Kuvan ® the first ‘drug’ treatment for PKU
28
Kuvan Kuvan ® the first ‘drug’ the first ‘drug’ treatment treatment for PKU for PKU Peter Galloway Adult Metabolic Clinic Glasgow Royal Infirmary March 2010
description
Kuvan ® the first ‘drug’ treatment for PKU. Peter Galloway Adult Metabolic Clinic Glasgow Royal Infirmary March 2010. Chart plotting median PHE level for all patients diagnosed with PKU with any data since 2001. Average male PHE value. Average female PHE value. Upper recommended - PowerPoint PPT Presentation
Transcript of Kuvan ® the first ‘drug’ treatment for PKU

KuvanKuvan®® the first ‘drug’ treatment the first ‘drug’ treatment for PKUfor PKU
Peter GallowayAdult Metabolic Clinic
Glasgow Royal InfirmaryMarch 2010

•

0
200
400
600
800
1000
1200
1400
1600
0-5 6-10 11-15 16-20 21-30 31-40 40+
Patient age (years)
seru
m P
HE c
once
ntra
tion
(μm
ol/l)
Chart plotting median PHE level for all patients diagnosed with PKU with any data since 2001
Average male PHE value
Average female PHE value
Upper recommended PHE limit
Lower recommendedPHE limit
•45% control their PHE levels to within current guidelines (42% for males, 47% for females)

0
200
400
600
800
1000
1200
1400
0-5 6-10 11-15 16-20 21-30 31-40 40+
Patient age (years)
Seru
m P
HE c
once
ntra
tion
(μm
ol/l)
Chart plotting median lowest PHE level for all patients diagnosed with PKU with any data since
2001
Average lowest male PHE value
Average lowest female PHE value
Upper recommendedPHE limit
Lower recommendedPHE limit

Target blood Phe levels <360 mol/L
• Phe-restricted diet
•Large Neutral Amino Acids
• Gene therapy
• Enzyme replacement with rPAL
• Tetrahydrobiopterin (BH4)
TreatmentTreatment


Phenylalanine ammonia lyase• An enzyme found widely in yeasts and red-purple coloured
plants and used in the synthesis of anthocyanins. It breaks down phenylalanine to hydrocinnamic acid
• Can be extracted from plants or synthesised by engineered E. coli bacteria
• Could be used to break down phenylalanine in the intestine, preventing its absorption and allowing liberalisation of the diet
• Easily destroyed by gastric acid and attempts to engineer a robust protected source of PAL have been abortive over more than 15 years…..
• Recently subcutaneous injection of pegylated enzyme has been successful in a mouse model of PKU
• First human trials involving 25 individuals in 2009

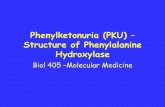
Tetrahydrobiopterin
HN
N
NH
NH
O
H2N
CH CH CH3OH OH


TetrahydrobiopterinTetrahydrobiopterin
• First reported 1963 by Kaufmann
– Proc. National Academy of Science, 1968: 5:1085-93
• and first suggested role in 1975.
– Journal of Biological Chemistry, 1975, 25: 4777-4781

In 1999• Kure reported 4 of 5 mild PKU, BH4
loading produced reductions in blood phenylalanine
Journal of Paediatrics, 1999: 135: 375-378

AvailabilityAvailability
• April 2009 – Launch of Kuvan
• Sapropterin licensed for use in Phenylketonuria in those over 4 years of age for the treatment of hyperphenylalaninaemia who have been shown to be responsive to such treatment.

Info:
• How is Kuvan taken?• Dose?
• 5-20 mg/kg body weight• 100 mg tablets• Dissolved in water and taken one per day
• 8 year old may need 1-4 tablets/day• Adult male may need 7-14 tablets/day

Blau & Erlandsen 2004
62% catalytic domain
21% regulatory domain
5% tetramerization
domain

Possible Mechanisms for the BH4-Responsiveness
• Km mutants with reduced affinity for BH4
• Chaperon-like activity of BH4
• Induction of PAH expression by BH4
• PAH mRNA stabilization
•Better assembly/stabilisationPossible Mechanisms for failure to respond
Truncated protein
Missing BH4 Binding Area

Tetrahydrobiopterin Loading Test in
Patients with Hyperphenylalaninemia
0
500
1000
1500
2000
0 4 8 12 24 48 72
20 mg/kg (BH4)
Hours
20 mg/kg
10 mg/kg
Bloo
d Ph
enyl
alan
ine
Bloo
d Ph
enyl
alan
ine
(( m
ol/L
)m
ol/L
)
PKU responderPKU responder
PKU non-responderPKU non-responder
BH4 def.BH4 def.

Burton et alPKU 001

Patients in PKU-003

PKU-003Absolute phenylalanine before and after BH4

PKU-003Change in phenylalanine with BH4

WHAT IS A RESPONSE
• > 30% reduction in phenylalanine
• While remaining on a constant protein intake
• Also need to be able to take an increased protein intake
• How long to show you respond?

Levy et al: test withBH4 10mg/kg/day for up to 28 days

Blau N: Guidelines for the definition of BH4 responsiveness should include the following
investigations…...
• Single loading test with 20 mg/kg BH4 and monitoring of phe at 0,8,12,(15?) and 24 hours
• Reduction of phe of over 20-30% an indicator for a trial of BH4 at initial doses of 10mg/kg/day over several weeks
• Titration of the individual BH4 requirement (5-20mg/kg/day)to maintain optimal phe levels
• Determination of the daily phenylalanine tolerance
• Genotyping

KUVAN
• Does it have other benefits than just reduction in levels?
• Not formally tested.
• Anecdotally – what does this mean?

Side-effects from Kuvan%
Diarrhoea 5 Abdominal pain 5 Nausea 3Flatulence 2Vomiting 2Decreased appetite 2Headache 10Fatigue 3Tremor 2
4 in 489 had severe SEs – migraine, headache, vomiting and low platelet count
No patient discontinued the study from side-effects.

Why not give to everyone?
Small proportion benefit – 1 in 5 30% reduction; 1 in 20 major dietary change
• Testing will be over a month – if don’t respond effect ?
• Could start based on genetic testing.
• Cost

Other Issues
• Age it should be started?• How long should it be continued?• e.g. Childhood/end of schooling Lifelong• If difficult complying with low protein diet,
– ? compliance with tablets.• Monitoring while on treatment• Other areas – pregnancy?

Current Progress -
• Where is Europe?
• Where is UK?
• What do you feel we should be doing?