Laparoscopic versus conventional pelvic lymphadenectomy for gynaecological malignancy in humans
3
902 SHORT COMMUNICATIONS Table 1. A comparison of the lymph node harvest obtained laparoscopically and through an abdominal incision. Each animal acted as its own control and had a laparoscopic and contralateral open lymphadenectomy in a single blind matched paired study using block random allocation. Laparoscopic lymphadenectomy Lymphadenectorny through an abdominal incision Approximate site Approximate site Subject External Internal Common TOTAL External Internal Common A 2 2 6 10 0 6 3 B 2 5 2 9 4 6 0 C 3 2 1 6 1 2 5 D 1 1 1 9 3 0 2 E 2 4 8 14 1 3 1 F 0 2 8 10 0 0 5 Total No. left behind l(PigF) 0 1 (PigB) 2 S(PigD&E) 0 2(PigB) TOTAL 9 10 8 5 11 5 7 Acknowledgments We are grateful to Ethicon Endo-surgery, Australia and New Zealand, for supporting laparoscopic lympha- denectomy training in the Royal Perth Hospital Animal Research and Laboratory, and to the Royal College of Obstetricians and Gynaecologists for a travel scholarship. References Dargent D. (1993) Laparoscopic surgery and gynaecologic cancer. Garry R. (1992) Laparoscopic alternatives to laparotomy : a new Curr Opin Obstet Gynecol5, 294300. approach to gynaecological surgery. Br J Obstet Gynaecol 99, 629-633. Nezhat C. R., Burrell M. 0.. Nezhat F. R., Benign0 B. B. & Welander C. E. (1992) Laparoscopic radical hysterectomy with para-aortic and pelvic node dissection. Am J Obstet Gynecol. 166, 864865. Nezhat C. R., Nezhat F. R. & Burrell M. 0. (1993) Laparoscopic radical hysterectomy and laparoscopic assisted vaginal radical hysterectomywith pelvic and para-aortic node dissection. JGynecol Surg 9, 105-120. Querleu D. (1993) Laparoscopic para-aortic node sampling in gynaecological oncology : a preliminary experience. Gynecol Oncol 49, 24-29. Received I3 April I994 Accepted 26 May 1994 British Journal of Obstetrics and Gynaecology October 1994, Vol. 101, pp. 902-904 Laparoscopic versus conventional pelvic lymphadenectomy for gynaecological malignancy in humans NICHOLAS JOHNSON Senior Lecturer & * Gynaecological Oncology Fellow Institute of Epidemiology, University of Leeh, UK and * King Edward Hospital, Perth, Western Australia It is technically possible to perform laparoscopically a Subjects and methods Pelvic lymphadenectomy in Western Australia is per- formed as part of the treatment for early (Stage 1 and 2a) cervical cancer and for Stage 1 G3, M3 endometrial during cervical or uterine cancer surgery in the Western Australian State Gynaecological Oncology Service was complete pelvic lymphadenectomy. In the previous article, appearing on page 901 of this issue, laboratory animal experiments suggest that minimal access surgery is as good was tested in clinical practice in a prospective observational study ‘Omparing the lymph node harvest from lapa- as (Johnson ef 1994)* This carcinoma. The number of nodes harvested from women roscopic bmphadenectomies and surgery’ recorded during a 12-month Deriod, from A ~ r i l 1993 to April 1994. A node was couited if it was palpated by a pathologist and confirmed on haematoxylin and eosin histology. Cases were contributed by three consultant surgeons, two of whom were experienced in oncology and Correspondence: Dr N. Johnson, Department of Obstetrics and Gynaecology, ‘ D’ Floor, Clarendon Wing, Leeds Infirmary, Belmont Grove, Leeds LS2 9NS, UK.
-
Upload
nicholas-johnson -
Category
Documents
-
view
212 -
download
0
Transcript of Laparoscopic versus conventional pelvic lymphadenectomy for gynaecological malignancy in humans

902 SHORT COMMUNICATIONS
Table 1. A comparison of the lymph node harvest obtained laparoscopically and through an abdominal incision. Each animal acted as its own control and had a laparoscopic and contralateral open lymphadenectomy in a single blind matched paired study using block random allocation.
Laparoscopic lymphadenectomy Lymphadenectorny through an abdominal incision
Approximate site Approximate site
Subject External Internal Common TOTAL External Internal Common
A 2 2 6 10 0 6 3 B 2 5 2 9 4 6 0 C 3 2 1 6 1 2 5 D 1 1 1 9 3 0 2 E 2 4 8 14 1 3 1 F 0 2 8 10 0 0 5
Total No. left behind l(PigF) 0 1 (PigB) 2 S(PigD&E) 0 2(PigB)
TOTAL
9 10 8 5
11 5 7
Acknowledgments We are grateful to Ethicon Endo-surgery, Australia and New Zealand, for supporting laparoscopic lympha- denectomy training in the Royal Perth Hospital Animal Research and Laboratory, and to the Royal College of Obstetricians and Gynaecologists for a travel scholarship.
References Dargent D. (1993) Laparoscopic surgery and gynaecologic cancer.
Garry R. (1992) Laparoscopic alternatives to laparotomy : a new Curr Opin Obstet Gynecol5, 294300.
approach to gynaecological surgery. Br J Obstet Gynaecol 99, 629-633.
Nezhat C. R., Burrell M. 0.. Nezhat F. R., Benign0 B. B. & Welander C. E. (1992) Laparoscopic radical hysterectomy with para-aortic and pelvic node dissection. Am J Obstet Gynecol. 166, 864865.
Nezhat C. R., Nezhat F. R. & Burrell M. 0. (1993) Laparoscopic radical hysterectomy and laparoscopic assisted vaginal radical hysterectomy with pelvic and para-aortic node dissection. JGynecol Surg 9, 105-120.
Querleu D. (1993) Laparoscopic para-aortic node sampling in gynaecological oncology : a preliminary experience. Gynecol Oncol 49, 24-29.
Received I3 April I994 Accepted 26 M a y 1994
British Journal of Obstetrics and Gynaecology October 1994, Vol. 101, pp. 902-904
Laparoscopic versus conventional pelvic lymphadenectomy for gynaecological malignancy in humans NICHOLAS JOHNSON Senior Lecturer & * Gynaecological Oncology Fellow Institute of Epidemiology, University of Leeh, UK and * King Edward Hospital, Perth, Western Australia
It is technically possible to perform laparoscopically a Subjects and methods Pelvic lymphadenectomy in Western Australia is per- formed as part of the treatment for early (Stage 1 and 2a) cervical cancer and for Stage 1 G3, M3 endometrial
during cervical or uterine cancer surgery in the Western Australian State Gynaecological Oncology Service was
complete pelvic lymphadenectomy. In the previous article, appearing on page 901 of this issue, laboratory animal experiments suggest that minimal access surgery is as good
was tested in clinical practice in a prospective observational study ‘Omparing the lymph node harvest from lapa-
as (Johnson ef 1994)* This carcinoma. The number of nodes harvested from women
roscopic bmphadenectomies and surgery’ recorded during a 12-month Deriod, from A ~ r i l 1993 to April 1994. A node was couited if it was palpated by a pathologist and confirmed on haematoxylin and eosin histology. Cases were contributed by three consultant surgeons, two of whom were experienced in oncology and
Correspondence: Dr N. Johnson, Department of Obstetrics and Gynaecology, ‘ D’ Floor, Clarendon Wing, Leeds Infirmary, Belmont Grove, Leeds LS2 9NS, UK.

SHORT COMMUNICATIONS 903
Lymph node harvest
70 0
0 .
60 0 .
0
50
0
0 0 .
0 40
30
0
0 0
20 0
0
0
0.0
0 0 .
0 . 0
0 .
0.0
0 0 . 0
0 0
0
10
La paroscopy La pa rot omy
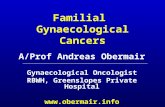
0 Fig. 1. Number of lymph nodes removed for gynaecological cancer surgery in Western Australia between April 1993 and April 1994.
the other was training and under supervision. Cases were selected for minimal access surgery by the consultant of the week.
One surgeon felt that minimal access surgery for gynaecological cancer was purely experimental, one was agnostic, and the other believed that the abdomen did not need to be opened to perform equivalent surgery.
Conventional lymphadenectomy involved a trans- peritoneal midline laparotomy extending approximately 3 to 5 cm above the umbilicus, exposure of all the large pelvic vessels below the aortic bifurcation, and clearance of the obturator fossa, internal, external, and common iliac vessels and exposure of the sacrum. Laparoscopic surgery involved a sub- or supra-umbilical videolaparoscopy and two or three suprapubic ports. The peritoneum over the vessels was reflected medially to expose the pelvic side walls, and curved retractors mobilised the vessels so all surfaces could be examined and the nodes plucked from them. The nodes were placed in a McCartney tube, a 4 cm tube placed in the vagina after the laparoscopic hyster- ectomy or radical hysterectomy to collect nodal tissue (McCartney 1994, in press).
Results One case was excluded because the lymphadenectomy for presumed G3 endometrial carcinoma was abandoned when the pathologist examined the uterus during the surgery and reported there was no obvious myometrial invasion. One laparoscopic lymphadenectomy was com- plicated by bleeding from the internal iliac vein which required a 5 cm transverse incision to secure haemostasis ; this patient was given four units of packed cells intra- operatively, thus her haemoglobin was maintained. On average, the operative time for a laparoscopic pelvic lymphadenectomy was 1 h per side (range 40 to 90 min). Conventional lymphadenectomy took 25 min for each side (range 14 to 60 min).
Fewer nodes were removed from women during minimal access surgery compared with conventional surgery (median = 39 compared with 42.5: Mann-Whitney test; P = 004) (Fig. 1). The duration of hospitalisation was shorter in those treated laparoscopically (median 5 compared with 10 days).
Discussion One problem with any nonrandomised study is selection bias. Younger women with early cervical cancer tend to be selected for minimal access surgery because it was possible to obtain a good clearance. The risk of lymph node metastases was low and only a courageous laparoscopic surgeon plucks a node underneath and adherent to the origin of the vena cava. Women with bulky tumours were more likely to be treated by conventional surgery, and this inevitably means that we were more aggressive.
A second potential cause of bias is surgical expertise. This was probably not a problem as the harvest did not improve with experience. Nevertheless, individual surgeons have different skills, and a skilled endoscopist may be better than a less committed conventional surgeon.

904 SHORT COMMUNICATIONS
The difference in lymph node harvest is statistically significant but is it clinically significant? The role of pelvic lymphadenectomy in gynaecology oncology is contentious, and there is no evidence that a complete lymphadenectomy is better than a thorough sampling. Lymphadenectomy for cervical cancer is thought to be therapeutic but Massi et al. (1993) have demonstrated how tenuous this belief is. Lymphadenectomy for endometrial carcinoma is not curative and suboptimal removal will not affect survival but may alter local recurrences. Despite this, many oncologists believe that the best chance of cure from uterine or cervical surgery comes from radical surgery and anything less may put the woman at a disadvantage. Therefore, if laparoscopic oncologists are to compete with their traditional colleagues, they must demonstrate equivalent clearances in their hands.
I had hoped to confirm the previous animal studies (Johnson et al. 1994), but these data suggest that we could
not remove as many nodes using minimal access surgery, compared with a conventional laparotomy. The difference is small but supports those who argue that more access n u s t mean better clearance.
References Johnson N., Johnson V., McKie G. & Knowles S. (1994) Laparoscopic
pelvic lymphadenectomy versus traditional surgery in pigs. Br J Obstet Gynaecol 101, 901-902.
Massi G., Savino L. & Sussini T. (1993) Schauta-Amreich I. Vaginal hysterectomy and Wertheims-Meigs abdominal hysterectomy in the treatment of cervical cancer: a retrospective analysis. Am J Obstet Gynecoll78, 928-934.
McCartney A. J. (1994) The transvaginal tube. Presented at the Second International Symposium of Gynaecological Endoscopy, Heidelberg, Germany, 1993. Obstet Gynecol (in press).
Received 6 June 1994 Accepted 16 June 1994
British Journal of Obstetrics and Gynaecology October 1994, Vol. 101, pp. 904-905
Small fetal transverse cerebellar diameter : a screening test for spina bifida R. H. B. D E C O U R C Y - W H E E L E R Research Fellow, M. M. P O M E R A N Z Research Fellow, *N. J. WALD Professor, K. H. NICOLAIDES Professor The Harris Birthright Research Centre for Fetal Medicine, King’s College Hospital Medical School; * Wolfson Institute of Preventative Medicine, The Medical College of St Bartholomew’s Hospilal, London
Prenatal diagnosis of spina bifida by ultrasonography has improved after the recognition of cranial (lemon-shaped head) and cerebellar (banana-shaped) signs in affected fetuses (Nicolaides et al . 1986). The use of these signs in high risk populations has a sensitivity of 98 % and a false positive rate of 0.8% (Van Den Hof et al. 1990). Among three low risk populations no cases of spina bifida were missed (Chitty et al. 1991 ; Luck 1992; Shirley et al . 1992). However, a recent regional study has reported that only 6070 of cases of spina bifida were detected (Northern Regional Survey Steering Group 1992).
Cranial and cerebellar signs are subjective but measure- ment of the fetal transcerebellar diameter (TCD) is quantitative. This study examines the value of TCD as a screening test for spina bifida.
Subjects and methods During an eight-year period (198&93), 261 cases of fetal open spina bifida were diagnosed in our unit by ultra- sonography at 16 to 24 weeks of gestation. In 53 cases
Correspondence: Professor K. H. Nicolaides, The Harris Birth- right Research Centre for Fetal Medicine, King’s College Hospital Medical School, Denmark Hill, London SE5 9RS, UK.
the cerebellum was not measured, although it was reported to be banana-shaped in 45. Gestational age was calculated from menstrual data and confirmed by ultrasonographic measurements of the fetal femur length (Hitachi EUB360, Aloka SSD-650 or Aloka SSD-68). In each case the fetal cerebellum was examined, and the TCD was measured in the sub-occipitobregmatic view of the head. A value of zero was given if the cerebellum was not detectable, presumably due to major herniation down the cisterna magna. Values of TCD in unaffected pregnancies (40 from each week of gestation 14 to 24 weeks) were derived from a study of 1040 pregnancies that resulted in term delivery of healthy, appropriately grown infants (Snijders & Nicolaides 1994). Measurements of the fetal TCD in unaffected and affected fetuses were converted into multiples of the median (MOM), and the sensitivity and false positive rates for each cut-off point were calculated.
Results In the 208 fetuses with spina bifida the cerebellum appeared normal in 15 (7%), was absent in 57 (28%) and was banana-shaped in 136 (65 %). Additionally, in 200 fetuses (96%) the head was lemon-shaped, and in 140 (69%) there was ventriculomegaly (anterior or posterior hemi-