Lapkas Dian and Dambo
51
Case Report ATRIAL SEPTAL DEFECT AND VENTRICULAR SEPTAL DEFECT Presenter : Qarina Hasyala Putri (080100367) Dian Primadia Putri (100100013) Day/Date : Tuesday/ April22 nd 2014 Supervisor : dr. Muhammad Ali,Sp.A(K) Introduction Cardiac defects are the most common type of birth defect. An infant with a cardiac defect is more likely to die from this type defect than other types of defects (Forrester 2002). An atrial septal defect (ASD) is a defect or hole in the septum between the two atria of the heart. ASDs are typically divided into several categories depending on the part of the atrial septum where Where the defect occurs secundum ASD (also called ASD 2 or ASD II), defect in the midroportion of the atrial septum concerning the fossa ovails. Primum ASD (also called ASD 1 or ASD I) defect is in the endocardial cushion section of the atrial septum and is typically grouped with other endocardial cushion defects such as endocardial cushion ventricular septal defect and atrioventricular canal. Sinus venous ASD defect is in the upper
-
Upload
dian-primadia-putri -
Category
Documents
-
view
227 -
download
2
Transcript of Lapkas Dian and Dambo
Case Report
ATRIAL SEPTAL DEFECT AND VENTRICULAR SEPTAL DEFECT
Presenter : Qarina Hasyala Putri (080100367)
Dian Primadia Putri (100100013)
Day/Date : Tuesday/ April22nd2014
Supervisor : dr. Muhammad Ali,Sp.A(K)
Introduction
Cardiac defects are the most common type of birth defect. An infant with a cardiac defect is
more likely to die from this type defect than other types of defects (Forrester 2002). An atrial
septal defect (ASD) is a defect or hole in the septum between the two atria of the heart. ASDs
are typically divided into several categories depending on the part of the atrial septum where
Where the defect occurs secundum ASD (also called ASD 2 or ASD II), defect in the
midroportion of the atrial septum concerning the fossa ovails. Primum ASD (also called ASD 1
or ASD I) defect is in the endocardial cushion section of the atrial septum and is typically
grouped with other endocardial cushion defects such as endocardial cushion ventricular septal
defect and atrioventricular canal. Sinus venous ASD defect is in the upper portion of the atrial
septum near the entry of the superior vena cava.1
Ventricular septal defect is one of the commonest congenital malformations of the heart.2
Ventricular septal defect (VSD) is a condition whereby there is a hole between the two pumping
chambers of the heart. The defect can be small or large. The VSD may be termed muscular,
perimembranous, inlet, outlet, apical or doubly committed depending on its position and the
surrounding substance of the heart. Where the VSD is small, there is no elevation of the low
pressures found in the right ventricle (pumping chamber to the lungs) and therefore the lungs are
also low pressure (as they should be). Where the hole is large, the pressure in this right ventricle
can be elevated; sometimes equal to that of the high pressure left ventricle (pumping chamber to
the body).3
Epidemiology
Research indicates that congenital heart disease is diagnosed in 0.8% of children in the first year
of life. Atrial septal defect is the second most common congenital heart defect in children and
adults and occurs in anywhere from 0.67-2.1 per 1000 live births. Secundum atrial septal defects
comprise just over 90% of all atrial septal defects, whereas sinus venosus and primum atrial
septal defects comprise between 3-4% each. About 15-30% of healthy adults have an unfused
foramen ovale in which the valve functions normally but has failed to fuse. In these individuals,
a cardiac catheter passed into the right atrium can pass into the left atrium through the foramen
ovale (ie, probe-patent foramen ovale). In developed countries, mortality rate of atrial septal
defect is low (< 1%). Morbidity secondary to atrial septal defect is unusual and typically limited
to 3 groups of patients.Approximately 1% of infants with moderate or large (ie, nonrestrictive)
atrial septal defects, but no other left to right shunting lesion (eg, patent ductus arteriosus,
ventricular septal defect), have tachypnea and failure to thrive. In these individuals, the
pulmonary artery pressure, when measured during catheterization or Doppler echocardiography,
is at or near systemic level. In most instances, this is a flow-related phenomena (high flow/low
resistance), but in infants predisposed to abnormal pulmonary vasculature, there may be a
combination of both elevated flow and resistance. Attempts to exclude mitral or left ventricular
diastolic abnormalities as a cause of these hemodynamics must be undertaken, as well as a
thorough assessment of pulmonary anatomy and mechanics, as both left-sided cardiac disease
and primary pulmonary disease can mimic symptoms of pretricuspid shunting. The female-to-
male ratio is approximately 2:1. Atrial septal defect , a congenital abnormality, is present at birth.
However, in most cases, a murmur is not audible until the child is a few months old. Symptoms
usually do not occur in individuals with atrial septal defect until late childhood, adolescence, or
adulthood.Secundum type (ie, ostium secundum), sinus venosus, and unroofed coronary sinus
defects are sometimes not diagnosed until the third decade of life.Ostium primum atrial septal
defects are usually diagnosed in the first few years of life because of mitral regurgitation murmur
or an abnormal ECG.A common atrium (ie, a combination of sinus venosus, ostium secundum,
and ostium primum defects) is usually diagnosed in the first few years of life because systemic
venous blood and pulmonary venous blood often partially mix before entering each ventricle;
this condition manifests as cyanosis. In addition, a common atrium may be associated with
complex CHD, and patients may present relatively early because of other intracardiac
abnormalities.4 VSDs affect 2-7% of live births. The patient’s area of residence may influence
the prevalence of known VSDs. For example, small muscular VSDs are most likely to be
identified in urban locations, possibly because of ready access to sophisticated healthcare in
these locations.An echocardiographic study revealed a high incidence of 5-50 VSDs per 1000
newborns. The defects in this study were small restrictive muscular VSDs, which typically
spontaneously close in the first year of life.VSDs are the most common lesion in many
chromosomal syndromes, including trisomy 13, trisomy 18, trisomy 21, and relatively rare
syndromes. However, in more than 95% of patients with VSDs, the defects are not associated
with a chromosomal abnormality.VSDs are slightly more common in female patients than in
male patients (56% vs 44%).4
Pathophysiology
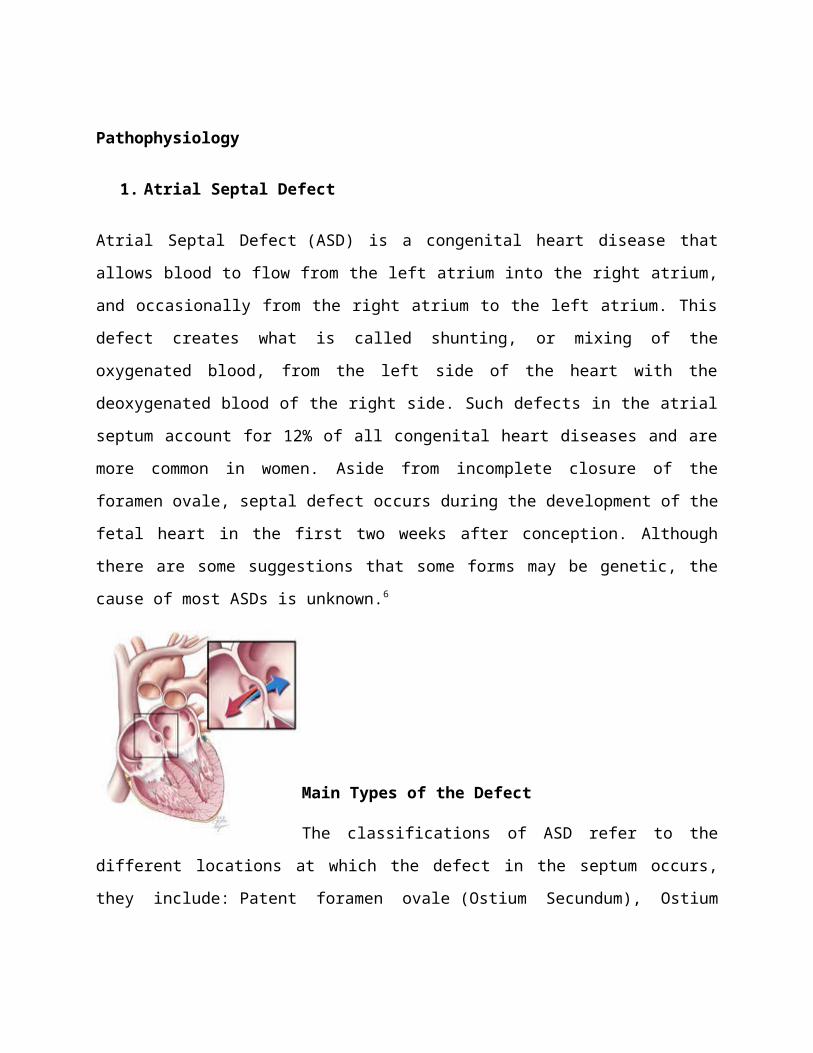
1. Atrial Septal Defect
Atrial Septal Defect (ASD) is a congenital heart disease that allows blood to flow from the left
atrium into the right atrium, and occasionally from the right atrium to the left atrium. This defect
creates what is called shunting, or mixing of the oxygenated blood, from the left side of the heart
with the deoxygenated blood of the right side. Such defects in the atrial septum account for 12%
of all congenital heart diseases and are more common in women. Aside from incomplete closure
of the foramen ovale, septal defect occurs during the development of the fetal heart in the first
two weeks after conception. Although there are some suggestions that some forms may be
genetic, the cause of most ASDs is unknown.6
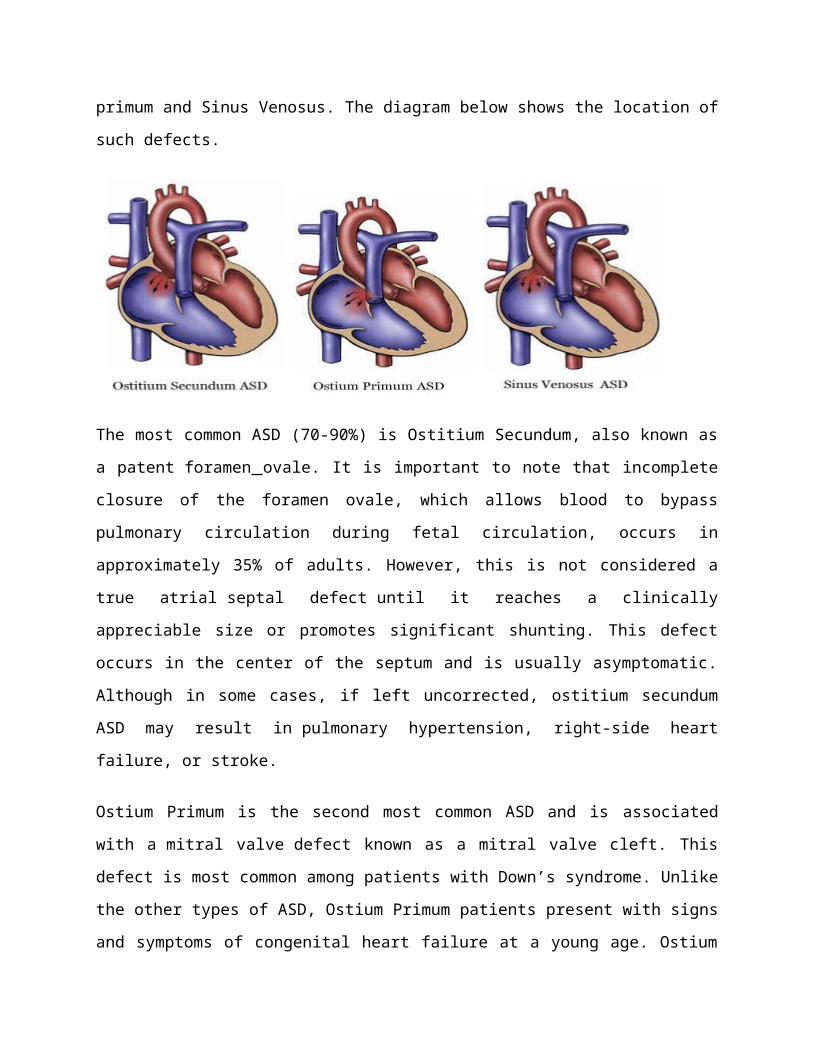
Main Types of the Defect
The classifications of ASD refer to the different locations at which the defect in the septum
occurs, they include: Patent foramen ovale (Ostium Secundum), Ostium primum and Sinus
Venosus. The diagram below shows the location of such defects.
The most common ASD (70-90%) is Ostitium Secundum, also known as a patent foramen ovale.
It is important to note that incomplete closure of the foramen ovale, which allows blood to
bypass pulmonary circulation during fetal circulation, occurs in approximately 35% of adults.
However, this is not considered a true atrial septal defect until it reaches a clinically appreciable
size or promotes significant shunting. This defect occurs in the center of the septum and is
usually asymptomatic. Although in some cases, if left uncorrected, ostitium secundum ASD may
result in pulmonary hypertension, right-side heart failure, or stroke.
Ostium Primum is the second most common ASD and is associated with a mitral valve defect
known as a mitral valve cleft. This defect is most common among patients with Down’s
syndrome. Unlike the other types of ASD, Ostium Primum patients present with signs and
symptoms of congenital heart failure at a young age. Ostium Primum is the most difficult ASD
to fix and requires the closure of the defect prior to valve reconstruction; however, if done before
the age of one, the surgery yields excellent results.
The rarest form of ASD is Sinus Venosus. This defect is in the upper portion of the atrial septum
and often results in an abnormal connection between the pulmonary veins and the heart. There
are four pulmonary veins that bring oxygenated blood from the lungs back to the heart. In Sinus
Venosus ASD patients, however, one of these veins is connected to the right atria instead of the
left, dumping oxygenated blood into the right atria where it mixes with deoxygenated blood that
has just been returned from the body.
In all forms of ASD, the magnitude of blood flowing through the defect depends on the size of
the defect and compliance of the ventricles. In general, the right ventricle is more compliant than
the left, and therefore blood flows from left to right through the defect. This extra blood in the
right ventricle causes the right ventricle to hypertrophy. This problem is exacerbated by the
development of pulmonary hypertension and incomplete ventricular emptying, which often
occurs later in adult life. As the resistance in the right ventricle increases the left to right shunt
declines and eventually the right ventricle becomes less compliant than the left – creating a shunt
from right to left. This right to left shunt can quickly become a serious problem as deoxygenated
blood is mixed with blood about to be pumped into systemic circulation, causing systemic
ischemia.6
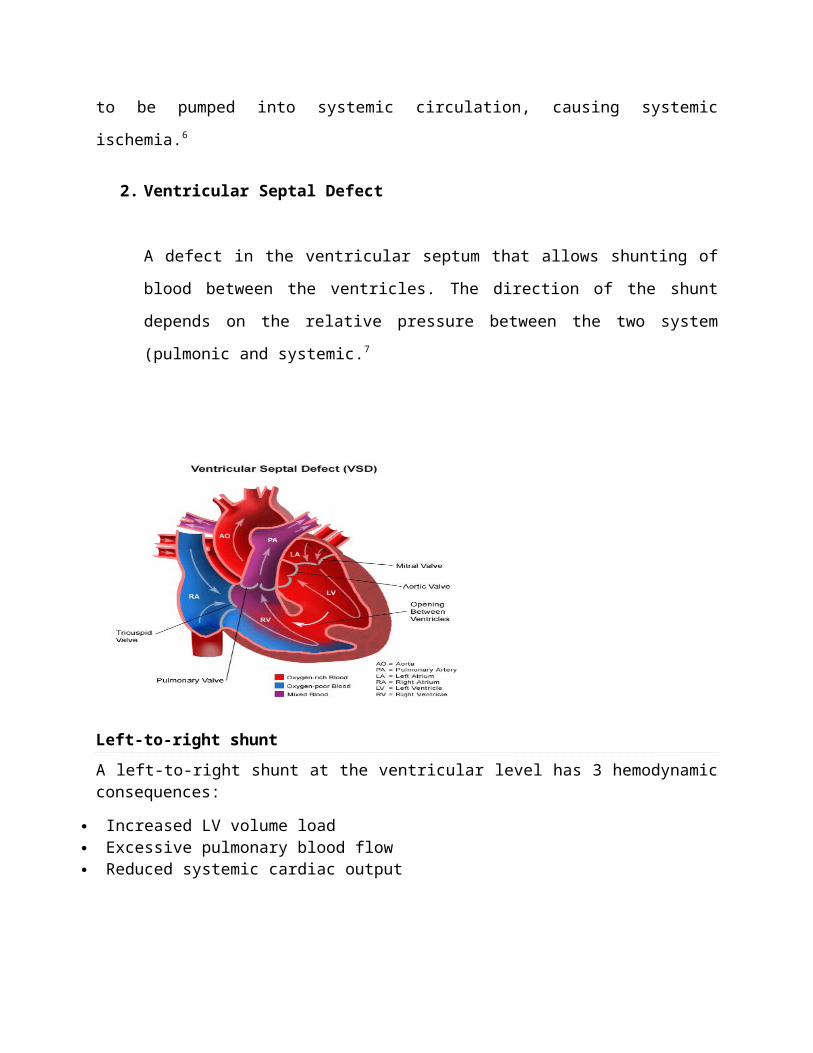
2. Ventricular Septal Defect
A defect in the ventricular septum that allows shunting of blood between the ventricles.
The direction of the shunt depends on the relative pressure between the two system
(pulmonic and systemic.7
Left-to-right shunt
A left-to-right shunt at the ventricular level has 3 hemodynamic consequences:
Increased LV volume load Excessive pulmonary blood flow Reduced systemic cardiac output
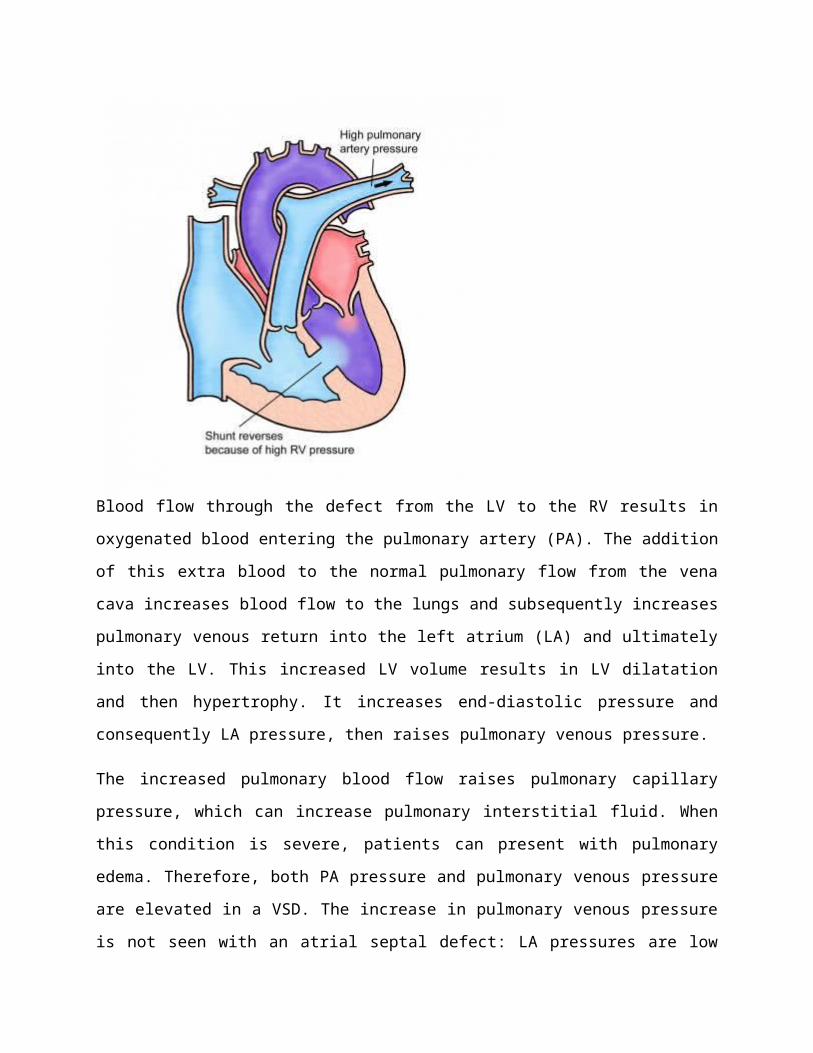
Blood flow through the defect from the LV to the RV results in oxygenated blood entering the
pulmonary artery (PA). The addition of this extra blood to the normal pulmonary flow from the
vena cava increases blood flow to the lungs and subsequently increases pulmonary venous return
into the left atrium (LA) and ultimately into the LV. This increased LV volume results in LV
dilatation and then hypertrophy. It increases end-diastolic pressure and consequently LA
pressure, then raises pulmonary venous pressure.
The increased pulmonary blood flow raises pulmonary capillary pressure, which can increase
pulmonary interstitial fluid. When this condition is severe, patients can present with pulmonary
edema. Therefore, both PA pressure and pulmonary venous pressure are elevated in a VSD. The
increase in pulmonary venous pressure is not seen with an atrial septal defect: LA pressures are
low because as blood can readily exit from this chamber through the atrial communication.
Finally, as blood is shunted through the VSD away from the aorta, cardiac output decreases, and
compensatory mechanisms are stimulated to maintain adequate organ perfusion. These
mechanisms include increased catecholamine secretion and salt and water retention by means of
the renin-angiotensin system.
The degree of the left-to-right shunt determines the magnitude of the changes described above.
The left-to-right shunt depends on 2 factors, of which one is anatomic and the other physiologic.
The anatomic factor is the size of the VSD. (The location of the VSD is irrelevant in terms of the
degree of the shunt.) In a normal heart, RV pressure is about 25-30% that of the LV. In a large
VSD, this pressure difference is no longer maintained, because a large hole offers no resistance
to blood flow. Consequently, these defects are called nonrestrictive VSDs.
On the other hand, in a small VSD, the normal pressure difference between the ventricles is
maintained. These defects are called restrictive VSDs because blood flow across the defects is
somewhat restricted, so that the normal pressure difference is maintained.
The physiologic factor is the resistance of the pulmonary vascular bed.
Changes in pulmonary vasculature
The terms pulmonary hypertension, high pulmonary resistance, and pulmonary vascular disease
are often confused. Pulmonary hypertension merely indicates a high blood pressure in the
pulmonary circuit; depending on the duration, it may be reversible. Pulmonary resistance is a
function of numerous factors, including age, altitude, hematocrit, and diameter of the pulmonary
arterioles.
A neonate has increased resistance secondary to the increase in the media of the pulmonary
arterioles; this decreases the effective diameter of the vessels. In addition, neonates have a
relative polycythemia. The elevated pulmonary resistance usually declines to adult levels by 6-8
weeks.
Pulmonary vascular disease is ultimately an irreversible condition and may occur over time in
individuals with a large left-to-right shunt. It may also occur in the absence of a shunt; this
condition is called primary pulmonary hypertension. A characteristic series of histologic changes
ranging from grade I to grade VI has been described. The ultimate consequences of pulmonary
vascular obstructive disease are irreversible vascular changes and pulmonary resistance equal to
or exceeding systemic resistance.
Natural history
The natural history of VSD has a wide spectrum, ranging from spontaneous closure to congestive
heart failure (CHF) to death in early infancy.
Spontaneous closure frequently occurs in children, usually occurs by age 2 years. Closure is
uncommon after age 4 years. Closure is most frequently observed in muscular defects (80%),
followed by perimembranous defects (35-40%). Outlet VSDs have a low incidence of
spontaneous closure, and inlet VSDs do not close.
Closure may occur by means of hypertrophy of the septum, formation of fibrous tissue, subaortic
tags, apposition of the septal leaflet of the tricuspid valve, or (in rare cases) prolapse of a leaflet
of the aortic valve. When perimembranous VSDs close because of development of fibrous tissue
or the apposition of the tricuspid valve, an aneurysm of the interventricular septum may appear.
A small VSD that does not spontaneously close is generally associated with a good prognosis.
Patients are at risk for infective endocarditis, but small muscular VSDs pose no other adverse
possibilities.
Small perimembranous VSDs, however, are associated with an increased risk of prolapse of the
aortic cusp over time. In addition, a small but definite risk of malignant ventricular arrhythmia
was reported in the Second Natural History Study. This study group consisted of about 1000
patients (about 76% of the original cohort). The original cohort was the First Natural History
Study, which included 1280 patients (mostly children) with VSDs admitted after cardiac
catheterization between 1958 and 1969.
Wu et al reported a 45% incidence of LV-to-RA shunts and a 6% incidence of subaortic ridges
during a 20-year follow-up of about 900 patients with perimembranous VSDs. This group later
reported an increased incidence of infective endocarditis in patients who had LV-to-RA shunts.8
Clinical Presentation of Atrial Septal Defect
1. Symptoms
Isolated ASD patients are usually asymptomatic and are most often detected at the time of
preschool physical examination. Sometimes these defects are detected when
echocardiographic studies are performed for some unrelated reason. A few patients do
present with symptoms of heart failure in infancy, although this is uncommon.
2.Physical examination.9
The right ventricular and right ventricular outflow tract impulses are increased and
hyperdynamic. No thrills are usually felt. The second heart sound is widely split and fixed
(splitting does not vary with respiration) and is the most characteristic sign of ASD. Ejection
systolic clicks are rare with ASDs. The ejection systolic murmur of ASD is soft and is of
grade I-II/VI intensity and rarely, if ever, louder. The murmur is secondary to increased
blood flow across the pulmonary valve and is heard best at the left upper sternal border. A
grade I-II/VI mid-diastolic flow rumble is heard (with the bell of the stethoscope) best at the
left lower sternal border. This is due to large volume flow across the tricuspid valve. There is no
audible murmur because of flow across the ASD.9
3. Noninvasive evaluation
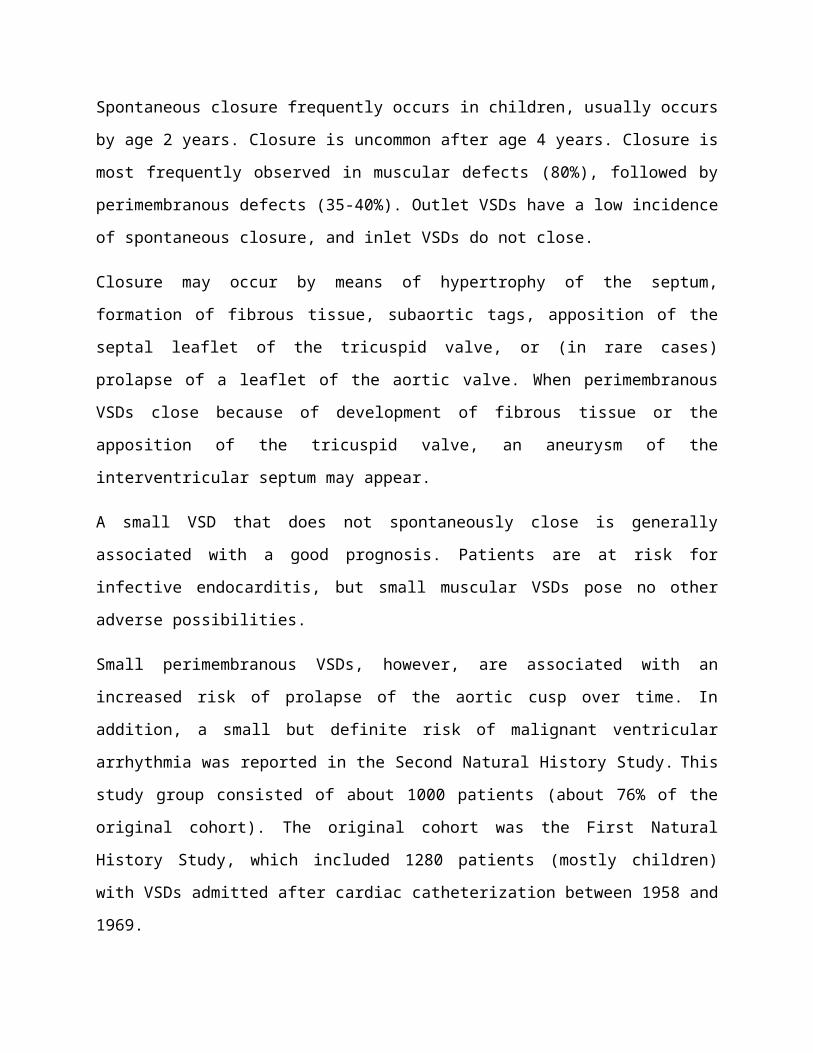
3.1. Chest x-ray
Chest film usually reveals mild to moderate cardiomegaly, prominent main pulmonary artery segment and increased pulmonary vascular markings.9
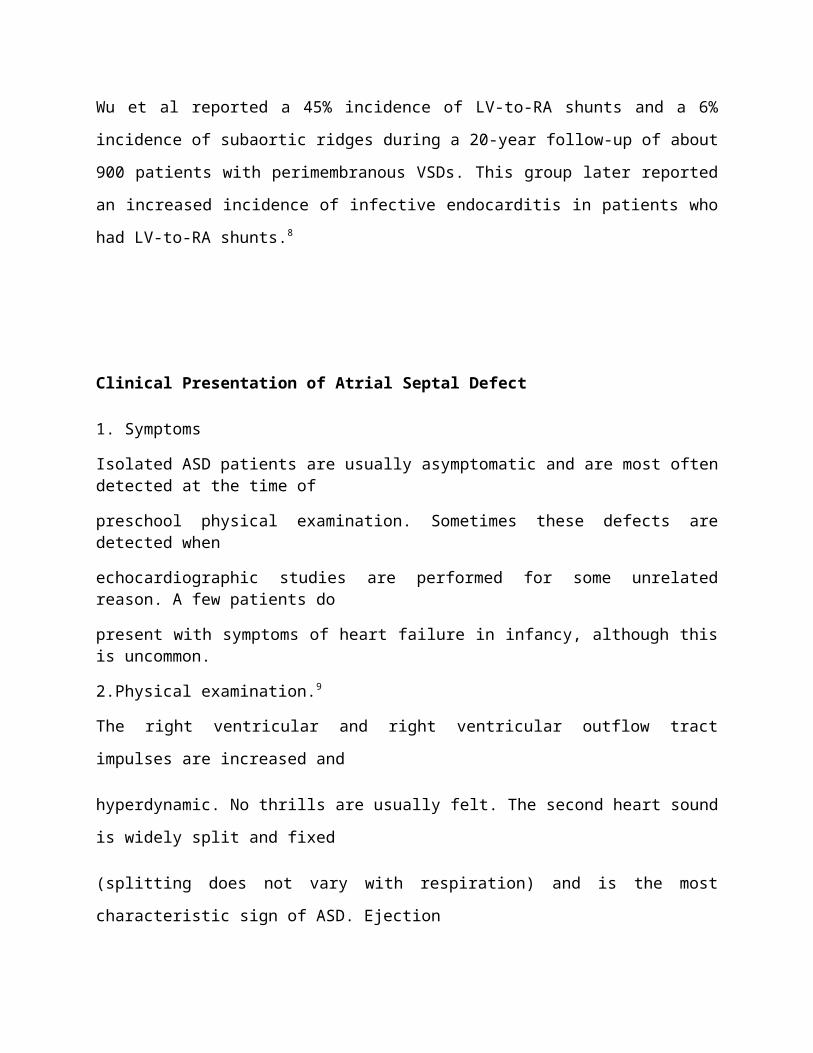
3.2. Electrocardiogram
This ECG also shows right atrial overload as evidenced by P wave amplitude of 0.3 mV in lead
II. Incomplete RBBB pattern is seen as slurred S waves in lead I and rSrS pattern in V1..9
3.3. Echocardiogram
Echocardiographic studies reveal enlarged right ventricle with paradoxical septal motion,
particularly well-demonstrable on M-mode echocardiograms in patients with moderate to
large ASDs. Dilatation of the right ventricle may not be present in small defects.9
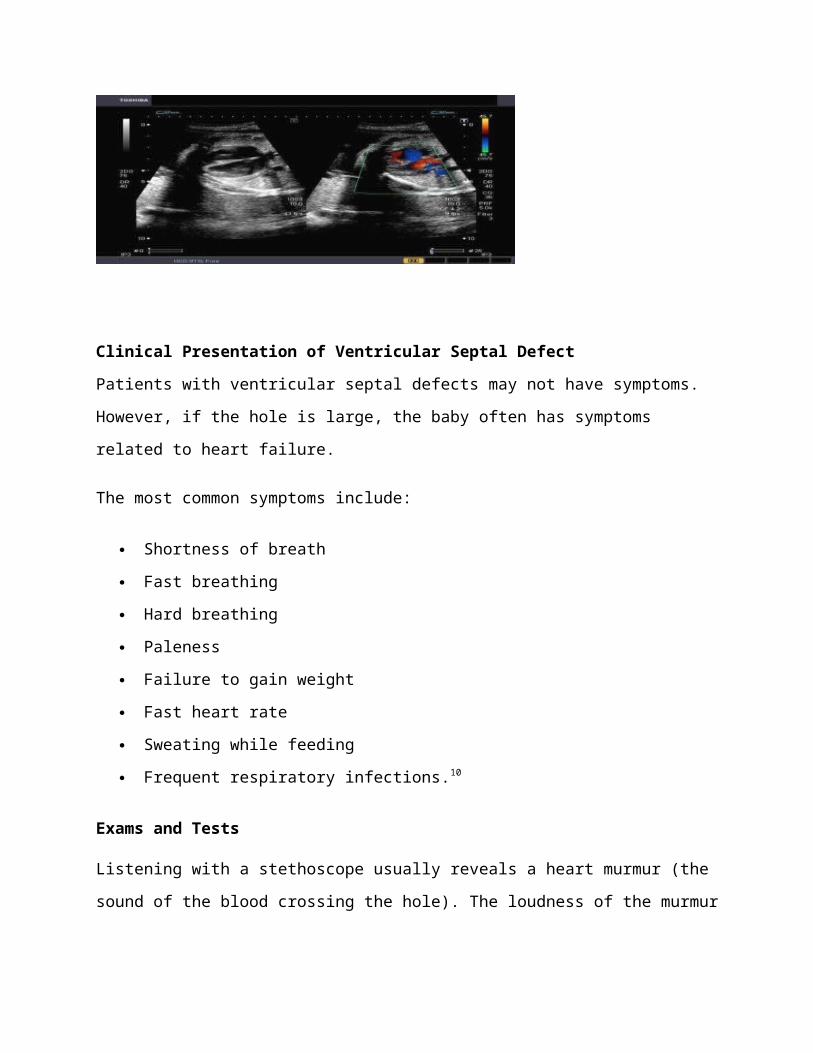
Clinical Presentation of Ventricular Septal Defect
Patients with ventricular septal defects may not have symptoms. However, if the hole is large,
the baby often has symptoms related to heart failure.
The most common symptoms include:
Shortness of breath
Fast breathing
Hard breathing
Paleness
Failure to gain weight
Fast heart rate
Sweating while feeding
Frequent respiratory infections.10
Exams and Tests
Listening with a stethoscope usually reveals a heart murmur (the sound of the blood crossing the
hole). The loudness of the murmur is related to the size of the defect and amount of blood
crossing the defect.
Tests may include:
Cardiac catheterization (rarely needed, unless there are concerns of high blood pressure
in the lungs)
Chest x-ray -- looks to see if there is a large heart with fluid in the lungs
ECG -- shows signs of an enlarged left ventricle
Echocardiogram -- used to make a definite diagnosis
MRI of the heart -- used to find out how much blood is getting to the lungs.10
Treatment
1. Treatment of Atrial Septal Defect
Treatment of an ASD depends on the type and size of the defect, its effect on the heart, and the
presence of any other related conditions, such as pulmonary hypertension, valve disease or
coronary artery disease. In general, when a patient has a large ASD that causes significant
shunting (flow of blood through the defect) and right-sided heart enlargement, Cleveland Clinic
specialists recommend correcting the defect. The size of the defect correlates with the degree of
shunting—the more shunting, the greater the risk of long-term complications such as atrial
fibrillation and pulmonary hypertension. The degree of shunting is determined by
echocardiography, MRI or oxygen saturations measured during catheterization. The degree of
right-heart enlargement, as measured by echocardiography or MRI, usually correlates with the
degree of shunting.11
ASD Repair
Nonsurgical Treatment
Nonsurgical, percutaneous (through the skin) repair is the preferred treatment for most secundum
ASDs, but surgery may be needed to repair other types of ASDs (see Surgerical Repair section
below for more information). Your doctor will determine what type of repair procedure is best
for you.Two different brands of closure devices are approved by the U.S. Food and Drug
Administration for percutaneous ASD closure—Amplatzer® Septal Occluder and the GORE
HELEX® Septal Occluder. The closure devices differ in design, but the placement method and
their function are similar.The device is attached to a catheter, which is inserted into a vein in the
groin and advanced to the heart and through the defect, guided by X-ray and intracardiac echo.
As the device slowly is pushed out of the catheter, it opens up to cover each edge of the defect,
sealing it closed. Over time, tissue grows over the implant and it becomes part of the heart.
Before a percutaneous closure device procedure, the patient will have a cardiac catheterization to
determine the size and location of the defect. Pressures inside the heart chambers also will be
measured. For at least the first six months after the repair, the patient will need to take an
anticoagulant such as aspirin, clopidogrel or warfarin (Coumadin) to prevent clots from forming
on the device.11
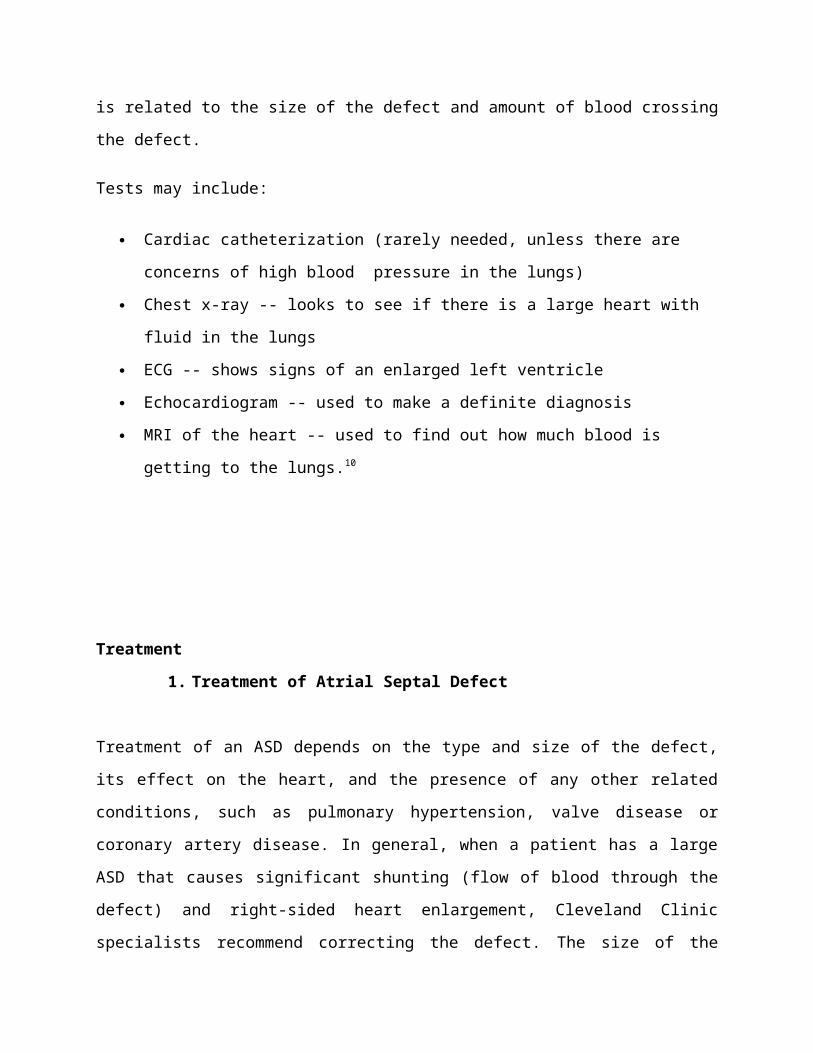
Percutaneous Closure Devices for ASD Repair
AMPLATZER® Septal Occluder
The AMPLATZER® Septal Occluder is a transcatheter closure device used to treat ASDs. It
consists of two Nitinol wire mesh discs filled with polyester fabric. It is folded into a special
delivery catheter, similar to the catheter used to cross the heart defect during catheterization.
The catheter is inserted into a vein in the leg, advanced into the atrial septum and through the
defect. When the catheter is in the proper position, the device slowly is pushed out of the catheter
until the discs of the device sit on each side of the defect, like a sandwich. The two discs are
linked together by a short connecting waist that matches the size of the defect. The discs and the
waist are filed with polyester fabric to increase the device’s closing ability. Over time, heart
tissue grows over the implant, and it becomes part of the heart, permanently correcting the
defect.
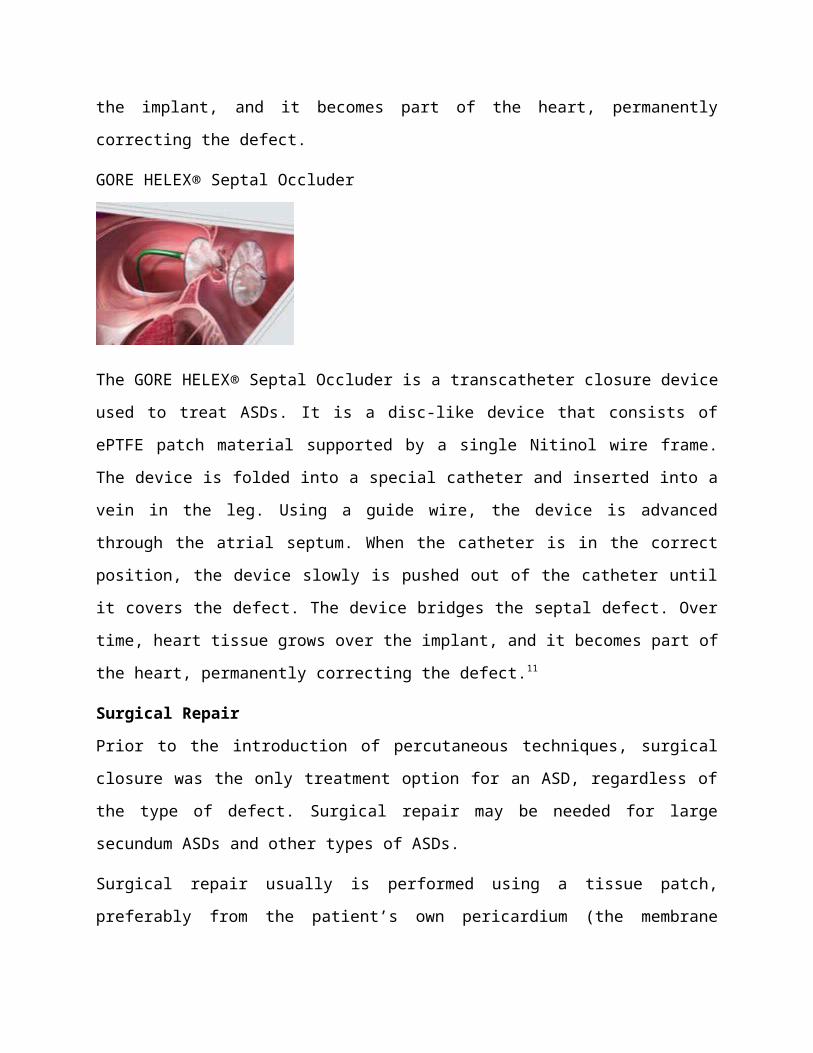
GORE HELEX® Septal Occluder
The GORE HELEX® Septal Occluder is a transcatheter closure device used to treat ASDs. It is a
disc-like device that consists of ePTFE patch material supported by a single Nitinol wire frame.
The device is folded into a special catheter and inserted into a vein in the leg. Using a guide wire,
the device is advanced through the atrial septum. When the catheter is in the correct position, the
device slowly is pushed out of the catheter until it covers the defect. The device bridges the
septal defect. Over time, heart tissue grows over the implant, and it becomes part of the heart,
permanently correcting the defect.11
Surgical Repair
Prior to the introduction of percutaneous techniques, surgical closure was the only treatment
option for an ASD, regardless of the type of defect. Surgical repair may be needed for large
secundum ASDs and other types of ASDs.
Surgical repair usually is performed using a tissue patch, preferably from the patient’s own
pericardium (the membrane around the heart). Some secundum ASDs can be surgically closed
with sutures alone.11
Follow-Up Care
The patient usually returns to the cardiologist 3, 6 and 12 months after a procedure for a follow-
up physical exam and echocardiogram, and once a year thereafter. After a secundum ASD is
repaired, most people can return to their regular activities without any activity restrictions (other
than those associated with all heart catheterizations). Patients usually take a blood thinner for six
months to a year after the repair to prevent blood clots and help the healing process. Patients who
have had a stroke may need to take blood thinners indefinitely, and those with other heart
problems, such as coronary artery disease or pulmonary hypertension, may need to take
additional medication.
Patients who have heart surgery to repair a defect or receive a transcatheter closure device will
need to take preventive antibiotics for at least six months after the repair procedure to reduce the
risk of infective endocarditis. The doctor will provide specific guidelines about when to take
antibiotics. According to the American Heart Association, there is not enough evidence
to recommend taking preventive antibiotics for longer than six months.11
2. Treatment of Ventricular Septal Defect
Medical Management
The management in the infant and child depends on symptoms. A small defect does not require
medical management or likely require any intervention. The medium and larger defects require
various degrees of medical management and eventual surgical closure. Congestive heart failure
in the infant is treated with diuretics, digoxin, and afterload reduction at times.
The adult with an unrepaired VSD in the current era likely has a small defect without evidence of
left ventricular volume overload or alterations in the adjacent structures. Those with evidence of
left ventricular volume overload or progressive aortic valve disease in most institutions are
referred for closure.
The adult who has had VSD repair needs surveillance for aortic valve dysfunction. Those adults
with residual defects need continued monitoring and consideration for reoperation if there is left
ventricular volume overload or progressive aortic valve dysfunction.
The patient with Eisenmenger syndrome needs very specialized care at centers, with trained
personnel capable of managing myriad medical problems. Arrhythmias, endocarditis, gallstones,
gouty arthritis, hemoptysis, pulmonary artery thrombosis, and symptomatic hypertrophic
osteoarthropathy are frequently seen. Pregnancy is poorly tolerated and many believe
contraindicated in this disorder. Echocardiography and magnetic resonance imaging are used to
evaluate right ventricular function. Cardiac catheterization is reserved for cases in which surgical
or device closure is a question. Vasodilator therapy is an important adjunct to management and
can provide functional improvement. Changes in VN O2with exercise or Qp:Qs from magnetic
resonance imaging–derived cardiac output can be determined but are not generally used to guide
therapy.
Endocarditis is a lifelong risk in unoperated patients (18.7 per 10 000 patient-years) and those
with residual defects. Proper prophylaxis and periodic follow-up are indicated.12
Surgical Closure
Location has been used as an indication for surgical closure regardless of the need for medical
management in the case of infundibular defects. Chamber enlargement is another measure of the
degree of shunting and may indicate the need for closure. Catheterization can be used in some
individuals to determine Qp:Qs and pulmonary artery pressure and resistance to help guide
clinicians. Generally, a Qp:Qs of 1.5:1 to 2:1 or evidence of increased pulmonary arteriolar
resistance is an indication for closure. Multiple “Swiss cheese” defects refractory to medical
management may require a palliative pulmonary artery band procedure.
Advances in surgical and bypass techniques and timing of surgical repair have decreased the
morbidity associated with surgical closure. The early era of repair showed an 80% closure rate in
catheterized patients at long-term follow-up. In that study, 9 of 258 patients had complete heart
block, 37 had transient heart block, and 168 had right bundle-branch block. Endocarditis
occurred in 9 patients (11.4 of 10 000 patient-years).
More recent studies have shown residual defects in 31% of patients and an incidence of complete
heart block of 3.1%. Another natural history study showed occurrence rates for pacemaker
placement of 9.8 per 10 000 patient-years and occurrence rates for endocarditis of 16.3 per 10
000 patient-years in operated patients.12
Catheter Closure
Advancements in catheter techniques and devices are leading us into the era of percutaneous
closure of VSDs. The benefits of avoiding bypass are intuitive, and the relative ease of
placement makes this procedure ultimately attractive. Currently, these devices are in the
investigational stage. In 1987, Lock and colleagues used the Rashkind double-umbrella device to
close VSDs. The defects closed in that study included congenital, postoperative congenital, and
post–myocardial infarction VSDs. The Amplatzer VSD occluder, of which there are the
muscular and perimembranous types (AGA Medical Corp, Golden Valley, Minn), is another
investigational devices. A phase 1 clinical trial for the Amplatzer membranous device showed a
96% complete closure rate at 6 months with a serious adverse event rate of 8.6%. Likewise, there
was 100% occlusion of single defects at 3 to 96 months of follow-up with the Amplatzer
muscular VSD occluder. Using the device for iatrogenic defects after aortic valve replacement
has also been successful.
Imaging during deployment traditionally has been transesophageal echocardiography.
Intracardiac echocardiography can now be used with accurate measurements and safety similar
to that with transesophageal echocardiography.
Device placement is not without its own risks and potential long-term complications. Complete
heart block has been observed as a temporary complication in 1.07% to 1.9% of patients. There
was also transient bundle-branch block in 2.8%. There was no late development of complete
heart block. Tricuspid stenosis was seen in 1 patient requiring ballooning of the valve as a result
of hemodynamic instability, after which the stenosis was reduced and remained stable. Tricuspid
regurgitation developed in 1 patient (0.7%). Placement failure was experienced by 5.1% of
patients as a result of proximity to the aortic valve and acute insufficiency, chordae of the
tricuspid valve, and inability to pass the delivery sheath.
Studies using an open chest animal model and perventricular technique for device deployment
have been successful for perimembranous defects. A similar technique has been used for
muscular or multiple muscular defects. This provides a further reduction in the invasiveness of
closure and could allow therapy for those with contraindications to bypass in the future.12
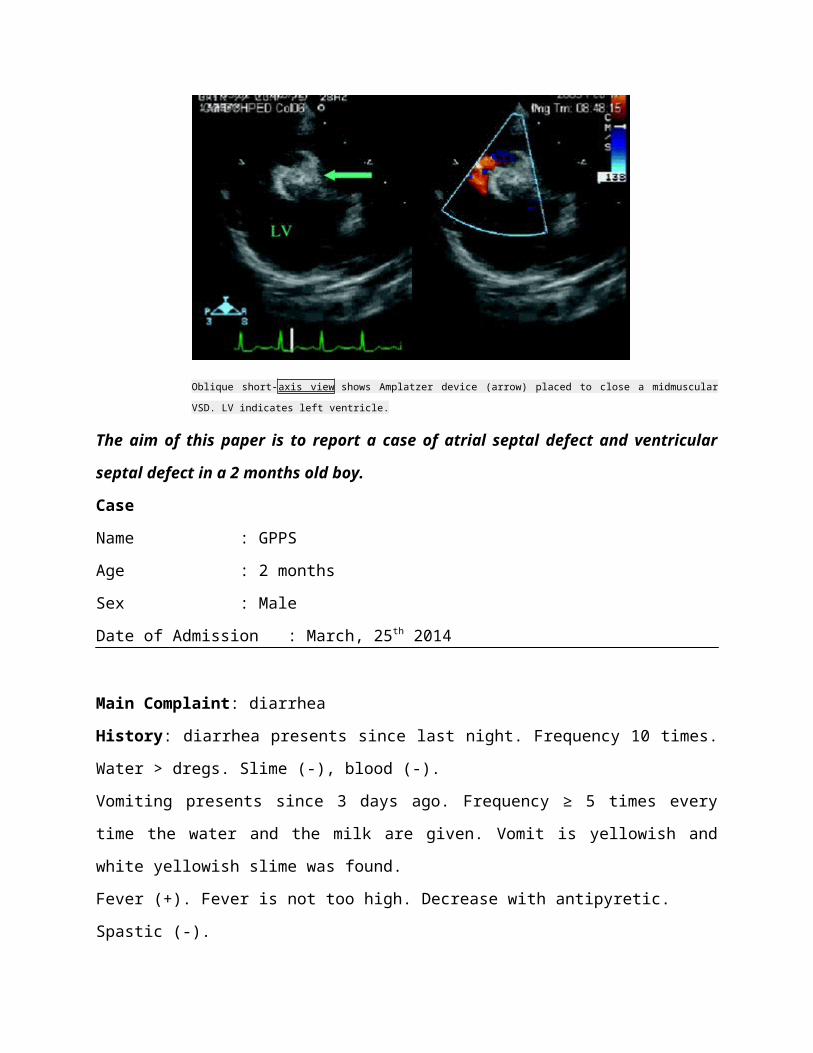
Oblique short-axis view shows Amplatzer device (arrow) placed to close a midmuscular VSD. LV
indicates left ventricle.
The aim of this paper is to report a case of atrial septal defect and ventricular septal defect in a
2 months old boy.
Case
Name : GPPS
Age : 2 months
Sex : Male
Date of Admission : March, 25th 2014
Main Complaint: diarrhea
History: diarrhea presents since last night. Frequency 10 times. Water > dregs. Slime (-), blood
(-).
Vomiting presents since 3 days ago. Frequency ≥ 5 times every time the water and the milk are
given. Vomit is yellowish and white yellowish slime was found.
Fever (+). Fever is not too high. Decrease with antipyretic.
Spastic (-).
Decreasing weight (+). Presents since 29 days ago when was hospitalized in RSUP Lubuk
Pakam.
Cyanotic (-). History of cyanotic (-).
Shortness of breath (-).
History of previous illness : the patient was referred from RSU Medistra Lubuk Pakam by a
general practitioner. Hospitalized for 1 night in RSU Medistra with diagnosis GE mild-moderate
dehydration. Was hospitalized in RSU Lubuk Pakam for 29 days. according to patients’ parents,
the patient has a heart disorder without knowing the name of the disorder.
History of previous medications: D10% 10 gtt/i micro
History of labor :secsio caesaria , no cyanosis
History of feeding :breast milk
History of immunization : (-)
Presens status
Sensorium : Compos Mentis Anemis : ( -)
Body temperature : 37,9oC Icteric : (-)
Respiratory Rate : 32 x/minute Cyanosis : (-)
Pulse : 170 bpm Dyspnea : ( -)
Physical Examination
weight : 2435 gr BW/Age: %
length : 47 cm BH/Age: %
Upper Arm Circumference (UAC): cm BW/BH: %
Abdomen Circumference (AC) : cm
1. Head: fonticulus anterior flatly opened. Eye: light reflexes(+/+), isocor pupil, pale
conjunctiva palpebra inferior (-/-), icteric (-/-), Ear : normal, Nose: normal, Mouth:
normal,
2. Neck: Lymph node enlargement (-), cannon wave (+), TVJ R+ 0 cmH2O
3. Thorax : Symmetrical fusiformis, retraction (-)
HR: 170 bpm, regular, continous murmur (+) grade III/6, LMCS III-IV
RR: 32 x/minute, regular, crackles (-/-), wheezing (-)
Abdomen: soepel, peristaltic (+) normal. Liver/Spleen/Renal: not palpable. Anogenital :
male, Anus (-)
4. Extremities: Baggy pants (+). Muscle hypotrophy (+). Thinning subcutaneous fat (+).
Pulse 170 bpm, regular, adequate vascular pressure and volume,
Warm acral, CRT< 3”, swelling (+), BP : 100/60 mmhg
Working Diagnosis
GE mild-moderate dehydration + failure to thrive + acyanotic CHD ec ASD/VSD/PDA
Treatment
IVFD RL 75cc/kgBW/4hr 45cc/hr RL maintenance
Follow up on March 25th 2014
S : diarrhea (+), fever (-), vomit (-)
O: Sensorium: ComposMentis, Body temperature: 36,8oC, RespiratoryRate: 32x/minute, Pulse:
110 bpm,Anemis (-),Icteric (-),Cyanosis(-),Dyspnea(-)
Head : Eye: light reflexes(+/+), isocor pupil, pale conjunctiva
palpebrainferior (-/-), icteric (-/-), Ear : normal, Nose:
normal, Mouth: normal
Neck : Lymph node enlargement (-)
Thorax : Symmetrical fusiformis, retraction (-),HR: 110 bpm, regular,
continous murmur (+) grade III/6, LMCS III-IV,RR: 32 x/minute, regular,
crackles
(-/-), wheezing (-)
Abdomen: soepel, peristaltic (+) normal,Liver/Spleen/Renal: not palpable,
Anogenital : male, Anus (-)
Extremities : Pulse 110 bpm, regular, adequate vascular pressure and volume,
warmacral, CRT< 3”
A : GE mild-moderate dehydration + failure to thrive + acyanotic CHD ec ASD/VSD/PDA
P:
IVFD RL 75cc/kgBW/4hr 45cc/hr IVFD D5% NaCl 0,225% 10 gtt/i
Vit. A 100.000 IU
Multivitamin without Fe 3xcthI
Zinc 1x10mg
Diet Neosure 30cc/2hr/NGT + 0,5cc mineral mix
Laboratory findings on March 25th 2014:
Carbohydrate metabolism : Random blood glucose 116 mg/dL
Electrolyte : Na 132 mEq, K 4.7 mEq, Cl 101 mEq
Complete Blood Count : HGB 7.5 g%, RBC 2.56 106/mm3, WBC 23.79103/mm3, haematocryte
22.7 %,Trombocyte 489 103/mm3, MCV 88.70 fL, MCH 29.30 pg, MCHC 33 g%, RDW 15.50
%, MPV 9.20 fL, PCT 0.45 %, PDW 9.8 fL, Neutrophil 77.90 %, lymphocyte 9.70 %, monocyte
11.70 %, eosinophil 0.30 %, basophil 0.400 %, Absolute neutrophil 18.52 103/µL, Absolute
lymphocyte 2.3 103/µL, Absolute monocyte 2.79 103/µL, Absolut eosinophil 0.08 103/µL,
Absolute basophil 0.10 103/µL.
Renal : urea 50.30, creatine 0.27
Advices : consult to nutrition and cardiology division
Follow up on March 26th 2014
S : diarrhea (-), fever (-), vomit (-)
O: Sensorium: ComposMentis, Body temperature: 37,1oC, RespiratoryRate: 20x/minute, Pulse:
110 bpm,Anemis (-),Icteric (-),Cyanosis(-),Dyspnea(-)
Head : Eye: light reflexes(+/+), isocor pupil, pale conjunctiva
palpebrainferior (-/-), icteric (-/-), Ear : normal, Nose:
normal, Mouth: normal
Neck : Lymph node enlargement (-)
Thorax : Symmetrical fusiformis, retraction (-),HR: 110 bpm, regular,
continous murmur (+) grade III/6, LMCS III-IV,RR: 20 x/minute, regular,
crackles (-/-), wheezing (-)
Abdomen: soepel, peristaltic (+) normal,Liver/Spleen/Renal: not palpable,
Anogenital : male, Anus (-)
Extremities : Pulse 110 bpm, regular, adequate vascular pressure and volume,
Warm acral, CRT< 3”
A : GE without dehydration + failure to thrive + acyanotic CHD ec ASD & VSD
P :
IVFD D5% NaCl 0,225% 10 gtt/i
Multivitamin without Fe 3xcthI
Zinc 1x10mg
Diet Neosure 30cc/2hr/NGT + 0,5cc mineral mix
Laboratory findings on March 26th 2014
ALP/AST/ALT : 95 / 53 / 43
Follow up on March 8th 2014
S : shortness of breathing (+)
O: Sensorium: Compos Mentis, Body temperature: 37.0oC ,
RespiratoryRate:32x/minute,Pulse: 118 bpm,Anemis (-),Icteric (-),Cyanosis(-),Dyspnea(+),
Weight: 20 kg, Height: 139 cm, UAC : 14 cm
Head :Eye: light reflexes(+/+), isocor pupil, pale conjunctiva palpebrainferior (-/-),
icteric (-/-), Ear : normal, Nose: normal, Mouth: normal
Neck : Lymph node enlargement (-),TVJ R+ 0 cmH2O
Thorax : Symmetrical fusiformis, retraction (-), Ictus (+), thrill(+)
HR: 100 bpm, regular, continous murmur (+) grade 4/6 lower mid
clavicula sinistra ICR IV-V, RR: 30 x/minute, regular, crackles
(-/-), wheezing (-)
Abdomen: soepel, peristaltic (+) normal,liver: palpable 4 cms below
the right Arcus costa, Spleen/Renal: not palpable,
Anogenital: female, Anus (+)
Extremities: Pulse 100 bpm, regular, adequate vascular pressure and volume,
warmacral, CRT< 3”, BP : 100/60 mmhg
A : Congestive Heart Failure ec moderate Patent Ductus Arteriosus+ mild PE+ vegetation of
pulmonary valve+mild Mitral insufficiency+ mild Tricuspid Insufficiency+ mild
Pulmonary insufficiency
P: Total bed rest
Semi fowler position
O2 1-2 L/minutes nasal canule
Ceftriaxone injection 1000 mg/12 hour/IV (day 2)
Gentamycin injection so mg/12 hour/ (day 2)
Furosemide injection 20 mg/12 hour/IV
Spironolacton 2x12,5 mg
Captopril 2x6,25 mg
Regular diet low salt 1500 kkal + 40 gr protein
Fluid balance every 6 hours
PRC transfusion 60 cc B+
Follow up on March 9th -10th 2014
S:shortness of breathing (+), cough (+), fever (+)
O:Sensorium: Compos Mentis, Body temperature: 37.9oC ,
RespiratoryRate:32x/minute,Pulse: 118 bpm,Anemis (-),Icteric (-),Cyanosis(-),Dyspnea(+),
Weight: 20 kg, Height: 139 cm, UAC : 14 cm
Head :Eye: light reflexes(+/+), isocor pupil, pale conjunctivapalpebrainferior (-/-),
icteric (-/-), Ear : normal, Nose: normal, Mouth: normal
Neck : Lymph node enlargement (-),TVJ R+ 0 cmH2O
Thorax : Symmetrical fusiformis, retraction (-), Ictus (+), thrill(+)
HR: 100 bpm, regular, continous murmur (+) grade 4/6 lower mid
clavicula sinistra ICR IV-V, RR: 30 x/minute, regular, crackles
(-/-), wheezing (-)
Abdomen: soepel, peristaltic (+) normal,liver: palpable 4 cms below
the right Arcus costa, Spleen/Renal: not palpable,
Anogenital: female, Anus (+)
Extremities: Pulse 100 bpm, regular, adequate vascular pressure and volume,
warmacral, CRT< 3”, BP : 100/60 mmhg
A : Congestive Heart Failure ec moderate Patent Ductus Arteriosus+ mild PE+ vegetation
of pulmonary valve+mild Mitral insufficiency+ mild Tricuspid Insufficiency+ mild Pulmonary
insufficiency
P: Total bed rest
Semi fowler position
O2 1-2 L/minutes nasal canule
Ceftriaxone injection 1000 mg/12 hour/IV (day 2)
Gentamycin injection so mg/12 hour/ (day 2)
Furosemide injection 20 mg/12 hour/IV
Spironolacton 2x12,5 mg
Captopril 2x6,25 mg
Reguler diet low salt 1500 kkal + 40 gr protein
PRC transfusion 60 cc (9th)and 100 cc (10th)
Follow up on March 11th-13th 2014
S:shortness of breathing (+), cough (+), fever (+)
O:Sensorium: Compos Mentis, Body temperature: 38.2oC ,
RespiratoryRate:32x/minute,Pulse: 118 bpm,Anemis (-),Icteric (-),Cyanosis(-),Dyspnea(+),
Weight: 20 kg, Height: 139 cm, UAC : 14 cm
Head :Eye: light reflexes(+/+), isocor pupil, pale conjunctivapalpebrainferior (-/-),
icteric (-/-), Ear : normal, Nose: normal, Mouth: normal
Neck : Lymph node enlargement (-),TVJ R+ 0 cmH2O
Thorax : Symmetrical fusiformis, retraction (-), Ictus (+), thrill(+)
HR: 100 bpm, regular, continous murmur (+) grade 4/6 lower mid
clavicula sinistra ICR IV-V, RR: 30 x/minute, regular, crackles
(-/-), wheezing (-)
Abdomen: soepel, peristaltic (+) normal,liver: palpable 4 cms below
the right Arcus costa, Spleen/Renal: not palpable,
Anogenital: female, Anus (+)
Extremities: Pulse 100 bpm, regular, adequate vascular pressure and volume,
warmacral, CRT< 3”, BP : 100/60 mmhg
A : Congestive Heart Failure ec moderate Patent Ductus Arteriosus+ mild PE+ vegetation
of pulmonary valve+mild Mitral insufficiency+ mild Tricuspid Insufficiency+ mild Pulmonary
insufficiency
P: Total bed rest
Semi fowler position
O2 1-2 L/minutes nasal canule
Ceftriaxone injection 1000 mg/12 hour/IV (day 2)
Gentamycin injection so mg/12 hour/ (day 2)
Furosemide injection 20 mg/12 hour/IV
Spironolacton 2x12,5 mg
Captopril 2x6,25 mg
Reguler diet low salt 1500 kkal + 40 gr protein
Ambroxol syr 3x 1 cth
Balance every 6 hours
Dipstick result (12th March 2014)
Leu Nit Uro Pro PH BLO SG Ket Bil Glu
- + 0.2(3x) 15(0.15)± 5.0 +++ 1.020 - - -
Follow up on March 14th-20th 2014
S:shortness of breathing (+), cough (+), fever (-)
O:Sensorium: Compos Mentis, Body temperature: 37.2oC , Respiratory Rate:36 x/minute,
Pulse: 112bpm, Anemis (-),Icteric (-),Cyanosis(-),Dyspnea(+), Weight: 20 kg, Height: 139 cm,
UAC : 14 cm, BP: 100/50 mmhg
Head : Eye: light reflexes(+/+), isocor pupil, pale conjunctiva
palpebrainferior (-/-), icteric (-/-), Ear : normal, Nose: normal, Mouth: normal
Neck : Lymph node enlargement (-),TVJ R+ 0 cmH2O
Thorax : Symmetrical fusiformis, retraction (-), Ictus (+), thrill(+)
HR: 100 bpm, regular, continous murmur (+) grade 4/6 lower mid clavicula
sinistra ICR II-III,RR: 22 x/minute, regular, crackles (-/-), wheezing (-)
Abdomen : soepel, peristaltic (+) normal,liver: palpable 4 cms below
the right Arcus costa, Spleen/Renal: not palpable,
Anogenital : female, Anus (+)
Extremities : Pulse 112 bpm, regular, adequate vascular pressure and volume,
warmacral, CRT< 3”, swelling (+), BP : 100/60 mmhg
A : Congestive Heart Failure ec moderate Patent Ductus Arteriosus+ mild PE+ vegetation of
pulmonary valve+mild Mitral insufficiency+ mild Tricuspid Insufficiency+ mild
Pulmonary insufficiency
P: Total bed rest
Semi fowler position
O2 1-2 L/minutes nasal canule
Ceftriaxone injection 1000 mg/12 hour/IV (day 2)
Gentamycin injection so mg/12 hour/ (day 2)
Furosemide injection 20 mg/12 hour/IV
Spironolacton 2x12,5 mg
Captopril 2x6,25 mg
Ambroxol syr 3x 1 cth
Balance every 6 hours
Regular diet low salt 1500 kkal + 40 gr protein
Laboratory findings on March 14th – 20th 2014
Immunoserology : Total T3 0.88ng/ml, Total T4 1.68 µg/ml, TSH 4.890 µIU/ml, qualitative
CRP (+), Procalcitonin 0.36 ng/ml
Electrolyte: Na 130 mEq/L, K 4.6 mEq/L, chloride 97 mEq/L
Complete Blood Count : HGB 11.60 g%, RBC 4.23 106/mm3, WBC 13.35 106/mm3,
haematocryte 35.50 %,Trombocyte 379 106/mm3, MCV 83.90 fL, MCH 27.40 pg, MCHC 32.70
g%, RDW 16.30%, MPV 8.70 fL, PCT 0.33 %, PDW 9.1 fL, Neutrophil 64.50 %, lymphocyte
20.10 %, monocyte 13.90 %, eosinophil 1.00 %, basophil 0.500 %, Absolute neutrophil 8.59
106/µL, Absolute lymphocyte 2.69 106/µL, Absolute monocyte 1.86 106/µL, Absolut eosinophil
0.14 106/µL, Absolute basophil 0.07 106/µL.
Follow up on March21st-24th 2014
S:shortness of breathing start to decrease, the food was not finished, cough(+)
O:Sensorium: Compos Mentis, Body temperature: 37.0oC , Respiratory Rate:34 x/minute,
Pulse: 108bpm, Anemis (-),Icteric (-),Cyanosis(-),Dyspnea(+), Weight: 20 kg, Height : 139
cm, UAC : 14 cm, BP: 100/50 mmhg,BBM: 17.5 kg, BBS: 17.5 kg, LLA : 13 cm
,BW/BH: 67.3%, BW/age : 46.05 %,BH/age: 88.15%
Head : Eye: light reflexes(+/+), isocor pupil, pale conjunctiva
palpebrainferior (-/-), icteric (-/-), Ear : normal, Nose: normal, Mouth: normal
Neck : Lymph node enlargement (-),TVJ R+ 0 cmH2O
Thorax : Symmetrical fusiformis, retraction (-), Ictus (+), thrill(+)
HR: 100 bpm, regular, continous murmur (+) grade 4/6 lower mid clavicula
sinistra ICR II-III
RR: 22 x/minute, regular, crackles (-/-), wheezing (-)
Abdomen : soepel, peristaltic (+) normal,liver: palpable 4 cms below
the right Arcus costa, Spleen/Renal: not palpable, Anogenital : female,
Anus (+)
Extremities : Pulse 100 bpm, regular, adequate vascular pressure and volume,
warmacral, CRT< 3”, swelling (+), BP : 100/60 mmhg
A : Congestive Heart Failure ec moderate Patent Ductus Arteriosus+ mild PE+ vegetation of
pulmonary valve+mild Mitral insufficiency+ mild Tricuspid Insufficiency+ mild
Pulmonary insufficiency+ marasmus type of malnutrition
P: Total bed rest
Semi fowler position
O2 1-2 L/minutes nasal canule
Ceftriaxone injection 1000 mg/12 hour/IV (day 2)
Gentamycin injection so mg/12 hour/ (day 2)
Furosemide injection 20 mg/12 hour/IV
Spironolacton 2x12,5 mg
Captopril 2x6,25 mg
Ambroxol syr 3x 1 cth
Balance every 6 hours
Reguler diet low salt 1500 kkal + 40 gr protein
Diet F100 125 cc/2 jam
Multivitamin without Fe 1x1 cth
Folic acid 1x 5 mg
R/ consule to Departement of Oral and Dental health
Consultation results from cardiology dept : repeat the Echocardiography after 6-8 weeks of
therapy
Culture result:
Throat swab culture: Streptococcus aglactie
Sensitif: Ceftriaxon, levolinezolid,levofloxacin
Resisten: Ampicilin,
azitromicin,erythromycin,clindamicin
Follow up 25th-27th March 2014
S: shortness of breathing (+), cough (+), fever (-),food was finished
O:Sensorium: Compos Mentis, Body temperature: 37.0oC , Respiratory Rate:34 x/minute,
Pulse: 108bpm, Anemis (-),Icteric (-),Cyanosis(-),Dyspnea(+), Weight: 20 kg, Height: 139 cm,
UAC : 14 cm, BP: 100/50 mmhg, BBM : 17.5 kg, UAC : 14 cm ,BH/age : 88.9 %, BBS :18
kg, BW/age: 46.5 %, BW/BH : 70.1 %
Head : Eye: light reflexes(+/+), isocor pupil, pale conjunctiva
palpebrainferior (-/-), icteric (-/-), Ear : normal, Nose: normal, Mouth: normal
Neck : Lymph node enlargement (-),TVJ R+ 0 cmH2O
Thorax : Symmetrical fusiformis, retraction (-), Ictus (+), thrill(+)
HR: 100 bpm, regular, continous murmur (+) grade 4/6 lower mid clavicula
sinistra ICR II-III
RR: 22 x/minute, regular, crackles (-/-), wheezing (-)
Abdomen : soepel, peristaltic (+) normal,liver: palpable 4 cms below
the right Arcus costa, Spleen/Renal: not palpable, Anogenital : female,
Anus (+)
Extremities : Pulse 100 bpm, regular, adequate vascular pressure and volume,
warmacral, CRT< 3”, swelling (+), BP : 100/60 mmhg
A : CHF ec moderate PDA+Mild PE+vegetation of the pulmonary valve+mild tricuspid
insufficiency+mild pulmonal insufficiency+ marasmus+ caries dentis+ ginggival pulpa
P: Bed rest+ semi fowler position
O2 1 liter/minute nasal canule (intermitten)
Furosemide injection 20 mg/12 hours/IV
Spironolacton 2x12.5 mg
Captopril 2x6,25 mg
Ampicilin injection 1 gram/6 hours/IV(day 12)
Gentamycin injection 50 mg/12 hours/IV (day 22)
Ambroxol syrup 3x1 Cth
Folic acid 1x5 mg
Multivitamin without Fe 1x1 cth
regular diet 1000 kkal + fluid consistency diet (F100) 3 x 200 cc
Follow up 28th-29th March 2014
S: shortness of breathing (+), cough (+), fever (-),food was finished
O:Sensorium: Compos Mentis, Body temperature: 37.0oC , Respiratory Rate:34 x/minute,
Pulse: 108bpm, Anemis (-),Icteric (-),Cyanosis(-),Dyspnea(+), Weight: 20 kg, Height: 139 cm,
UAC : 14 cm, BP: 100/50 mmhg, BBM : 17.5 kg, UAC : 14 cm ,BH/age : 88.9 %, BBS :18
kg, BW/age: 46.5 %, BW/BH : 70.1 %
Head : Eye: light reflexes(+/+), isocor pupil, pale conjunctiva
palpebrainferior (-/-), icteric (-/-), Ear : normal, Nose: normal, Mouth: normal
Neck : Lymph node enlargement (-),TVJ R+ 0 cmH2O
Thorax : Symmetrical fusiformis, retraction (-), Ictus (+), thrill(+)
HR: 100 bpm, regular, continous murmur (+) grade 4/6 lower mid clavicula
sinistra ICR II-III
RR: 22 x/minute, regular, crackles (-/-), wheezing (-)
Abdomen : soepel, peristaltic (+) normal,liver: palpable 4 cms below
the right Arcus costa, Spleen/Renal: not palpable, Anogenital : female,
Anus (+)
Extremities : Pulse 100 bpm, regular, adequate vascular pressure and volume,
warmacral, CRT< 3”, swelling (+), BP : 100/60 mmhg
A : CHF ec moderate PDA+Mild PE+vegetation of the pulmonary valve+mild tricuspid
insufficiency+mild pulmonal insufficiency+ marasmus+ caries dentis+ ginggival pulpa
P: Bed rest+ semi fowler position
O2 1 liter/minute nasal canule (intermitten)
Furosemide injection 20 mg/12 hours/IV
Spironolacton 2x12.5 mg
Captopril 2x6,25 mg
Ampicilin injection 1 gram/6 hours/IV(day 12)
Gentamycin injection 50 mg/12 hours/IV (day 22)
Ambroxol syrup 3x1 Cth
Folic acid 1x5 mg
Multivitamin without Fe 1x1 cth
regular diet 1000 kal + fluid consistency diet (F100) 3 x 200 cc
Laboratory findings on March 28th 2014
Complete Blood Count : HGB 12.80 g%, RBC 4.59 106/mm3, WBC 14.68106/mm3,
haematocryte 37 %,Trombocyte 361 106/mm3, MCV 80.6 fL, MCH 27.90 pg, MCHC 34.60 g%,
RDW 15.80%, MPV 8.40 fL, PCT 0.3 %, PDW 8.8 fL,ESR 15 mm/hrs, Neutrophil 64.90 %,
lymphocyte 22.70 %, monocyte 9 %, eosinophil 3.1 %, basophil 0.3 %, Absolute neutrophil
9.52 106/µL, Absolute lymphocyte 3.33 106/µL, Absolute monocyte 1.32 106/µL, Absolut
eosinophil 0.14 106/µL, Absolute basophil 0.07 106/µL.
Immunoserology : CRP positive, procalcitonine 0.12 ng/ml
Discussion
Patient RAR came to Adam malik general hospital with main complaint shortness of breathing
since 5 months ago. RAR have consultated with dr. Tina C.L Tobing, Sp.A(K) and diagnosed
with PDA moderate, mild Aorta Insufficiency,and mild mitral Insufficiency by
echocardiography on november 2013. Since RAR had refered at Adam Malik, RAR diagnosed
with moderate PDA , mild PE , vegetation on pulmonary valve, mild PI, mild TI, mild MI from
echocardiography on 5 march 2014.
This patient had typical clinical manifestation of Patent ductus arteriosus, such as
shortness of breathing from medical history and continous murmur from physical examination.
Shortness of breathing in this patient caused by increased pulmonary flow from patent ductus
arteriosus shunting and leads to increased pulmonary fluid volume. This condition causes
decreased lung compliance, which may result in increased work of breathing. Continuous
murmur or often reffered to as a “machinery” murmur is the hallmark physical finding in PDA.
Murmur located at the upper left sternal border and a thrill may be present. In this patient
continuous murmur and thrill present at the lower mid clavicula sinistra intercostal IV-V so it
classified as grade IV/VI of murmur.
On other physical diagnostic, hepatomegaly is present. This is found by abdomen
palpation, normally liver is not palpable. But in this patient liver is palpable 4cm below arcus
costae dextra. Hepatomegaly in this patient is one of the clinical manifestation from congestive
heart failure. Congestive heart failure in this patient occured for the result of the volume overload
on right side of heart. Increased pressure on right side of heart caused by pulmonary valve
insufficiency, which create a back flow of blood from artery pulmonal and leads to volume
overload on right side of heart. Volume overload caused high pressure on right side of heart and
leads to back flow to superior and inferior cava veins. This condition caused jugular vein high
pressure and hepatomegaly
The diagnosis of moderate PDA was confirmed by echocardiogram. Echocardiogram is
the procedure of choice to confirm the diagnosis and to characterize a PDA. In addition to
evaluating the ductus arteriosus, the echocardiogram is used to identify and evaluate other
associated cardiac defects. In this case mild PE, vegetation on pulmonary valve, mild MI, mild
TI, and mild PI is found as other associated cardiac defects. M-mode echocardiography is used to
measure the cardiac chamber sizes and quantitate left ventricular systolic function. In a patient
with a small ductus arteriosus, chamber sizes are usually normal, although mild left atrial and or
left ventricular enlargement may be present. In a patient with a moderate or large patent ductus,
the left atrium and left ventricle are enlarged. On echocardiogram examination, dilated left
ventricle and left atrium is found in this patient.
RAR is given Furosemid, Spironolactone, Captopril, Ceftriaxone (which is stopped
because of bacterial resistant, and exchange with Ampicillin), and Gentamicin. Furosemid,
spironolactone, and captopril is treatment for congestive heart failure which is complication from
PDA on this patient. This drugs reduce pre-load and after-load in aim to decreased burden of the
heart. Furosemid is Loop diuretics drug, mechanism of action furosemid inhibits reabsorption of
sodium and chloride ions at proximal and distal renal tubules and loop of henle by interfering
with chloride-binding cotransport system, causes excretion increases in water, calcium,
magnesium, sodium and chloride.
Mechanism of action of spironolactone is aldosterone antagonist with diuretic and
antihypertensive effects. Competitive binding of receptors at aldosterone-dependent Na-K
exchange site in distal tubules results in increased excretion of Na+, Cl-, and H2O and retention
of K+ and H+. Aldosterone receptor antagonist medicines may be a good option for people with
heart failure who are already taking other medicines such as ACE inhibitors, other diuretics,
digoxin, and beta blocker.
Captopril perevents the conversion of angiotensin I to angiotensin II (a potent
vasoconstrictor) through inhibition of ACE by competing with physiologic subtrate (angiotensin
I) for active site of ACE; inhibition of ACE initially results in decreased plasma angiotensin II
concentrations and consequently, blood pressure may be reduced in part through decreased
vasoconstriction, increases renin activity, and decreases aldosterone secretion; also increases
renal blood flow, results to afterload reduction.
Until the patency of the ductus is corrected, administer antibiotics in patient during
instances of high exposure to bacteremia is needed. As recommended bye the american heart
association for the prevention of bacterial endocarditis. Ceftriaxone, ampicillin and gentamicin is
antibiotics drugs which used for eliminate and prevention bacterial endocarditis. Ceftriaxon is
Third generation cephalosporin with broad spectrum gram negative activity, has lower efficacy
against gram-positive organisms but higher efficacy against resistant organism, highly stable in
presence of beta lactamase (penicilinase and cephalosporinase) of gram-negative and gram-
positive bacteria. bactericidal activity results from inhibiting cell wall synthesis by binding to 1
or more penicillin binding proteins, exerts antimcrobial effect by interferingwith syhthesis of
peptidoglycan (major structural component of bacterial cell wall). bacteria eventually lyse
because activity of cell wall autolytic enzymes continues while cell wall assembly is arrested.
Ampicilin is Broad spectrum penicillin. Interferes with bacterial cell wall synthesis during active
replication, causing bactericidal activity against susceptible organism.alternative to amoxicilin
when unable to take medication orally.
Gentamycin is Aminoglycoside antibiotic for gram negatif coverage bacteria including
pseudomonas species. Synergistic with beta-lactamse against enterococci. Interferes with
bacterial protein synthesis by binding to 30s and 50s ribosomal subunits.
Conclusion
This paper reports a case of a 11 years old female diagnosed with congestive heart failure et
causamoderate Patent Ductus Arteriosus + vegetation o/t pulmonary valve + mild PE + mild PI +
mild MI + mild TI. A comprehensive work up had been done to confirm the diagnosis. The
treatment for this patient includes Furosemide and Spironolactone for reducing pre-load,
Captopril for reducing after-load, Ampicillin and Gentamicin for bacterial endocarditis
prevention and eradication, ambroxol for cough. O2 and semi fowler position are meant to treat
shortness of breath, and adequat diet for malnutrition.
References
1. Austin,.Birth Defect Risk Factor Series Atrial Septal defect.Departement of State Health
Services Birth Defects Epidemiology and Surveillance.2005;1-9.
2. Penny D.J.,Vick G.W., Ventricular Septal Defect.2011;377:1103-1112.
3. Congenital and Children’s Heart Centre. [Accesed at Further information at the
Children’s Heart Federation :http://www.childrens-heart-fed.org.uk.]
4. Carr M.R.,Pediatric Atrial Septal Defect.2014. Accesed at http://emedcine.medscape.com
5. Ramaswamy P.Ventricular Septal Defects.2013.Accesed at htt://emedcine.medscape.com
6. Alexander R. Pathophsyoology of Atrial Septal Defect.2008.Accesed at
[http://biomed.brown.edu/Courses/BI108/BI108_2008_Groups/group03/
Pathophysiology.html]
7. Wu H.M.,Ventricular Septal Defect with Secondary Left Ventricular-to-Right Atrial
Shunt Associated with a Higher Risk for Infective Endocarditis and a Lower Late Chance
of Closure. Official journal of The American Academy of Pediatric.2013;262-267.
8. Berger S.,Ventricular Septal Defect.2013.Accesed at at http://emedcine.medscape.com
9. Rao P.S.,Atrial Septal Defect-A Review. University of Texas at Houston Medical School,
Houston, Texas,.2012;1-18
10. Schumacher K.R.Ventricular Septal Defect.Medline Plus.2011.Accesed at
http://www.gov/medlineplus/ency/article/001099.htm
11. Krasuski R.A., When and How to Fix a “Hole in the Heart” : Aprroach to ASD and PFO.
Cleveland Clinic Journal of Medcine.2007.137-147.
12. Minnette M.S.,Ventricular Septal Defect.Circulation.2013.
Accesed at http://circ.ahajournals.org/content/114/20/2190.full