Learning Disability Census
44
Learning Disability Census Awareness event Manchester 11 September 2013
-
Upload
mohammad-jennings -
Category
Documents
-
view
33 -
download
1
description
Learning Disability Census. Awareness event Manchester 11 September 2013. Programme. Background Purpose of event Census coverage Data collection Questions. Zawar Patel. Learning Disability Policy Lead Department of Health. Winterbourne View Hospital. Opened in December 2006 - PowerPoint PPT Presentation
Transcript of Learning Disability Census

2
Programme
• Background
• Purpose of event
• Census coverage
• Data collection
• Questions
Zawar Patel
Learning Disability Policy LeadDepartment of Health

4
Winterbourne View Hospital
• Opened in December 2006• Registered for assessment and treatment and
rehabilitation for people with learning disabilities• Most patients placed there under the Mental
Health Act by commissioners from across England• Closed in 2011 after abuse of patients exposed• Several reports into events at Winterbourne View
– NHS Report looked at how people were placed there– Serious Case Review gave details of what happened

5
Transforming care
• Department of Health Review from May 2011 to December 2012
• Looked at how people with behaviour that challenges are supported across England
• Informed by: – Other reports and evidence, including CQC inspections of
services for people with learning disabilities– Involvement and engagement with people with learning
disabilities or autism, family carers, providers, commissioners and staff
• Final report published in December 2012

6
Transforming care - Issues identified
• Around half of patients were far from home• Very long stays. In some cases over 3 years• Patients frequently subject to restraint• Families not allowed to visit patients on wards
or in bedrooms• Closed culture made abuse hard to spot• Inadequate access to advocacy for patients• Complaints not handled properly
7
Concordat: Programme of Action
• Signed by more than 50 organisations • Over 60 actions focused on:
– Improving the quality of care and outcomes– Planning around needs of patients from childhood– Ensuring provision of local, personalised services– Avoiding unnecessary inpatient assessment and treatment– Moving people from hospital back home or to community
support quickly– Clear line of sight and responsibility from commissioners to
each individual in inpatient settings
8
Concordat: Programme of Action
• Key commitments – Commissioners to identify people with a learning disability or
autism and / or behaviour that challenges, who may also have a mental health condition
– To review identified people’s care and if appropriate move individuals to community settings
– Local joint plans in every area based on models of good care for people of all ages
– Joint Improvement Programme led by NHS England and Local Government Association to work with local areas
• Oversight of progress through the Learning Disability Programme Board

9
Learning Disability Census• Concordat action to commission an audit of current (inpatient)
services for people with challenging behaviour to take a snapshot of provision, numbers of out of area placements and lengths of stay
• The audit will be repeated one year on to enable the Learning Disability Programme Board to assess what is happening
• Learning Disability Census identified as way of delivering this action
• Based on Count Me In census methodology, but questions changed to focus on issues identified in Transforming care
• Data will be:– Published to show what is happening nationally– Shared with commissioners to support plans to review
people’s care

10
Census coverage – who is included?
• People in inpatient beds for mental and / or behavioural healthcare
• Who have either Learning disabilities or Autistic Spectrum Disorder (including Asperger’s Syndrome)– Any age– Any level of security (General / Low / Medium / High)– Any status under the Mental Health Act (Informal or detained)
• Do not include:– People in accommodation not registered with the CQC as hospital beds– People in beds for physical health care– People who do not have either learning disabilities or autism

11
What do we want from the Census?• How many people with a learning disability or autism
are currently in in-patient mental and behavioural care beds?
• How many have personality disorders or mental illnesses requiring hospital in-patient treatment now?
• How many are known to local commissioners and being actively managed by learning disability specialists from their home area?
• How many are working towards a planned discharge?• How satisfactory or unsatisfactory are current
placements?• How does this vary around the country?

12
National policy drivers
• Everyone counts: Planning for Patients 2013/14 – Guaranteeing no community is left behind or disadvantaged– Better outcomes from mental health services
• NHS Mandate– “The NHS Commissioning Board’s (NHS England) objective
is to ensure that vulnerable people, particularly those with learning disabilities and autism receive safe, appropriate, high quality care. The presumption should always be that services are local and that people remain in their communities; we expect to see a substantial reduction in reliance on inpatient care for these groups of people”

Giovanna Polato
Team Leader - IntelligenceCare Quality Commission

14
CQC Learning Disability Inspection Programme - Background
• An advisory group was established to provide experience and expertise to CQC
• 150 locations were inspected across NHS, independent healthcare and adult social care settings
• We reviewed whether people experienced safe and appropriate care, treatment and support and whether they are protected from abuse
• Inspections were carried out by CQC inspectors, professional advisors and ‘experts by experience’ both people who have used services and family carers

15
Key overall findings
• Overall just under half (48%) of locations did not meet the required standards
• Just over half assessment and treatment services were compliant with both outcomes (52%), but more people were in services that were non compliant (58%)
• Independent health care locations were twice as likely to be non compliant as NHS locations (68% and 33% respectively)

Professor Gyles Glover
Co-DirectorLearning Disabilities team
Public Health England

17
Count Me In Census
• Designed to look at ethnic inequalities in treatment for mental and behavioural conditions
• Ran annually from 2005 to 2010 – Learning disability only covered from 2006
• Covered all mental and behavioural in-patient hospitals – NHS and independent
• Following Winterbourne View, a key source of information about the scale of inpatient care for people with learning disabilities
• Census asked about normal use of beds (for people with mental illness or learning disabilities, also about disabilities (including whether each person had a learning disability))

18
Count Me In Census
• The next four slides show what the Count Me In census has shown about inpatient care of people who were reported to have learning disabilities. Some were in learning disability beds, some in mental illness beds
• The census also identified 330 people with autism, but without learning disability in mental illness beds - they are not covered here

19
Trends in in-patients with LD - 1
• Numbers steady since 2007• Increasing proportion in
mental illness beds since 2009
• Increasing proportion in independent sector beds
Mental Illness vs Learning disability beds:
NHS vs independent sector beds:

20
Trends in in-patients with LD - 2
• Numbers in A&T beds fairly steady
• Increase in number in Rehabilitation beds
• Decrease in numbers in Long Stay and ‘other’ beds
(Bed type data lost for 2008)
• Proportion staying over 5 years falling
• Since 2007, small increase in proportion staying less than 12 months
Type of in-patient bed:
Stay length at time of census:

21
Substantial proportion with apparently unknown commissioner
Type of commissioner

22
Frequency of incidents
Learning Diability
Mental Illness
TotalLearning Diability
Mental Illness
Total
Seclusion 123 (3%) 53 (4%) 176 (4%) 26 (1%) 6 (0%) 32 (1%)Restraint 783 (21%) 197 (14%) 980 (19%) 262 (7%) 42 (3%) 304 (6%)Self-harm 582 (16%) 124 (9%) 706 (14%) 238 (7%) 39 (3%) 277 (6%)Assaults 592 (16%) 146 (11%) 738 (15%) 182 (5%) 22 (2%) 204 (4%)Accidents 374 (10%) 106 (8%) 480 (10%) 51 (1%) 11 (1%) 62 (1%)Patients 3642 1385 5027 3642 1385 5027
Twice or more in three months Ten times or more in three monthsBed type
The table shows the numbers (and percentage) of patients experiencing each of the types of adverse event shown at least twice and at least ten times in the three months up to the census date. Ten times in three months is on average roughly once per week.

23
Rate of use varies widely
between areasMap shows in-patients in A&T beds for people with learning disability per 1000 people known to GPs in the areas in which they live
Note this map uses a narrower set of data – LD beds only, and only A&T beds, also omits people whose commissioner is unknown
London
In-patients per 1000 known to GPs with LD

Catherine Faley Data Collection Section Head
&Robert Cavalleri
Specialist Learning Disabilities Project Lead
Health and Social Care Information Centre

25
Learning Disability Census - Data Collection
• Overview of system• Registration process (During September)• Data entry and validation (First 2 weeks of
October)• Data and definitions• Key messages
26
System
Clinical Audit Platform:• Lots of benefits• Internet Explorer 7 or above,
Google Chrome or Firefox recent versions

27
Registration Process Part 1
You will be invited to register when the registration period is open
Registration is a two step process, first of all you get a single sign on (SSO) account.
https://login.ic.nhs.uk/Login.aspx?
You use an email to register, you need to remember this for the next step.
28
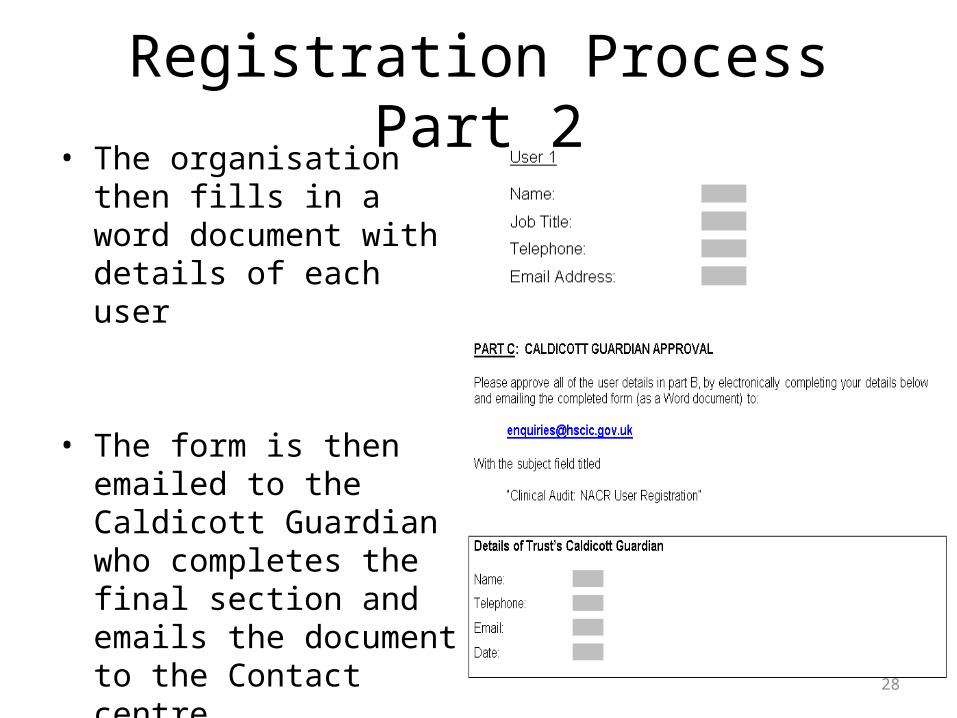
Registration Process Part 2• The organisation then fills in
a word document with details of each user
• The form is then emailed to the Caldicott Guardian who completes the final section and emails the document to the Contact centre

29
Registration
• The Health and Social Care Information Centre Contact Centre will:– verify the Caldicott Guardian; then– they will add the users to the system; and,– send them an email letting them know they can
start using the system

30
Data Entry
• Prepare data in advance– Spreadsheet – format, accurate, complete (refer
to dataset)
• Individual patient record (if “small” numbers, 20 or so), or
• File upload

31
Data Entry – Individual Record
You can add a new record here
LD Census
LD Census Home

32
Data Entry – Individual RecordEnter NHS Number
And date of birth
33
Data Entry – Individual RecordMandatory items are clearly
shown
Help text will be provided for each data item

34
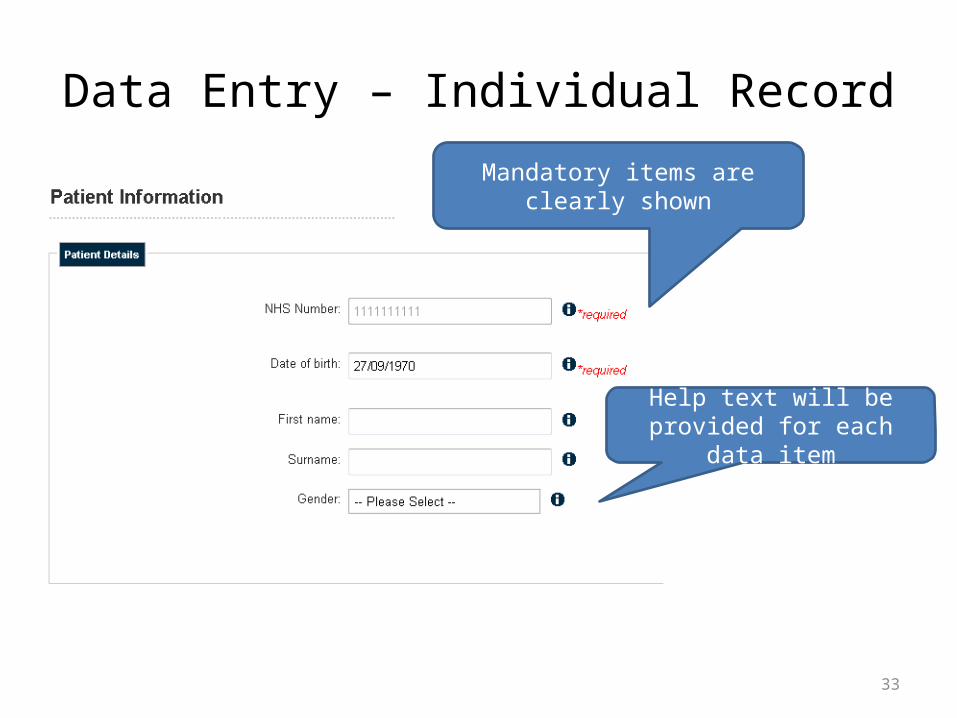
Data Entry – Individual Record
Then add all required data as per dataset:
• Fields are either mandatory or “required”• On the web form and file submission,
validation errors will show up as data are submitted
• Help text will be available where required next to the data item to which it refers

35
Data Entry – File UploadIf many patients – use file upload (csv format)• Guidance will be available• Mandatory fields MUST be completed in order
to upload• Upload file, report shows errors against
relevant row• Correct any errors and resubmit

36
Data and Definitions
• Some Key Fields:– NHS Number (Q2)– Postcode of patient’s usual address (Q5)– Patient’s date of birth (Q8)– Reason for Hospitalisation (Mental Illness, Learning Disability,
Challenging Behaviour, Personality Disorder/Self Harm/Other (Q15)– Disability (Sight, Hearing, Learning Disability, Autistic Spectrum
Disorder, Mobility Impairment) (Q17 - 21)– Hospital Site Location ID (Q32)– Hospital Site Location name (Q33)– Hospital Site Location postcode (Q34)– Service Type (MH or LD ward) (Q35)

37
Data and Definitions
• Learning disability includes the presence of:– A significantly reduced ability to understand new or
complex information, to learn new skills (impaired intelligence), with;
– A reduced ability to cope independently (impaired social functioning) which started before adulthood, with a lasting effect on development
Valuing PeopleA New Strategy for Learning Disability
for the 21st CenturyA White Paper
March 2001
38
Content and rationale
• Patient registration information– As at 30 September 2013. Provides national
snapshot of service receipt– Definitive (actual) rather than estimated– Identifies how close to home people are receiving
services– Why they are receiving this type of service

39
Information on admission
• Determines formal / informal nature of accommodation treatment and if current
• Patterns of referral – which agencies are referring to specialist services
• Are stays lengthy – residential accommodation or assessment and treatment?
• Which needs are not being met in communities close to home?

40
Experience of care
• Determination of the frequency of incidents:– Self harm– Accidents– Physical assault– Restraint– Seclusion
• What is the national picture for incidents and how do provider units compare with this?

41
Accommodation and location
• Type of environment – are outcomes associated to facilities?
• Where are services being provided and for how many patients?

42
Patient care details
• Is care planned, agreed and reviewed with access to support from services and families locally?
• Is medication a significant factor in the provision of treatment and care?
• Are safeguards in place?• What is the cost of care?

43
Key Messages
• Census date = 30 September 2013• Register before then• Please complete form in pack with details of
contact• Prepare data in advance• Helpdesk = [email protected]• www.cqc.org.uk• www.hscic.gov.uk/ldcensus

44
Health and Social CareInformation Centre - Contacts
Catherine Faley [email protected] Ellison [email protected]
Robert Cavalleri [email protected] HSCIC Contact Centre:
• 0845 300 6016• [email protected]