Sanroz Lifescience, Ahmedabad, Pharmaceutical Formulations & Products

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this site.
1
Copyright 2006, The Johns Hopkins University and Alan Lyles. All rights reserved. Use of these materials permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for obtaining permissions for use from third parties as needed.

Session 1:Pharmaceutical Products and
Under-served Populations
Alan Lyles, Johns Hopkins School of Public Health
2

Overview of Course Sessions (1)
1. The global context of pharmaceutical products and underserved populations
2. International Policy and Legal framework3. Drug manufacture, industrial pharmacy considerations,
quality assurance and regulation4. The Drug Management Cycle: Selection5. Forecasting and Quantification6. The Drug Management Cycle: Procurement7. Drug Donations8. The Drug Management Cycle: Distribution
3

Overview of Course Sessions (2)
9. The Drug Management Cycle: Use10. Budgeting and Cost Control11. Management Support Systems: Planning Cycle12. Access to Essential Drugs13. Pharmaceutical Care and Drug Utilization in an
HIV/AIDS Clinic14. Financing and Sustainability15. Laboratory Exercise on Planning with an Emphasis on
Budgets and Sensitivity Analysis16. Student Presentations
4

“The right context is worth 50 IQ points.”-Alan Kay, Inventor of Object Oriented Programming &
Laptop Computer Visionary
5

World Drug Purchases: Retail PharmaciesIMS Health –Retail Drug Monitor: 12 Months to Sept 2005*
Sept 2005 Sept 2004 % Growth US$ % Growth Constant Exchange
Selected World 365,348 341,483 7% 5%
North America 192,649 182,200 6% 5%
• USA 180,994 172,182 5% 5%
• Canada 11,656 10,017 16% 7%
Europe 90,685 84,132 8% 3%
• Germany 27,055 24,281 11% 7%
• France 22,639 20,641 10% 5%
• Italy 14,619 14,249 3% (2%)
• UK 15,408 15,083 2% (1%)
• Spain 10,965 9,879 11% 6%
Source: IMS Health, Retail Drug Monitor Sept 2005 in US$ millions. www.imshealth.com/vgn/images/portal/cit_40000873/53/63/76322469IMS%20Retail%20Drug%20Monitor%20September2005.pdf
6

World Drug Purchases: Retail Pharmacies
IMS Health –Retail Drug Monitor: 12 Months to Sept 2005*
Sept 2005 Sept 2004 % Growth US$ % Growth Constant Exchange
Selected World 365,348 341,483 7% 5%
Japan* 60,820 57,122 6% 5%
Latin America†15,524 13,935 20% 19%
• Mexico 7,184 6,338 13% 11%
• Brazil 6,369 4,844 31% 31%
• Argentina 1,971 1,752 13% 13%
Australia/NZ 5,670 5,094 11% 5%
*Including hospitals; †Leading three.
Source: IMS Health, Retail Drug Monitor Sept 2005 in US$ millions. www.imshealth.com/vgn/images/portal/cit_40000873/53/63/76322469IMS%20Retail%20Drug%20Monitor%20September2005.pdf
7

Percent of All US Firms Offering Health Benefits:1996-2005
Adapted from Employer Health Benefits Survey 2005. Kaiser Family Foundation. http://www.kff.org/insurance/7315/sections/upload/7375.pdf.
8

OP Prescription Drugs as Percentage of US National Health Expenditures: 1993 v 2003
Adapted from: Smith C, et al. Health Spending Growth Slows in 2003. Health Affairs 2005;24(1):185-194. Exhibit 5.
9

Relative Contributions to Rising US Rx Expenditures: 1993-1997 vs 1997-2002
1993-1997 1997-2002
Price 19% 25%
Rx Type 34% 34%
Utilization 47% 42%
Adapted from: Kaiser Family Foundation. Trends and Indicators, 2004 Update, Exhibit 1.17.
10

Access Barriers: Drugs Are Costly
• Major out-of-pocket expense• Can represent as much as 20 percent of total national
health expenditures, 60 percent of total recurrent health expenditures
• Drug expenditures are often second only to personnel salaries and benefits
11

Many Health Interventions Depend on Pharmaceuticals: Prevention & ACSCs
• Expanded Program on Immunization• Integrated Management of Childhood Illness• Directly Observed Treatment, Short-course• Roll Back Malaria• HIV prevention (social marketing of condoms)• AIDS treatment and care
12

Coverage Distribution
13

US Non-compliance from Out-of-Pocket Costs*
Out-Of-Pocket Health Status
Due to cost:Base:
All Adults
Have Condition
for Rx
$0-$100
$101-$250
$251-500
>$500
Excellent to Very Good
Fair to Poor
Did not ask MD for an Rx 18% 23% 14% 37% 42% 42% 12% 33%
Did not fill an Rx 22% 30% 19% 50% 48% 44% 13% 41%
Used a lower dose to extend Rx
15% 21% 10% 35% 36% 41% 8% 29%
Used less than Rx’d 18% 25% 13% 45% 42% 46% 11% 37%
14
*Adapted from: Harris Interactive. Higher Out-of-Pocket Costs Cause Massive Non-Compliance in the Use of Prescription Drugs, and This Is Likely to Grow. Health Care News. 2002;2(22):2. http://www.harrisinteractive.com/

US Rx Compliance: Disease Specific Behaviors in the Past 12 Months
Multiple Sclerosis Hypertension Depression
Not filled 15% 17% 30%
Delayed filling 24% 26% 41%
Taken in lower doses than prescribed 23% 14% 25%
Taken less often than prescribed 30% 29% 43%
Discontinued sooner than prescribed 15% 15% 30%
Adapted from: http://www.bcg.com/publications/files/TheHiddenEpidemic_Rpt_HCDec03.pdf
15

US Rx Compliance Behaviors & Gender:How does female compliance affect household behaviors?
Women Men
Not filled 21% 15%
Delayed filling 30% 20%
Taken in lower doses than prescribed 15% 12%
Taken less often than prescribed 33% 26%
Discontinued sooner than prescribed 23% 18%
Adapted from: http://www.bcg.com/publications/files/TheHiddenEpidemic_Rpt_HCDec03.pdf
16

Drug coverage among Medicare beneficiaries with CHD/MI increases use
of lifesaving drugs*
• Medicare beneficiaries with coronary heart disease– Statins recommended to lower cholesterol– Statins are costly
• 27.4 % with coverage used statins• 4.1% without coverage used statins
17

What Is Known about Drug Management?
• Effective ambulatory Rx use can reduce morbidity and mortality
• Wise drug selection underlies all other improvements• Effective management saves money and improves
performance• Rational drug use requires more than drug information• Systematic assessment and monitoring are essential
18

Increased Efficiencies: Pooled Procurement
19Source: MSH: Management Sciences for Health. Used with permission.
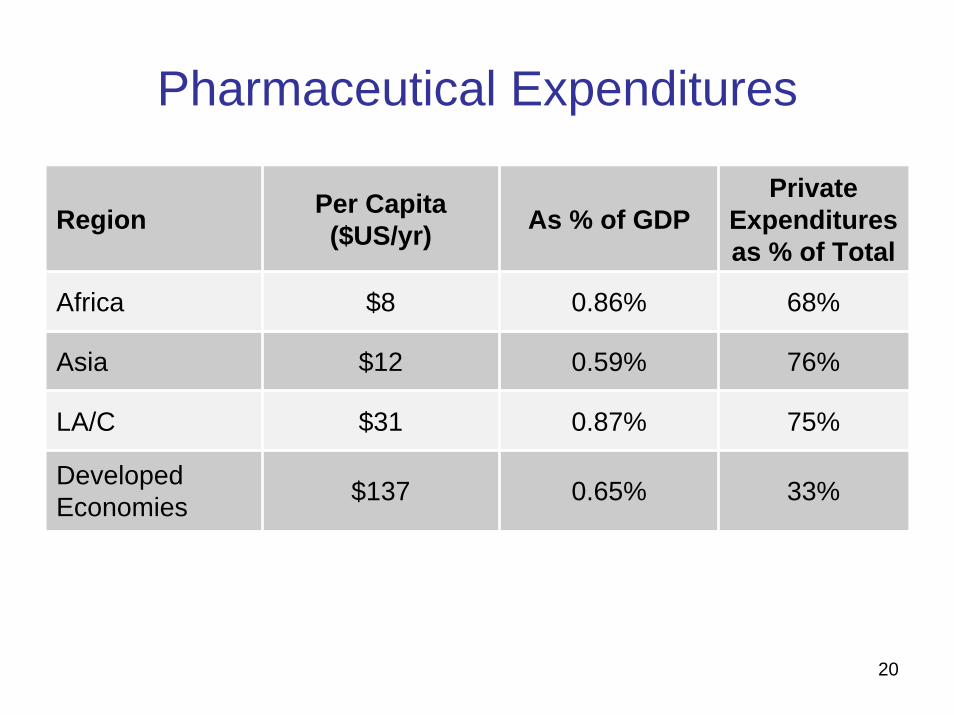
Pharmaceutical Expenditures
Region Per Capita ($US/yr) As % of GDP
Private Expenditures as % of Total
Africa $8 0.86% 68%
Asia $12 0.59% 76%
LA/C $31 0.87% 75%
Developed Economies $137 0.65% 33%
20

Understanding Medication Use
21Source: MSH: Management Sciences for Health. Used with permission.

Geographic Accessibility: Tanzania
PublicDistance to Health Facility
14% >10 km to public facility
6% >10 km to private drug retailer
Private Clinics
Private Pharmacy
Duka La Dawa
NGO
Source: MSH: Management Sciences for Health. Used with permission.
22

Affordability: Cambodia, El Salvador, Ghana, India
*Child 1-5 years old, co-trimoxazole; **Adult, amoxicillin
23Source: MSH: Management Sciences for Health. Used with permission.

Pharmaceutical Management, Access, and Use of Medicines
24Source: MSH: Management Sciences for Health. Used with permission.

Pharmaceutical Management Cycle
Policy and Legal Framework
25Source: MSH: Management Sciences for Health. Used with permission.

Dimensions of Access & Potential Barriers
26

Essential Medicines Definition
Essential medicines are:– those that satisfy the priority health care needs of the
population– selected with due regard to public health relevance,
evidence on efficacy and safety, and comparative cost-effectiveness
– intended to be available within the context of functioning health systems at all times in adequate amounts, in the appropriate dosage forms, with assured quality and adequate information, and at a cost that individuals and the community can afford
27

Substandard Essential Medicines in Developing Countries
28Source: MSH: Management Sciences for Health. Used with permission.

Percentage of Medicines Prescribed from Essential Medicines List, by Sector
29Source: MSH: Management Sciences for Health. Used with permission.

Understanding and Improving Access to Essential Medicines
30

Increased Efficiencies: STGs
Total Annual drug costs in a Latin American country for treatments during a cholera epidemic, costs in millions of US$ (1991)
31Source: MSH: Management Sciences for Health. Used with permission.

Challenges for Improved Public Drug Supply
• Health reform, equity, and financial sustainability• Efficiency• Rational use• Changing roles of public and private sectors
32

Essential Medicines Availability & Dispensing in Dispensaries
33Source: MSH: Management Sciences for Health. Used with permission.

Number of Medicines on National Essential Medicines Lists
34Source: MSH: Management Sciences for Health. Used with permission.

Goals of a National Drug PolicyHealth-Related• Available essential drugs• Improve attendance at health facilities• Safe, affordable, and effective drugs• Rational useProper selection of drugs• Efficient supply
Economic• Lower cost of drugs• Reduce foreign exchange• Provide jobs• Improve efficiency and cost-effectiveness
Development• Human resource development• Improve infrastructure• National production of drugs
35

Components of a National Drug Policy
• Legislative Framework• Choice of Drugs• Supply• Rational Use of Drugs• Economic Strategies for Drugs• Human Resources Development• Monitoring and Evaluation• Research• Technical Cooperation Among Countries
36