (RSV) Respiratory syncytial virus (RSV) Enteroviruses, rubella virus, and varicella-zoster virus)Enteroviruses, rubella virus, and varicella-zoster virus)

/ 42 16
CauseCause
• 80 % Influenzae virus• Parainfluenza %2-9• Rhinovirus %3• Adenovirus %4

These viruses tend to have seasonal variations in their peak incidence.
They gain entry to the body through the nasal mucosa and the surfaces of the eye. They are readily spread from person to person via respiratory secretions.
Manifestations of the common cold include: Rhinitis: Inflammation of the nasal mucosa Sinusitis :Inflammation of the sinus mucosa Pharyngitis : Inflammation of the pharynx and throat Headache Nasal discharge and congestion, coughcough Sore throat, sneezing, and hoarsenessSore throat, sneezing, and hoarseness Fever, malaise, fatigue , fever are more common Fever, malaise, fatigue , fever are more common
among infants and young.among infants and young.
The common cold

TREATMENTTREATMENT
Antibiotics to prevent bacterial infection (Antibiotics to prevent bacterial infection (amoxicillinamoxicillin)) Treatment remains entirely symptom-basedTreatment remains entirely symptom-based Decongestants: Decongestants: Phenylephrine and Antihistamines Phenylephrine and Antihistamines
((Claritin/ AcrivastineClaritin/ Acrivastine) )
Nonsteroidal anti-inflammatory drugs (Nonsteroidal anti-inflammatory drugs (ibuprofenibuprofen)) Dextromethorphan for cough Dextromethorphan for cough

Influenza is a viral infection that can affect the upper or lower respiratory tract.
The influenza virus is a highly transmissible respiratory pathogen.
Influenza A virusInfluenza A virus Family Family OrthomyxoviridaeOrthomyxoviridae Negative-stranded RNA genomeNegative-stranded RNA genome
Influenza B & C viruses Influenza B & C viruses only circulate in humansonly circulate in humans
Type A is the most common and causes the most serious illness.
Upper respiratory tract InfectionsInfluenza

InfluenzaInfluenza Because the organism has a high tendency for genetic
mutation, new variant of the virus are constantly arising in different places around the world.
Serious pandemics (spread of infection across a large region) of influenza are seen every 8 to 10 years as a result of this genetic mutation .


Influenza A Transmission CycleInfluenza A Transmission Cycle
Circulates withlimited pathology
Transmission todomestic fowl
Adaptation/reassortment
with swineinfluenza viruses
Transmissionto humans

PathogenesisPathogenesis Acquired through inhalation of infected Acquired through inhalation of infected
respiratory secretionsrespiratory secretions Virus attaches to host cells via hemagglutinin Virus attaches to host cells via hemagglutinin
spikesspikes Once attached viral envelope fuses with host membrane, Once attached viral envelope fuses with host membrane,
leading to viral replication within the cell leading to viral replication within the cell Mature viruses Mature viruses budbud from host cell from host cell
Budding allows mature virus to pick up envelopeBudding allows mature virus to pick up envelope
Infected cells Infected cells die and slough offdie and slough off Host immunity quickly controls viral spreadHost immunity quickly controls viral spread
Anti-HA neutralizing IgGAnti-HA neutralizing IgG is protective is protective
Mortality rate is lowMortality rate is low
Seasonal Influenza

Symptoms of influenza infection: Headache Fever, chills Muscle aches Nasal discharge Unproductive cough Sore throat
Influenza infection can cause marked inflammation of the respiratory epithelium leading to acute tissue damage and a loss of ciliated cells that protect the respiratory passages from other organisms As a result may lead to co-infection of the respiratory passages with bacteria.
It is also possible for the influenza virus to infect the tissues of the lung itself to cause a viral pneumonia.
Upper respiratory tract InfectionsInfluenza


TREATMENTTREATMENT
Antibiotics to avoid bacterial infectionAntibiotics to avoid bacterial infection Antiviral (Amantadine)Antiviral (Amantadine) Treatment remains entirely symptom-basedTreatment remains entirely symptom-based Decongestants (Decongestants (Phenylephrine)Phenylephrine) Nonsteroidal anti-inflammatory drugsNonsteroidal anti-inflammatory drugs Dextromethorphan for cough Dextromethorphan for cough Influenza vaccine: The influenza vaccine is
particularly indicated in elderly people, in individuals weakened by other disease and in health-care workers

vasoconstriction
Decongestants:
nasal airway lumen
nasalturbinates
nasal septum

Drugs for Treating Influenza: Amantadine
Used orally or by aerosol administration Effective only against type A influenza Inhibits viral fusion, assembly and release from the
infected host cell Neuraminidase inhibitors (Zanamavir, Oseltamivir)
New drugs that can be used by inhalation (Zanamavir) or orally (Oseltamivir)
Effective against both type A and B influenza Inhibits the activity of viral neuraminidase enzyme that is
necessary for spread of the influenza virus
Upper respiratory tract InfectionsInfluenza

PharyngitisPharyngitis Definition: Definition: Inflammatory syndrome of the Inflammatory syndrome of the
pharynx caused by several microorganismspharynx caused by several microorganisms
Causes: Causes: most viral but may also occur as part of most viral but may also occur as part of common cold or influenza syndromecommon cold or influenza syndrome
The most bacterial cause is Group A The most bacterial cause is Group A Streptococcus (Streptococcus pyogenes)-5-20%Streptococcus (Streptococcus pyogenes)-5-20%

Pharyngitis PresentationPharyngitis Presentation

Pharyngitis Clinical PresentationPharyngitis Clinical Presentation Clinical presentation with Clinical presentation with
soreness of the throat, soreness of the throat, may be dysphagia and may be dysphagia and pain on swallowingpain on swallowing
FeverFever additional upper additional upper
respiratory symptoms may respiratory symptoms may also be present, also be present, tender tender cervical lymphadenopathycervical lymphadenopathy

Figure 21.3

SinusitisSinusitis Acute Bacterial Acute Bacterial : Bacterial Infection of the paranasal sinuses : Bacterial Infection of the paranasal sinuses
lasting less than 30days in which symptoms resolve lasting less than 30days in which symptoms resolve completelycompletely
Subacaute Bacterial SinusitisSubacaute Bacterial Sinusitis: Lasting between 30 and 90 : Lasting between 30 and 90 days in which synptoms resolve completelydays in which synptoms resolve completely
Recurrent acute bacterial sinusitisRecurrent acute bacterial sinusitis: Each episode lasting : Each episode lasting less than 30 days and separated by intervals of at least less than 30 days and separated by intervals of at least 10days during which the patient is asymptomatic10days during which the patient is asymptomatic
Chronic SinusitisChronic Sinusitis: Episode lasting longer than 90 : Episode lasting longer than 90 days .Patients have persistent residual respiratory days .Patients have persistent residual respiratory stmptomssuch as cough, rhinnorrhoea or nasal obstruction.stmptomssuch as cough, rhinnorrhoea or nasal obstruction.

/ 42 34

Bacterial SinusitisBacterial Sinusitis Acute sinusitis
S.pneumoniaeH.infuenzaM.catarrhalis
Chronic sinusitis S.pneumoniae H.infuenza M.catarrhalis Oral anaerobes

Clinical Presentations of SinusitisClinical Presentations of Sinusitis

Bacterial sinusitisBacterial sinusitis Acute sinusitis Children Mainly clinical diagnosis Aspiration in case T
failure Dx X-rays CT/MRI Periorbital cellulitis R/O
sinusitis by CT/MRI Post-septal involvement
treat as meningitis
Chronic sinusitis Less local symptoms Mimic allergic rhinitis Dx Image less useful
than acute (changes persist after T and to R/O tumor
Obtain odontogenic X-rays if maxillary sinus

ManifestationsManifestations Nasal drainage and congestionNasal drainage and congestion Facial pain or pressureFacial pain or pressure Headache.Headache. Thick, purulent or discolored nasal dischargeThick, purulent or discolored nasal discharge Is often thought to indicate bacterial sinusitis, but Is often thought to indicate bacterial sinusitis, but
it also occurs early in viral infections such as the it also occurs early in viral infections such as the common coldcommon cold
Other nonspecific symptoms include cough, Other nonspecific symptoms include cough, sneezing, and feversneezing, and fever
Tooth pain, most often involving the upper molars, Tooth pain, most often involving the upper molars, is associated with bacterial sinusitisis associated with bacterial sinusitis

ManifestationsManifestations Sinus pain or pressure often localizes and be Sinus pain or pressure often localizes and be
worse when the patient bends over or is supine.worse when the patient bends over or is supine. Symptoms of advanced sphenoid or ethmoid Symptoms of advanced sphenoid or ethmoid
sinus: sinus: severe frontal or retroorbital pain severe frontal or retroorbital pain radiating radiating to the occiput, thrombosis of the cavernous to the occiput, thrombosis of the cavernous sinus, and signs of orbital cellulitissinus, and signs of orbital cellulitis
Advanced frontal sinusitis,Advanced frontal sinusitis, swelling and pitting swelling and pitting edema over the frontal bone ,subperiosteal edema over the frontal bone ,subperiosteal abscessabscess

Symptoms associated with Symptoms associated with RhinosinusitisRhinosinusitis
Major symptoms: Minor symptoms:
Facial pain/pressure HeadacheFacial congestion/fullness FeverNasal obstruction/blockage HalitosisNasal discharge/purulence/postnasal drip FatigueHyposmia/Anosmia Dental painFever Cough
Ear pain/fullness

SinusitisSinusitis Diagnosis is based on clinical criteria who Diagnosis is based on clinical criteria who
have upper RT symptoms that are have upper RT symptoms that are persistent or severepersistent or severe
Diagnosis: > or = 10,000 cfu/ml from the Diagnosis: > or = 10,000 cfu/ml from the cavity of paranasal sinus- but this is cavity of paranasal sinus- but this is invasiveinvasive

X-ray of SinusesX-ray of Sinuses

Nasal endoscopic view showing Aspergillus fungal mass arising from the sphenoid sinus

TreatmentTreatment Antibiotics are recommended for Acute Antibiotics are recommended for Acute
Bacterial Sinusitis to achieve a more rapid Bacterial Sinusitis to achieve a more rapid clinical cureclinical cure
AmoxicillinAmoxicillin at 45 or 90 mg/kg.day or at 45 or 90 mg/kg.day or Ceftriaxone Ceftriaxone
Most response in 48-72 hoursMost response in 48-72 hours Duration : until symptom free plus 7 daysDuration : until symptom free plus 7 days
Chronic treatment Same as acute sinusitis (Duration For 2-4 weeks)
If not resolving in 24 to 48 hours of Rx may need surgical intervention ( frontal sinus trephination or external sinusectomy)

Support TherapySupport Therapy DecongestantsDecongestants
Short duration 3-5 daysShort duration 3-5 days AntihistaminesAntihistamines
If allergyIf allergy Normal salineNormal saline Local steroidsLocal steroids

List of Complications from Acute Sinusitis
ƒ Mucocele or mucopyoceleƒ Osteomyelitisƒ Facial cellulitisƒ Oroantral fistulaƒ Orbital cellulitisƒ Cavernous sinus thrombosisƒ Septic thrombophlebitisƒ Meningitisƒ Epidural, subdural, or intracerebral
abscess

LARYNGITISLARYNGITIS
Inflammatory process involving the larynx Inflammatory process involving the larynx Are acuteAre acute By the same viruses responsible for many By the same viruses responsible for many
other URIother URI

EtiologyEtiology Rhinovirus, influenza virus, parainfluenza virus, Rhinovirus, influenza virus, parainfluenza virus,
adenovirus, coxsackievirus, coronavirus.adenovirus, coxsackievirus, coronavirus. Acute bacterial respiratory infections, such as Acute bacterial respiratory infections, such as
group A group A streptococcus streptococcus or or C. Diphtheriae , C. Diphtheriae , M. CatarrhalisM. Catarrhalis

Chronic laryngitisChronic laryngitis Mycobacterium tuberculosis Mycobacterium tuberculosis Histoplasma Histoplasma and and Blastomyces Blastomyces may cause may cause
laryngitislaryngitis Candida Candida species :thrush or esophagitis and species :thrush or esophagitis and
particularly in immunosuppressed patients to particularly in immunosuppressed patients to Coccidioides Coccidioides and and CryptococcusCryptococcus..
Acid Reflux (GERD)Acid Reflux (GERD) AllergiesAllergies AgingAging Voice stressVoice stress


ManifestationsManifestations Hoarseness Hoarseness Other symptoms and signs of URI, including Other symptoms and signs of URI, including
rhinorrhea, nasal congestion and cough rhinorrhea, nasal congestion and cough Sore throat, Dry throat Sore throat, Dry throat
Direct laryngoscopy Direct laryngoscopy : : Diffuse laryngeal erythema Diffuse laryngeal erythema and edema, along with vascular engorgement of the and edema, along with vascular engorgement of the vocal foldsvocal folds
Tuberculous laryngitis, mucosal nodules and Tuberculous laryngitis, mucosal nodules and ulcerations visible on laryngoscopyulcerations visible on laryngoscopy
These lesions are sometimes mistaken for laryngeal These lesions are sometimes mistaken for laryngeal cancercancer

TREATMENTTREATMENT
Humidification, Humidification, Increase fluidsIncrease fluids Voice restVoice rest Antibiotics are not recommended except when Antibiotics are not recommended except when
group A group A streptococcus streptococcus is culturedis cultured Chronic laryngitis usually requires biopsy with Chronic laryngitis usually requires biopsy with
culture.culture. Avoid smoking, recreational drugs, and alcoholAvoid smoking, recreational drugs, and alcohol

CROUPCROUP
Viral respiratory illnessesViral respiratory illnesses Characterized by marked swelling of the Characterized by marked swelling of the
subglottic region of the larynxsubglottic region of the larynx Croup primarily affects children <6 years oldCroup primarily affects children <6 years old
Signs and symptoms Barking cough or hoarseness.Worse at night and can last 5 to 6 days.Decrease breath sounds.DyspneaFever

Nursing interventions Nursing interventions Exposure of child to cool water. Exposure of child to cool water. Cool humidification during sleep with cool mist tent or Cool humidification during sleep with cool mist tent or
room humidifier.room humidifier. Encourage clear liquid intake to keep mucus thin.Encourage clear liquid intake to keep mucus thin. Monitor vital signs and pulse oximetry.Monitor vital signs and pulse oximetry. Administer medication (Antipyretic, antibiotics, Administer medication (Antipyretic, antibiotics,
corticosteroids.corticosteroids. Oxygen administration if necessary. Oxygen administration if necessary. IV fluid to prevent dehydration. IV fluid to prevent dehydration.

Strep ThroatStrep Throat Upper Respiratory Upper Respiratory
Infection: inflamed mucous Infection: inflamed mucous membranes of the throatmembranes of the throat
Caused by Group A Caused by Group A --hemolytic streptococci hemolytic streptococci ((Streptococcus pyogenesStreptococcus pyogenes))
Virulence factors: resistance Virulence factors: resistance to phagocytosisto phagocytosis Streptokinases: lyse fibrin Streptokinases: lyse fibrin
clotsclots Streptolysins: cytotoxic to Streptolysins: cytotoxic to
tissue cells, RBCs, and tissue cells, RBCs, and protective leukocytesprotective leukocytes

Strep ThroatStrep Throat Transmission:Transmission:
Person to person by direct contact with saliva or nasal discharge. Most people do not get group a strep infections from casual
contact with others, but a crowded environment like a dormitory, school, or an institutional setting can make it easier for the bacteria to spread.

A person becomes sick within 3 days after being exposed to the germ.
Once people become infected, they can pass the infection to others for up to 2 to 3 weeks even if they don't have symptoms.
After 24 hours of antibiotic treatment, a person will no longer spread the bacteria to others.

Strep ThroatStrep Throat Throat may be red with white patchesThroat may be red with white patches Trouble swallowing Trouble swallowing Have tender swollen glands (lymph nodes) on the sides of Have tender swollen glands (lymph nodes) on the sides of
your neck, toward the frontyour neck, toward the front Usually the tonsils are red and enlargedUsually the tonsils are red and enlarged May also have white craters or specks of pus on your May also have white craters or specks of pus on your
tonsils or your tonsils may be covered with a gray or white tonsils or your tonsils may be covered with a gray or white coating. Headache coating. Headache
Abdominal (lower stomach) pain Abdominal (lower stomach) pain Fever , Rash Fever , Rash General discomfort, uneasiness, or ill feeling General discomfort, uneasiness, or ill feeling Loss of appetite and nausea Loss of appetite and nausea Muscle pain ,Joint stiffness Muscle pain ,Joint stiffness

Strept Throat DxStrept Throat Dx Diagnosis:Diagnosis: Throat swabThroat swab Rapid testRapid test Indirect agglutination Indirect agglutination
diagnostic testsdiagnostic tests Use microscopic latex Use microscopic latex
particles coated with Abs particles coated with Abs against group A streptococci.against group A streptococci.
Negative tests are double Negative tests are double checked by culturing checked by culturing organismorganism

Strept Throat TxStrept Throat Tx
No treatment or incomplete treatment of strep throat also No treatment or incomplete treatment of strep throat also increases your risk of complications, such as rheumatic increases your risk of complications, such as rheumatic fever (which can cause permanent damage to your heart), fever (which can cause permanent damage to your heart), scarlet fever, blood infection, or kidney disease.scarlet fever, blood infection, or kidney disease.

Question?Question? Show in diagram the nasal allergic response. Identify the causes and treatment of Chronic
laryngitis.

62