Laboratory Assesment of Thyroid Function PMC2003
14
Introduction This review summarizes principles for the appropriate use of laboratory assays in the diagnosis and follow-up of thyroid disorders. Symptoms, physical signs, imaging techniques and cytological examination will not be considered in detail, although it is self-evident that laboratory results should be interpreted in this broader context. The recent monograph “Laboratory support for the diagnosis of thyroid disease” from the National Academy of Clinical Biochemistry, USA, should be consulted for detailed guidelines on the preparation, la boratory use an d application of current thyro id assays. 1 References for specific points in this review are cited at www.thyroidmanager.org. 2 It is now well known that the presentations of thyrotoxicosis and hypothyroidism are so diverse (Table 1) that it is difficult to rule out these conditions clinically , or to make a conclusive diagnosis until the disorder is far advanced. Any of the presentations summarized in Ta ble 1 is reason to seek confirmatory clinical features, and to measure serum TSH, using an assay sufficiently sensitive to clearly separate the suppressed values characteristic of thyrotoxicosis from the lower limit of the normal reference interval. Apart from using laboratory tests when thyroid dysfunction is suspected, or in groups with an increased risk of thyroid dysfunction (Table 2), there are several situations where routine testing is appropriate. First, neonatal screening for 109 Clin Biochem Rev Vol 24 November 2003 Review Article Assessment of Thyroid Function: Towards an Integrated Laboratory - Clinical Approach Jim Stockigt Department of Endocrinology and Diabetes and Ewen Downie Metabolic Unit, and Monash University Department of Medicine, Alfred Hospital, Prahran, VIC 3181, Australia For correspondence: Prof J Stockigt e-mail: [email protected] Abstract Laboratory assessment of thyroid function is now often initiated with a low pre-test probability , by clinicians who may not have a detailed knowledge of current methodology or testing strategies. Skilled laboratory staff can significantly enhance the choice of appropriate tests and the accuracy of clinical response; such involvement requires both appropriate training and relevant information from the clinician. Measurement of the serum thyroid stimulating hormone (TSH) concentration with an assay of adequate sensitivity is now the cornerstone of thyroid function testing; for untreated populations at risk of primary thyroid dys- function, a normal TSH concentration rules out an abnormality with a high degree of certainty. However, in several important situations, most notably pituitary abnormalities and early treatment of thyroid dysfunction, serum TSH can give a misleading indication of thyroid status. An abnormal TSH concentration alone is never an adequate basis for initiation of treatment, which should be based on the typical relationship between trophic and target gland hormones, based on serum TSH and an estimate of serum free thyroxine (T4). Six basic assumptions, some clinical, some laboratory-based, need to be considered, together with the relevant limiting conditions, for reliable use of this relationship. Current methods of free T4 estimation remain imperfect, especially during critical illness. Diagnostic approach differs significantly between initial diagnosis and follow-up of treated thyroid dysfunction. In some situations, serum triiodothyronine (T3) is also required, but serum T3 lacks sensitivity for diagnosis of hypothyroidism, and has poor specificity during non-thyroidal illness. Where assay results are anomalous, most atypical findings can be resolved by attention to the clinical context, without further investigation. (Clin Biochem Rev 2003; 24:110-23)
-
Upload
dadan-kurniawan -
Category
Documents
-
view
7 -
download
0
description
njk
Transcript of Laboratory Assesment of Thyroid Function PMC2003
-
Introduction
This review summarizes principles for the appropriate use oflaboratory assays in the diagnosis and follow-up of thyroiddisorders. Symptoms, physical signs, imaging techniques andcytological examination will not be considered in detail,although it is self-evident that laboratory results should beinterpreted in this broader context. The recent monographLaboratory support for the diagnosis of thyroid diseasefrom the National Academy of Clinical Biochemistry, USA,should be consulted for detailed guidelines on the preparation, laboratory use and application of current thyroidassays.
1References for specific points in this review are cited
at www.thyroidmanager.org.2
It is now well known that the presentations of thyrotoxicosis and hypothyroidism are so diverse (Table 1) that it is difficultto rule out these conditions clinically, or to make a conclusivediagnosis until the disorder is far advanced. Any of the presentations summarized in Table 1 is reason to seek confirmatory clinical features, and to measure serum TSH,using an assay sufficiently sensitive to clearly separate thesuppressed values characteristic of thyrotoxicosis from thelower limit of the normal reference interval.
Apart from using laboratory tests when thyroid dysfunction issuspected, or in groups with an increased risk of thyroid dysfunction (Table 2), there are several situations where routine testing is appropriate. First, neonatal screening for
109Clin Biochem Rev Vol 24 November 2003
Review Article
Assessment of Thyroid Function: Towardsan Integrated Laboratory - Clinical Approach
Jim Stockigt Department of Endocrinology and Diabetes and Ewen Downie Metabolic Unit, and Monash University Department ofMedicine, Alfred Hospital, Prahran, VIC 3181, AustraliaFor correspondence: Prof J Stockigt e-mail: [email protected]
Abstract
Laboratory assessment of thyroid function is now often initiated with a low pre-test probability, by clinicians who may not havea detailed knowledge of current methodology or testing strategies. Skilled laboratory staff can significantly enhance the choiceof appropriate tests and the accuracy of clinical response; such involvement requires both appropriate training and relevantinformation from the clinician. Measurement of the serum thyroid stimulating hormone (TSH) concentration with an assay ofadequate sensitivity is now the cornerstone of thyroid function testing; for untreated populations at risk of primary thyroid dys-function, a normal TSH concentration rules out an abnormality with a high degree of certainty. However, in several important situations, most notably pituitary abnormalities and early treatment of thyroid dysfunction, serum TSH can give amisleading indication of thyroid status. An abnormal TSH concentration alone is never an adequate basis for initiation of treatment, which should be based on the typical relationship between trophic and target gland hormones, based on serum TSHand an estimate of serum free thyroxine (T4). Six basic assumptions, some clinical, some laboratory-based, need to be considered, together with the relevant limiting conditions, for reliable use of this relationship. Current methods of free T4 estimation remain imperfect, especially during critical illness. Diagnostic approach differs significantly between initial diagnosis and follow-up of treated thyroid dysfunction. In some situations, serum triiodothyronine (T3) is also required, butserum T3 lacks sensitivity for diagnosis of hypothyroidism, and has poor specificity during non-thyroidal illness. Where assayresults are anomalous, most atypical findings can be resolved by attention to the clinical context, without further investigation. (Clin Biochem Rev 2003; 24:110-23)
-
congenital hypothyroidism is widely established. Second,recommendations from the American College of Physicians(Table 3) suggest that thyroid dysfunction is sufficientlycommon in women over 50 to justify routine testing at presentation for medical care (case-finding); the majority ofabnormal findings in this group will identify subclinicalrather than overt dysfunction (see below). Third, the findingof significant intellectual impairment in the offspring ofwomen who were mildly hypothyroid early in pregnancy
3
may justify routine testing of thyroid function, either before conception, or as early as possible in pregnancy.
The application of population reference intervals to individuals can obscure rather than clarify the diagnosis ofminimal or mild thyroid dysfunction. Serial assessment ofthyroid function shows that individuals remain close to a particular set-point for TSH and T4.
4Such studies suggest
that potentially important variations from the individual set-point can still fall within the population norm. This issueis most relevant for serum TSH values in the upper tail of thelogarithmically distributed normal range, especially in theassessment of optimal replacement therapy, or diagnosis ofmild thyroid failure. Notably, TSH values of 2-4 mU/L, stillwithin the reference interval, are associated with an increasedprevalence of positive thyroid peroxidase (TPO) antibody.
5
In practice, individualized interpretation of laboratory dataremains difficult unless there is information on set-point priorto assessment for possible thyroid dysfunction.
Current laboratory techniques make the diagnosis and follow-up of thyroid disorders straightforward in the large
majority of patients, but, in a small minority, problems due to assay artefacts or atypical clinical presentations can lead tomisdiagnosis, inappropriate treatment, or unnecessary furtherinvestigation. Such cases emphasize the importance of continuing review of diagnostic methodology by careful clinical correlation.
Terminology
The distinction between overt and subclinical hypothyroidism or thyrotoxicosis is based on whether anabnormal serum TSH concentration is associated with abnormal levels of the circulating thyroid hormones, T3 andT4, or whether serum TSH alone is abnormal. The terminology mild thyroid failure rather than subclinicalhypothyroidism is gaining support, based on evidence thatpotentially important tissue abnormalities can occur duringprogressive thyroid failure before the serum T4 concentrationbecomes clearly subnormal. It should be noted that the morefrequently thyroid function is tested in the absence of clinicalfeatures, the greater the proportion of results with serum TSHas the sole abnormality.
The terminology of thyroid antibody assays can be ambiguous. The terms microsomal and TPO antibody refer tothe same moiety, which is the most sensitive marker ofimmune thyroid damage, usually associated with the lymphocytic infiltration that is most extreme in Hashimotosthyroiditis. The more sensitive and specific radioimmunoassayfor TPO antibody has now superseded microsomal antibodytechniques. Anti-thyroglobulin assays are less relevant for thediagnosis of immune thyroid disease, but are crucial for the
110 Clin Biochem Rev Vol 24 November 2003
Stockigt J
Common to Both Thyrotoxicosis Hypothyroidism
Classical presentations Heart failure AnaemiaGoitre Arrhythmia ConstipationPostpartum Eye disease DepressionMenstrual disturbance Anxiety state DementiaNeonatal Weight loss MyalgiaIncidental finding Diarrhoea Nerve entrapment
Apathetic hyperthyroidism HyperlipidaemiaMyopathy HypoventilationPeriodic paralysis GalactorrhoeaDermopathy InfertilityItch Puberty, precocious or delayedThyroid storm Delayed growth
Hypothermia, coma
Table 1. Diverse clinical presentations of thyrotoxicosis and hypothyroidism
-
valid interpretation of serum thyroglobulin assays, for example in the follow-up of differentiated thyroid cancer.Measurement of TSH receptor antibody (TRAb) identifiesthe probable causative agent in Graves disease, generally bymeasuring the extent to which a test serum inhibits binding oflabelled TSH to a receptor preparation. Such assays do notdistinguish between stimulatory and inhibitory activity.
Prevalence of Thyroid Dysfunction
The Whickham study, from an iodine replete region inNorthern England, showed a prevalence of 1.9-2.7% overtthyrotoxicosis and 1.4-1.9% overt hypothyroidism in women,with progressive increase with age; prevalence in males was10-fold lower.
5Estimates of subclinical hypothyroidism were
4-5 fold higher, with about 10% of women over 50 showingan increase in serum TSH, again with progressive increasewith age. Further studies from the UK, USA and Australiandata from the Busselton study suggest a similar prevalence.
6,7
The 20 year Whickham follow-up showed that the likelihoodof women developing hypothyroidism rose with age and wasincreased about 8-fold if either TPO antibody was positive orserum TSH increased in the initial study; this risk rose toalmost 40-fold if both were abnormal. The likelihood ofeventual hypothyroidism increased progressively for initialTSH values over 2 mU/L, values still well within the reference interval.
Thyroid dysfunction is also common when younger womenare tested post-partum. A Perth study found abnormal thyroidfunction in 11.5% of women tested 6 months after delivery,with TSH values over 4.8 mU/L in 6%, of whom almost 90%had positive TPO antibody, indicating an autoimmune abnormality.
8In about half the untreated women with initial
TSH elevation, TSH remained increased 30 months afterdelivery, consistent with other studies that show an increased
111Clin Biochem Rev Vol 24 November 2003
Assessing Thyroid Function
Table 2. Groups at increased risk of thyroid dysfunction
GeneralPositive family historyPrevious postpartum thyroid dysfunctionPositive thyroid peroxidase antibodyPrevious thyroid disease or surgeryWomen over age 55Origin from areas of endemic iodine deficiencyVery low birth weight premature infants
Associated diseasesDiabetes mellitusAny autoimmune diseaseOther endocrine deficienciesDown syndromeTurner syndromeThalassaemia majorPituitary or hypothalamic abnormalitySevere head injuryRecent Cushing's syndrome
TherapyPituitary surgery or irradiationHead and neck irradiation Radical laryngeal/pharyngeal surgeryTreatment of growth hormone deficiencyCytotoxic therapyLithiumAmiodaroneExposure to iodine excess, eg contrast agentsInterferon , interferon Interleukin 2Therapeutic monoclonal antibodiesGranulocyte colony stimulating factor
Recommendations of American College of Physicians, 1998 (modified from reference 20)
It is reasonable to screen women older than 50 years of age for unsuspected thyroid dysfunction, using a sensitive TSH assay.
Free T4 should be measured when the TSH level is undetectable or >10 mU/L. An undetectable TSH leveland an elevated free T4 level identify overt thyrotoxicosis. A TSH >10 mU/L and a low free T4 identify overthypothyroidism. Patients with either of these conditions are likely to benefit from treatment.
There is evidence that subclinical thyrotoxicosis and hypothyroidism have adverse effects (Table 4), but therapeutic benefit has not yet been conclusively demonstrated.
Table 3. Case Finding / Screening for Thyroid Disease
-
prevalence of late hypothyroidism after postpartum dysfunction.
Findings from one region do not necessarily apply in otherpopulations, because of ethnic differences or environmentalvariations such as iodine intake. For example, in Hong Kong,where iodine intake is marginally deficient, only 1.2% ofChinese women aged over 60 years had serum TSH values>5 mU/L, with a comparable prevalence of suppressed values indicating possible thyrotoxicosis. In general, hypothyroidism is more common with abundant iodineintake, with goitre and subclinical thyrotoxicosis more common with low iodine intake. Hence, optimal strategiesfor thyroid testing may vary between regions.
Accuracy and Sensitivity of Clinical and LaboratoryAssessment
To place laboratory testing in perspective we need to consider the sensitivity and accuracy of clinical assessmentfor thyroid dysfunction. Studies of patients evaluated in primary care show that clinical acumen alone lacks sensitivityand specificity. In two Scandinavian studies of over 3000unselected patients who were assessed by both clinical andlaboratory criteria, a thyroid disorder was not suspected byprimary care physicians in over 90% of those who tested positive, even when clinical features were apparent in retrospect.
9,10Further, in up to one-third of patients evaluated
for suspected thyroid dysfunction by specialists, laboratoryresults led to revision of the clinical assessment.
There are some dissenting opinions on the relative value ofclinical and laboratory evaluation of thyroid function. Somehave expressed the view that the clinical criteria are beingsidelined, while biochemical assessments are lacking inspecificity. This point is generally made by considering TSHand free T4 measurements individually, rather than in thetrophic hormone - target gland relationship that is the cornerstone of endocrine diagnosis (see below).Thyrotoxicosis and hypothyroidism can each have importantconsequences before the usual clinical features appear (Table 4). It may be no more valid to consider these diagnoses only when typical symptoms or signs appear, thanto wait for the thirst and polyuria before considering the possibility of diabetes!
While laboratory tests facilitate early diagnosis before clinical features are obvious, increased sensitivity carries theprice of decreased diagnostic specificity. It remains difficultto distinguish spurious results from those that indicate milddysfunction, especially in the presence of associated illness,where abnormal TSH and free T4 results lack specificity.
All current methods of measuring TSH, free T4 or free T3 inserum, whether by immunoassay or immunometric techniques, are comparative, i.e. they depend on the assumption that the unknown sample and the assay standardsare identical in all measured characteristics other than theconcentration of analyte. A result will be spurious when thiscondition is not fulfilled, for example when a sample showsanomalous binding of tracer to serum proteins or antibodies,or non-specific interference, either with the system that separates bound from unbound tracer, or the assay signal.Heterophilic antibodies remain a potential cause of spuriousassay results and there are currently no techniques that conclusively rule out this type of interference.
Measurement of Serum TSH
Secretion of TSH from the anterior pituitary is regulated bynegative feedback from the serum free thyroid hormone concentrations. Immunometric TSH assays that use two antibodies against different epitopes of TSH show greatlyimproved assay sensitivity. Serum TSH can be preciselymeasured to at least 0.03 mU/L, so that the lowest concentrations in normal subjects are clearly distinguishablefrom those found in thyrotoxicosis. However, assay specificity is not perfect, and false-positive detectable serumTSH is still found in occasional patients with definite thyrotoxicosis. The serum TSH response to changes in serumfree T4 is logarithmic; a two-fold change in free T4 inducesinverse 10-100 fold changes in TSH. This feedback amplification of the serum TSH response as the serum freeT4 increases or decreases, accounts for the fact that serumTSH can fall outside the reference interval several yearsbefore there is a diagnostic change in serum free T4.
Typical values for the lower reference limit for TSH are 0.3-0.5 mU/L, with upper limits of 4-5 mU/L, but the meanand median values are in the range 1-1.5 mU/L because of thelogarithmic distribution. The terminology for subnormalserum TSH values needs to be clarified. Values associatedwith thyrotoxicosis, either overt or subclinical are suppressed, (ie
-
Estimation of Serum Free T4
There have been many approaches to the estimation of freethyroid hormone concentrations in serum; some ingeniousapproaches have been of questionable validity.
11Some free
T4 methods have been marketed before they have been rigorously assessed, so that unexpected interferences mayonly be noted after methods have been used for some time.Currently available assays compensate well when changes intotal T4 and T3 are due to altered concentration of thyroidbinding globulin (TBG), but no current method reflects the invivo concentration of free hormone in undiluted serum.Equilibrium dialysis is often considered the referencemethod, but it is also subject to error, especially as a result ofgeneration of fatty acids during sample incubation, andunder-estimation of the effect of competitors that displace T4and T3 from binding proteins in vivo (see below). Two-stepmethods that separate a fraction of the free T4 pool from thebinding proteins before the assay step are generally leastprone to analytical artefacts.
Numerous medications can displace T4 and T3 from TBG(Table 5), but it is technically difficult to get an accuratereflection of these effects with current free T4 methods thatuse diluted samples. Competitors are usually less protein-bound than T4 itself, so that with progressive
113Clin Biochem Rev Vol 24 November 2003
Assessing Thyroid Function
Subclinical thyrotoxicosis (suppressed TSH, normal freeT4, free T3 )Progression to overt thyrotoxicosisExposure to iodine may precipitate severe thyrotoxicosisThreefold increased risk of atrial fibrillation after 10 yearsOsteoporosis risk is increased
Subclinical hypothyroidism (Mild thyroid failure) (increased TSH, normal free T4)Non specific symptoms may improve with treatment Progression to overt hypothyroidism (~ 5% per year)Adverse effect on foetal brain development in pregnancy Adverse effects on vascular complianceIndependent risk factor for atherosclerotic disease? Beneficial effect of treatment on lipids? Increased prevalence of depressive illness?
Table 4. Importance of Subclinical Thyroid Dysfunction21
Inhibit pituitary TSH secretionDopamine, dobutamine, glucocorticoids, octreotide
Iodine load increases thyroid hormone synthesis Contrast agents, amiodarone, topical preparations
Impair thyroid hormone releaseIodine excess, lithium, glucocorticoids, aminoglutethimide
Inhibit T4-T3 5' deiodinationAmiodarone, glucocorticoids, beta blockers *Contrast agents, e.g. iopanoic acid, ipodate
Augment abnormal immune functionInterleukin 1, interferon , interferon Monoclonal antibody therapy
Modify binding of T4, T3 to plasma proteinsa. Increase concentration of T4 binding globulinEstrogen, heroin, methadoneClofibrate, 5-fluorouracil, perphenazine, tamoxifenb. Decrease concentration of T4 binding globulinGlucocorticoids, androgens, l-asparaginasec. Displace T4 and T3 from binding proteinsFurosemide, salicylates, phenytoin, carbamazepineNon-steroidal antiinflammatory agents # Heparin
Displace T4 from tissue poolOral cholecystographic agents, some alkylating agents
Modify thyroid hormone actionAmiodarone, phenytoin
Increase clearance of T4,T3Barbiturates, phenytoin, carbamazepine, rifampicinSertraline?, fluoxetine?, dothiepin?
Impair absorption of ingested T4Aluminium hydroxide, ferrous sulfate, cholestyramine, calcium carbonateColestipol, sucralfate, soya preparations, kayexalate
* those with membrane-stabilizing effect, e.g. propranolol# some members of the group In vitro effect of in vivo heparin administration
Table 5. Medications that influence thyroid hormone orTSH levels
-
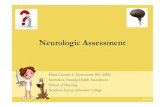
dilution, the free concentration of competitor declines beforethe free T4 concentration. If T4, with a free fraction of about1:4000 in undiluted serum, is compared with a drug that hasa free fraction in serum of 1:50, progressive dissociation willsustain the free T4 concentration at 1:100 dilution, while thefree drug concentration decreases markedly after a dilution ofonly 1:10. This difference leads to an under-estimate of freeT4 after sample dilution, as demonstrated by comparing theT4-displacing effect of frusemide in three commercial freeT4 assays; the effect of frusemide was least obvious in themethod with highest sample dilution (Figure 1). Because ofthis effect, the apparent free T4 concentration in diluted samples will be an under-estimate in the presence of hightherapeutic concentrations of drugs such as phenytoin, carbamazepine, frusemide, mefenamic acid (Ponstan) andsalicylate.
11
Figure 1. Effect of addition of frusemide to normal serum onestimates of free T4 using three commercial free T4 methodsthat involve varying degrees of sample dilution. The effect ofthe competitor is progressively obscured with increasingsample dilution. Redrawn from reference 22.
In contrast to such under-estimates of free T4, heparin has theopposite effect to increase the apparent free T4 concentration,due to an in vitro artefact of sample storage.
12In the presence
of a normal serum albumin concentration, non-esterified fattyacid (NEFA) concentrations >3 mmol/L will increase free T4by displacement from TBG, but such concentrations areuncommon in vivo. However, serum NEFA may increase tothese levels during storage or incubation of samples fromheparin-treated patients, as a result of heparin-induced lipaseactivity (Figure 2). This effect is accentuated if serum triglyceride concentrations are high, serum albumin concentration is low, or incubation at 37
oC is prolonged;
under these conditions doses of heparin as low as 10 units may produce this artefact, low molecular weight heparinpreparations have a similar effect.
The fallibility of current free T4 methodology is demonstratedby a study of bias in nine commonly used commercial methods in relation to an equilibrium dialysis referencemethod,
13see below. Hence it is absolutely essential, especially
in pregnant women and in patients with an associated illness, to interpret results only in relation to a specific method.
13 It is becoming clear that, in numerous
clinical situations, free T4 estimation does not serve as arobust, reliable index of thyroid function. Despite the theoretical attraction of measuring the concentration of freeor biologically active hormone, it remains uncertain whethercurrent free T4 methodology is any improvement over anuncontentious measurement of total T4. The limitations of freeT4 methodology are most evident where the diagnosis of thyroid dysfunction is clinically and analytically most difficult. For this reason, it is important that total T4 methodsbe retained for reference.
The TSH-T4 Relationship
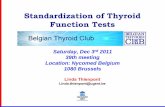
Whatever strategy is used for first-line testing, a sensitiveserum TSH assay and an estimate of serum free T4 are both necessary for definitive assessment of thyroid status. Asshown in Figure 3, the common types of thyroid dysfunctioncan be identified in a single sample from characteristic diagonal deviations in the normal free T4-TSH relationship.
114 Clin Biochem Rev Vol 24 November 2003
Stockigt J
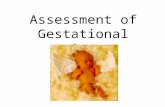
Figure 2. Mechanism of heparin-induced increase in apparent serum free T4.
9Heparin acts in vivo (left) to
liberate lipoprotein lipase from vascular endothelium. Lipaseacts in vitro to increase the concentration of non-esterifiedfatty acids; concentrations above 2-3 mmol/L displace of T4and T3 from TBG. This effect is accentuated by low serumalbumin and high triglyceride concentrations and by sample incubation at 37C.
-
The figure shows primary hypothyroidism due to target glandfailure (high serum TSH, low free T4 : A), failure of TSHsecretion (both low: B), autonomous or abnormally stimulatedtarget gland function (high free T4, suppressed TSH: C), andprimary excess of TSH, or thyroid hormone resistance (both high: D). Abnormal results that fall outside these areas suggest that some other factor has disturbed the TSH-free T4relationship. (The link between components of other feedback systems can also be applied to the investigation ofhypogonadism, glucocorticoid and mineralocorticoid abnormalities, hypoglycaemia, hypercalcaemia etc.)
The diagnostic validity of this relationship depends on anumber of assumptions and limiting conditions (Table 6). Itis notable that only the last three of these assumptions can bevalidated in the laboratory; the first three must be verifiedclinically. The first assumption, steady-state conditions, should be questioned when associated illness or medicationsperturb the pituitary-thyroid axis; the large differencebetween the half-lives of TSH (one hour) and T4 (one week)
115Clin Biochem Rev Vol 24 November 2003
Assessing Thyroid Function
Assumptions and Limiting Conditions
1. Steady-state conditions (N.B. difference in half-life of TSH and T4 )Acute effects of medications Early response to therapy Evolution of transient thyroid dysfunction Recovery from severe illness
2. Normal trophic-target hormone relationshipAlternative thyroid stimulators
ImmunoglobulinsChorionic gonadotrophin
MedicationsT3 , triiodothyroacetic acidGlucocorticoidsDopamineAmiodarone
Recent thyrotoxicosisRecent longstanding hypothyroidism (Figure 5)Variable individual setpointTSH receptor mutations
3. Tissue responses proportional to serum free T4 concentrationT3 excessHormone resistance syndromesSlow onset/offset of thyroid hormone actionDrug effects ? (amiodarone, phenytoin)
4. Accurate estimate of active hormone concentrationAlternative agonist in excess (e.g.T3)Changes in serum binding proteinsTSH of altered biologic activity (pituitary disorders)Spurious assay results
TSHHeterophilic antibodies
Free T4 Circulating inhibitors of bindingHeparin artefact (Figure 2)Rheumatoid factor
5. Appropriate reference rangesInfluence of ageMedicationsAssociated illnessNutrition
6. Adequate assay sensitivityPoor precision at TSH detection limit.
Table 6. The free T4 -TSH relationship in the assessmentof thyroid status.
Figure 3. The relationship between serum TSH and total freeT4 concentrations in normal subjects (N) and in various typical abnormalities of thyroid function: primary hypothyroidism (A); central or pituitary-dependent hypothy-roidism (B); thyrotoxicosis due to autonomy or abnormalthyroid stimulation (C); and TSH-dependent thyrotoxicosisor generalised thyroid hormone resistance (D).Note that linear free and total T4 responses correspond tologarithmic TSH changes. Findings at A and C represent primary thyroid abnormalities, while results in areas B and Dsuggest a primary pituitary abnormality. Results in the intermediate areas are most often due to non-steady state sampling conditions, or an altered T4 -TSH relationship.
-
accounts for many transient non-diagnostic abnormalities, especially during critical illness. In several situationsT3 as well as T4 is an important, or dominant, determinant of thyroid status.The relevance of serum free T3 measurement is summarized in Table 7.Note that serum free T3 is of little value inmonitoring T3 treatment because of widevariations that depend on the intervalbetween dosage and sampling.
The TSH First Testing Strategy
Either serum TSH or free T4 can be usedfor initial screening and case finding, butTSH gives better first line testing than freeT4, at slightly higher cost. Because thyroidgland abnormalities are 10-20 times morecommon than variations due to pituitary dysfunction, TSHchanges can generally be regarded as giving an inversereflection of thyroid status. An algorithm for the assessment of thyroid function based on initial measurement of TSH is shown in Figure 4. However, thereare important situations in which TSH alone can give a misleading or ambiguous assessment of thyroid status (Table8), despite the high negative predictive value of a normal serum TSH concentration in ruling out primaryhypothyroidism or thyrotoxicosis.
Clinical Applications
Application of diagnostic strategy will differ depending onthe test group, i.e. testing of untreated subjects in whom clinical features suggest thyroid dysfunction, screening orcase finding in at risk groups, evaluation of the response totreatment, or assessment when associated illness or drug therapy are likely to complicate both clinical and laboratoryassessment.
Untreated Subjects
Assessment of untreated subjects now commonly begins withmeasurement of TSH alone, with free T4 and/or free T3added only if TSH is abnormal, or if an abnormality of TSHsecretion is suspected. According to this algorithm, free T4should be measured to distinguish between overt and subclinical hypothyroidism when serum TSH is elevated,while a suppressed or subnormal TSH level should be followed by assay of both free T4 and free T3 to distinguishsubclinical from overt thyrotoxicosis and to identify T3 toxicosis.
116 Clin Biochem Rev Vol 24 November 2003
Stockigt J
RequiredPotential thyrotoxicosis with suppressed TSH
and normal serum free T4.During antithyroid drug therapy to identify
persistent isolated T3 excess. Diagnosis of amiodarone-induced thyrotoxicosis.
Useful Early recurrence of thyrotoxicosis.Extent of T3 excess during suppressive T4 therapy
or after T4 overdose
Not required or misleadingDiagnosis of hypothyroidismDuring critical illnessDuring routine T4 replacementScreening of asymptomatic subjectsMonitoring of T3 treatment
Table 7. Indications for measurement of serum free T3
Figure 4. Algorithm for the assessment of thyroid functionbased on initial assay of serum TSH. Abnormal TSH valueslead to further assays as shown. Assays of free T4 are alwaysrequired if pituitary dysfunction is suspected, during theearly treatment of thyroid dysfunction, during critical illnessand with the use of drugs that influence the pituitary-thyroidaxis. (* Further testing is indicated if pituitary dysfunction isknown or suspected, during critical illness and in the first 6-12 months of treatment for thyroid dysfunction).
-
Response to Treatment
In patients with newly treated thyrotoxicosis, TSH mayremain suppressed for several months after normalisation ofserum free T4 and free T3; serious over-treatment may resultif TSH alone is used for adjustment of antithyroid drugdosage. Furthermore, during drug treatment, thyrotoxicosis may persist due solely to T3 excess. Hence, reassessment ofserum free T4 and free T3 levels is recommended after about3-4 weeks drug treatment of thyrotoxicosis to allow appropriate dose adjustment. During long-term treatment,TSH generally gives a reliable guide to optimal drug dosage.
Similarly, during long-term replacement or suppressive therapy with T4, serum TSH is the best single index of
appropriate dosage. Optimal replacement is generally reflected by a low-normal TSH value of about 1 mU/L, often with a slightly increased level of serum free T4. However,during the early phase of treatment of hypothyroidism, freeT4 should also be measured because TSH may remain inappropriately elevated for many months after normalisationof T4 (Figure 5). In general, serum TSH should initially be checked after 2-3 months, but need only be checked annually after the first year of treatment.
During TSH suppressive therapy with T4, for example in the management of differentiated thyroid cancer, periodic assessment of free T4 and free T3 in addition to TSH, is
117Clin Biochem Rev Vol 24 November 2003
Assessing Thyroid Function
Condition TSH Free T4 Free T3
Abnormal TSH secretionThyrotoxicCentral TSH excess N-H H HHypothyroidPituitary-hypothalamic disturbance L-N LVery low birth weight premature infants L-N LEuthyroidThyroid hormone resistance N,H H H
ThyrotoxicosisSubclinical U N NEarly Treatment U H-N-L H-N-L
HypothyroidismSubclinical H NEarly Treatment H L-N
TSH Assay ArtefactEuthyroid subject H N NThyrotoxic subject L-N-H H H
MedicationsDopamine L NGlucocorticoids L N
Critical illnessEuthyroid subject U,L L,N LHypothyroid subject N L,N
____________________________________________U: undetectable TSH
-
appropriate to limit the degree of thyroid hormone excess,because over-treatment can have important adverse effects onthe cardiovascular system and on bone density. In the treatment of hypothyroidism due to pituitary or hypothalamicdisease, serum TSH is of no value in assessing T4 dosage,which should be judged from clinical response and serumfree T4.
Difficult Diagnostic Situations
Especially in hospital practice, interpretation of thyroid function is often compromised by associated illness or bymedications. There is a high prevalence of abnormal serumfree T4 or TSH values in patients with acute medical or psychiatric illness, but when TSH and free T4 are consideredtogether, as in Figure 3, few of these abnormalities indicatetrue thyroid dysfunction. Clinical assessment of thyroid status is difficult in the face of associated disease and somehave advocated widespread laboratory testing. However,because of low specificity, opinion has moved away fromroutine testing during critical illness unless there is a clinicalindication.
During any severe illness, one or more of the assumptionsoutlined in Table 6 may not be valid, for example when thereare wide fluctuations from the steady state due to acute inhibition of TSH secretion or abnormally rapid T4 clearance. Serum free T4 estimates are prone to multiplemethod-dependent interferences, for example due to heparin(see above Figure 2). Measurement of total T4 continues to
have a definite place in the assessment of potential difficultieswith various free T4 estimates, particularly during critical illness, as demonstrated by a key study of severely ill euthyroid patients (Figure 6).
14Various free T4 assays gave
widely discrepant method-dependent abnormal free T4 estimates, while the total T4 assay suggested that the majority of these patients remained euthyroid, with subnormal serum TSH, probably attributable to glucocorticoidtreatment.
14Free T4 methods that were influenced by
albumin binding of tracer tended to give subnormal estimates, while equilibrium dialysis and related methodsappeared to be vulnerable to the heparin-NEFA artefact, witha trend towards high free T4 estimates.
There are important issues in selecting a panel of thyroid teststhat will best serve a particular clinical population. Forexample, the multiple effects of severe illness on free T4 estimates may be of minor importance for a laboratory thatserves predominantly ambulatory patients. A different assayprofile will be required in a laboratory that needs to excludethyroid dysfunction during critical illness or in pregnancy.
Effects of Medications on Serum T4 and TSH
The multiple effects of medications on the pituitary-thyroidaxis are summarized in Table 5. Effects on serum TSH aregenerally physiological, whereas most effects on free T4estimates are methodological. Notably, lithium and iodine-rich compounds, in particular amiodarone, can causethyroid function to become abnormal. Amiodarone is themost complex and difficult drug that affects thyroid status.
15
There may be poor correlation between circulating thyroidhormone levels and clinical manifestations in amiodarone-induced thyroid dysfunction, because of interaction of thisdrug or its metabolites with thyroid hormone receptors. Iniodine-replete regions the predominant amiodarone-inducedthyroid abnormality is hypothyroidism, which is especiallyprevalent in those with associated autoimmune thyroiditis.Amiodarone causes two forms of thyrotoxicosis, one duedirectly to iodine excess and the other attributed to a uniquetype of thyroiditis. Benign euthyroid hyperthyroxinaemiaoccurs in up to 25% of treated patients, who show increasedserum concentrations of free T4, with normal TSH and normal or low concentrations of free T3.
Lithium, used in the management of bipolar illness, has multiple effects on the pituitary-thyroid axis, the most important being inhibition of hormone release. Lithium canexacerbate, or may initiate autoimmune thyroid disease withdevelopment of goitre and eventual hypothyroidism; thereare also some reports of lithium-induced thyrotoxicosis.Serum TSH, free T4 and free T3 assays generally give a trueindex of thyroid status during lithium treatment.
118 Clin Biochem Rev Vol 24 November 2003
Stockigt J
Figure 5. Serial changes in serum free T4 and TSH inresponse to T4 replacement in a patient with longstandingsevere untreated primary hypothyroidism without evidenceof pituitary enlargement or tumour. Normalization of serumTSH lagged 7-10 months behind normalization of serum freeT4.
-
Phenytoin commonly results in subnormal serum total T4,with an apparent lowering of free T4, due predominantly to the dilution-related artefact described above, without theanticipated increase in TSH. Such findings are hard to distinguish from central hypothyroidism due to pituitary deficiency, but the major discrepancy is probably a methodological artefact related to underestimation of free T4in diluted serum samples.
16The assessment of patients who
have had pituitary surgery and are also taking phenytoin,remains very difficult.
Antibody Measurements17
In subclinical hypothyroidism, the presence of TPO antibodies indicates a 4-5-fold increase in the chance of developing overt hypothyroidism. The presence of this antibody also indicates an increased likelihood of postpartum thyroiditis or amiodarone-induced hypothyroidism. The finding of persistently positive thyrotropin receptor antibody(TRAb) is useful in indicating that apparent remission ofGraves disease is unlikely to be sustained. TRAb measurement can also indicate the possibility of neonatal orintrauterine thyrotoxicosis in the infant of a mother withautoimmune thyroid disease and may also define the aetiology of atypical eye disease.
Thyroglobulin18
Serum thyroglobulin concentrations should always be interpreted in relation to the prevailing level of TSH, whichis responsive to alterations in thyroid hormone dosage. In thelong-term follow-up of differentiated thyroid cancer, anundetectable serum thyroglobulin concentration in the presence of high serum TSH indicates effective ablation ofdifferentiated thyroid tissue, benign and malignant. Such afinding may justify less rigorous long-term T4-induced suppression of TSH. Thyroglobulin is undetectable in thyrotoxicosis factitia, and generally extremely high in subacute thyroiditis and in amiodarone-induced thyrotoxicosisdue to thyroiditis.
There are still unsolved technical problems in the optimisation of thyroglobulin assays. Major issues relate to assay standardization, interference from endogenous anti-thyroglobulin antibodies and heterophilic antibodies, aswell as inherent problems of assay sensitivity.
The Laboratory-Clinical Interface
The diverse clinical presentations of thyroid dysfunctionmandate laboratory requests from clinicians who may beunfamiliar with the interpretation of current assays, or witheffects that interfere with these techniques. Comments fromthe laboratory can improve clinical response; the quality ofthis assistance depends on both the training and experience of the reporter and the available clinical information.
119Clin Biochem Rev Vol 24 November 2003
Assessing Thyroid Function
Figure 6. Free T4 estimates by six different kit methods in euthyroidpatients after bone marrow transplantation. Therapy included heparinand glucocorticoids. Mean values arenormalized to 100%, with reference limits shown by the boxes. A high proportion of free T4 estimates areabnormal, either increased or decreased,depending on the method. Serum total T4remained normal in 19 of the 20 studysubjects, while serum TSH was subnormal in 11, independent of themethod. Redrawn from reference 14.
-
The competitive binding assays that are used for thyroiddiagnosis were developed about 30 years ago with in house reagents. Optimal diagnostic technology was initially available only to specialists and results were often slow.Sophisticated standardised reagents and automated instrumentation (eg solid phase antibodies, magnetic separation systems, chemiluminescent detection systems)have now replaced these early methods; results are rapidlyavailable to a wide range of practitioners. Non-specialistusers of endocrine assays are most likely to benefit from laboratory-based assistance in the interpretation of results,but with assay automation, laboratorians have become more distant from the bedside. As clinicians receive less assistance,they provide progressively less relevant information and viceversa. Laboratorians, in turn may see results that are uninterpretable or ambiguous unless the relevant clinical information is available (Table 9). In these situations, thepossibility of an assay artefact would need to be considered,but review of the clinical context often resolves an apparentlyanomalous result, so that assay validity is affirmed andunnecessary further investigation is avoided.
Discordant or Anomalous Results
After review of the clinical context, the following steps arehelpful in evaluating anomalous thyroid results: a. Review of the medication history.b. Confirmation of serum TSH by an alternative
method that identifies the degree of TSH suppression.
c. Follow-up sampling to establish whether the abnormality is transient or persistent.
d An alternative estimation of serum free T4, avoiding one-step methods that are known to frequently give spurious results, especially during critical illness.
e. Measurement of serum total T4 to establish whether the serum free T4 estimate is disproportionately high or low, due to a pre-analytical or method-dependent artefact.
f. Evaluation of the sample for possible heterophilic antibody interference; note that there are no established criteria that rule out such interference.
g. Investigation of propositus and family members forevidence of unusual binding abnormalities or hormone resistance.
120 Clin Biochem Rev Vol 24 November 2003
Stockigt J
Clinical context Assay Results
Free T4 Free T3 TSH
Pregnancy L* L,N NAntithyroid drug treatment, initial months H,N,L H,N,L URecent T4 therapy for hypothyroidism N N HHypothyroidism, appropriate T4 dose H N NHypothyroidism, intermittent compliance H,N HAppropriate T4 suppressive therapy H N U,LExcessive T3 treatment L H,N
U
Recombinant TSH, suppressive T4 H N HHHypopituitarism L L,NPhenytoin L* L,NCritical illness L* L LHeparin effect in critical illness L,N,H* L LRecovery phase of critical illness L,N HDrugs that inhibit T4&T3 binding to TBG L* L* L,NAmiodarone effect in euthyroid subject H L NAcute T4 overdose HH H,N N___________________________________________________________U undetectable; L low; N normal; H high; * effect dependent on assay method # typical reference intervals are shown in Table 10. depends on interval between dosage and sampling
Table 9. Clinical correlation is required for interpretation of laboratory results #
-
Clinical Feedback, Quality Assurance and CostEffectiveness
Clinical feedback will remain a key aspect of quality assurance in laboratory testing. While assay precision orreproducibility can be evaluated from the laboratory, diagnostic accuracy requires clinical correlation.
The majority of thyroid diagnosis is now quite straightforward, but it is easy to underestimate problems thatremain, since they represent only a small fraction of the total.Despite the elegance and ingenuity of current assay techniques, diagnostic inaccuracy of immunoassays still wastes substantial resources and studies of "cost effectiveness" do not evaluate the human costs that result from unnecessary further testing, false alarms and inappropriate management.
19
Some thyroid disorders, notably papillary, follicular andmedullary carcinomas require follow-up by tumour markerassays over many years. Changes in thyroglobulin and calcitonin assay methodology made without clinical consultation, in particularly changes made before the lowerlimits of detection have been critically defined, (i.e. apparentincrease in sensitivity with loss of specificity), can give afalse and at times disastrous impression of reactivation of disease.
Footnote: Typical reference intervals for common thyroidassays are given in Table 10.
References
1. National Academy of Clinical Biochemistry.Laboratory Medicine Practice Guidelines.Laboratory Support for the Diagnosis of Thyroid Disease. Thyroid 2003;13:1-126 andwww.nacb.org/lmpg/thyroid_LMPG_word.stm
2. For references to specific points in this text see:Thyroid Disease Manager Chapter 6b. ClinicalStrategies for Thyroid Function Testing. www.thyroidmanager.org
3. Haddow JE, Palomaki GE, Allan WC et al. Maternalthyroid deficiency during pregnancy and subsequentneuropsychological development of the child. NewEngl J Med 1999;341:549-55.
4. Andersen S, Pedersen KM, Bruun NH, Laurberg P.Narrow individual variations in serum T4 and T3 in normal subjects: a clue to the understanding of sub-clinical thyroid disease. J Clin Endocrinol Metab2002;87:1068-72.
5. Vanderpump MPJ, Tunbridge WMG, French JM, etal. The incidence of thyroid disorders in the com-munity: a twenty-year follow-up of the WhickhamSurvey. Clin Endocrinol 1995;43:55-68.
6. Hollowell JG, Staehling NW, Flanders WD, et al.Serum TSH, T4 and thyroid antibodies in the UnitedStates population (1988 to 1994): national healthand nutrition examination survey (NHANES III). JClin Endocrinol Metab 2002;87:489-99.
7. Michelangeli V, Feddermal P, Chew G, Kaye J,Knuiman M, Leedman P. Prevalence of thyroid anti-bodies in a community population. Proc Endo SocAust 2001;44:53 (Abstract No. 208).
8. Stuckey BG, Kent GN, Allen JR. The biochemicaland clinical course of post-partum thyroid dysfunc-tion; the treatment decision. Clin Endocrinol2001;54:377-83.
9. Eggertsen R, Petersen K, Lundberg P-A, et al.Screening for thyroid disease in a primary care unitwith a thyroid stimulating hormone assay with a lowdetection limit. Br Med J 1988;297:1586-92.
10. Petersen K. Lindstedt G. Lundberg PA, et al.Thyroid disease in middle-aged and elderly Swedishwomen; thyroid-related hormones, thyroid dysfunc-tion and goitre in relation to age and smoking. JIntern Med 1991;229:407-13.
11. Stockigt JR, Free thyroid hormone measurement: acritical appraisal. Endocr Metab Clin N Am2001;30:265-89.
12. Mendel CM, Frost PH, Kunitake ST, Cavalieri RR.Mechanism of the heparin-induced increase in theconcentration of free thyroxine in plasma. J ClinEndocrinol Metab 1987;65:1259-64.
13. Sapin R, d'Herbomez M. Free thyroxine measuredby equilibrium dialysis and nine immunoassays insera with various thyroxine-binding capacities. Clin
121Clin Biochem Rev Vol 24 November 2003
Assessing Thyroid Function
Table 10. Typical Reference Ranges for Serum ThyroidHormones and TSH*
Hormone Reference Range
Total thyroxine (T4) 60-140 nmol/L
Free T4 10-25 pmol/L
Total triiodothyronine (T3) 1.1-2.7 nmol/L
Free T3 3-8 pmol/L
TSH 0.4-4.0 mU/L
* Ranges should be determined for the particular methods used in each laboratory.
Higher values in childhood.
-
Chem 2003;49:1531-5.14. Sapin R, Schleinger J-L, Gasser F et al. Intermethod
discordant free thyroxine measurements in bonemarrow transplanted patients. Clin Chem2000;46:418-22.
15. Daniels GH. Amiodarone-induced thyrotoxicosis JClin Endocrinol Metab 2001;86:3-8.
16. Surks MI, DeFesi CR. Normal serum free thyroidhormone concentrations in patients treated withphenytoin or carbamazepine. JAMA1996;275:1495-8
17. Saravanan P, Dayan CM. Thyroid autoantibodiesEndocr Metab Clin N Am 2001;30:315-38.
18. Torrens JI, Burch HB. Serum thyroglobulin meas-urement: utility in clinical practice. Endocr MetabClin N Am 2001;30:429-68.
19. Kricka LJ. Interferences in radioimmunoassay - stilla threat. Clin Chem 2000;46:1037-8.
20. Helfand M, Redfern CC. Screening for thyroid disease; an update. Ann Int Med 1998;129:144-58.
21. Parle JV, Maisonneuve M, Sheppard MC et al.Prediction of all-cause and cardiovascular mortalityin elderly people from one low serum thyrotropinresult: a ten year cohort study. Lancet2001;358:861-5.
22 Hawkins RC: Furosemide interference in newer freethyroxine assays. Clin Chem 1998;44:2550-1.
122 Clin Biochem Rev Vol 24 November 2003
Stockigt J
/ColorImageDict > /JPEG2000ColorACSImageDict > /JPEG2000ColorImageDict > /AntiAliasGrayImages false /CropGrayImages true /GrayImageMinResolution 300 /GrayImageMinResolutionPolicy /OK /DownsampleGrayImages true /GrayImageDownsampleType /Bicubic /GrayImageResolution 300 /GrayImageDepth -1 /GrayImageMinDownsampleDepth 2 /GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true /GrayImageFilter /DCTEncode /AutoFilterGrayImages true /GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict > /GrayImageDict > /JPEG2000GrayACSImageDict > /JPEG2000GrayImageDict > /AntiAliasMonoImages false /CropMonoImages true /MonoImageMinResolution 1200 /MonoImageMinResolutionPolicy /OK /DownsampleMonoImages true /MonoImageDownsampleType /Bicubic /MonoImageResolution 1200 /MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000 /EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode /MonoImageDict > /AllowPSXObjects false /CheckCompliance [ /None ] /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false /PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox true /PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXOutputIntentProfile () /PDFXOutputConditionIdentifier () /PDFXOutputCondition () /PDFXRegistryName () /PDFXTrapped /False
/Description > /Namespace [ (Adobe) (Common) (1.0) ] /OtherNamespaces [ > /FormElements false /GenerateStructure true /IncludeBookmarks false /IncludeHyperlinks false /IncludeInteractive false /IncludeLayers false /IncludeProfiles true /MultimediaHandling /UseObjectSettings /Namespace [ (Adobe) (CreativeSuite) (2.0) ] /PDFXOutputIntentProfileSelector /NA /PreserveEditing true /UntaggedCMYKHandling /LeaveUntagged /UntaggedRGBHandling /LeaveUntagged /UseDocumentBleed false >> ]>> setdistillerparams> setpagedevice