Learning Objectives - Northwest Chicago...
10
TEVAR: Thoracic Endovascular TEVAR: Thoracic Endovascular Aortic Repair Aortic Repair Postoperative Nursing Care Postoperative Nursing Care Leslie Collins APN-CNS, CCRN-CSC, CCNS CNS Cardiothoracic Surgery Northwest Community Hospital Learning Objectives Learning Objectives At the end of this session, the participant will be able to: OIdentify three conditions that are associated with thoracic aortic disease OList two indications for thoracic endovascular repair OName two nursing priorities during the postoperative period OList three interventions appropriate for the management of a lumbar drain OIdentify two possible complications post thoracic endovascular aortic repair Diseases of the Aorta Diseases of the Aorta – Vascular Vascular Emergencies Emergencies O Aortic aneurysm were primary cause of 10,597 deaths in 2009 and a contributing cause in 17,215 deaths O Delayed diagnosis secondary to symptoms mimicking other conditions O ACS O CVA O Anatomy of Aorta O Ascending O Arch O Descending O Abdominal “ Normal Normal” Aorta Aorta Size in CM Root 3.5-3.91 Ascending 2.86 Mid Descending 2.39-2.98 Diaphragmatic 2.40-2.69 Aortic Dissection Facts Aortic Dissection Facts O Results from intimal layer of the aorta that allows blood to flow into the medial layer - “false lumen” O Pressure changes in the aorta plays a significant role in the propagation or extension of dissection O Perfusion of major arteries can be reduced or eliminated with blood flow thru false lumen O Aortic dissection is defined as acute if it occurred within 2 weeks O About two-thirds of people with aortic dissection are male
Transcript of Learning Objectives - Northwest Chicago...
-
TEVAR: Thoracic Endovascular TEVAR: Thoracic Endovascular
Aortic RepairAortic Repair
Postoperative Nursing CarePostoperative Nursing Care
Leslie Collins APN-CNS, CCRN-CSC, CCNS
CNS Cardiothoracic Surgery
Northwest Community Hospital
Learning ObjectivesLearning Objectives
At the end of this session, the participant will be able to:
OIdentify three conditions that are associated with thoracic aortic disease
OList two indications for thoracic endovascular repair
OName two nursing priorities during the postoperative period
OList three interventions appropriate for the management of a lumbar drain
OIdentify two possible complications post thoracic endovascular aortic repair
Diseases of the Aorta Diseases of the Aorta Vascular Vascular
EmergenciesEmergencies
O Aortic aneurysm were primary cause of 10,597 deaths in 2009 and a contributing cause in 17,215 deaths
O Delayed diagnosis secondary to symptoms mimicking other conditions
O ACS
O CVA
O Anatomy of Aorta
O Ascending
O Arch
O Descending
O Abdominal
NormalNormal AortaAorta
Size in CM
Root 3.5-3.91
Ascending 2.86
Mid
Descending
2.39-2.98
Diaphragmatic 2.40-2.69
Aortic Dissection FactsAortic Dissection Facts
O Results from intimal layer of the aorta that allows blood to flow into the medial layer - false lumen
O Pressure changes in the aorta plays a significant role in the propagation or extension of dissection
O Perfusion of major arteries can be reduced or eliminated with blood flow thru false lumen
O Aortic dissection is defined as acute if it occurred within 2 weeks
O About two-thirds of people with aortic dissection are male
-
Aortic Dissection EtiologyAortic Dissection Etiology
O Iatrogenic
O Procedures with retrograde catheter insertion
O CPB and aortic cross clamping
O Trauma
O MVC or falls
O Diseases
O Hereditary connective tissue disorders: Marfans or Ehlers-Danlos syndrome affect the medial layer of the aorta
O HTN and atherosclerosis weaken medial layer
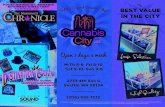
Classification Classification DeBakey SystemDeBakey System
O Type I: involve entire
aorta
O Type II: ascending
aorta
O Type III: descending
aorta distal to left SC
artery
-
Classification: Stanford SystemClassification: Stanford System
O Type A: Involves ascending or proximal aorta (DeBakey Types I and II)
O Significant risk for death
O Aortic regurgitation/pericardial tamponade
O Urgent surgical intervention required
O Type B: Descending aorta or distal aorta (DeBakey Type III)
O Medical management for BP control unless symptoms of ischemia are present
O TEVAR
Aortic Aortic
Dissection Dissection
ClassificationClassification
Complications Complications
of Aortic of Aortic
DissectionsDissections
Signs and SymptomsSigns and Symptoms
Location Impairment/Problem Symptoms
Ascending Aorta Damage to aortic valve
Impaired coronary blood flow
Cardiac Tamponade
Laryngeal Nerve Compression
Bleeding into pleural space
Diastolic murmur
Chest pain
Muffled heart tones, JVD, BP,
pulsus paradoxus
Hoarseness
Dyspnea, hemothorax
Aortic Arch blood flow to brain
Interruption of cervical
sympathetic ganglia
Impaired brachialcephalic flow
Syncope, altered MS
Ptosis, miosis, anhidrosis
BP differential, asymmetric
pulses in UE
Descending Aorta Spinal cord ischemia
Mesenteric artery ischemia
Limb paresthesia or paralysis
Acute abdominal pain, melena,
hyper BS
Thoraocabdominal aorta Renal artery ischemia
Lower limb ischemia
Flank pain, oliguria
Diminished or absent pulses in
LE
Indications for Aortic SurgeryIndications for Aortic SurgeryAscending Aorta/Arch Symptomatic or rapidly expanding aneurysm
Aneurysm > 5.5 cm
Aneurysm > 4-5 cm if AI or AS present
All acute Type A dissections
Descending thoracic Symptomatic or rapidly expanding aneurysm
Aneurysm > 6.5 cm
Complicated acute Type B dissections
Thoracoabdominal Symptomatic or rapidly expanding aneurysm
Aneurysm > 5.5-6.0 cm
Abdominal Symptomatic or rapidly expanding aneurysm
Aneurysm > 5.5 cm in low risk patients
Aneurysm > 4.5-5.0 cm in women
-
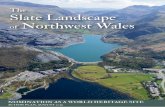
Aortic Endovascular GraftsAortic Endovascular Grafts
The Endovascular graft is
intended to exclude the
aneurysm/dissection by
placing the graft inside the
diseased aorta to make a
new path for blood flow
TEVAR: TEVAR: Thoracic Endovascular Aortic RepairThoracic Endovascular Aortic Repair
O Indications
O Descending Thoracic
Aneurysm
O Acute and Chronic Type B
Aortic Dissection
O Mortality for open repair is
high!!
O Goal for repair of dissection:
re-expand true lumen to
ensure flow to vital organs
and false lumen to resolve
Timing of RepairTiming of Repair
Type B DissectionType B DissectionO If repair 3-5 days after dissection
significant risk of re-dissection due to
friable tissue
O If repair > 9 days, then the true lumen may
not re-expand
O Best time frame 8-9 days. Decreased risk
of complications
Preop EvaluationPreop Evaluation
O CTA of chest, abdomen and pelvis with 3-dimensional formatting
O Provides accurate information regarding the external and endoluminal diameter of aorta at the proximal and distal seal zones landing zones
O Evaluate the length of aorta that needs to be repaired
O Identify branches off aorta that may be involved
O Evaluate external iliac artery morphology
O Evaluation for co-morbidities: Cardiac, renal and pulmonary
O CPB standby in case open conversion required
Hybrid ProceduresHybrid Procedures
O Combines standard
operative approaches and
endografts and/or conduit
creation/debranching
O Debranching: the
transposition of the origin
of critical branch vessels
to facilitate a seal zone.
Utilized when arch
arteries at risk for
occlusion with endograft
-
Postoperative Postoperative
Care of PatientsCare of Patients
Goal of Care
Ensure adequate tissue
perfusion to prevent
ischemia
ComplicationsComplications
O Endoleaks: Aneurysm sac remains pressurized
O Extremity Ischemia
O Renal Failure
O Bowel Ischemia
O Abdominal Compartment Syndrome
O Spinal Cord Ischemia
O Stroke
O Metabolic Acidosis
O Respiratory Complications
EndoleaksEndoleaks
O Defined as persistent
flow of blood into the
aneurysmal sac after
device placement
O Associated with a
continued risk for
aneurysm expansion
or rupture due to
persistent pressure
Classification Classification
of Endoleaksof Endoleaks
Type I EndoleakType I Endoleak
O Due to an incompetent seal at the proximal or
distal attachment sites
O Repaired as soon as they are discovered
O Spontaneous closure is uncommon
O Typically treated with addition of
endograft extensions
Type II EndoleakType II Endoleak
O Due to a patent inferior mesenteric or patent lumbar artery branches that allow retrograde flow into the aneurysm sac abdominal aortic repair
O Spontaneous resolution occurs in many cases.
O Require careful follow up imaging
O An increase of 5-10mm or
persistent endoleak (> 6 months)
are indications for repair
-
Type III EndoleakType III Endoleak
O Due to a junctional leak or disconnect on the
endograft components, holes in fabric
O Results in pressurized aneurysm sac with
increase risk of rupture
O Treated with deploying additional
stent graft components to seal
defect
Type IV EndoleakType IV Endoleak
O Associated with graft porosity and is self
limited
O Usually resolve in 24 hours
O Can obscure type I and type III leaks
Type V EndoleakType V Endoleak
O Referred to as endotension
O Endotension is defined as continued expansion of the
aneurysm sac greater than 5mm, without evidence of a
leak site.
O It is a poorly understood phenomenon
but thought to be formation of a
transudate due to ultrafiltration of
blood by the graft membrane or
unidentified leak.
TEVAR: Spinal Cord IschemiaTEVAR: Spinal Cord Ischemia
O Paralysis occurs in about
3-6% of all repairs of the
descending aorta due to
interference of the blood
supply to the spinal cord
O May occur immediately
postop from 1-21 days.
Prevention Prevention
and and
Management Management
of Spinal Cord of Spinal Cord
IschemiaIschemia
-
Spinal Cord IschemiaSpinal Cord Ischemia
O Leads to cord edema and can cause the lumbar ICP to rise and impede normal flow of CSF within the spinal canal and blood flow to the spinal cord
O Mechanism of Injury: The interruption of multiple branch vessels that provide spinal cord perfusion.
O Increase risk
O Complicated Type B Dissections
O Hybrid Aortic Procedures
O Aortic Transection
O Chronic Renal Failure
O Smoking
O Prevent hypotension. Keep MAP > 70-90 mmHg
Spinal Cord IschemiaSpinal Cord Ischemia
O Spinal cord is like the
brain:
O No room for
anything but the
cord, CSF and blood
O Unyielding to
increased spinal
pressures
Lumbar DrainLumbar Drain
O Goal: Patient will remain neurologically intact with no evidence of spinal cord ischemia
O Utilized to minimize risk of spinal cord ischemia by promoting spinal cord blood flow by controlling cerebrospinal fluid pressure
O SCPP: Spinal Cord Perfusion Pressure (>70 mm Hg)
O CSFP: Cerebrospinal Fluid Pressure
SCPP = MAP - CSFP
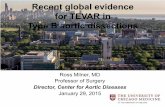
Medtronic Medtronic
Duet External Duet External
Drainage and Drainage and
Monitoring Monitoring
SystemSystem
Nursing Care of Patient with Nursing Care of Patient with
Lumbar DrainLumbar DrainO Assessment
O Neurologic status
O Obtain baseline assessment
O Subsequent assessments focus on signs of spinal
cord ischemia and/or meningeal irritation
O Signs of infection
O CSF drainage: Amount, color, clarity
O Integrity, function and position of EVD
O Catheter site q 4 hours
Nursing Care of Patient with Nursing Care of Patient with
Lumbar DrainLumbar DrainO External Ventricular Drain Care
O Maintain aseptic technique
O Zero pressure transducer to atmospheric pressure when patient arrives to ICU
O Level drainage system to phlebostatic axis
O Set drip chamber to desired pressure level (typically set at 0)
O Ensure stopcock on transducer is off to drip chamber allows for continuous CSFP monitoring
-
Nursing Care of Patient with Nursing Care of Patient with
Lumbar DrainLumbar DrainO Activity
O Maintain bedrest to prevent dislodgement of
catheter
O HOB may be elevated for patient comfort
O Re-level transducer with each position change
O Ensure that system is clamped during any
position change
Nursing Care of Patient with Nursing Care of Patient with
Lumbar DrainLumbar DrainO Safety Concerns
O Do NOT flush catheter
O Maintain bed in locked position so patient/family cannot adjust HOB
O Ensure drip chamber is set at level ordered by MD
O Ensure that stopcocks are set so that patient is NOT continuously draining
O Re-level transducer with each position change
O Reposition patient ONLY when catheter is clamped
O No anticoagulants when drain in place. SCDs for DVT prophylaxis
Management of CSFPManagement of CSFP
O Therapy is directed at maintaining a
cerebrospinal fluid pressure (CSFP) between
10-15 mmHg and a MAP between 70 - 90
O If CSFP is > 15 mmHg, may result in decreased
blood flow and perfusion to the spinal cord
Management of CSFPManagement of CSFP
O Therapeutic measures
O Increased CSFP drain CSF. No more than 10ml/hr. Call MD if CSFP remains elevated after drainage
O Increased MAP vasodilator
O Decreased MAP fluids and/or vasopressors
Monitor for signs of spinal cord ischemia and notify surgeon if patient develops changes in motor/sensory function!!
Treatment of Spinal Cord Treatment of Spinal Cord
IschemiaIschemiaO Goal MAP 90-99 mmHg
O Fluid
O Vasopressors
O Drain CSF to obtain CSFP < 10 mmHg
O Frequent neuro assessments to monitor for
resolution of symptoms
Complications of CSF DrainageComplications of CSF Drainage
O Infection
O Overdrainage
O Subdural hematoma
O Herniation
O Spinal Cord Hematoma
O Headache
O Pneumocranium from air entering system
PREVENTION IS KEY!!PREVENTION IS KEY!!
-
Lumbar Drain RemovalLumbar Drain Removal
O Removal of Drain by anesthesia
O Typically 48-72 hours after procedure
O Clamped for 24 hours prior to removal
O Monitor for S&S of spinal cord ischemia
O Sterile, occlusive dressing applied to site
O Patient to lay flat for 4 hours after removal
O Monitor patient for signs of headache
O Notify anesthesia if patient develops HA or
drainage from drain site
ComplicationsComplications
O Extremity Ischemia
O Due to thrombosis of graft or groin hematoma at insertion site
O Renal Failure
O Due to occlusion of renal arteries by graft (abdominal)
O Due to contrast induced nephropathy
O Bowel Ischemia
O Mesenteric artery occlusion/hypoperfusion (abdominal)
O Paralytic ileus
ComplicationsComplications
O Abdominal Compartment Syndrome
O Secondary to bowel ischemia
O Stroke
O 4-7% risk secondary to diseased aorta
O Metabolic Acidosis
O Hypoperfusion somewhere
O Respiratory Complications
O Prolonged bedrest with lumbar drain
Discharge and FollowDischarge and Follow--upup
O Typically discharged 1-2 days after drain
removal
O Ambulating
O Pain controlled
O CT scan at 1, 2, 6 and 12 months and then
annually to assess for aortic growth
Discharge InstructionsDischarge Instructions
O Activity
O No heavy lifting or strenuous activity for 2 weeks after surgery
O Increase in intra-thoracic pressure resulting in dramatic increase in systemic arterial pressure (300 mmHg)
O No driving for minimum of 1 week
O Diet: Resume preop diet
O Medications: Beta-blocker!!
O Shower: May shower on POD#3. No tub baths until cleared by surgeon
ReferencesReferences
O Fedorow, C. A., Moon, M.C., Mutch, A. C., Grocott, H. P., LumbarCerebrospinal Fluid Drainage for Thoracoabdominal Aortic surgery: Rationale and Practical Considerations for Management. Anesthesia & Analgesia, 2010, 111(1), 46-57.
O Littlejohns, L. Bader, M. (Ed.) AACN-AANN Protocols for Practice: Monitoring Technologies for Critically Ill Neuroscience Patients (2009). Jones & Bartlett Publishers; Sudbury, MA.
O Mehta, M., Hnath, J.C., Sternbach, Y., Taggert, J.B., Kreienberg, P.B., Spirig, A., Roddy, S.P., Paty, P.S.K., Ozsvath, K., Chang, B., Darling III, R.C., and Shah, D. Cerebrospinal Fluid Drainage During TEVAR. Endovascular Today, 2008, 44-46.
O Svensson, L.G., Kouchoukos, N. T., Miller C., et al. Expert Consensus Document on the Treatment of Descending Thoracic Aortic Disease Using Endovascular Stent-Grafts. Ann Thorac Surg 2008: 85:S1-41.
O Thompson, H. J. (ed). AANN Clinical Practice Guidelines Series: Care of the Patient Undergoing Intracranial Pressure Monitoring/External Ventricular Drainage or Lumbar Drainage. (2011). From www.aann.org.
-
Questions???Questions???