Lateropulsion Due to a Lesion of the Dorsal ...
3
Abstract We report three cases showing body lateropulsion as the sole or predominant symptom of caudal lateral medullary infarction. All of them presented a small in- farction on the lateral surface of the caudal medulla cor- responding to the dorsal spinocerebellar tract (DSCT). Disturbed unconscious proprioception of the lower trunk and the lower limb conveyed by the DSCT might have been responsible for the isolated lateropulsion. Although lateropulsion itself improved within two weeks, one pa- tient’s condition progressed to typical lateral medullary infarction. Lateropulsion caused by DSCT infarction could be a prodromal symptom of perfusion failure of a vertebral artery or the posterior inferior cerebellar artery. (Internal Medicine 44: 1295–1297, 2005) Key words: medulla oblongata, gait ataxia, infarction, poste- rior spinocerebellar tract Introduction Lateropulsion is known to be one of the symptoms of lat- eral medullary infarctions (LMIs). Although it is usually as- sociated with ipsilateral Horner syndrome, ipsilateral limb ataxia, superficial sensory disturbance of the ipsilateral face and contralateral limbs, dysarthria, dysphagia, and vertigo, isolated body lateropulsion is rare. Although the lesion re- sponsible for lateropulsion is controversial (1), recent studies (2–4) have identified possible corresponding lesions for lateropulsion. Here, we present three cases of caudal LMIs in which lateropulsion was the sole or predominant manifesta- tion. Although lateropulsion due to LMIs is reported to im- prove within a few weeks (4), the condition of one of our patients progressed to typical Wallenberg syndrome. Case Report Case 1 A 78-year-old woman noted acute lateropulsion to the right on June 16, 2002. She had diabetes mellitus and angina pectoris. On examination, there was no vertigo, nystagmus, hearing deficit, dysarthria, dysphagia, deficit in either super- ficial or deep sensation, ophthalmoplegia, Horner syndrome, hemiparesis, or limb ataxia. Magnetic resonance imaging (MRI) showed a fresh small infarction selectively involving the right superficial lateral portion of the caudal medulla (Fig. 1A). MR angiography showed stenosis of the right ver- tebral artery. Her symptom slowly resolved within two weeks. Case 2 A 76-year-old man experienced lateropulsion to the right on January 9, 2003. He was receiving medication for hyper- tension. He showed no vertigo, nystagmus, hearing loss, dysarthria, dysphagia, sensory loss, ophthalmoplegia, Horner syndrome, or hemiparesis. MRI showed a fresh small infarc- tion situated in the same position as in Case 1 (Fig. 1B). MR angiography showed weak flow in the vertebral arteries. Three days later, vomiting, decreased temperature sensation on the right face and the left limbs and trunk, and right Horner syndrome appeared abruptly. MRI revealed expan- sion of the infarct area (Fig. 1C). The lateropulsion itself im- proved within two weeks. Case 3 An 84-year-old man presented with acute onset of veering of his body to the right on February 20, 2004. He was receiv- ing medication for hypertension and diabetes mellitus. He did not have vertigo, nausea, or tinnitus, nor did he have hoarseness, dysphagia, or dysarthria. There was no ophthal- moplegia, Horner syndrome, limb ataxia, or hemiparesis. Pain and thermal sensations were decreased on his right face and over the contralateral side of his body. MRI showed a Internal Medicine Vol. 44, No. 12 (December 2005) 1295 Lateropulsion Due to a Lesion of the Dorsal Spinocerebellar Tract Kengo MAEDA, Michiko SAIKYO, Atsushi MUKOSE, Hirotaka TOMIMATSU and Hitoshi YASUDA □ CASE REPORT □ From the Division of Neurology, Department of Medicine, Shiga University of Medical Science, Otsu Received for publication April 22, 2005; Accepted for publication August 31, 2005 Reprint requests should be addressed to Dr. Kengo Maeda, the Division of Neurology, Department of Medicine, Shiga University of Medical Science, Seta- Tsukinowa-cho Otsu, Shiga 520-2192
Transcript of Lateropulsion Due to a Lesion of the Dorsal ...

Abstract
We report three cases showing body lateropulsion asthe sole or predominant symptom of caudal lateralmedullary infarction. All of them presented a small in-farction on the lateral surface of the caudal medulla cor-responding to the dorsal spinocerebellar tract (DSCT).Disturbed unconscious proprioception of the lower trunkand the lower limb conveyed by the DSCT might havebeen responsible for the isolated lateropulsion. Althoughlateropulsion itself improved within two weeks, one pa-tient’s condition progressed to typical lateral medullaryinfarction. Lateropulsion caused by DSCT infarctioncould be a prodromal symptom of perfusion failure of avertebral artery or the posterior inferior cerebellarartery.(Internal Medicine 44: 1295–1297, 2005)
Key words: medulla oblongata, gait ataxia, infarction, poste-rior spinocerebellar tract
Introduction
Lateropulsion is known to be one of the symptoms of lat-eral medullary infarctions (LMIs). Although it is usually as-sociated with ipsilateral Horner syndrome, ipsilateral limbataxia, superficial sensory disturbance of the ipsilateral faceand contralateral limbs, dysarthria, dysphagia, and vertigo,isolated body lateropulsion is rare. Although the lesion re-sponsible for lateropulsion is controversial (1), recent studies(2–4) have identified possible corresponding lesions forlateropulsion. Here, we present three cases of caudal LMIs inwhich lateropulsion was the sole or predominant manifesta-tion. Although lateropulsion due to LMIs is reported to im-prove within a few weeks (4), the condition of one of ourpatients progressed to typical Wallenberg syndrome.
Case Report
Case 1A 78-year-old woman noted acute lateropulsion to the
right on June 16, 2002. She had diabetes mellitus and anginapectoris. On examination, there was no vertigo, nystagmus,hearing deficit, dysarthria, dysphagia, deficit in either super-ficial or deep sensation, ophthalmoplegia, Horner syndrome,hemiparesis, or limb ataxia. Magnetic resonance imaging(MRI) showed a fresh small infarction selectively involvingthe right superficial lateral portion of the caudal medulla(Fig. 1A). MR angiography showed stenosis of the right ver-tebral artery. Her symptom slowly resolved within twoweeks.
Case 2A 76-year-old man experienced lateropulsion to the right
on January 9, 2003. He was receiving medication for hyper-tension. He showed no vertigo, nystagmus, hearing loss,dysarthria, dysphagia, sensory loss, ophthalmoplegia, Hornersyndrome, or hemiparesis. MRI showed a fresh small infarc-tion situated in the same position as in Case 1 (Fig. 1B). MRangiography showed weak flow in the vertebral arteries.Three days later, vomiting, decreased temperature sensationon the right face and the left limbs and trunk, and rightHorner syndrome appeared abruptly. MRI revealed expan-sion of the infarct area (Fig. 1C). The lateropulsion itself im-proved within two weeks.
Case 3An 84-year-old man presented with acute onset of veering
of his body to the right on February 20, 2004. He was receiv-ing medication for hypertension and diabetes mellitus. Hedid not have vertigo, nausea, or tinnitus, nor did he havehoarseness, dysphagia, or dysarthria. There was no ophthal-moplegia, Horner syndrome, limb ataxia, or hemiparesis.Pain and thermal sensations were decreased on his right faceand over the contralateral side of his body. MRI showed a
Internal Medicine Vol. 44, No. 12 (December 2005) 1295
Lateropulsion Due to a Lesion ofthe Dorsal Spinocerebellar Tract
Kengo MAEDA, Michiko SAIKYO, Atsushi MUKOSE, Hirotaka TOMIMATSU and Hitoshi YASUDA
□ CASE REPORT □
From the Division of Neurology, Department of Medicine, Shiga University of Medical Science, OtsuReceived for publication April 22, 2005; Accepted for publication August 31, 2005Reprint requests should be addressed to Dr. Kengo Maeda, the Division of Neurology, Department of Medicine, Shiga University of Medical Science, Seta-
Tsukinowa-cho Otsu, Shiga 520-2192

MAEDA et al
fresh infarction on the right dorsolateral medulla (Fig. 1D).His lateropulsion improved gradually within two weeks.
Discussion
Of 214 consecutive acute stroke patients treated in ourward from April of 2000 to March of 2004, three showedlateropulsion as the sole or predominant symptom of LMIs.Thömke et al recently reported that involvement of the as-cending dorsal spinocerebellar tract (DSCT) and the de-scending lateral vestibulospinal tract (LVST) identified usingthree-dimensional brainstem mapping were associated with
lateropulsion with and without limb ataxia, respectively (2).Since the lesions in the present cases were located on the sur-face of the dorsolateral medulla, they were considered to in-volve the spinocerebellar tract rather than the LVST, whichruns more ventromedially (5). The possibility of ventralspinocerebellar tract (VSCT) involvement may be low be-cause the VSCT conveys the proprioception of the contra-lateral lower limb. The DSCT contains the ascending fiberswhich originate from the ipsilateral column of Clarke, tra-verse the dorsolateral surface of the caudal medulla, enter thecerebellum through the inferior cerebellar peduncle, and ter-minate in the ipsilateral anterior lobe and paramedian lobule
Internal Medicine Vol. 44, No. 12 (December 2005)1296
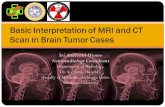
Figure 1. Diffusion-weighted (left) and fluid attenuating inversion recovery (right) images for each of the three cases. A: Case1; B: the initial MRI for Case 2; C: the second MRI for Case 2; D: Case 3. Arrowheads indicate the fresh infarctions.

as mossy fibers. The column of Clarke receives fibers fromthe muscle spindle and the Golgi tendon organ of theipsilateral trunk and lower limb. The DSCT conveys uncon-scious proprioception. In our patients, dysfunction of theDSCT might have given rise to the lateropulsion. The infarc-tion in Case 3 was larger and affected the spinal tract of thetrigeminal nerve and the lateral spinothalamic tract as well asthe DSCT.
Lee and Sohn (3) described a lesion located at the rostralmedulla. They considered the olivocerebellar tract to havebeen responsible for the lateropulsion in their case. TheDSCT and the olivocerebellar tract run close together in therostral medulla. The lesion in their case might have involvedthe DSCT. Recently, Kim et al reported six cases of isolatedlateropulsion caused by infarctions located at the same re-gion as observed in the present cases (4). The lateropulsionitself improved over the subsequent few weeks in their cases(4) as in all of our cases. However, the present Case 2 devel-
oped Wallenberg syndrome, suggesting that lateropulsionmight be a prodromal symptom of typical LMI in some pa-tients.
References
1) Ropper AH, Brown RH. Disorders of stance and gait. in: Adam’s andVictor’s principles of neurology, 8th ed. Foltin J, Nogueira I,Edmonson KG, Sheinis LA, Eds. McGraw-Hill, 2005: 100–108.
2) Thömke F, Marx JJ, Iannetti GD, et al. A topodiagnostic investigationon body lateropulsion in medullary infarcts. Neurology 64: 716–718,2005.
3) Lee H, Sohn CH. Axial lateropulsion as a sole manifestation of lateralmedullary infarction: A clinical variant related to rostral-dorsolaterallesion. Neurol Res 24: 773–774, 2002.
4) Kim SH, Cho YJ, Cho JH, et al. Isolated lateropulsion by a lesion ofthe dorsal spinocerebellar tract. Cerebrovasc Dis 18: 344–345, 2004.
5) Carpenter MB. The Medulla. in: Core text of neuroanatomy, 3rd ed.Tracy TM, Vaughn VM, Vinck W, Eds. Williams & Wilkins,Baltimore, MD 1985: 102–132.
Internal Medicine Vol. 44, No. 12 (December 2005)
Lateropulsion Due to Medullary Infarct
1297