KU Midwestern MUSIC Camp 2014
14
KU Midwestern MUSIC Camp 2014 Parent Handbook Jazz Workshop Please bring this guide with you for registration on Sunday and take it home with you for your reference. Quick Guide to Sunday, July 13 th (Registration/Check-in Day): Commuters also check in at Ellsworth Hall. Commuter students are free to go after theory placement and auditions are complete on Sunday afternoon. 10:00-12:00 Registration/Check in at Ellsworth Hall (1734 Engel Road) If you will be late, please make arrangements in advance with the camp office. Students with large instruments (rhythm section) may unload instruments at the Murphy Hall loading dock after registration. Please use the map and follow signs at Murphy Hall. 12:00-1:00 Lunch on your own 1:00-1:45 Opening Meeting/Faculty Recital at Murphy Hall 1 Room 130 (1530 Naismith Drive) We will introduce our faculty and staff and get students and parents oriented. 1:45-3:30 Auditions and Theory Placement Exam These are informal, one-at-a-time auditions to determine placement in ensembles. 3:30-5:00 Resident Campers meet in Murphy Hall Room 130; Commuter Campers are done for the day Commuter campers are done for the day but are encouraged to come back for the Ice Cream Social at 7:30 at Ellsworth Hall. 5:00-7:00 Dinner at the Mrs. E’s (1530 Engel Road) 7:00 Resident Camper Meeting at Ellsworth Hall Resident campers will meet with camp staff to go over rules and important information for the week. 7:30-9:30 Ice Cream Social – Ellsworth Hall (1734 Engel Road) 1 Residential Student’s parents are free to leave after the opening meeting, which is in Room 130 in Murphy Hall. Commuting Student’s parents, please stay until your child has completed auditions, after which time they are done for the day, but are welcome and encouraged to come back to the Ice Cream Social at 7:30 PM.
Transcript of KU Midwestern MUSIC Camp 2014

KU Midwestern MUSIC Camp 2014 Parent Handbook Jazz Workshop Please bring this guide with you for registration on Sunday and take it home with you for your reference.
Quick Guide to Sunday, July 13th
(Registration/Check-in Day): Commuters also check in at Ellsworth Hall. Commuter students are free to go after theory placement and auditions are complete on Sunday afternoon.
10:00-12:00 Registration/Check in at Ellsworth Hall (1734 Engel Road)
If you will be late, please make arrangements in advance with the camp office. Students with large instruments (rhythm section) may unload instruments at the Murphy Hall loading dock after registration. Please use the map and follow signs at Murphy Hall.
12:00-1:00 Lunch on your own
1:00-1:45 Opening Meeting/Faculty Recital at Murphy Hall1 Room 130 (1530 Naismith Drive)
We will introduce our faculty and staff and get students and parents oriented.
1:45-3:30 Auditions and Theory Placement Exam These are informal, one-at-a-time auditions to determine placement in ensembles.
3:30-5:00 Resident Campers meet in Murphy Hall Room 130; Commuter Campers are done for the day
Commuter campers are done for the day but are encouraged to come back for the Ice Cream Social at 7:30 at Ellsworth Hall.
5:00-7:00 Dinner at the Mrs. E’s (1530 Engel Road)
7:00 Resident Camper Meeting at Ellsworth Hall Resident campers will meet with camp staff to go over rules and important information for the week.
7:30-9:30 Ice Cream Social – Ellsworth Hall (1734 Engel Road)
1 Residential Student’s parents are free to leave after the opening meeting, which is in Room 130 in Murphy Hall. Commuting Student’s parents, please stay until your child has completed auditions, after which time they are done for the day, but are welcome and encouraged to come back to the Ice Cream Social at 7:30 PM.

Monday (14th) through Thursday (17th) Jazz Workshop Classes 9:00 AM – 5:00 PM Activities 7:00 PM – 9:30 PM
Commuters: Drop Off no later at 8:45 AM at the Murphy Hall Loading Dock
Pick-Up at 5:00 PM at the Murphy Hall Loading Dock Commuter students may bring their lunch or purchase lunch at Mrs. E’s for $9.50. We strongly encourage commuter students to stay for evening activities. Pick-up will be at 9:30 PM at the Murphy Hall Loading Dock.
Quick Guide to Thursday, July 17th
(Student Combo Concert Day): Commuters: Drop Off at 8:45 AM at the Murphy Hall Loading Dock Pick-Up directly after the concert
9:00-11:45 Classes and Rehearsals at Murphy Hall (1530 Naismith Drive)
12:00 – 1:15 Lunch (Mrs. E’s, 1530 Engel Road)
1:30 – 4:00 Classes and Rehearsals at Murphy Hall (1530 Naismith Drive)
4:00 – 6:00 Dinner (Mrs. E’s, 1530 Engel Road)
6:30 Student Combos Concert Murphy Hall, Room 130
(1530 Naismith Drive)
PARKING: Parents may park in any of the lots adjacent to Murphy Hall beginning at 5pm. Do not park in metered or handicap spots or you will be ticketed.
Quick Guide to Friday, July 18th
(Student Big Band Concert Day): Commuters: Drop Off at 8:45 AM at the Murphy Hall Loading Dock Pick-Up directly after the concert
9:00-11:45 Classes and Rehearsals at Murphy Hall (1530 Naismith Drive)
12:00 – 1:15 Lunch2 (Mrs. E’s, 1530 Engel Road)
1:30 Student Big Band Concert Murphy Hall, Room 130
(1530 Naismith Drive)
PARKING: Parents is available in the Allen Fieldhouse Parking Garage for $1.50 an hour. Do not park in campus lots, metered, or handicap spots or you will be ticketed. 2 Parents may collect their child’s belongings during check-out before the concert at Ellsworth Hall.

KU Midwestern MUSIC Camp 2014 For your reference:
Contacting your child If a resident, your child will receive a room phone number when s/he registers at the residence hall. Each room has a telephone jack but not a phone. The Ellsworth Hall front desk number is (785)- 864-4190 if you need to leave a message for your child. Any long distance calls made by the students from their rooms must be collect or by calling card. Campers will not regularly be in their rooms, at the desk, or in the Camp Office, so plan for your child to call you. Phone use is restricted after 10:00 PM for Jazz Workshop students. Students are permitted to have cell phones, however there are certain times when cell phones must be off: during classes, rehearsals, concerts, activities, and after 10:00 PM. Concert Dress There are no specific requirements for concert dress for the Jazz Workshop. Students should wear their comfortable camp clothing. Audition Results Audition results are posted at Murphy Hall and in Ellsworth Hall before the first rehearsal. Please see attached information regarding audition music. T-Shirts and Recordings T-shirts were available for pre-order for $15 each with the registration form, and will also be available for purchase during the week at camp. DVD recordings will be available for pre-order at the final concert. Meals All meals for campers are served at the Mrs. E’s. Commuters and guests may eat in the cafeteria, or may bring a sack lunch and stay in Murphy Hall for the lunch hour. Meal rates are as follows: $8.50, $9.50, $9.50 (breakfast, lunch, and dinner). Meal plans begin with dinner on Sunday and end with lunch on Friday. Health Care Health forms are located on the last six pages of this document. Please fill them out in advance and bring them with you to camp registration. These forms are required for camp attendance.
s Confidential Medical Record (1 page) Please complete and bring it to registration.
s Notice of Privacy Policy (2 pages) Please read this; you will need to sign an acknowledgement that you have done so on the next page.
s Consent Form (1 page) Please complete and bring it to registration.
s Treatment Agreement (1 page) Please complete and bring it to registration.
Campers needing non-emergency medical attention are taken to Watkins Health Center. Report health problems, chronic ailments, and continuing medications to your Resident Assistant/ Counselor when you check in. Watkins Health Center is on campus and open 8:00 AM-4:30 PM. Students requiring emergency medical attention will be taken to Lawrence Memorial Hospital. All charges for medical services are the responsibility of the camper and their parent/guardian.

KU Midwestern MUSIC Camp 2014 For your reference:
Photo Release Form Included in this packet is a release form to allow the Midwestern Music Camp and the University of Kansas to utilize pictures of your child in promotional materials for the Midwestern Music Camp. No names will be used in conjunction with any photographs. If you do not wish your child to be photographed during camp, please indicate “not approved” and do not sign the form.
Refunds There are no refunds for campers who leave early for homesickness, health, or other reasons.
Private Lessons A limited number of private lessons are available. Students may sign up for up to two lessons for the week. Private lessons are $30 per half hour; checks should be made payable to the individual instructor. Sign-up for lessons takes place during registration.
Lockers Lockers will be provided for students who require them at Murphy Hall. They will be assigned based on instrumentation. Parking Parking on the KU campus is by permit only and all parking rules are strictly enforced, Monday through Friday, 8AM – 5PM. Handicap, metered parking, and no-parking zones are strictly enforced 24 hours a day, 7 days a week. You are permitted to park in campus lots during Sunday’s activities and in the evenings after 5PM during the week (which includes Thursday evening’s concert). During the Friday afternoon concert, parking is available in the Allen Fieldhouse Parking garage for $1.50 an hour. If you do receive a parking ticket, it is your responsibility to pay the fine. The Midwestern Music Camp cannot be held responsible for parking tickets incurred. What To Pack Clothing: Bring neat, casual hot-weather attire with comfortable shoes for daily activities. T-shirts must reflect good taste and shorts are acceptable as long as they provide adequate coverage. For strapped shirts, follow the ‘two-finger rule‘: straps should be at least as wide as the index and middle fingers combined. Shirts must not show an inappropriate amount of skin. Open back shirts (i.e. halter tops) are not permitted. No undergarments should be visible for either boys or girls. A sweater, jacket, or sweatshirt is also recommended in case it gets chilly. Also, don’t forget concert attire (see above for details). Please note: there is a great deal of walking up and down hill every day. Be sure to bring comfortable shoes made for walking (i.e. sneakers) not just flip-flops or sandals. Your feet will thank you!
Linens: The residence hall does not provide linens. You must bring your own bedding, sheets, pillow, towels, and washcloths. Mattresses in Ellsworth Hall are extra-long twin. If you don't have an extra long twin sheet set, two regular (flat) twin sheets may be used, however a fitted sheet from a normal twin sheet set will not fit. Please note: mattress pads are not provided.
Toiletries: Make sure to bring your own soap, shampoo, toiletries, sunscreen, and shower shoes.

What To Pack (continued) Instruments and Music: Please don’t forget to bring your instrument and a folding music stand. Bring sufficient reeds, cork grease, valve oil, mutes, etc. All students must bring pencils and manuscript paper for the week. Drummers must bring their own drum sets, cymbals, sticks, brushes and mallets. Guitar/Bass Players must bring your own amps and patch cords. Smaller amps are encouraged as you may be required to move between different rooms for rehearsal. There will be secure, locked rooms to store your equipment. Please remember to bring your audition music. If you have a “real book” please bring those for our student jam sessions. Also, if you are planning on signing up for private lessons, you should bring music that you would like to work on. Make sure all equipment is labeled with your name on it!
Other Items: Here are a few other items that might be helpful to bring: an umbrella, hangers, alarm clock, reusable water bottle, healthy snacks, camera, playing cards, games, etc. Please note: the KU School of Music and the Midwestern Music Camp are not responsible for any lost or broken items. Students may also want to bring a small amount of cash for vending machines or laundry facilities.

KU Midwestern MUSIC Camp 2014 For your reference:
Jazz Workshop Auditions All Jazz Workshop auditions will consist of:
• A short excerpt or selection of any style of the student’s choice (jazz standard, classical etude, popular song, etc.)
• Scales • Sight reading as selected by faculty • A short improvised solo with a play-along CD (most likely 12-bar blues in B-flat or F; more
advanced students will be asked to play an additional selection) as provided by the faculty
Additional audition material for Rhythm Section Instruments:
• Demonstrate certain grooves as requested by faculty (i.e. drummers might be asked to play a “swing” groove, bass players may be asked to play a walking bass line over a chord progression, etc.)

Exit #202
To Topeka, West KS To KC Metro, MO
Interstate 70
McD
onal
d D
rive
Iow
a St
reet
/US
59
6th Street
9th Street
23rd Street/K-10
19th Street
Iow
a St
reet
/US
59
To Johnson County
Mas
sach
uset
ts S
tree
t
MurphyHall
EllsworthHall
15th Street
Nai
smith
Driv
e
Nai
smith
Driv
e
Irving Hill Road
Enge
l Roa
d
Cres
tline
Driv
e
Bob Billings
LiedCenter
KU Midwestern MUSIC Camp 2014Location Map
Cons
tant
Ave
nue
Research Circle
21st Street
NOTE: Construction is possible around the residence halls, (Engel and Irving Hill Roads) please allow extra time.
Parking
ParkingGarage
Irving Hill Road
To Ellsworth Hall
15th Street
Nai
smit
h D
rive
Nai
smit
h D
rive
Sunnyside Avenue
Sum
mer
field
Hal
l Dri
ve
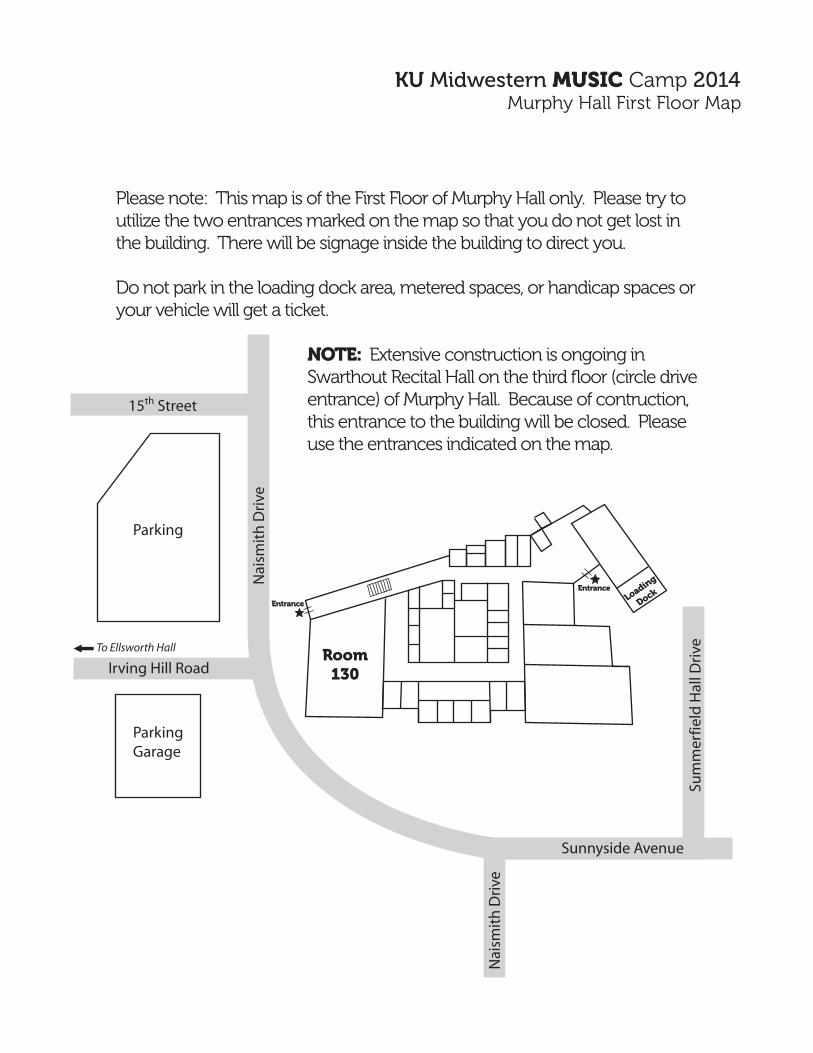
KU Midwestern MUSIC Camp 2014Murphy Hall First Floor Map
Room130
Loading
DockEntrance
Entrance
Please note: This map is of the First Floor of Murphy Hall only. Please try to utilize the two entrances marked on the map so that you do not get lost in the building. There will be signage inside the building to direct you.
Do not park in the loading dock area, metered spaces, or handicap spaces or your vehicle will get a ticket.
NOTE: Extensive construction is ongoing in Swarthout Recital Hall on the third floor (circle drive entrance) of Murphy Hall. Because of contruction, this entrance to the building will be closed. Please use the entrances indicated on the map.

KU Midwestern MUSIC Camp 2014 Photo and Information Release Form
Name of Camper: ______________________________________ Instrument or Voice: ____________________________________ Camp (check one):
❏ Middle School Music Camp ❏ High School Band/Choir/Orchestra Camp ❏ High School Jazz Workshop
As the parent or legal guardian of the minor child listed above, I hereby grant consent to the University of Kansas the right to use, display, distribute, and create derivative works of University-related photographs or videotaped images of my child for use in connection with the activities of the University of Kansas for promoting, publicizing or explaining its activities. This grant includes, without limitation, the right to publish such images in newspapers, magazines, PR/promotional materials, fund-raising materials, and any other University-related publication. These images may appear in any of the wide variety of formats, including hard copy and electronic/online media. I have read this document and understand its contents.
I give permission for the above: ❏ YES or ❏ NO ________________________________________________________ Printed Name of Parent or Legal Guardian ________________________________________________________ Signature of Parent or Legal Guardian ___________________________ Date

CONFIDENTIAL MEDICAL RECORD
Name of Camp: _________________________________
This completed form must accompany the camper on their first health center visit. It is essential that consent for treatment of a minor is signed by a parent or guardian.
Camper’s Name ____________________________________________ Birth Date_____________ Sex _______________________
Last______________________________________________________ First _________________ Middle_____________________
Parent Name _______________________________________________ Home Phone ____________________________________
Address ___________________________________________________________________________________________________ Street City, State Zip Person to notify in case of emergency, if other than above: Name _____________________________________________________ Day Phone ___________________ Night Phone__________________ Address _________________________________________ Name of Family Physician ____________________________________ Phone # _________________________________________ 1. Does camper have any significant illness or disability? YES NO If yes, please explain, __________________________
______________________________________________________________________________________________________ 2. Please check if camper has or has had any of the following: asthma chicken pox diabetes epilepsy kidney problems polio rheumatic fever tuberculosis other ______________________________________________________ 3. Has camper had any other significant illnesses, injuries, or surgeries? YES NO If yes, please explain _______________
______________________________________________________________________________________________________ 4. What routine medications & their dosages does the camper take? __________________________________________________
______________________________________________________________________________________________________ 5. Date of last tetanus/diphtheria: _________________________ Date of last MMR: ____________________________________
6. Is camper allergic to any medications? YES NO If yes, please list ___________________________________________
7. Does camper have any other allergies? YES NO If yes, please list ___________________________________________
______________________________________________________________________________________________
HEALTH INSURANCE BILLING INFORMATION
Please note: (1) if any charges are to be billed to an insurance company, a copy of the camp participant’s insurance card(s) must also be provided during the visit. (2) We cannot bill Medicare, Medicaid or Healthwave as we are not participating providers with these programs.
Insurance Company _________________________________________________________________________________________
Claim Form Address _________________________________________________________________________________________
I.D. No. ______________________ Group No. ___________________ Name of Policyholder ______________________________
Address of Policyholder ______________________________________________________________________________________
I hereby authorize Student Health Services to disclose to the above named insurance company, information from the camper’s medical record as needed in presenting my claim for benefits. Camper’s signature _________________________________________ Date ____________________________________________
Parent’s signature __________________________________________ Date ____________________________________________ __________________________________________________________________________________________________________
CONSENT FOR TREATMENT OF A MINOR I hereby give my consent for treatment of:___________________________________________________ _________________ Last First Middle Birth Date This authorization covers any procedure, which may be deemed advisable by the attending staff physician.
_____________________________________________________ __________________________ _________________ Signature of person authorized to give consent for camper treatment Relationship to camper Date AD 021-1 STUDENT HEALTH SERVICES REV. 03/07 THE UNIVERSITY OF KANSAS

care operations as described in this section. a. Treatment. Student Health Services will use and disclose medical information about you to provide and coordinate your health care and any related services. For example, the information will be used by all members of the staff that are involved in your treatment, including but not limited to physicians and nurses, to coordinate the different services you may need. In addition, your medical information may be provided to another health care provider, such as a physician or CAPS, to whom you have been referred to ensure that they have the necessary information to diagnose and treat you. Student Health Services may also contact you to tell you about possible treatment alternatives. b. Payment. Student Health Services will use and disclose medical information about you to bill and collect payment from you, your insurance company or a third party payer. For example, Student Health Services may need to give your insurance company information about your visit to determine coverage and/or coordinate payment for your treatment. If you have any questions regarding the privacy practices of your insurance company or third party payer, you should contact them directly. Student Health Services may respond to inquiries of a family member involved in
This section of the Notice of Privacy Practices (NPP) provides a brief summary of the privacy practices of Student Health Services and your privacy rights. Please read the entire document for a full description of our practices and your rights. If you need more information, you may call (785) 864-9525.Our responsibilities regarding your medical information.Each time you utilize Student Health Services, a record is generated. This record contains medical information about you. Student Health Services is required by law to protect the privacy of your medical information, provide you with the NPP, abide by the terms of the NPP currently in effect, and notify you if we are unable to agree to a requested restriction on use or disclosure of your medical information.Uses and Disclosures of Protected Health Information. a. You will be asked to sign a written consent that enables Student Health Services to use and disclose your medical information for treatment (such as sending medical information to a physician we refer you to or exchanging information with KU Counseling and Psychological Services [CAPS] if you are referred to them), payment (such as sending a bill to your insurance carrier), and operations (such as registering you for services). Student Health Services may also contact you regarding your appointments or prescriptions or to tell you about health-related benefits or services. In certain limited circumstances Student Health Services may disclose medical information about you to a friend or family member involved in your care. b. Under certain circumstances, uses and disclosures without your written consent or authorization may take place. For example, Student Health Services may disclose information about you when there is an emergency or a communication barrier, for public health purposes, for health oversight audits or inspections, as required by law, for research studies (as permitted by law), and for law enforcement/legal proceedings.Your Rights Regarding Your Medical Information.You have the right to inspect and copy your medical information, request an amendment of medical information you believe to be incorrect or incomplete, request an accounting of non-routine disclosures, request restrictions on uses and disclosures, request special confidential communications, and receive a written copy of this NPP. You may file a complaint by contacting our Privacy Officer at 864-9525. Student Health Services reserves the right to make changes to this NPP. Any changes will be posted in Watkins Memorial Health Center and on our website www.studenthealth.ku.edu.
this notice describes how medical information about you may be used and disclosed and how you can get access to this information. please review it carefully.
paying for your care by providing them with very limited information, but not specific details regarding your care. We will share only an amount owed and that it was for a medical visit or prescription, but not the type of visit or medication dispensed. c. Health Care Operations. Student Health Services will use and disclose medical information about you to schedule and coordinate your health care and related services. Student Health Services may disclose information to doctors, nurses, medical students, and/or residents for educational purposes. Members of Student Health Services staff involved in quality improvement may use information in your health record to assess the care and outcomes in your case and others like it. For example, Student Health Services may analyze medical information about many patients to evaluate the need for new services, resources, or treatment and to see where we can make improvements. The results will then be used to continually improve the quality of care for all patients we serve. If you are a student at the University of Kansas, Student Health Services may release limited medical information to authorized staff of the University to verify receipt of certain tests or vaccinations required for you to be enrolled at the University or in a specific field of study.
Watkins MeMorial HealtH Center student HealtH serviCes 02/08/10 tHe university of kansas
NOTICE OF PRIVACY PRACTICESstudent health services
Effective Date: February 8, 2010
Each time you visit Student Health Services, a record of your visit is made. This record typically contains medical information about you, including information regarding symptoms, observations, assessments (including test results, diagnoses, treatment, and mental health), a plan for future care or treatment, and billing-related information. This NPP describes how Student Health Services may use and disclose your medical information. It also describes your rights and our responsibilities regarding the use/disclosure of your medical information. This NPP applies to all of the records of your care generated by Student Health Services.
Student Health Services is required by law to protect the privacy of your medical information, provide you with this NPP, abide by the terms of the NPP currently in effect, and notify you if it is unable to agree to a requested restriction on use or disclosure of your medical information.1. uses and disclosures with your written
consentYou will be asked to sign a written consent form enabling Student Health Services to use and disclose your medical information for treatment, payment, and health
OUR RESPONSIBILITIES REGARDING YOUR MEDICAL
INFORMATION

Student Health Services may also contact you to remind you that you have an appointment, to tell you that your appointment has been cancelled or to let you know that your prescription is ready, to assess your satisfaction with our services, to tell you about health-related benefits or services, or to complete the process of registering you for services. d. Other Related Uses and Disclosures. Student Health Services may use and/or disclose medical information: · To business associates, when we have contracted out for services, so that they can perform the job we’ve asked them to do, and to bill you or your third party payer for services rendered; · To a friend or family member who is involved in your care. If you are not present and able to agree or object, such communications shall be made only by authorized healthcare providers when, in their professional judgment, such disclosure is in your best interest.
2. uses and disclosures without your consent or authorization
In certain situations, Student Health Services may use or disclose medical information about you without your consent or authorization, for example, when there is an emergency or when there are substantial communication barriers to obtaining consent from you. Further, Student Health Services may use or disclose your medical information without your consent or authorization in the following circumstances: a. As Required by Law. Student Health Services may use and disclose medical information to the following types of entities, including but not limited to: · Food and Drug Administration · Public health authorities or legal
authorities charged with tracking, preventing or controlling diseases (e.g., STDs, HIV), injuries or disabilities
· Workers compensation agents · Military command, national security
or intelligence authorities · Health oversight agencies
b.Law Enforcement/Legal Proceedings. Student Health Services may disclose health information for law enforcement purposes as required by law or in response to a valid subpoena or other legal process. c.Research. Student Health Services may disclose medical information to researchers when their research has been approved by an institutional review board
NOTICE OF PRIVACY PRACTICES
request unless the information is needed to provide you emergency treatment. To request restrictions, you must make your request in writing on a form that Student Health Services will provide to you. · Right to Request Confidential Communications. You have the right to request that Student Health Services communicate with you about medical matters in a certain way or at certain locations. You must make your request in writing on a form that Student Health Services will provide to you. Student Health Services will accommodate all reasonable requests. · Right to a Paper Copy of This Notice. You have the right to obtain a paper copy of this NPP, and you may ask Student Health Services to give you a copy of this NPP at any time. You may obtain a copy of this NPP at our website www.ku.edu/~shs/. You may obtain a copy of the forms mentioned above by contacting the Records and Registration Department at 864-9500.
If you believe your privacy rights have been violated, you may file a complaint with Student Health Services by contacting the Privacy Officer for Student Health Services at (785) 864-9525 or by contacting the University’s HIPAA Privacy Officer, Lawrence Campus, at (785) 864-9528. You may also contact the Secretary of Health and Human Services. There will be no retaliation for filing the complaint.
Student Health Services reserves the right to change this NPP and the revised NPP will be effective for information Student Health Services already has about you as well as information received in the future. Should our practices change, Student Health Services will post a revised NPP on the Student Health Services website and in the facility where you receive services. Paper copies will be available upon request.
If you have any questions about this notice, please contact our Privacy Officer at (785) 864-9525.
that has reviewed the research proposal and established protocols to ensure the privacy of your medical information.
3. other uses and disclosures of medical information based on your authorization.
Other uses and disclosures of medical information not covered by this NPP or by the laws that apply to Student Health Services, will be made only with your written permission. If you provide Student Health Services with permission to use or disclose medical information about you, you may revoke that permission, in writing, at any time.
You have the following rights regarding medical information we maintain about you: · Right To Inspect and Copy. You have the right to inspect and have copied medical information used to make decisions about your care. Usually, this includes medical and billing records, but does not include some records such as psychotherapy notes. Your request must be submitted in writing on a form Student Health Services will provide to you. A fee may be charged for the costs of processing your request. · Right To Amend. If you feel that medical information Student Health Services has about you is incorrect or incomplete, you may ask us to amend the information. To request an amendment to your record, you must submit your request in writing on a form Student Health Services will provide to you. You will be asked to provide a reason to support the request. · Right to an Accounting of Disclosures. You have the right to receive a list of disclosures. This list will not include all disclosures made. For example, this list will not include disclosures for treatment, payment, health care operations, disclosures made prior to April 14, 2003, or disclosures you specifically authorized. To request this list you must submit your request in writing on a form Student Health Services will provide to you. · Right to Request Restrictions. You have the right to request a restriction or limitation on the medical information Student Health Services uses or discloses about you for treatment, payment or health care operations. Student Health Services is not required to agree to your request. If the request is approved, Student Health Services will comply with your
QUESTIONS AND INFORMATION
CHANGES TO THIS NOTICE
COMPLAINTS
YOUR RIGHTS REGARDING YOUR MEDICAL
Watkins MeMorial HealtH Center student HealtH serviCes 02/08/10 tHe university of kansas

CONSENT FOR THE USE OR DISCLOSURE OF HEALTH INFORMATION FOR TREATMENT, PAYMENT OR HEALTH CARE OPERATIONS
In our Notice of Privacy Practices (NPP) we provide you information about how Student Health Services can use or disclose your medical information. As described in our NPP, we request your consent for any use or disclosure of medical information to carry out treatment, payment, or health care operations. You have a right to review our NPP before signing this Consent. By signing this Consent form, you: (1) Acknowledge that a copy of the NPP has been provided to you; and (2) Consent to our use and disclosure of your health information for treatment, payment, or health care operations, as described in the NPP. You have the right to revoke this Consent in writing at any time, except where we have already used or disclosed your health information in reliance upon this Consent. ________________________________________ _____________________________ Patient’s Name (Printed) KUID ________________________________________ _____________________________ Signature of Patient or Personal Representative Date Personal Representative’s relationship to Patient: ________________________________________ Personal Representative’s Address and Phone Number:
___________________________________________
___________________________________________
___________________________________________
___________________________________________
............................................................... DOCUMENTATION OF GOOD FAITH EFFORT
Check the applicable box showing Good Faith Effort.
Emergency situation. Provide patient with copy of NPP as soon as reasonably practicable after the
emergency treatment situation.
Patient/Legal representative given NPP, but declines to acknowledge receipt.
Patient/Legal Representative states that they have already received the NPP.
Other: ____________________________________________________________________ ________________________________________ ________________ Employee Name (Printed) Date ________________________________________ Signature of Employee AD-309-1 STUDENT HEALTH SERVICES 04-16-09 THE UNIVERSITY OF KANSAS
PLACE LABEL HERE
PLEASE DO NOT WRITE BELOW THIS LINE

TREATMENT AGREEMENT STUDENT HEALTH SERVICES AT THE UNIVERSITY OF KANSAS
AD-410-1 STUDENT HEALTH SERVICES R- 8/25/11 THE UNIVERSITY OF KANSAS
CONSENT TO TREATMENT 1. I hereby consent to such health care as may be deemed necessary by the Student Health Services (SHS) providers including x-ray examination,
lab tests, administration of medications, and any other diagnostic or therapeutic treatments. 2. I understand that under some circumstances, an additional lab test (called a “reflex test) may be necessary due to an initial lab result and that I
am consenting to such tests as part of the standard of care. (This reflex test is usually done without the need for a return visit or additional specimen.) My provider will explain when these tests may be needed.
3. I understand that SHS is a teaching health facility and that students and residents acting under the supervision of licensed clinical staff may observe or be involved in my care. I understand that I may decline such involvement by the student or resident.
4. I understand that persons involved in SHS operations who are in the area during my patient care experience (e.g. SHS administrative staff or surveyors, building maintenance staff, or medical equipment surveyors) may receive incidental knowledge of my care. I further understand that these individuals are bound by the same confidentiality regulations as the SHS providers.
GENERAL CONDITIONS FOR TREATMENT BY STUDENT HEALTH SERVICES 5. I understand that I should fully participate in my care by asking any questions about my condition or treatment and that I should provide
complete and accurate information to the best of my ability about my health, including all medications and over-the-counter products and dietary supplements and any allergies and sensitivities. I understand that I must follow the treatment plan prescribed by my provider.
6. I understand that SHS is not responsible for loss or damage to clothing, jewelry or other valuables in my possession. 7. I acknowledge that the use of any video capturing devices (cameras, cell phones, etc.) by other than authorized personnel for official business
is prohibited. 8. I understand that if I have tests or services performed at SHS which are ordered by an outside provider, the reports on those services will be
sent to the ordering provider and will be included in my SHS medical record. I further understand that it is my responsibility to follow-up with the outside provider concerning those results.
9. I acknowledge that it is my responsibility to provide a responsible adult to remain with me during treatment and transport me home from this facility if required by my provider.
10. It is my responsibility to inform my provider about any living will, medical power of attorney, or other directive that could affect my care. 11. I understand that treatment / services will not be provided while I am using a cell phone. 12. I will be respectful of all the healthcare providers and staff in Student Health Services, as well as other patients. INSURANCE ASSIGNMENT 13. I hereby assign all benefits payable under the terms of my insurance policy/healthcare coverage to SHS, and I authorize payment directly to
SHS for any claim filed on my behalf or on the behalf of the person for whom I am duly authorized to sign for insurance benefits. I understand that if my healthcare coverage changes, I am to notify SHS Business Office.
ACKNOWLEDGEMENT OF FINANCIAL RESPONSIBILITY 14. I understand that if I am enrolled as a part-time student or otherwise had part or all of my Health Fee waived I will be charged the unpaid
amount of the Health Fee in order to receive patient care. 15. I understand that SHS does not contract with all insurance companies and it is my responsibility to know if my insurance plan
provides coverage for SHS services or requires a referral or pre-approval for such services. 16. Further, I understand that SHS is not a contracting provider for and cannot bill Medicare, Medicaid, or Healthwave. If I have
these types of government healthcare benefits, I am responsible for paying all SHS charges and it is my responsibility to seek reimbursement from these programs.
17. I understand that I am financially responsible to SHS for any charges, co-pays and deductibles not covered by my insurance company/health plan. And, I understand that if I do not pay my bill within 120 days of my date of service, my overdue account will be sent to the University’s Bursar for collection.
18. If I do not want my insurance company/health plan billed or a statement sent for charges, it is my obligation to immediately advise the SHS Business Office. I understand that I may address any questions concerning my charges, coverage, billing or payments, to the SHS Business Office.
19. I understand if I make an appointment and then fail to keep the appointment without notifying SHS I will be assessed a fee for “Did Not Keep Appointment” (DNKA), also known as a “no show” fee.
A copy of this document shall be as valid as the original. ___________________________________ Date: ____________ KU ID# ___________________ Print Patient Name ___________________________________ _______________________________________________ Signature (Patient, Agent or Representative) Relationship to Patient ___________________________________ Print Name of Agent or Representative
Patient Label