Lean 6-Sigma Programbusiness.ca.gov/Portals/0/Files/LEAN6-2018/CDCR-presentation1.pdf · Lean...
19
Lean 6-Sigma Program Gretchen Deel, M.D. ( Project Greenbelt) CALIFORNIA DEPARTMENT OF CORRECTIONS AND REHABILITATION S. Roberts, MD M. Farrell, SRN III (Project Champions) Mary Ann Glynn, CEO, RJD (Executive Sponsor)
Transcript of Lean 6-Sigma Programbusiness.ca.gov/Portals/0/Files/LEAN6-2018/CDCR-presentation1.pdf · Lean...

Lean 6-Sigma Program
Gretchen Deel, M.D.
(Project Greenbelt)
CALIFORNIA DEPARTMENT OF CORRECTIONS
AND REHABILITATION
S. Roberts, MD
M. Farrell, SRN III
(Project Champions)
Mary Ann Glynn, CEO, RJD
(Executive Sponsor)

Project Team: Gretchen Deel, MD – Green Belt Candidate
Chris Carlson – Master Black Belt Coach
Tera TranOn – Black Belt Coach
Mary Ann Glynn, CEO – Executive Sponsor
Steve Roberts, MD – Project Champion
Mia Farrell, SRN III – Project Champion
Ryan Barenchi – Team Member
Lia Stephenson, SirPatrick Paragas – Telemed RNs
Beth Kadani – Telemed Scheduling, Local
Lean 6-Sigma Program
Lean Six Sigma Project: Improving Compliance of Urgent Recommendations from Telemed Specialists

RJ Donovan Telemed Program
Largest volume of Telemed Specialist appointments
Telemed reduces cost and improves safety

Problem Statement/Metrics
Primary Metric: Improve compliance of Urgent Recommendations made by TelemedSpecialist
Urgent = 14 days
Secondary Metric: Improve quality of medical care, reduce cost of medical care
Lean 6-Sigma Program

Upper Spec Limit = 336 hours (14 days) to meet compliance Current Average = 723 hours (30 days) Current maximum 2,800 hours (117 days) % within spec limit = 32% 68% of time = Not meeting goal
Lean 6-Sigma Program
Baseline Capability

Lean 6-Sigma Program
Initial Process Map
insert process map
42 steps5 VA steps37 NVA steps2 rework loops
40 Steps2 VA Steps38 NVA Steps2 Rework Loops

FISHBONE DIAGRAM
TIME VALUE CHART
FMEA
PARETO CHART
SECONDARY PARETO CHART
MULTI-VARI ANALYSIS
HYPOTHESIS TESTING
MOOD’S MEDIAN TEST
Lean 6-Sigma Program
Analysis Tools

Lean 6-Sigma Program
Key Analytical Findings
FMEA – Potential Critical X’s
Pareto Chart – Critical X’s Failure of RN to
Identify a Recommendation as Urgent
Variable Availability of Specialist note for the PCP

Failure to identify urgent recommendations primarily associated with lack of training/experience
Access to Specialist note did not vary between 16 different PCP’s
Varying the Specialist did not significantly influence the timing
Lean 6-Sigma Program
Key Analytical Findings 2

Root Cause of Critical X’s: 5 Why’s
Failure to identify Urgent accounted for 47% of defects
Follow-up wasn't done in 3d causing delay
Variability in RN ordering Urgent PCP follow-up
different experience levels of RNs
Urgent Rec not recognized as different from Routine
RN's that were new to the process did not know Urgent Recs are different
Failure to consistently alert Urgent Recommendations
No standardized training
Urgent Recommendations may occur during a routine visit
Variability in training
Variability in level of care needed with each visit
No standardized process re Urgent Telemed recommendations
No standardized training re Routine v Urgent Recommendations
Defect was not identified in the past
The process was not evaluated as each change happened
The initial workflow process had to change to accommodate RJD large volume
Why?
Why?
Why?
Why?
Failure to access specialist rec accounted for 23% of defects
The specialist's note is difficult to access
It is in MedWeb, retrieved by HIM
HIM has one of the few licenses given out to the facility
When a note is missed there is no notification that it has not been retrieved
Only a few licenses for MedWeb are given out by HQ
HIM pulls the note from all the notes written that day
Cost constraint/HIPAA regulations?
HIM chose not to use the email notification method
A Specialist's note that is not accessible by the PCP causes delay
HIM thought the email notification method would be inefficient
If there is not a note in the chart, the I/P 3d FU visit gets rescheduled
RJD Telemed volume is much larger than other institutions
Specialist notes sometimes are not in the chart in time for the PCP to read it on the 3 day FU
If a note is missed or not put in chart, there is no detection process
One person is responsible for retrieving the note, with no alerts for missed notes
Not Identified as Urgent Note Access VariabilitySPECIFICPROBLEM
DETECTIONFAILURE
SYSTEMIC FAILURE

Failure to Identify/Alert Recommendation as Urgent Standardize process for Telemed RN Training
• RN• PCP
Variable Availability of Information Standardize process Training
• PCP• RN• Telemed Scheduler• HIM• Specialist
Process changes• Email notification – failed/volume• PCP access to MedWeb – requires individual license/add steps• Minimize NVA steps to free up time/improve accuracy
Lean 6-Sigma Program
Improvement Targets based on Root Causes

Standard Work for each process/Visual aid reminder
PCP
Telemed RN
Telemed Scheduler
Urgent Alert Stamp
Standardized training
Educated employees on 5S organization aided by moving centrally
Distance decrease: TM Scheduler moved to HUB near TM RN
eRFS
Decrease NVA steps
Lean 6-Sigma Program
Improvement Implementation
Lean 6-Sigma Program
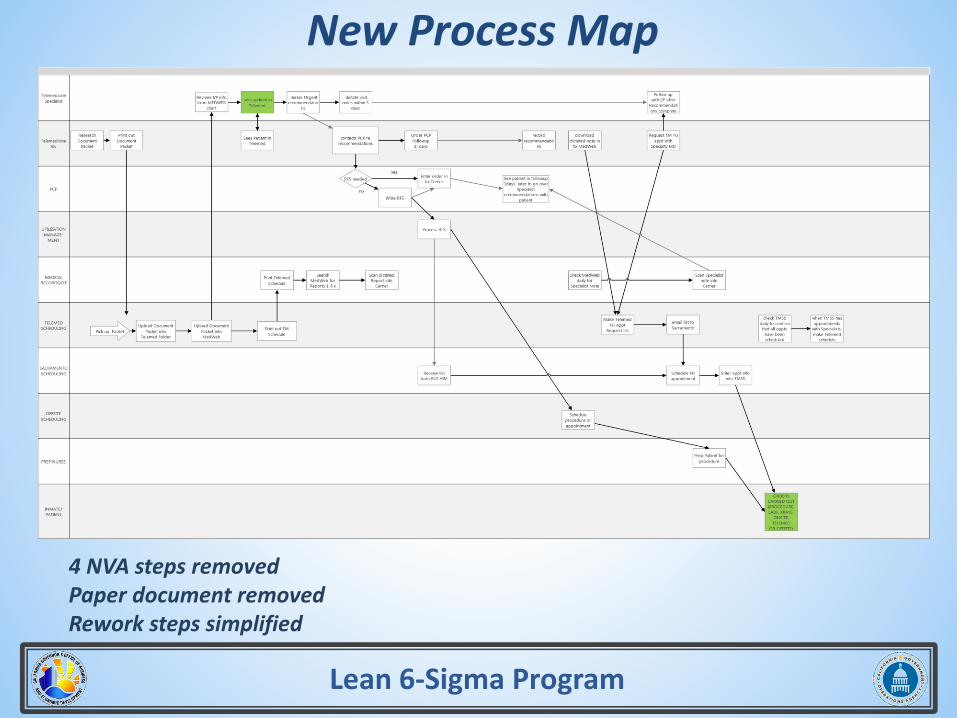
New Process Map
insert new process map
4 NVA steps removedPaper document removedRework steps simplified

Initial Process Capability: 32%
Final Process Capability: 88%, 87% and 93% for past 3 months
Lean 6-Sigma Program
New Capability Analysis
old capability

Controls to be Implemented
Identification of Recommendation as Urgent
Availability of Specialist’s note in chart
Evaluate 10 Charts each month x 6 months, then 20 charts every 6 months
Update Process Capability
Update Process Control
Update FMEA as needed
Re-evaluate process for improvements
Lean 6-Sigma Program
Control Plan

Hard Costs
No “increased revenue”
Telemed Professional/Technical = $35,000; this is < 1 emergent sendout
Cost savings – average of 10 incidences of delay
$2,198 x 4,000 pts/year x .68 failures = $5,978,560
$2,198 x 4,000 pts/year x .13 failures = $1,142,960
Savings = $ 4,835,600 per year
Emergent or offsite visit v onsite
Custody Officer time travelling v inhouse
Transportation time to & from hospital
Hospitalization time – if extended for emergency
Telemed RN/Scheduler/Specialist time
Main acute sources of cost – Cardiac procedure, Sepsis
Specialties with the highest difference in costs
Lean 6-Sigma Program
Financial Benefits
Most Expensive Delays by Specialty
cardiology general surgery ortho
oncology urology other

Improved healthcare for patients
Increased customer satisfaction
Fewer grievances/appeals/lawsuits
Improve morale for employees
Less employee turnover
Less tax burden
Lean 6-Sigma Program
Additional Benefits/Soft Cost

Lean 6-Sigma Program
A3

Name: Gretchen Deel, MD
Phone: (619)661-8634
Email: [email protected]
Lean 6-Sigma Program
Green Belt Contact Information