Large Scale Implementation of Patient Decision Aids in an Integrated Group Practice: the Group...
28
Large Scale Implementation of Patient Decision Aids in an Integrated Group Practice: the Group Health Experience David Arterburn, MD, MPH Group Health Research Institute May 25, 2011 “University of Washington SDM Conference - Implementing Shared Decision Making:
-
Upload
baylee-harte -
Category
Documents
-
view
216 -
download
2
Transcript of Large Scale Implementation of Patient Decision Aids in an Integrated Group Practice: the Group...

Large Scale Implementation of Patient Decision Aids in an Integrated Group Practice: the Group Health Experience
David Arterburn, MD, MPHGroup Health Research InstituteMay 25, 2011
“University of Washington SDM Conference - Implementing Shared Decision Making: Lessons from the Front”

About Group HealthGroup Health is an integrated health plan
and care delivery system that provides medical coverage and care to more than 674,900 residents in Washington state and North Idaho.
Nearly two-thirds of members receive care in Group Health-owned/operated medical facilities from Group Health-salaried providers.

Patient-centered care at Group Health
Shared electronic medical record
Medical home pilot
Decision aids for shared decision making
20052005
20072007
20092009
Implementationtimeline 20112011
Evaluation of decision aids continues

Shared decision making research
System-wide implementation
3-year research project
Foundation support

Primary aims of the evaluation
Assess impact on surgery useAssess impact on surgery use
Assess impact on total health care use and costs
Assess impact on total health care use and costs
Estimate ROI from health plan and purchasers’ viewEstimate ROI from health plan and purchasers’ view
Assess process barriers and facilitators
Assess process barriers and facilitators

How did we implement decision aids at Group Health?

Treatment choices in 6 specialty areas
OrthopedicsOrthopedics
CardiologyCardiology
UrologyUrology
Women’s healthWomen’s health
Breast cancerBreast cancer
Back careBack care
1
2
3
4
5
6

12 preference-sensitive conditions
Orthopedics Cardiology Urology
Women’s Health
Breast Cancer Back Care
1. Hip osteoarthritis
2. Knee osteoarthritis
3. Coronary artery disease
4. Benign prostatic hyperplasia
5. Prostate cancer
6. Uterine fibroids
7. Abnormal uterine bleeding
11. Spinal stenosis
12. Herniated disc
8. Early stage9. Ductal
carcinoma in situ
10. Breast reconstruction

Providers can order DAs through Epic

Patient portal access
DVDs can be viewed on the
Web

What have we learned about the use of decision aids at Group Health?

Evaluation
Ordering & viewingOrdering & viewing
Provider interviewsProvider interviews
Patient survey link
Patient survey link

Decision aid distribution (4/11)
Number of videosDistributed, by monthTotal 10, 700

Decision aid distribution (4/11)

Decision aid distribution in Ortho0
100
200
300
Vid
eos
Jan 09 Jul 09 Jan 10 Jul 10 Jan 11Month
Hip Osteoarthritis Knee Osteoarthritis
Orthopedics: Service Line Video Distribution

DA distribution in Women’s Health0
2040
60V
ideo
s
Jan 09 Jul 09 Jan 10 Jul 10 Jan 11Month
Uterine Fibroids Uterine Bleeding
Women's Health: Service Line Video Distribution

DA distribution in Urology0
2040
6080
Vid
eos
Jan 09 Jul 09 Jan 10 Jul 10 Jan 11Month
Enlarged Prostate (BPH) Prostate Cancer
Urology: Service Line Video Distribution

DA distribution for Cardiology0
2040
60V
ideo
s
Jan 09 Jul 09 Jan 10 Jul 10 Jan 11Month
Cardiology: Coronary Artery DiseaseVideo Distribution

DA distribution for Gen Surgery0
510
1520
Vid
eos
Jan 09 Jul 09 Jan 10 Jul 10 Jan 11Month
Early Stage Breast Cancer Breast Reconstruction
DCIS
General Surgery: Service Line Video Distribution

DA distribution for Neurosurgery0
2040
6080
Vid
eos
Jan 09 Jul 09 Jan 10 Jul 10 Jan 11Month
Spinal Stenosis Herniated Disc
Neurosurgery: Service Line Video Distribution

Percentage of procedures for preference sensitive conditions where patient did not receive the video
Fewer missed opportunities

Provider perspectives “It’s almost like you can’t give them too much information. You know? When it
really comes down to it, you need to give people enough information so that they sort of really understand the impact of the decision and all the implications and not just the surgeon’s view.” ~Orthopedics MD
“I don’t have any problem with any kinds of information given to any patients at any time. The more information a patient has, the easier it is for me. Even if it’s wrong, because then they can ask me intelligent questions.” ~Cardio MD
“It’s complicated because you don’t have all the clinical data that you need to make a decision until you’ve taken the angiogram. And there is a strong incentive to deal with it right after you’ve done the angiogram. So, the incentives being: it’s more efficient, it’s more comfortable for the patient, and… if you ask them the question, “Do you want us to just do what we think is best or do you want us to stop and then we can have plenty of time to talk it over later,” they nearly always will tell you, “No, just do what you think is best.” That’s the clear majority view in this.” ~Cardiology MD
“Some patients seem to really appreciate them. Some patients seem really scared after watching the DA and some of the material on there...It really does increase the time I’m spending with them, almost uniformly… It doesn’t save any time at all. And it’s making me run late having to address all the issues the patient has after watching the DA.” ~General Surgery MD
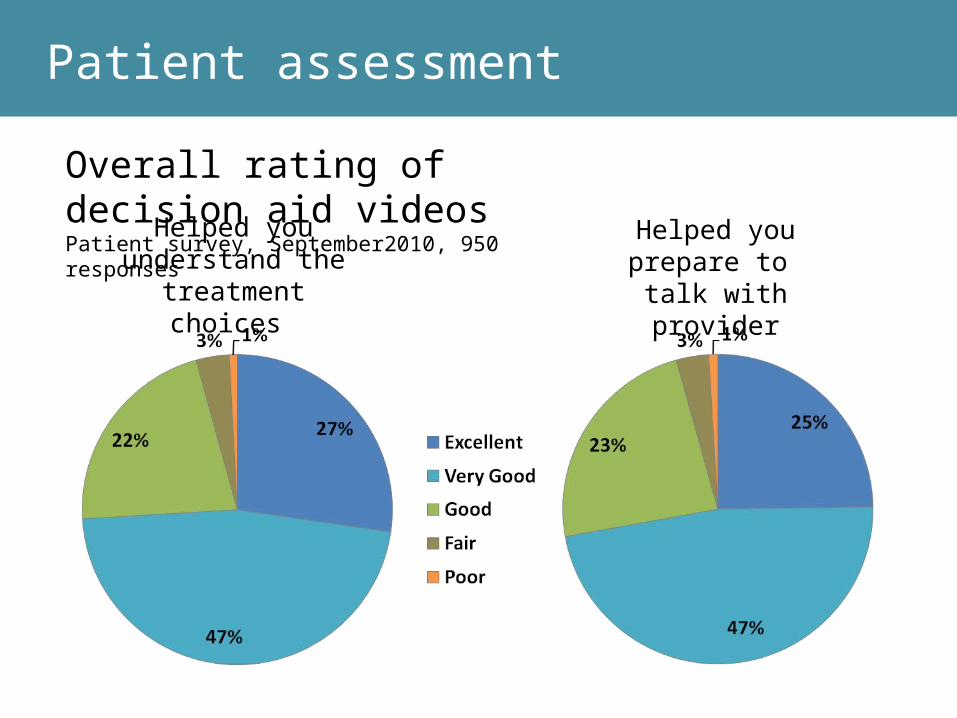
Overall rating of decision aid videosPatient survey, September2010, 950 responses
Helped you understand the treatment choices
Helped you prepare to talk with provider
Patient assessment

Patient assessment
Overall rating of decision aid videosPatient survey, September 2010, 975 responses
How important is it that providers make programs like this available?
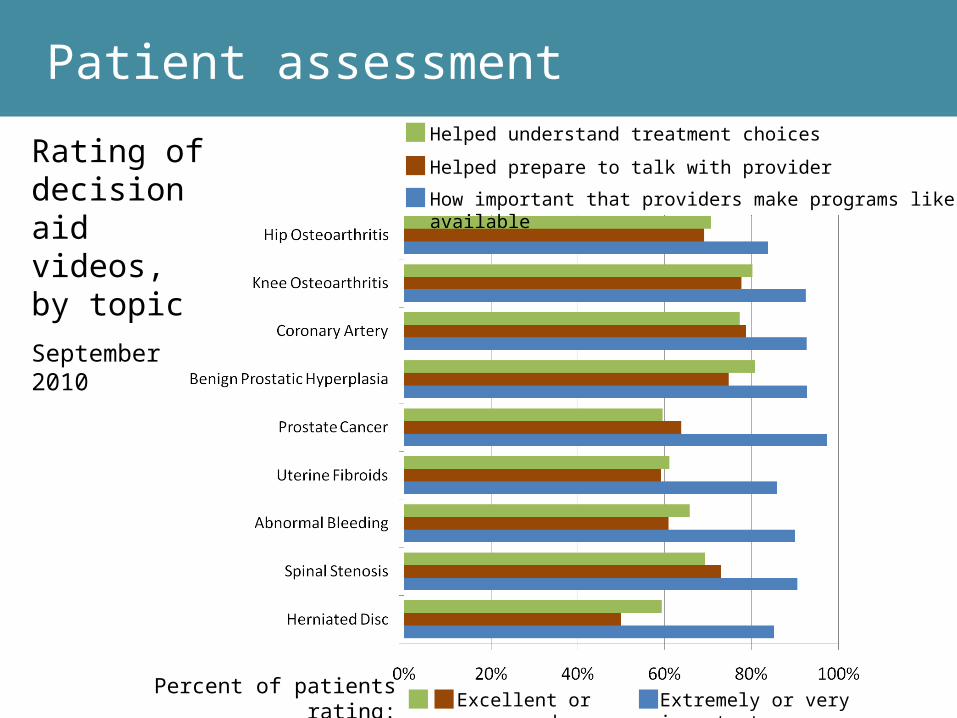
Rating of decision aid videos, by topicSeptember 2010
Patient assessmentHelped understand treatment choices
Helped prepare to talk with provider
How important that providers make programs like this available
Excellent or very good Extremely or very importantPercent of patients rating:

Barriers & FacilitatorsEngaging providers in establishing the implementation
processes is important for buy-in.Overall, the amount of time spent by providers talking
to patients has not changedChanging providers’ practice regarding how they talk
with patients about health care choices and personal values needs to be actively cultivated.
Having a mechanism for pre-visit ordering increases distribution of the DAs and allows for efficient follow up conversations about treatment choices with patients.
Using DAs for conditions that are perceived by patients and/or providers as life threatening is more difficult to implement (e.g., DA for coronary artery disease).

Problems/issues/things to improve…?
Getting the right patient at the right time.Knowing that the patient watched the DA.Knowing that a follow-up conversation took
place.Tracking which patients watched the DA and
decided NOT to have surgery at this time.Getting follow-up with patients at 12mo+ to
check if they were happy with their decision.

Questions?