
Learning Evidence-Based Practice and Quality ... - chw.org/media/Files/For Patients And...
19
10/8/2014 1 Learning Evidence-Based Practice and Quality Improvement Following a Team of Child Life Specialists in their Journey to Create a More Comfortable Injection Experience Evidence-Based Practice Learning Objectives • Gain experience with the Evidence-Based Practice (EBP) process • Recognize how recommendations, when implemented systematically, can change hospital practice • Feel empowered to begin EBP by developing a clinical question and search terms • Develop an enhanced understanding on best practices surrounding injections by following a child life EBP project Evidence-Based Practice History of Evidence-Based Practice • Dr. Archie Cochrane, a British epidemiologist challenged the public to pay only for care that had be empirically supported with evidence. In 1972 he published a foundational book that criticized the medical profession for not providing rigorous reviews of evidence. • Founded the Cochrane Collaboration to assist individuals in making well-informed decisions about healthcare by developing a public systematic reviews of healthcare interventions. • This work began in medicine, but spread to all areas of healthcare including: Occupational and Physical Therapy, Nursing Care, Respiratory Therapy, and Speech Therapy.
Transcript of Learning Evidence-Based Practice and Quality ... - chw.org/media/Files/For Patients And...

10/8/2014
1
Learning Evidence-Based Practice and
Quality Improvement
Following a Team of Child Life Specialists in
their Journey to Create a More Comfortable
Injection Experience
Evidence-Based Practice
Learning Objectives
• Gain experience with the Evidence-Based Practice
(EBP) process
• Recognize how recommendations, when
implemented systematically, can change hospital
practice
• Feel empowered to begin EBP by developing a
clinical question and search terms
• Develop an enhanced understanding on best
practices surrounding injections by following a child
life EBP project
Evidence-Based Practice
History of Evidence-Based Practice
• Dr. Archie Cochrane, a British epidemiologist challenged the
public to pay only for care that had be empirically supported with
evidence. In 1972 he published a foundational book that
criticized the medical profession for not providing rigorous
reviews of evidence.
• Founded the Cochrane Collaboration to assist individuals in
making well-informed decisions about healthcare by developing
a public systematic reviews of healthcare interventions.
• This work began in medicine, but spread to all areas of
healthcare including: Occupational and Physical Therapy,
Nursing Care, Respiratory Therapy, and Speech Therapy.
10/8/2014
2
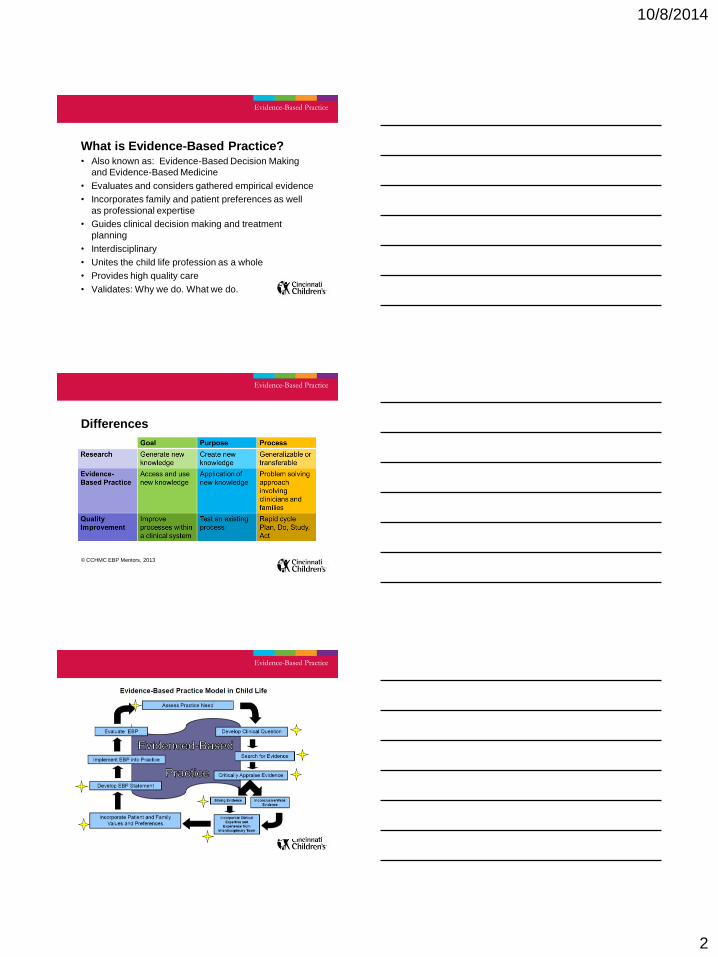
What is Evidence-Based Practice? • Also known as: Evidence-Based Decision Making
and Evidence-Based Medicine
• Evaluates and considers gathered empirical evidence
• Incorporates family and patient preferences as well
as professional expertise
• Guides clinical decision making and treatment
planning
• Interdisciplinary
• Unites the child life profession as a whole
• Provides high quality care
• Validates: Why we do. What we do.
Evidence-Based Practice
Differences
© CCHMC EBP Mentors, 2013
Evidence-Based Practice
Evidence-Based Practice

10/8/2014
3
1. Assess Practice Need
• Identify need for change or clarification of
best clinical practice
• Consider the priority level of addressing this
need
Resource: Cochrane Handbook
Child Life Council
Evidence-Based Practice
Develop Clinical Question
Use PICOT format
• Population of interest
• Intervention or issue of interest
• Comparison intervention or issue of interest
• Outcome of interest
• Time involved to demonstrate outcome
Resource: Evidence‐Based Practice in Nursing and Healthcare: A Guide to Best
Practice by Bernadette Mazurek Melnyk and Ellen Fineout‐Oveholt, Chapter 2.
Child Life Council
Evidence-Based Practice
Questions in Practice
Evidence-Based Practice
Should I provide
medical play for
medical procedure
preparation in a
child with an abuse
history?
Does teaching a child
coping skills help
them with general
anesthesia?
Is using praise
more effective
than using a
reward
system?
Do numbing
agents help
with
injections?
Does offering support during
procedures decrease a child’s
anxiety?
In what ways
should I process
grief with
siblings?

10/8/2014
4
Your Turn: What clinical questions are
you wondering about?
• What is a problem that you consistently
encounter?
• What is an area of interest?
• A clinical problem that you encounter in your
practice could be related to patients,
therapeutic approaches or interventions,
personnel, collaboration, technology, physical
materials, etc.?
Define a Clinical Question
P
I
C
O
T
Evidence-Based Practice
What clinical issue are
you passionate about?
What questions do you
have?
Search for Evidence
• Use PICO question to determine search
criteria or search terms
• Include all appropriate databases
• Cochrane Database of Systematic
Reviews, CINAHL, MEDLINE,
PsychINFO, National Guideline
Clearinghouse, Children’s Hospital
Association
• Eliminate articles that do not address the
clinical question
Resource: Cochrane Handbook
Child Life Council
Evidence-Based Practice
Search Terms:

10/8/2014
5
Critically Appraise the Evidence
• Determine whether each study
is valid and reliable
• Use the LEGEND (Let
Evidence Guide Every New
Decision) system to evaluate
the quality level for each article
Resource: LEGEND (Let Evidence Guide Every New
Decision): Tools for Evaluating the Evidence, available
at:
http://www.cincinnatichildrens.org/research/project/cpe‐rebp/resources.htm
Child Life Council
Evidence-Based Practice
Valid: Were the results of the study
obtained using sound scientific
methods? Does the test measure
what the test says it is really
measuring?
Reliable: Can you reproduce it?
Does the test consistently produce
the same results when administered
to the same individuals under the
same conditions?
Cookie Analogy
Warm chocolate chip cookies
from the oven
Oreos
Cookies from your favorite
bakery
Systematic Reviews, Meta-
analysis
Randomized Control Trials
Chips Ahoy chocolate chip
cookies
Frosted animal cookies
Qualitative, Case Control, Longitudinal,
Cross Sectional, Descriptive Studies,
Case Series
Published expert opinion,
Guidelines, General
consensus
Controlled Clinical Trials,
Cohort- Prospective
Evidence-Based Practice
Levels of Evidence Evidence-Based Practice

10/8/2014
6
Incorporate Clinical Expertise and
Experience
• Use clinical expertise to make
recommendations when
evidence is inconclusive
• An interdisciplinary group of
experts may be formed to help
evaluate and make
recommendations
• Resource: Child Life Council
Evidence-Based Practice
Incorporate Patient and Family Values
and Preferences • Are my patient’s and family’s values and preferences
satisfied by the treatment and its consequences?
• Is the treatment feasible in my care setting?
• Do the patient outcomes apply to my population or
question of interest?
• Are the likely benefits worth the potential harm and
costs?
• Were the patients in this study similar to my
population of interest?
Develop EBP Statement
• Summarize the evidence
incorporating clinical expertise
and patient/family values and
preferences
• Include possible implications
for practice and future
research needs
Resource: Child Life Council
Evidence-Based Practice

10/8/2014
7
EBP Journey for Injections
• Request for “helping your child with injections”
came from the hospital wide pain team task
force and child life staff in July 2011.
• Completed the evidence-based decision
making process and created a PICO question:
– In pediatric patients receiving injections, do
pharmacological interventions (including topical
anesthetic agents), psychological, and physical
interventions versus no intervention reduce pain
during injections?
BESt: “Reducing Pain for Children and
Adolescents Receiving Injections”
• Completed in January 2013
• Recommendations:
1. It is strongly recommended that age-appropriate interventions
with strong evidence, be used to reduce pain during
injections* See cells marked “Strongly” in following table.
2. It is recommended that, when strongly recommended
interventions are not sufficient or feasible to reduce pain
during injections, additional age-appropriate consensus-based
interventions are used. See cells marked “Local Consensus”
in the following table.
Note: Combining an intervention with distraction is more effective
than a single intervention.

10/8/2014
8
Successes
• Strong support from EBP mentor program within the hospital
• Literature produced evidence which answered our PICO question
and strongly supports our practice as CCLSs
• Positive feedback from hospital BESt review committee
• “This statement has the potential to impact patients and
families at all points of care within the institution”
• Core group of CCLSs committed to completing EBP statement
• Team with mixed levels of experience in EBP
• Less experienced staff received support and guidance
from those more experienced
• BEST of the BESt award 2013
Challenges
• Lack of resources, time, and staffing
– Completing article appraisals
– Developing recommendation
– Disseminating recommendation
– Implementing practice change while maintaining
one’s patient-care load
• Limited number of child life staff
– Staff interested in learning more about EBP
– Staff with a passion for completing EBP work
• Scheduling conflicts with EBP team

10/8/2014
9
Following up with a Quality
Improvement (QI) Project
Implement EBP into Practice
• When there is little
evidence
• Research project
• Where there is
evidence to make a
practice change
• Quality improvement
project
• Education plan
Evidence-Based Practice
Resource: Child Life Council
Disseminate Recommendation
March 2013: Educational Materials
• Helping you Child Cope with Getting an Injection (Tips for Newborns and Children up to 5 years)
• Helping your Child Cope with an Injection
(Tips for School-age Children)
• Coping with an Injection
(Tips for Teens)

10/8/2014
10
October 2013: Educational slides for
Televisions in waiting area
• Created three slides based on developmental
level
• Currently being shown in cafeteria and 3rd floor
waiting areas within the 3430 building
What is Quality Improvement (QI)?
With the customer* as top priority:
• Improving what we’re already doing, by altering
how we do it
• Producing a measurable & positive difference by
changing outcomes
• That has a lasting impact
Why do QI or make changes?
• To meet or exceed customer expectations.
*Customer: staff, patients, families, those impacted by practice change
© CCHMC EBP Mentors, 2014
Evidence-Based Practice

10/8/2014
11
Steps of Quality Improvement
Identify Problem
Document Current Process
Develop SMART AIM & Measures
Identify Key Drivers
Identify Potential Interventions
Identify & Analyze Process Failures
Design & Execute PDSAs
Run Charts
Scale-up Successful Interventions
Plan for Sustainability & Spread
Identify Root Causes
Develop SMART Aim
• An Aim statement describes what a team’s
focus is for their improvement work
• It indicates their goal as well as the baseline
to clearly define what the team is trying to
achieve
• Lastly, it gives a time frame for the work
• S - Specific
• M - Measurable
• A – Actionable
• R – Relevant
• T – Time bound
Develop SMART AIM & Measures
Key Driver Diagram
• Connects the aim/outcomes, key drivers, and
interventions
• Provides a roadmap for project
• Helps to focus the interventions accurately,
aligning the interventions to address root
causes and failures ultimately helping you
to achieve your SMART aim
Identify Key Drivers

10/8/2014
12
KEY DRIVER DIAGRAM
Project Name: Project Leader:
SMART AIM
KEY DRIVERS INTERVENTIONS (LOR)
Key
Dotted box = Placeholder for future additions
Green shaded = what we’re working on right now
Revision Date: __-__-__
GLOBAL AIM
2003 - 2009 © Cincinnati Children's Hospital MedicalCenter. All rights reserved.
Identify Potential Interventions
• HOW to address the failures
• HOW to accomplish the Key Drivers, which
ultimately help you achieve your goal
• Example:
– Failure identified = staff lack of knowledge with
positioning
– Potential Interventions:
• Provide education for staff on positioning
• Visual resources and signage re: positioning
– Staff resources and visual reminders in procedure rooms
– Materials for parents/caregivers in exam rooms, waiting rooms
Identify Potential Interventions
Design and Execute PDSAs
Plan
• What is the objective of the
test?
• What is needed to complete
test?
• How will you measure
outcome?
• Make a plan of action
Do
• Carry out your plan
• What were the results?
Design & Execute PDSAs

10/8/2014
13
PDSAs Study
• Was your prediction correct?
• What should be done for the next
test?
• What did you learn from the first
test?
ACT
• Adapt – make revisions to the
change
• Adopt – keep the change and try
on a larger scale
• Abandon
PDSA #1 • Global Aim: Reduce pain, distress, anxiety in infants, children,
and adolescents receiving injections.
• Smart Aim: Increase percentage of infants, children, and adolescents who receive the flu vaccine by December 31, 2014.
• Clear plastic brochure containers with educational materials were placed in all check-in areas and registration waiting areas.
• Created data collection form which prompted registration personnel to ask families, “Have you received the coping with injections brochure today?”
• Results: Families were more educated about strategies to help their child with vaccinations. 88% of high risk patients who came to Cardiac Clinic received a flu vaccine.
• Conclusions: Incorporate staff earlier in the quality improvement process. Identify key stakeholders from each discipline to provide knowledge and functioning of their area.
Oct. 2013: Cardiac Clinic
PDSA #1 Reflection
• Adapt, Adopt, or Abandon?
• Adapt what we learned from #1
– Involve staff as early as possible in the QI process
– Identify and team with key stakeholders as early
as possible

10/8/2014
14
April 2014: PPC proposal
• Partnering with the staff in PPC to reduce pain
during injections.
• Held an open forum
• Presentation to “Research Group”
• Areas of focus
– Patient and Family Education
– Staff Education
– Pain Relief Methods
• Standard Order Set
• Sucrose Solution for Infants
Implementation: SMART Aim 1
SMART Aim 2

10/8/2014
15
Patient and Family Education
• Use previously created educational pamphlets
for families.
• Provide educational slides on TVs in waiting
area.
• Child Life Specialist will provide informal
education to families and role model
approaches.
Staff Education
• Cross train with MAs from DDBP clinic.
• Provide hands on education and modeling by CLS one nurse, medical assistant/ one pod at a time.
• Provide an on-line education session
– Education focused on developmental appropriate strategies to decrease distress associated with injections
– This will include videos with these techniques being used with patients.
– Interacting with patients who have anxiety, anger, or are in acute distress related to injections. This will emphasize “safety.”
Pain Relief Methods
• Educate staff on use of EMLA & Elamax
– Appropriate ages
– Ways to administer
– Guidelines regarding which procedures and situations it is appropriate for use in
• Standard Order Set
– Create a standard order set for pain medications to be available when injections, blood draws, or IV’s are ordered.
– Need the ability to un-select this option when not appropriate.
– Need a physician to help champion this.

10/8/2014
16
Sucrose Solution for Infants
• Evidence-based intervention
• Used before injections to
change the perception of
pain for the infant
• Age range: up to 4-6 months
• Concern voiced that
potentially using sucrose in
clinic is modeling
inappropriate behavior for
parents with dental
implications
Scale-Up Successful Interventions
• Start in one small area
• After first round was
successful, scale up in 2
areas
• Then 4 areas
• Continue to scale up until
you’ve reached all areas
Scale-up Successful Interventions
Evaluate EBP
• Obtain outcome measures and concurrent
feedback on implementation of EBP
• Continually re-evaluate
Resource: Child Life Council
Evidence-Based Practice

10/8/2014
17
Plan for Sustainability and Spread
• Sustain - Make improvements “stick”
• Spread - Improvements from one practice
team or site are adopted by another team
• Both endeavors require change processes
but strategies are fundamentally different
from QI rapid change process
Objective:
• To successfully spread the improvement
beyond the original target patient population
or department if appropriate.
Plan for Sustainability & Spread
QI Journey: Implementation Challenges
• Difficulty finding/ keeping stakeholders
• Resistance from staff to change one’s practice
• Absence of standard order sets in the electronic
medical record
• Impact on patient and clinic flow
• Lack of resources, time, and staffing to
implement practice change while maintaining
one’s patient-care load
• Scheduling conflicts with QI team
• Prioritizing commitments with QI team
Implementation Successes
• Potential to help children and families who
are vulnerable
• Potential to affect the practice of many
nurses, medical assistants, and physicians

10/8/2014
18
What Can You Do to Help?
• Follow the BESt guidelines when helping patients
receive injections
• Encourage/ refer others to the guidelines and
information too
• Pass out educational brochures to families and role
model appropriate interventions
• Promote the use of non-pharmacological
interventions proven through research
• Help us with creating standard order sets
• Can we show our educational slides in your area?
• Be a part of an EBP project!
EBP Modules: http://childlife.org/Resource%20Library/EBPModules.cfm
Evidence-Based Practice
References • Cincinnati Children’s Hospital Medical Center (2014). BESt Template.
http://centerlink.cchmc.org/content2/67597/
• Cincinnati Children’s Hospital Medical Center (2014). Quality Improvement
Education. Retrieved from http://centerlink.cchmc.org/content1/11151/
• Cincinnati Children’s Hospital Medical Center (2014). Strength of Evidence
Pyramid. Retrieved from http://centerlink.cchmc.org/content2/67597/
• Higgins, J.P.T., & Green, S. (Eds). Cochrane Handbook for Systematic Reviews of
Interventions Version 5.0.2 [updated September 2009]. The Cochrane
Collaboration, 2009. Retrieved from www.cochrane‐handbook.org.
• Lohr, K.N., Eleazer, K., & Mauskopf, J. (1998). Health policy issues and
applications for evidence‐based medicine and clinical practice guidelines. Health
Policy, 461‐19.
• Melnyk, B. M. and E. Fineout-Overholt (2005). Evidence-based practice in nursing
& healthcare : a guide to best practice. Philadelphia, Lippincott Williams & Wilkins.
• Morris, J. (2012). Child Life Council Evidence-Based Practice Position Statement.
Retrieved from http://childlife.org/files/CLCPositionStatementEBP.pdf
• Shamszad, K. (2014). Introduction to Quality Improvement Lecture Series.
Personal collection of K. Shamszad, Cincinnati Children’s Hospital Medical Center,
Cincinnati, OH.
Evidence-Based Practice

10/8/2014
19
Questions?


















