
BUILDING THE DX LAB FROM SCRATCH: WHAT IS THIS AND WHY DO IT?
Upload
krishna-rathodCategory
view
40download
3description
10ALaboratoryDiagnosis of Upper RespiratoryTract Infections
KEN B. WAITES, MICHAEL A. SAUBOLLE, DEBORAH F. TALKINGTON, STEPHEN A. MOSER, AND VICKIE BASELSKI
COORDINATING EDITOR
SUSAN E. SHARP
CumitechCUMULATIVE TECHNIQUES AND PROCEDURES IN CLINICAL MICROBIOLOGY

Cumitech 1C Blood Cultures IV
Cumitech 2B Laboratory Diagnosis of Urinary Tract Infections
Cumitech 3B Quality Systems in the Clinical Microbiology Laboratory
Cumitech 7B Lower Respiratory Tract Infections
Cumitech 10A Laboratory Diagnosis of Upper Respiratory Tract Infections
Cumitech 12A Laboratory Diagnosis of Bacterial Diarrhea
Cumitech 13A Laboratory Diagnosis of Ocular Infections
Cumitech 16A Laboratory Diagnosis of the Mycobacterioses
Cumitech 18A Laboratory Diagnosis of Hepatitis Viruses
Cumitech 19A Laboratory Diagnosis of Chlamydia trachomatis Infections
Cumitech 21 Laboratory Diagnosis of Viral Respiratory Disease
Cumitech 23 Infections of the Skin and Subcutaneous Tissues
Cumitech 24 Rapid Detection of Viruses by Immunofluorescence
Cumitech 26 Laboratory Diagnosis of Viral Infections Producing Enteritis
Cumitech 27 Laboratory Diagnosis of Zoonotic Infections: Bacterial Infections Obtained from Companion andLaboratory Animals
Cumitech 28 Laboratory Diagnosis of Zoonotic Infections: Chlamydial, Fungal, Viral, and Parasitic InfectionsObtained from Companion and Laboratory Animals
Cumitech 29 Laboratory Safety in Clinical Microbiology
Cumitech 30A Selection and Use of Laboratory Procedures for Diagnosis of Parasitic Infections of theGastrointestinal Tract
Cumitech 31 Verification and Validation of Procedures in the Clinical Microbiology Laboratory
Cumitech 32 Laboratory Diagnosis of Zoonotic Infections: Viral, Rickettsial, and Parasitic Infections Obtainedfrom Food Animals and Wildlife
Cumitech 33 Laboratory Safety, Management, and Diagnosis of Biological Agents Associated with Bioterrorism
Cumitech 34 Laboratory Diagnosis of Mycoplasmal Infections
Cumitech 35 Postmortem Microbiology
Cumitech 36 Biosafety Considerations for Large-Scale Production of Microorganisms
Cumitech 37 Laboratory Diagnosis of Bacterial and Fungal Infections Common to Humans, Livestock, and Wildlife
Cumitech 38 Human Cytomegalovirus
Cumitech 39 Competency Assessment in the Clinical Microbiology Laboratory
Cumitech 40 Packing and Shipping of Diagnostic Specimens and Infectious Substances
Cumitech 41 Detection and Prevention of Clinical Microbiology Laboratory-Associated Errors
Cumitech 42 Infections in Hemopoietic Stem Cell Transplant Recipients
Cumitechs should be cited as follows, e.g.: Waites, K. B., M. A. Saubolle, D. F. Talkington, S. A. Moser, and V. Baselski. 2006. Cumitech10A, Laboratory Diagnosis of Upper Respiratory Tract Infections. Coordinating ed., S. E. Sharp. ASM Press, Washington, D.C.Editorial board for ASM Cumitechs: Alice S. Weissfeld, Chair; Maria D. Appleman, Vickie Baselski, B. Kay Buchanan, Mitchell l.Burken, Roberta Carey, Linda Cook, Lynne Garcia, Mark LaRocco, Susan L. Mottice, Michael Saubolle, David L. Sewell, Daniel Shapiro,Susan E. Sharp, James W. Snyder, Allan Truant.Effective as of January 2000, the purpose of the Cumitech series is to provide consensus recommendations regarding the judicioususe of clinical microbiology and immunology laboratories and their role in patient care. Each Cumitech is written by a team of clinicians,laboratorians, and other interested stakeholders to provide a broad overview of various aspects of infectious disease testing. Theseaspects include a discussion of relevant clinical considerations; collection, transport, processing, and interpretive guidelines; the clini-cal utility of culture-based and non-culture-based methods and emerging technologies; and issues surrounding coding, medical neces-sity, frequency limits, and reimbursement. The recommendations in Cumitechs do not represent the official views or policies of anythird-party payer.Copyright © 2006 ASM PressAmerican Society for Microbiology1752 N Street NWWashington, DC 20036-2904All Rights Reserved10 9 8 7 6 5 4 3 2 1

Laboratory Diagnosis of Upper Respiratory
Tract Infections
Ken B. WaitesDepartment of Pathology, Clinical Microbiology Section, and Diagnostic
Mycoplasma Laboratory, Division of Laboratory Medicine WP 230, 619 19th St.South, University of Alabama at Birmingham, Birmingham, AL 35233
Michael A. SaubolleInfectious Disease Division, Laboratory Sciences of Arizona, Good Samaritan
Medical Center, 1111 E. McDowell Rd., Phoenix, AZ 85006
Deborah F. TalkingtonNational Center for Infectious Diseases, Division of Bacterial and Mycotic
Diseases, Mailstop G03, Centers for Disease Control and Prevention, Atlanta, GA30333
Stephen A. MoserDepartment of Pathology, Clinical Microbiology Section, Laboratory InformaticsSection, and Fungal Reference Laboratory, Division of Laboratory Medicine WP
230, 619 19th St. South, University of Alabama at Birmingham, Birmingham, AL35233
Vickie BaselskiDepartment of Pathology, University of Tennessee at Memphis,
899 Madison Ave., Memphis, TN 38163
COORDINATING EDITOR: Susan E. SharpDepartment of Microbiology, Kaiser Permanente,
13705 Airport Way, Portland, OR 97230
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Normal Upper Respiratory Tract Microbial Flora . . . . . . . . . . . . . . . . . . . . . . . 2
Clinical Aspects and Pathogenesis of Upper Respiratory Tract Infections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Pharyngitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Streptococcal Pharyngitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Nonstreptococcal Pharyngitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Laryngeal Syndromes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Acute Laryngitis and Laryngotracheobronchitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Epiglottitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Otitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Otitis Externa . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .17Otitis Media . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Sinusitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Other Infections Caused by Unusual and/or Uncommon Bacteria . . . . . . . 25Pertussis (Whooping Cough) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25Diphtheria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .28Pharyngeal and Peritonsillar Abscesses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .30Lemierre’s Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .30Vincent’s Angina . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .31
Candidiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32
Zygomycoses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32
Nasal Screening for MRSA Carriers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .34
1

INTRODUCTION
This Cumitech serves as a concise laboratoryresource for characterizing upper respiratorytract infections including pharyngitis, laryngi-
tis, rhinitis, epiglottitis, sinusitis, otitis media, and oti-tis externa. Detailed information regarding the mostcommon bacterial and fungal etiologies, laboratorytest selection, specimen collection, specimen process-ing, and reporting and interpretation of test results isincluded. Greatest emphasis is placed on detectionand identification of common bacterial infections ofadults and children by using methods suitable forhospital microbiology laboratories. However, lesscommon bacterial infections such as diphtheria, per-tussis, Lemierre’s disease, and Vincent’s angina andfungal infections including oropharyngeal candidia-sis and rhinocerebral zygomycosis are also discussed.Nucleic acid amplification tests (NAATs) such as PCRare discussed when their use can be important forlaboratory detection of fastidious microorganismssuch as Mycoplasma pneumoniae and Chlamydophi-la (Chlamydia) pneumoniae, even though commer-cial kits for these assays are not yet available. As anadditional aid to the clinical microbiologist, there isa complete listing of the reimbursement codes for allof the procedures that are described.
The respiratory tract is arbitrarily divided into theupper tract, which includes the anatomic areas fromthe anterior nasal passages to the larynx, includingthe nasopharynx, oropharynx, larynx, epiglottis,inner and middle ear, and paranasal sinuses, and thelower respiratory tract, which includes all structuresbeyond the larynx. It is sometimes difficult to sepa-rate upper respiratory tract infections and their etio-logic microorganisms from those that also involvethe lower respiratory tract, since in clinical practicepatients may have components of both conditionssimultaneously resulting from a single infection. Inview of the fact that a very comprehensive Cumitechon lower respiratory tract infections was recently pub-lished (106) and another Cumitech dealt with ocularinfections (127), we have attempted not to duplicateinformation covered in detail in those documents.Moreover, although we acknowledge that the greatmajority of respiratory tract infections are caused byviruses, this Cumitech is limited in scope to bacterialand fungal infections, and a revised Cumitech focus-ing on viral respiratory infections is forthcoming.
NORMAL UPPER RESPIRATORY TRACTMICROBIAL FLORA
The microbial flora of the upper respiratory tract isinfluenced by many variables, including the age andhealth of the host, the status of the innate and adap-tive immune systems, environment, hospitalization,and prior exposure to antimicrobial agents. In recentyears, with the expansion of routine immunizationsfor Haemophilus influenzae and Streptococcus pneu-moniae in young children, the vaccine status mayalso be an important factor affecting the microbialflora.
A dense and diverse bacterial flora including aero-bic and anaerobic organisms resides in the nasal andoral passages, with numbers of up to 1012 CFU/ml(106). The types of organisms in the oropharynx candiffer from individual to individual, but in otherwisehealthy persons, the microbial flora is dominated byaerobic, facultative anaerobic, and obligate anaerobicorganisms. These organisms include alpha-hemolyticstreptococci, staphylococci, micrococci, neisseriae,Moraxella catarrhalis, corynebacteria (other thanCorynebacterium diphtheriae), and Haemophilus spp.Anaerobic bacterial genera including Porphyromo-nas, Prevotella, Fusobacterium, Veillonella, Pepto-streptococcus, and Actinomyces may also be present.Pathogenic bacteria such as S. pneumoniae, Strepto-coccus pyogenes, and Neisseria meningitidis maysometimes be present in small numbers in the oro-pharynxes and nasopharynxes of healthy persons.Gram-negative bacilli may occasionally be present inhealthy persons, but they more often colonize personswho are currently or have recently been hospitalizedand/or given antimicrobial agents. The anterior naresare colonized predominantly by Corynebacterium spp.and staphylococci, sometimes including methicillin-resistant Staphylococcus aureus (MRSA). Yeasts suchas Candida spp. may also be present in small num-bers in the orpharynxes of healthy persons.
In contrast to the oropharynx, the sublaryngealregions of the respiratory tract, the paranasal sinuses,and the middle and inner ear are generally devoid ofmicroorganisms in healthy persons. The sublaryngealregion may be colonized by a variety of bacteria inpersons with chronic lung diseases or a history includ-ing endotracheal intubation. Viruses are not usuallyconsidered important components of the normalupper respiratory tract microbial flora, although some
2 Waites et al. CUMITECH 10A
Appendix: Coding and Reimbursement Issues . . . . . . . . . . . . . . . . . . . . . . .34
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .38

viruses may be cultured from asymptomatic personswith subclinical infections.
CLINICAL ASPECTS AND PATHOGENESIS OF UPPER RESPIRATORY TRACT INFECTIONS
Upper respiratory tract infections are among the mostcommon, yet least preventable, infections that occurin humans. They account for more visits to cliniciansthan any other type of infectious disease (26). Therespiratory tract is an especially common site forinfections because of its direct exposure to potentialpathogens that may be inhaled from the environ-ment. Despite the anatomical barriers such as nasalhairs to filter large particles, mucous secretions inthe nasopharynx to trap the smaller particles, themucociliary elevator, secretory immunoglobulins (Igs),the cough reflex, and phagocytic cells that assist inremoval and inactivation of infectious microorgan-isms, many microorganisms are still able to gainaccess to the tissues of the upper and lower respira-tory tract. Many of the millions of microorganisms,including the most common ones described above,that reside in the human upper respiratory tract haveadapted to a commensal relationship with the host,and their presence is believed to actually help preventacquisition and multiplication of exogenous patho-gens that must compete for the available space andnutrients necessary to survive. Clinical illness occurswhen a new pathogen is introduced that is able toovercome the host immune defenses, when the deli-cate balance between the existing microbial flora andthe human host is upset through trauma to the tissues,or when a change occurs in the health and/or immunestatus of the host. Some very successful pharyngealpathogens such as S. pyogenes produce severe localinflammatory disease but may also be carried asymp-tomatically for variable periods of time. On the otherhand, there are pathogens such as toxigenic C. diph-theriae whose presence in the upper respiratory tractrarely or never occurs in the absence of disease.
Upper respiratory tract infections may manifestclinically when the invading pathogens damage therespiratory epithelium as a result of their attachmentand elaboration of biochemical substances, such asperoxides in the case of M. pneumoniae (123), or theirproduction of a variety of exotoxins in the case ofsuch organisms as S. pyogenes, C. diphtheriae, andBordetella pertussis (89). Intracellular invasion asoccurs with organisms such as C. pneumoniae, S. pyo-genes, and perhaps M. pneumoniae may facilitate per-sistence of infection, difficulty in eradication by anti-microbial agents, and long-term carriage. Furtherdamage may be mediated by the host response tothe invasion of microorganisms through proliferation
and chemotaxis of leukocytes and elaboration of pro-inflammatory cytokines and other mediators of theacute and chronic inflammatory responses. Epithelialdestruction leads to erythema, edema, hemorrhage,and sometimes the presence of an exudate. Local andsystemic effects of inflammation in the form of fever,coughing, sneezing, pain in the affected areas, lym-phadenopathy, leukocytosis, and sometimes blood-stream invasion with systemic spread can occur,depending on the type of infection, anatomic site ofmicrobial invasion, host variables, and the specificmicrobes involved. Clinical involvement may take theform of acute or chronic disease. Additional specificclinical characteristics are described with individualinfections and their respective etiologic agents.
PHARYNGITIS
Pharyngitis is an inflammation and/or infection of thepharyngeal and/or tonsillar area. It can involve theoropharynx, nasopharynx, hypopharynx, adenoids,and tonsils. Tonsillitis refers to inflammation of thepharyngeal tonsils, and the term may be used inter-changeably with pharyngitis.
In most types of acute pharyngitis caused by bac-teria such as the beta-hemolytic streptococci, infec-tion is acquired from other persons by spread throughrespiratory aerosols or fomites. Alternatively, pharyn-geal infection with Neisseria gonorrhoeae and Trepo-nema pallidum can occur by direct mucosal contactduring orogenital sexual relations. Yersinia enteroco-litica is considered primarily a cause of bacterialenteritis, but milk-borne illness due to this organismin which pharyngitis is a prominent feature can occur(99). Oropharyngeal tularemia can be acquiredthrough contact with infected animals or arthropods.Some conditions such as Lemierre’s disease and peri-tonsillar abscesses can occur as a result of diseaseinduced by endogenous floras composed of a diversearray of aerobic, facultative, and anaerobic organisms.
The signs and symptoms of bacterial and viralpharyngitis are nonspecific and overlapping. How-ever, some manifestations such as conjunctivitis,coryza, cough, viral exanthem, ulcerative pharyngeallesions, and diarrhea are more commonly associatedwith viral than with bacterial infections (13). Thepharynx and tonsils are often very erythematous, andsmall petechiae may be seen on the soft palate. How-ever, the classic signs of fever, headache, sore throat,tonsillar swelling and/or the presence of an exudateand anterior cervical adenitis are not always present.The nonspecific nature of clinical signs and symp-toms accompanying pharyngitis mandates that clini-cians rely on laboratory findings and submit an ap-propriate specimen if a microbiological diagnosis is tobe obtained.
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 3

Pharyngitis causes more than 40 million medicaloffice visits by adults in the United States each year(16), making it one of the most common conditionsfor which ambulatory medical care is sought and forwhich antibiotics are prescribed. An even greaternumber of children than adults contract pharyngitis.Epidemiological and diagnostic aspects of pharyngi-tis are discussed individually in conjunction witheach of the predominant etiologic agents that differwith respect to frequencies of occurrence and labora-tory detection methods.
Etiology
Most pharyngeal infections are due to respiratoryviruses, with bacterial agents causing 5 to 40% of cas-es. Rhinoviruses, adenoviruses, respiratory syncytialvirus, parainfluenza viruses, and various herpesvirus-es are the principal viral causes of pharyngeal infec-tions (5). Not to be overlooked as a cause of pharyn-gitis is primary human immunodeficiency virus (HIV)infection. The initial presentation of HIV infectionmay be flu-like symptoms, including pharyngitis.Patient history, including an assessment of HIV riskfactors, may suggest the need for HIV testing. Thegroup A beta-hemolytic streptococcus (GAS) is themost common bacterial pathogen that causes phar-yngitis. Other beta-hemolytic streptococci in groupsC and G may also cause pharyngitis. S. pneumoniaeand Haemophilus spp. may sometimes be detectedin pharyngeal specimens, but these organisms areunlikely to be of etiologic significance in uncompli-cated pharyngitis. However, Haemophilus spp. suchas H. parahaemolyticus have been isolated fromthroat cultures from persons with pharyngitis in theabsence of other known bacterial pathogens andhave also been isolated from oral abscesses, suggest-ing a possible role for these organisms in some cir-cumstances (68). However, in view of the high fre-quency of Haemophilus spp. colonizing the upperrespiratory tracts of healthy persons, laboratoriesshould not normally report their presence in pharyn-geal cultures as it might cause confusion and misleada clinician into unnecessary therapy (5). H. influen-zae presents a special circumstance that is addressedfurther in the section on epiglottitis. Although manyhospitalized persons are colonized in the upper respi-ratory tracts with gram-negative bacilli, some ofwhich are of enteric origin, these organisms are notnormally considered to be clinically significant caus-es of pharyngitis and their presence is not normallyacknowledged in laboratory reports for throat cul-tures. A possible exception is for immunosuppressedhosts, in whom pharyngitis may be one of multipleconcurrent maladies. Other rare exceptions to thisgeneral guideline are Y. enterocolitica (99) and Fran-cisella tularensis in special circumstances. Laborato-
ry aspects for detection of these agents are discussedin Cumitech 12A and Cumitech 33, devoted to bac-terial diarrheal diseases and agents of bioterrorism,respectively (47a, 48). Mycobacterium tuberculosisrarely appears on lists of microorganisms that causepharyngitis. However, a neck mass, sore throat, orthroat discomfort, usually accompanied by cervicallymphadenopathy, is sometimes reported on initialpresentation (2). Mycobacterium bovis and Myco-bacterium avium-M. intracellulare also must be con-sidered in a differential diagnosis of pharyngitis inimmunocompromised patients, although they arerarely sought in throat cultures. It is beyond the scopeof this Cumitech to go into detail regarding methodsfor the detection and identification of mycobacterialdiseases. The reader is referred to Cumitech 16A formore information on laboratory detection of themycobacterioses (28). There are several other rare oruncommon infections in which pharyngitis may beinvolved that require consultation with the labora-tory in order to ensure that appropriate diagnostictests are performed. One such example is pharyngealulceration (chancre formation) and lymphadenopa-thy associated with T. pallidum infection in primarysyphilis following orogenital contact. If syphilis issuspected, material collected from the chancre can beexamined by direct fluorescent-antibody assay for T.pallidum and serologic tests should be performed.Bacterial agents known to cause pharyngitis aredescribed in more detail in subsequent sections. Someagents were chosen because of their frequent occur-rence, whereas others were included because of theirimportant epidemiologic aspects.
Streptococcal Pharyngitis
The primary cause of bacterial pharyngitis in theUnited States is S. pyogenes, also referred to as GAS,based on the Lancefield schematic classification forgrouping streptococci according to their carbohy-drate cell wall antigens. GAS pharyngitis is a com-mon infection in the throat and skin, causing an esti-mated 4 to 5 million cases in the United States eachyear (107). The incidence is greatest during the latefall, winter, and early spring months, and GAS is espe-cially prevalent among children between the ages of5 and 12 years, in whom it may account for about30% of all cases of pharyngitis. GAS causes only10% of pharyngitis cases in adults (23). In additionto oropharyngeal infections and other autoimmunesequelae such as rheumatic fever and acute glomeru-lonephritis, the more serious deep-tissue GAS infec-tions (such as necrotizing fasciitis) and streptococcaltoxic shock syndrome have resurfaced over the pastseveral years (33, 59). Much of this organism’s suc-cess as a human pathogen is owed to the M protein
4 Waites et al. CUMITECH 10A

surface antigen that allows GAS to avoid phagocyto-sis and survive in the human host (40). A compre-hensive review of the pathogenesis of streptococcaldisease provides details of the complex process ofadherence, cell invasion, and toxin production in thepathogenesis of S. pyogenes pharyngitis (33). Someindividuals who are carriers may harbor GAS in theirupper respiratory tracts without clinical symptoms.These individuals do not exhibit complications fromthe colonization, nor do they seroconvert when pairedsera are tested for streptococcal antibodies. Diagno-sis from clinical signs and symptoms is difficult, andmere isolation of the organism from a throat cultureis not diagnostic. Infection may move beyond thepharynx to encompass the tonsils, uvula, and fauces.The scarlet fever variety of GAS throat infection isassociated with a characteristic rash caused by theerythrogenic exotoxin.
In addition to GAS, organisms from the Lancefieldgroups C and G large-colony forms may cause phar-yngitis with clinical symptoms similar to those ofGAS pharyngitis. Streptococcus dysgalactiae subsp.equisimilis (previously designated “S. equisimilis”)may be grouped into Lancefield groups A, C, G, andL. Streptococcus equi subsp. zooepidemicus belongsto Lancefield group C. Group C streptococci may berelatively common causes of acute pharyngitis amongcollege students and adults (47), and pharyngitiscaused by both C and G groups has been associatedwith food-borne outbreaks (12). The small-colony-forming member of the beta-hemolytic Streptococcusanginosus group (Streptococcus constellatus subsp.pharyngis), belonging to Lancefield group C, mayalso be associated with throat infections according toone study (126), whereas others (116) have suggestedthat organisms in the S. anginosus group are normalinhabitants of the upper respiratory tract. Group Anon-S. pyogenes strains are not common but maycause confusion in the laboratory (40). Beta-hemo-lytic streptococci other than GAS are not associatedwith autoimmune sequelae such as rheumatic fever.There is no supportive evidence to suggest that strep-tococci in groups B and F are important causes ofpharyngitis (16).
It is obvious from the above discussion that theLancefield grouping system cannot be used alone foraccurate identification of individual beta-hemolyticstreptococcal species, but it can be a useful part ofthe overall identification procedure (40). Complicat-ing matters even further, non-beta-hemolytic variantsof S. pyogenes may occur (131). Streptococcus mitis,a viridans group alpha-hemolytic streptococcus thatis usually a commensal oral organism, can also causesevere pharyngitis often accompanied by toxic shock-like syndrome complications. One outbreak in Chinainvolved a single clone that produced a potent exo-
toxin and resulted in thousands of pharyngitis casesover an 8-year period (79).
Diagnosis
Historically, culture has been the cornerstone fordiagnosis of streptococcal pharyngitis. Gram stains ofpharyngeal swabs are not performed because of theubiquitous presence of commensal oral streptococci.Over the past several years, however, the importanceof rapid antigen detection tests (RADTs) in the initialdiagnosis has increased as the sensitivities and speci-ficities of the many assays have improved. Serology isnot useful for diagnosis of acute streptococcal phar-yngitis, but measurement of titers of antibodies tovarious GAS toxins such as streptolysin-O is valuablefor confirmation of prior infections in persons sus-pected of having acute rheumatic fever or acute glo-merulonephritis (13).
Specimen Collection,Transport, and
Processing for Culture
The collection, processing, and culture identifica-tion methods described are suitable for all strepto-cocci. Dacron polyester or calcium alginate swabsare acceptable for specimen collection. The tongue isdepressed, and the swab is rubbed vigorously overthe tonsillar area and posterior pharynx and otherinflamed areas. Take care to avoid touching thetongue and uvula. If processing will be delayedbeyond 2 h after collection, place the swab into a suit-able transport medium such as Amies gel and storefor �24 h at room temperature (112).
Fifty years ago, Breese and Disney first establishedthe culture of a throat swab on a sheep blood agar(SBA) plate as the diagnostic standard for GAS phar-yngitis, and it has remained so to the present time(18). Although a major disadvantage of culture is thetime required for incubation (24 to 48 h), it is oftenused in conjunction with the newer RADTs for con-firmation of infection.
Upon arrival in the laboratory, the swab is rolledover one-sixth of the surface of an SBA plate. A ster-ile loop is then used to streak for isolation in fourquadrants. The loop is stabbed into the agar severaltimes in an unstreaked area, and the remainingplate surface is streaked for isolation. The subsurfacegrowth in the stabbed areas provides a more reliableindication of true hemolysis due to the activity of bothoxygen-stable and oxygen-labile hemolysins. Beta-hemolysis appears as a complete lysis of the red bloodcells of the medium, especially in the areas of loweredoxygen tension. The basal medium must not containa high dextrose concentration, as that would inhibitthe production of hemolysins. SBA is preferred tomedia containing blood from other animals because itis less likely to support growth of beta-hemolyticHaemophilus spp., which can cause confusion with
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 5

beta-hemolytic streptococci. Inoculated plates areincubated at 35 to 37°C, examined after 18 to 24 h,and reincubated if negative, with a final reading at48 h. Kellogg (67) concluded that 90 to 95% of spec-imens from symptomatic patients containing GAScan be detected by incubating SBA anaerobically for48 h, incubating SBA aerobically without CO2 sup-plementation for 48 h, or incubating SBA containingtrimethoprim-sulfamethoxazole (SXT) anaerobicallyfor 48 h. Use of CO2 supplementation may enhancerecovery of non-GAS beta-hemolytic streptococci andother organisms such as Arcanobacterium spp. whichmay be of significance in pharyngitis, but it is notrecommended for routine throat cultures on SBA inwhich GAS is of primary interest since heavier growthof the normal flora may hinder detection (5, 23, 44).
Bacterial Identification and Reporting Results
The presence of any beta-hemolytic streptococcusgrown in a throat culture should be evaluated forpossible clinical significance. S. pyogenes and large-colony group C and G streptococci form colonies of�0.5 mm in diameter, in contrast to other strepto-cocci, and some may appear mucoid. Colonies maybe opaque or transparent with a matte or smoothsurface. They are surrounded by a wide area of beta-hemolysis which is more prominent in the areas oflowered oxygen tension. Beta-hemolytic colonies canbe identified as streptococci based on a positiveGram stain reaction, arrangement of the coccoid cellsin chains, and lack of catalase reaction with 3%hydrogen peroxide. The bacitracin susceptibility testis sometimes used for presumptive differentiation ofS. pyogenes from other beta-hemolytic streptococcibecause �95% of GAS are susceptible whereas acomparable percentage of other beta-hemolytic strep-tococci are resistant (13). A 0.04-U bacitracin disk isapplied to an SBA plate that has been inoculated witha pure culture of streptococci. After 18 to 24 h ofincubation at 37°C, any detectable zone of inhibitionaround the disk is interpreted to indicate susceptibil-ity. This test should be performed only on pure cul-tures and not on primary inoculation plates. How-ever, some strains of group B, C, and G streptococcialso test as bacitracin susceptible. Consequently, anadditional procedure using a disk containing 1.25 �gof trimethoprim and 23.75 �g of sulfamethoxazolecan be added in order to improve specificity. GroupsC and G are usually SXT susceptible, whereas groupsA and B are resistant. Detection of any inhibitoryzone around the disk can be interpreted to indicatesusceptibility. Alternatively, inhibitory SBA supple-mented with SXT can be used as the primary inocu-lation medium, since growth of GAS will be enhancedas other organisms from the normal flora may beinhibited. Use of this selective SXT-containing medi-
um can retard growth in primary culture of strepto-cocci of groups C and G, so it should not be used ifthese organisms are being sought. The pyrrolidony-larylamidase (PYR) test is used for detection of PYRor pyrrolidonyl aminopeptidase. This test can be per-formed rapidly on pure cultures by using com-mercially available reagents and reacting bacterialcolonies with the substrate incorporated into a paperdisk to which a color developer is then added. Devel-opment of a pink area on the disk after a few minutesof incubation at room temperature constitutes a pos-itive test. S. pyogenes is PYR positive, as are entero-cocci, Streptococcus porcinus, and Streptococcusiniae. Other beta-hemolytic streptococci are PYRnegative, including some strains of group A that arenot S. pyogenes. A number of companies market latexparticles coated with antibody directed against group-specific carbohydrate antigens. These reagents can beused to rapidly distinguish the major group A, B, C,F, and G beta-hemolytic streptococci causing infec-tions in humans without overnight incubation orother means for determination of biochemical reac-tions. From a practical standpoint, clinical laborato-ries may limit reporting of pharyngeal isolates ofbeta-hemolytic streptococci to the Lancefield groupsbased on reactions with group-specific-antibody-coated latex particles and not attempt to classifythem further into individual species. However, it isadvisable to verify any small-colony beta-hemolyticstreptococcus that belongs to group A as S. pyogenesby using the PYR test. PYR-negative strains are con-sidered part of the normal flora. Similarly, one canperform the Voges-Proskauer (VP) test on group C orG isolates to help differentiate commensal organismsin the small-colony S. anginosus group that are VPpositive from potential pharyngeal pathogens such asS. dysgalactiae subsp. equisimilis and S. equi subsp.zooepidemicus that are VP negative (40). Until moreevidence accumulates to support a significant role forS. constellatus subsp. pharyngis in pharyngitis, differ-entiating it from other members of the S. anginosusgroup on a biochemical basis is not warranted forroutine throat cultures, although distinguishing char-acteristics have been enumerated by Facklam (40).Despite the known association of beta-hemolyticstreptococci in groups C and G with pharyngitis,some laboratories may choose to identify and reportonly the presence of GAS in throat cultures. Anyother beta-hemolytic streptococci are designated as“beta-hemolytic streptococcus—not group A.” Thisapproach is economical since it eliminates the need tocharacterize non-GAS isolates by using latex-basedreagents or other methods. Decisions regardingwhether or not to identify non-GAS isolates in throatcultures should be made in consultation with clini-cians who utilize the laboratory’s services.
6 Waites et al. CUMITECH 10A

Reporting the presence or the absence of patho-genic beta-hemolytic streptococci without descriptionof other organisms which may be commensals pro-vides the clearest message for directing patient man-agement. However, a positive culture for beta-hemolytic streptococci does not distinguish betweenacute infection and colonization. It is also helpful tocharacterize the numbers of pathogenic streptococcias few (growth limited primarily to the first quad-rant), moderate (growth primarily in the first andsecond quadrants), or abundant (growth in the thirdand fourth quadrants) on the agar plate used for pri-mary inoculation in the event that further differen-tiation beyond Lancefield grouping is desired. Table 1describes the major beta-hemolytic streptococcalspecies isolated from humans based on the organisms’biochemical reactions.
The alpha-hemolytic viridans group streptococciare rarely sought individually in pharyngeal culturesbecause of their infrequency of association with dis-ease and their ubiquity in the oral commensal flora.The taxonomy of these organisms has been under-going revision which has made the identification ofthe organisms to the species level both complex anddifficult. Although a number of commercially avail-able biochemical systems, including automatedmicrobiology instruments, can be employed to identi-fy these streptococci to the species level, the perform-ance of these systems in general has been less thanideal and there is no compelling reason to attempt toisolate, identify, or classify these organisms in pha-ryngeal cultures under normal circumstances. Refer-ences 100 and 40 provide tabular information useful
to assist in differentiation of these organisms; how-ever, nomenclature is subject to change.
AST
Development of antimicrobial resistance in GAS isnot widespread. Penicillin remains the treatment ofchoice, and there is no resistance to this agent or other comparable �-lactams. Macrolides and clin-damycin can be used for penicillin-allergic or intoler-ant patients. A recent large-scale in vitro surveillancestudy detected erythromycin resistance in only 4.5%and clindamycin resistance in �1% of clinical iso-lates acquired over a broad geographic area in theUnited States (118), but higher rates are known tooccur in other countries (100). Tetracycline resistancemay also occur. Antimicrobial susceptibility testing(AST) of pharyngeal isolates of beta-hemolytic strep-tococci is not indicated except by special request inthe event that drugs other than penicillin are needed.Penicillin and erythromycin resistance is now rathercommon among the viridians group streptococci,however (40, 100).
Rapid Diagnosis of Streptococcal Pharyngitis
Commercial point-of-care RADTs for GAS weredeveloped primarily because of the 24- to 48-h turn-around time required for bacterial culture and theneed to initiate antimicrobial treatment in a timelymanner. RADTs use acid extraction to solubilize thecell wall carbohydrate, followed by an immunologicreaction. A latex agglutination test was the first typeof rapid test to be developed, but this format has beenreplaced by a variety of enzyme immunoassays (EIAs)and optical immunoassays (OIAs) that have the ad-
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 7
Table 1. Laboratory identification of beta-hemolytic streptococci known to occur in humansa
Lancefield Result for:Species
group(s) Bac SXT PYR CAM VP Hip Str Sbl Tre Rib
S. pyogenes A Sus Res � � � � � � NA �
S. agalactiae B Res Res � � � � � � NA NAS. dysgalactiae A, C, G, L Res V � � � � � � � �
subsp. equisimilisb
S. equi subsp. C Res Sus � � � � � � V NAzooepidemicus
S. canisb G Res Sus � � � � � � V NAS. anginosus (group)c A, C, G, F, Res V � � � � � � � NA
noneS. constellatus C Res Sus � � � � � � � NA
subsp. pharyngis
aAbbreviations: Bac, bacitracin; CAM, CAMP reaction; Hip, hippurate; Str, hydrolysis of starch; Sbl, Tre, and Rib, production of acid in sorbitol, trehalose,and ribose broth; Sus, susceptible; Res, resistant; V, variable reaction; NA, not available; �, positive; �, negative. This table has been derived from infor-mation provided in references 40 and 100. Only data for streptococcal species that have been isolated from humans are included.
bTo differentiate between group G S. canis and group G S. dysgalactiae subsp. equisimilis, S. canis is positive for �- and �-galactosidase and negative forbeta-glucoronidase; S. dysgalactiae subsp. equisimilis gives the opposite reaction. S. canis strains tested were of animal origin, and it is not known ifhuman strains will have the same phenotype.
cThe S. anginosis group includes beta-hemolytic strains of S. anginosis, S. constellatus, and S. intermedius. They are also referred to as the S. milleri group.There are insufficient data to know the percentage of each of these species that contain carbohydrate antigens.

vantages of clearer end points and improved sensitiv-ities (47).
The majority of RADTs currently available in theUnited States have high specificities (�95%) andmoderate sensitivities (70 to 96%) compared to cul-ture (16). A negative RADT in a patient with culture-confirmed GAS pharyngitis may occur due to aninoculum with a low number of organisms. Rarefalse-positive RADTs may possibly be due to thepresence of nonhemolytic commensal S. anginosusexpressing the group A antigen or a nonhemolyticvariant of GAS (47). RADTs cannot detect strepto-cocci in groups C and G, which may cause illnessindistinguishable from that caused by GAS. Howev-er, since the autoimmune sequelae of GAS infectiondo not occur to any extent with streptococci fromthese other groups and controlled clinical trials havenot shown convincing evidence of a clinical responseto antibiotics, missing the occasional pharyngitis caseby the use of RADTs may not be clinically important(47).
The American Academy of Pediatrics (AAP) rec-ommends that laboratory testing be performed in allcases of pharyngitis in children due to the nonspecif-ic nature of the illness and the likelihood that GASmay be involved. A negative RADT for GAS shouldbe followed by culture (47). Despite this recommen-dation, a large study in a pediatric clinical practicefound that only 2.4% of negative RADTs corre-sponded to a positive confirmatory culture and theauthors concluded that confirming negative RADTsby culture is costly and may not be medically neces-sary for most patients (83). The 2002 Infectious Dis-ease Society of America (IDSA) clinical practice guide-lines (13) also recommend that laboratory testingshould be performed unless a clinician is able toexclude GAS pharyngitis on clinical and epidemio-logical grounds. Clinicians can choose whether to useRADTs or culture in the initial evaluation. For chil-dren and adolescents, the IDSA recommends that anegative RADT result be confirmed by culture, unlessthe clinician has ascertained directly that the RADTbeing used is of sensitivity comparable to that of cul-ture. These practice guidelines provide a differentrecommendation for adult pharyngitis because of alower incidence of GAS disease and a lower risk fordevelopment of rheumatic fever in adults. A negativeRADT in adults does not require confirmation byculture, and antibiotic therapy is not necessary. Posi-tive RADTs need not be confirmed by culture. TheCenters for Disease Control and Prevention (CDC),the American College of Physicians, the AmericanSociety of Internal Medicine, and the American Acad-emy of Family Physicians published clinical practiceguidelines for acute pharyngitis in adults in 2001(32). This document goes a step further than the AAP
and IDSA guidelines in stating that adults meetingone or none of the following specific clinical criteriaincluding history of fever, presence of tonsillar exu-dates, absence of cough, and presence of tender ante-rior cervical adenopathy need not be tested or treatedwith antimicrobials. For patients meeting two ormore criteria, recommended strategies include (i) test-ing patients meeting two to four criteria by RADTsand limiting antibiotic therapy to patients with posi-tive test results or patients meeting four criteria and(ii) not performing any diagnostic tests and limitingantibiotic therapy to patients meeting three to fourcriteria.
As with any type of microbiological tests, cost andreimbursement play an important role when clini-cians and laboratory directors select diagnostic tests.RADTs are more expensive than culture, but theyprovide more rapid results, allowing initiation of spe-cific treatment and potentially shortening the dura-tion of illness, and they may reduce the risk of thespread of infection within the community. The num-ber of new RADTs has increased in recent years.Many, but not all of them, are in the waived categoryin the Clinical Laboratory Improvement Amendment(CLIA) classification, meaning that physician officelaboratories do not have to meet the more rigorouscertification requirements of laboratories performingmoderate- and high-complexity testing. The CLIAInternet website (http://www.cms.hhs.gov/clia) con-tains up-to-date information concerning laboratorytests meeting the waived criteria that are most suit-able for point-of-care tests in physicians’ offices.
In addition to the RADTs in current use that arebased on EIA and OIA formats, a chemiluminescentsingle-stranded DNA probe is now sold commercial-ly (Gen-Probe, Inc., San Diego, Calif.). This GASDi-rect test detects GAS rRNA directly from throatswabs with a sensitivity of 86 to 94.8% and a speci-ficity of 95 to 100% compared to culture on SBA (47).Another molecular biology-based assay, the Light-Cycler Strep-A assay (Roche Applied Science, Indi-anapolis, Ind.), is a one-rapid-cycle PCR to detectspecific S. pyogenes DNA. This assay has a sensitivi-ty of 93% and a specificity of 98% compared to SBAculture (47). Both assays are most suitable for batchtesting of specimens in laboratories experienced inmolecular biology-based testing. The cost of theseadvanced molecular biology-based assays and theirinstrumentation is considerable. Due to their com-plexity and the 1.5- to 2-h time period required tocomplete the assays, they cannot be adapted forpoint-of-care testing. Some laboratories utilize theGASDirect test for confirmation of negative RADTsin lieu of culture (16). It is likely that the LightCyclerStrep-A assay is also a suitable confirmatory test fora negative RADT.
8 Waites et al. CUMITECH 10A

Gerber and Shulman (47) reviewed the OIAs, EIAs,and nucleic acid RADTs for GAS. They underscoredthe need for studies based on standardized compar-isons of RADTs with one another, including waivedand nonwaived tests, and suggested that cliniciansperform their own evaluations to determine whichRADT works best in their clinical setting.
Nonstreptococcal Pharyngitis
The beta-hemolytic streptococci are the most impor-tant bacteria sought in throat cultures from patientswith acute pharyngitis. However, some laboratoriesprefer to offer a variety of different categories forthroat cultures to allow clinicians to choose the mostappropriate and cost-effective test based on thepatient presentation and history. For example, a testordered as “strep culture” would use techniques andprovide results only for detecting the presence orabsence of beta-hemolytic streptococci, whereas a“GC culture” would provide results only for N. gon-orrhoeae. A broader category of “miscellaneousthroat culture” could include specific examinationfor other organisms that may cause throat infections,such as N. meningitidis and Arcanobacterium spp.,etc., and could be used when patient presentation andepidemiological data do not point directly towards aspecific pathogen. Laboratory methods for detectingsome of these other bacterial pathogens and circum-stances in which they should be considered aredescribed below.
Arcanobacterium haemolyticum and Arcanobacterium pyogenes
Arcanobacterium haemolyticum and Arcanobacteri-um pyogenes (previously classified as “Corynebac-terium haemolyticum” and “Actinomyces pyogenes,”respectively) are rare causes of pharyngitis, and theyhave also been implicated in a wide variety of cuta-neous and invasive infections including sinusitis, cel-lulitis, and septicemia (76). A. haemolyticum has beenisolated from the pharynx in �0.4% of adult patientsin the United States and Canada, 2% in Sweden, and0.2% in Israel (24, 30, 80, 87). Pharyngitis due tothese bacteria is often associated with a rash similarto that observed with scarlet fever (13). Under-standing the true importance of the arcanobacteria inpharyngitis is complicated since they can be isolatedfrom some individuals without disease and are oftenisolated in association with other potential patho-gens (16).
The detection of arcanobacteria does not requireany special specimen collection procedures or platingmedia beyond what have been described above forstreptococci. These bacteria should be suspected whenstreptococcal antigen tests are negative and gram-
positive, beta-hemolytic coccobacilli grow slowly onSBA after 48 h of incubation in an atmosphere sup-plemented with 5% CO2. Both species are catalasenegative and nonmotile. A. haemolyticum forms twomorphotypes, but it is the rough type that is typical-ly isolated from the respiratory tract. This speciesmay be distinguished by a CAMP inhibition reactionwhen incubated with a beta-hemolysin-producingstrain of S. aureus (44). A. pyogenes forms larger beta-hemolytic colonies (1 mm in diameter) on SBA after48 h of incubation and is the only species that pro-duces acid from xylose. The API RAPID Coryne Sys-tem Database 2.0 (bioMérieux) can identify bothspecies according to one study, although the numberof strains evaluated was small (45). A summary ofthe medically relevant corynebacteria and other cory-neform bacteria, including the arcanobacteria, andtheir biochemical reactions may be found in refer-ence 44. Laboratories should report the presence ofArcanobacterium spp. in throat cultures if the organ-isms are present in large numbers, i.e., moderate toabundant, on SBA. AST is not standardized forarcanobacteria and other coryneforms, but MICs of�-lactams, macrolides, tetracyclines, and rifampinare very low for these bacteria, suggesting the utilityof these drugs for therapeutic purposes. Treatmentfailure with �-lactams and response to macrolidesmay be due to intracellular localization of the bacte-ria since �-lactams, in contrast to macrolides, pene-trate host cells poorly, rendering them unable to killthe organisms (94).
N. gonorrhoeae and N. meningitidisThe most common clinical syndrome caused by N.gonorrhoeae is acute urethritis with dysuria and aurethral discharge, but the organism may also causepharyngitis and/or tonsillitis. Although this is uncom-mon, over 500 cases of gonococcal pharyngitis havebeen described since 1961. Such cases are typicallyfound in sexually active homosexual and bisexualmen and heterosexual women who acquire the infec-tion by engaging in orogenital sexual relations (4). Astudy in Seattle showed that 84% of individuals whohad pharyngeal N. gonorrhoeae were asymptomaticand that 64% of these infections occurred in individ-uals without genital gonorrhea (70). Most asympto-matic infections have been diagnosed by throat cul-ture using appropriate media and growth conditionsfor detection of neisseriae, but newer molecular assayssuch as the ligase chain reaction (LCR) and othertechnologies have improved detection in pharyngealspecimens. In a sexually transmitted disease clinic inSan Francisco, 4.5% of throat swabs were positivefor N. gonorrhoeae by culture and 11% were posi-tive by LCR (95). Regardless, N. gonorrhoeae mustbe included in a differential diagnosis of pharyrngitis
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 9

in sexually active adults, in high-risk groups, andamong those presenting with urogenital gonorrhea.
N. meningitidis can be isolated from the naso-pharynxes of 10% of individuals overall and fromthose of about 20 to 30% of teenagers and youngadults. It is believed that invasive disease follows ini-tial colonization of the upper respiratory tract, butthese bacteria can be cultured from throat swabs inonly 50% of cases (27). Carriage can be transient,intermittent, or chronic. Despite the complexity ofconfirming N. meningitidis pharyngitis, given thenumber of healthy carriers, case reports indicate thatthis organism can be an etiologic agent of simplepharyngitis (82), although its frequency is not known.
Diagnosis
Appropriate laboratory methods must be includedif N. gonorrhoeae is to be detected in clinical speci-mens. Gram stains are not appropriate for diagnosisof pharyngeal infection with N. gonorrhoeae becauseof the presence of saprophytic neisseriae in a normalpharyngeal flora. Diagnosis of pharyngeal infectionswith neisseriae rests on detection by culture. Tech-niques described are also suitable for cultures screen-ing for carriage of N. meningitidis.
Specimen Collection,Transport, and
Processing for Culture
Dacron or rayon swabs are used to obtain oro-pharyngeal specimens for culture of Neisseria spp. ina manner similar to that described above for detectionof streptococci. If possible, plate specimens at the timeof collection. Otherwise, place the swab into trans-port medium and keep it at room temperature. TheCopan swab system (Copan Diagnostics, Corona,Calif.) containing Amies gel without charcoal hasbeen shown to maintain satisfactory viability of N.gonorrhoeae in urogenital specimens for several hours(93). Complete transport systems that include a sealedpouch and catalyst to generate an appropriate incu-bation atmosphere are available commercially frommultiple manufacturers. Plates should be warmed toroom temperature, swabbed in a “Z” pattern, andthen cross-streaked with an inoculating loop. Thereare a variety of commercially available enriched selec-tive media that support the growth of neisseriae,including Thayer-Martin medium, Martin-Lewismedium, GC-Lect medium, and New York City medi-um. These media contain antimicrobial agents suchas vancomycin, colistin, nystatin, and trimethoprimto inhibit normal flora. However, other organismsthat are part of the normal flora of the oropharynxdo grow on these selective media and must be differ-entiated from N. gonorrhoeae. A nonselective medi-um such as chocolate agar should also be inoculatedbecause some strains of N. gonorrhoeae may be inhib-
ited by antibiotics contained in selective agars. Inoc-ulated plates are incubated at 35 to 37°C in air sup-plemented with 5% CO2 under humid conditions.Avoid CO2 concentrations higher than 7% becausegrowth may be inhibited. Inspect plates at 24, 48, and72 h for growth.
Bacterial Identification and Reporting Results
N. gonorrhoeae colonies are 0.5 to 1 mm in diam-eter and appear beige to gray-brown, smooth, andtranslucent. Subculture oxidase- and catalase-positivecolonies consisting of gram-negative diplococci ontochocolate agar for further testing as necessary forspecies confirmation. N. gonorrhoeae can be distin-guished from other neisseriae by production of acidwhen inoculated into cysteine trypticase agar basewith 1% glucose, but not maltose, fructose, lactose,or sucrose. There are several commercial biochemicaland chromogenic enzyme substrate kits, productscontaining a combination of biochemicals and chro-mogenic substrates, and immunologic methods thatare useful for identifying N. gonorrhoeae isolates.These are described in more detail in reference texts(e.g., reference 62).
In view of the important social and medicolegalconsequences regarding diagnosis of any sexuallytransmitted disease, laboratories must be aware of thepotential for erroneous results with respect to Neis-seria sp. confirmation using biochemical tests. Forexample, the occasional maltose-negative N. menin-gitidis isolate may be misidentified as N. gonorrhoeae.Confirmation of species identification by two inde-pendent methods may sometimes be necessary, espe-cially for nonurogenital sites in which the presence ofN. gonorrhoeae is uncommon and because confusionwith nonpathogenic Neisseria species may sometimesoccur.
N. meningitidis may be isolated from nasopharyn-geal or oropharyngeal swabs by using the same col-lection and culture procedures described above forN. gonorrhoeae, except that N. meningitidis oftengrows on unsupplemented SBA. Colonies on choco-late agar are larger than those of N. gonorrhoeae,reaching �1 mm in diameter, and are smooth andtranslucent. Confirmation of species identity can beachieved by acid production or chromogenic enzymesubstrate tests as described for N. gonorrhoeae. N.meningitidis produces acid from glucose and maltosebut not from lactose, sucrose, and fructose.
The presence of N. gonorrhoeae isolates in anynumbers in a pharyngeal culture should be reported.However, whether or not N. meningitidis should bereported routinely is controversial, since naming it ina report for a throat culture implies that the organ-ism is pathogenic and requires treatment when, infact, much of the time it is part of the commensal flo-
10 Waites et al. CUMITECH 10A

ra (62). The presence of N. meningitidis in a throatculture should be reported only if the organism isthere in abundance or if the clinician ordering the testspecifically requests such documentation for epi-demiological purposes.
In the reference laboratory, N. meningitidis isolatescan be serogrouped for epidemiological purposes byslide agglutination using commercially available anti-sera. They may also be serotyped based on their outermembrane proteins.
AST
AST of neisseriae is currently not recommended orneeded in hospital laboratories, even though methodsand interpretive criteria for N. gonorrhoeae and morerecently N. meningitidis have been developed by theClinical and Laboratory Standards Institute (CLSI)(62). Treatment of N. gonorrhoeae infection is givenempirically and is usually limited to specific extended-spectrum cephalosporins and fluoroquinolones. Peni-cillin and cephalosporins remain the treatments ofchoice for meningococcal infections. Changes in anti-microbial resistance in N. gonorrhoeae are moni-tored at specified locations in the United States by theCDC, and data acquired are used as a basis for revi-sions in treatment recommendations (62). Antimicro-bial resistance in N. meningitidis has not occurred tothe extent that it has in N. gonorrhoeae, but dimin-ished susceptibilities to penicillin and several otheragents have been described (62). In the event of a clin-ically significant case of documented pharyngeal in-fection with Neisseria spp. that does not respond totreatment, an isolate may be sent to a public healthor reference laboratory for susceptibility testing inaccordance with current guidelines (62).
Molecular Biology-Based Tests
Several new DNA hybridization-amplificationassays in a variety of formats are gaining popularityfor detection of N. gonorrhoeae directly in urogeni-tal specimens since they do not require viable organ-isms, can be performed on voided urine, and can alsodetect Chlamydia trachomatis. Findings of the studycited above using LCR for detection of pharyngealgonorrhea (95) are encouraging regarding the poten-tial use of these types of assays for diagnosis andscreening. However, non-culture-based moleculartests are not yet approved by the U.S. Food and DrugAdministration for testing pharyngeal or rectal spec-imens and cannot be recommended for this purpose(62). Moreover, the LCR system is no longer soldcommercially for urogenital specimens. The chemilu-minescent DNA probe Accuprobe Neisseria gonor-rhoeae Culture Confirmation Test (Gen-Probe, Inc.)can be used for species confirmation when bacterialisolates are available.
M. pneumoniae
M. pneumoniae is well known as a pathogen causingtracheobronchitis and pneumonia. Its role in humandisease has been recently reviewed (123). Studies fromItaly demonstrated that M. pneumoniae accounts forthe majority of single-isolate pediatric pharyngitiscases compared with other viral and bacterial etiolo-gies as determined using PCR and serology for itsdetection (38, 39). M. pneumoniae was associatedstatistically with a history of recurrent pharyngitis,an increased duration of fever, and increased proba-bility of future recurrent pharyngitis. This associa-tion with recurrent infections is consistent with theorganism’s ability to cause chronic respiratory carrierstates (111). A significant proportion of pharyngitiscases associated with M. pneumoniae infections hada negative course in the studies cited above, withlonger duration of fever and recurrence of symptomswithin a short time since no treatment effectiveagainst this organism was rendered. Sore throatassociated with M. pneumoniae infection may bepart of the overall infection process that also involvesthe lower respiratory tract. Since no clinical sign orsymptom or laboratory test reliably differentiatesbetween mycoplasmal and nonmycoplasmal pharyn-gitis, diagnosis with serology, PCR, and/or culture isrequired if the etiology is to be known. Macrolidesare effective against M. pneumoniae but may notalways be effective against GAS and are rarely usedin uncomplicated pharyngitis when GAS is suspect-ed. Thus, empiric treatment of acute pharyngitis ismore complex if M. pneumoniae is considered signif-icant. No studies comparable to those from Europehave been published from North America using ap-propriate diagnostic methods to quantitate the fre-quency of pharyngitis due to M. pneumoniae in adultsor children, and no controlled studies have been per-formed to determine precisely the benefit of antimi-crobial therapy. M. pneumoniae may colonize therespiratory tract along with other pathogens, andmycoplasmal infection may intensify subsequentinfections with viral and other bacterial agents (123).In light of the studies cited above, M. pneumoniaeshould be considered as a possible etiologic agent ofpharyngitis when tests for beta-hemolytic streptococ-ci are negative and perhaps even when streptococciare present because of the possibility of coinfection.
Diagnosis
Cumitech 34 (122) is devoted to a discussion oflaboratory diagnosis of mycoplasmal infections.Detailed descriptions of laboratory procedures, medi-um formulations, serologic tests, and molecularbiology-based tests are provided there. The ClinicalMicrobiology Procedures Handbook, second edition(119), has step-by-step procedures for detection of
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 11

M. pneumoniae by culture. In view of the availabilityof this information from these other sources, treamentof diagnostic aspects in this publication is limited tobrief summaries.
M. pneumoniae detection by culture is not practi-cal for most laboratories or for patient management,although it is performed in some large clinical labo-ratories and reference laboratories. The media areexpensive and nutritionally complex, the culture pro-cess is labor-intensive, and the time from inoculationof clinical specimens to isolation can be several weeks.M. pneumoniae should be identified to the specieslevel, as other commensal mycoplasmas present inthe upper respiratory tract can cause diagnostic con-fusion. If culture is attempted, scrupulous attention toproper methodology and specimen handling is essen-tial for success.
Specimen Collection,Transport, and
Processing for Culture
Appropriate specimens for diagnosis of M. pneu-moniae pharyngitis are oropharyngeal or nasophar-yngeal swabs. Take care to collect material from thenasopharyngeal area and not merely the anteriornares. Either Dacron or calcium alginate swabs aresuitable. Avoid wooden-shaft cotton swabs that canbe inhibitory. The swab is then placed into a trans-port medium such as 2SP or into a culture mediumsuch as SP4 broth with antibiotics (122). Swabsshould be swirled and pressed against the side of thetube before they are removed prior to submission tothe laboratory. If there is lower respiratory tractinvolvement and the patient is able to produce spu-tum, it can also be inoculated into transport mediumand submitted to the laboratory. Refrigerate speci-mens in transport media if they cannot be inoculatedonto culture media immediately. If the specimen mustbe held more than 24 h, freeze it at �70°C. If sub-mission to a reference laboratory is required, speci-mens must be shipped on dry ice.
SP4 agar and broth (122) are the best media for cul-tivation of M. pneumoniae. The complete formula-tion and instructions for their preparation are pro-vided in Cumitech 34 (122), and both are soldcommercially in the United States by Remel Labora-tories. Upon receipt in the laboratory, a specimen intransport medium is centrifuged at 8,000 to 10,000� g for 20 min and then the bottom 200 �l of trans-port medium containing the clinical specimen is trans-ferred to 1.8 ml of culture medium. From this initialtube, serial 10-fold dilutions of specimens are madeto 10�5 and then a portion of each dilution is sub-cultured onto agar. The centrifugation step can beomitted if specimens are collected directly into culturemedium such as SP4 broth. Broths are incubated at37°C under atmospheric conditions. Agar plates
must be kept moist and incubated at 37°C in 5 to10% CO2.
Bacterial Identification and Reporting Results
M. pneumoniae and many other bacteria changethe phenol red indicator in the broth medium fromred to yellow due to the hydrolysis of glucose. How-ever, M. pneumoniae does not produce any turbidity.Subculture any clear broth culture showing a colorchange to fresh broth and to agar. After 7 to 10 daysof incubation, all original dilutions not showing acolor change should be passaged into fresh SP4 brothand reincubated. Protocols at the CDC specify hold-ing cultures for up to 12 weeks before designatingthem as negative, although most positive specimensare detected by 2 to 6 weeks. Agar plates are exam-ined with a stereomicroscope at regular intervals forspherical colonies of up to 100 �m in diameter. Thesensitivity of culture may be no more than 60%,compared to PCR (123), but culture is 100% specif-ic if performed correctly. Tests to identify mycoplas-mas to species level include hemadsorption of guineapig erthrocytes, reduction of tetrazolium, agar growthinhibition with appropriate antisera, immunofluores-cent assays or immunoperoxidase staining, mono-clonal antibody tests, and PCR assays (122, 123).Detection of M. pneumoniae by culture in any clini-cal specimen should always be reported since M.pneumoniae is not considered a commensal organ-ism, even though it may be carried in the upper res-piratory tract for long periods in some asymptomaticpersons.
AST
AST of M. pneumoniae is not usually performedbecause clinically significant resistance to macrolides,tetracyclines, and fluoroquinolones has not beenverified on any large scale, even though macrolide-resistant strains have been known to occur (123).Methods for MIC determinations that provide repro-ducible results have been described but have not beenreviewed or endorsed by the CLSI (119, 122). Treat-ment trials evaluating the clinical response of M.pneumoniae infections of the lower respiratory tractto treatment with macrolide antibiotics and drugs inother classes such as fluoroquinolones have shownbeneficial effects (123). If pharyngitis occurs in asso-ciation with M. pneumoniae infection, it may be partof an illness involving the lower tract as well. There-fore, specific treatment may be helpful in speedingrecovery overall.
Molecular Biology-Based Tests
Development of testing modalities such as the PCRassay has lessened the importance of culture as ameans for detecting M. pneumoniae. Studies using
12 Waites et al. CUMITECH 10A

simulated clinical specimens, animal models, and clin-ical trials have validated the ability of PCR to detectM. pneumoniae, often in conjunction with serologyand/or culture (123). The same types of clinical spec-imens that can undergo culture can also be tested byPCR. The use of two different targets can maximizethe ability to detect the organism. The conventionalPCR procedure used at the CDC uses primers derivedfrom the M. pneumoniae ATPase gene (9). The CDChas also developed a real-time PCR using a uniqueinternal control, which targets a different portion ofthis gene. Other sequences, primarily those of the P1adhesin gene and conserved regions of 16S rRNA,have also been utilized as targets (123). For addi-tional information on various NAATs for detectionof M. pneumoniae, the reader is referred to recentpublications on this topic (35, 78, 88).
Comparison of PCR with culture and/or serologyhas yielded varied results, and large-scale experiencewith this procedure is still limited for M. pneumo-niae. To date, there has not been formal standard-ization of the approach for validation of the pub-lished PCR methods as there has been for C.pneumoniae PCR methods (36). Reznikov et al. (96)showed that PCR inhibition was much more likely tooccur with nasopharyngeal aspirates than with throatswabs. Dilution of samples may sometimes overcomeinhibition of PCR, but this may also diminish thesensitivity because the nucleic acid is diluted alongwith any inhibitors that may be present. There arealso commercial reagents for nucleic acid purificationthat are effective in removing most inhibitors ofamplification in PCR assays. Until PCR assays can bestandardized, made available at a reasonable cost,and sold commercially as complete diagnostic kits,this method of diagnosis is unlikely to gain wide-spread use for detection of M. pneumoniae infectionfor clinical as opposed to epidemiological purposes.
Specimen collection and transport for PCR analysisare identical to those described above for culture. Forculture and PCR from the same specimen, it is sug-gested that 400 �l be left, allowing 200 �l for cultureand 200 �l for DNA extraction. There are numerousDNA extraction kits sold commercially, and mostinclude the necessary enzymes and spin columns tocollect the extracted material. The extracts are refrig-erated or frozen at �70°C if they are to be held morethan 7 days prior to processing. Freezing and thawingof these specimens is strongly discouraged. Watershould be extracted as a control from each kit, as ithas been shown that some lots of commercial kits arecontaminated with bacterial DNA and in-house wateris often a source of contamination.
Any of the published PCR methods cited abovemay be used for analysis. Because inhibition is a majorfactor in creating false-negative results from PCR
assays, it is recommended that additional dilutions(1:5, 1:10, or 1:25) be run in the assay along with theundiluted sample. This step may dilute inhibitorsenough to allow detection of the target DNA. A pos-itive result in the undiluted and/or any of the dilutedsamples is valid. Proper controls should be run witheach assay, including a low-copy-number positivecontrol (�5 gene copies per sample), depending onthe sensitivity of the assay. The real-time assays aremuch more sensitive than the conventional assays,and the inclusion of a specific probe increases speci-ficity. Overall, PCR analyses have decreased the timerequired to diagnose infections, but it is suggestedthat serology or culture be used as an adjunct. Inview of the enhanced analytical sensitivity of PCRover that of culture, a positive PCR result and a neg-ative culture result can be easily explained. However,in a case with a negative PCR assay and a positiveculture (or serology), the presence of inhibitors orsome other technical problem with the PCR assaymust be considered.
Serology
Measurement of antibody remains the cornerstonefor M. pneumoniae diagnosis. The complement fixa-tion test was the standard for antibody detection formany years and is still used today in some state healthlaboratories. However, it is a laborious assay to per-form and has inherent disadvantages such as nonspe-cific cross-reactions. Complement fixation has beenlargely replaced by commercial assays utilizing immu-nofluorescence, particle agglutination, or EIA formats(120). EIAs offer several advantages over the otherassay designs, including increased sensitivity, smallvolume demands, isotypic discrimination, and ease ofuse. Commercially available serologic assays sold inthe United States are described in reference texts(120–122). A recent study comparing the commercialEIAs available in the United States showed that someperform significantly better than others and thatpaired sera are recommended for serodiagnosis ofM. pneumoniae infections (110). Among the testsevaluated in that study are two qualitative rapidmembrane-based EIAs with a moderate-complexityCLIA classification that can be performed as point-of-care procedures in a physician’s office or in a clin-ical laboratory. These are the IgM ImmunoCard(Meridian Diagnostics, Cincinnati, Ohio) and theRemel IgG and IgM antibody test (Remel Laborato-ries). These tests do not require any specialized equip-ment, and they are cost-effective when performed onsingle serum samples or small batches. Even in the ear-ly phases of infection, with use of single acute-phaseserum samples, approximately 25% of M. pneumo-niae infections may be diagnosed serologically usingan IgM-based EIA (110). Therefore, these tests may
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 13

afford health care providers timely information need-ed to diagnose and treat patients with M. pneumoni-ae infections. However, it is important to understandthat although specific IgM antibodies to M. pneumo-niae are detectable in most pediatric patients with arecent infection of at least a week’s duration, inadults, where reinfection is common, IgM is notalways produced. Adults may produce only IgG anti-bodies, particularly to protein antigens, which aredetected only with IgG-IgM-combined EIAs or IgG-specific EIAs. Duration of the IgM response is vari-able, and in some instances the response may persistfor several weeks. This observation supports the needto test paired sera for optimum diagnosis of currentor recent infection.
C. pneumoniae and Chlamydophila psittaciC. pneumoniae may cause up to 10% of community-acquired pneumonias, and it can also cause pharyn-gitis (41). The true incidence of pharyngitis due to thisorganism is unknown because relatively few caseshave included successful isolation of the organism toaccompany a serologic diagnosis (53). Sore andscratchy throat with hoarseness is a very commoninitial manifestation of C. pneumoniae respiratorytract infection that may progress to tracheobronchi-tis and pneumonia. Sinusitis and otitis may also occur.Some studies have found a low incidence of pharyn-gitis due to this organism and suggest its role inpharyngitis to be as more of a copathogen than a pri-mary pathogen since it is often detected in the pres-ence of other organisms known to produce the illness(38).
C. psittaci is a less common cause of pneumoniathan C. pneumoniae, and only a few hundred casesof C. psittaci pneumonia are reported in the UnitedStates each year. The true incidence is probably muchgreater because in many cases no attempt is made toobtain a microbiological diagnosis and patients aretreated empirically. This illness is usually acquiredfrom inhalation of respiratory droplets from infectedbirds, but human-to-human transmission can occurin rare circumstances. Many cases of psittacosis beginwith sore throat and pharyngitis before progressingto pneumonia.
Diagnosis
Diagnosis of Chlamydophila infections is highlyvariable among laboratories due to the lack of refer-ence methods and the use of nonstandardized tech-niques. In 2000, the CDC and the Laboratory Centrefor Disease Control (Ottawa, Ontario, Canada) host-ed a meeting to draft and provide consensus recom-mendations for culture, serology, and PCR for C.pneumoniae. This interest was due to the importanceof this organism in acute respiratory illnesses as wellas a purported role in other chronic inflammatory
conditions. Their report was subsequently published(36).
Specimen Collection,Transport, and
Processing for Culture
To detect C. pneumoniae by culture, oropharyn-geal swabs can be collected as described above forstreptococci, placed into 2SP transport medium (120),and held at 4°C until processed. If the specimens areto be held longer than 24 h they must be frozen at�70°C and transported on dry ice if not processedlocally. Most hospital-based laboratories cannot offerC. pneumoniae culture due to the complexity of theprocedures and the very limited need to performthese tests on a regular basis to be cost-effective andto maintain technical proficiency.
To process the specimens, swabs are mixed on avortex mixer for 20 s and then pressed against theside of the tube to extract all the liquid. Two hundredmicroliters of the resulting fluid is centrifuged at8,000 to 10,000 � g, resuspended in cell culturemedium such as Eagle’s minimal essential medium orIscove’s modified Dulbecco’s medium supplementedwith fetal calf serum (10%), L-glutamine (2 mM),Eagle’s minimal essential medium nonessential aminoacids, HEPES buffer, gentamicin (10 �g/ml), van-comycin (25 �g/ml), and amphotericin B (2 �g/ml),and homogenized. Tissue specimens are suspended incell culture medium before homogenization.
Both HEp-2 cells and HL cells support chlamydi-al growth and are primarily cultured in 96-well plateor shell vial formats. To inoculate cells, the specimensare centrifuged onto the monolayer at 900 to 3,000� g for 60 min. After centrifugation, replace themedium with cycloheximide-supplemented medium.Incubate at 35°C with 5% CO2 and examine cultureson day 3 and thereafter daily to check for inclusionbodies.
Bacterial Identification and Reporting Results
Genus- and species-specific monoclonal antibodiescan be used to identify C. pneumoniae inclusions. Itis recommended that an average of �1 inclusion perwell or tube be considered a “presumptive” positive,and only if the strain is propagated by subsequent pas-sage or confirmed by another test such as PCR shouldit be considered a “confirmed” positive. The use ofserum-free media, multiple centrifugations, or pre-treatment of cells is not warranted. Further details onculture and suggested controls can be found in thesummary by Dowell et al. (36). When C. pneumoni-ae is detected anywhere in the respiratory tract byany method, it should be reported and considered tobe clinically significant since it is not part of the com-mensal flora. Culturing of C. psittaci is possible but
14 Waites et al. CUMITECH 10A

should not be done because it can be hazardous tolaboratory personnel.
AST
Since Chlamydophila culture is seldom performed,AST is an even rarer procedure. Chlamydophilaorganisms are susceptible to the expected agents inthe macrolide, ketolide, tetracycline, and fluoro-quinolone classes. Methods for AST for C. pneumo-niae have been described and have been used for invitro evaluation of new antimicrobial agents (52), butthere are no guidelines or recommendations from theCLSI.
Molecular Biology-Based Tests
Difficult-to-culture organisms such as Chlamy-dophila are readily adaptable to detection by PCR.Collection, transport, and processing of specimensfor PCR are similar to those used for culture. Onemilliliter of the inoculated transport medium is cen-trifuged at 18,000 � g for 15 min. The pellet is thenprocessed for DNA extraction by using an efficientand reliable protocol or a commercial kit. Of themany PCR methods published, four have met the cri-teria for validation according to the CDC (22, 46,81, 114). A sensitive and specific real-time PCR assayhas been developed which detects the VD4 region ofthe ompA gene of C. pneumoniae (113). Each runshould include low-copy-number positive controls(�1 inclusion-forming unit) and water controls withevery fifth extraction (36). No PCR assays for detec-tion of C. pneumoniae have been approved for com-mercial sale thus far in the United States.
There is a PCR assay for the detection of C. psittaciDNA which uses the touchdown PCR method (81).Other assays have been developed, but thus far thereare no validation criteria for PCR diagnosis of C.psittaci infection. An immunochromatographic assayto detect specific C. psittaci antigens in respiratorytract specimens has also been described (115).
Serology
Serologic diagnosis of C. pneumoniae infection isnot optimum for patient management, as paired seraare required to show a four-fold rise in IgM or IgGtiter, but in epidemiologic studies it is often the bestapproach. The microimmunofluorescence (MIF) assayis the only serologic method that has been evaluatedwith good results, and it is the only assay that canmeasure isotype-specific antibodies to C. pneumoniaeand C. psittaci simultaneously. The MIF assay usespurified species-specific elementary bodies as theantigen and is therefore recommended as the standardfor serologic diagnosis. Acute infection is defined bya fourfold rise in IgG or IgM titer to �16, and pastexposure is defined by an IgG titer of �16. In theinterpretation of results, one has to consider the usu-
al caveats of persistent titers or titers in persons withchronic infections, the absence of antibodies in per-sons with culture-confirmed infections which some-times occur, and false-positive IgM results if serumis not absorbed before testing (36). MIF serologicassays have been developed for commercial use andare available through reference laboratories.
LARYNGEAL SYNDROMES
Acute Laryngitis and Laryngotracheobronchitis
Laryngitis is a common manifestation of upper respi-ratory tract infections characterized by rhinorrhea,cough, and sore throat, usually affecting older chil-dren, adolescents, and adults. Diagnosis of acutelaryngitis is usually made by history alone. Illnessbegins as a common cold with minimal or no associ-ated fever. The patient complains of hoarseness, andvocal cords appear hyperemic, resulting from edema.
Acute laryngotracheobronchitis, the “croup syn-drome,” encompasses several types of infections ofthe larynx, with hoarseness and a barking cough andvariable respiratory distress, and affects primarilyyoung children. Croup can be a serious infectionwhich extends downward from the larynx to involvethe trachea and sometimes the bronchi. The onset isgradual, also following upper respiratory tract infec-tion. Severe respiratory distress, especially in younginfants, and fever are common manifestations. Croupproduces narrowing of the airway and similar signsand symptoms as seen in epiglottitis, but childrenwith croup tend to have a longer course of illness,worsening at night, and a barking cough. However, inchildren younger than 6 months, the presentation ofcroup and epiglottitis can be indistinguishable.
The primary etiologic agents for both of these con-ditions are respiratory viruses (57). However, bacter-ial respiratory tract infections due to B. pertussis,Bordetella parapertussis, and C. diphtheriae have alsobeen associated with acute laryngitis, and these agentsare discussed in subsequent pathogen-specific sec-tions (86). Isolation of M. catarrhalis and H. influen-zae from adults with laryngitis has been frequentlyreported (103). In many instances, initial infection iscaused by various viruses, and bacteria play a roleas superinfecting agents taking advantage of thedamaged respiratory tract mucosa. Unusual causesdescribed in case reports include Candida spp. (71),Coccidioides immitis (117), Cryptococcus neofor-mans (21), and Streptococcus agalactiae (90). Laryn-gitis can also be associated with pulmonary tuber-culosis, blastomycosis, and histoplasmosis. In viewof the viral etiology for most cases of acute laryngitisand croup, bacterial or fungal cultures are neededonly when there is no other apparent cause or when
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 15

differentiating the more chronic infections (e.g.,histoplasmosis and tuberculosis) from laryngealmalignancies.
Epiglottitis
Epiglottitis is an infectious process that producesinflammation and edema of the supraglottic struc-tures, which include the epiglottis, uvula, base of thetongue, aryepiglottic folds, arytenoids, false vocalcords, and adjacent pharyngeal walls. In contrast tolaryngitis and croup, epiglottitis is primarily of bac-terial etiology. Acute epiglottitis typically occurs inchildren between 2 and 6 years of age and character-istically presents with an acute onset of high fever,sore throat, and respiratory obstruction with stridor,dysphagia, drooling, and agitation. It is important todifferentiate this condition from viral croup becauseof therapeutic implications (Table 2). Epiglottitis isuncommon in U.S. children today owing to theimmunity provided by the conjugate vaccine for H.influenzae type b given during infancy. Adults withepiglottitis usually have a less acute presentationcharacterized by odynophagia and a change in voice.Less common manifestations in adults are dyspnea,drooling, stridor, pharyngitis, fever, cervical adeno-pathy, cough, and hemoptysis. Epiglottitis affects ap-proximately 1 in 100,000 adults annually.
Etiology
Even though the incidence of invasive disease in thepediatric population due to H. influenzae has de-creased dramatically as a result of vaccination, withfewer than 100 cases annually in the United States, the
vaccine is not 100% effective and rare cases of H.influenzae epiglottitis have been described in previ-ously vaccinated children (85). Other bacterial speciesthat have been associated with epiglottitis includenontypeable H. influenzae, Haemophilus parain-fluenzae, S. pneumoniae, S. pyogenes, and S. aureus.Various respiratory viruses may also account for somecases.
Diagnosis
Endoscopy or indirect laryngoscopy can be per-formed to assess the supraglottic structures for evi-dence of supraglottitis in adults, but this should notbe attempted in young children without support of ananesthesiologist because slight agitation may precipi-tate acute and life-threatening respiratory obstruc-tion requiring intubation. Alternatively, characteristicradiographic changes indicating an enlarged epiglot-tis and leukocytosis with a left shift are supportive ofthe diagnosis. Recovery of H. influenzae or otherbacteria associated with epiglottitis that may alsooccur in the pharynxes of healthy persons from cul-tures from the epiglottis may simply represent localcontamination. The high rates of asymptomatic car-riage make it difficult to accurately assess the role ofHaemophilus spp. in other upper respiratory tractinfections such as pharyngitis. Moreover, manipula-tion of the epiglottis may lead to respiratory obstruc-tion. Thus, diagnosis is essentially clinical withoutthe need for isolation of etiologic organisms directlyfrom the affected site, but blood culture can often beconfirmatory since as many as 50% of cases are bac-teremic. Blood is collected and processed according
16 Waites et al. CUMITECH 10A
Table 2. Differential characteristics of common infectious laryngeal syndromes
Laryngotracheobronchitis Characteristic Epiglottitis Laryngitis
(croup)
Age groups most Children 2–6 yr of age Older children, adolescents, Infants and young commonly and adults children 3 mo–3 yr of ageaffected
Microbial etiologies H. influenzae, H. parainfluenzae, Influenza virus, adenovirus, Parainfluenza viruses, respiratory S. pneumoniae, S. pyogenes, rhinovirus, parainfluenza viruses, syncytial virus, adenovirus, S. aureus respiratory syncytial virus, H. influenzae, M. pneumoniae,
papillomavirus, M. catarrhalis, S. pyogenes, S. aureus, M. pneumoniae, C. pneumoniae, M. catarrhalisS. pyogenes; rare causes: B. pertussis, B. parapertussis, C. diphtheriae, M. tuberculosis, Candida spp., other yeasts
Clinical presentation Acute onset of fever, sore throat, Hoarseness, sore throat, fever, Fever, barking cough, wheezing, drooling, agitation nasal congestion, coryza respiratory distress, stridor
Diagnostic test(s) Blood cultures, radiographic Laryngoscopy Radiographic imagingimaging, laryngoscopy
Management Artificial airway, systemic Voice rest, surgical resection of Mist therapy, racemic antibiotics papillomas (if present), systemic epinephrine, dexamethasome,
antibiotics if bacterial disease systemic antibiotics if bacterial is suspected infection is suspected

to recommended procedures outlined in Cumitech 1C(7) and in accordance with individual laboratoryprotocols by using automated or nonautomatedmethods.
AST
H. influenzae isolates from bacteremic personswith epiglottitis should be tested for �-lactamase pro-duction by the chromogenic cephalosporin nitrocefin(cefinase) method, since many strains have this resist-ance marker, but measurement of MICs is not neces-sary. Based on the appearance of the supraglotticstructures and overall status of the patient, insertionof an artificial airway (intubation or tracheostomy)may be required. Administration of parenteral anti-biotics such as an extended-spectrum cephalosporinshould be initiated as soon as possible after the patientwith epiglottitis presents for medical treatment. Hos-pitalization is usually indicated.
OTITIS
Otitis Externa
Otitis externa is an infection of the external ear canalthat is usually caused by excessive moisture thatallows bacteria to multiply in the cerumen of the earcanal, leading to maceration and inflammation.However, it can also be the result of trauma to theexternal auditory canal, sometimes induced byattempts to clean or scratch the itching ear, or a vari-ety of dermatologic conditions such as eczema andpsoriasis. Otitis externa is technically not a disease ofthe upper respiratory tract, but it is included herebecause of the importance in distinguishing it fromotitis media with discharge secondary to a rupturedtympanic membrane. Otitis externa can be acute,chronic, localized, diffuse, or malignant (26).
Otitis externa can occur in persons of any age,most commonly affecting children aged 7 to 12 years.It occurs most commonly in swimmers and individu-als who have other types of exposure that allow con-taminated water to be trapped in the external canal.Deep-seated infection (malignant otitis externa)occurs almost exclusively in the patients who areimmunocompromised or have chronic diseases suchas diabetes mellitus (26). Untreated malignant otitisexterna can lead to cellulitis and osteomyelitis.
Otitis externa typically presents with a serosan-guinous or purulent discharge from the erythematousand swollen external ear canal in association with earpain and itching. In some cases there may be furun-cles in the ear canal. Severe cases may be associatedwith preauricular, postauricular, or cervical adenopa-thy and fever. Otitis externa is distinguished frompurulent otitis media with perforation of the tympan-ic membrane and drainage by careful examination of
the ear canal after debris and discharge have beenremoved. In contrast to that in a case of otitis media,the tympanic membrane is mobile on insufflation.
Etiology
The most common causative organisms of acuteotitis externa are Pseudomonas aeruginosa and S.aureus (20). Other aerobic gram-negative bacilli andgram-positive cocci such as S. pyogenes may occa-sionally be involved (5). Vibrio alginolyticus has beenimplicated as a cause of otitis externa in persons whoswim in salt water (42). Commensal cutaneous organ-isms such as corynebacteria and coagulase-negativestaphylococci may be isolated from the external earcanal, but they are not normally considered to be ofclinical significance in this setting. Chronic otitisexterna may be secondary to a persistent, suppura-tive middle-ear infection accompanied by tympanicmembrane perforation. Thus, the bacterial etiologiesof this condition are reflective of those involved withthe middle-ear disease (26). Rare bacterial causes ofchronic otitis externa include Mycobacterium andNocardia spp. These organisms are not normallysought in microbiological evaluations without priorconsultation with the clinician or evidence of theirpresence based on Gram-stained smears of dischargefrom the ear canal. Anaerobic bacteria were oncethought to be insignificant in otitis externa (5), butmore recent evidence suggests that anaerobes may bedetected in as many as 25% of persons with otitisexterna in the absence of aerobic and facultative bac-teria or in mixed infections (20). Anaerobic bacteriainvolved in otitis externa include Peptostreptococcusspp., Bacteroides spp., Fusobacterium spp., Porphy-romonas spp., Propionibacterium acnes, and Prevo-tella spp. (20). Herpesviruses have also been impli-cated in some cases (17). Fungi cause approximately10% of cases of otitis externa, with the most com-mon pathogens being Aspergillus spp., followed byCandida albicans (17). Fungal otitis externa can bethe result of prolonged treatment of bacterial otitisexterna that alters the flora of the ear canal, some-times leading to mixed bacterial and fungal infec-tions. However, fungi are occasionally the primarypathogens.
Diagnosis
The clinical diagnosis of otitis externa can be madeby direct examination of the affected ear. Since sev-eral different microorganisms can be involved, amicrobiological diagnosis requires demonstration ofthe organisms by Gram staining and identification incultures. However, from a practical standpoint, casesof only mild to moderate severity are usually man-aged empirically without microbial evaluation. Deep-seated infections are likely due to P. aeruginosa,
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 17

which can be confirmed by Gram staining, culture,and AST.
Specimen Collection,Transport, and
Processing for Culture
Material can be collected for Gram staining andculture by swabbing of the ear canal, by needle aspi-ration of furuncles, or by surgical debridement. Use ofseparate swabs for Gram staining and culture is pre-ferred. Use of swab transport systems with supportivemedia such as Amies gel facilitates maintenance oforganism viability until cultures can be inoculated.Fluid can be sent to the laboratory in a sterile capsyringe with the needle removed. Tissue obtained bysurgical debridement can be sent to the laboratory ina sterile screw-cap container. Fluids or tissue speci-mens collected without transport media must berefrigerated at 4°C if they cannot be processed with-in 2 h of collection. If anaerobe cultures are specifi-cally requested through direct consultation with theclinician, a swab, fluid, or tissue is placed into the ap-propriate anaerobic transport system, such as thePort-A-Cul (Becton Dickinson), and sent to the labo-ratory as soon as possible. Anaerobe cultures are keptat room temperature until inoculated onto appropri-ate media. Primary inoculation media for specimensobtained from the external ear canal for aerobic bac-terial culture should include SBA and an enteric indi-cator medium such as MacConkey agar that areincubated at 35 to 37°C in air (MacConkey agar) orin air plus 5% CO2 (SBA) and read after 18 to 24 hand again after 48 h. Primary inoculation mediafor anaerobic bacteria include Brucella agar withsheep blood, phenyl-ethyl-alcohol agar with sheepblood, laked kanamycin-vancomycin blood agar,Bacteroides-bile esculin agar, thioglycolate brothwith hemin and vitamin K, or chopped meat glucosebroth.
Bacterial Identification and Reporting Results
Spores and hyphae may be observed with the Gramstain if the etiology is fungal, and they should benoted in the report. Otherwise, the Gram reaction,the cellular arrangement of bacteria, and the presenceof inflammatory cells should be described. The nor-mal flora of the external ear canal includes coagulase-negative staphylococci and Corynebacterium spp., sothe presence of these organisms is not considered to beof clinical importance or reported as other than “nor-mal flora.” All other aerobic and facultative bacteriaisolated are identified to the species level when possi-ble unless there are mixed cultures of gram-negativerods. The most common aerobic bacterial agents ofotitis externa can be readily identified by standardbiochemical methods available in clinical laborato-ries. Simple tests such as the appearance of gram-pos-
itive cocci in clusters and cream-colored raised beta-hemolytic colonies on SBA, supplemented by positivecatalase and coagulase reactions, a negative PYR reac-tion, and growth and yellow coloration on mannitolsalt agar, can presumptively identify S. aureus. How-ever, many laboratories prefer to use one of thenumerous commercial biochemical or automated sys-tems such as MicroScan (Dade MicroScan, WestSacramento, Calif.) and Vitek (bioMérieux) that pro-vide acceptable identification of S. aureus and differ-entiate this organism from other gram-positive cocci.These products are described more completely in ref-erence texts (e.g., reference 6). Rapid species-levelidentification of S. aureus can also be accomplishedusing molecular biology-based assays such as theAccuProbe (Gen-Probe, Inc.). Discussion of strepto-coccal identification is included in the previous sec-tion on pharyngitis. P. aeruginosa and other gram-negative bacilli that may be present in cases of otitisexterna can be identified using widely available man-ual or automated commercial biochemical systems.Common anaerobes can also be identified biochemi-cally or by Gram stain morphology supplemented bya variety of phenotypic tests, including high-potencyantibiotic disk assays, as outlined in reference texts(e.g., reference 63).
An external ear specimen culture with growth ofS. aureus, beta-hemolytic streptococci, or a predomi-nant gram-negative rod usually indicates infectionwith that agent (129). Growth of a predominantanaerobe alone is also likely to be of etiologic signif-icance. However, growth of anaerobes such as P. acnesor Peptostreptococcus spp. concomitantly with otherorganisms presents a more complex situation sincethese organisms can sometimes be found as commen-sals in the external ear canal.
AST
AST should be performed on the predominantpathogenic bacteria isolated in culture except in casescaused by beta-hemolytic streptococci. However,administration of systemic antibiotics is not alwaysnecessary. Local measures, including gentle removalof debris and discharge and treatment with topicalantimicrobial agents directed at the causative patho-gens, often suffice. More severe cases in which infec-tion extends beyond the skin of the ear canal and cas-es of malignant otitis externa may require systemicantimicrobials accompanied by analgesics, topicalcorticosteroids to reduce local inflammation, and sur-gical debridement of necrotic tissue. Use of acidifyingotic drops following exposure to water may be bene-ficial in reducing recurrences of otitis externa.
Fungal Culture
Inoculation of media specific for fungal isolationand utilization of incubation conditions and identifi-
18 Waites et al. CUMITECH 10A

cation procedures necessary for characterization offungi should be performed only if fungal infection isstrongly suspected and/or evidence of fungal elementsis present upon Gram staining of ear discharge. Ageneral discussion of appropriate techniques for iso-lation and identification of Candida spp. is providedin the subsequent section on oropharyngeal candidi-asis. Many Candida infections can be readily detect-ed using SBA. Aspergillus spp. and other yeasts ormolds should be identified and reported if present byusing appropriate biochemical and morphologicalmethods as described in reference texts (e.g., refer-ence 108). Use of inhibitory mold agar which containsantimicrobials such as chloramphenicol and gentam-icin to reduce bacterial overgrowth can be helpful torecover organisms such as Aspergillus.
Otitis Media
Acute otitis media is an infection of the middle earwith rapid onset, presence of middle-ear effusion, andsigns of middle-ear inflammation. Otitis media witheffusion is characterized by fluid collection in the mid-dle ear without signs or symptoms of infection, andit is usually caused when the Eustachian tube isblocked and fluid becomes trapped in the middle ear.Signs and symptoms of acute otitis media usuallyoccur when fluid in the middle ear becomes infected,although microorganisms may be detected in somecases of otitis media with effusion when sensitivetechniques such as PCR are used (64). Otitis mediawith effusion is more common than acute otitis media,and it may be a prelude or sequelae of that condition.Recurrent otitis media is defined as three episodes ofacute otitis media within 6 months or four or moreepisodes within 1 year (75). Some patients developchronic suppurative otitis media.
Infection of the middle ear usually arises as a com-plication of a preceding viral upper respiratory tractinfection in which the acute inflammatory responsecaused swelling and occlusion of the Eustachiantubes. Normally, air in the middle ear is absorbed bythe ear’s mucosal lining. If air is not replaced due tothe relative obstruction of the Eustachian tube, a neg-ative pressure is generated, resulting in secretion of aserous effusion which easily becomes infected byupper-airway viruses and/or bacteria. If the infectionand the resultant inflammatory reaction persist, per-foration of the tympanic membrane or extension intothe adjacent mastoid air cells may occur, leading tomastoiditis.
Acute otitis media is the most common reasonantibiotics are prescribed for young children in theUnited States (75). As many as 80% of children haveexperienced at least one episode by the time they are3 years old. This condition occurs more often in boysthan in girls, and its incidence has increased over the
past 2 decades as more children are placed in daycarecenters where they have greater exposure to patho-genic microorganisms (26). Children with anatomicmalformations such as a cleft palate are especiallyprone to frequent episodes of acute otitis media. Eventhough acute otitis media is most common in youngchildren, it can occur in persons of any age. Thehigher frequency in children is presumably related toimmunologic factors, such as a lack of pneumococcalantibodies, and anatomic factors, including a lowerangle of the Eustachian tube with relation to the naso-pharynx, and the higher frequency in young childrenof viral respiratory tract infections that can lead toblockage of the Eustachian tubes.
Clinical diagnosis of otitis media can be madebased on a typical history of fever, ear pain, and hear-ing loss and an inflamed, bulging, immobile, tympan-ic membrane assessed by otoscopy. Infants and veryyoung children may often tug at their ears but can beasymptomatic otherwise except for irritability (75).Some cases, when left untreated, progress to sponta-neous perforation of the tympanic membrane withdrainage of purulent material into the external earcanal. Significant concerns in young children withsevere otitis media with recurrence and tympanicmembrane perforation are hearing deficit and speechdelay. Otitis media is not considered a common sourceof bacteremia or meningeal seeding, but local brainabscesses and systemic spread can occur (75). Hear-ing loss may be the only evidence of serous otitismedia with effusion.
Etiology
Even though middle-ear infection is quite oftenpreceded by viral infections of the upper respiratorytract, viruses are less likely to be pathogenic in thiscondition than common bacteria. Overall, variousviruses have been isolated from middle-ear effusionsof 8 to 25% patients with otitis media (101). Amongthe viruses known to cause acute otitis media, respi-ratory syncytial virus, influenza virus, adenovirus,and rhinovirus are the most common agents impli-cated as primary pathogens.
The most common bacterial pathogens in acuteotitis media are S. pneumoniae, nonencapsulated H.influenzae, M. catarrhalis, and S. pyogenes. Compar-ison of culture with the more sensitive detectionmethod of PCR has shown that these common bac-teria may actually be present in middle-ear effusionsmore often than was formerly appreciated. Other lesscommon bacterial etiologies include S. aureus, viri-dans group Streptococcus spp., P. aeruginosa, andother gram-negative bacilli. C. pneumoniae has beenreported as an uncommon pathogen in otitis media(14), and Chlamydia trachomatis may cause someinfections in very young infants. M. pneumoniae has
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 19

been detected occasionally in middle-ear fluids andhas been associated with bullous myringitis, but evidence based on PCR results suggests that thisorganism is uncommon in this condition, and it,along with the chlamydiae, is not routinely sought inclinical material (69). Anaerobic bacterial species,similar to those described above for otitis externa,have been recovered from the middle ears of childrenwith acute and chronic otitis media (19, 37). Neitheryeasts nor molds have an important role as patho-gens in acute otitis media, but they may sometimes beof etiologic significance in chronic otitis mediaand/or otitis media in children who are immunocom-promised (84).
Utilization of the conjugate pneumococcal vaccinein infants has led to changes in the bacteriology ofacute otitis media. Specifically, there has been a reduc-tion in the occurrence of those pneumococcal sero-types included in the vaccine, a reduction in anti-biotic resistance, and replacement with nonvaccineserotypes (34). Most H. influenzae strains associatedwith otitis media are not type b and are therefore notcovered by the H. influenzae type b vaccine (68).
In recent years, attention has been given to a fas-tidious gram-positive coccus, Alloiococcus otitidis(73). This organism is difficult to culture, and mostavailable data on its role in middle-ear disease havebeen obtained by PCR. This bacterium has beendetected in patients with otitis media with effusion,especially chronic cases (73), and in children withacute otitis media (72). Despite the frequency ofoccurrence, the role of A. otitidis as a primary patho-gen in middle-ear infection has not been firmly estab-lished, especially in otitis media (72).
Diagnosis
Most cases of otitis media are diagnosed on clini-cal grounds alone and managed empirically withoutthe benefit of specific microbiological tests. Tympa-nometry is sometimes used to determine whether amiddle-ear effusion is present, but this technique can-not reliably differentiate acute otitis media and chron-ic serous otitis media.
If there is spontaneous perforation of the tym-panic membrane, drainage fluid may be available forGram staining and culture. Tympanocentesis alsoyields drainage fluid suitable for microbiologicalevaluation, but this invasive procedure is rarely per-formed except in infants younger than 2 months ofage, immunocompromised children, patients in whomantimicrobial treatment has failed, patients withsevere otalgia, and those in whom there have beencomplications requiring more aggressive diagnosisand management strategies. Cultures of the nasophar-ynx are unreliable compared to culture of middle-ear
aspirates for determination of the etiologic agents ofotitis media (50).
Specimen Collection,Transport, and
Processing for Culture
Drainage fluid can be collected from the externalear canal on swabs for culture most efficiently whenguided by an otoscope. A second swab should be col-lected for Gram staining. If tympanocentesis is per-formed, fluid is aspirated into a suction trap and sub-mitted directly to the laboratory. Swabs submittedfor culture should be immersed into transport mediasuch as Amies gel to facilitate maintenance of organ-ism viability and prevent desiccation until culturescan be inoculated. Tympanocentesis fluid collectedwithout transport media can be stored at room tem-perature if it cannot be processed within 2 h of col-lection. Anaerobe cultures performed with fluid col-lected by tympanocentesis can be kept at roomtemperature until inoculated onto the appropriatemedia.
Bacterial Identification and Reporting Results
The relative numbers of microorganisms observedand the types of inflammatory cells are evaluated inconjunction with the Gram stain reaction and bacte-rial cell arrangements. Specific attention must begiven to the presence of any yeast or other fungal ele-ments. Middle-ear drainage fluid should be inocul-ated onto SBA and MacConkey and chocolate agarsand incubated at 35 to 37°C for up to 4 days fordetection of the most common bacterial pathogens.SBA and chocolate agar are incubated in an atmos-phere of air with 5% CO2. All bacteria that grow,with the exception of mixtures of commensal skinflora organisms, such as coagulase-negative staphy-lococci and Corynebacterium spp., are identified tothe species level to the extent possible and consideredto be of possible etiologic significance unless there isa mixture of several organisms with no predominantpathogen evident. In this circumstance, a report of“mixed flora” is appropriate, with instructions forthe clinician to contact the laboratory if further eval-uation is desired. A pure culture of large numbers oforganisms such as coryneform bacteria may some-times be significant, and such cultures can be evalu-ated biochemically by using systems such as the APIRAPID Coryne system (bioMérieux).
S. pneumoniae is the organism most commonlydetected in clinical specimens from cases of otitismedia. Most pneumococci can be easily identified bytheir typical characteristics of gram positivity, arrange-ment in pairs and short chains, formation on SBA ofalpha-hemolytic colonies that are indented in thecenter, a negative catalase reaction, and the develop-ment of an inhibitory zone �14 mm in diameter
20 Waites et al. CUMITECH 10A

around an optochin disk. Identification methods forother streptococci, S. aureus, and gram-negativebacilli have already been discussed.
M. catarrhalis produces smooth, grayish, opaquecolonies on SBA or chocolate agar that are oxidaseand catalase positive. The organism does not produceacid from carbohydrates and is DNase positive. Apositive �-lactamase test using the nitrocefin (cefi-nase) method in conjunction with the other pheno-typic tests is sufficient to identify M. catarrhalis.Many of the commercial biochemical systemsdescribed above for the neisseriae can also identifyM. catarrhalis.
The presence of Haemophilus spp. may be sus-pected with evidence of small gram-negative rods orcoccobacilli that may be pleomorphic and grow onchocolate agar incubated in 5% CO2 but not onunsupplemented SBA. H. influenzae appears onchocolate agar as grayish, semiopaque, smooth, andflat convex colonies 1 to 2 mm in diameter. A clue tothe presence of an encapsulated strain is confluenceof growth in dense areas of the agar plate, whereascolonies of nonencapsulated strains remain separate(68). Suspicious colonies can be distinguished fromother fastidious gram-negative organisms and identi-fied to the species level by a variety of phenotypictests. Classically, the differential requirements for X(hemin) and V (NAD) factors and other biochemicalfeatures allow identification to the species levelaccording to the scheme shown in Table 3. Filterpaper disks containing X, V, or X and V factors com-bined are available commercially from a variety ofsuppliers. Quadplates composed of Mueller-Hintonagar containing X factor, V factor, or both, along witha separate compartment with horse blood agar todemonstrate hemolysis, are also available (RemelLaboratories) and convenient to use for separatingHaemophilus spp. Use caution when relying solely
on tests for requirements of X and V factors on mediasuch as Trypticase soy agar to distinguish H. influen-zae from other Haemophilus species because of thepossibility that X factor can be carried over in bacte-ria subcultured from blood-containing media. Use ofthe �-aminolevulinic acid (ALA)–porphyrin test dis-tinguishes species that require exogenous X factor(H. influenzae and Haemophilus haemolyticus),which test negative. This test is performed by inocu-lating bacteria growing on agar onto a filter paperdisk containing the ALA reagent, incubating for 4 h,and examining for fluorescence under UV light. Evi-dence of brick-red fluorescence indicates the abilityof the organism to synthesize protoporphyrins fromALA and constitutes a positive test result. There areseveral commercial products that can distinguishHaemophilus spp. with a battery of biochemical testsbased to some degree on characteristics shown inTable 3. Use of special selective Haemophilus isola-tion agar is probably not cost-effective or practicalfor most laboratories. Inoculation of a clinical speci-men onto SBA with a streak of S. aureus to watch forsatelliting colonies of Haemphilus spp. has been usedas a screening test for the presence of these organ-isms, which grow only in proximity to the staphylo-coccus as a result of its localized release of X and Vfactors, but this procedure does not provide clues tospecies identification and does not have significantadvantage over primary inoculation onto a nonselec-tive medium such as chocolate agar. There is also aDNA probe available for identifying H. influenzaecolonies (Gen-Probe, Inc.) that has been shown to besensitive and specific compared to other methods(68).
Serotyping of encapsulated H. influenzae isolatescan be accomplished with an agglutination techniqueusing type-specific antisera available commerciallyand also with other methods including PCR. While
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 21
Table 3. Biochemical characteristics of Haemophilus species encountered in the human respiratory tracta
Factors
Species requiredResult for: Fermentation of:
X V Hem Cat ALA ODC H2S Ure Ind Glu Suc Lac Man Xyl
H. influenzae � � � � � VR � VR VR � � � � �
H. aegyptius � � � � � VR � � VR � � � � �
H. haemolyticus � � � � � � � � VR � � � � �
H. parainfluenzae � � � VR � VR � VR VR � � � � �
H. parahemolyticus � � � � � VR � � � � � � � �
H. segnis � � � VR � � � � � � �w � � �
H. paraphrophilus � � � � � � � � � � � � � �
H. paraphrophaemolyticus � � � NA � � NA � � � � � � �
H. aphrophilus � � � � � � � � � � � � � �
aAbbreviations: X, hemin; V, NAD; Hem, hemolysis on horse or rabbit blood agar; Cat, catalase; ODC, ornithine decarboxylase; H2S, hydrogen sulfide; Ure,urease; Ind, indole; Glu, glucose; Suc, sucrose; Lac, lactose; Man, mannose; Xyl, xylose; NA, not available; �w, weak positive reaction; VR, variable reac-tion; �, positive reaction; �, negative reaction.

this procedure may not be necessary for routine test-ing and reporting on clinical specimens, documenta-tion of invasive infections with H. influenzae type bto investigate vaccine failure can be important. Typeb invasive disease has become so uncommon that lab-oratories may find it impractical to offer serotypingas an internal test and instead choose to submitappropriate clinical isolates to state public health lab-oratories. Biotyping of H. influenzae and H. parain-fluenzae on the basis of the urease, indole, and orni-thine decarboxylase reactions has been proposed byKilian (68). These determinations appear to be ofgreater value for epidemiological purposes than forclinical patient management. Some of the commercialbiochemical systems include the necessary reagentsso that the biotype is determined along with speciesidentification. The other seven Haemophilus speciescommonly detected in the human respiratory tract areless commonly associated with disease. A report ofpredominance of Haemophilus spp. in a clinical spec-imen is more valuable to a clinician than merely astatement of their presence or absence.
Brain heart infusion agar with 5% defibrinatedrabbit blood has been used successfully for cultureisolation of A. otitidis after 72 h of aerobic incuba-tion. This organism occasionally grows on SBA in 5days, but it does not grow on chocolate or Mueller-Hinton agar with lysed horse blood, buffered char-coal yeast extract, or Columbia agar with colistin andnalidixic acid (15). A. otitidis appears as tiny coloniesthat may be slightly yellow in appearance, and itresembles staphylococci upon Gram staining. The fol-lowing reaction results confirm identification of A.otitidis when used in conjunction with growth re-quirements described above: catalase negative orweakly positive, PYR positive, leucine aminopepti-dase positive, and vancomycin susceptible. Testing forthis organism by culture is currently beyond the capa-bilities or needs of most hospital laboratories and istherefore not recommended for routine purposes(129). Perform anaerobic cultures only by specialrequest. They can be processed as described above forotitis externa.
AST
AST should be performed on S. pneumoniae, S.aureus, and gram-negative rods by using current CLSIguidelines. It is important to use the most up-to-dateprocedures because MIC breakpoints and recommen-dations for susceptibility tests on S. pneumoniae haveundergone several changes over the past few years inthe CLSI documents. �-Lactamase tests (nitrocefinmethod) can be performed on H. influenzae, butother susceptibility tests are not necessary to guidepatient management in view of the infrequent occur-rence of other types of resistance in this organism as
determined by large-scale surveillance studies (118).Since M. catarrhalis almost always produces �-lactamase, performance of this test is optional whenthis organism is isolated.
Historically, administration of systemic antimicro-bials empirically to cover the most common bacterialpathogens, along with analgesics and decongestants,has been the mainstay of treatment for acute otitismedia. More recently, partially as a result of increasedantimicrobial resistance in S. pneumoniae and outcome-based data from clinical trials, the AAP andthe American Academy of Family Practitioners haveprovided recommendations for management that donot include administration of antimicrobial agents forselected children based on diagnostic certainty, age,illness severity, and assurance of follow-up (75).Despite increasing resistance of S. pneumoniae to �-lactams, oral amoxicillin remains the first-line treat-ment of choice (75).
Fungal Culture
Inoculation of media specific for fungal isolationsuch as the nonselective Sabouraud dextrose agar andselective inhibitory mold agar should be performedonly if fungal infection is strongly suspected and/orevidence of fungal elements is present upon Gramstaining of ear discharge. Persons with chronic sup-purative otitis media comprise the patient group mostlikely to have fungi involved (61). Yeasts and moldscan be sought using methods described above in thesection on otitis externa and below in the section onoropharyngeal candidiasis.
SINUSITIS
Sinusitis includes one or more of the paranasal sinuses with characteristic inflammation of the sinusmucosa, blockage of the sinus ostia, and impairmentof the mucociliary apparatus (102). Maxillary sinus-es are most frequently involved, but frontal and eth-moid sinuses may also be affected, albeit less com-monly. Paranasal sinuses are normally consideredsterile, but contiguous surfaces are heavily colonizedby resident or transitory respiratory bacterial floras.The sinuses can therefore become contaminated bysmall numbers of bacteria which are normally clearedrapidly by the mucociliary apparatus (102). Any con-dition such as a viral upper respiratory infection thatimpedes drainage from the sinuses will enhance thelikelihood of bacterial colonization. Ensuing inflam-mation further obstructs drainage and causes edemaof the mucosal lining. Acute sinusitis can progress tochronic sinusitis, especially in persons with underly-ing predispositions such as allergies, nasal septumdeviation, and the presence of nasal polyps (102).
22 Waites et al. CUMITECH 10A

Acute sinusitis affects over 32 million adults a yearin the United States, accounting for 11.7 million officeor clinic visits annually; it is one of the most commoncomplaints seen in primary-care medicine. Addition-ally, 37 million cases of chronic sinusitis are reportedyearly (102).
Etiology
Sinusitis may be caused by viruses, bacteria, or fun-gi. In most instances the etiology of sinusitis is viral(rhinovirus, influenza virus, parainfluenza virus, oradenovirus) or allergy related, but in a small percent-age of cases, secondary bacterial infections mayevolve. This is especially true in children, in whomviral infections of the upper respiratory tract maybecome complicated by bacterial sinusitis in 5 to13% of cases. Bacterial sinusitis can complicate up to2% of cases in adults with viral upper respiratorytract infections (102). Bacterial contributors to bothacute and chronic sinusitis consist of organisms nor-mally colonizing the upper respiratory tract mucosa,most commonly S. pneumoniae (20 to 35% of cases)and nonencapsulated H. influenzae (6 to 26% ofcases). Anaerobes such as Bacteroides, Fusobacteri-um, and the anaerobic cocci as well as M. catarrhalisare also involved (102). S. pyogenes, S. aureus, andgram-negative bacilli are also associated, althoughless frequently (5). Gram-negative bacilli, includingdrug-resistant strains, have to be considered in casesof nosocomial sinusitis, especially in patients whohave been mechanically ventilated or otherwise intu-bated for any length of time.
Fungi are most frequently involved with chronicsinusitis and occur especially in patients with under-lying immunologic or mechanical abnormalities. Fun-gal etiologies include Aspergillus spp., Fusarium spp.,the dematiaceous fungi (especially Bipolaris spicifera,Cladosporium spp., Curvularia spp., and Alternariaspp.), and the zygomycetes (Mucor spp. and Rhizo-pus spp.). The frequencies of individual organismscan vary according to geographic location.
The general symptoms of sinusitis include nasalcongestion, purulent nasal discharge, dental discom-fort, and facial pain in the maxillary areas. Childrenwith ethmoid sinusitis may develop periorbital cel-lulitis and bacteremia if infection spreads beyond thesinuses (5). More severe complications can includespread to the central nervous system, but these occur-rences are uncommon.
Diagnosis
A diagnosis of sinusitis is most frequently made onclinical grounds alone and is based on the persistenceand chronic nature of symptoms and their severity. Inappropriate clinical settings, additional diagnosticmeasures can include anterior rhinoscopy, fiberopticendoscopy, radiographic evaluations, and, in more
advanced or complicated cases, sinus aspirationand/or biopsy with submission of specimens col-lected from the involved sinuses for microbiologicalexamination. Nasopharyngeal or oropharyngealspecimens are inappropriate for diagnosis of sinusitis.
Specimen Collection,Transport, and
Processing for Culture
The reference standard for microbiologic docu-mentation of sinusitis and its etiologies is microscop-ic examination and culture of secretions, wash speci-mens, and curettage or biopsy material collecteddirectly from the involved sinuses by needle punctureand aspiration or surgical debridement. Such invasiveapproaches are not indicated in most patients. Aggres-sive attempts at diagnosis may be considered forpatients who are deteriorating rapidly or in whomintracranial extension of infection is suspected. Sinusaspiration can be helpful in patients with nosocomi-al sinusitis since this approach also allows the clini-cian to irrigate the sinus as part of the treatment.
Visually guided, endoscopically collected purulentdrainage from the middle meatus of the maxillarysinus may also be helpful when examined microscop-ically and cultured appropriately (128). The specimenmust be collected carefully to ensure that it is not con-taminated. Culture results from such specimens aresimilar to those obtained via puncture and aspiration.
Transport sinus specimens to the laboratory insterile containers. Biopsy tissue, scrapings, and otherdebridement material are kept moist during transportby addition of a small volume of nonbacteriostaticsaline. Aspirates can be sent in the original syringewith a Luer-Lok cap to stop leakage. Specimensobtained by unguided swabbing of the nasopharyn-geal area or anterior nares, sputum specimens, andsalivary specimens are unacceptable for culture in thediagnosis of sinusitis (5, 128).
Specimens with orders for fungal culture and/orsmear are stained by a fungal stain such as the fluore-scent calcofluor white, periodic acid-Schiff, Grocottmethenamine silver, or hematoxylin-eosin stain. Fun-gal cultures should be considered in cases of chronicsinusitis. Eosinophilic material with large pyknoticesosinophil concretions is usually present in cases ofacute fungal sinusitis. Sinus aspirates can be stored atroom temperature until inoculation within 24 h ofcollection.
Bacterial Identification and Reporting Results
Appropriately collected sinus secretions can beGram stained to evaluate the presence and quantity ofmicroorganisms and cellular material. The presenceof neutrophils in numbers greater than “few” is sup-portive of the diagnosis of sinusitis. The presence ofbacteria or fungi in association with the neutrophils
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 23

is also an indicator of their complicity in the infec-tious process. All microorganisms and cell morpholo-gies should be described and enumerated accordingto individual laboratory policy. For example, reportsmight state, “Many WBCs [white blood cells], manygram-positive cocci resembling staphylococci,” or“Few WBCs, moderate squamous epithelial cells, fewgram-positive cocci resembling streptococci, fewdiphtheroids.”
Sinus specimens for routine bacterial culture areset up on SBA and chocolate agar plates (124, 128).Inoculate MacConkey agar plates if significant num-bers of enteric gram-negative bacilli are seen on directsmear preparations or if the sinusitis is nosocomial inorigin. Plates are incubated at 35°C in an atmosphereof air with 5% CO2 and read after 18 to 24 h and 48 h of incubation. Plates can be incubated for longerperiods of up to 4 days if specifically requested or ifslow-growing organisms are suspected in cases ofchronic sinusitis.
Culture workup is directed by the initial directmicroscopic observations on the specimen, and allresults of culture should be correlated to these micro-scopic findings. Common etiologies of sinusitis areidentified to the species level when present in signifi-cant or predominant numbers (e.g., greater than few)and associated with WBCs (128). Appropriate meth-ods of identification described in standard texts andreferences can be used to identify significant isolatesas described in earlier sections. Identify up to threespecies of potentially significant pathogens. If morethan three species are present in significant numbers,they may be identified descriptively. Common colo-nizing or contaminating organisms of the upper res-piratory tract (e.g., Corynebacterium spp., Bacillusspp., respiratory neisseriae, and coagulase-negativestaphylococci) can be reported as genera (e.g., mod-erate numbers of respiratory Neisseria species). Yeastsdo not have to be identified to the species level asthey have not been commonly implicated in sinusitis.Identify any mold to the genus level based on mor-phologic appearance. Any additional identificationof molds can be reserved for specific problem situa-tions and special requests.
Requests for anaerobic culture of sinus materialare uncommon and are normally reserved for prob-lematic cases of chronic sinusitis or cases in whichnosocomial sinusitis is considered. Specimens areprocessed as per routine culture with the addition ofanaerobic culture plates and appropriate incubationconditions. Broth culture tubes are not necessary.The same general principles used for observing andinterpreting routine cultures apply to anaerobic cul-tures. Results of culture should be correlated to directmicroscopic examination, and isolate workup shouldbe directed by their presence in numbers greater thanfew and in association with WBCs.
AST
AST should be performed per laboratory policy onall clinically significant bacterial pathogens as identi-fied in the microscopic evaluation of the specimenand culture results. Policies for AST should be essen-tially the same for sinusitis and otitis media for S.pneumoniae, H. influenzae, and M. catarrhalis. ASTfor S. aureus and gram-negative bacilli should be per-formed, especially if chronic sinusitis and/or nosoco-mial sinusitis is suspected or if their role as significantetiologic agents is indicated by culture and micro-scopic findings. Laboratory policies for AST shouldbe developed in consultation with clinicians whoorder the cultures. Susceptibility testing of anaerobicisolates is not routinely necessary but may be specif-ically requested in recalcitrant cases.
Fungal susceptibility testing is not routinely neces-sary. When specifically requested, isolates may be sentto reference laboratories if tests are not performedlocally. Standard methods for susceptibility testing ofboth the yeasts and the molds have been described bythe CLSI, but interpretation of such results is com-plex and the significance for the outcome in cases ofsinusitis is unknown and of questionable value.
Therapeutic approaches are often empiric andvary depending on suspected etiologies, on severityof symptoms, and, if infections are bacterial, on cat-egory. Treatment choice would also be dependent onthe recent history of antimicrobial use. A patient withacute sinusitis would not require aggressive therapy,but one with chronic sinusitis and exacerbations ofchronic sinusitis would need to be treated moreaggressively. Appropriate choices of antimicrobialagents may include penicillins or cephalosporins,newer macrolides, ketolides, fluoroquinolones, andantifungal agents when necessary. In some instancesof protracted disease, surgical debridement may benecessary to increase the chance of cure.
Fungal Culture
Fungal cultures are appropriate in cases of chron-ic sinusitis. Frequently, the direct microscopic visual-ization of mold forms in the sinus material is crucial.It is important in some cases to debride the sinus andto evaluate fungal involvement with tissue histo-pathologically. Specimens for fungal culture shouldbe plated onto selective (containing inhibitory anti-bacterial agents) fungal culture media according tolaboratory policy and procedures. Multiple plates arehelpful in increasing recovery of fungi, and a combi-nation of two to three media, such as Sabouraud dex-trose, inhibitory mold, and brain heart infusion agarswith antibiotics, is appropriate. Plates are incubatedat 30°C without CO2. Plates are read per laboratoryfungal culture protocol, which typically includes dai-ly reading for the first 5 days followed by more peri-odic reading for a full 3 to 5 weeks of incubation. All
24 Waites et al. CUMITECH 10A

molds should be identified at least to the genus levelby using standard phenotypic or genotypic proce-dures as available in the laboratory.
Serology
Serologic evaluations for specific organisms haveno value in the diagnosis of sinusitis. Patients withallergic fungal sinusitis can have elevated total serumIgE levels and increased levels of fungus-specific IgGbut not fungus-specific IgE (104). Assays for theseconditions are not available commercially, however.
OTHER INFECTIONS CAUSED BYUNUSUAL AND/OR UNCOMMONBACTERIA
Pertussis (Whooping Cough)
Bronchitis is technically an inflammatory processinvolving the lower respiratory tract rather than theupper tract. Bronchitis presents in at least two verydifferent forms (acute and chronic), each requiringsubstantially different approaches to management.Because symptoms often include the upper respirato-ry tract, including cough, clinicians may mistakenlyconsider it an upper respiratory tract problem andattempt to identify possible etiologies of bronchitisby erroneously using upper respiratory tract secre-tions. Except for Bordetella spp., M. pneumoniae,and C. pneumoniae, bacteria have not been com-monly associated with cases of acute bronchitis inotherwise well patients. Bordetella spp. are associat-ed with prolonged, persistent coughing which oftentends to be paroxysmal. Approaches to microbiolog-ical evaluation of bronchitis were reviewed in Cumi-tech 7B (106), and only pertussis is dealt with here.
Pertussis is caused by a fastidious gram-negativecoccobacillus, B. pertussis, and occasionally by itsrelative B. parapertussis (3, 56, 77). Rarely, coinfec-tion with both has been reported (10, 11). Infre-quently, Bordetella bronchiseptica and Bordetellaholmesii have been implicated in pertussis-like respi-ratory symptoms (10, 11). When airborne dropletscontaining B. pertussis are inhaled, the organism uti-lizes a variety of adhesins to enable it to efficientlycolonize the ciliated epithelium of the upper respira-tory tract and elaborate multiple potent exotoxinsthat initiate local tissue damage and inflammationthat lead to the clinical manifestations.
Pertussis remains a major contributor to morbidi-ty and mortality worldwide, causing an estimated 5million infections and 60,000 deaths each year. It hasreemerged in the United States, with the number ofcases skyrocketing from only 1,000 in 1976 to 9,771in 2002 and topping 11,000 in 2003. The number ofcases in adolescents and adults has increased signifi-cantly (11, 51, 77). Reasons for this dramatic increase
are unclear but may include an increase in the preva-lence of circulating B. pertussis in the general popu-lation and transmission of infection from adults toinfants. Revaccination of older children and adultswith pertussis vaccine is contraindicated because ofside effects, yet immunity wanes about 5 to 10 yearsafter the initial administration of the vaccine (3). Thenewer acellular vaccines used against Bordetella inchildren are being evaluated in adults but are not yetapproved (55).
Traditionally, pertussis has been considered achildhood illness. Classic symptoms of pertussisinclude a catarrhal stage lasting approximately 1 to 2weeks, followed first by a paroxysmal stage lasting 1to 6 to 10 weeks and finally by a convalescent stagewhich can stretch from 2 to 4 weeks to severalmonths. The paroxysmal stage is characterized byfrequent episodes of convulsive coughing, inspirato-ry whoop, and postcough emesis. The symptoms inolder children and adults may be more atypical (espe-cially in previously vaccinated individuals) and areusually milder. In these older patients, paroxysmalcoughing may still be prolonged (often lasting for 1to 6 weeks), but the whooping is present in only 20to 40% of cases and may not be as characteristic asit is in younger children and infants.
Leukocytosis (50,000 WBCs/mm3 with absolutelymphocyte counts greater than 10,000/mm3) is com-monly present in classical pertussis but may be dimin-ished or absent in atypical cases. Posttussive emesisoccurs frequently in pediatric cases but in fewer adultcases. The CDC definition of a clinical case of per-tussis includes “a cough illness of at least two weeksduration, with either paroxysms of coughing, inspi-ratory whoop, or posttussive emesis, and withoutany other apparent cause” (10). The differential diag-nosis may include viral infection, bacterial infections,tuberculosis, and exacerbation of chronic bronchitis,as well as noninfectious causes such as asthma, thepresence of a foreign object, postnasal drip, gastroin-testinal reflux, and malignancy.
Diagnosis
Rapid diagnosis and appropriate therapy of per-tussis may lessen the severity of symptoms to somedegree and can shorten the period of communicabil-ity (10). Diagnosis by culture is recommended by theCDC as isolates are available for in vitro susceptibil-ity testing and molecular typing when clinically orepidemiologically necessary (10). Although highlyspecific, culture may not be as sensitive as serologic ormolecular biology-based tests. Cultures may be leastsensitive in diagnosis of pertussis in older children andadults, especially if these patients have been previous-ly vaccinated. Direct fluorescent-antigen (DFA) test-ing is also available and can be performed rapidly onnasopharyngeal secretions, but due to variability in
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 25

specificity and poor overall sensitivity (30 to 71%), itcannot be used alone to diagnose pertussis (10, 77).
Specimen Collection,Transport, and
Processing for Culture
Preferred specimens include aspirates or swabbedspecimens taken from the posterior nasopharynx(Table 4). Although aspirates may be slightly superi-or to specimens collected by swabbing, they are moredifficult to collect. When appropriately collected,aspirates or swabbed specimens contain ciliatedepithelial cells with which Bordetella is associated.Small-tipped Dacron or calcium alginate flexibleswabs can be used in collecting specimens, and caremust be taken to collect samples from the posteriornasopharynx. Rayon and cotton-tipped swabs areunacceptable. Dacron swabs should be used, sincecalcium alginate swabs may inhibit PCR (77). Swab-bings of throat and anterior nostrils are not accept-able for culture and DFA tests because of thedecreased yield from those sites. However, throatswabs may be adequate for NAATs (77). “Coughplates” are unsatisfactory and are not recommendedbecause of difficulty in appropriate collection and
transportation to the laboratory as well as the poten-tial of cross-infection during the collection process.
Process specimens within 3 h as Bordetella spp. aresusceptible to drying (5, 77). If immediate processingis not possible, the specimens for culture must beplaced in transport medium. Transport media avail-able commercially include Regan-Lowe (RL) enrich-ment medium containing cephalexin, defibrinatedhorse blood and semisolid (half strength) charcoalagar, and nonenrichment media such as CasaminoAcids made of 1% acid-hydrolyzed casein and Amiescharcoal medium. Transport media maintain ade-quate viability for less than 24 h, and specimens mustbe processed within a day of collection (5, 77). Prein-cubation of specimens at 36°C in RL medium withcephalexin, although advocated by some, is not nec-essary and may increase contamination. Transport at4°C maintains better viability than that at ambientroom temperature (77). Only nasopharyngeal speci-mens are acceptable for detection of B. pertussis.Throat swabs, nares swabs, and sputum should notbe processed.
Bacterial Isolation and Reporting Results
Culture remains an important tool in the diagno-sis of pertussis. Its efficacy is, however, influenced bya number of factors, including clinical presentationand age of patient, as well as previous vaccination andantimicrobial therapy.
Specimens can be inoculated per standard micro-biological protocols onto RL medium and/or Bordet-Gengou (BG) agar (potato infusion with 10% glyc-erol and 20% sheep blood) both with and withoutcephalexin added (40�g/ml). The cephalexin-containing selective plates may inhibit a small per-centage of Bordetella spp. and should not be usedalone. The longer shelf life of the RL medium and itsbetter isolation rates favor its use (77). SBA can beinoculated in order to compare presence or absenceof growth.
Incubate plates in a humidified chamber for 7 daysat 35°C (no higher) in ambient air; CO2 should notbe used. In some instances longer incubation may berequired (66). The plates may be examined daily forsmall colonies described as “mercury droplets”because of their mercury-silver color. B. pertussis canbe recognized after 3 to 4 days, and B. parapertussisnormally can be seen within 2 to 3 days. Both specieshave slight zones of beta-hemolysis on BG agar. B.pertussis may be round and domed, and B. paraper-tussis may be grayer and not as domed (Table 5).Viewing colonies with the aid of a magnifying glassmay be helpful. Suspicious colonies can be consid-ered to be Bordetella spp. if they are shown to begram-negative coccobacilli which either agglutinateor fluoresce with appropriate B. pertussis or B. para-
26 Waites et al. CUMITECH 10A
Table 4. Methods for collection of respiratory specimens
in the diagnosis of pertussis
Nasopharyngeal swabsUse only small Dacron or calcium alginate-tipped swabs (not
rayon or cotton) for culture and DFA studies; use onlyDacron swabs (not calcium alginate) for NAATs.
Insert the swab nasally to the posterior nasopharnyx (appro-priate placement is crucial).
Rotate the swab for several seconds and withdraw.It is best to collect a second, similarly manipulated swab
through the other nostril.Swabs should be plated within 3 h or placed into appropriate
transport media.Swabs for NAATs can be submitted in dry form, in saline, or
in transport media.Smears for DFA can be prepared by rolling a swab onto a
glass slide (the clinician may do this at the time of collec-tion, or it may be done in the laboratory after receipt) andair drying.
Nasopharyngeal aspiratesUse a soft narrow catheter or tubing.Insert the instrument intranasally to the back of the
nasopharynx.Using a manual vacuum pump at the other end of the tubing,
suction secretions from the back of the nasopharynx whilewithdrawing the line through the nares.
Capture the secretions in a mucous trap; flush the secretionremaining in the line into the trap using Bordetella trans-port medium or nonbacteriostatic phosphate-bufferedsaline.
The catheter tip may be cut off and placed into transportmedium.
Process secretions for culture within 3 h or place in appropri-ate transport medium.

pertussis antisera. Confirmed clinical isolates or com-mercially obtained strains of both species, as well asnegative controls, should be included when perform-ing serologic identification of colonies. The instruc-tions of the reagents’ manufacturers should alwaysbe followed. Common Bordetella spp. can also bedistinguished from one another by growth patternsand biochemical features (Tables 5 and 6).
Direct Detection
Bordetella spp. do not stain well by routine meth-ods and are difficult to view and recognize in direct-specimen preparations. However, they can be rapidlydetected by commercially available monoclonal orpolyclonal fluorescent-conjugated antibodies. Themonoclonal antibodies (Accu-MAb Plus; QuestPharmaTech Inc., Edmonton, Alberta, Canada) are
available as a dual-fluorochrome reagent that detectsboth B. pertussis and B. parapertussis simultaneous-ly on the same slide. Several manufacturers offer thepolyclonal antibody. Both types of antibody are sim-ilar in sensitivities and specificities. Test methodolo-gies and reagent costs vary among available systems,so laboratories must evaluate these in deciding on thebest products for their setting (77).
The manufacturers’ instructions must be followedin processing and testing of specimens, and appro-priate quality control/quality assurance measuresmust be maintained. Antibody should be titrated(undiluted through a 1:120 dilution) to assess thebest fluorescence before use; control slides consistingof B. pertussis, B. parapertussis, and a negative con-trol should be utilized during each test run. After theinitial review of the test slide at a lower magnifica-tion (�400), the morphology of any fluorescentorganisms should be reviewed with high-poweredobjectives (�1,000 to �1,200). In direct-specimenpreparations, the Bordetella spp. appear as short coc-cobacillary forms showing peripheral fluorescence ofmoderate to strong intensity and dark centers (77).
DFA tests should be performed only in conjunc-tion with culture or NAATs. Results of DFA tests areconsidered presumptive and correlated to clinicalconsiderations as well as to results of other laborato-ry findings. Laboratories that encounter pertussisinfrequently may not have sufficient practical experi-ence with DFAs and should refer them to an appro-priate reference facility. Pertussis is a disease thatrequires notification of authorities. Laboratories needto review the specific reporting requirements of eachlocal and state health authority in order to comply.
AST
Clinical resistance of B. pertussis to the macrolideswas first reported in 1995 (74). Since then, at leastfour additional cases have been documented in theUnited States (8). Nonetheless, routine AST is notrecommended because of the rarity of resistant iso-lates (10). Clinical cases which do not respond to
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 27
Table 5. Morphologies and other characteristics of
Bordetella spp. on isolation media
Medium and species
Description
RL mediumB. pertussis . . . . . .Colonies are tiny, convex, gray, and
smooth with very shiny surfaces (mercury droplets); appear in 3-4 days.
B. parapertussis . . .Colonies resemble those of B. pertussisbut are grayer and less domed; appearmore rapidly than those of B. pertussis.
B. bronchiseptica . .Colonies appear in a day, vary in size, and may have a putrid odor.
BG mediumB. pertussis . . . . . .Colonies are smooth, transparent,
glistening, and convex; small zone ofbeta-hemolysis possible; coloniesappear in 3-4 days.
B. parapertussis . . .Colonies are similar to those of B. pertussis but are larger, duller, or grayer; might be slightly brownish andbeta-hemolytic; appear in 2-3 days.
B. bronchiseptica . .Colonies are tiny with round-pitted surface resembling beaten metal;appear in about 1 day.
Table 6. Diffferential characteristics of the most commonly isolated Bordetella
speciesa
CharacteristicResult for:
B. pertussis B. parapertussis B. bronchiseptica
Growth on blood agar � � �
Growth on MacConkey agar � V (delayed) �
Oxidase positivity � � �
Motility � � �
Urease production � � (24 h) � (4 h)Nitrate reduction � � �
aV, variable reaction; �, positive reaction; �, negative reaction.

appropriate therapy can be screened by in vitrosusceptibility studies. Therapy of active pertussis andprophylaxis of close contacts may minimize transmis-sion (10). Erythromycin remains the antimicrobial ofchoice for therapy and postexposure prophylaxis ofpertussis (10). The newer macrolides, clarithromycinand azithromycin, may also be used (77). SXT is rec-ommended for patients intolerant of the macrolidesor for cases of B. pertussis resistant to macrolides(74). In general, antimicrobials active against B. per-tussis are also active against B. parapertussis (77).
Susceptibility studies have not yet been standard-ized but have been described and evaluated (58). Themost amenable methods for screening for resistancein clinical laboratories capable of performing suchtests include disk diffusion and the Etest (AB Biodisk,Solna, Sweden) using RL agar without cephalexin(58). Resistant strains tested show no zone of inhibi-tion around the erythromycin disk, and Etest-deter-mined MICs for these strains are �256 �g/ml,whereas susceptible strains show zones 43 to 46 mmin diameter and modal MICs for these strains are0.12 �g/ml (58). A susceptible strain of B. pertussisshould be run concurrently with the isolate for qual-ity control. Isolates found to be resistant by screeningcan be submitted to the local health department forconfirmation and epidemiologic evaluation.
Molecular Biology-Based Tests
PCR methods have been described that use a num-ber of gene targets, including the B. pertussis toxingene or its S1 promoter, the adenylate cyclase gene,and the insertion sequence elements, e.g., IS481 in B. pertussis and IS1001 in B. parapertussis. PCRincreases diagnostic yields significantly, and resultsshow a high level of agreement with those of sero-logic studies (43). PCR has a higher recovery ratethan culture in patients who present with atypicaldisease manifestations (e.g., older patients or thosewith a history of vaccination) and can continue todetect organisms for longer periods of time than cul-ture during pertussis, even after initiation of therapy.Sensitivities of PCR as well as culture decrease withevolution of the disease process.
Methods for PCR have not been standardized andrequire validation against culture in individual labo-ratories. False-positive results can occur due to con-tamination in the laboratory or during specimen col-lection (10). False-negative results can also occurbecause of inhibitory substances in respiratory secre-tions. Both problems can be minimized by takingappropriate quality control steps in the processingand testing of specimens.
Molecular biology-based NAATs for pertussis arepresently recommended as adjunct tests with cultureand isolation of the etiologic agent as recommended
by the CDC. However, real-time PCR technologynow allows rapid screening for B. pertussis, with thecapability for same-day results, and may replace thefar less sensitive DFA or even culture in the future.
Serology
Assays available for serological evaluations includeEIAs, the complement fixation test, immunoblotting,agglutination, indirect hemagglutination, and toxinneutralization (77). EIAs are the most commonlyused. Levels of IgA, IgG, and IgM against a numberof Bordetella antigens can be measured. A four-foldrise in the level of IgG against the pertussis toxin isthe most specific indicator of B. pertussis infection.
Although serologic studies have been shown to beuseful in some clinical situations, they are nonstan-dardized and difficult to interpret and should not beroutinely relied upon for diagnosis and confirmationof pertussis (10, 77). The CDC recommends thatcases that are culture and PCR negative but serolog-ically positive and that fit the clinical definition ofpertussis be considered as “probable” cases. Individ-ual laboratories that require more information onserologic diagnosis in specific cases can consult theirstate health departments for guidance.
Diphtheria
Diphtheria presents as an acute pseudomembranouspharyngitis caused by toxigenic or nontoxigenicstrains of C. diphtheriae, a pleomorphic gram-posi-tive rod. Transmission occurs by contact with air-borne respiratory droplets from infected individualsor contact with exudate from infected skin lesions.Disease is produced when the C. diphtheriae exotox-in disrupts protein synthesis in the targeted cells ofthe respiratory mucosa, causing cell necrosis andsloughing and resulting in pseudomembrane forma-tion. Cutaneous diphtheria, consisting of nonspecificsore-like wounds and ulcers, can also occur but isnormally mild with few systemic complications. Itcan, however, become blood-borne. Myocarditis,neuritis, and less commonly nephritis may be com-plications of severe disease with toxigenic strains.Although diphtheria has had resurgence in Europe inrecent years and remains endemic in developingcountries, cases in the United States are a rarity butcan happen on occasion in unimmunized or under-immunized individuals. Zero to five respiratory casesare reported annually, with an overall rate of 0.001cases per 100,000 people since 1980.
Manifestations of diphtheria include nonspecificsigns such as pharyngitis, low-grade fever, and cervi-cal lymphadenopathy. More indicative clinical signssuch as systemic toxicity, stridor, paralysis of thepalate, and a unilateral discharge of serosanguinousnasal fluid are often present in more severe cases.
28 Waites et al. CUMITECH 10A

Characteristic gray pseudomembranes are formedadherent to the pharyngeal, palatal, or nasal mucosa;these pseudomembranes are difficult to dislodge, andthe mucosa to which they are attached may bleedupon attempts at removal.
Diagnosis
A presumptive diagnosis can be made based onclinical symptoms and presentation. The laboratoryshould be alerted when diphtheria is suspected. Con-firmation of diphtheria is achieved through isolationof the etiologic agent, with further strain biotypingand toxigenicity studies using the Elek technique (atoxin-antitoxin test) performed by reference labora-tories, state health laboratories, or the CDC.
Because diphtheria is extremely rare in the UnitedStates, most laboratories have neither the expertisenor the resources to isolate and identify C. diphtheri-ae. However, laboratories should have a process orprocedure in place to obtain immediate help andguidance from the local state health department andthe CDC. Since diphtheria is a reportable disease withimportant public health significance, local healthdepartments usually want to be notified by telephonewhen a case is suspected and want to becomeinvolved as rapidly as possible. They can provide thenecessary transport or plating media and informa-tion as to how best to proceed to confirm the diag-nosis. Additional information and consultative ser-vices can be accessed through individual state healthdepartment websites or the CDC website at http://www.cdc.gov.
Specimen Collection,Transport, and
Processing for Culture
Cotton- or polyester-tipped swabs are used to col-lect exudate from multiple sites, including the naso-pharynx and pharynx, for best recovery of the agent.Material swabbed from underneath the pseudomem-branes and pieces of pseudomembrane can be sub-mitted in conjunction with the exudate. Culturesshould be collected from patients with suspected cases and from their close contacts (nasopharyngealand pharyngeal swabs in the latter case). Specimensshould be processed and cultured as soon as possibleor be submitted in semisolid transport medium suchas Amies gel.
Directions provided by the state health laborato-ries should be followed for collection, submission,and/or workup of specimens. In general, specimensare plated onto a selective medium such as cystine-tellurite blood agar or fresh Tinsdale medium as wellas onto SBA. Dehydrated swabs in silica gel addi-tionally require an initial overnight incubation inbroth medium supplemented with plasma or bloodprior to subculture on the primary media listedabove. Although C. diphtheriae isolates produce cel-
lular polar bodies when grown on nonselective Loef-fler agar slants, these are not recommended for pri-mary isolation because of bacterial overgrowth.Plates are incubated at 25 to 27°C in an atmospherecontaining 5% CO2 prior to a first reading. Tinsdaleagar must be less than 4 weeks old and supplementedwith horse serum but affords the best medium forisolation of C. diphtheriae. C. diphtheriae coloniesare black (indicating tellurite reductase activity) witha brown halo around them (indicating cystinase activ-ity). Tellurite is not specific for C. diphtheriae andcannot be used to differentiate it from other coryne-bacteria based on phenotypic growth characteristics.It may even inhibit some strains of C. diphtheriae.Colistin-nalidixic acid blood agar plates can be usedif cystine-tellurite blood agar and Tinsdale mediumare not available.
Bacterial Identification and Reporting Results
The diagnosis of diphtheria can be supported bymicroscopic evidence of many gram-positive rods dis-tributed in what looks like “Chinese letters” uponGram staining of material collected from the involvedpharyngeal and nasal mucosae. C. diphtheriae can besuspected by its colony growth patterns and pigmentproduction on various media as noted above. Isolatescan be identified by some commercial systems such asthe API Coryne system (bioMérieux) (45). However,isolates suspected of being C. diphtheriae that arecystinase positive on Tinsdale agar and pyrazinami-dase negative should be submitted to the local statehealth department for confirmation of identity andfor biotyping and toxigenicity studies where needed.These studies are performed by only a few labora-tories and are described in detail elsewhere (44).
Molecular Biology-Based Methods
Molecular amplification techniques for detectionof both C. diphtheriae and diphtheria toxin have beendescribed, but no commercially available kits andreagents exist. The CDC has a PCR assay for detec-tion of the C. diphtheriae toxin production regulato-ry gene (dtxR) and the diphtheria toxin gene (tox)directly in clinical specimens (92). Additional clinicalspecimens (e.g., swabs, tissue specimens, and piecesof pseudomembrane) can be collected and submittedthrough state health departments to the CDC.
AST
Therapy must be initiated promptly to decreasemortality. The therapeutic approach includes admin-istration of an antitoxin obtainable from the CDCand of antimicrobial agents such as erythromycin andpenicillin. Patients with suspected cases and closecontacts of patients should receive antimicrobialagents for therapy and prophylaxis. AST is not rou-tinely performed.
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 29

Serology
Serological testing is available through only a fewlaboratories and is too slow in turnaround time to beof much help in initiation of therapy. The presence oflow levels of antibody does not rule out diphtheria,whereas serious disease is less likely to occur inpatients with high levels of antibody induced by vac-cination. The state health departments and CDCshould be contacted for further consultation andinterpretation of results.
Pharyngeal and Peritonsillar Abscesses
Peritonsillar abscess or “quinsy” can be a local com-plication of pharyngitis in children, but it can alsooccur in persons of any age and can develop withoutany preceding history of tonsillitis (23). The diagno-sis of peritonsillar, lateral pharyngeal, and retro-pharyngeal abscesses is based primarily on historyand physical examination. Patients usually presentwith a sore throat, lethargy, fever, poor oral intake,difficulty breathing, dysphagia, odynophagia, otal-gia, and inability to swallow. They usually have ten-der cervical lymph nodes. The examination of thepharynx often reveals a unilateral or occasionallybilateral erythematous bulging soft palate that is ten-der to palpation. This soft tissue mass may displacethe uvula to the contralateral side, and there mayalso be significant edema of the soft palate, uvula,and pharyngeal walls.
Etiology
Most oropharyngeal abscesses are the result ofpolymicrobial infections. Predominant anaerobes arePrevotella, Porphyromonas, Fusobacterium, and Pep-tostreptococcus spp. Aerobic organisms are mainly S.pyogenes, S. aureus, and H. influenzae. Anaerobicbacteria can be isolated from most abscesses when-ever appropriate techniques for their cultivation havebeen used.
Diagnosis
Confirmation of the microbiological causes of pha-ryngeal abscesses can be made with needle aspirationand drainage, which is also important therapeutical-ly. Obtaining appropriate specimens for culturesfrom pharyngeal abscesses is important, as a varietyof organisms can be recovered.
Specimen Collection,Transport, and
Processing for Culture
Specimens are best collected through surgicaldrainage or needle aspiration. Attempting to obtaincultures after an abscess has been drained makes con-tamination with normal flora unrelated to the ab-scess more likely. Abscess material should be inocu-lated into an anaerobe transport system at the time of
collection. Maintain the specimen at room tempera-ture until it can be processed for culture. Gram stain-ing should be performed, and the results should becorrelated with the presence of microorganismsgrown in culture. SBA, MacConkey, chocolate, andcolistin-nalidixic acid blood agars and brain heartinfusion broth are inoculated for isolation of aerobicand facultative bacteria. The basic anaerobic mediaas described in previous sections should also be inoc-ulated by pipetting a drop of abscess fluid onto eachagar plate and making a 1:10 dilution in broths.Anaerobic plates are incubated under appropriateanaerobic conditions according to laboratory policies.MacConkey agar plates are incubated at 35 to 37°Cin room air, and the remaining plates are incubatedin air with 5% CO2. Additional procedures for pro-cessing of cultures for staphylococci, streptococci, H.influenzae, and anaerobes have been described inprevious sections.
Bacterial Identification and Reporting Results
Numbers of bacteria and types of morphologiesalong with the Gram stain reaction and the presenceand approximate quantities of WBCs are evaluated.Attention should be given to identification of likelypathogens such as S. pyogenes, S. aureus, and H.influenzae and various anaerobes by using tech-niques described in earlier sections. In the case ofpolymicrobial infections in which no organism is pre-dominant, limit identification to no more than thethree most common organisms. The names of pre-dominant organisms, in addition to a report of“mixed flora,” when appropriate, are sufficient.
AST
The isolation of aerobic and anaerobic �-lacta-mase-producing bacteria from most abscesses man-dates the use of antimicrobial agents effective againstthese organisms. AST should be performed on pre-dominant pathogens, such as S. aureus, when suchpathogens are present, and �-lactamase tests shouldbe performed on H. influenzae. Susceptibility testingof streptococci and anaerobes is not done unlessspecifically requested. If gram-negative bacilli are de-tected, perform AST on predominant organisms.
Lemierre’s Disease
Lemierre’s disease is an uncommon fulminant condi-tion primarily affecting young adults that is charac-terized by primary oropharyngeal infection, bacter-emia, thrombosis of the internal jugular vein, andmetastatic abscesses resulting from septic emboli inthe lungs, liver, joints, and other sites. The typicalpresentation is a patient with high fever, lateral neckpain, and swelling. Usually, these symptoms occurafter the symptoms of pharyngitis subside. The infec-tion can also produce renal disease which mimics
30 Waites et al. CUMITECH 10A

post-streptococcal glomerulonephritis (25). Themajority of cases of Lemierre’s disease are caused byFusobacterium necrophorum, a gram-negative, obli-gate anaerobic bacterium, but some are polymicro-bial, involving other anerobes as well as facultativeorganisms such as A. haemolyticum and streptococci(130). F. necrophorum is part of the normal oropha-ryngeal flora in many people and is peculiar in itsability to cause invasive disease without the presenceof serious underlying comorbid conditions. Diagno-sis is based mainly on a history of oropharyngealinfection, clinical or radiographic evidence of throm-bophlebitis of the internal jugular vein, and isolationof the etiologic agent (65). A recent study using PCRfound F. necrophorum in 10 (10%) of 100 throatswabs from patients with pharyngitis and none ofthose from 100 healthy controls. Eight of 10 speci-mens were PCR positive for F. necrophorum in theabsence of beta-hemolytic streptococci, suggestingthat this organism may be a more common causeof pharyngitis than previously thought. However,viruses and other bacteria that might be responsiblefor pharyngitis were not sought (1).
Diagnosis
Anaerobic culture of throat specimens is not usu-ally performed, so clinicians must notify the labora-tory if F. necrophorum infection is suspected so thatproper procedures can be implemented. The choiceof specimen for culture of F. necrophorum may differfrom the type used for detection of DNA. PCR is notavailable in a commercial product approved for diag-nostic use.
Specimen Collection,Transport, and
Processing for Culture
Material collected from the throat for culture canbe placed in an appropriate anaerobe transport medi-um such as a Port-A-Cul (Becton Dickinson). Aspira-tion of abscess fluid provides the best specimen.Depending on the state of disease at the time of pres-entation, blood cultures may also be desirable. Swabsare the least desirable specimens for isolation ofanaerobic bacteria, but they are acceptable for pro-cessing for detection of S. pyogenes and Arcanobac-terium spp. which may also be associated with thiscondition. Specimens should not be refrigerated. Inoc-ulation of anaerobe cultures can be done as describedfor otitis media, and cultures should be incubated at35°C under anaerobic conditions.
Bacterial Identification and Reporting Results
Isolation of Fusobacterium spp. is facilitated byusing neomycin-vancomycin agar or Fusobacteriumselective agar (63). Colonies are umbonate and mayproduce greening of the agar. Hold plates for 5 to 7
days before reporting lack of growth. F. necrophorumis vancomycin resistant and colistin and kanamycinsensitive when tested with high-potency disks. It isindole positive and nitrate negative; F. necrophorumsubsp. necrophorum is lipase positive, is often bilesensitive, and fluoresces chartreuse. F. necrophorumsubsp. funduliforme is lipase negative. Fusobacteriumspp. can be identified with a variety of the commer-cial identification panels using chromogenic and/orfluorogenic substrates for constitutive enzymes. Onmicroscopic examination, F. necrophorum isolatesare pleomorphic with long rods and rounded ends.Other anaerobes of clinical importance can be identi-fied according to procedures described in referencetexts (e.g., reference 63). Methods for isolation andidentification of S. pyogenes and Arcanobacteriumspp. have been described earlier. Predominantpathogens including the above organisms should bereported. There is no need to work up more thanthree different species present simultaneously.
AST
AST may sometimes be needed for F. necro-phorum to direct therapy. Up to several weeks of ag-gressive intravenous antimicrobial therapy utilizingbroad-spectrum agents known to cover anaerobes, incombination with surgical drainage of abscesses, maybe necessary.
Vincent’s Angina
Vincent’s angina, also known as “trench mouth” dueto the accompanying halitosis, is an ulcerative,necrotizing gingivitis. It is caused by an overgrowthof a combination of bacterial species usually found aspart of the normal flora within the gingival crevicesand is associated with patients who have poor denti-tion and oral hygiene. A sore throat, with ulcerationof the pharynx and the presence of a thin, grayish-yellow pseudomembrane, may also accompany theprocess. Borrelia vincenti and Fusobacterium spp.have frequently been associated with the infection(5). Diagnosis is usually based on clinical presenta-tion and physical exam. Culture of the purulent exu-date is unnecessary and not indicated. Gram staining(or one of its modifications enhancing visualizationof anaerobic microorganisms) of the material canconfirm the diagnosis by revealing mixed microor-ganisms with the presence of numerous characteristicspirochetes and fusobacteria. A staining procedureusing Ziehl-Neelsen stain diluted with 10 to 15 vol-umes of water and applied to the smear for 15 to 30 shas been described to enhance visualization of thespirochetes (5). Collection of blood cultures is indi-cated in cases of severe disease with possible sepsis ormetastasis to other organ systems.
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 31

CANDIDIASIS
The genus Candida comprises as many as 200 species,but only a small number of them are involved inhuman disease and may be the cause of oropharyn-geal candidiasis (OPC). The most common is C. albi-cans (causing 80 to 90% of cases) (31), followed byC. tropicalis, C. parapsilosis, and C. glabrata (91).Acute pseudomembranous candidiasis, also knownas “thrush,” is characterized by white pseudomem-branes consisting of hyphae, pseudohyphae, blasto-spores, epithelial cells, and fibrin. These white patchesoccur on the lips, hard and soft palate, tongue, buccalmucosa, and oropharynx. Predisposing factors forOPC include extremes of age, diabetes mellitus, im-munosuppression secondary to HIV infection, malig-nancy, treatment with antibacterial drugs, and use ofsteroid inhalers. Rare complications such as isolatednecrotizing epiglottitis have also been reported (105).Some cases of apparent OPC, particularly in neu-tropenic patients, may have other causes, includingherpes simplex virus and mixed oral bacterial flora.This underscores the need to examine material fromoral lesions microscopically.
Diagnosis
The gross appearance of typical oral lesions andmicroscopic findings are usually sufficient for diag-nosis of OPC. Fungal culture may not be necessaryunless the condition is chronic or therapeutic failurehas occurred, indicating the need for antifungal sus-ceptibility testing.
Specimen Collection,Transport, and
Processing for Culture
Exudative material from the pharynx collected ona swab should be examined microscopically in a wetmount by using the Gram stain, calcofluor white, ora KOH preparation (5).
Candida infections of the oral cavity are usuallyvisible to the naked eye and can be sampled using aswab which is then immersed in an appropriatetransport system such as Amies gel to prevent desic-cation. If a smear is to be examined, it is optimum tocollect a second swab in addition to the one used forculture. Specimens should be transported to the lab-oratory within 2 h. If a longer delay is anticipated,refrigerate specimens at 4°C until processing to min-imize the overgrowth of contaminating bacteria.
Candida Identification and Reporting Results
The presence of blastospores and pseudo- and/ortrue hyphae in smears from infected lesions is diag-nostic of OPC without specifically identifying thespecies by culture. The exception is C. glabrata, whichdoes not form hyphae or pseudohyphae and whichappears as yeasts. Most Candida spp. grow on SBA,chocolate agar, and MacConkey or eosin-methyleneblue agar. Colonies usually become apparent after
overnight incubation on noninhibitory media but takelonger on inhibitory media. An exception is C.glabrata, which may not grow on media containingsheep blood. Special media such as inhibitory moldagar containing gentamicin and chloramphenicol maybe necessary to detect yeasts that might otherwise beovergrown by oropharyngeal bacteria. Many proto-cols for performing fungal cultures on nonsterile sitesinclude media such as Sabouraud dextrose agar con-taining cycloheximide. However, some clinicallyimportant yeasts, e.g., Cryptococcus neoformans, C.glabrata, Candida krusei, and Candida lusitaniae,are inhibited in the presence of cycloheximide. Thischaracteristic can be used in an identificationscheme. However, cycloheximide-containing mediashould not be used exclusively for primary isolation.Inoculation of media such as CHROMagar (BectonDickinson) allows visual differentiation and pre-sumptive identification of C. albicans, C. tropicalis,and C. krusei based on their utilization of propri-etary chromogenic substrates incorporated into theagar after 48 h of incubation.
Candida spp. do not require a special atmosphereand tolerate a wide range of incubation temperatures,including room temperature and 30 and 37°C. Thereare a variety of methods available for the identifica-tion of single species. Examples are the rapid germtube test, which provides presumptive identificationof C. albicans, and the rapid trehalose assimilationtest for C. glabrata. Multiple genera can be identifiedbiochemically by using commercial products such asAPI 20C AUX (bioMérieux). Most of these systemsare unable to reliably distinguish Candida dublinien-sis from C. albicans (54).
Candida spp. are members of the normal micro-bial flora of the oral cavity, and therefore, isolatingCandida in the absence of any clinical signs of infec-tion is without value. A positive culture should beconsidered in addition to evidence of numerous blas-tospores and pseudo- and/or true hyphae on a directsmear and in the context of the clinical conditionwhich prompted performance of the culture.
AST
Initial therapy of OPC usually involves topicalantifungal agents such as nystatin. Refractory andmore severe cases may require oral or intravenoussystemic agents such as the azoles. AST is rarely nec-essary but may be performed in instances when treat-ment with first-line agents is not successful.
ZYGOMYCOSES
The class Zygomycetes includes two orders withhuman pathogens, the Mucorales, comprising themost common agents, and the Entomophthorales.Among the Mucorales, members of the genera Rhi-
32 Waites et al. CUMITECH 10A

zopus, Mucor, Absidia, Rhizomucor, and Apophy-somyces have all been implicated in human disease,with Rhizopus spp. being the most common. Thegenera Conidiobolus and Basidiobolus are membersof the Entomophthorales, and they have also beenidentified as human pathogens (49). The term “mu-cormycosis” correctly refers only to infections causedby members of the Mucorales but has been usedextensively in the literature to refer to an infectioncaused by any of the Zygomycetes. Although taxo-nomically incorrect and often misinterpreted as iden-tifying the etiologic agent as a Mucor sp., it is soingrained in the medical literature that it is frequent-ly used interchangeably with zygomycosis.
Disease ensues when airborne spores of the zygo-mycetes are inhaled into the nose, the pharynx, andthe lungs. The fungi invade tissues of the nose andspread to the paranasal sinuses, orbit, eye, cavernoussinuses, and brain sequentially. Pyogenic inflamma-tion, angioinvasion, tissue infarction, and widespreadnecrosis lead to clinical manifestations consistingprogressively of dark blood-tinged nasal discharge,headache, fever, ocular pain and swelling, proptosis,decreased visual acuity, cranial nerve palsies, seizures,and eventually death in as many as 80% of cases.Physical examination may reveal blackened nasalturbinates and a necrotic eschar on the palate. Organ-isms such as Rhizopus spp. grow best at an acidic pHin a high-glucose-concentration environment, hencethe strong association between persons with diabeticketoacidosis and invasive zygomycosis. Other hostrisk factors include neutropenia, sustained immuno-suppressive therapy, chronic prednisone use, ironchelation therapy, broad-spectrum antibiotic use,severe malnutrition, and primary breakdown in theintegrity of the cutaneous barrier such as that causedby trauma, surgical wounds, needle sticks, or burns(97).
Diagnosis
Establishing the diagnosis of mold infection causedby one of the zygomycetes relies on demonstratinghistopathologic evidence of fungal elements and/orisolating the organism in culture from the involvedtissue.
Specimen Collection,Transport, and
Processing for Culture
The laboratory should receive biopsy material col-lected from areas with evidence of tissue necrosis.Material from black necrotic eschars either in thenasopharynx or on the palate is most productive, butit is desirable to make the diagnosis earlier by inves-tigating the cause of sinusitis by fine needle aspirationor curettage of the involved sinus. Material should besent to the laboratory as quickly as possible in a ster-ile screw-cap container. Addition of a small volumeof nonbacteriostatic saline at the time of collection
helps prevent desiccation if tissue samples are small.Swabs of the nares are inappropriate since spores ofthese organisms are ubiquitous and isolation withoutevidence of tissue invasion cannot differentiate colo-nization from infection.
Specimen storage and processing require specialattention in order to maximize the yield of positivecultures. Inoculate fungal growth media as soon aspossible. Maintain biopsy material at room tempera-ture until processing. Homogenizing tissue may resultin a reduction in viability. The preferred method is tomince tissue and place it directly onto primary isola-tion plates.
Fungal Identification and Reporting Results
Culture is the most definitive diagnostic test, andwhen isolated these organisms can be challenging toidentify. They grow well on glucose-peptone agars(e.g., Sabouraud agar) with or without antibacterialagents (e.g., inhibitory mold agar) incubated at 30°C.Cycloheximide should not be used in selective mediasince it inhibits these organisms. Zygomycetes growrapidly and may sometimes be encountered on rou-tine bacteriology cultures, although this cannot berelied upon since they may be overgrown or sup-pressed by the competing bacterial flora. Once iso-lated, they rapidly expand to cover the plate andexhibit an erect aerial mycelium which is cottoncandy-like and may extend to the lid of the agar plate.Thus, they are commonly referred to as lid lifters.Though most zygomycetes grow in 1 to 7 days, fun-gal cultures are held for at least 30 days before beingdesignated negative for any clinically significant fun-gal pathogens. Excellent resources are available foridentifying isolates based on colony growth appear-ance and microscopic morphologic features (97, 98).Due to the possibility of aerosolized fungal elements,plates must be sealed with tape during incubationand manipulated in an appropriate class 2 biologicalsafety cabinet.
Unfortunately, cultures are often negative evenwhen processed with ideal procedures and in the faceof clear histopathologic findings. Therefore, it is oftennecessary to establish a diagnosis based solely upontissue examination. Zygomycetes can be seen onhematoxylin-eosin-, Grocott methenamine silver-,and periodic acid-Schiff-stained sections when exam-ined under high-power and oil immersion microscopeobjectives. The major distinction to be made is fromother hyaline molds such as Aspergillus spp., Fusari-um spp., and Pseudallescheria boydii. Wet prepara-tions of minced tissue or sinus aspirates can be exam-ined using calcofluor white or KOH for optimumdetection and visualization of fungal hyphae. Themajor histologic findings are hyaline, broad, irregu-larly branching hyphae which have few if any septa-tions. Detailed descriptions and illustrations of
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 33

individual zygomycete species can be found in manypublications (e.g., references 97 and 98).
Presumptive isolation of any zygomycete in theproper clinical setting is considered a critical labora-tory value and must be reported immediately. Speciesidentification may take several days or even weeks ifspecimens are sent to a reference laboratory, so it iscritical that clinicians receive a preliminary reportindicating the presence of a zygomycete. The identifi-cation of the genus and species does not significantlyinfluence the therapy but should follow when avail-able. However, the finding of a culture positive for azygomycete in the absence of either clinical suspicionor tissue invasion must be interpreted with caution.
AST
AST methods published by the CLSI for filamen-tous fungi have been used to provide in vitro MICsfor zygomycetes to evaluate activities of some ofthe newer azole drugs in an attempt to improveunderstanding of potential treatment alternatives(109). Aggressive treatment with systemic antifungalagents is an important part of overall management inaddition to surgical debridement of infected and ne-crotic tissues, but mortality remains extremely high,nonetheless.
NASAL SCREENING FOR MRSA CARRIERS
MRSA is increasing in frequency in hospitals to thepoint that more than 50% of all S. aureus isolatesfrom inpatients have this characteristic in many insti-tutions (125). Due to the propensity for endemicclones of MRSA to spread from patient to patient, itis valuable to know which persons are colonized sothat they can be placed into contact isolation, eventhough they may not manifest evidence of active dis-ease. Hospital infection control officers may chooseto perform screening cultures for high-risk patientsand/or those cared for in locations with high rates ofMRSA infections, such as intensive care units. Col-lection of nasal swabs is the most commonly usedmeans for detection of MRSA carriage since the ante-rior nares are the most frequent site of colonization(60).
A calcium alginate swab, previously moistenedwith nonbacteriostatic sterile saline, is carefully in-serted a short distance into each nostril and gentlyrotated for 5 s. The swab is then inserted into a trans-port medium such as Amies gel immediately after thesample is obtained. Specimens can be transported atroom temperature and tested within 24 h after col-lection. For the identification of MRSA, the swabscan be streaked directly onto 1% mannitol salt agarselective for growth of staphylococci. Plates areexamined after 1 and 2 days of incubation for typi-
cal S. aureus colonies surrounded by a yellow zoneindicative of acid production from mannitol. Pre-sumptive identification of S. aureus can be accom-plished by demonstration of catalase production anda positive coagulase test. Growth of subcultures onoxacillin salt agar can be used to confirm the pres-ence of MRSA.
Drawbacks of traditional culture-based methodsfor MRSA screening are related to the labor-intensivenature of culture and the fact that it may require72 h or more from the time of collection until resultsare available for use in determining whether patientsshould be isolated. An alternative method is to iden-tify growth of S. aureus as MRSA by demonstratingthe presence of altered penicillin binding proteinPBP2a by using the Oxoid PBP2a latex test (RemelLaboratories), which detects the product of the mecAgene. This method still requires primary cultivationof the bacteria from the original specimen but avoidsan overnight incubation required for performance ofa conventional susceptibility test after pure culturesof S. aureus are isolated. An assay for detection ofthe mecA gene directly in clinical isolates (Velogene),using an EIA-based format, was sold briefly in theUnited States, but the product was discontinued oncethe simpler and quicker PBP2a latex test becameavailable. Even though detection of mecA is the ref-erence standard for identifying MRSA (29), no com-mercial products are currently available for this pur-pose in the United States and most hospital-basedlaboratories do not have sufficient resources and tech-nology to develop and adapt internal PCR assays forclinical application.
BBL CHROMagar MRSA (Becton Dickinson) canbe used as a selective medium for direct inoculationof nasal specimens to be screened for MRSA. Devel-opment of mauve colonies after 24 h is sufficient forreporting MRSA. Mauve colonies that develop after48 h of incubation should be tested with coagulaseto confirm that they are S. aureus. Despite initialincreased costs for the special media containingchromogenic substrates, this method has the advan-tages of allowing a shortened turnaround time andsignificantly reducing technologist time for handlingspecimens and reporting results. Use of CHROMagarMRSA is most cost-effective for laboratories thatperform a large number of MRSA screening culturesbut may not be practical for smaller laboratories.
APPENDIX
CODING AND REIMBURSEMENT ISSUES
CPT-4 CODES
Correct selection of Current Procedural Terminology (CPT)codes (2a) for upper respiratory tract laboratory diagnosticprocedures ensures appropriate reimbursement for testing
34 Waites et al. CUMITECH 10A

performed as well as documentation of the workload forprocedures performed. All regulations and guidelines thatgovern correct coding should be followed. For specimencollection, a specific code exists for venipuncture to obtainserum for serologic procedures but not for collection ofother upper respiratory tract specimen types. Most of thesenonvenipuncture specimen collection procedures are as-sumed to be included in the physician payment for officeservices, so there is little incentive for microbiology per-sonnel to assume this responsibility. For procedural coding,the general rule for selection of a code is to identify thecode that best describes the procedure based on the fol-lowing, in order of priority: specific analyte, specific
method, and generic procedure. As a last resort, an unlist-ed code may be used. Note that for infectious disease diag-nostics, many non-culture-dependent codes are both ana-lyte and method specific (e.g., RADTs using OIAs for GAShave a specific CPT code, 87880). It is appropriate todevelop reflex and composite code sets when justified byregulatory standards and accreditory guidelines or by pub-lished literature as long as all compliance conditions out-lined by the Office of the Inspector General for ClinicalLaboratories are met (91a). Table A1 provides an overviewof codes or code series applicable to the procedures usedfor diagnosis of specific upper respiratory tract infectionsas described in this Cumitech. Coding is provided only for
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 35
Table A1. CPT-4 coding guidance for laboratory diagnosis of upper respiratory tract infectionsa
Infection(s) or CPT-4 diagnostic objective
Test procedure(s)codeb Coding issue(s)
Streptococcal pharyngitis GAS culture with presumptive identification 87081 May reflex to bacterial isolate identification of isolatesc and antimicrobial susceptibility codes
(see below).c
RADT for GAS with direct specimen 87880d Follow manufacturer recommendations for antigen detection by OIA coding RADTs; for waived POLe tests,
use modifier -QW.RADT for GAS with direct specimen antigen 87430d
detection by EIADirect probe 87650d
Amplified probe 87651d
Serology for streptozyme 86403 For waived POL tests, use modifier -QW; may reflex positives to titer code, 86406.
Serology for ASOf, screening 86063 May reflex positives to titer code, 87060.Serology for anti-DNAase 86215
Bacterial pharyngitis Miscellaneous aerobic isolate throat culture 87070 If primary plates are incubated anaero-with presumptive identification of isolates bically, use 87075; may reflex to bacterial
isolate identification and antimicrobialsusceptibility codes (see below).
Gonococcal pharyngitis N. gonorrhoeae culture 87081 May reflex to bacterial isolate identification and antimicrobial susceptibility codes(see below).
N. gonorrhoeae amplified probe 87591M. pneumoniae infection Mycoplasma culturec 87109 Additional coding guidance may be found in
Cumitech 34 (122).M. pneumoniae amplified probe 87581Mycoplasma serology 86738 Used once per acute-phase and
convalescent-phase sample and per antibody type (e.g., IgG and IgM).
Chlamydophila sp. Chlamydia culture plus culture 87110 �infections confirmation by fluorescent- 87140 Used per antiserum.
antibody stainingC. pneumoniae amplified probe 87486C. psittaci amplified probe 87798 Infectious agent not otherwise specified.Chlamydia serology, IgG 86631 Used once per acute-phase and
convalescent-phase sample.Chlamydia serology, IgM 86632
Laryngeal syndromes Specific bacterial pathogen culture with 87102 May reflex to fungal identification and presumptive identification of isolates antimicrobial susceptibility codes (see
below).Acid-fast bacillus culture with presumptive 87116 May reflex to acid-fast bacillus identification
identification of isolates and antimicrobial susceptibility codes(see below); if concentration performed,add 87015.
(Table continues)
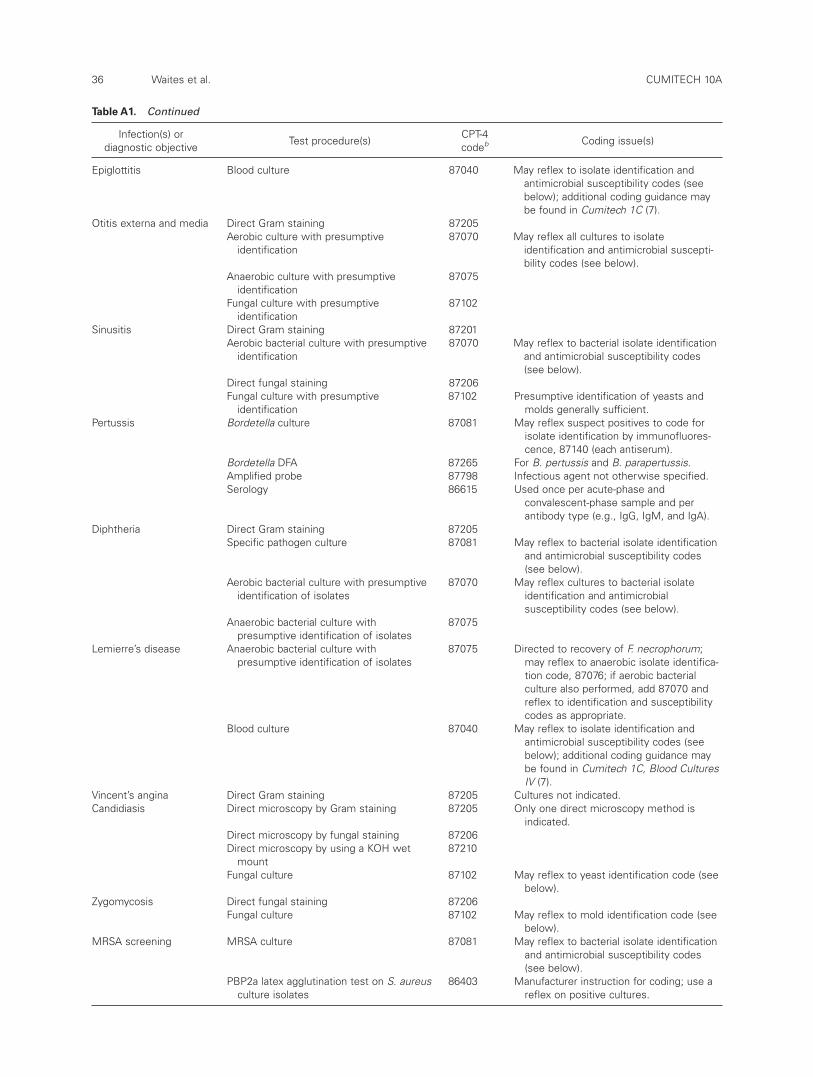
36 Waites et al. CUMITECH 10A
Table A1. Continued
Infection(s) or CPT-4 diagnostic objective
Test procedure(s)codeb Coding issue(s)
Epiglottitis Blood culture 87040 May reflex to isolate identification and antimicrobial susceptibility codes (seebelow); additional coding guidance maybe found in Cumitech 1C (7).
Otitis externa and media Direct Gram staining 87205Aerobic culture with presumptive 87070 May reflex all cultures to isolate
identification identification and antimicrobial suscepti-bility codes (see below).
Anaerobic culture with presumptive 87075identification
Fungal culture with presumptive 87102identification
Sinusitis Direct Gram staining 87201Aerobic bacterial culture with presumptive 87070 May reflex to bacterial isolate identification
identification and antimicrobial susceptibility codes(see below).
Direct fungal staining 87206Fungal culture with presumptive 87102 Presumptive identification of yeasts and
identification molds generally sufficient.Pertussis Bordetella culture 87081 May reflex suspect positives to code for
isolate identification by immunofluores-cence, 87140 (each antiserum).
Bordetella DFA 87265 For B. pertussis and B. parapertussis.Amplified probe 87798 Infectious agent not otherwise specified.Serology 86615 Used once per acute-phase and
convalescent-phase sample and per antibody type (e.g., IgG, IgM, and IgA).
Diphtheria Direct Gram staining 87205Specific pathogen culture 87081 May reflex to bacterial isolate identification
and antimicrobial susceptibility codes(see below).
Aerobic bacterial culture with presumptive 87070 May reflex cultures to bacterial isolate identification of isolates identification and antimicrobial
susceptibility codes (see below).Anaerobic bacterial culture with 87075
presumptive identification of isolatesLemierre’s disease Anaerobic bacterial culture with 87075 Directed to recovery of F. necrophorum;
presumptive identification of isolates may reflex to anaerobic isolate identifica-tion code, 87076; if aerobic bacterial culture also performed, add 87070 andreflex to identification and susceptibilitycodes as appropriate.
Blood culture 87040 May reflex to isolate identification and antimicrobial susceptibility codes (seebelow); additional coding guidance may be found in Cumitech 1C, Blood CulturesIV (7).
Vincent’s angina Direct Gram staining 87205 Cultures not indicated.Candidiasis Direct microscopy by Gram staining 87205 Only one direct microscopy method is
indicated.Direct microscopy by fungal staining 87206Direct microscopy by using a KOH wet 87210
mountFungal culture 87102 May reflex to yeast identification code (see
below).Zygomycosis Direct fungal staining 87206
Fungal culture 87102 May reflex to mold identification code (see below).
MRSA screening MRSA culture 87081 May reflex to bacterial isolate identification and antimicrobial susceptibility codes(see below).
PBP2a latex agglutination test on S. aureus 86403 Manufacturer instruction for coding; use a culture isolates reflex on positive cultures.

CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 37
Table A1. Continued
Infection(s) or CPT-4 diagnostic objective
Test procedure(s)codeb Coding issue(s)
Amplified probe 87798 Infectious agent not otherwise specified.Bacterial identificationc Presumptive identification Included in Presumptive identification includes
primary examination of cellular and colonial code morphology and �3 basic biochemical
tests (e.g., catalase and PYR).Definitive biochemical identification of 87077 Used per isolate.
aerobesDefinitive biochemical identification of 87076
anaerobesFluorescent-antibody culture typing 87145 May be used in addition to definitive identi-Immunologic culture typing 87147 fication code; typing codes are for each Probe culture typing 87149 reagent (e.g., per antiserum and probe).
Identification of Definitive identification of yeast 87106 Used per isolate.nonbacterial Definitive identification of molds 87107microorganisms Definitive identification of mycobacteria 87118
Probe identification of acid-fast bacilli or 87149 Used per probe.systemic fungi
Testing of isolate Disk diffusion 87184 Code based on method per isolate; if antimicrobial �1 method required, must use modifier susceptibilityc for NCCI.
MIC determination 87186Etest 87181�-Lactamase testing 87185
aThe American Medical Association CPT-4 manual (2a) is a copyrighted document that must be reviewed annually for additions, deletions, and descriptorchanges.
bModifiers may be appended for billing purposes. For example, for procedures performed in a point-of-care setting and meeting Food and Drug Adminis-tration criteria as waived tests, modifier -QW may be used. This applies primarily to RADT or serology procedures. It is expected that more than one codemay be used to detect multiple analytes from each specimen on the same date of service. It may be necessary to add an appropriate modifier (�59, dis-tinct procedural service) or other indication that a duplicate service has not been performed where acceptable to do so. Replicates of the same codewhen “each” is in the descriptor are generally billed as “units.” Refer to quarterly NCCI manual updates for guidance (27a).
cIndication of presumptive identification of isolates is included in the primary culture codes. Additional codes may be added to indicate definitive identifi-cation, culture typing, and susceptibility testing performed on significant isolates when medically appropriate.
dThe NCCI allows the use of only a single non-culture-dependent code per specimen; may reflex negatives to GAS culture.ePOL, physician office laboratory.fASO, anti-streptolysin O.
nonviral infectious etiologies, the diagnosis of viral upperrespiratory tract syndromes being considered primarilyclinical. Coding recommendations are based on theauthors’ understanding of current coding conventions. Itshould be recalled that CPT-4 codes are updated andshould be reviewed on an annual basis, since new codesthat affect these recommendations may be in effect eachJanuary.
NCCI
Edits found in the National Correct Coding Policy Manu-al for Part B Medicare Carriers (27a) are of particular sig-nificance to correct coding and billing for procedures forupper respiratory tract infections. These edits, developed in1985 as a component of the National Correct Coding Ini-tiative (NCCI), are designed to identify procedures thatwould not ordinarily be expected to be performed togeth-er on the same date of service. The NCCI manual for lab-oratory medicine is found in chapter X, “Pathology andLaboratory Services,” and may be obtained either on theCenters for Medicare and Medicaid Services website (http://www.cms.hhs.gov/physicians/edits) or in hard copy fromthe National Technical Information Service (27a). The edits
in chapter X delineate test procedures that would not beexpected to be performed on the same specimen on thesame date of service. The manual is composed of a narra-tive which describes general correct coding concepts andtwo tables of billing edits. The edits are placed into two cat-egories: mutually exclusive, indicating that the procedureswould be used in an either/or fashion but not together, andcolumn 1-column 2 edits (previously termed comprehen-sive component codes), indicating that there is a high like-lihood that these procedures would not be medicallyappropriate on the same specimen from the same date ofservice. The NCCI tables also identify specific CPT codesthat may be modified by appending modifier �59 when a“distinct procedural service” unrelated to the edit pair butusing one of the same codes has been performed on thesame date of service (termed “edit bypass”). A third cate-gory, termed “medically unbelievable edits,” will also bepublished in the near future. It should be noted that NCCIedits are updated on a quarterly basis, and the narrative isupdated annually in October. These documents should bereviewed upon each new issuance.
In the laboratory diagnosis of upper respiratory tractinfections, the edit set that is most problematic is thatwhich disallows more than one non-culture-dependent

assay to be performed for the same infectious analyte on asingle specimen. Thus, one cannot bill for both proceduresif a negative RADT for GAS is reflexed to a direct or ampli-fied probe for the same organism. Another example wouldbe the diagnosis of pertussis using DFA initially, followedby PCR to confirm the finding. Problematic edits such asthese may be discussed with the Medicare contractor withresponsibility for NCCI edit maintenance to effect changeif medically appropriate based on published evidence.
ICD-9 CODES
Justification of the medical necessity of procedures forupper respiratory tract infections in outpatients requiresthat for each CPT-4-coded procedure performed and billedfor, there must be an ICD-9-CM diagnostic code (2b) sub-mitted that is found on the “meets medical necessity” list-ing in reimbursement policies (“National Coverage Deci-sions,” or NCDs, and “Local Coverage Decisions,” orLCDs, in the case of Medicare payment and payment guide-lines generated by other third-party payers). For diagnosisof upper respiratory tract infections, one may provide anonspecific “symptom, sign or ill-defined condition” code(e.g., fever, malaise) or a clinical diagnosis based on signsand symptoms referable to the respiratory tract (e.g., phar-yngitis, tonsillitis, rhinitis). In the case of screening for apotential pathogen (e.g., MRSA), one may code for theunderlying disease or clinical condition leading to the testrequest. One should note, however, that in the case ofMedicare, procedures performed in the absence of currentsigns and symptoms may be considered “screening” and,therefore, not reimbursed per statute.
DRG CODES
The majority of upper respiratory tract infections likelyoccur in nonhospitalized patients who therefore are notsubject to “medical necessity determinations.” However, incritically ill patients (e.g., those with diphtheria) and inpatients hospitalized for another diagnosis presenting witha secondary upper respiratory tract process (e.g., sinusitisin intubated patients) or requiring screening for an upperrespiratory tract pathogen (e.g., MRSA), the clinical situa-tion is generally categorized by the final inpatient diagno-sis. The Medicare system classifies inpatient admissionsaccording to the Diagnosis Related Groups (DRG) system.Each DRG is tied to reimbursement through a prospectivepayment system. It is important to classify both primarydiagnosis and all secondary diagnoses to ensure paymentfor complicating conditions, which upper respiratory tractinfections and pathogen screening protocols may represent.Coding of procedures is still important, however, in orderto collect data on utilization, costs, and workload.
CODING DATA REVIEW
Correct procedure and diagnosis coding is critical for uti-lization review and outcome assessment, both of which areused to determine effectiveness of care. For example, a CPT-4 utilization review can be mapped to specific diagnosiscodes to ensure compliance with care pathways. DRG can
be mapped to the clinical outcome (e.g., survival) to deter-mine effectiveness of inpatient care, or DRG can be mappedto the inpatient expense outlay to determine the financialoutcome. These are issues which have assumed increasingimportance under a new pay-for-performance Medicarereimbursement system. In the case of upper respiratorytract infections, procedure code data may also be used toevaluate compliance with standards of care (e.g., reflex toGAS culture when RADTs are negative for pediatric butnot adult patients) or even to assess the performances ofindividual clinical laboratory scientists by comparingresults on more than one procedure performed on a singledate of service (e.g., RADT and culture for GAS). There-fore, correct coding has utility not only in ensuring appro-priate reimbursement, but also in evaluating the cost andclinical effectiveness of medical care, including the appro-priateness of testing.
REFERENCES
1. Aliyu, S. H., R. K. Marriott, M. D. Curran, S. Parmar,N. Bentley, N. M. Brown, J. S. Brazier, and H. Lud-lam. 2004. Real-time PCR investigation into theimportance of Fusobacterium necrophorum as a causeof acute pharyngitis in general practice. J. Med. Micro-biol. 53:1029–1035.
2. Al-Serhani, A. M. 2001. Mycobacterial infection ofthe head and neck: presentation and diagnosis. Laryn-goscope 111:2012–2016.
2a. American Medical Association. 2005. Current Proce-dural Terminology: CPT 2005, professional ed. AMAPress, Chicago, Ill.
2b.American Medical Association. 2005. InternationalClassification of Diseases, 9th rev., Clinical Modifica-tion, vol. 1 and 2. Physician ICD-9-CM. AMA Press,Chicago, Ill.
3. Anonymous. 2004. Summary of notifiable disease—United States. Morb. Mortal. Wkly. Rep. 51:1–88.
4. Balmelli, C., and H. F. Gunthard. 2003. Gonococcaltonsillar infection—a case report and literature review.Infection 31:362–365.
5. Bannatyne, R. M., C. Clausen, and L. R. McCarthy.1979. Cumitech 10, Laboratory Diagnosis of UpperRespiratory Tract Infections. Coordinating ed., I. B.R. Duncan. American Society for Microbiology,Washington, D.C.
6. Bannerman, T. L. 2003. Staphylococcus and Micro-coccus and other catalase-positive cocci that grow aer-obically, p. 384–404. In P. R. Murray, E. J. Baron,J. H. Jorgensen, M. A. Pfaller, and R. H. Yolken (ed.),Manual of Clinical Microbiology, 8th ed. ASM Press,Washington, D.C.
7. Baron, E. J., M. P. Weinstein, W. M. Dunne, Jr., P.Yagupsky, D. F. Welch, and D. M. Wilson. 2005.Cumitech 1C, Blood Cultures IV. Coordinating ed., E.J. Baron. ASM Press, Washington, D.C.
8. Bartkus, J. M., B. A. Juni, K. Ehresmann, C. A. Miller,G. N. Sanden, P. K. Cassiday, M. Saubolle, B. Lee, J.Long, A. R. Harrison, Jr., and J. M. Besser. 2003.
38 Waites et al. CUMITECH 10A

Identification of a mutation associated with erythro-mycin resistance in Bordetella pertussis: implicationsfor surveillance of antimicrobial resistance. J. Clin.Microbiol. 41:1167–1172.
9. Bernet, C., M. Garret, B. de Barbeyrac, C. Bebear, andJ. Bonnet. 1989. Detection of Mycoplasma pneumoni-ae by using the polymerase chain reaction. J. Clin.Microbiol. 27:2492–2496.
10. Bisgard, K., F. B. Pascual, T. Tiwari, and T. V. Mur-phy. 2002, posting date. Surveillance Manual for Vac-cine Preventable Diseases, 3rd ed., Chapter 8.[Online.] Centers for Disease Control and Prevention,Atlanta, Ga. http://www.cdc.gov/nip/publications/surv-manual/chpt08_pertussis.pdf.
11. Bisgard, K. M., F. B. Pascual, K. R. Ehresmann, C. A.Miller, C. Cianfrini, C. E. Jennings, C. A. Rebmann, J.Gabel, S. L. Schauer, and S. M. Lett. 2004. Infant per-tussis: who was the source? Pediatr. Infect. Dis. J. 23:985–989.
12. Bisno, A. L. 1996. Acute pharyngitis: etiology anddiagnosis. Pediatrics 97:949–954.
13. Bisno, A. L., M. A. Gerber, J. M. Gwaltney, Jr., E. L.Kaplan, and R. H. Schwartz. 2002. Practice guidelinesfor the diagnosis and management of group A strepto-coccal pharyngitis. Clin. Infect. Dis. 35:113–125.
14. Block, S. L., M. R. Hammerschlag, J. Hedrick, R.Tyler, A. Smith, P. Roblin, C. Gaydos, D. Pham, T. C.Quinn, R. Palmer, and J. McCarty. 1997. Chlamydiapneumoniae in acute otitis media. Pediatr. Infect. Dis.J. 16:858–862.
15. Bosley, G. S., A. M. Whitney, J. M. Pruckler, C. W.Moss, M. Daneshvar, T. Sih, and D. F. Talkington.1995. Characterization of ear fluid isolates of Alloio-coccus otitidis from patients with recurrent otitismedia. J. Clin. Microbiol. 33:2876–2880.
16. Bourbeau, P. P. 2003. Role of the microbiology labo-ratory in diagnosis and management of pharyngitis. J.Clin. Microbiol. 41:3467–3472.
17. Boustred, N. 1999. Practical guide to otitis externa.Aust. Fam. Physician 28:217–221.
18. Breese, B. B., and F. A. Disney. 1954. The accuracy ofdiagnosis of beta streptococcal infections on clinicalgrounds. J. Pediatr. 44:670–673.
19. Brook, I. 1995. Role of anaerobic bacteria in chronicotitis media and cholesteatoma. Int. J. Pediatr. Oto-rhinolaryngol. 31:153–157.
20. Brook, I., E. H. Frazier, and D. H. Thompson. 1992.Aerobic and anaerobic microbiology of external otitis.Clin. Infect. Dis. 15:955–958.
21. Browning, D. G., D. A. Schwartz, and R. L. Jurado.1992. Cryptococcosis of the larynx in a patient withAIDS: an unusual cause of fungal laryngitis. South.Med. J. 85:762–764.
22. Campbell, L. A., M. Perez Melgosa, D. J. Hamilton,C. C. Kuo, and J. T. Grayston. 1992. Detection of
Chlamydia pneumoniae by polymerase chain reaction.J. Clin. Microbiol. 30:434–439.
23. Campos, J. 2004. Group A streptococcus culture anddirect antigen detection, p. 3.11.8.1–3.11.8.7. InH. D. Isenberg (ed. in chief), Clinical MicrobiologyProcedures Handbook, 2nd ed. ASM Press, Washing-ton, D.C.
24. Carlson, P., O. V. Renkonen, and S. Kontiainen. 1994.Arcanobacterium haemolyticum and streptococcalpharyngitis. Scand. J. Infect. Dis. 26:283–287.
25. Carrie, S., and P. A. Fenton. 1994. Necrobacillosis—an unusual case of pharyngotonsillitis. J. Laryngol.Otol. 108:1097–1098.
26. Carroll, K., and L. Reimer. 1996. Microbiology andlaboratory diagnosis of upper respiratory tract infec-tions. Clin. Infect. Dis. 23:442–448.
27. Cartwright, K. 2001. Microbiology and laboratorymethods, p. 1–8. In A. J. Pollard and M. C. J. Maiden(ed.), Methods in Molecular Medicine Series, Men-ingococcal Disease, Methods and Protocols. HumanaPress, Totowa, N.J.
27a.Centers for Medicare and Medicaid Services. 2005.National Correct Coding Policy Manual for Part BMedicare Carriers. National Technical InformationService, Springfield, Va.
28. Cernoch, P. L., R. K. Enns, M. A. Saubolle, and R. J.Wallace, Jr. 1994. Cumitech 16A, Laboratory Diagno-sis of the Mycobacterioses. Coordinating ed., A. S.Weissfeld. ASM Press, Washington, D.C.
29. Chambers, H. F. 1997. Methicillin resistance in staphy-lococci: molecular and biochemical basis and clinicalimplications. Clin. Microbiol. Rev. 10:781–791.
30. Chen, Y., R. Colodner, B. Chazan, and R. Raz. 2005.Pharyngotonsillitis due to Arcanobacterium haemoly-ticum in Northern Israel. Isr. Med. Assoc. J. 7:241–242.
31. Coleman, D. C., D. E. Bennett, D. J. Sullivan, P. J.Gallagher, M. C. Henman, D. B. Shanley, and R. J.Russell. 1993. Oral Candida in HIV infection andAIDS: new perspectives/new approaches. Crit. Rev.Microbiol. 19:61–82.
32. Cooper, R. J., J. R. Hoffman, J. G. Bartlett, R. E.Besser, R. Gonzales, J. M. Hickner, and M. A. Sande.2001. Principles of appropriate antibiotic use for acutepharyngitis in adults: background. Ann. Emerg. Med.37:711–719.
33. Cunningham, M. W. 2000. Pathogenesis of group Astreptococcal infections. Clin. Microbiol. Rev. 13:470–511.
34. Dagan, R. 2004. The potential effect of widespreaduse of pneumococcal conjugate vaccines on the prac-tice of pediatric otolaryngology: the case of acute oti-tis media. Curr. Opin. Otolaryngol. Head Neck Surg.12:488–494.
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 39

35. Daxboeck, F., R. Krause, and C. Wenisch. 2003. Lab-oratory diagnosis of Mycoplasma pneumoniae infec-tion. Clin. Microbiol. Infect. 9:263–273.
36. Dowell, S. F., R. W. Peeling, J. Boman, G. M. Carlone,B. S. Fields, J. Guarner, M. R. Hammerschlag, L. A.Jackson, C. C. Kuo, M. Maass, T. O. Messmer, D. F.Talkington, M. L. Tondella, and S. R. Zaki. 2001.Standardizing Chlamydia pneumoniae assays: recom-mendations from the Centers for Disease Control andPrevention (USA) and the Laboratory Centre for Dis-ease Control (Canada). Clin. Infect. Dis. 33:492–503.
37. Erkan, M., T. Aslan, E. Sevuk, and E. Guney. 1994.Bacteriology of chronic suppurative otitis media. Ann.Otol. Rhinol. Laryngol. 103:771–774.
38. Esposito, S., F. Blasi, S. Bosis, R. Droghetti, N. Faelli,A. Lastrico, and N. Principi. 2004. Aetiology of acutepharyngitis: the role of atypical bacteria. J. Med.Microbiol. 53:645–651.
39. Esposito, S., R. Cavagna, S. Bosis, R. Droghetti, N.Faelli, and N. Principi. 2002. Emerging role of Myco-plasma pneumoniae in children with acute pharyngi-tis. Eur. J. Clin. Microbiol. Infect. Dis. 21:607–610.
40. Facklam, R. 2002. What happened to the streptococ-ci: overview of taxonomic and nomenclature changes.Clin. Microbiol. Rev. 15:613–630.
41. Falck, G., I. Engstrand, A. Gad, J. Gnarpe, H. Gnarpe,and A. Laurila. 1997. Demonstration of Chlamydiapneumoniae in patients with chronic pharyngitis.Scand. J. Infect. Dis. 29:585–589.
42. Feingold, M. H., and M. L. Kumar. 2004. Otitis mediaassociated with Vibrio alginolyticus in a child withpressure-equalizing tubes. Pediatr. Infect. Dis. J. 23:475–476.
43. Fry, N. K., O. Tzivra, Y. T. Li, A. McNiff, N. Doshi,P. A. Maple, N. S. Crowcroft, E. Miller, R. C. George,and T. G. Harrison. 2004. Laboratory diagnosis ofpertussis infections: the role of PCR and serology. J. Med. Microbiol. 53:519–525.
44. Funke, G., and K. A. Bernard. 2003. Coryneformgram-positive rods, p. 472–501. In P. R. Murray, E. J.Baron, J. H. Jorgensen, M. A. Pfaller, and R. H.Yolken (ed.), Manual of Clinical Microbiology, 8th ed.ASM Press, Washington, D.C.
45. Funke, G., F. N. Renaud, J. Freney, and P. Riegel.1997. Multicenter evaluation of the updated andextended API (RAPID) Coryne database 2.0. J. Clin.Microbiol. 35:3122–3126.
46. Gaydos, C. A., T. C. Quinn, and J. J. Eiden. 1992.Identification of Chlamydia pneumoniae by DNAamplification of the 16S rRNA gene. J. Clin. Microbi-ol. 30:796–800.
47. Gerber, M. A., and S. T. Shulman. 2004. Rapid diag-nosis of pharyngitis caused by group A streptococci.Clin. Microbiol. Rev. 17:571–580.
47a.Gilchrist, M. J. R., W. P. McKinney, J. M. Miller, andA. S. Weissfeld. 2000. Cumitech 33, Laboratory Safe-ty, Management, and Diagnosis of Biological Agents
Associated with Bioterrorism. Coordinating ed., J. W.Snyder. ASM Press, Washington, D.C.
48. Gilligan, P. H., J. M. Janda, M. A. Karmali, and J. M.Miller. 1992. Cumitech 12A, Laboratory Diagnosis ofBacterial Diarrhea. Coordinating ed., F. S. Nolte.American Society for Microbiology, Washington, D.C.
49. Gonzalez, C. E., M. G. Rinaldi, and A. M. Sugar. 2002.Zygomycosis. Infect. Dis. Clin. N. Am. 16:895–914.
50. Groothuis, J. R., J. Thompson, and P. F. Wright. 1986.Correlation of nasopharyngeal and conjunctival cul-tures with middle ear fluid cultures in otitis media. Aprospective study. Clin. Pediatr. 25:85–88.
51. Guris, D., P. M. Strebel, B. Bardenheier, M. Brennan,R. Tachdjian, E. Finch, M. Wharton, and J. R. Liven-good. 1999. Changing epidemiology of pertussis in theUnited States: increasing reported incidence amongadolescents and adults, 1990–1996. Clin. Infect. Dis.28:1230–1237.
52. Hammerschlag, M. R. 1994. Antimicrobial suscepti-bility and therapy of infections caused by Chlamy-dia pneumoniae. Antimicrob. Agents Chemother. 38:1873–1878.
53. Hammerschlag, M. R. 2000. The role of Chlamydia inupper respiratory tract infections. Curr. Infect. Dis.Rep. 2:115–120.
54. Hazen, K. C., and S. A. Howell. 2003. Candida, Cryp-tococcus, and other yeasts of medical importance, p. 1693–1711. In P. R. Murray, E. J. Baron, J. H. Jor-gensen, M. A. Pfaller, and R. H. Yolken (ed.), Manualof Clinical Microbiology, 8th ed. ASM Press, Wash-ington, D.C.
55. Heininger, U., J. D. Cherry, and K. Stehr. 2004. Sero-logic response and antibody-titer decay in adults withpertussis. Clin. Infect. Dis. 38:591–594.
56. Heininger, U., K. Stehr, S. Schmitt-Grohe, C. Lorenz,R. Rost, P. D. Christenson, M. Uberall, and J. D.Cherry. 1994. Clinical characteristics of illness causedby Bordetella parapertussis compared with illnesscaused by Bordetella pertussis. Pediatr. Infect. Dis. J.13:306–309.
57. Higgins, P. B. 1974. Viruses associated with acute res-piratory infections 1961–71. J. Hyg. 72:425–432.
58. Hill, B. C., C. N. Baker, and F. C. Tenover. 2000. Asimplified method for testing Bordetella pertussis forresistance to erythromycin and other antimicrobialagents. J. Clin. Microbiol. 38:1151–1155.
59. Hoge, C. W., B. Schwartz, D. F. Talkington, R. F.Breiman, E. M. MacNeill, and S. J. Englender. 1993.The changing epidemiology of invasive group A strep-tococcal infections and the emergence of streptococcaltoxic shock-like syndrome. A retrospective popula-tion-based study. JAMA 269:384–389.
60. Huletsky, A., P. Lebel, F. J. Picard, M. Bernier, M.Gagnon, N. Boucher, and M. G. Bergeron. 2005.Identification of methicillin-resistant Staphylococcus
40 Waites et al. CUMITECH 10A
aureus carriage in less than 1 hour during a hospitalsurveillance program. Clin. Infect. Dis. 40:976–981.
61. Ibekwe, A. O., Z. al Shareef, and A. Benayam. 1997.Anaerobes and fungi in chronic suppurative otitismedia. Ann. Otol. Rhinol. Laryngol. 106:649–652.
62. Janda, W. M., and J. S. Knapp. 2003. Neisseria andMoraxella catarrhalis, p. 585–608. In P. R. Murray, E. J. Baron, J. H. Jorgensen, M. A. Pfaller, and R. H.Yolken (ed.), Manual of Clinical Microbiology, 8th ed.ASM Press, Washington, D.C.
63. Jousimies-Somer, H. R., P. H. Summanen, D. M. Cit-ron, E. J. Baron, H. M. Wexler, and S. M. Finegold.2002. Wadsworth Anaerobic Bacteriology Manual,6th ed. Star Publishing Co., Belmont, Calif.
64. Kalcioglu, M. T., S. Oncel, R. Durmaz, B. Otlu, M. C.Miman, and O. Ozturan. 2002. Bacterial etiology ofotitis media with effusion; focusing on the high posi-tivity of Alloiococcus otitidis. New Microbiol. 25:31–35.
65. Karkos, P. D., A. Karkanevatos, S. Panagea, A. Dingle,and J. E. Davies. 2004. Lemierre’s syndrome: how asore throat can end in disaster. Eur. J. Emerg. Med. 11:228–230.
66. Katzko, G., M. Hofmeister, and D. Church. 1996.Extended incubation of culture plates improves recov-ery of Bordetella spp. J. Clin. Microbiol. 34:1563–1564.
67. Kellogg, J. A. 1990. Suitability of throat culture pro-cedures for detection of group A streptococci and asreference standards for evaluation of streptococcalantigen detection kits. J. Clin. Microbiol. 28:165–169.
68. Kilian, M. 2003. Haemophilus, p. 623–635. In P. R.Murray, E. J. Baron, J. H. Jorgensen, M. A. Pfaller,and R. H. Yolken (ed.), Manual of Clinical Microbiol-ogy, 8th ed. ASM Press, Washington, D.C.
69. Kotikoski, M. J., M. Kleemola, and A. A. Palmu. 2004.No evidence of Mycoplasma pneumoniae in acutemyringitis. Pediatr. Infect. Dis. J. 23:465–466.
70. Lafferty, W. E., J. P. Hughes, and H. H. Handsfield.1997. Sexually transmitted diseases in men who havesex with men. Acquisition of gonorrhea and nongono-coccal urethritis by fellatio and implications forSTD/HIV prevention. Sex. Transm. Dis. 24:272–278.
71. Lawson, R., G. Bodey, and M. Luna. 1980. Casereport: Candida infection presenting as laryngitis. Am.J. Med. Sci. 280:173–177.
72. Leskinen, K., P. Hendolin, A. Virolainen-Julkunen, J.Ylikoski, and J. Jero. 2004. Alloiococcus otitidis inacute otitis media. Int. J. Pediatr. Otorhinolaryngol.68:51–56.
73. Leskinen, K., P. Hendolin, A. Virolainen-Julkunen, J.Ylikoski, and J. Jero. 2002. The clinical role of Alloio-coccus otitidis in otitis media with effusion. Int. J.Pediatr. Otorhinolaryngol. 66:41–48.
74. Lewis, K., M. A. Saubolle, F. C. Tenover, M. F. Rudin-sky, S. D. Barbour, and J. D. Cherry. 1995. Pertussis
caused by an erythromycin-resistant strain of Borde-tella pertussis. Pediatr. Infect. Dis. J. 14:388–391.
75. Lieberth, A. S., T. Ganiats, E. O. Cox, L. Culpepper,M. Mahoney, D. Miller, E. K. Runyan, N. L. Shapiro,and E. R. Wald. 2004. Diagnosis and management ofacute otitis media. Pediatrics 113:1451–1465.
76. Limjoco-Antonio, A. D., W. M. Janda, and P. C.Schreckenberger. 2003. Arcanobacterium haemoly-ticum sinusitis and orbital cellulitis. Pediatr. Infect.Dis. J. 22:465–467.
77. Loeffelholz, M. J. 2003. Bordetella, p. 780–788. InP. R. Murray, E. J. Baron, J. H. Jorgensen, M. A. Pfall-er, and R. H. Yolken (ed.), Manual of Clinical Micro-biology, 8th ed. ASM Press, Washington, D.C.
78. Loens, K., D. Ursi, H. Goossens, and M. Ieven. 2003.Molecular diagnosis of Mycoplasma pneumoniae res-piratory tract infections. J. Clin. Microbiol. 41:4915–4923.
79. Lu, H. Z., X. H. Weng, B. Zhu, H. Li, Y. K. Yin, Y. X.Zhang, D. W. Haas, and Y. W. Tang. 2003. Major out-break of toxic shock-like syndrome caused by Strepto-coccus mitis. J. Clin. Microbiol. 41:3051–3055.
80. Mackenzie, A., L. A. Fuite, F. T. Chan, J. King, U.Allen, N. MacDonald, and F. Diaz-Mitoma. 1995. Inci-dence and pathogenicity of Arcanobacterium haemo-lyticum during a 2-year study in Ottawa. Clin. Infect.Dis. 21:177–181.
81. Madico, G., T. C. Quinn, J. Boman, and C. A. Gaydos.2000. Touchdown enzyme time release-PCR for detec-tion and identification of Chlamydia trachomatis, C.pneumoniae, and C. psittaci using the 16S and 16S-23S spacer rRNA genes. J. Clin. Microbiol. 38:1085–1093.
82. Mattila, P. S., and P. Carlson. 1998. Pharyngolaryngi-tis caused by Neisseria meningitidis. Scand. J. Infect.Dis. 30:198–200.
83. Mayes, T., and M. E. Pichichero. 2001. Are follow-upthroat cultures necessary when rapid antigen detectiontests are negative for group A streptococci? Clin. Pedi-atr. 40:191–195.
84. McDonald, J. A., and F. T. Saulsbury. 1997. ChronicCandida albicans otitis media in children with immun-odeficiency. Pediatr. Infect. Dis. J. 16:529–531.
85. McEwan, J., W. Giridharan, R. W. Clarke, and P.Shears. 2003. Paediatric acute epiglottitis: not a disap-pearing entity. Int. J. Pediatr. Otorhinolaryngol. 67:317–321.
86. McMillan, J. A., C. Sandstrom, L. B. Weiner, B. A.Forbes, M. Woods, T. Howard, L. Poe, K. Keller, R. M. Corwin, and J. W. Winkelman. 1986. Viral andbacterial organisms associated with acute pharyngitisin a school-aged population. J. Pediatr. 109:747–752.
87. Miller, R. A., F. Brancato, and K. K. Holmes. 1986.Corynebacterium haemolyticum as a cause of pharyn-gitis and scarlatiniform rash in young adults. Ann.Intern. Med. 105:867–872.
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 41

88. Murdoch, D. R. 2003. Nucleic acid amplification testsfor the diagnosis of pneumonia. Clin. Infect. Dis. 36:1162–1170.
89. Murray, P. R., K. S. Rosenthal, G. S. Kobayashi, andM. A. Pfaller. 2002. Medical Microbiology, 4th ed., p. 176–184. Mosby, St. Louis, Mo.
90. Nasri, S., L. D. True, and E. Abemayor. 1995. Upperairway obstruction caused by group G streptococcallaryngitis. Am. J. Otolaryngol. 16:53–55.
91. Odds, F. C. 1988. Candida and Candidosis, 2nd ed.Bailliere Tindall, London, United Kingdom.
91a.Office of the Inspector General. 1998. Complianceprogram guidance for clinical laboratories. Fed. Reg-ist. 63:45076–45087.
92. Ohuabunwo, C. J., K. M. Bisgard, T. Popovic, and M.Warton. 2002, posting date. Surveillance Manual forVaccine Preventable Diseases, 3rd ed., Chapter 1.[Online.] Centers for Disease Control and Prevention,Atlanta, Ga. http://www.cdc.gov/nip/publications/surv-manual/chpt01_dip.pdf.
93. Olsen, C. C., J. R. Schwebke, W. H. Benjamin, Jr., A.Beverly, and K. B. Waites. 1999. Comparison of directinoculation and Copan transport systems for isolationof Neisseria gonorrhoeae from endocervical speci-mens. J. Clin. Microbiol. 37:3583–3585.
94. Osterlund, A. 1995. Are penicillin treatment failuresin Arcanobacterium haemolyticum pharyngotonsillitiscaused by intracellularly residing bacteria? Scand. J.Infect. Dis. 27:131–134.
95. Page-Shafer, K., A. Graves, C. Kent, J. E. Balls, V. M.Zapitz, and J. D. Klausner. 2002. Increased sensitivityof DNA amplification testing for the detection of pha-ryngeal gonorrhea in men who have sex with men.Clin. Infect. Dis. 34:173–176.
96. Reznikov, M., T. K. Blackmore, J. J. Finlay-Jones, andD. L. Gordon. 1995. Comparison of nasopharyngealaspirates and throat swab specimens in a polymerasechain reaction-based test for Mycoplasma pneumoni-ae. Eur. J. Clin. Microbiol. Infect. Dis. 14:58–61.
97. Ribes, J. A., C. L. Vanover-Sams, and D. J. Baker. 2000.Zygomycetes in human disease. Clin. Microbiol. Rev.13:236–301.
98. Richardson, M. D., P. Koukila-Kähkolä, and G. S.Shankland. 2003. Rhizopus, Rhizomucor, Absidia,and other agents of systemic subcutaneous zygomy-coses, p. 1761–1780. In P. R. Murray, E. J. Baron, J. H.Jorgensen, M. A. Pfaller, and R. H. Yolken (ed.), Man-ual of Clinical Microbiology, 8th ed. ASM Press,Washington, D.C.
99. Rose, F. B., C. J. Camp, and E. J. Antes. 1987. Fami-ly outbreak of fatal Yersinia enterocolitica pharyngitis.Am. J. Med. 82:636–637.
100. Ruoff, K. L., R. A. Whiley, and D. Beighton. 2003.Streptococcus, p. 405–421. In P. R. Murray, E. J.Baron, J. H. Jorgensen, M. A. Pfaller, and R. H.
Yolken (ed.), Manual of Clinical Microbiology, 8thed. ASM Press, Washington, D.C.
101. Ruuskanen, O., M. Arola, T. Heikkinen, and T.Ziegler. 1991. Viruses in acute otitis media: increas-ing evidence for clinical significance. Pediatr. Infect.Dis. J. 10:425–427.
102. Sande, M. A., and J. M. Gwaltney. 2004. Acute com-munity-acquired bacterial sinusitis: continuing chal-lenges and current management. Clin. Infect. Dis.39(Suppl. 3):S151–S158.
103. Schalen, L., P. Christensen, C. Kamme, H. Miorner,K. I. Pettersson, and C. Schalen. 1980. High isolationrate of Branhamella catarrhalis from the nasophar-ynx in adults with acute laryngitis. Scand. J. Infect.Dis. 12:277–280.
104. Schubert, M. S., and D. W. Goetz. 1998. Evaluationand treatment of allergic fungal sinusitis. I. Demo-graphics and diagnosis. J. Allergy Clin. Immunol.102:387–394.
105. Sengor, A., A. Willke, O. Aydin, S. Gundes, and A.Almac. 2004. Isolated necrotizing epiglottitis: reportof a case in a neutropenic patient and review of theliterature. Ann. Otol. Rhinol. Laryngol. 113:225–228.
106. Sharp, S. E., A. Robinson, M. Saubolle, M. SantaCruz, K. Carroll, and V. Baselski. 2004. Cumitech7B, Lower Respiratory Tract Infections. Coordinat-ing ed., S. E. Sharp. ASM Press, Washington, D.C.
107. Shet, A., and E. L. Kaplan. 2002. Clinical use andinterpretation of group A streptococcal antibodytests: a practical approach for the pediatrician or pri-mary care physician. Pediatr. Infect. Dis. J. 21:420–426.
108. Summerbell, R. C. 2004. Mould identification, p. 8.9.1–8.9.59. In H. D. Isenberg (ed. in chief), Clin-ical Microbiology Procedures Handbook, 2nd ed.ASM Press, Washington, D.C.
109. Sun, Q. N., A. W. Fothergill, D. I. McCarthy, M. G.Rinaldi, and J. R. Graybill. 2002. In vitro activities ofposaconazole, itraconazole, voriconazole, ampho-tericin B, and fluconazole against 37 clinical isolatesof zygomycetes. Antimicrob. Agents Chemother. 46:1581–1582.
110. Talkington, D. F., S. Shott, M. T. Fallon, S. B.Schwartz, and W. L. Thacker. 2004. Analysis of eightcommercial enzyme immunoassay tests for detectionof antibodies to Mycoplasma pneumoniae in humanserum. Clin. Diagn. Lab. Immunol. 11:862–867.
111. Talkington, D. F., K. B. Waites, S. B. Schwartz, andR. E. Besser. 2001. Emerging from obscurity: under-standing the pulmonary and extrapulmonary syn-dromes, pathogenesis, and epidemiology of humanMycoplasma pneumoniae infections, p. 57–84. InW. M. Scheld, W. A. Craig, and J. M. Hughes (ed.),Emerging Infections 5. ASM Press, Washington, D.C.
42 Waites et al. CUMITECH 10A
112. Thomson, R. B., Jr., and J. M. Miller. 2003. Speci-men collection, transport, and processing: bacteriolo-gy, p. 286–330. In P. R. Murray, E. J. Baron, J. H.Jorgensen, M. A. Pfaller, and R. H. Yolken (ed.),Manual of Clinical Microbiology, 8th ed. ASM Press,Washington, D.C.
113. Tondella, M. L., D. F. Talkington, B. P. Holloway,S. F. Dowell, K. Cowley, M. Soriano-Gabarro, M. S.Elkind, and B. S. Fields. 2002. Development and eval-uation of real-time PCR-based fluorescence assays fordetection of Chlamydia pneumoniae. J. Clin. Micro-biol. 40:575–583.
114. Tong, C. Y., and M. Sillis. 1993. Detection of Chlamy-dia pneumoniae and Chlamydia psittaci in sputumsamples by PCR. J. Clin. Pathol. 46:313–317.
115. Toyokawa, M., T. Kishimoto, Y. Cai, M. Ogawa, S.Shiga, I. Nishi, H. Hosotsubo, M. Horikawa, and S.Asari. 2004. Severe Chlamydophila psittaci pneumo-nia rapidly diagnosed by detection of antigen in spu-tum with an immunochromatography assay. J. Infect.Chemother. 10:245–249.
116. Turner, J. C., A. Fox, K. Fox, C. Addy, C. Z. Garri-son, B. Herron, C. Brunson, and G. Betcher. 1993.Role of group C beta-hemolytic streptococci in phar-yngitis: epidemiologic study of clinical features asso-ciated with isolation of group C streptococci. J. Clin.Microbiol. 31:808–811.
117. Vrabec, D. P. 1993. Fungal infections of the larynx.Otolaryngol. Clin. N. Am. 26:1091–1114.
118. Waites, K., and S. Brown. 2003. Antimicrobial resis-tance among isolates of respiratory tract infectionpathogens from the southern United States: datafrom the PROTEKT US surveillance program 2000/2001. South. Med. J. 96:974–985.
119. Waites, K., L. B. Duffy, D. F. Talkington, and S. B.Schwartz. 2004. Mycoplasma pneumoniae, Myco-plasma hominis, and Ureaplasma cultures from clin-ical specimens, p. 3.15.1–3.15.17. In H. D. Isenberg(ed. in chief), Clinical Microbiology ProceduresHandbook, 2nd ed. ASM Press, Washington, D.C.
120. Waites, K. B., Y. Rikihisa, and D. Taylor-Robinson.2003. Mycoplasma and Ureaplasma, p. 972–990. InP. R. Murray, E. J. Baron, J. H. Jorgensen, M. A.Pfaller, and R. H. Yolken (ed.), Manual of ClinicalMicrobiology, 8th ed. ASM Press, Washington, D.C.
121. Waites, K. B., D. F. Talkington, and C. M. Bébéar.2002. Mycoplasmas, p. 201–224. In A. L. Truant
(ed.), Manual of Commercial Methods in ClinicalMicrobiology. ASM Press, Washington, D.C.
122. Waites, K. B., C. M. Bébéar, J. A. Robertson, D. F.Talkington, and G. E. Kenny. 2001. Cumitech 34,Laboratory Diagnosis of Mycoplasmal Infections.Coordinating ed., F. S. Nolte. ASM Press, Washing-ton, D.C.
123. Waites, K. B., and D. F. Talkington. 2004. Mycoplas-ma pneumoniae and its role as a human pathogen.Clin. Microbiol. Rev. 17:697–728.
124. Wald, E. R., W. C. Bordley, D. H. Darrow, K. T.Grimm, J. M. Gwaltney, S. M. Marcy, M. O. Senac,and P. V. Williams. 2001. American Academy of Pedi-atrics—clinical practice guidelines: management ofsinusitis. Pediatrics 108:798–808.
125. Warren, D. K., R. S. Liao, L. R. Merz, M. Eveland,and W. M. Dunne, Jr. 2004. Detection of methicillin-resistant Staphylococcus aureus directly from nasalswab specimens by a real-time PCR assay. J. Clin.Microbiol. 42:5578–5581.
126. Whiley, R. A., L. M. Hall, J. M. Hardie, and D.Beighton. 1999. A study of small-colony, beta-haemolytic, Lancefield group C streptococci withinthe anginosus group: description of Streptococcusconstellatus subsp. pharyngis subsp. nov., associatedwith the human throat and pharyngitis. Int. J. Syst.Bacteriol. 49:1443–1449.
127. Wilhelmus, K., T. J. Liesgang, M. S. Osato, and D. B.Jones. 1994. Cumitech 13A, Laboratory Diagnosisof Ocular Infections. Coordinating ed., S. C. Specter.ASM Press, Washington, D.C.
128. York, M. K., and P. Gilligan. 2004. Nasal sinus cul-tures, p. 3.11.9.1–3.11.9.4. In H. D. Isenberg (ed. inchief), Clinical Microbiology Procedures Handbook,2nd ed. ASM Press, Washington, D.C.
129. York, M. K., and P. Gilligan. 2004. Otitis cultures, p. 3.11.5.1–3.11.5.6. In H. D. Isenberg (ed. in chief),Clinical Microbiology Procedures Handbook, 2nded. ASM Press, Washington, D.C.
130. Younus, F., A. Chua, G. Tortora, and V. E. Jimenez.2002. Lemierre’s disease caused by co-infection ofArcanobacterium haemolyticum and Fusobacteriumnecrophorum: a case report. J. Infect. 45:114–117.
131. Zaoutis, T., M. Attia, R. Gross, and J. Klein. 2004.The role of group C and group G streptococci inacute pharyngitis in children. Clin. Microbiol. Infect.10:37–40.
CUMITECH 10A Laboratory Diagnosis of Upper Respiratory Tract Infections 43


















