
Analyse longitudinale de la qualité de vie en cancérologie ...

1
PY Bondiau PhD. MD.
Centre Antoine Lacassagne. Nice. France
High Precision Radiotherapy Unit
Cyclotron / Cyberknife
La radiothérapie stéréotaxique
en cancérologie digestiveMarseille 22 novembre 2012

2
Clinical indicationsClinical indications
LiverHKMets
Lung T1-2 N0 Mets
Prostate
PancreasKidney
Brain. shwanoma. meningioma. glia.…lHead/neckRe irradiationBoost
Bladder
BreastNeoadjBoost
Spine MetsChondrosarcoma…
Lung boost IIIB

3
High PrecisionTreatment Site in Nice
High PrecisionTreatment Site in Nice
MEDICYC CYCLOTRON
PROTON TREATMENT ROOM (65MeV)
FLUOR 18 PRODUCTION (20MeV)
CYBERKNIFE

4
0
200
400
600
800
1000
1200
1400
2007 2008 2009 2010 2011 2012
Cyberknife : new treatment and number of fractions (December 2011)
Cyberknife : new treatment and number of fractions (December 2011)
Year New T Nb Fr Fr/T2007 131 443 3.32008 129 534 4.12009 240 898 3.82010 315 1.159 3.62011 349 1.218 3.3

5
0
50
100
150
PatientsPatients
Provence AlpesProvence Alpes --Côte dCôte d ’’AzurAzurPACA: 4.743.000 PACA: 4.743.000 inhabitantsinhabitants
MarseilleToulonCannesMonacoGap
Nice 39%
PACA 49%
CAL
3 0 %
Te a c h
Hospi t a l
3 7 %
C l i ni c s
2 3 %
CHG
10 %
2007
2011
Bordeaux LyonOther French areas 12%
ParisParis11.362.000 11.362.000 inhabitantsinhabitants
Bordeaux
Caen
Lille
Nancy

6
LungBrain
SkullSpine
BreastHandN
LiverOther
0
20
40
60
80
100
120
140
LungBrain
SkullSpine
BreastHandN
LiverOther
0
20
40
60
80
100
120
140
Evolution N patient/localization 2007-2011Evolution N patient/localization 2007-2011
20072008
20092010
2011

7
Defining Radio Surgery [1]Defining Radio Surgery [1]
– Lars Leksell Gammaknife
– Radiosurgery (1 fraction)
– 1967 Stockholm Karolinska Institut
– High precision RT
– >100 converging mini-beam
– Target : 3 cm max
– 1-3 Loc (5?)
– Millimetric accuracy
– Image matching PET/MRI and CT
– Mechanical accuracy => only intra cranial
– Volume is spherical
– Lars Leksell Gammaknife
– Radiosurgery (1 fraction)
– 1967 Stockholm Karolinska Institut
– High precision RT
– >100 converging mini-beam
– Target : 3 cm max
– 1-3 Loc (5?)
– Millimetric accuracy
– Image matching PET/MRI and CT
– Mechanical accuracy => only intra cranial
– Volume is spherical

8
Patient PositioningPatient Positioning
• Robotic couch
– 3 rotations
– 3 translations
• Numeric X Rays
– 2 sources of X Rays with 2 flat panels at 90°
– Automatic.
– Discontinued
– 41 * 41 cm 1024 *1024 pxl
– Pxl : 0.4 mm²
• Robotic couch
– 3 rotations
– 3 translations
• Numeric X Rays
– 2 sources of X Rays with 2 flat panels at 90°
– Automatic.
– Discontinued
– 41 * 41 cm 1024 *1024 pxl
– Pxl : 0.4 mm²
0.4 mm
0.3 mm

9
ConventionalRT
ConventionalRT
70
RadiosurgeryRadiosurgery CyberKnifeCyberKnife
?
Accuracy < cmAccuracy < cm
multiple fractionsmultiple fractions
Accuracy < mmAccuracy < mm
unique fractionunique fraction
Accuracy < mmAccuracy < mm
multiple fractionsmultiple fractions
10

11

12

13

14

15

16
RadiosurgeryRadiosurgery
• Varian
• Electa
• Vero
• Varian
• Electa
• Vero

17
5 – Tumormotion
2 - Patient movement
4 - Treatment planning
6 - Beam delivery
3 - Imaging quality(CT. MRI.…)1- Patient
Positioning
Defining AccuracyDefining Accuracy
• Traditional Definition: Mechanical Accuracy
• New Definition: Total Clinical Accuracy
• Traditional Definition: Mechanical Accuracy
• New Definition: Total Clinical Accuracy
Total Total Clinical Clinical
AccuracyAccuracy

18
Comparison of Hybrid Gantry and CyberKnife ® SBRTComparison of Hybrid Gantry and CyberKnife ® SBRT
TUMOR
Subclinical Disease
TUMOR
Subclinical Disease
GTV: Gross Tumor Volume
CTV: Clinical Target Volume
PTV: Planning Target Volume
Healthy Tissue
Hybrid Gantry SBRT CyberKnife® SBRT
Video courtesy of MD Anderson

19
Patient: Flowchart (cont.)Patient: Flowchart (cont.)Patient: Flowchart (cont.)
•Radiologist / Lung specialist Consultation +/- PET
•Fiducial insertion (1-4) – + histology (8 cases)
•1 week
•Dosimetric CT scan
•Treatment
•Radiologist / Lung specialist Consultation +/- PET
•Fiducial insertion (1-4) – + histology (8 cases)
•1 week
•Dosimetric CT scan
•Treatment

20
Mvt thorax/tumor MvtMvt thorax/tumor thorax/tumor
X
Y
Z
Diodsthorax
Fiducials

21

22

23

24

25

26
27
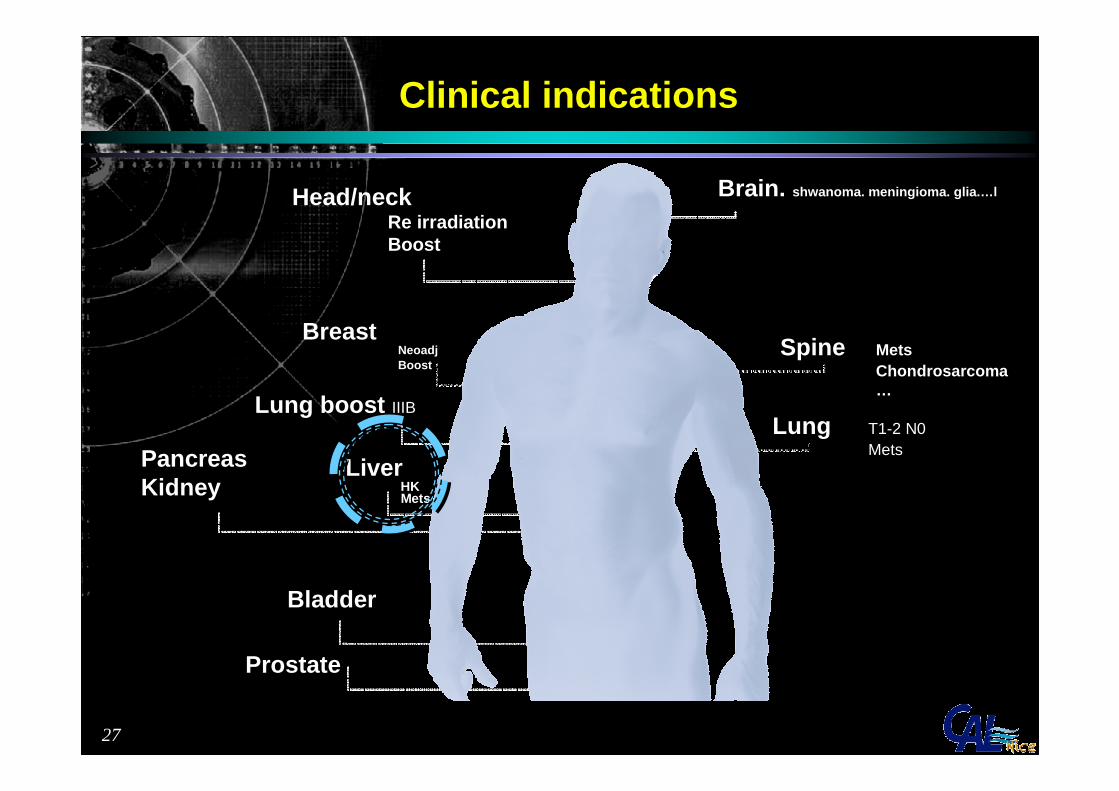
Clinical indicationsClinical indications
LiverHKMets
Lung T1-2 N0 Mets
Prostate
PancreasKidney
Brain. shwanoma. meningioma. glia.…lHead/neckRe irradiationBoost
Bladder
BreastNeoadjBoost
Spine MetsChondrosarcoma…
Lung boost IIIB

28
• Its motion (translation and rotation) depends on the patient breathing pattern and needs to be tracked in real time.
• Liver moves with respiration and deforms• Liver moves with respiration and deforms
Liver is difficult to treatLiver is difficult to treat

29
Fiducial implantation allows to :
- localize the region to be treated (difficult in a uniform-density organ like liver)
- assess for the target motion in 6D (translation + rotation)
- assess for the target deformation during treatment
Based on fiducial tracking
Fiducials SOLVES THE EQUATION Fiducials SOLVES THE EQUATION

30
Dr Xavier MirabelDépartement Universitaire de Radiothérapie
Centre Oscar Lambret – Lille - [email protected]
www.centreoscarlambret.frwww.ckno.fr
Dr Xavier MirabelDépartement Universitaire de Radiothérapie
Centre Oscar Lambret – Lille - [email protected]
www.centreoscarlambret.frwww.ckno.fr
Oligométastases :
Radiothérapie des métastases hépatiques …à visée curative ?
Oligométastases :
Radiothérapie des métastases hépatiques …à visée curative ?

31
Traitement « curatif » des métastaseshépatiques
Traitement « curatif » des métastaseshépatiques
• Résection complète de métas pulmonaires ou hépatiqu es de CCR
• Survie à 1/3/5/10 ans 85/50/40/20 %
• Mortalité opératoire 1 à 3 %– Timmermann ; CA Cancer J Clin 2009
• Survie– récidive locale– récidive hépatique– récidive à distance
• Quel critère pour évaluer un tt local ? Contrôle loc al
• Résection complète de métas pulmonaires ou hépatiqu es de CCR
• Survie à 1/3/5/10 ans 85/50/40/20 %
• Mortalité opératoire 1 à 3 %– Timmermann ; CA Cancer J Clin 2009
• Survie– récidive locale– récidive hépatique– récidive à distance
• Quel critère pour évaluer un tt local ? Contrôle loc al

32
• Lille
• Patients 42
• Métas 62
• Technique cyber
• Dose 3 x 15 Gy
• Contrôle local
• 1 an 90 %
• 2 ans 86 %
– Vautravers-Dewas ; IJROBP 2011
• Lille
• Patients 42
• Métas 62
• Technique cyber
• Dose 3 x 15 Gy
• Contrôle local
• 1 an 90 %
• 2 ans 86 %
– Vautravers-Dewas ; IJROBP 2011

33
Author Patients/Mets Dose (Gy) / fractionation
Medianfollow-up (months)
ActuarialLC 1 year %
ActuarialLC 2 years
%
Actuarialsurvival 1
year %
Actuarialsurvival 2 years %
OS median
Herfarth 2001 Heidelberg /46 14-26/1 5.7 67 72
Wulf 2006 Wurtzburg, Bern /39 26-37.5 /1-4 15 92 66 72 32
Mendez Romero 2006 Rotterdam /34 30-37.5/3 12.9 100 86 (mets) 85 62 (mets)
Hoyer 2006 Aarhus /97 45/3 52 79 67 38
Katz 2007 Cleveland 0/174 48/7-24 14.5 76 57 78 (10 months)
37 (20 months) 14.5
Milano 2008 Rochester 120 50/10 41 77 50 24
Rusthoven 2009USA
Multicentric
47/63 60/3 16 95 92 30 20.5
Lee 2009 Toronto 68/143 27-60/6 10.8 71 47 (18 months) 17.6
Ambrosini 2009 Vicenza 27/ 25-60/3 13 85
Vautravers-Dewas 2010 Lille 42/62 40-45/3-4 14.3 90 86 94 48
Chang 2011USA
Multicentric
65/102 variable/1-6 18 67 55 72 38

34
Facteurs pronostiquesFacteurs pronostiques
facteurs pronostiques défavorables
contrôle local
survie sans
maladie survie
sexe masculin + Hoyer 2006
métas synchrones ++ ++ Hoyer 2006
lésions extra-hépatiques ++ Chang 2011
nombre de cibles hépatiques ++
taille cible hépatique ++ +Hoyer 2006 ; Chang 2011
nombres de lignes de traitement + ++ ++
dose ++Dewas 2010 ; Chang 2011

35
ToxicitéToxicité
Author Patients/Mets
Dose (Gy) / fractionation
Median
follow-up
(months)
Actuarial LC 1 year
%
Actuarial LC
2 years
%
Toxicités G3/4
Herfarth 2001 Heidelberg /46 14-26/1 5.7 67
Wulf 2006 Wurtzburg, Bern /39
26-37.5 /1-4
15 92 66 0 0
Mendez Romero 2006 Rotterdam /34 30-37.5/3 12.9 100 86
(mets) 4/34 12 %
Hoyer 2006 Aarhus /97 45/3 52 79 1 dc RILD, 3 ulcérations digestives
Katz 2007 Cleveland 0/174 48/7-24 14.5 76 57 0 0
Milano 2008 Rochester 120 50/10 41 77
Rusthoven 2009 USA Multicentric 47/63 60/3 16 95 92 1/47 2 %
Lee 2009 Toronto 68/143 27-60/6 10.8 71 7/63 10 %
Ambrosini 2009 Vicenza 27/ 25-60/3 13 85 0 0
Vautravers-Dewas 2010 Lille 42/62 40-45/3-4 14.3 90 86 1/42 2 %
Chang 2011 USA Multicentric 65/102 variabl
e/1-6 18 67 55 2 3%

36
CRCliver mets
CRCliver mets
N = 51
Local controldose
Survivaltumor size
N = 51
Local controldose
Survivaltumor size
p < 0,05
p < 0,05
p < 0,05
p < 0,05

37
Phase II : liver metastases from colorectal cancerPhase II : liver metastases from colorectal cancer
• 1 to 3 metastases
• Cumulative size < 10 cm
• No extra-hepatic disease
• 72 patients
• Multicentric international
• 3 x 15 Gy
• Primary objective = local control
• 1 to 3 metastases
• Cumulative size < 10 cm
• No extra-hepatic disease
• 72 patients
• Multicentric international
• 3 x 15 Gy
• Primary objective = local control

38
3 études ouvertes en Europe3 études ouvertes en Europe
ClinicalTrials.gov 2012-09-25
Condition Intervention Sponsor
France multicentric Ph II Liver mets
CRCConformal or SRT 4 X 10
Centre RenéGauducheau
PHRC
International Ph II Liver mets CRC
Robotic SRT 3 x 15 Gy Accuray
International Ph III Liver mets CRC RTS vs RFA U of Aarhus

39
Hepatocellular carcinomaHepatocellular carcinoma
• Surgery can be a curative optionsnevertheless only 15-35% of the patients are surgically resectable
• Some typical causes of inoperability are – the diffusion of the illness– the liver functional status– and the tumor position
• For those patients not suitable for resection, there are possible loco-regional techniques
– Radiofrequency– Percutaneous alcoholization– Chemoembolization– Cryotherapy
• Surgery can be a curative optionsnevertheless only 15-35% of the patients are surgically resectable
• Some typical causes of inoperability are – the diffusion of the illness– the liver functional status– and the tumor position
• For those patients not suitable for resection, there are possible loco-regional techniques
– Radiofrequency– Percutaneous alcoholization– Chemoembolization– Cryotherapy

40
Radiotherapy is efficient for HCCRadiotherapy is efficient for HCC
nb HCC
dose volume median
follow-up
median
local control
1y
local control
2y
survival1y
survival2y
remarks
Blomgren 1998 2030 Gy 2 or
3f 22 cm3 11 100% retrospective
Mendez 2006 11 25-37,5 Gy 22 cm3 12.9 75% 75% 75% 40% Ph I/II
Tse 2008 31 24-54 6f 73 cm3 17.6 65% 48% Ph I
Choi 2008 32 30-39 3f 25 cm3 17.3 71.90% 81% retrospective
Cardenes 2010 25 36-48 3f 34 cm3 24 100% 75% 60% Ph I
Mirabel 2010 48 45 Gy 3 f 73 cm3 15 90.50% 90.50% 72% 42% retrospective

41
Robotic stereotactic radiotherapy for 153 liver tumors
Robotic stereotactic radiotherapy for 153 liver tumors
0.00
0.25
0.50
0.75
1.00
Pro
babi
lity
0 6 12 18 24 30 36
Months
Relapse free survival – 153 targets
0.00
0.25
0.50
0.75
1.00
Pro
babi
lity
0 6 12 18 24 30 36
Months
Relapse free survival – 153 targets
0.00
0.25
0.50
0.75
1.00
Pro
babi
lity
0 6 12 18 24 30 36
Months
Relapse free survival – 153 targets
0.00
0.25
0.50
0.75
1.00
Pro
babi
lity
0 6 12 18 24 30 36
Months
Relapse free survival – 153 targets
HCC 48
Metastases 99
Cholangio… 6
Local control
1 year 84 %(CI 95% : 75.6 – 89.7%)
2 years 74.6 %(CI 95% : 63.7 – 82.7%)
HCC 48
Metastases 99
Cholangio… 6
Local control
1 year 84 %(CI 95% : 75.6 – 89.7%)
2 years 74.6 %(CI 95% : 63.7 – 82.7%)
42
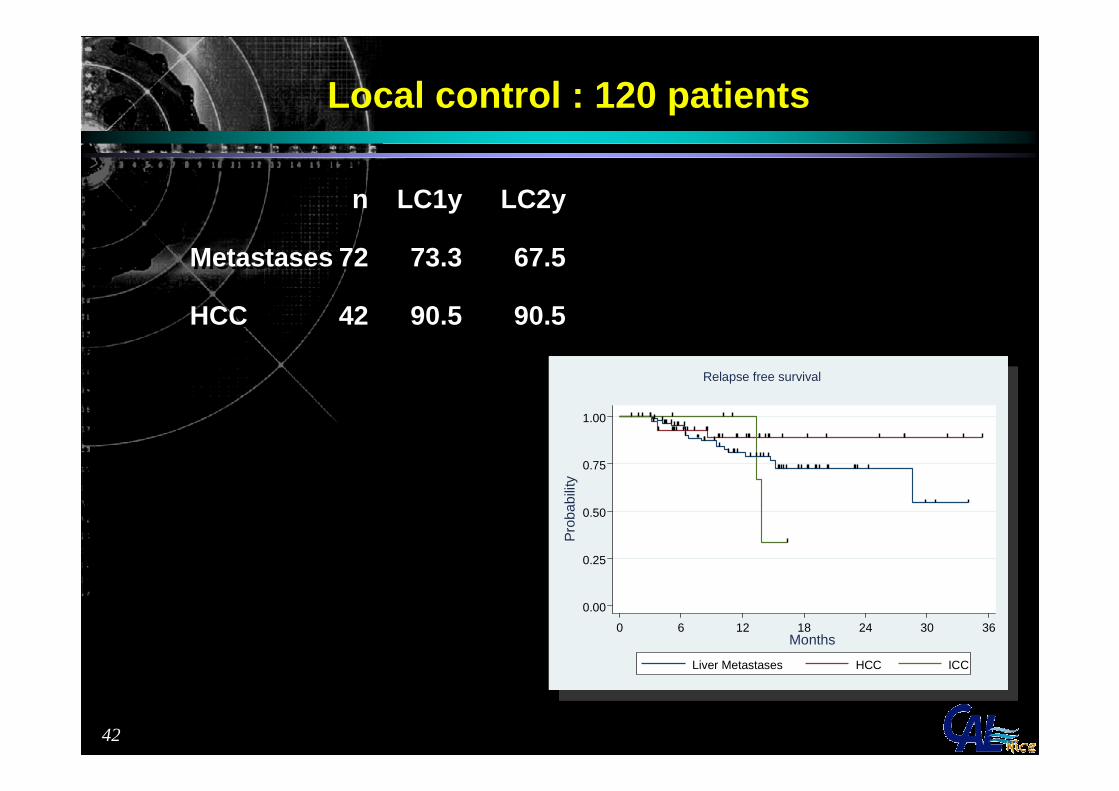
Local control : 120 patientsLocal control : 120 patients
0.00
0.25
0.50
0.75
1.00
Pro
babi
lity
0 6 12 18 24 30 36Months
Liver Metastases HCC ICC
Relapse free survival
0.00
0.25
0.50
0.75
1.00
Pro
babi
lity
0 6 12 18 24 30 36Months
Liver Metastases HCC ICC
Relapse free survival
0.00
0.25
0.50
0.75
1.00
Pro
babi
lity
0 6 12 18 24 30 36Months
Liver Metastases HCC ICC
Relapse free survival
0.00
0.25
0.50
0.75
1.00
Pro
babi
lity
0 6 12 18 24 30 36Months
Liver Metastases HCC ICC
Relapse free survival
n LC1y LC2y
Metastases 72 73.3 67.5
HCC 42 90.5 90.5
n LC1y LC2y
Metastases 72 73.3 67.5
HCC 42 90.5 90.5

43
Diameter < 5 cmp = 0,019
local control 1 year 2 years
< 5 cm 88 % 79 %
> 5 cm 75 % 63 %
Diameter < 5 cmp = 0,019
local control 1 year 2 years
< 5 cm 88 % 79 %
> 5 cm 75 % 63 %
Local control is size-relatedLocal control is size-related
44
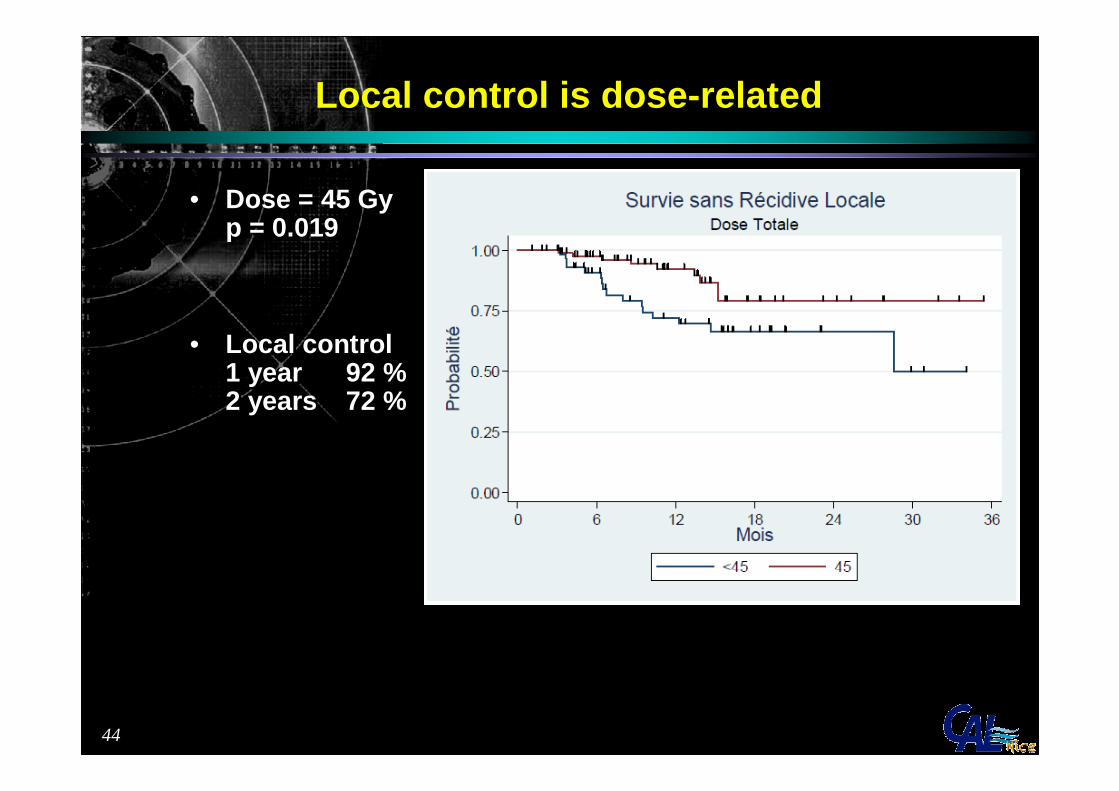
• Dose = 45 Gyp = 0.019
• Local control1 year 92 %2 years 72 %
• Dose = 45 Gyp = 0.019
• Local control1 year 92 %2 years 72 %
Local control is dose-relatedLocal control is dose-related

45
ConclusionConclusion
• La radiothérapie est un traitement curatif des métastases hépatiques
• Les techniques évoluent rapidement. C’est dorénavant un traitementde routine
• Inclure dans des études de Phase II pour consolider les résultats
• Aujourd’hui traitement de recours, son positionnement dans la stratégie thérapeutique va évoluer
• La radiothérapie est un traitement curatif des métastases hépatiques
• Les techniques évoluent rapidement. C’est dorénavant un traitementde routine
• Inclure dans des études de Phase II pour consolider les résultats
• Aujourd’hui traitement de recours, son positionnement dans la stratégie thérapeutique va évoluer

46
Stereotactic radiotherapy indications for liver tumors
Stereotactic radiotherapy indications for liver tumors
• HCC– 1 (or 2) lesions– N0 M0– Cirrhosis Child A or (B7-8)
• Liver metastases– 1 to 3 lesions– no other possibility of local treatment– resistance to chemotherapy or toxicity
• Possibility to implant and visualize the fiducials
• HCC– 1 (or 2) lesions– N0 M0– Cirrhosis Child A or (B7-8)
• Liver metastases– 1 to 3 lesions– no other possibility of local treatment– resistance to chemotherapy or toxicity
• Possibility to implant and visualize the fiducials

47
Limites de la RTS hépatiqueLimites de la RTS hépatique
• Fonction hépatique précaire
• Taille > 8-10 cm
• Nombre de lésions > 3
• Obésité
• Lésions volumineuses à proximité de l’estomac / duodénum
• Contre-indication à la pose des fiduciels– Ascite– Dilatation des voies biliaires
• Fonction hépatique précaire
• Taille > 8-10 cm
• Nombre de lésions > 3
• Obésité
• Lésions volumineuses à proximité de l’estomac / duodénum
• Contre-indication à la pose des fiduciels– Ascite– Dilatation des voies biliaires

48
Ne sont pas des limitesNe sont pas des limites
• Taille > 3-4 cm
• Proximité des vaisseaux ou des voies biliaires
• Thrombose porte
• Antécédents de chirurgie, de radiofréquence, de chimioembolisation
• Taille > 3-4 cm
• Proximité des vaisseaux ou des voies biliaires
• Thrombose porte
• Antécédents de chirurgie, de radiofréquence, de chimioembolisation
49
2 atouts de la RTS2 atouts de la RTS
• Simplicité de mise en œuvre– Traitement ambulatoire– Fiduciels +scan dosi + IRM + 3 séances
• Coût
• Simplicité de mise en œuvre– Traitement ambulatoire– Fiduciels +scan dosi + IRM + 3 séances
• Coût

50
Thank you for your attention
G. ANGELLIER (PhD)K. BENEZERY (MD)J. THARIAT (MD)G. PALAMINI (radiotherapist)L. MILAN (Secretary)B. GRANIER (Secretary)M. MAURIN (ACR) P.Y. BONDIAU (MD. PhD)


















