
Leadership is getting results in a way that builds trust—A Public … · 2013-08-16 ·...
14
Leadership is getting results in a way that builds trust—A Public Health Accreditation Update Tomás J. Aragón, M.D., Dr.P.H. Health Officer, City & County of San Francisco Director, Population Health Division, SFDPH Karen Pierce, Public Health Accreditation Coordinator 20 August 2013 Introduction and review The San Francisco Health Commission has identified three strategic priorities for the Department of Public Health which aligns with the nationally recognized “Triple Aim” (Figure 1). Figure 1: The Public Health Triple Aim 1. Public Health Accreditation (Health) 2. Integrated Delivery System (Care) 3. Financial & Operational Efficiency (Cost) The purpose of public health accredition is to create a high per- forming learning organization that is responsive and accountable to our community stakeholders. We will be evaluated on public health services using 12 domains: No. Domain Description 1 Assess Conduct and disseminate assessments on population health status 2 Investigate Investigate health problems and environmental health hazards 3 Inform & Educate Inform and educate about public health issues and functions 4 Community Engagement Engage the community to identify and address health problems 5 Policies & Plans Develop public health policies and plans 6 Public Health Laws Enforce public health laws 7 Access to Care Promote strategies to improve access to health care services 8 Workforce Ensure competent workforce and professional growth 9 Quality Improvement Ensure continuous improvement of performance and quality 10 Evidence-Based Practices Contribute to and apply the evidence base of public health 11 Administration & Management Maintain administrative and management capacity 12 Governance Maintain capacity to engage the public health governing entity Public health accreditation consists of seven steps: 1. Pre-application 2. Application 3. Documentation 4. Site Visit
Transcript of Leadership is getting results in a way that builds trust—A Public … · 2013-08-16 ·...

Leadership is getting results in a way that buildstrust—A Public Health Accreditation UpdateTomás J. Aragón, M.D., Dr.P.H.Health Officer, City & County of San FranciscoDirector, Population Health Division, SFDPHKaren Pierce, Public Health Accreditation Coordinator20 August 2013
Introduction and review
The San Francisco Health Commission has identified three strategicpriorities for the Department of Public Health which aligns with thenationally recognized “Triple Aim” (Figure 1).
Figure 1: The Public Health Triple Aim
1. Public Health Accreditation (Health)
2. Integrated Delivery System (Care)
3. Financial & Operational Efficiency (Cost)
The purpose of public health accredition is to create a high per-forming learning organization that is responsive and accountable toour community stakeholders. We will be evaluated on public healthservices using 12 domains:
No. Domain Description
1 Assess Conduct and disseminate assessments on population health status2 Investigate Investigate health problems and environmental health hazards3 Inform & Educate Inform and educate about public health issues and functions4 Community Engagement Engage the community to identify and address health problems5 Policies & Plans Develop public health policies and plans6 Public Health Laws Enforce public health laws7 Access to Care Promote strategies to improve access to health care services8 Workforce Ensure competent workforce and professional growth9 Quality Improvement Ensure continuous improvement of performance and quality
10 Evidence-Based Practices Contribute to and apply the evidence base of public health11 Administration & Management Maintain administrative and management capacity12 Governance Maintain capacity to engage the public health governing entity
Public health accreditation consists of seven steps:
1. Pre-application
2. Application
3. Documentation
4. Site Visit

leadership is getting results in a way that builds trust 2
5. Accreditation Decision6. Reports7. Reaccreditation
We are currently in the pre-application step. The application processbegins once we submit a completed application form and requiredsupporting material (see Table ). This material includes, but is notlimited to, three prerequisite documents, updated in the last 5 years:
Table 1: Accreditation TimelineStep Date
Prerequisites December 2013
Application December 2013
Documentation September 2014
PHAB Site Visit January 2015
Accreditation March 2015
1. Community Health Assessment (CHA) and Profile;2. Community Health Improvement Plan (CHIP),3. Public Health Strategic Plan (focus of this update)
The Community Health Assessment and Profile, and the CommunityHealth Improvement Plan have been completed and have been pre-sented to the San Francisco Health Commission. In this update, wefocus on our strategic planning.
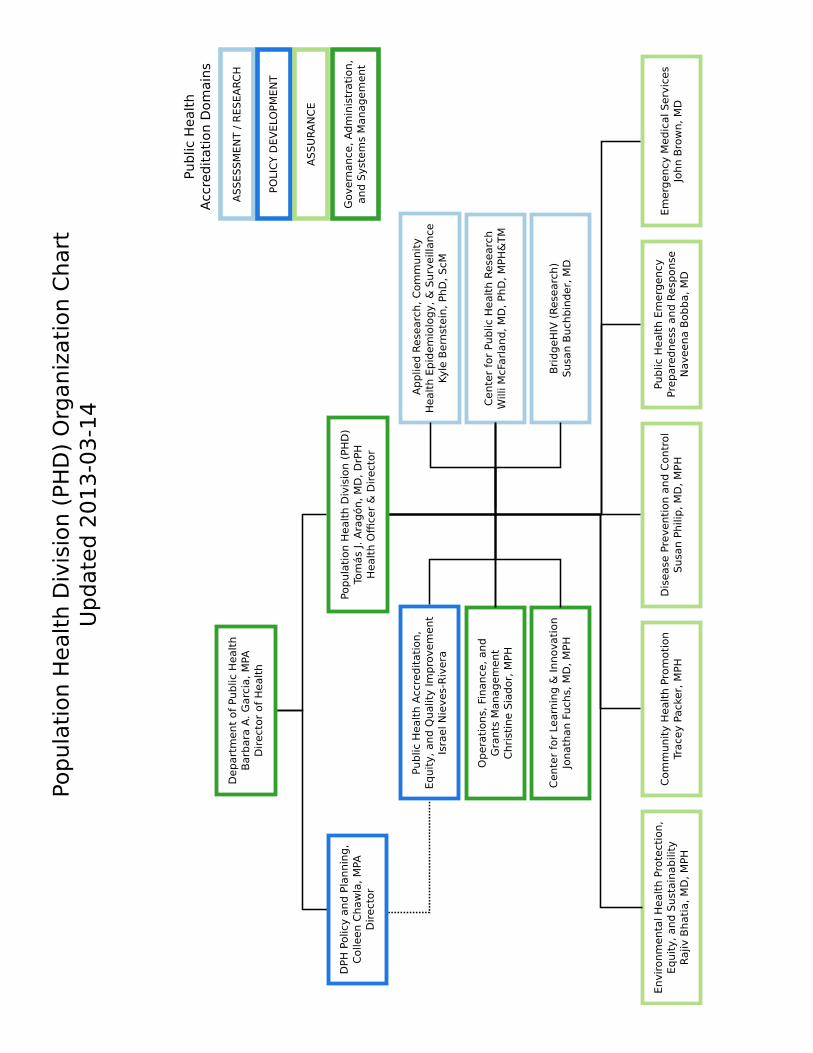
Because public health accreditation involves the evaluation ofpublic health (not medical) services, the effort is being lead by theOffice of Policy and Planning,1 and the Population Health Division.2 1 Director, Colleen Chawla, MPA
2 Director, Tomás Aragón, MD, DrPH
Figure 2: The Baldrige Criteria forPerformance Excellence
Population Health Division Strategic Plan
As part of accreditation, the Population Health Division is undergingan extensive reorganization. To guide the reorganization, accredita-tion, and strategic planning we are adapting the Baldrige Criteria for

leadership is getting results in a way that builds trust 3
Performance Excellence as our overarching framework (Figure 2).3 3 http://www.nist.gov/baldrige/
Baldrige is a national award program in existence since 1987, andits goal is to guide businesses, non-profits, education and healthagencies to become innovative, high performing, and continuouslyimproving organizations. The Baldrige Criteria build on core valuesand concepts which are embedded in systematic processes (Criteria1–6) yielding performance results (Criterion 7) (Figure 3).
Figure 3: The Baldrige Criteria, CoreValues and Concepts, and Results. Corevalues and concepts include Visionaryleadership, Patient-focused excellence,Organizational and personal learning,Valuing workforce members andpartners, Agility, Focus on the future,Managing for innovation, Managementby fact, Societal responsibility, Focuson results and creating value, Systemsperspective
The six of seven Baldridge Criteria are grouped into the Leader-ship Triad (leadership, strategic planning, customer focus) and theResults Triad (workforce focus, operations focus, and results). TheLeadership and Results Triads anchor the Baldrige Criteria, ener-gizing us to focus on leadership development and results-basedmodels. Therefore, our initial primary focus is on the following Cri-teria:
Criterion 1 Leadership using Authentic Transformation Leadership4 4 John J. Sosik and Dongil (Don) Jung.Full Range Leadership Development:Pathways for People, Profit and Planet.Psychology Press, 1 edition, 9 2009.ISBN 9781848728066
Criterion 7 Results using Results-Based Accountability5
5 Mark Friedman. Trying Hard Is NotGood Enough. BookSurge Publishing, 5
2009. ISBN 9781439237861
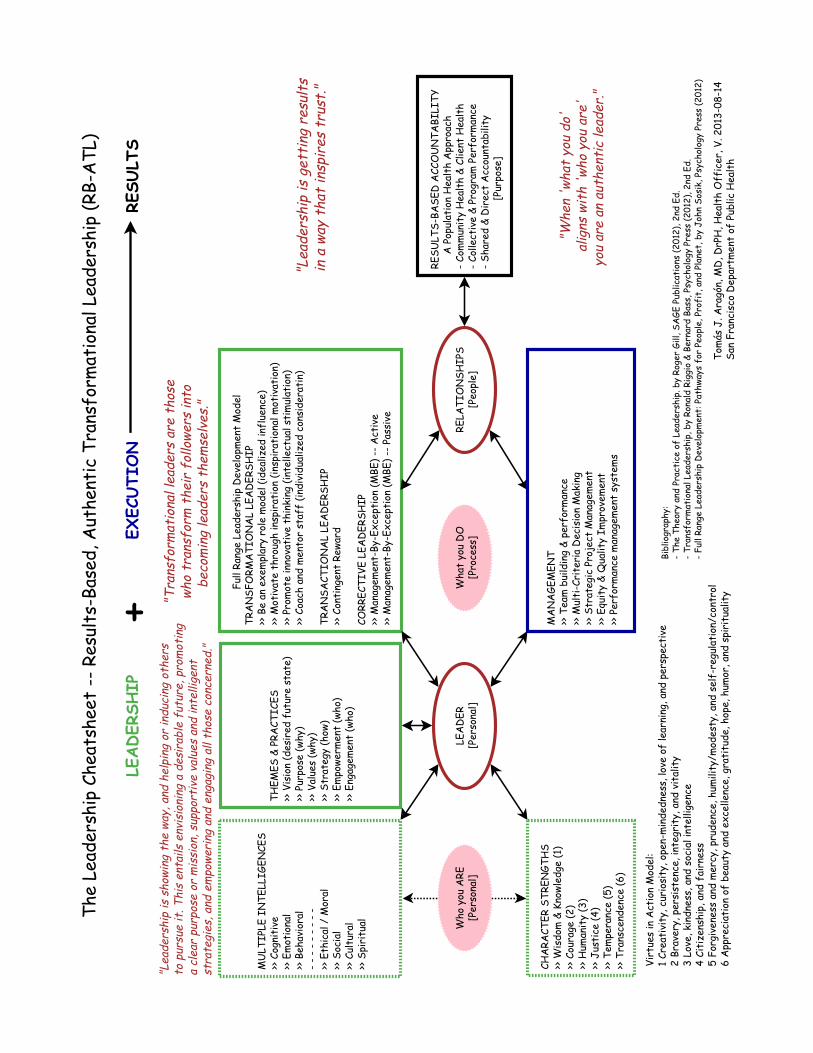
For leadership, we are using the authentic transformational leader-ship model. For results, we are adapting the Results-Based Account-ability (RBA) model where “results” are always defined in terms ofhaving measurable impacts on community health and well-being, orclient health and well-being. The RBA framework is very popularwith public sector and non-profit agencies.

leadership is getting results in a way that builds trust 4
Our overarching goal is to create an organizational culture andsystem of processes to support creativity, innovation, and discovery,and to drive service excellence, continuous quality improvement, andresults-based performance. To achieve this we are implementing thefollowing:
1. Strategic planning retreat on September 24–25, 2013 using RBA todevelop Action Plan for high-priority, citywide health initiatives.
(a) Community Health Improvement Plan6 6 In partnership with San FranciscoHealth Improvement Partnership(SFHIP)(b) African American health
(c) HIV Prevention(d) Public housing(e) Children’s health
2. PHD Leaderhip Academy (Fall 2013: Directors, Year 2+: staff)3. RBA/Equity & Quality Improvement Training Academy (2013)
Summary
For public health accreditation, we are adapting the Baldrige Cri-teria for Performance Excellence. The Baldrige Criteria starts withLeadership (“Driver”) and ends with Results (“Destination”). Forour leadership foundation (Criterion 1) we are adopting the authen-tic transformational leadership model which is evidence-based withvalidated assessment and development tools.
For our results foundation (Criterion 2) we are adopting theResults-Based Accountability framework. RBA is used extensivelyaround the world. In California, RBA is used by Marin, Alameda,San Mateo, Contra Costa, and Los Angeles Counties. LAC PublicHealth as agreed to mentor us.
References
Mark Friedman. Trying Hard Is Not Good Enough. BookSurge Pub-lishing, 5 2009. ISBN 9781439237861.
Roger Gill. Theory and Practice of Leadership. SAGE Publications Ltd,second edition edition, 1 2012. ISBN 9781849200240.
John J Sosik. Leading with Character: Stories of Valor and Virtue and thePrinciples They Teach (PB). Information Age Publishing, 7 2006. ISBN9781593115418.
John J. Sosik and Dongil (Don) Jung. Full Range Leadership Devel-opment: Pathways for People, Profit and Planet. Psychology Press, 1
edition, 9 2009. ISBN 9781848728066.

leadership is getting results in a way that builds trust 5
Appendix A—Results-Based Accountability
Results-Based Accountability (RBA) is “a disciplined way of thinkingand taking action that can be used to improve the quality of life incommunities . . . ” RBA was popularized by Mark Friedman’s bookTrying Hard in Not Good Enough. RBA (also called Outcomes-BasedAccountability) is used by public sector and non-profit agencieswhose missions include addressing complex social challenges usingcollaborative partnerships.
RBA “starts with ends and works backwards, step by step, tomeans. For communities, the ends are conditions of well-being forchildren, adults, families and the community as a whole . . . For pro-grams, the ends are how customers are better off when the programworks the way it should . . . ”
Figure 4: RBA for Community Resultsusing Partnership Shared Accountabil-ity to Improve Community Health andWell-being (Source: Friedman book)
For communities (Figure 4), we ask the following seven questions:
1. What are the quality of life conditions we want for the children,adults and families who live in our community?
2. What would these conditions look like if we could see them?
3. How can we measure these conditions?
4. How are we doing on the most important of these measures? And,what is the story behind the curve?
5. Who are the partners that have a role to play in doing better?
6. What works to do better, including no-cost and low-cost ideas?
7. What do we propose to do?
For programs (Figure 5), we ask the following seven questions:
1. Who are our customers?
2. How can we measure if our customers are better off?
3. How can we measure if we are delivering services well?
4. How are we doing on the most important of these measures? And,what is the story behind the curve?
5. Who are the partners that have a role to play in doing better?
6. What works to do better, including no-cost and low-cost ideas?
7. What do we propose to do?
Figure 5: RBA for Program Perfor-mance using Program Direct Account-ability to Improve Customer (Client)Health and Well-being (Source: Fried-man book)
Notice that questions 4 through 7 are identical; only the first threequestions differ depending on whether the focus is population account-ability for outcomes in a community population, or program accountabilityfor program performance for outcomes in a customer population. In ei-ther case, the term “Results” always applies to improving well-beingoutcomes in communities or customers (“Is anyone better off?”).Figure 6 depicts the connection between population (shared) account-ability and program performance (direct) accountability.

leadership is getting results in a way that builds trust 6
Results-Based Accountability is a powerful, community-centered,data-driven, continuous quality improvement method with the fol-lowing special features:
Figure 6: In the RBA framework,Program Performance and DirectAccountability contribute to PopulationResults and Shared Accountability(Source: Friedman book)
• Designed for public sector and non-profit agencies who are mis-sion and results driven
• Designed for engaging and empowering community stakeholdersto tackle complex social problems
• Focused on Results, which is defined as improving communityand/or client well-being
• Starts with ENDS (results), and uses data and community voice, todevelop and implement MEANS (strategy and action plan)
• Distinguishes between shared accountability with partners vs.direct accountability for our program performance
• Contains comprehensive approach to selecting community out-come indicators and program performance measures
• Built on the empirical sciences of epidemiology and quality im-provement
• All the materials are free for use by governments and non-profits
RBA complements emerging and powerful approaches such asCollective Impact that has been popularized by inspiring colleaguesat FSG (http://www.fsg.org/).
Appendix B—Authentic Transformational Leadership
For leadership development there are many good models,7 programs, 7 Roger Gill. Theory and Practice ofLeadership. SAGE Publications Ltd,second edition edition, 1 2012. ISBN9781849200240
and consultants—and it can be very confusing! From our experiencesat the SFDPH, we have come to appreciate that relationships play ahuge and central role! In contrast to individual development, for or-ganizational development, learning, and performance improvement,a leadership development model should have the following strengths:
• Emphasis on relationships
• Based on extensive research
• Available validated tools for assessment and development
• Inclusion of method for spread throughout the organization
• Implementable and sustainable at low costs
• Practical and common sense to implement
Based on these criteria, we are adapting—as our core foundation—authentic transformational leadership (ATL).8 ATL is an extension of 8 John J. Sosik and Dongil (Don) Jung.
Full Range Leadership Development:Pathways for People, Profit and Planet.Psychology Press, 1 edition, 9 2009.ISBN 9781848728066
transformational leadership.

leadership is getting results in a way that builds trust 7
Transformational leadership
Transformational leaders are those who transform their followers into becom-ing leaders themselves.
From mindgarden.com: “Transformational leadership is a lead-ership approach that is defined as leadership that creates valuableand positive change in the followers. A transformational leader fo-cuses on ‘transforming’ others to help each other, to look out for eachother, to be encouraging and harmonious, and to look out for theorganization as a whole. In this leadership, the leader enhances themotivation, morale and performance of his follower group.”
“Transformational leaders are those who stimulate and inspirefollowers to both achieve extraordinary outcomes and, in the process,develop their own leadership capacity. Transformational leaders helpfollowers grow and develop into leaders by responding to individualfollowers’ needs by empowering them and by aligning the objectivesand goals of the individual followers, the leader, the group, and thelarger organization. . . . ”
We can identify transformational leaders by what they do (behav-iors) and who they are (character strengths). Here is our summary ofwhat transformational leaders do:
1. Be an exemplary role model (Idealized Influence)
2. Motivate through inspiration (Inspirational Motivation)
3. Promote innovative thinking (Intellectual Stimulation)
4. Mentor and coach your staff (Individualized Consideration)
Transformational leadership is critical for health organizations!The work of health professionals is knowledge-based and requireshigh educational attainment, experience, problem-solving, creativity,and innovation. The work of health professionals is also trust-basedand requires high ethical/moral standards and behaviors. Also,health professionals train and practice within mentor-mentee rela-tionships. Given all the above, extrinsic motivation (via contingentrewards) is insufficient—we need the 4 Is of transformational leader-ship
Authentic leadership—Role of character strengths
Now that we know “what they do,” we must learn what ideal char-acter strengths define “who they are.” When our TL behaviors alignwith our character strengths and our character strengths are vir-tuous, then we are authentic transformational leaders.9 “Virtues 9 John J Sosik. Leading with Character:
Stories of Valor and Virtue and the Princi-ples They Teach (PB). Information AgePublishing, 7 2006. ISBN 9781593115418
are core characteristics universally valued by moral philosophersand religious thinkers as exemplars of good character. . . . Character

leadership is getting results in a way that builds trust 8
strengths are positive traits or psychological processes or mechanismsfor displaying the virtues. For example, love of learning is a characterstrength that reflects the virtue of wisdom.”
Peterson and Seligman10 (pioneers in positive psychology) have 10 Christopher Peterson and MartinSeligman. Character Strengths andVirtues: A Handbook and Classification.Oxford University Press, 1st edition,2004.
identified 24 character strengths, clustered within six virtues, that areassociated with positive personal qualities and beneficial outcomes.These “Virtues in Action” are the foundation of authentic transforma-tional leadership (Table 2):
Virtue Character strengths
Wisdom & knowledge Creativity, curiosity, open-mindedness, love of learning, and perspectiveCourage Bravery, persistence, integrity, and vitalityHumanity Love, kindness, and social intelligenceJustice Citizenship, fairness, and leadershipTemperance Forgiveness and mercy, humility/modesty, prudence, and self-regulation/controlTranscendence Appreciation of beauty and excellence, gratitude, hope, humor, and spirituality
Table 2: Virtues In Action Model
Authentic leadership is measured by the following domains:
• Self Awareness: To what degree is the leader aware of his or herstrengths, limitations, how others see him or her and how theleader impacts others?
• Transparency: To what degree does the leader reinforce a level ofopenness with others that provides them with an opportunity tobe forthcoming with their ideas, challenges and opinions?
• Ethical/Moral: To what degree does the leader set a high standardfor moral and ethical conduct?
• Balanced Processing: To what degree does the leader solicit suf-ficient opinions and viewpoints prior to making important deci-sions?
360 evaluations and leadership development To date, we have been verydissatisfied with the leadership 360 evaluations we have evaluated.Fortunately, the Full Range Leadership Development model11 has 11 John J. Sosik and Dongil (Don) Jung.
Full Range Leadership Development:Pathways for People, Profit and Planet.Psychology Press, 1 edition, 9 2009.ISBN 9781848728066
been extensively studied with the Multifactor Leadership Question-naire. MLQ is used for 360 evaluations and leadership developmentplans. The short form has only 45 items and takes 15 minutes to com-plete! The MLQ and the Authentic Leadership Questionnaire areboth available at http://www.mindgarden.com.
Appendix C—Attachments (6)

OUR MISSION
OUR VISION
Drawing upon community wisdom and science, we support, develop, implement evidence-based policies, practices, and partnerships that protect and promote health, prevent disease and injury, and create sustainable environments and resilient communities.
To be a community-centered leader in public health practice and innovation.
POPULATION HEALTH DIVISION SAN FRANCISCO DEPARTMENT OF PUBLIC HEALTH
TRANSFORMING PUBLIC HEALTH IN SAN FRANCISCO
ASS
UR
AN
CE
GO
VER
NA
NC
E,
AD
MIN
ISTR
ATI
ON
, AN
D
SYST
EMS
MA
NA
GEM
ENT
4. Assurance of healthy places and healthy people
GOAL 4: Lead public health systems efforts to ensure healthy people and healthy places OBJECTIVES: • 4.1 Establish community-centered approaches that address the social determinants of health and increase
population well-being. • 4.2 Sustain and improve the infrastructure and capacity to support core public health functions, including
legally mandated public health activities. 5. Sustainable funding and maximize collective resources
GOAL 5: Increase administrative, financial and human resources efficiencies within the division. OBJECTIVES: • 5.1 Establish a centralized business office for the division. • 5.2 Appropriately address the human resource issues regarding civil service and contract employees. • 5.3 Establish a centralized grants management and development system for the division.
6. Learning organization with a culture of trust and innovation.
GOAL 6: Build a division-wide learning environment that supports public health efforts. OBJECTIVE: • 6.1 Establish a division-wide Workforce Development program.
ASS
ESSM
ENT
/ R
ESEA
RC
H
1. Superb knowledge management systems and empowered users
GOAL 1 : Build an integrated information and knowledge management infrastructure that enables us to monitor health, to inform and guide activities, and to improve staff and systems performance. OBJECTIVES: • 1.1.Build a strong, highly functional information technology (IT) and technical assistance infrastructure in
alignment with Department of Public Health IT strategy. • 1.2 Establish a highly functional, integrated infectious disease system to collect and report data, and to deliver
and monitor public health actions.
2. Assessment and research aligned with our vision and priorities
GOAL 2: Integrate, innovate, improve, and expand efforts in community and environmental assessments, research, and translation. OBJECTIVES: • 2.1 Create an action plan that supports division priorities. • 2.2 Build cross-section interdisciplinary teams to improve health outcomes and programmatic activities.
PO
LIC
Y D
EVEL
OP
MEN
T
3. Policy development with collective impact
GOAL 3: Conduct effective policy & planning that achieves collective impact to improve health and well-being for all San Franciscans. OBJECTIVES: • 3.1 Establish a division-wide Performance Management, Equity & Quality Improvement Program. • 3.2 Establish systems and partnerships to achieve and maintain Public Health Accreditation. • 3.3 Develop a prioritized legislative agenda and strategic implementation plan to address health status and
inequities.
PU
BLI
C H
EALT
H A
CC
RED
ITA
TIO
N (
PH
A)
DO
MA
INS
CA
TEG
OR
IES
STRATEGIC DIRECTIONS GOALS AND OBJECTIVES 2012-2015

DPH
Com
munit
yH
ealt
h P
rog
ram
s-
MC
AH
**-
CO
PC
- C
BH
S-
HU
H
SF
Genera
l H
osp
.La
gund
a H
ond
aH
osp
ital
CO
MM
UN
ITY
OR
GA
NIZ
ATIO
NS
- K
ais
er
Perm
.,-
UC
SF
/ S
FSU
- S
F Pla
nnin
g,
DC
YF,
MTA
, etc
.
DIS
AS
TER
S-
- -
Em
erg
ency
Pre
pare
dness
and
Med
ical
Serv
ices
HEA
LTH
Y P
LAC
ES
- -
-Envir
onm
enta
lH
ealt
h P
rote
ctio
n,
Eq
uit
y,
and
Sust
ain
ab
ility
HEA
LTH
Y P
EO
PLE
- -
-C
om
munit
yH
ealt
h P
rom
oti
on
DIS
EA
SES
- -
-D
isease
Pre
venti
on
and
Contr
ol
Hig
h p
riori
ty,
inte
rdis
cip
linary
, cr
oss
-bra
nch
init
iati
ves,
pro
gra
ms,
task
forc
es,
team
s, p
roje
cts,
etc
.
STR
ATEG
IC A
LIG
NM
EN
T: P
ub
lic H
ealt
h A
ccre
dit
ati
on, Eq
uit
y,
and
Qualit
y Im
pro
vem
ent
OPER
ATIO
NS
FO
CU
S:
Op
era
tions,
Fin
ance
, and
Gra
nts
Manag
em
ent
Exam
ple
s: H
IV/S
TD
Pre
venti
on, C
om
munit
y H
ealt
h Im
pro
vem
ent
Pla
n,
Afr
ican A
meri
can H
ealt
h Init
iati
ve,
etc
.
Hig
h-p
riori
ty init
iati
ves
may b
e led
or
coord
inate
d b
y a
PH
D B
ranch
, co
mm
unit
y p
art
ner,
or
com
munit
y c
oalit
ion.
PR
OFE
SS
ION
AL
DEV
ELO
PM
EN
T: C
ente
r fo
r Le
arn
ing
and
Innovati
on
Pop
ula
tion H
ealt
h D
ivis
ion (
PH
D)
**M
CA
H =
Mate
rnal, C
hild
& A
dole
scent
Healt
h;
CO
PC
= C
om
m.
Ori
ente
d P
rim
ary
Care
; C
BH
S =
Com
m.
Behavio
rial H
ealt
h S
erv
ices;
HU
H =
Housi
ng
and
Urb
an H
ealt
h;
DC
YF
=
Dep
t of
Child
ren,
Youth
, &
their
Fam
ilies;
MTA
=M
uni. T
ransp
ort
ati
on A
gency
; S
FSU
= S
F S
tate
Univ
ers
ity;
Vers
ion 2
01
3.0
3.1
1
KN
OW
LED
GE M
AN
AG
EM
EN
T &
DIS
CO
VERY:
AR
CH
ES
*, C
PH
R, and
Bri
dg
eH
IV
PH
Acc
redit
ati
on
Dom
ain
Cate
gori
es
Ass
ess
ment
Ass
ura
nce
Polic
y D
evelo
pm
ent
Govern
ance
, A
dm
inis
trati
on,
& S
yst
em
s M
anag
em
ent
* A
RC
HES
= A
pp
lied
Rese
arc
h,
Com
munit
y H
ealt
h E
pid
em
iolo
gy,
and
Surv
eill
ance
; C
PH
R =
Cente
r fo
r Pub
lic H
ealt
h R
ese
arc
h
Pop
ula
tion H
ealt
h D
ivis
ion (
PH
D)
Org
aniz
ati
on D
esi
gn
Up
date
d 2
01
3-0
3-1
4
Ap
plie
d R
ese
arc
h,
Com
munit
yH
ealt
h E
pid
em
iolo
gy,
& S
urv
eill
ance
Kyle
Bern
stein
, PhD
, S
cM
Pub
lic H
ealt
h A
ccre
dit
ati
on,
Eq
uit
y,
and
Qualit
y Im
pro
vem
ent
Isra
el N
ieves-
Riv
era
Envir
onm
enta
l H
ealt
h P
rote
ctio
n,
Eq
uit
y,
and
Sust
ain
ab
ility
Rajiv
Bhati
a,
MD
, M
PH
Com
munit
y H
ealt
h P
rom
oti
on
Trace
y P
ack
er,
MPH
Dis
ease
Pre
venti
on a
nd
Contr
ol
Susa
n P
hili
p,
MD
, M
PH
Cente
r fo
r Le
arn
ing
& Innovati
on
Jonath
an F
uch
s, M
D,
MPH
Pub
lic H
ealt
h E
merg
ency
Pre
pare
dness
and
Resp
onse
Naveena B
ob
ba, M
D
Dep
art
ment
of
Pub
lic H
ealt
hB
arb
ara
A.
Garc
ia,
MPA
Dir
ect
or
of
Healt
h
Em
erg
ency
Med
ical S
erv
ices
John B
row
n,
MD
Cente
r fo
r Pub
lic H
ealt
h R
ese
arc
hW
illi M
cFarl
and
, M
D,
PhD
, M
PH
&TM
Op
era
tions,
Fin
ance
, and
Gra
nts
Manag
em
ent
Chri
stin
e S
iad
or,
MPH
Pop
ula
tion H
ealt
h D
ivis
ion (
PH
D)
Tom
ás
J. A
rag
ón,
MD
, D
rPH
Healt
h Offi
cer
& D
irect
or
DPH
Polic
y a
nd
Pla
nnin
g,
Colle
en C
haw
la,
MPA
Dir
ect
or
AS
SES
SM
EN
T /
RES
EA
RC
H
PO
LIC
Y D
EV
ELO
PM
EN
T
AS
SU
RA
NC
E
Govern
ance
, A
dm
inis
trati
on,
and
Syst
em
s M
anag
em
ent
Public
Healt
hA
ccre
dit
ati
on D
om
ain
s
Bri
dg
eH
IV (
Rese
arc
h)
Susa
n B
uch
bin
der,
MD
Popula
tion H
ealt
h D
ivis
ion (
PH
D)
Org
aniz
ati
on C
hart
Update
d 2
01
3-0
3-1
4

Equi
ty
MED
ICA
L CA
RE S
YSTE
MS
PUBL
IC H
EALT
H S
YSTE
MS
Hea
lth
Prot
ecti
onH
ealt
h Pr
omot
ion
Dis
ease
& I
njur
y Pr
even
tion
Dis
aste
r Pr
epar
edne
ss
Soci
oeco
nom
icFa
ctor
s
Ups
trea
mFa
ctor
sIn
divi
dual
/ H
ouse
hold
/ F
amily
Com
mun
ity
Fact
ors
Inte
rmed
iate
Out
com
esSt
ates
of
Hea
lth
Qua
lity
ofLi
fe
Phys
ical
Envi
ronm
ent
Beha
vior
alFa
ctor
s
Gene
tic
Endo
wmen
t
Spir
itua
lity
Phys
iolo
gic
Fact
ors
Resi
lienc
e
Dis
ease
and
Inju
ry
Hea
lth
and
Func
tion
Mor
talit
y
Wel
l-Bei
ng
INTE
RVEN
TIO
NS
Inst
itut
e fo
r H
ealt
hcar
e Im
prov
emen
t (I
HI)
Pop
ulat
ion
Hea
lth
Com
posi
te M
odel
*Po
pula
tion
Hea
lth
Div
isio
n, S
an F
ranc
isco
Dep
artm
ent
Publ
ic H
ealt
h
Tom
ás J
Ara
gón,
MD
, DrP
H, H
ealt
h O
ffic
er, V
. 201
3-07
-31
Life
Cou
rse
Proc
esse
s
* Fo
r a
spec
ifie
d po
pula
tion
, the
"po
pula
tion
hea
lth"
app
roac
h is
a s
yste
ms
fram
ewor
k fo
r st
udyi
ng a
nd im
prov
ing
the
dist
ribu
tion
of
heal
th a
nd q
ualit
y of
life
sta
tes
(wel
l-bei
ng, h
ealt
h an
d fu
ncti
on, m
orta
lity,
dis
ease
, and
inju
ry)
and
thei
r de
term
inan
ts (s
ocio
econ
omic
, env
iron
men
tal,
life
cour
se p
roce
ss, b
ehav
iora
l, re
silie
nce,
etc
.) th
roug
hco
llabo
rati
ve, s
usta
inab
le, i
mpa
ctfu
l sol
utio
ns (e
.g.,
colle
ctiv
e im
pact
, hea
lth
in a
ll po
licie
s).
IHI
Mod
el a
dapt
ed f
rom
Sto
to, M
. A. P
opul
atio
n H
ealt
h in
the
Aff
orda
ble
Care
Act
Era
, Aca
dem
y H
ealt
h, 2
013

2St
rate
gic
Plan
ning
6O
pera
tion
sFo
cus
3Cu
stom
erFo
cus
5W
orkf
orce
Focu
s
Lead
ersh
ip
+
E
xecu
tion
->
Re
sult
s
Infl
uenc
ed b
y CH
ALL
ENGE
S an
d O
PPO
RTU
NIT
IES
Guid
ed b
y ST
RATE
GY a
nd A
CTIO
N P
LAN
S
4M
easu
rem
ent,
Ana
lysi
s, a
nd K
nowl
edge
Man
agem
ent
Supp
orte
d by
VA
LUES
:Vi
sion
ary
lead
ersh
ip *
Cus
tom
er-d
rive
n ex
celle
nce
Org
aniz
atio
nal a
nd p
erso
nal l
earn
ing
* Va
luin
g wo
rkfo
rce
and
part
ners
Agi
lity
* Fo
cus
on t
he f
utur
e *
Man
agin
g fo
r in
nova
tion
Man
agem
ent
by f
act
* So
ciet
al r
espo
nsib
ility
Focu
s on
res
ults
and
cre
atin
g va
lue
* Sy
stem
s pe
rspe
ctiv
e
1LE
AD
ERSH
IP7
RESU
LTS
Clie
nt H
ealt
h &
Wel
l-bei
ng (R
esul
t)Pr
ogra
m P
erfo
rman
ce (E
ffor
t)
Com
Hea
lth
goal
sEf
fect
ive
stra
tegi
esPr
ogra
mro
les
Perf
orm
ance
goal
sPe
rfor
man
cem
easu
res
Perf
orm
ance
stan
dard
s
Goal 1
Stra
tegy
1Ro
le 1
Stra
tegy
2
Stra
tegy
3
Goal 1
Goal 2
Goal 3
Role
2
Role
3
Mea
sure
1
Mea
sure
6
Mea
sure
5
Mea
sure
4
Mea
sure
3
Mea
sure
2
Stan
dard
1
Stan
dard
6
Stan
dard
5
Stan
dard
4
Stan
dard
3
Stan
dard
2(n
one)
Perf
orm
ance
Exc
elle
nce
Usi
ng B
aldr
ige
Crit
eria
& R
esul
ts-B
ased
Acc
ount
abili
tyPo
pula
tion
Hea
lth
Div
isio
n, S
FDPH
Bald
rige
Cri
teri
a fo
r Pe
rfor
man
ce E
xcel
lenc
eRe
sult
s-Ba
sed
Acc
ount
abili
ty:
A P
opul
atio
n H
ealt
h A
ppro
ach
Shar
edA
ccou
ntab
ility
Publ
ic H
ealt
hM
issi
on &
Vis
ion
Dir
ect
Acc
ount
abili
ty
1. Ba
ldri
ge P
erfo
rman
ce E
xcel
lenc
e Pr
ogra
m. 2
013.
201
3–20
14 H
ealt
h Ca
re C
rite
ria
for
Perf
orm
ance
Exc
elle
nce.
Ga
ithe
rsbu
rg, M
D: U
.S. D
epar
tmen
t of
Com
mer
ce, N
atio
nal I
nsti
tute
of
Stan
dard
s an
d Te
chno
logy
. htt
p://
www.
nist
.gov
/bal
drig
e.2.
Ins
ight
to
Perf
orm
ance
Exc
elle
nce
2013
-201
4: U
nder
stan
ding
the
Int
egra
ted
Man
agem
ent
Syst
em a
nd t
he B
aldr
ige
Crit
eria
, by
Mar
k Bl
azey
, ASQ
Qua
lity
Pres
s, 2
013
3. T
ryin
g H
ard
is N
ot G
ood
Enou
gh: H
ow t
o Pr
oduc
e M
easu
rabl
e Im
prov
emen
ts f
or C
usto
mer
s an
d Co
mm
unit
ies,
by
Mar
k Fr
iedm
an, T
raff
ord
Publ
ishi
ng, 2
005
4. Q
ualit
y Im
prov
emen
t Ex
peri
ence
in a
Hig
h-Pe
rfor
min
g Lo
cal H
ealt
h D
epar
tmen
t, b
y Je
ffre
y D
. Gun
zenh
ause
r, e
t al
. J P
ublic
Hea
lth
Man
agem
ent
Prac
tice
, 201
0, 1
6(1)
, 39–
48
3, 4
1, 2
Tom
ás J
. Ara
gón,
MD
, DrP
HH
ealt
h O
ffic
er, V
. 201
3-07
-30
"Lea
ders
hip
is g
etti
ng r
esul
ts in
a w
ay t
hat
insp
ires
tru
st."
Com
mun
ity
Hea
lth
& W
ell-b
eing
(Res
ult)
Colle
ctiv
e Pe
rfor
man
ce (E
ffor
t)
Indi
cato
rs
Goal 2
THEM
ES &
PRA
CTIC
ES>>
Vis
ion
(des
ired
fut
ure
stat
e)>>
Pur
pose
(why
)>>
Val
ues
(why
)>>
Str
ateg
y (h
ow)
>> E
mpo
werm
ent
(who
)>>
Eng
agem
ent
(who
)
Full
Rang
e Le
ader
ship
Dev
elop
men
t M
odel
TRA
NSF
ORM
ATI
ON
AL
LEA
DER
SHIP
>> B
e an
exe
mpl
ary
role
mod
el (i
deal
ized
infl
uenc
e)>>
Mot
ivat
e th
roug
h in
spir
atio
n (in
spir
atio
nal m
otiv
atio
n)>>
Pro
mot
e in
nova
tive
thi
nkin
g (in
telle
ctua
l sti
mul
atio
n)>>
Coa
ch a
nd m
ento
r st
aff
(indi
vidu
aliz
ed c
onsi
dera
tin)
TRA
NSA
CTIO
NA
L LE
AD
ERSH
IP>>
Con
ting
ent
Rewa
rd
CORR
ECTI
VE L
EAD
ERSH
IP>>
Man
agem
ent-
By-E
xcep
tion
(MBE
) --
Act
ive
>> M
anag
emen
t-By
-Exc
epti
on (M
BE) -
- Pa
ssiv
e
MU
LTIP
LE I
NTE
LLIG
ENCE
S>>
Cog
niti
ve>>
Em
otio
nal
>> B
ehav
iora
l-
- -
- -
- -
- -
>> E
thic
al /
Mor
al>>
Soc
ial
>> C
ultu
ral
>> S
piri
tual
RESU
LTS-
BASE
D A
CCO
UN
TABI
LITY
A
Pop
ulat
ion
Hea
lth
App
roac
h-
Com
mun
ity
Hea
lth
& Cl
ient
Hea
lth
- Co
llect
ive
& Pr
ogra
m P
erfo
rman
ce-
Shar
ed &
Dir
ect
Acc
ount
abili
ty
[Pu
rpos
e]
The
Lead
ersh
ip C
heat
shee
t --
Res
ults
-Bas
ed, A
uthe
ntic
Tra
nsfo
rmat
iona
l Lea
ders
hip
(RB-
ATL
)
RELA
TIO
NSH
IPS
[Peo
ple]
"Tra
nsfo
rmat
iona
l lea
ders
are
tho
sewh
o tr
ansf
orm
the
ir f
ollo
wers
into
beco
min
g le
ader
s th
emse
lves
."
"Lea
ders
hip
is g
etti
ng r
esul
tsin
a w
ay t
hat
insp
ires
tru
st."
"Whe
n 'w
hat
you
do'
alig
ns w
ith
'who
you
are
'yo
u ar
e an
aut
hent
ic le
ader
."
+LE
ADER
SHIP
EXEC
UTI
ON
RESU
LTS
Wha
t yo
u D
O[P
roce
ss]
Virt
ues
in A
ctio
n M
odel
:1
Crea
tivi
ty, c
urio
sity
, ope
n-m
inde
dnes
s, lo
ve o
f le
arni
ng, a
nd p
ersp
ecti
ve2
Brav
ery,
per
sist
ence
, int
egri
ty, a
nd v
ital
ity
3 Lo
ve, k
indn
ess,
and
soc
ial i
ntel
ligen
ce4
Citi
zens
hip,
and
fai
rnes
s5
Forg
iven
ess
and
mer
cy, p
rude
nce,
hum
ility
/mod
esty
, and
sel
f-re
gula
tion
/con
trol
6 A
ppre
ciat
ion
of b
eaut
y an
d ex
celle
nce,
gra
titu
de, h
ope,
hum
or, a
nd s
piri
tual
ity
CHA
RACT
ER S
TREN
GTH
S>>
Wis
dom
& K
nowl
edge
(1)
>> C
oura
ge (2
)>>
Hum
anit
y (3
)>>
Jus
tice
(4)
>> T
empe
ranc
e (5
)>>
Tra
nsce
nden
ce (6
)
LEA
DER
[Per
sona
l]W
ho y
ou A
RE[P
erso
nal]
MA
NA
GEM
ENT
>> T
eam
bui
ldin
g &
perf
orm
ance
>> M
ulti
-Cri
teri
a D
ecis
ion
Mak
ing
>> S
trat
egic
Pro
ject
Man
agem
ent
>> E
quit
y &
Qua
lity
Impr
ovem
ent
>> P
erfo
rman
ce m
anag
emen
t sy
stem
s
Tom
ás J
. Ara
gón,
MD
, DrP
H, H
ealt
h O
ffic
er, V
. 201
3-08
-14
San
Fran
cisc
o D
epar
tmen
t of
Pub
lic H
ealt
h
Bibl
iogr
aphy
:-
The
Theo
ry a
nd P
ract
ice
of L
eade
rshi
p. b
y Ro
ger
Gill,
SA
GE P
ublic
atio
ns (2
012)
, 2nd
Ed.
- Tr
ansf
orm
atio
nal L
eade
rshi
p, b
y Ro
nald
Rig
gio
& Be
rnar
d Ba
ss, P
sych
olog
y Pr
ess
(201
2), 2
nd E
d.-
Full
Rang
e Le
ader
ship
Dev
elop
men
t: P
athw
ays
for
Peop
le, P
rofi
t, a
nd P
lane
t, b
y Jo
hn S
osik
, Psy
chol
ogy
Pres
s (2
012)
"Lea
ders
hip
is s
howi
ng t
he w
ay, a
nd h
elpi
ng o
r in
duci
ng o
ther
sto
pur
sue
it. T
his
enta
ils e
nvis
ioni
ng a
des
irab
le f
utur
e, p
rom
otin
ga
clea
r pu
rpos
e or
mis
sion
, sup
port
ive
valu
es a
nd in
telli
gent
stra
tegi
es, a
nd e
mpo
weri
ng a
nd e
ngag
ing
all t
hose
con
cern
ed."








![cooltech club presentation.ppt [Read-Only] · Continuous integration, unbreakable daily builds, build results and log archive, remote multiplatform builds Rudimentary Continuous integration](https://static.fdocuments.in/doc/165x107/603632e051782f187730642a/cooltech-club-read-only-continuous-integration-unbreakable-daily-builds-build.jpg)









