
Laboratory Monitoring Measurement of the DOACs
24
1 Laboratory Monitoring Measurement of the DOACs ACC Anticoagulation Consortium Roundtable Meeting October 24, 2015 Adam Cuker, MD, MS Perelman School of Medicine University of Pennsylvania
Transcript of Laboratory Monitoring Measurement of the DOACs

1
Laboratory Monitoring Measurement of the DOACs
ACC Anticoagulation Consortium Roundtable Meeting
October 24, 2015
Adam Cuker, MD, MS Perelman School of Medicine
University of Pennsylvania

2
Full disclosures (last 12 months) • Research support
• NIH • FDA • T2 Biosystems
• Consultant/Advisory Board • Sanofi/Genzyme • Bracco • Amgen
• Patents • Laboratory assays for HIT
• Off-label use • Some assays are not FDA-approved for DOAC measurement

3
Outline
• Basic principles • Variability in drug levels • On-therapy vs. therapeutic range • Why measure?
• Attributes of an ideal assay • Dabigatran • Factor Xa inhibitors • Recommendations

4
Plasma drug levels
Drug Dose Trough plasma level (ng/mL)
Peak plasma level (ng/mL)
Median 5th-95th percentile
Median 5th-95th percentile
Dabigatran 150 mg BID 90 31-225 184 64-443 Rivaroxaban 20 mg daily 26 6-87 270 189-419 Apixaban 5 mg BID 103 41-230 171 91-321 Edoxaban 60 mg daily 22 10-40a 170 120-250a
Ezekowitz MD et al., Am J Cardiol 2007;100:1419; Mueck W et al., Clin Pharmacokinet 2014;53:1; Kowalski et al., J Pharmacokinet Pharmacodyn 2014;41(Supp 1):S19; Weitz JI et al., Thromb Haemost 2010;104:633
aInterquartile range

5
Variability in trough levels
US adult male height:
5th percentile: 5’4’’ 95th percentile: 6’ 3’’
If variation in height was equivalent to variation in rivaroxaban trough levels
U.S. Census Bureau, Statistical Abstract of the United States: 2012

6
DOAC level 0
Below on-therapy range
On-therapy range
Above on-therapy range
5th percentile trough level
95th percentile peak level
Therapeutic On-therapy range

7
Why measure?
Drug level 0
Below on-therapy range
On-therapy range
Above on-therapy range
Bleeding Overdose
Renal dysfunction Low body weight Advanced age
Drug interaction
Treatment failure Preoperative state Non-compliance
Obesity Renal hyperfunction
GI malabsorption Drug interaction
Trauma Emergent procedure
Reversal agent

8
Attributes of an ideal assay
Plasma drug concentration
Assa
y re
sult
1. Linear correlation between assay result and drug levels (r2 > 0.9)
2. Across a broad range of drug levels
3. Sensitive 4. Specific 5. Available 24-7,
short TAT Below On-therapy Above

9
Dabigatran

10
Dabigatran (TT)
Hapgood et al., Thromb Haemost 2013;64:1128
Use: Normal TT excludes clinically significant drug levels
Problem: Too sensitive. Cannot be used to quantify drug. Drug Drug Trough: 90 (31-225)
Peak: 184 (64-443)
>
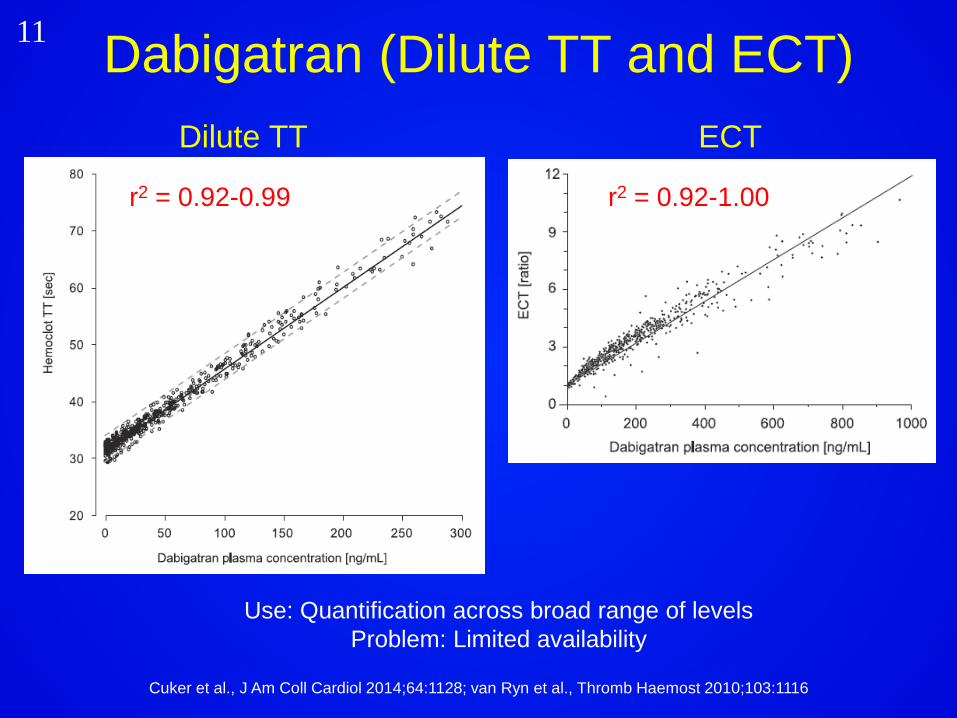
11 Dabigatran (Dilute TT and ECT) Dilute TT ECT
r2 = 0.92-1.00 r2 = 0.92-0.99
Cuker et al., J Am Coll Cardiol 2014;64:1128; van Ryn et al., Thromb Haemost 2010;103:1116
Use: Quantification across broad range of levels Problem: Limited availability

12 Dabigatran (APTT)
van Ryn et al., Thromb Haemost 2010;110:308; Harenberg et al., Semin Thromb Hemost 2012;38:16
Problems: Curvilinear, insufficient sensitivity (normal APTT does not exclude clinically relevant drug levels), reagent variability
Use: Normal APTT excludes above on-therapy levels
Trough: 90 (31-225) Peak: 184 (64-443)

13 Dabigatran (PT/INR)
Antovic et al., Eur J Clin Pharmacol 2013;69:1875; Helin et al., Clin Chem 2013;59:807
Problem: Poor correlation, insufficient sensitivity, reagent variability Use: None
Trough: 90 (31-225) Peak: 184 (64-443)

14
FXa inhibitors (Rivaroxaban, Apixaban, Edoxaban)

15
FXa-inhibitors (Anti-Xa activity)
Rivaroxaban (r2 0.95-1.00)
Cuker et al., J Am Coll Cardiol 2014;64:1128; Cuker et al., J Thromb Thrombolysis 2015;39:288 Douxfils et al., Thromb Haemost 2013;110:723; Becker et al., J Thromb Thrombolysis 2011;32:183;
Zafar et al., Thromb Haemost 2007;98:883
Apixaban (r2 0.89-0.95) Edoxaban (r2 0.96-0.99)
Use: Quantification across broad range of levels Problem: Limited availability

16
FXa-inhibitors (PT/INR) Edoxaban
Samama et al., Thromb Haemost 2010;103:815; Barrett et al., Thromb Haemost 2010;104:1263; Zafar et al., Thromb Haemost 2007;98:883
Rivaroxaban Apixaban
Use: Normal PT excludes above on-therapy levels of rivaroxaban and edoxaban (but not apixaban)
Problem: Normal PT does not exclude clinically relevant levels, reagent variability
Trough: 26 (6-87) Peak: 270 (189-419)
Trough: 103 (41-230) Peak: 171 (91-321) Trough: 22 (10-40)
Peak: 170 (120-250)

17
FXa-inhibitors (APTT)
Rivaroxaban
Dale et al., J Thromb Haemost 2014;12:1810; Zafar et al., Thromb Haemost 2007;98:883
Apixaban Edoxaban
Problem: Normal APTT does not exclude clinically relevant levels, reagent variability Use: None
Trough: 26 (6-87) Peak: 270 (189-419)
Trough: 103 (41-230) Peak: 171 (91-321)
Trough: 22 (10-40) Peak: 170 (120-250)

18 Suggestions for DOAC measurement if specialized assays are available
Exclude clinically relevant drug levels
Measure on-therapy levels
Determine whether above on-therapy levels are present
Dabigatran TT Normal TT excludes clinically relevant levels
Dilute TT, ECT
- Dilute TT, ECT
-
FXa inhibitors
Anti-Xa Absent anti-Xa activity likely excludes clinically relevant levels
Anti-Xa Anti-Xa -
ECA, ecarin chromogenic assay; ECT, ecarin clotting time; TT, thrombin time
Cuker et al., J Thromb Thrombolysis 2015; Epub ahead of print

19
Exclude clinically relevant drug
levels
Determine whether above on-therapy levels are present
Dabigatran TT Normal TT excludes clinically relevant levels
APTT • Prolonged APTT suggests that on-therapy or above on-therapy levels are present.
• Normal APTT likely excludes above on-therapy levels.
• Normal APTT may not exclude on-therapy levels.
Suggestions for dabigatran measurement if specialized assays are not available
Cuker et al., J Thromb Thrombolysis 2015; Epub ahead of print
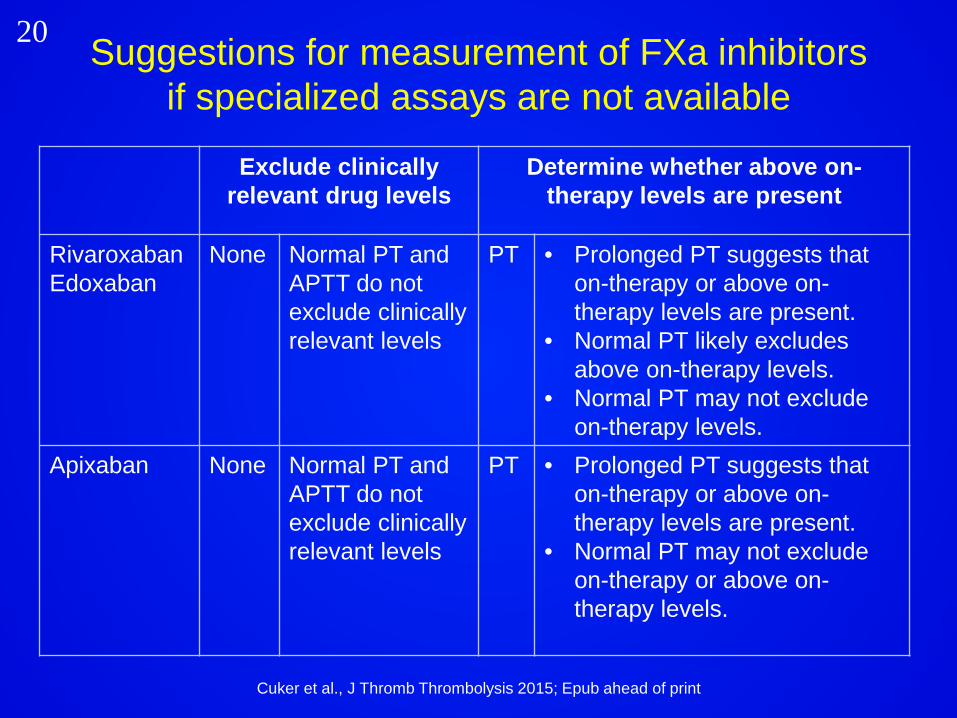
20
Exclude clinically relevant drug levels
Determine whether above on-therapy levels are present
Rivaroxaban Edoxaban
None Normal PT and APTT do not exclude clinically relevant levels
PT • Prolonged PT suggests that on-therapy or above on-therapy levels are present.
• Normal PT likely excludes above on-therapy levels.
• Normal PT may not exclude on-therapy levels.
Apixaban None Normal PT and APTT do not exclude clinically relevant levels
PT • Prolonged PT suggests that on-therapy or above on-therapy levels are present.
• Normal PT may not exclude on-therapy or above on-therapy levels.
Suggestions for measurement of FXa inhibitors if specialized assays are not available
Cuker et al., J Thromb Thrombolysis 2015; Epub ahead of print

21 Will we monitor DOACs in the future?
Reilly PA et al., J Am Coll Cardiol 2014;63:321

22 Thrombin generation assay
Hoffman et al., Anesthesiology 2015;122:353
Peak thrombin
generation
Rate
ETP
Time to peak
Lag time

23 Thromboelastography (TEG)
Escolar et al., PLoS One 2013;8:e78696
R
MA
Alpha angle
K

24 Take-home points • The DOACs have variable effects on coagulation assays • Laboratory measurement may be desirable in special
circumstances • Selection of the optimal assay depends on the drug, indication
for measurement, and assay availability • Dabigatran
• Normal TT excludes clinically relevant levels • Dilute TT and ECT can be used for quantification across a broad
range of levels • Normal APTT excludes excess levels
• FXa inhibitors • Normal anti-Xa excludes clinically relevant levels • Anti-Xa can be used for quantification across a broad range of
levels • Normal PT excludes excess levels of rivaroxaban and edoxaban,
but not apixaban


















