
Learning 2.0: Robust, Rigorous, Relevant, and Rapid
29
he Health Services Researcher of 2020: Summit on the Future of HSR Data and Methods Learning 2.0: Robust, Rigorous, Relevant, and Rapid Paul Wallace MD Permanente Federation Kaiser Permanente [email protected]
-
Upload
felicia-korbin -
Category
Documents
-
view
35 -
download
1
description
Learning 2.0: Robust, Rigorous, Relevant, and Rapid. Paul Wallace MD Permanente Federation Kaiser Permanente [email protected]. “Gray Areas”. The last 115 new technologies examined:. ?. Generally not medically appropriate. Medically appropriate. 7. - PowerPoint PPT Presentation
Transcript of Learning 2.0: Robust, Rigorous, Relevant, and Rapid
The Health Services Researcher of 2020: A Summit on the Future of HSR Data and Methods
Learning 2.0: Robust, Rigorous, Relevant, and Rapid
Paul Wallace MDPermanente FederationKaiser [email protected]

“Gray Areas”...
3
Insufficient evidence because the evidence is:
A. Of insufficient quantity and/or quality
B. Conflicting or inconsistent
C. There is no evidence
Medically appropriate
Generally not medically appropriate
66
3
738
1
The last 115 new technologies examined:
?

“Gray Areas”...
4
Insufficient evidence because the evidence is:
A. Of insufficient quantity and/or quality
B. Conflicting or inconsistent
C. There is no evidence
Medically appropriate
Generally not medically appropriate
66
3
738
1
The last 115 new technologies examined:

Comparative Population Effectiveness: The Kaiser Permanente National Joint Replacement Registry
[Evaluation]feedback
changed practicewith respect to:
implant selection,minimallyinvasive
procedures,uncementedknees, and
surgicalindications and
preoperative care.
Paxton,EW et al; The Permanente Journal
15:12-16, 2008

Predictive Modeling...In patients with diabetes, Aspirin-Lisinopril-Lovastatin (ALL) as a daily combination, has a greater impact on cardiovascular risk than aggressive HbA1c (glucose) control
Average annual risk of various events
0
0.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
0.045
MI Stroke ESRD Blind Dying
Nothing
HbA1c control
ALL


8
Sea
n T
un
is,
CM
TP

DiabetesHeart FailureCoronary Artery
DiseaseDepressionChronic PainCancerAsthma and COPDDementiaFallsObesity…CO-MORBIDITIES
The Business of Health Care in 2009… chronic health conditions increasingly underlie the bulk of health care costs
0%
20%
40%
0% 20% 40% 60% 80% 100%0% total cost
30 + % of total cost
% of People
1% of people
70% of people20% of people
Premium level
100%
80%
60%

Is “more care better” for the patient with Multi-Morbidity?
N Engl J Med 351;27 2870-2874 December 30, 2004
What is the “dose response” for relating the number of things you do to achieving clinical outcomes?
# of Interventions D
es
ired
Re
sult

11
20 30 40 50 60 70 80 90
AgeWorking or Not?Working Years
$
FFS Medicare
Prevention
Usual Care
A key challenge
Phil Madvig MD The Permanente Medical Group
(Not
to
scal
e at
hig
her
ages
–
not
even
clo
se!)

12
20 30 40 50 60 70 80 90
AgeMortality diffWorking or Not?Working Years
$
FFS Medicare
Prevention
DM +End-of-Life
PalliativeCare
Usual Care
A key challenge: Living to utilize...
Phil Madvig MD The Permanente Medical Group
(Not
to
scal
e at
hig
her
ages
–
not
even
clo
se!)

Care in the last 6 months of life...
KPMedicalCenters
Non-KPMedicalCenters
(Same Cities)
Non-KPMedicalCenters(All US)
The Dartmouth Atlas Applied to Kaiser Permanente: Analysis of Variation in Care at the End of LifeBy Matt Stiefel, MPA, Paul Feigenbaum, MD, and Elliott S Fisher, MD, MPH The Permanente Journal/ Winter 2008/ Volume 12/ Number 1



Health 0.0“Rules of the Game” model
Coverage policies, prior approval, ‘utilization management’
? Evidence Based Medicine
Health 0.0“Rules of the Game” model
Coverage policies, prior approval, ‘utilization management’
? Evidence Based Medicine
“Skin in the game” model Co-payment and Deductibles Financial incentives High Deductible, Value Based and
Consumer Directed Health Plans (Shared Decision Making)

Health 0.0“Rules of the Game” model
Coverage policies, prior approval, ‘utilization management’
? Evidence Based Medicine
“Skin in the game” model Co-payment and Deductibles Financial incentives High Deductible, Value Based and
Consumer Directed Health Plans (Shared Decision Making)
“Brain in the game” model Sustainable behavior change Motivational interviewing and
coaching Shared Decision Making
Health 1.0...

Health 2.0
User Generated Content
Patient Networks and Communities
“Dis-intermediation”
Patient-centered Personalized
Health 2.0
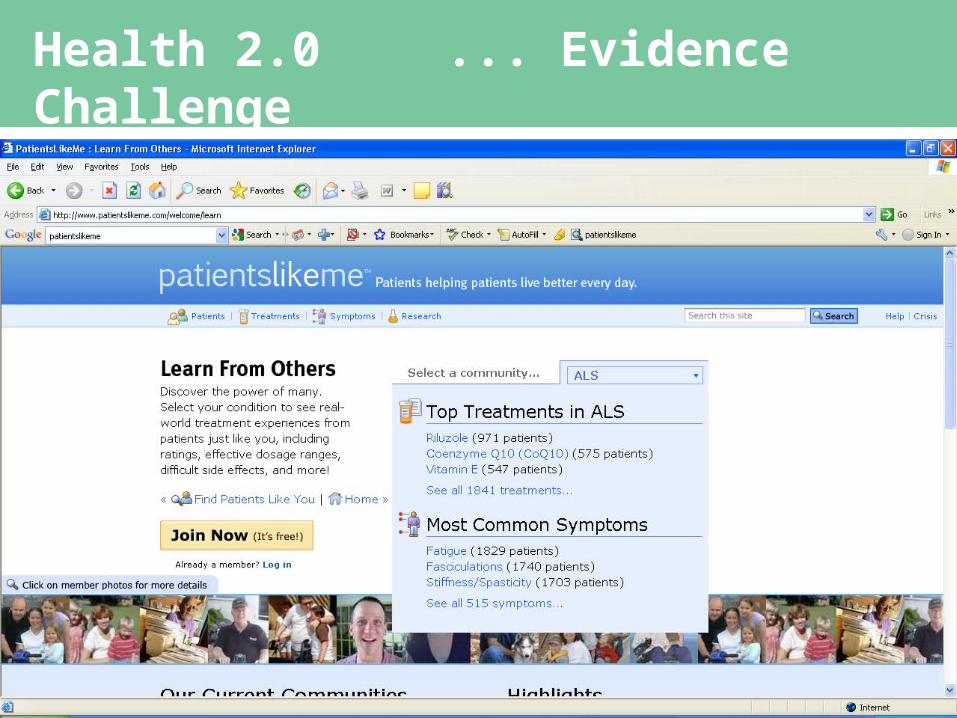
Health 2.0 ... Evidence Challenge
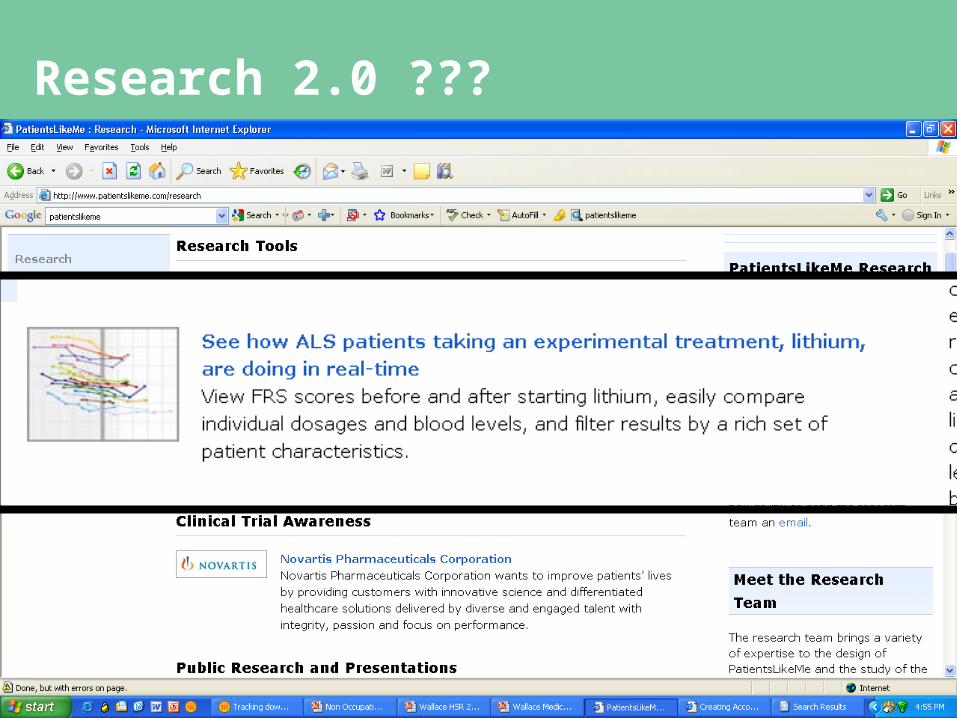
Research 2.0 ???

Cross cutting values...Health 0.0 thru 2.0
The Trusted source
Knowledge-based
Values-based
An Oncology Patient in 2020...

An Oncology Patient in 1996...

An Oncology Patient in 1996...
“Don’t tell me what to do, doc...
An Oncology Patient in 1996...
“Don’t tell me what to do, doc...
Help me understand what all this information means for me.”


















