
LAPORAN KEGIATAN KERJASAMA
63
LAPORAN KEGIATAN KERJASAMA BIDANG : PERTUKARAN MAHASISWA TEMPAT : Internal Medicine-Nephrology, Hospital Clínico, Spain (IFMSA-Spain) – Valencia City, Spain, IFMSA-Spain PERIODE : 01/04/2019 sampai 29/04/2019
Transcript of LAPORAN KEGIATAN KERJASAMA

LAPORAN KEGIATAN KERJASAMA
BIDANG : PERTUKARAN MAHASISWA
TEMPAT : Internal Medicine-Nephrology,
Hospital Clínico, Spain (IFMSA-Spain) – Valencia City,
Spain, IFMSA-Spain
PERIODE : 01/04/2019 sampai 29/04/2019

AF Number 83763
Exchange Contract Information
AF Number 83763
Origin NMO Indonesia (CIMSA-ISMKI)
Exchange is unilateral No
Contract signed 11/10/2018
Personal Student Information
Family name (as written in passport) Suryanto
First name (as written in passport) Nandhan Seftiyan
Sex Male
Date of birth (dd/mm/yyyy) 14/09/1994
Email [email protected]
Alternative Email [email protected]
Acceptance details
Accepted in city/LC Spain (IFMSA-Spain) - Valencia
Accepted at Department of Internal Medicine-Nephrology
Accepted in hospital Hospital Clínico
Accepted start date (dd/mm/yyyy) 01/04/2019
Accepted end date (dd/mm/yyyy)) 29/04/2019
Boarding 1 time(s) per day, at Pocket Money, at the cost of Hosting association
Other Boarding Tickets for take away dish at a restaurant
Lodging At Student flat, at the cost of Hosting association
Other Lodging
Lodging Address Avenida Gaspar Aguilar 9
Social Program Yes
Social Program Information more info soon by email or WhatsApp group
Pocket money No
Pickup Yes “Please contact your contact persons as soon as possible”.
Special remarks Department and/or hospital might still change, we will confirm by email as soon as we know.

AF Number 83763
Contact Person 1
First Name Carla
Last Name Sanchez Hidalgo
Street & Number Av. Blasco Ibanez 17
City Valencia
Post Code 46010
Region
Country Spain
Phone +34 628154377
Cellular +34 963695568
E-mail [email protected]
Role LEO/NEO
Contact Person 2
First Name
Last Name
Street & Number
City
Post Code
Region
Country
Phone
Cellular --
Role
Additional notes
Notes from LEO
Notes from NEO Welcome to your exchange in Valencia! We will send you an email soon with more information :)

AF Number 83763
Exchange Contract Information
AF Number 83763
Origin NMO Indonesia (CIMSA-ISMKI)
Exchange is unilateral No
Contract signed 11/10/2018
Personal Student Information
Family name (as written in passport) Suryanto
First name (as written in passport) Nandhan Seftiyan
Sex Male
Date of birth (dd/mm/yyyy) 14/09/1994
Email [email protected]
Alternative Email [email protected]
Acceptance details
Accepted in city/LC Spain (IFMSA-Spain) - Valencia
Accepted at Department of Internal Medicine-Nephrology
Accepted in hospital Hospital Clínico
Accepted start date (dd/mm/yyyy) 01/04/2019
Accepted end date (dd/mm/yyyy)) 29/04/2019
Arrival details
Do you need pick up by the Hosting Comittee Yes
Arrival date and time 31/03/2019 14:15
Arrival Location Bus station
Flight/Bus/Train number ALSA
Arrival location details Valencia estacion bus
Departure date 30/04/2019
Other details I arrive with with Wiryanti Ambarita, thank you :)
AF Number 83763
Other
Diet No
Do you have any allergies? No
In case of emergency, please contact :
Suryanto / +6282244939300 / [email protected]
Insurance Information
Insurance Company Tokio Marine
Policy Number TM/VOTP/19-V8003672
Contact telephone +625725772
Other comments

IgA
NEPHROPATHY CURRENT TREATMENT
Valencia – April 22th 2019
Nandhan Seftiyan Suryanto
(Wijaya Kusuma Surabaya University)
Nephrology Department
Hospital Clinico Universitario de Valencia

1
Glomerular Disease Classification
Robbins Cotran Pathologic basic disease 8th edition
Primary Glomerular Diseases
1. Minimal-change disease
2. Focal and segmental glomerulosclerosis
3. Membranous nephropathy
4. Acute postinfectious GN
5. Membranoproliferative GN
6. IgA nephropathy
7. Chronic GN
Glomerulopathies Secondary to
Systemic Diseases
1. Lupus nephritis (systemic lupus
erythematosus)
2. Diabetic nephropathy 3. Amyloidosis
4. GN secondary to
lymphoplasmacytic disorders
5. Goodpasture syndrome
6. Microscopic polyangiitis
7. Wegener's granulomatosis
8. Henoch-Schonlein purpura
9. Bacterial endocarditis-related GN
10. GN secondary to extrarenal
infection
11. Thrombotic microangiopathy
Hereditary Disorders
1. Alport syndrome
2. Fabry disease
3. Podocyte/slit-diaphragm protein
mutations

2
1. Epidemiology
2. Pathogenesis
3. Clinical features
4. Cause
5. Diagnosis
6. Prognosis
7. Treatment

3
1.Epidemiology

4
doi: 10.1111/nep.13592
Prevalence of IgA Nephropathy worldwide
Africa;
America; 5% 12%
Asia; 40%
Europe; 25%

5
(Yeo, et al. 2019)
5
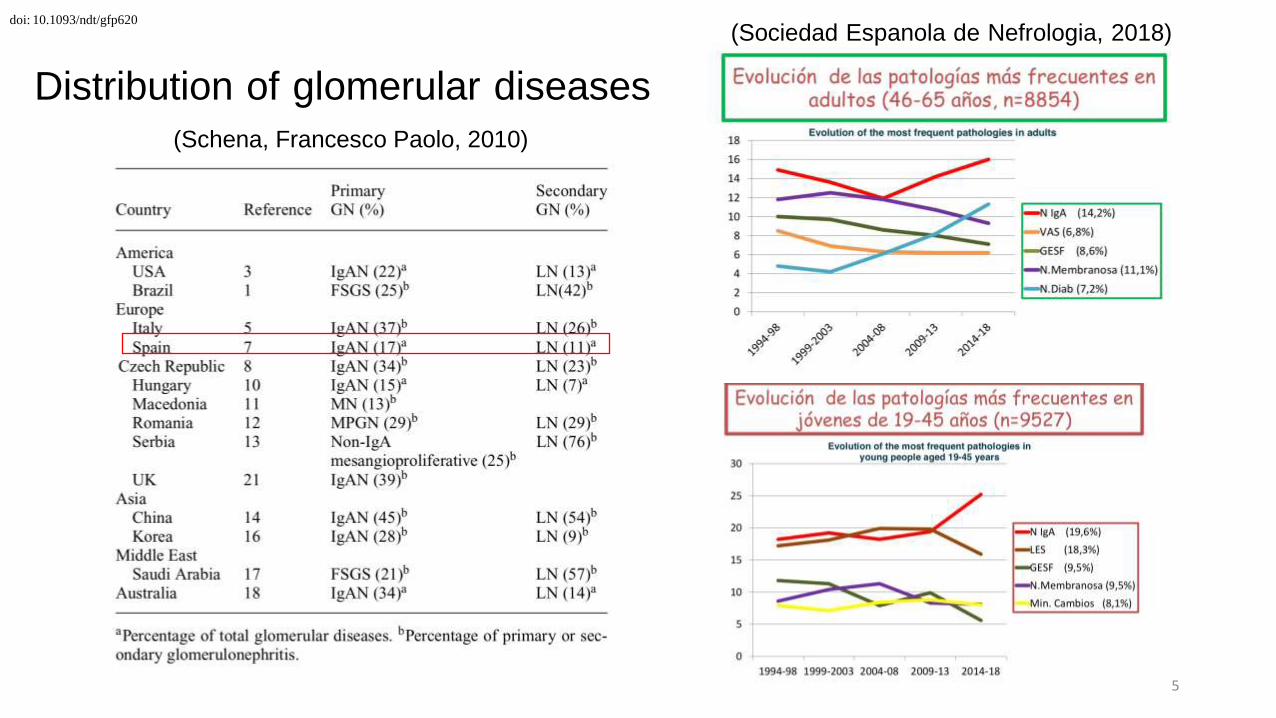
doi: 10.1093/ndt/gfp620
Distribution of glomerular diseases
(Schena, Francesco Paolo, 2010)
(Sociedad Espanola de Nefrologia, 2018)

6
Most common form of primary glomerulonephritis
The peak age : second and third decades
Epidemiology 0.2 to 2.9 per100.000 annual incidence
More common in Asia and Australia
Less common in blacks both in the United States and in Africa
2 : 1 male to female ratio in North America and Western Europe
(Naimeh Tashakkorinia and Maria E. Tudor, 2018)

7
2. Pathogenesis

8
'
•
Genetic predisposition(s)
Hit 1 Increased production of
galactose-deficient lgAl Hit 2 Production of
autoantibodies
Lectin pathway
complement
activation /
' I
Formation of pathogenic
Hit 3 circulating immune
complexes
Renal deposition and
Alternative pathway • complement
activation
Hit 4 injury
FIGURE 1 IProposed four-hit pathogenesis of lgAN. Circulatory galactose-deficient lgA1 (Gd-lgA1) (Hit 1) is recognized by specific autoant ibodies (Hit 2) to form
circulating immune complexes (Hit 3). Some of these immune complexes deposit in the kidneys, thereby leading to mesangial activation, enhanced proliferation of
mesangial cells, and ult imately kidney injury (Hit 4) . Certain genetic loci have been associated with increased risk for developing lgAN. The activation of the alternative
and, at least in some patients, mannan-binding lectin (MBL) pathways by immune complexes is involved in disease pathogenesis .
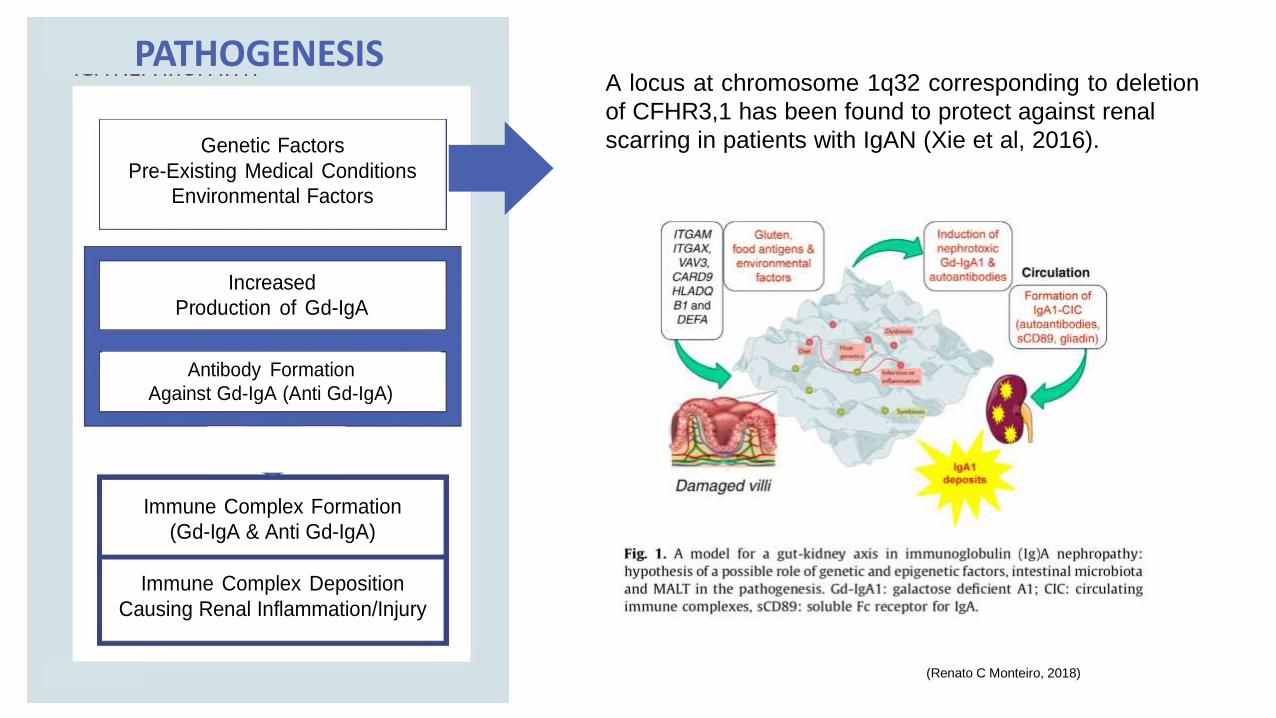
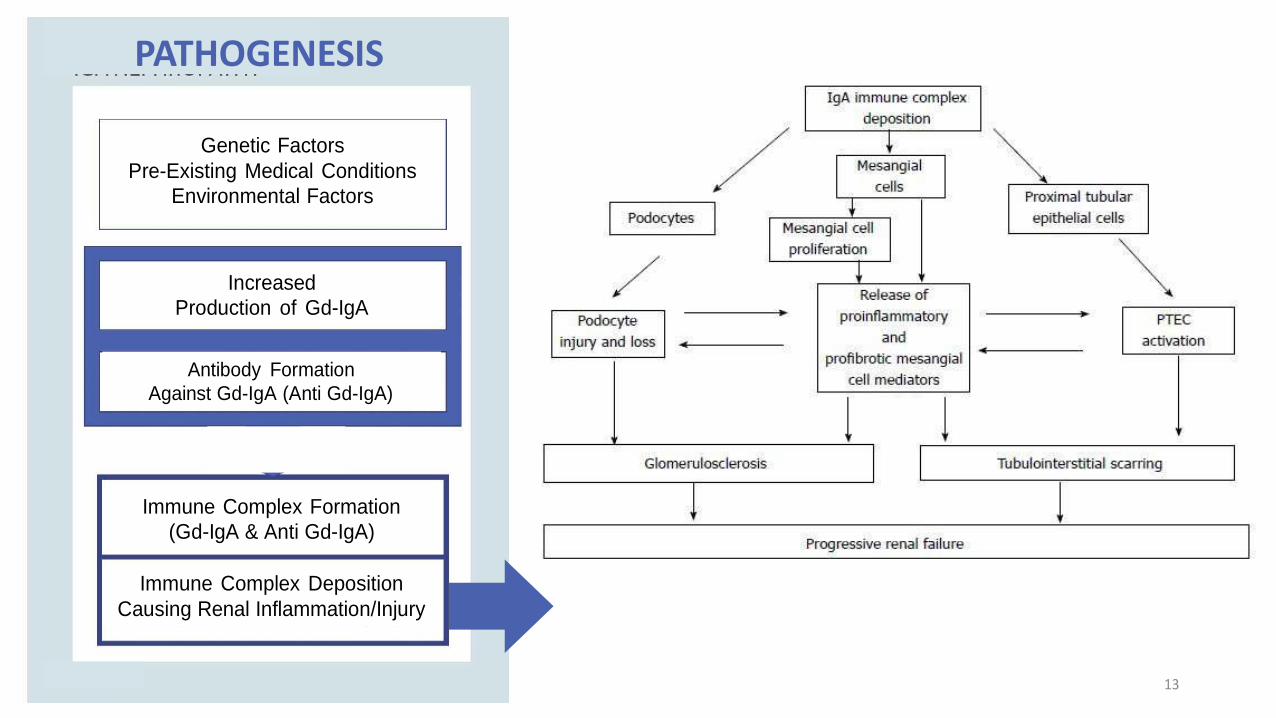
PATHOGENESIS
Genetic Factors
Pre-Existing Medical Conditions
Environmental Factors
Increased
Production of Gd-IgA
Antibody Formation
Against Gd-IgA (Anti Gd-IgA)
Immune Complex Formation
(Gd-IgA & Anti Gd-IgA)
Immune Complex Deposition
Causing Renal Inflammation/Injury
A locus at chromosome 1q32 corresponding to deletion
of CFHR3,1 has been found to protect against renal
scarring in patients with IgAN (Xie et al, 2016).
(Renato C Monteiro, 2018)

Abnormal Gl
cosilation
PATHOGENESIS
Genetic Factors
Pre-Existing Medical Conditions
Environmental Factors
IgA1
Hinge Region
Normal Glycosilation
(Galactose)
O-Linked Glycosilation O-Linked Glycosila2on
O-Linked Glycosilation
O-Linked Glycosilation
Amino acid O-Linked Glycosila2on
Glycosilated IgA1
↓
Identifed by body
↓
Degraded when (Gives Flexibility to bind antibgen)
O-Linked Glycosilation accumulated too much
Increased
Production of Gd-IgA
Ser = Serine Thr = Threonine
O-Linked Glycosila2on
O-Linked Glycosilation
O-Linked Glycosilation
Antibody Formation
Against Gd-IgA (Anti Gd-IgA)
IgA1
(Galactose deficient) = Gd → Gd-IgA (Galactose)
O-Linked Glycosilation O-Linked Glycosila2on
Immune Complex Formation
(Gd-IgA & Anti Gd-IgA)
Hinge Region
O-Linked Glycosila2on
O-Linked Glycosilation
Amino acid O-Linked Glycosila2on
Abnormal Glycosilated
IgA1
↓
Not Identifed by body
Immune Complex Deposition
Causing Renal Inflammation/Injury
(Gives Flexibility to bind antigen)
Ser = Serine Thr = Threonine
O-Linked Glycosilation
O-Linked Glycosilation
O-Linked Glycosilation
O-Linked Glycosilation
↓ Not Degraded when
accumulated too much
↓
ACCUMULATES
10
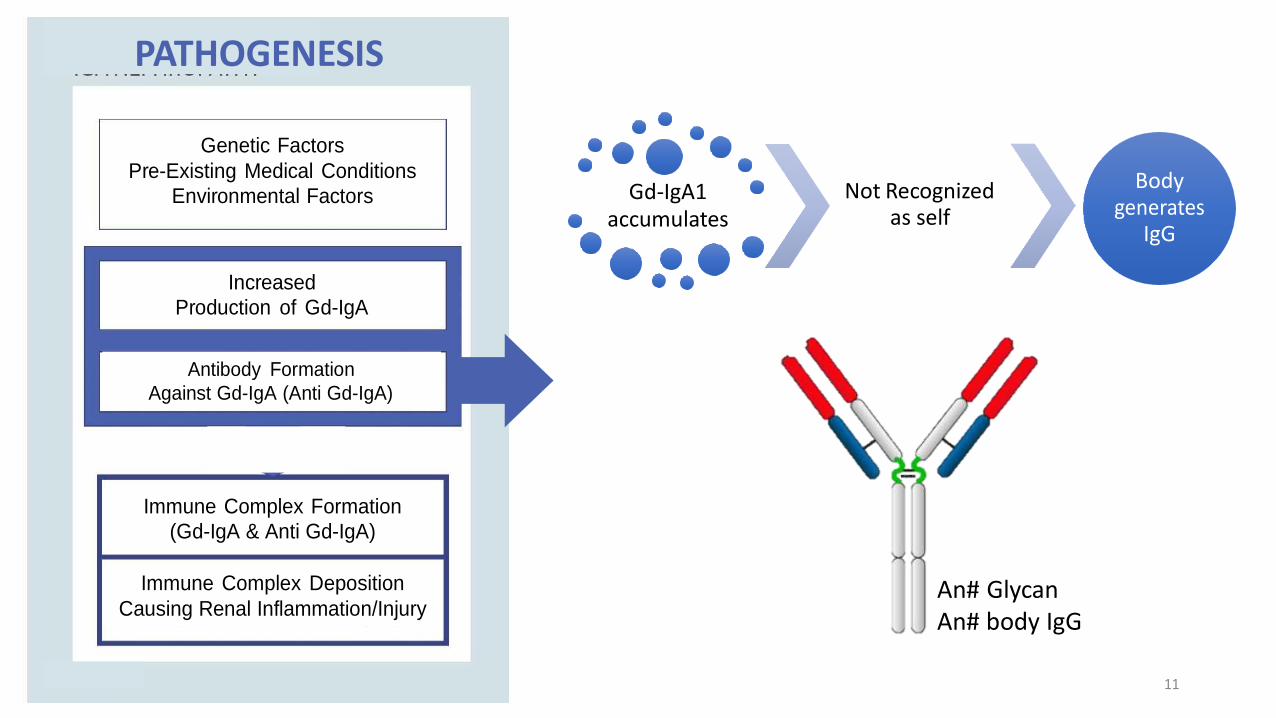
PATHOGENESIS
Genetic Factors
Pre-Existing Medical Conditions
Environmental Factors
Gd-IgA1 accumulates
Not Recognized as self
Body generates
IgG
Increased
Production of Gd-IgA
Antibody Formation
Against Gd-IgA (Anti Gd-IgA)
Immune Complex Formation
(Gd-IgA & Anti Gd-IgA)
Immune Complex Deposition
Causing Renal Inflammation/Injury
An# Glycan An# body IgG
11

PATHOGENESIS
Genetic Factors
Pre-Existing Medical Conditions
Environmental Factors
Gd-IgA1 accumulates
Not Recognized as self
Body generates
IgG
Increased
Production of Gd-IgA
Antibody Formation
Against Gd-IgA (Anti Gd-IgA)
Immune Complex Formation
(Gd-IgA & Anti Gd-IgA)
Anti Glycan Anti body IgG
Immune Complex Deposition
Causing Renal Inflammation/Injury
Gd-IgA1
Immune complex 12
PATHOGENESIS
Genetic Factors
Pre-Existing Medical Conditions
Environmental Factors
Increased
Production of Gd-IgA
Antibody Formation
Against Gd-IgA (Anti Gd-IgA)
Immune Complex Formation
(Gd-IgA & Anti Gd-IgA)
Immune Complex Deposition
Causing Renal Inflammation/Injury
13

fGJE
Renal corpuscle
Efferent art riot
oot process
Bas m nt m mbran
Bowman's space
Distal convolu ed tubul
r====
Pro imal tubule
H ealthy
lgAN
Afferent arteriofe matrix ,
Proliferation of mesangial cells
,.
lit
diaphragm
GBM
ndothelial cells I
---------------------
pith lialc II
It; II esangial cell
r cell
acroph ge
onocy
Podocyte
Protein
lgA
Gd·l gA1
lgG
N ture Review: I Di e Prim r
(Lai, Kar Neng, et al. 20"16) 14
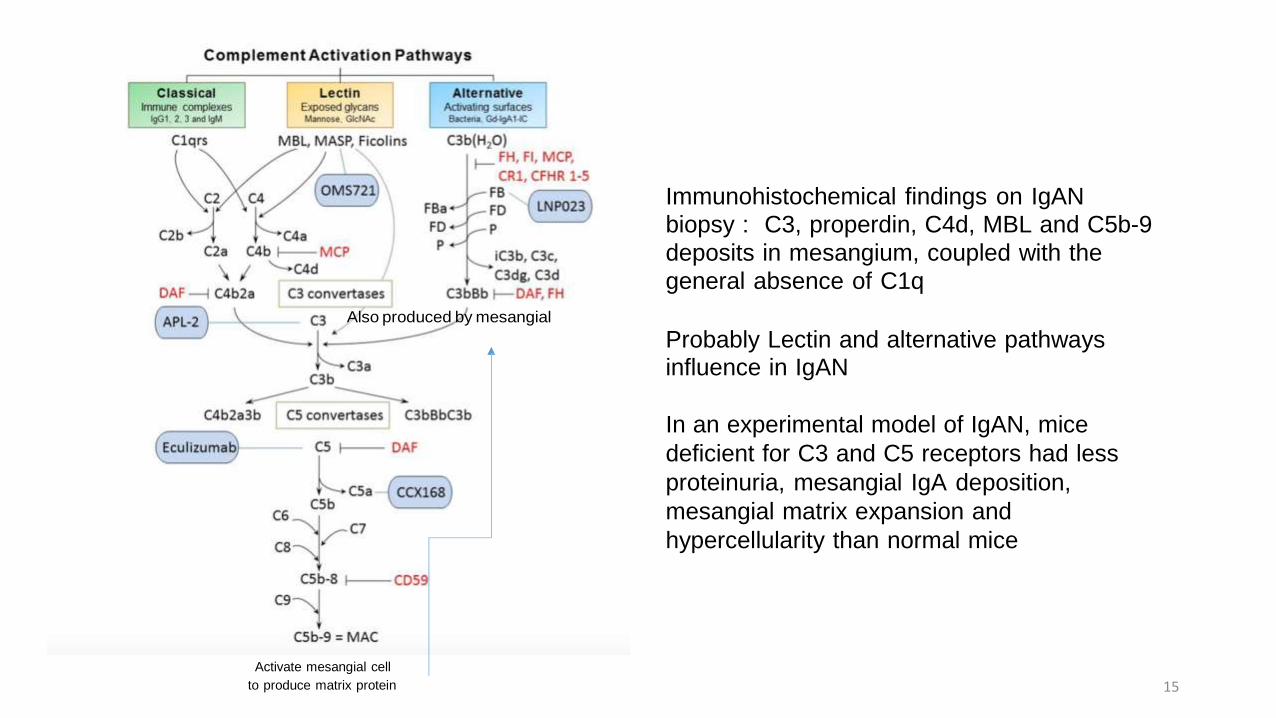
Also produced by mesangial
Immunohistochemical findings on IgAN
biopsy : C3, properdin, C4d, MBL and C5b-9
deposits in mesangium, coupled with the
general absence of C1q
Probably Lectin and alternative pathways influence in IgAN
In an experimental model of IgAN, mice
deficient for C3 and C5 receptors had less
proteinuria, mesangial IgA deposition,
mesangial matrix expansion and
hypercellularity than normal mice
Activate mesangial cell
to produce matrix protein 15

16
3. Clinical Features

1. Micro/Hematuria – during/after
infection – mostly mucosal infection
2. Proteinuria
3. High blood pressure
4. Nephrotic Syndrome
(Naimeh Tashakkorinia, Maria E. Tudor, 2018) 17

18
4. Cause

Cause? Unknown, Risk associated
• Genes
• Liver diseases
• Celiac disease,
• Dermatitis herpetiformis
• Infections
• Family History
19

20
5. Diagnosis
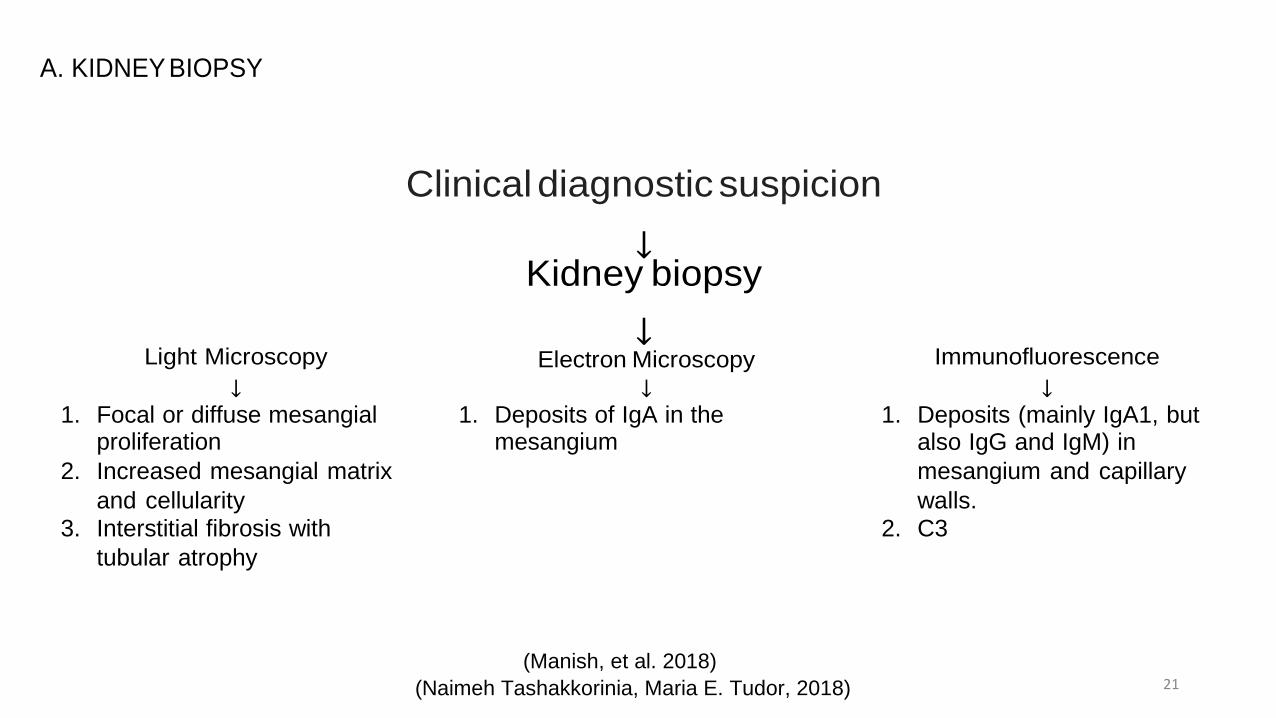
A. KIDNEY BIOPSY
Light Microscopy
↓
Clinical diagnostic suspicion
↓ Kidney biopsy
↓ Electron Microscopy
↓
Immunofluorescence
↓ 1. Focal or diffuse mesangial
proliferation
2. Increased mesangial matrix
and cellularity 3. Interstitial fibrosis with
tubular atrophy
1. Deposits of IgA in the mesangium
1. Deposits (mainly IgA1, but also IgG and IgM) in
mesangium and capillary
walls. 2. C3
(Manish, et al. 2018)
(Naimeh Tashakkorinia, Maria E. Tudor, 2018) 21
22
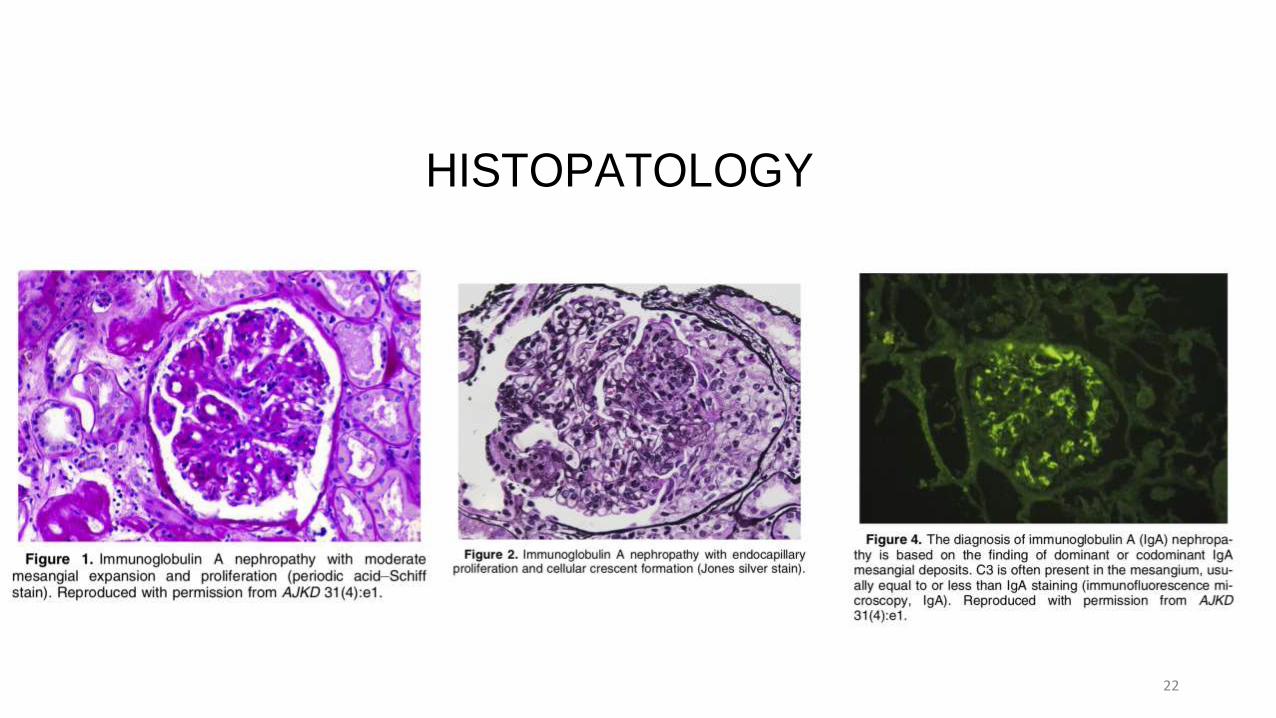
HISTOPATOLOGY

B .BIOMARKERS doi:10.1371/journal.pone.0098081
A Panel of Serum Biomarkers Differentiates IgA Nephropathy from Other Renal Diseases
(Yanagawa, Hiroyuki. et al, 2014)
23

24
A Panel of Serum Biomarkers
Differentiates IgA Nephropathy
from Other Renal Diseases (Yanagawa, Hiroyuki. et al, 2014)
doi:10.1371/journal.pone.0098081
1. Serum Gd-IgA1
2. Serum Gd-IgA1 specific
IgG
3. Serum Gd-IgA1 specific
IgA
25
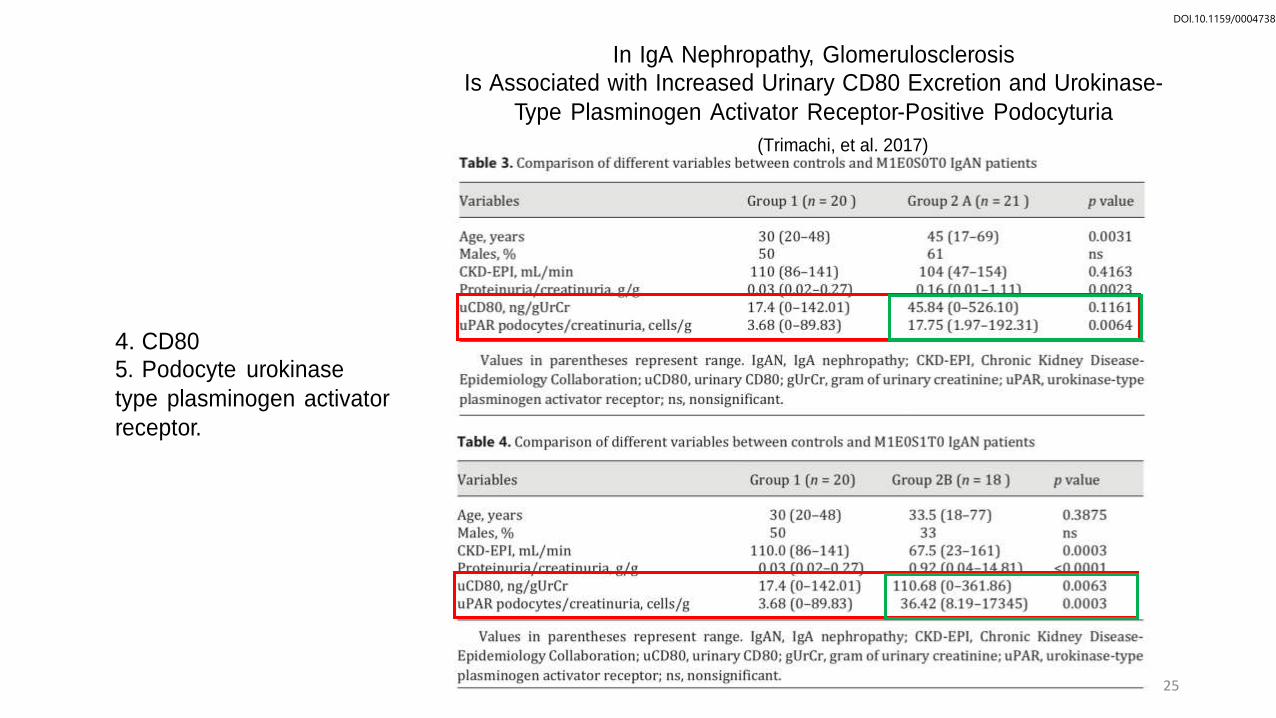
In IgA Nephropathy, Glomerulosclerosis
Is Associated with Increased Urinary CD80 Excretion and Urokinase-
Type Plasminogen Activator Receptor-Positive Podocyturia
(Trimachi, et al. 2017)
DOI.10.1159/0004738
4. CD80 5. Podocyte urokinase
type plasminogen activator
receptor.

26
Predict renal outcome independent of proteinuria, BP, and eGFR.

27
6. Prognosis

Prognosis
IgA nephropathy reduces life expectancy by more than 10 years and leads to kidney failure in 20–40% of patients within 20 years of diagnosis
CLINICAL
1. Hypertension >140/90
2. Reduce GFR
3. High creatinine
4. Persistence hematuria
5. High Trigliserida
6. High ureum
7. Proteinuria >1g/24hour
8. Obesity
HISTOPATOLOGY
1. Cresent (>30%)
2. Sclerotic glomerulus
3. Tubular atrophy
4. Interstitial tissue fibrotic
5. Mesangial Hypercelullarity > 50%
(Naimeh Tashakkorinia, Maria E. Tudor, 2018)
(Dana, et al. 2019) 28

29
7. Treatment

recurrence rate is high after tranplantation
30

31
Conservative therapy
1. Angiotensin-converting enzyme inhibitors or angiotensin-receptor blockers, adequate blood pressure control <125/75
2. Low-sodium intake diet
3. Physical exercise
4. Adequate loss of weight
5. Lipid control
6. Tobacco avoidance

Current Study
1. Intensive Supportive Care plus Immunosuppression in IgA Nephropathy (STOP-IgAN)
2. Rituximab
3. Targeted-release budesonide versus placebo in patients with IgA nephropathy (NEFIGAN)
4. Tonsilectomy (Japan), european? 5. Effect of Oral Methylprednisolone on Clinical Outcomes in Patients With IgA Nephropathy
The TESTING Randomized Clinical Trial
6. US trials mycophenolat mofetil (MMF) terminated early – not proven
7. Chinese MMF + low dose Steroid = Endocapillary hypercellularity, crescents, and necrosis lesions in glomeruli had improved or disapeared after immunosuppressive therapy (KDIGO Basic)
8. Tacrolimus – decrease proteinuria, in China
9. Fish Oil = remain unclear, some research failed to show benefit but a European trial of 30 patients
suggested that a RAS blocker combined with polyunsaturated fatty acids reduced proteinuria more
than a RAS blocker alone
32

Intensive Supportive Care plus Immunosuppression in IgA Nephropathy (STOP-IgAN)
(Raumen, et al. 2015) Comparing
a. Supportive (RASB)
b.RASB + Cyclophosphamide + azathioprine + prednisolon
Conclusion : The addition of immunosuppression did not significantly improve the outcome 33

A R
doi: 10.1681/ASN.2016060640
andomized, Controlled Trial of Rituximab in IgA Nephropathy with Proteinuria and Renal Dysfunction (Laffayete, Richard. et al. 2017)
Rituximab
1-year follow-up
34 adult patients with
biopsy–proven IgA nephropathy
Conclusion : Neither eGFR and Proteinuria not statistically significant, otherwise more adverse effect 34

Tonsillectomy reduces recurrence of IgA nephropathy DOI 10.1007/s10157-015-1170-7
in mesangial hypercellularity type categorized by the Oxford classification (Hirano, keita. et al, 2016)
Conclusion : Tonsillectomy reduce recurrence of IgAN (proteinuria and IgA/C3)
Meeting report 15th International Symposium on IgA Nephropathy 2019 Argentina: Tonsillectomy may
considered in recurrent tonsillitis 35

dx.doi.org/10.1016/S0140-6736(17)30550-0
Targeted-release budesonide versus placebo in patients with IgA nephropathy
(NEFIGAN): a double-blind, randomised, placebo-controlled phase 2b trial
(FellstrOm̈ , Bengt C. et al, 2017)
UPCR
36
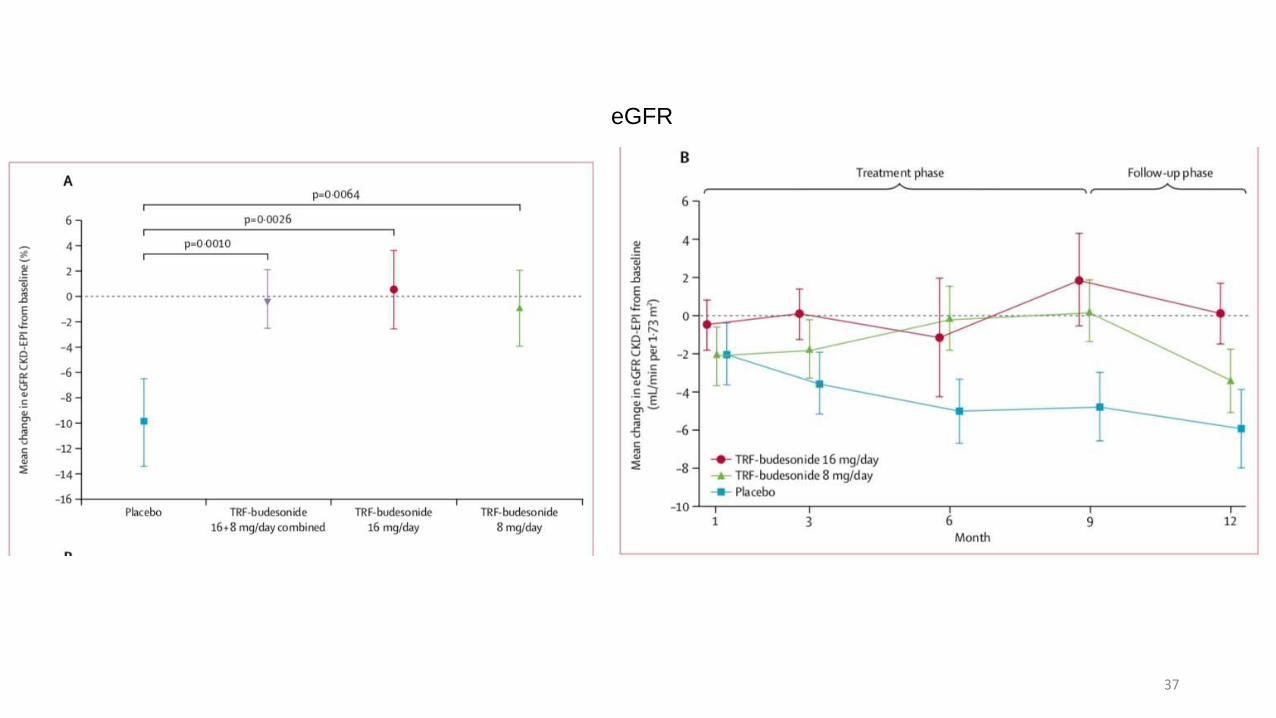
eGFR
37

Placebo
(n=50)
TRF-budesonide 8 mg/day
(n=51)
TR F-budesonide 16 mg/day
(n=49)
Total
(n=150)
Patients {%) Events Patients {%) Even ts Patients {%) Events Patients {%) Events
Any adverse event 42{84%) 162 48(94%) 270 43{88%) 305 133 (89%) 737
Nasopharyngi tis 10 {20%) 14 8{16%) 16 10 {20%) 16 28 {19%) 46
Acne* 3{6%) 3 8{16%) 9 9 {18%) 10 20 {13%) 22
Joint swelling 2 (4%) 2 8(16%) 8 9 {18%) 14 19 (13%) 24
Cushingoid* 3{6%) 3 5 {10%) 5 8{16%) 8 16 {11%) 16
Insomnia* 2 {4%) 2 6 {12%) 6 8{16%) 9 16 {11%) 17
Diarrhoea 7 {14%) 9 1{2%) 1 5 {10%) 5 13{9%) 15
Dyspepsia t 4{8%) 5 2 {4%) 2 7 {14%) 9 13{9%) 16
Headache 3{6%) 4 3{6%) 3 6 {12%) 6 12 {8%) 13
Alopecia* 2 {4%) 2 4{8%) 5 4{8%) 4 10 {7%) 11
Back pain 1{2%) 1 6 {12%) 8 3{6%) 3 10 {7%) 12
Mood swings* 2 {4%) 2 3{6%) 3 5 {10%) 5 10 {7%) 10
Oedema peripheral 2{4%) 3 2{4%) 3 6 {12%) 9 10 {7%) 15
Blood creatine 3{6%) 3 3{6%) 4 3{6%) 3 9 {6%) 10 phosphokinase increased Hirsu tism* 1{2%) 1 3{6%) 3 5 {10%) 5 9 {6%) 9
Hypertension 1{2%) 1 3{6%) 3 5 {10%) 5 9 {6%) 9
Muscle spasms 2{4%) 3 5 {10%) 5 2{4%) 2 9 {6%) 10
Abdominal pain t 1{2%) 1 4{8%) 4 3{6%) 4 8{5%) 9
Nausea 1{2%) 1 4{8%) 4 3{6%) 5 8{5%) 10
Upper respi ratory tract
infection 3{6%) 3 2 {4%) 3 3{6%) 3 8{5%) 9
Adverse events reporte d by ;.:5% ofthe total pat ient population. TRF-budesonide=targeted-release formulation-budesonide. •corticosteroid-related adverse events solicited
by questionnaire at every visit. tGastrointestinal-related adverse events solicited by q uestionnaire at every visit
Table 2: Treatment-emergent adverse events reported by l!:5% of all pat ients by preferred term (safety set)
Conclusion : Budesonide 8 mg or 16 mg reduce UPCR and stabilize eGFR 38

40
doi:10.1001/jama.2017.9362
Effect of Oral Methylprednisolone on Clinical Outcomes in Patients With IgA Nephropathy
The TESTING Randomized Clinical Trial (Jicheng, et al. 2017)
All patient Proteinuria >1 g/d
Methylprednisolon 0.6 to 0.8 mg/kg/d reduce proteinuria (P<0.001) + GFR p(<0.01)
Plan for 5 years, Stopped at 3rd year due to adverse event infection
including lethal Pneumocystis jirovecii pneumonia
TESTING 2 – Lower doses 0.4 mg, complete in 2023

40
Conclusion : Final conclusian cannot be made

40
Table 1. From the KDIGO guidelines for corticosteroids in lgAN34
(A) Supportive care with antiproteinuric and antihypertensive drugs (statement 10.2). We recommend long-term ACE-I or ARB (RASBs) treatment
when proteinuria is >1 g/d, with uptitration of drug depending on BP (1B). Suggestions to uptitrate RASBs as far as tolerated to achieve
proteinuria <1 g/d (2C). Target BP <125/75 mmHg when proteinuria is >1 g/d (not graded).
(B) Corticosteroids (statement 10.3.1). We suggest that patients with persistent proteinuria >1 g/d, despite 3-6 mo of optimized supportive care
(including RASBs and BP control) and GFR>50 ml/min per 1.73m2 , receive a 6-mo course of corticosteroid therapy (2C) .
(C) Corticosteroid regimens
(a) iv Bolus injection of 1 g methylprednisolone for 3d each at months 1, 3, and 5 followed by oral steroid (0.5 mg/kg prednisone) on alternate
days for 6 mo.26
(b) Oral prednisone starting with 0.8-1 mg/kg per d for 2 mo and then reduced by 0.2 mg/kg per d permo for the next 4 mo.27 •28
(D) Immunosuppressive agents cyclophosphamide and azatiophrine (statement 10.4.1). We suggest not treating with corticosteroids combined
with cyclophosphamide or azathioprine in patients with lgAN (unless there is a crescentic lgAN with rapidly progressive course; 2D).
Evidence is graduated in levels: 1, recommendations; 2, suggestions; A to D indicates high quality to very low quality, respectively.34

42
Future Therapy
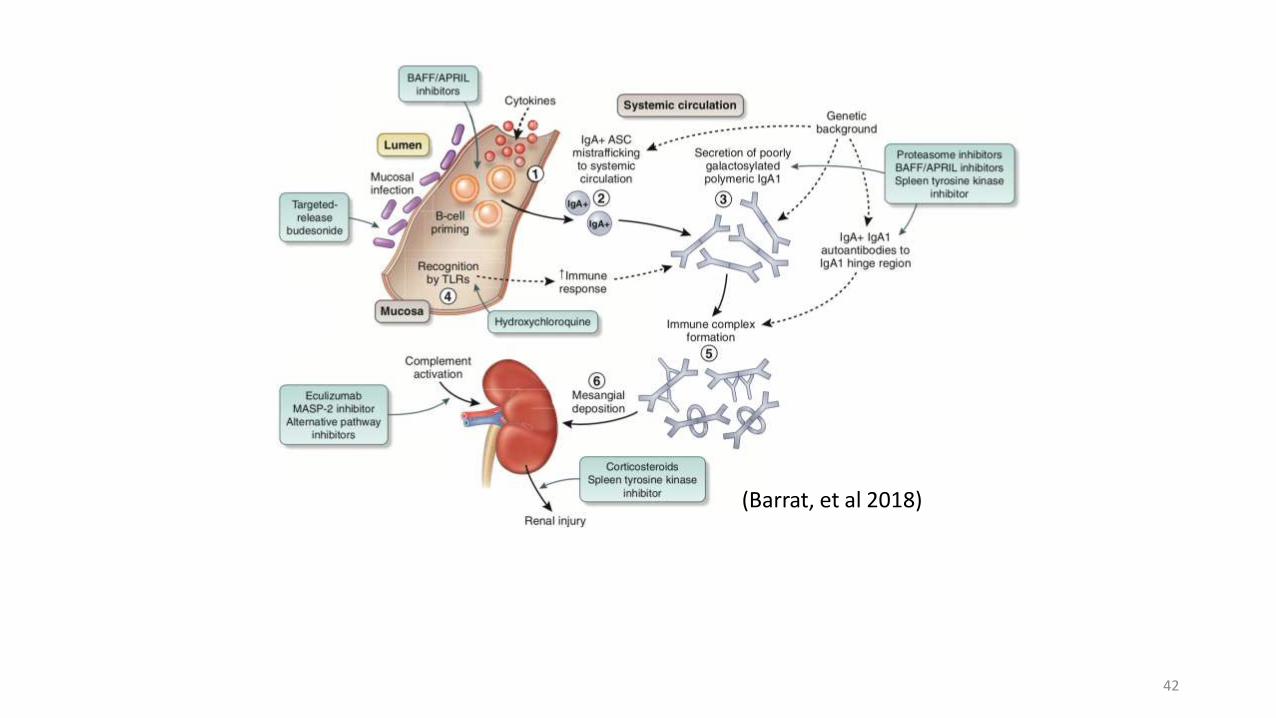
42
(Barrat, et al 2018)

Short story:
1. 16-year-old male with crescentic IgAN who had failed
treatment with corticosteroids, cyclophosphamide, and
plasma exchange subsequently had transient
improvement in renal function with eculizumab
2. Sweden; a young 16-year-old white male with biopsy-
proven crescentic IgAN had failed to respond to
corticosteroids and mycophenolate but stabilized when
treated with eculizumab 43

Future therapy
1. Modulation of mucosal B-cell programming (TLR antagonist) Hydroxychloroquine –TLR-9 inhibitor –
China – reduction proteinuria in 24 weeks significantly 200 mg twice daily compare to RASB only, 2
more RCT’s on going in China 2. Modulation of mucosal B-cell programming (BAFF/APRIL antagonist) - BAFF is necessary for B-cell
maturation - Tonsillar mononuclear cells from IgAN patients exposed to CpG-oligodeoxynucleotide
produce high levels of BAFF and IgA. TLR-9 stimulation induces APRIL (TNF) expression in tonsillar
B cells.
a. Blisibimod = antagonist BAFF (started in 2013, Study completed. Not yet published)
b. Atacicept = BAFF/APRIL dual inhibitor (started in 2017, complete in 2020)
3. Spleen tyrosine kinase (Syk) inhibitor Fostamatinib – Syk mediates maturation and survival of the B-
cell lineage (started in 2014) 4. Proteasomal ihibition = bortezomib (completed in 2017, not yet published)
5. B-cell activating factor = inhibition (LNP023)
6. Complement inhibition (lectin and alternative pathway)
a. Eculizumab = antibody monoclonal C5
b. APL-2 = C3 inhibitor c. CCX168 = C5a Receptor antagonist
d. LNP023 = Factor B inhibitor
e. OMS721 = mAb MASP-2
44

Mbl serine association protease
doi: 10.3389/fimmu.2019.00504
The Emerging Role of Complement Proteins as a Target for Therapy of IgA Nephropathy
(Dana Rizk V., et al. 2019)
45

Conclusions
IgA Nephropathy the most common form GN in worldwide, 40% in Asia, in Spain (2018) 14,2 -19.6%
Pathogenesis influenced by genetic factor chromosome 1q32 corresponding to deletion of CFHR3, 4 hits mechanism, Complement, MALT
Prognosis based on proteinuria, eGFR and MEST-C
46

47
Conclusion
Conservative therapy is basic for IgAN
Systemic Steroid use IgAN may be considered when the patient has persistent proteinuria
The addition of immunosuppression neither cyclophosphamide and azathioprine nor MMF did not significantly improve the outcome
MMF in cresent may be considered
Tonsilectomy may be considered in recurrent tonsilitis with IgAN
Renal transplant may be preferred for the last choice but considered that IgA nephropathy recurrence rate is high after tranplantation

Conclusion
Awhile, budesonide has better prognostic for the steroid therapy
We are still waiting for the published of these study
- Complement inhibition
- Modulation of mucosal B-cell programming
- Spleen tyrosine kinase (Syk) inhibitor
- Proteasomal ihibitor
- B-cell activating factor
48
49
Thank You
1st February, 2019
To whom it may concern, This is to confirm that the following student is accepted to participate in our bilateral exchange program for medical students:
NAME OF STUDENT: Suryanto Nandhan Seftiyan DATE OF BIRTH: 14-09-1994 NATIONALITY: Indonesia COUNTRY OF ORIGIN: Indonesia PASSPORT NUMBER: C1063625
Our organization, which is a member of International Federation of Medical Students’ Associations(IFMSA), will arrange a clerkship at one of our universities or affiliated university hospitals. We will, during the mentioned period, provide full board and lodging at no charge. The student will be placed under supervision of the administrating chief doctor at the department and will not get any salary.
DEPARTMENT: Internal Medicine-Nephrology HOSPITAL: Hospital Clínico UNIVERSITY, CITY: Spain (IFMSA-Spain) - Valencia HOST COUNTRY: Spain HOST ORGANISATION: IFMSA-Spain PERIOD: 01/04/2019 at 29/04/2019
We urge all authorities to be helpful in order for the medical student to acquire a visa for the arranged Clerkship.
Any further questions regarding the mentioned student’s clerkship should be directed to the National Exchange Officer:
NATIONAL EXCHANGE OFFICER: Jose Antonio Hurtado Aguilar TEL: +34 665965901 EMAIL: [email protected]
Stamp and signature of the NEO
Yours sincerely,

AF Number 95527
Exchange Contract Information
AF Number 95527
Hosting NMO Serbia (IFMSA-Serbia)
Contract signed 21-09-2019
Exchange is unilateral No
Exchange is for a specific month No
Personal Student Information
Family name Adetasia
First name Tesa
Sex Female
Date of birth (dd/mm/yyyy) 19/04/1998
Nationality Indonesia
Language spoken English (Good)
Serbian (Unknown)
Passport number C5880199
Passport valid until (dd/mm/yyyy) 06/01/2025
Student's Medicine Related Information
Medical School Wijaya Kusuma Surabaya
# Medical student since 2016
# Clinical student since 2021
Expected day of graduation 09-2023

AF Number 95527
Student's Mailing and Electronic Information
Street & Number Jl. Parang Tirto RT 16/RW 08 Tambakrejo, Krembung
City Sidoarjo
Post Code 61275
Country Indonesia
Phone Number 082231801976
Alternative phone number
Email [email protected]
Alternative Email
Exchange Preferences
1st Desired City Serbia (IFMSA-Serbia) - Beograd
2nd Desired City Serbia (IFMSA-Serbia) - Novi Sad
3rd Desired City Serbia (IFMSA-Serbia) - Kragujevac
1st Desired Department Surgery-Plastic Surgery
Field studied : Yes
Exam passed : Yes
2nd Desired Department Gynaecology/Obstetrics Field studied : Yes
Exam passed : Yes
3rd Desired Department Radiotherapy Field studied : Yes
Exam passed : Yes
4rt Desired Department Physical Medicine and Rehabilitation
Field studied : Yes
Exam passed : Yes
Exchange Details
# Duration (in weeks) 4
Exchange Start Date (dd/mm/yyyy) 01/10/2021
Exchange End Date (dd/mm/yyyy) 31/10/2021
Type of Clerkship Clinical Clerkship
Do you need an official invitation letter? (for visa or other purpose)
“I will obtain insurance coverage for the Exchange period. Otherwise my exchange will be cancelled
Yes
Yes
Would like to be placed together with this student No
Would like to be placed based on City first

AF Number 95527
Student Remarks

Space for notes/messages to the Exchange Officer of your Country/Local Committee

Notes from the student : The reasons because of my religion, I cannot eat a certain food or drink that contains pork or alcohol. Thank you.
Note


















