Lean Six Sigma – Intake Process Streamlining
32
Lean Six Sigma – Intake Process Streamlining Presented by : Nathan McKenzie, Christine Peneyra, Manpreet Bhella
Transcript of Lean Six Sigma – Intake Process Streamlining

Lean Six Sigma – Intake Process Streamlining
Presented by : Nathan McKenzie, Christine Peneyra, Manpreet Bhella

Why Integrate Lean & Six Sigma?
Copyright © NOVACES, LLC. All rights reserved.

Lean: A Strategy and Philosophy
Copyright © NOVACES, LLC. All rights reserved.

Six Sigma

The Hidden “Factory”
Copyright © NOVACES, LLC. All rights reserved.

Understanding Process
Copyright © NOVACES, LLC. All rights reserved.

Intake Process Background
During the intake process, candidates are being asked similar questions regarding past history by the enrollment team, intake RN, intake team and SB/EB (South Bay/East Bay) IDT.
SF Region: 12 of 32 topic questions (37.5%) are asked by 4 or more of the 5 team members
SB/EB Region: 29 of 32 topic questions (90%) are asked by 3 or more of the 9 team members
SF Region: 5 hrs total assessment timeSB/EB Region: 6hrs total assessment time
By analyzing the redundancy identified during the Lean Six Sigma assessment process, the intake team can assess the potential impact a reduction in assessment time will have on health care hospitality initiative goals, team efficiency in assessing new candidates and organizational productivity with non-intake related tasks.

Rapid Improvement Event (RIE)
The RIE is an approach to team-based problem solving and helps teams focus on process problems
• Describe the current state• Identify gaps & problems (wastes)• Brainstorm solutions• Define the future state• Implement as much as possible and develop a
plan for remaining items

SIPOCSUPPLY INPUT PROCESS
Intake ProcessOUTPUT CUSTOMERS
Who supplies the process inputs?
What inputs are required for the
process to function properly?
What are the major steps in the process?
What are the process outputs?
Who receives the outputs?
-Intake Coordinator-Enrollment Specialist (ES)-Intake RN-Intake Tean Manager-MD/SW/OT/PT/PM/HC RN/ RD-Center coordinator (SF)-MBHC-Front Desk/Center Coord.(SB/EB)-OL CG (SB/EB)-Medical Records-Transportation-Activity Dept.
-Inquiry received through calls, events, emails, referrals- Intake form and home visit request createdScreening by ES, Intake RN, SW (entire team SB/EB)-Documentation in EHR or Salesforce-Complete level of care form and submission to MR, then to State-State decision w/in 5 business days or less-Transfer summary sent to ProgramManager (SF)-Schedule Enrollment Conference & update enrollment record-HV,FV, MD/SW assess (all assess)
-Initial Contact w/ Enrollment Specialist/Intake Coord.-In-person meeting (tour, friendly visit)-Home Visit by Intake RN & ES-Eligibility assessment & care plan meeting:· Intake team (SF)· Entire team (SB/EB)· 30th St.: HomeCare visits candidates home before enrollment-State submission-Enrollment conference(OT/PT assessment completed SF region)
-Candidate enrolls with OnLok-Candidate withdraws-Team denial-State denial/approval
-Candidate-Family-Caregiver-Intake Coordinator-Enrollment Specialist-Intake RN-Intake team Manager-MD/SW/OT/PT/PM/HC RN/ RD-Center coordinator (SF)-MBHC-Front Desk/Center Coord.(SB/EB)-OnLok Caregiver (SB/EB)-Medical Records-Transportation-Activity Dept.-Outside agencies

TIMWOOD 7 DEADLY WASTES
Copyright © NOVACES, LLC. All rights reserved.

TIMWOOD

Perform a Value Analysis

Perform a Value Analysis (cont)
VALUE ADDTHEMES
• Assessments
• Medical records review• Communication with
candidates• Mental health assessment
• Home visit• Friendly visit• Enrollment conference
BUSINESS VALUE ADDTHEMES
• Salesforce.com updates
• Deferrals
• Referrals
• State approvals
• TB tests
• Level of Care (LOC) form
• Enrollment meetings
• Care plan meetings
• Friendly visits
• Home visits by Intake RN
• Transfer summary (SF)
• MD & SW assessments

Perform a Value Analysis (cont)
WASTE THEMES• Post enrollment-extra HC visit (30th)
• Follow-up assessment
Example: POWELL center waitlist few months. F/U visit needed as candidate health may have changed
• Candidate withdraws
• Candidate decides not to give up IHSS or PCP
• Lack of interpreter
• Different assessments scheduled on different dates
• Limitations of physical space (internal: conference rooms, desk space, dedicated space for privacy)
• TRAVEL TIME: home visits, center to center, large territory
• TIME: assessments by different team members, couples assessments, home visits, waitlist process
• Change in health status
• Decision making capacity (fail fast-how to determine sooner)
• Redundancy of questions being asked by enrollment team to cdt
• Conflicting history reports within IDT
• On-going call to cdt to determine interest level
• TMAHC process

ROOT CAUSE ANALYSIS
Increased cycle time (Active & Wait) -FISHBONE (mother nature, measurement, machine, materials, manpower, method)

RIE Outcomes
• IDT team members and Lean Six Sigma Green/Black Belts held a 3 days long work session.
• 2 new intake process improvement initiatives were identified by the IDT team
• Standardization of assessment questions + Customized assessments + Addition of intake coordinators

RIE Outcomes - Team Take Ons
STANDARDIZATION-universal document for all to view-remove redundant questions
Why we should do it? • Reduction in assessment time• Reduction in duplicate efforts• Increase in team morale

RIE Outcomes - Team Take Ons
COORINATOR / USING RESOURCES WELL-coordination between ES, PM, & IDT-admin support-review medical records (software?)-provide meals & activities calendar (Just Do It)-determine if all MR is needed-requesting MR more precisely (Just Do It)-pre-review of MR: tabbing/sorting
Why we should do it? • IDT needs help with administrative tasks that are shared among
different team members.
RIE Outcomes - Team Take Ons
CUSTOMIZED ASSESSMENTS
-minimum assessment set-buy in-borderline “unsafe” candidate
Why we should do it? • Make the process Lean (reduction of waste)

LSS Intake and Enrollment Tiger Team Members

Current State
1) Initial Contact w/ Enrollment Specialist/Intake Coordinator2) In-person meeting (tour, friendly visit)3) Home Visit by Intake RN & Enrollment Specialist4) Eligibility assessment & care plan meeting:
• Intake Team (SF)• Entire team (SB/EB)• 30th St.: Home Care visits candidate home before enrollment conference
5) State submission6) Enrollment conference7) (OT/PT assessment completed SF region)

Future State RIE Recommendation
1) INITIAL CONTACT 2) FRIENDLY VISIT 3) CUSTOMIZED What is minimum?
ASSESMENT IDT rep at this time? Buy In for borderline “unsafe” cdtFloat assessment?
4) STATESUBMISSION
5) IDT ASSESSMENTCARE PLANNINGENROLLMENT CONFERENCE

Future State – Intake Process

Data: Total potential candidates (SB/EB)
• What is known:• 166* candidates between January to August 2019• 65% conversion rate of candidates from home visit to state approval• 35% drop out rate (100% potential candidates – 65% conversion rate)
• Current total candidates for 2019: 166 (from January to August 2019 = 75% of 2019)
• Assuming trend remains: multiply by 25% for remainder of year (September – December 2019)
• Potential total candidates per year = 166 x 0.25 = 41.5 potential participants for September to December 2019.
• Round 41.5 to 42 potential participants from September to December 2019• Total potential candidates for all of 2019 = 208 (166 current + 42 potential)• Total potential dropouts = 73 (rounded from 72.8)
• 208 potential candidates x 35% drop out rate = 72.8* = Data gathered from SalesForce
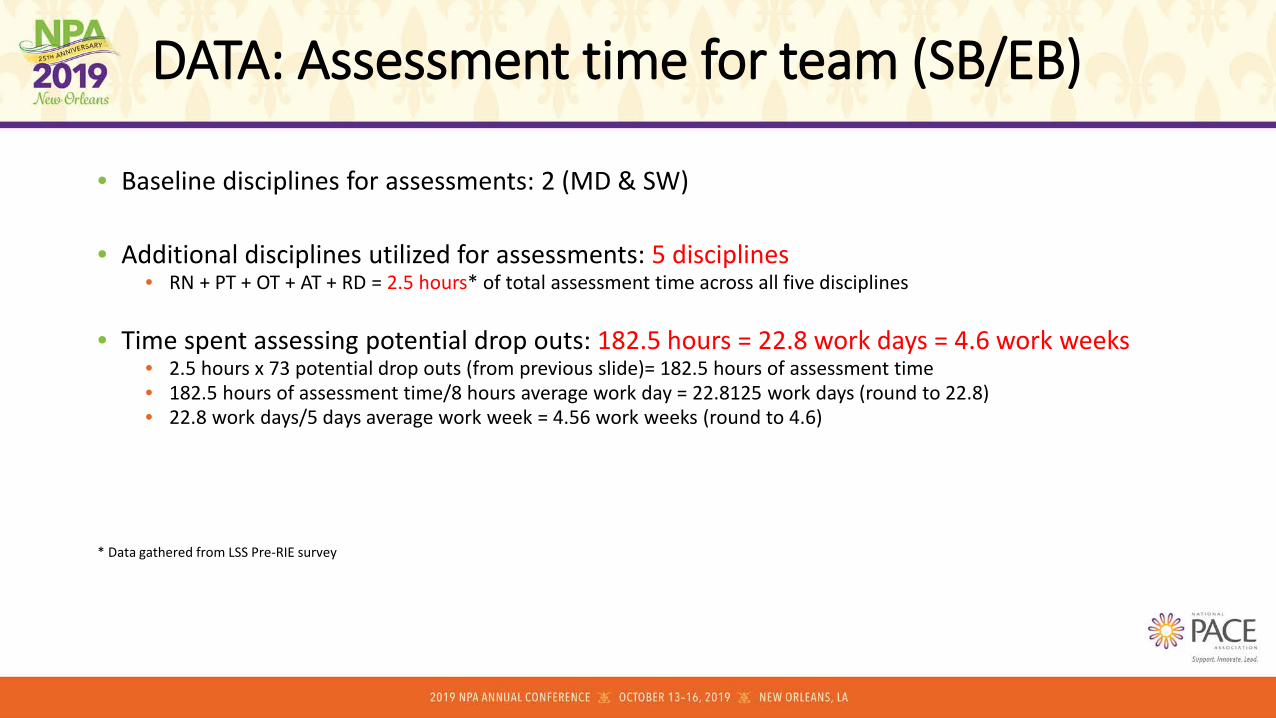
DATA: Assessment time for team (SB/EB)
• Baseline disciplines for assessments: 2 (MD & SW)
• Additional disciplines utilized for assessments: 5 disciplines• RN + PT + OT + AT + RD = 2.5 hours* of total assessment time across all five disciplines
• Time spent assessing potential drop outs: 182.5 hours = 22.8 work days = 4.6 work weeks• 2.5 hours x 73 potential drop outs (from previous slide)= 182.5 hours of assessment time• 182.5 hours of assessment time/8 hours average work day = 22.8125 work days (round to 22.8)• 22.8 work days/5 days average work week = 4.56 work weeks (round to 4.6)
* Data gathered from LSS Pre-RIE survey

DATA: Assessment time per discipline
• What we know:• 2.5 hours* per assessment x 73 potential drop outs =
182.5 hours of assessment 22.8 work days 4.6 work weeks
• Calculations: time of assessment/73 drop outs = # hours/8 hours per work day = # work weeks/5 days in work week (all figures rounded):
• RN: 45 min per assessment (0.75/hour) x 73 potential drop outs = 54.75 hours = 6.84 work days = 1.37 work weeks
• PT: 30 min per assessment (0.5/hour) x 73 potential drop outs = 36.5 hours = 4.56 work days = 0.91 work weeks
• OT: 30 min per assessment (0.5/hour) x 73 potential drop outs = 36.5 hours = 4.56 work days = 0.91 work weeks
• AT: 30 min per assessment (0.5/hour) x 73 potential drop outs = 36.5 hours = 4.56 work days = 0.91 work weeks
• RD: 15 min per assessment (0.25/hour) x 73 potential drop outs = 18.25 hours = 2.28 work days = 0.46 work weeks
+---------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
Total combined = 2.5 hours 182.5 hours 22.8 work days 4.56 work weeks
per assessment hours of total assessment of assessments of assessments
* Data gathered from LSS Pre-RIE survey

Data: cost savings
• Combined average compensation for all 5 disciplines per hour: $174.18*• HCRN+ PT + OT + AT + RD = $174.18
• Total compensation cost for assessment time: $435.45 • 2.5 hours of assessment time x $174.18 discipline cost per hour = $435.45
• Total compensation costs for potential dropouts: $31,787.85• $435.45 cost per assessment x 73 potential dropout candidates annually= $31,787.85
POTENTIAL SAVINGS = $31,787.85 PER YEAR
*Data gathered from On Lok HR

• Current state - Redundant questions• SF Region: 12 of 32 topic questions (37.5%) are asked by 4 or more of the 5
team members.• SB/EB Region: 29 of 32 topic questions (90%) are asked by 3 or more of the 9
team members
• Standardization of Electronic Health Records • Customized assessments = less redundant questions• Universal electronic health records document for eligibility assessments
IDT will use information collected from other disciplines for the purpose of eligibility assessments.
Success Metrics – Standardization of EHR

• Current state – IDT members are fulfilling the administrative role to coordinate -between ES, PM, & IDT-admin support-review medical records-determine if all MR is needed-pre-review of MR: tabbing/sorting
• Re-evaluate and re-distribute the job roles of IDT and/or administrative staff and see if certain tasks can be assigned to other staff.
Success Metrics – Intake Coordinator

Change Management
Awareness Desire Knowledge Ability Reinforcement
-Increased productivity and efficiency amongst staff-Increased transparency between intake dept.-Reduction in task duplication-Decreased frustration from cdt from redundancy of questions-Decreased candidate assessment time-Improved cdt experience-Increase in the capacity to enroll new cdts-Leadership team will have the ability to easily manage a standard intake process across all regions-Decreasing utilization of center resources
-Cumulative assessment time reduced by 20%-Increased IDT assessment capacity per day-Increasing IDT productivity outside of intake assessments-increased employee satisfaction-increased cdt satisfaction/experience-Meet census goals-Increase conversion rate between stages of the enrollment process
-Change management guided by process owners-Present to organization: senior team, managers/supervisors-IDT team will need to be familiar with intake assessments topics/questions from all departments-How to use Electronic Health Records system-Coordinator position: knowledgeable about individual healthcare needs of cdts in pipeline. Determine most appropriate course of action
-Involve Medical Records, IT, PL-Coordinator position: knowledgeable about individual healthcare needs of cdts in pipeline. Determine most appropriate course of action-Change management guided by process owners-Identify process owners/ champion involvement
-Project Manager-Develop a control plan:
-process standardization-documented procedures-process capability-monitoring plan-response plan -process audits
-Identify process owners-Champion involvement
Lessons Learned
• Charter – Keeping an open mind for all project activities.• Edit project charter based on new findings, RIE discussion, organizational
focus.
• Change Management - Receptiveness to RIE findings once Tiger Team projects were launched.
• Addressing change management for additional RIE recommendations.
• Green Belts/RIE/Tiger Team members’ availability.• Lean Six Sigma Green Belts – Conflict of interest. • Assign a Project Manager in the beginning of a project.

QUESTIONS ?