Lab Rounds Juliette Sacks CCFP-EM August 10, 2006.
23
Lab Rounds Lab Rounds Juliette Sacks Juliette Sacks CCFP-EM CCFP-EM August 10, 2006 August 10, 2006
-
Upload
elaine-henry -
Category
Documents
-
view
220 -
download
1
Transcript of Lab Rounds Juliette Sacks CCFP-EM August 10, 2006.
Lab RoundsLab Rounds
Juliette SacksJuliette Sacks
CCFP-EMCCFP-EM
August 10, 2006August 10, 2006
CaseCase
L.W. 49 y.o. FemaleL.W. 49 y.o. Female 3-4 day hx of:3-4 day hx of:
disorientationdisorientation dysarthriadysarthria progressing ataxiaprogressing ataxia dysphagiadysphagia no vomiting no vomiting acute on chronic diarrheaacute on chronic diarrhea no hx of trauma, seizures or LOCno hx of trauma, seizures or LOC no drug or EtOH abuseno drug or EtOH abuse
Case cont’dCase cont’d
FHx: adoptedFHx: adopted Collateral Hx: from pt’s daughter who is Collateral Hx: from pt’s daughter who is
primary caregiverprimary caregiver NKDANKDA Meds:Meds:
Lithium 120mg qhsLithium 120mg qhs Zyprexa 10mg at noon and 20mg qhsZyprexa 10mg at noon and 20mg qhs Zopiclone 22.5mg qhsZopiclone 22.5mg qhs Propanolol 40mg at noon and 40mg qhsPropanolol 40mg at noon and 40mg qhs
Case cont’d:Case cont’d: PMHx/Sx: PMHx/Sx:
Bipolar disorderBipolar disorder Chronic diarrheaChronic diarrhea Multiple laparotomies with ileostomyMultiple laparotomies with ileostomy
Px:Px: Tremulous, dysarthricTremulous, dysarthric 118/56 61 18 36.7C 02 sats 97% on 3L by NP118/56 61 18 36.7C 02 sats 97% on 3L by NP Chest clearChest clear CVS NCVS N Abdo distended but nontenderAbdo distended but nontender CN intact, clonus, incr. DTRs, generalized muscle CN intact, clonus, incr. DTRs, generalized muscle
weaknessweakness
ResultsResults
Na 133, K 3.9Na 133, K 3.9 Troponin, CK, LFTs N, Cr 100Troponin, CK, LFTs N, Cr 100 EtOH, APAP, ASA negativeEtOH, APAP, ASA negative Hgb 136, WBC 5.2, Plt 272Hgb 136, WBC 5.2, Plt 272 Li 3.96Li 3.96 EKG: Anterior T wave depressionEKG: Anterior T wave depression AXR: ++ dilated loops of large bowel with air AXR: ++ dilated loops of large bowel with air
fluid levels; no free airfluid levels; no free air CT head: NCT head: N
LithiumLithium
Commonly used to treat depressive and Commonly used to treat depressive and bipolar affective disorderbipolar affective disorder
Low therapeutic indexLow therapeutic index Intoxication seen with acute and chronic Intoxication seen with acute and chronic
useuse Multisystem dysfunction with intoxicationMultisystem dysfunction with intoxication T1/2: 29hT1/2: 29h
Lithium DosingLithium Dosing
Therapeutic indices: Therapeutic indices: 0.6 - 1.2 mEq/L (prophylactic control)0.6 - 1.2 mEq/L (prophylactic control) 1.0 - 1.5 mEq/L (acute mania)1.0 - 1.5 mEq/L (acute mania)
Oral administration onlyOral administration only Absorbed from GIT 2-4h postingestionAbsorbed from GIT 2-4h postingestion Minimally protein boundMinimally protein bound Steady state plasma levels achieved in 5d Steady state plasma levels achieved in 5d
Lithium ExcretionLithium Excretion
Excreted through the kidneys therefore Excreted through the kidneys therefore dosing is dependent on: renal function, dosing is dependent on: renal function, volume status, age volume status, age
Reabsorbed in the proximal tubuleReabsorbed in the proximal tubule 20% is excreted in urine20% is excreted in urine LiLi reabsorption follows Na reabsorption but reabsorption follows Na reabsorption but
may be reabsorped preferentially to may be reabsorped preferentially to counter Na losses in volume depleted ptscounter Na losses in volume depleted pts

More about Li…More about Li…
Lithium alters the cation transport across Lithium alters the cation transport across cell membranes in nerve and muscle cellscell membranes in nerve and muscle cells
Influences reuptake of serotonin and Influences reuptake of serotonin and epinephrineepinephrine
Inhibits second messenger systems Inhibits second messenger systems involving phosphatidylinositol cycleinvolving phosphatidylinositol cycle
Inhibits postsynaptic D2 receptor Inhibits postsynaptic D2 receptor sensitivitysensitivity
Factors predisposing to Li ToxicityFactors predisposing to Li Toxicity(courtesy of Tintinalli)(courtesy of Tintinalli)
Renal failureRenal failure Volume depletionVolume depletion Hyperthermia/NMSHyperthermia/NMS InfectionInfection CHFCHF Diabetes mellitusDiabetes mellitus GastroenteritisGastroenteritis Surgery Surgery CirrhosisCirrhosis Decreased Na intakeDecreased Na intake
Drug interactions with LiDrug interactions with Li(courtesy of Tintinalli)(courtesy of Tintinalli)
Major: HaloperidolMajor: Haloperidol Moderate: Moderate:
ACEIACEI - Methyldopa- Methyldopa AnorexiantsAnorexiants - Metronidazole- Metronidazole BenzodiazepinesBenzodiazepines - NSAIDs- NSAIDs CaffeineCaffeine - Phenytoin- Phenytoin CCBCCB - Tetracyclines- Tetracyclines CarbamazepineCarbamazepine - Theophyllines- Theophyllines ClozapineClozapine - Thiazide diuretics- Thiazide diuretics FluoxetineFluoxetine - Urea- Urea Iodide saltsIodide salts - Succinylcholine- Succinylcholine Loop diureticsLoop diuretics - Nondepolarizing muscle paralytics- Nondepolarizing muscle paralytics- PhenothiazinesPhenothiazines - TCAs- TCAsMinor: Carbonic anhydrase inhibitors, sympathomimeticsMinor: Carbonic anhydrase inhibitors, sympathomimetics
Clinical ManifestationsClinical Manifestations GI:GI:
Nausea and vomitingNausea and vomiting DiarrheaDiarrhea
CNS:CNS: Weakness and fatigueWeakness and fatigue Lethargy and confusionLethargy and confusion Tremor (coarse, irregular)Tremor (coarse, irregular) AtaxiaAtaxia SeizuresSeizures Neuromuscular excitability/fascicular twitchingNeuromuscular excitability/fascicular twitching StuporStupor ComaComa
Clinical Manifestations 2Clinical Manifestations 2
Renal: Renal: May cause acute renal failureMay cause acute renal failure Decreased CrClDecreased CrCl Nephrogenic diabetes insipidusNephrogenic diabetes insipidus
• With polyuria and polydipsiaWith polyuria and polydipsia
CV:CV: HypotensionHypotension Sinus bradycardiaSinus bradycardia Ventricular dysrhythmias (including complete heart block)Ventricular dysrhythmias (including complete heart block) EKG findings in chronic Li use: depressed ST segments and T EKG findings in chronic Li use: depressed ST segments and T
wave flattening/inversion; QTc prolongationwave flattening/inversion; QTc prolongation CV collapse and respiratory failureCV collapse and respiratory failure
Clinical Manifestations 3Clinical Manifestations 3
Neurological sequelae:Neurological sequelae: 10% risk of permanent damage10% risk of permanent damage Truncal and gait ataxiaTruncal and gait ataxia NystagmusNystagmus Short term memory deficitsShort term memory deficits DementiaDementia
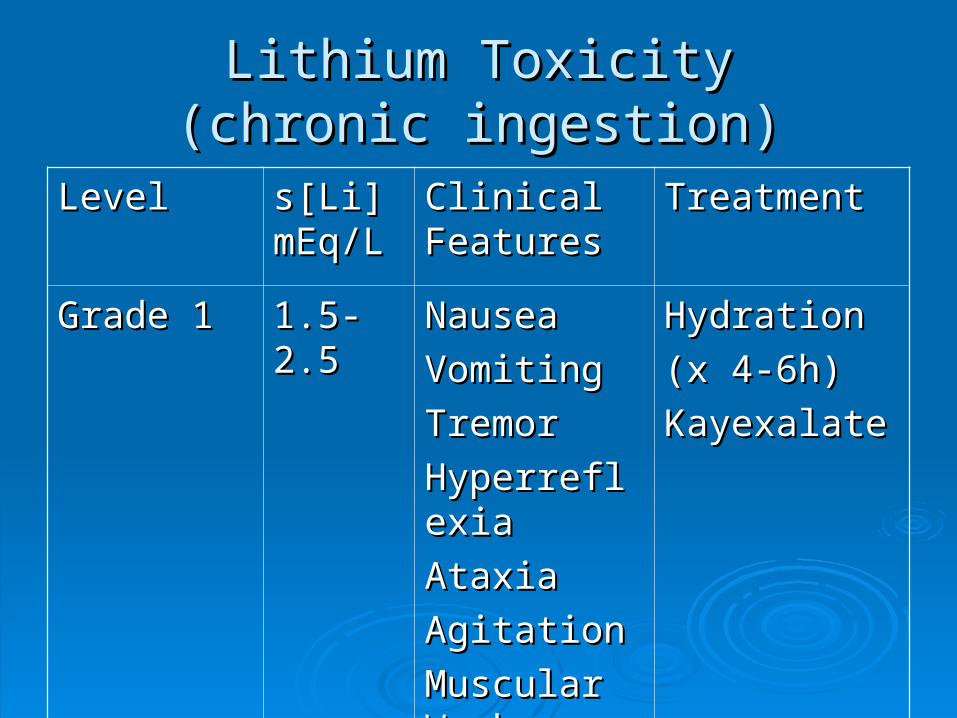
Lithium ToxicityLithium Toxicity(chronic ingestion)(chronic ingestion)
LevelLevel s[Li] s[Li] mEq/LmEq/L
Clinical Clinical FeaturesFeatures
TreatmentTreatment
Grade 1Grade 1 1.5-2.51.5-2.5 NauseaNausea
VomitingVomiting
TremorTremor
HyperreflexiaHyperreflexia
AtaxiaAtaxia
AgitationAgitation
Muscular Muscular WeaknessWeakness
Hydration Hydration
(x 4-6h)(x 4-6h)
KayexalateKayexalate
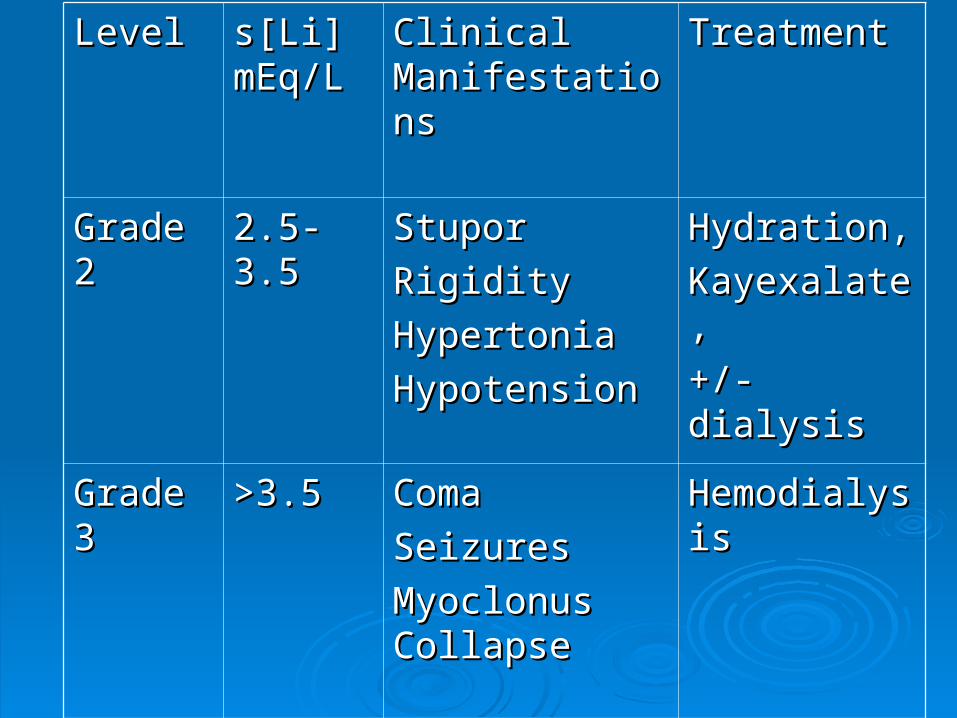
LevelLevel s[Li] s[Li] mEq/LmEq/L
Clinical Clinical ManifestationsManifestations
TreatmentTreatment
Grade 2Grade 2 2.5-3.52.5-3.5 Stupor Stupor
RigidityRigidity
HypertoniaHypertonia
HypotensionHypotension
Hydration,Hydration,
Kayexalate,Kayexalate,
+/- dialysis+/- dialysis
Grade 3Grade 3 >3.5>3.5 Coma Coma
SeizuresSeizures
Myoclonus Myoclonus CollapseCollapse
HemodialysisHemodialysis
TreatmentTreatment
ABCsABCs iv fluids, cardiac monitoringiv fluids, cardiac monitoring EKG EKG Identification of agents and amount ingested (get the pill Identification of agents and amount ingested (get the pill
bottles if possible) bottles if possible) Beware sustained release preparations!Beware sustained release preparations! Rule out co-ingestionsRule out co-ingestions Serum Li with 2Serum Li with 2ndnd sLi 2h later sLi 2h later Lytes, Cr, BUN, tox screenLytes, Cr, BUN, tox screen Hx and PxHx and Px +/- CT head depending on neurological presentation+/- CT head depending on neurological presentation
Treatment cont’dTreatment cont’d
Restore fluid volume and correct Restore fluid volume and correct electrolyte abnormalitieselectrolyte abnormalities
Oral charcoal does not bind Li but may Oral charcoal does not bind Li but may bind other drugs takenbind other drugs taken
Whole bowel irrigation may be considered Whole bowel irrigation may be considered especially with SR preparationsespecially with SR preparations If given within 1h of ingestion may remove If given within 1h of ingestion may remove
60% of drug60% of drug
HemodialysisHemodialysis
For severe lithium toxicityFor severe lithium toxicity When?When?
s[Li] >4.0 mEq/L regardless of clinical statuss[Li] >4.0 mEq/L regardless of clinical status s[Li] >2.5 mEq/L with symptoms; with renal s[Li] >2.5 mEq/L with symptoms; with renal
insufficiency or other factor(s) that limit Li insufficiency or other factor(s) that limit Li excretionexcretion
s[Li] 2.5-4.0 mEq/L asymptomatic patient but s[Li] 2.5-4.0 mEq/L asymptomatic patient but who is not expected to have s[Li] <1.0mEq/L who is not expected to have s[Li] <1.0mEq/L w/i 36h w/i 36h
Goal: decrease sLi levels to <1 mEq/L Goal: decrease sLi levels to <1 mEq/L within 6-8h post dialysiswithin 6-8h post dialysis
Li clearance of 70-170 ml/minLi clearance of 70-170 ml/min Use of continuous venovenous Use of continuous venovenous
hemofiltration reduces the post dialysis hemofiltration reduces the post dialysis rebound in sLi levelrebound in sLi level
Addition of bicarbonate to dialysate may Addition of bicarbonate to dialysate may improve Li extractionimprove Li extraction
AdjunctsAdjuncts
Consult renal serviceConsult renal service Consult psychiatric serviceConsult psychiatric service Consult poison control/toxicology serviceConsult poison control/toxicology service
What about L.W.?What about L.W.?
After 4h of fluid replacement, Li level was 3.53 After 4h of fluid replacement, Li level was 3.53 but she remained symptomaticbut she remained symptomatic
Sent for hemodialysisSent for hemodialysis No role for gastric lavage, whole bowel irrigationNo role for gastric lavage, whole bowel irrigation Serial Li levels and >1 course of dialysisSerial Li levels and >1 course of dialysis Persistent neurological deficits despite s[Li] of Persistent neurological deficits despite s[Li] of
1.0-1.1 mEq/L1.0-1.1 mEq/L Lithium discontinued; replaced by olanzepineLithium discontinued; replaced by olanzepine