Kraig Wasik OMS V¹; Carly Ann Crider OMS IV¹; Tobin Rummel ...
1
] ABSTRACT INTRODUCTION: Low back pain (LBP) remains the primary cause of disability in the United States. Etiologies include muscular as well as postural imbalances in the lower extremities. Various muscular firing patterns in the lower extrem- ity have been described in the osteopathic, physical therapy, and kinesiology literature. This observational study aims to investigate whether there is a pal- pable atypical muscle firing pattern associated with prone hip extension (PHE) in patients suffering from LBP. METHODS: 28 volunteers were recruited from a community osteopathic ma- nipulative medicine practice. Participants were asked about the presence or absence of LBP. Blinded examiners assessed PHE firing patterns bilaterally using palpation. RESULTS: Data was analyzed for left and right sidedness independently. A two tailed Fishers Exact Test was used to compare typical vs atypical muscle firing patterns and LBP vs no LBP. No statistically significant relationship between PHE firing pattern and low back pain (Left side, p=0.6056; Right side p=0.1720) was identified. Significant variability was observed in muscular firing patterns with poor correlation between abnormal PHE and low back pain symptoms. CONCLUSION: This study did not find a significant association between PHE firing patterns and LBP. OBJECTIVE The purpose of this observational study was to determine whether there was a palpable abnormal muscle firing pattern associated with prone hip extension in patients suffering from low back pain. INTRODUCTION Low back pain (LBP) poses a significant medical, psychosocial and economic burden with a 40% lifetime prevalence of LBP worldwide, with some estimates as high as 85%. Newer data suggest that 24-50% of patients will suffer from LBP. Presently, it is the leading cause of years lost to disability (YLD) and the primary cause of disability for 7.6 million U.S. adults. Estimated costs in the U.S. for health care related services are reported to be upwards of 50 billion dollars per year. Prone hip extension (PHE) has been used as a surrogate to assess muscular firing in the lower extremity as LBP has been associated with alterations in muscular firing. Vladimir Janda described the typical PHE muscular firing pattern as: hamstrings, gluteus maximus, contralateral erector spinae, and ipsilateral erector spinae. Others have found different firing patterns and it has been argued that there may not be a single normal pattern. RESULTS The study found that palpable abnormal muscle firing patterns were not satisi- cally significantly associated with PHE in patients suffering from LBP. Right sided P value: 0.1720 Left sided P value: 0.6056 DISCUSSION This study sought to correlate atypical PHE muscle firing patterns with symp- toms of lower back pain. There was not a statistically significant relationship between LBP and atypical firing patterns (B-X from Table 1) on either the right or left side. Multiple firing patterns were seen in subjects without LBP (16/24 possible) and had variable predominant patterns bilaterally. A limited number of patterns were seen in subjects with LBP (5/24). Data argues against a single typical PHE muscle firing pattern in healthy adults. This supports other authors who have shown a lack of consistent firing pattern in prone hip extension. These findings suggests that the firing pattern order may not be as important with re- gards to LBP. Lack of muscle strength or lack of firing in theory could be more pathological in regards to LBP. It has been theorized that low back and sacroiliac pain may be caused at least in part due to muscular imbalance. These imbalances result in a phenomenon known by Janda called pseudoparesis. This study was limited by a small sample size (n=28). All patients were already under going OMT resulting in likely over representation of musculoskeletal dysfunction even in the absence of low back pain symptoms. Additionally, limi- tations including reliance on the palpatory skills of the investigators, which are inherintly subjective, and may have become more sensitive over time. CONCLUSION This observational study did not show any significance with regards to prone hip extension muscle firing patterns and low back pain. Future research should aim to include a more in depth study on the etiology of low back pain, as well as further investigation of the validitity in muscle firing patterns. ACKNOWLEDGEMENTS The NMM/OMM department at Western University, the staff, patients and providers of Crossroads PHC, and special thanks to Dr’s Janice Blumer and Michael Seffinger MUSCULAR FIRING PATTERN AND LOWER BACK PAIN IRB APPROVAL 16/ RFD/002 Kraig Wasik OMS V¹; Carly Ann Crider OMS IV¹; Tobin Rummel DO²; Sandra Sleszynski DO, FAAO² ¹ Western University of Health Sciences, College of Osteopathic Medicine of the Pacific - Northwest, 200 Mullins Ave, Lebanon, OR 97355. ² Crossroads Premiere Health Care, 1760 SW Third St, Corvallis, OR 97333. METHODS Data was collected over 1 week at Crossroads Premiere Health Care. The 28 study participants were asked about current symptoms of LBP on a researcher generated questionnaire. The evaluating researcher was blinded from this information. Patients were positioned prone with feet off the end of the treatment table. They were then instructed to extend at the hip. Set up for palpation of PHE: Stand on ipsilateral leg with hand placement as follows: • Caudal 5th digit: Ipsilateral hamstring (1) • Caudal 1st digit: Ipsilateral gluteus maximus (2) • Cephalad 1st digit: Ipsilateral erector spinae (4) • Cephalad 2nd-4th digit: Contralateral erector spinae (3) Typical Atypical 2 7 3 16 FIGURE 2: FREQUENCY OF LEFT SIDED PRONE HIP EXTENSION FIRINGPATTERN AND RELATIONSHIP TO LBP Back Pain No Back Pain Figure 2: Left sided PHE typical vs atypical mus- cle firing patterns and relation to LBP. Typical fir- ing pattern is defined in Table 1 as “A.” Figure 1: Right sided PHE typical vs atypical mus- cle firing patterns and relation to LBP. Typical fir- ing patterns defined in Table 1 as “A.” Typical Atypical 5 4 3 16 FIGURE 1: FREQUENCY OF RIGHT SIDED PRONE HIP EXTENSION FIRINGPATTERN AND RELATIONSHIP TO LBP Back Pain No Back Pain Table 1 : Firing Pattern Sequence The following short-hand was used for each muscle: (1) hamstring, (2) gluteus maxi- mus, (3) contra- lateral erector spinae, and (4) ip- silateral erector spinae. The firing Table 1: Firing Pattern Sequences REFRENCES 1. Manchikanti L, Singh V, Falco FJE, Benyamin RM, Hirsch JA. Epidemiology of low back pain in Adults. Neuromodulation. 2014;17(S2):3-10. doi:10.1111/ner.12018. 2. Becker A, Held H, Redaelli M, et al. Low back pain in primary care: costs of care and prediction of future health care utilization. Spine (Phila Pa 1976). 2010;35(18):1714- 1720. doi:10.1097/BRS.0b013e3181cd656f. 3. Chou R, Qaseem A, Snow V, et al. Diagnosis and Treatment of Low Back Pain : A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147(July):478-494. doi:10.7326/0003-4819-147-7-200710020-00006. 4. Ma VY, Chan L, Carruthers KJ. Incidence, prevalence, costs, and impact on disability of common conditions requiring rehabilitation in the united states: Stroke, spinal cord injury, traumatic brain injury, multiple sclerosis, osteoarthritis, rheumatoid arthritis, limb loss, and back pa. Arch Phys Med Rehabil. 2014;95(5):986-995.e1. doi:10.1016/j. apmr.2013.10.032. 5. Murray CJL. The State of US Health, 1990-2010. JAMA J Am Med Assoc. 2013;310(6):591-608. doi:10.1001/jama.2013.13805.Dagenais S, Caro J, Haldeman S. A system- atic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008;8(1):8-20. doi:10.1016/j.spinee.2007.10.005. 6. Greenman PE. Principles of Manual Medicine. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2003. Janda V, Frank CC, Liebenson C. Evaluation of Muscular Imbalance. In: Rehabilitation of the Spine: A Practitioner’s Manual. 2nd ed. Baltimore: Lippincott Williams & Wilkins; 2006:97-112. 7. Janda V. On the concept of postural muscles and posture in man. Aust J Physiother. 1983;29(3):83-84. doi:10.1016/S0004-9514(14)60665-6. 8. Singer KP. A new musculoskeletal assessment in a student population. J Orthop Sports Phys Ther. 1986;8:34-41. 9. Sakamoto ACL, Teixeira-Salmela LF, Paula-Goulart FR, Faria CDCM, Guimarães CQ. Muscular activation patterns during active prone hip extension exercises. J Eletcro- myography Kinesiol. 2009;19:105-112. doi:10.1016/j.jelekin.2007.07.004 10. Nygren Pierce M, Lee W a. Muscle firing order during active prone hip extension. J Orthop Sports Phys Ther. 1990;12(July):2-9. 11. Lehman GJ, Lennon D, Tresidder B, Rayfield B, Poschar M. Muscle recruitment patterns during the prone leg extension. BMC Musculoskelet Disord. 2004;5:3. doi:10.1186/1471- 2474-5-3 Letter Order A 1234 B 1243 C 1324 D 1342 E 1432 F 1423 G 2134 H 2143 I 2341 J 2314 K 2413 L 2431 M 3124 N 3142 O 3214 P 3241 Q 3412 R 3421 S 4123 T 4132 U 4213 V 4231 W 4312 X 4321
Transcript of Kraig Wasik OMS V¹; Carly Ann Crider OMS IV¹; Tobin Rummel ...

]
ABSTRACTINTRODUCTION: Low back pain (LBP) remains the primary cause of disability in the United States. Etiologies include muscular as well as postural imbalances in the lower extremities. Various muscular firing patterns in the lower extrem-ity have been described in the osteopathic, physical therapy, and kinesiology literature. This observational study aims to investigate whether there is a pal-pable atypical muscle firing pattern associated with prone hip extension (PHE) in patients suffering from LBP. METHODS: 28 volunteers were recruited from a community osteopathic ma-nipulative medicine practice. Participants were asked about the presence or absence of LBP. Blinded examiners assessed PHE firing patterns bilaterally using palpation. RESULTS: Data was analyzed for left and right sidedness independently. A two tailed Fishers Exact Test was used to compare typical vs atypical muscle firing patterns and LBP vs no LBP. No statistically significant relationship between PHE firing pattern and low back pain (Left side, p=0.6056; Right side p=0.1720) was identified. Significant variability was observed in muscular firing patterns with poor correlation between abnormal PHE and low back pain symptoms. CONCLUSION: This study did not find a significant association between PHE firing patterns and LBP.
OBJECTIVEThe purpose of this observational study was to determine whether there was a palpable abnormal muscle firing pattern associated with prone hip extension in patients suffering from low back pain.
INTRODUCTIONLow back pain (LBP) poses a significant medical, psychosocial and economic burden with a 40% lifetime prevalence of LBP worldwide, with some estimates as high as 85%. Newer data suggest that 24-50% of patients will suffer from LBP. Presently, it is the leading cause of years lost to disability (YLD) and the primary cause of disability for 7.6 million U.S. adults. Estimated costs in the U.S. for health care related services are reported to be upwards of 50 billion dollars per
year.
Prone hip extension (PHE) has been used as a surrogate to assess muscular firing in the lower extremity as LBP has been associated with alterations in muscular firing. Vladimir Janda described the typical PHE muscular firing pattern as: hamstrings, gluteus maximus, contralateral erector spinae, and ipsilateral erector spinae.
Others have found different firing patterns and it has been argued that there may not be a single normal pattern.
RESULTSThe study found that palpable abnormal muscle firing patterns were not satisi-cally significantly associated with PHE in patients suffering from LBP.
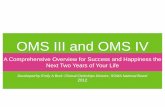
Right sided P value: 0.1720 Left sided P value: 0.6056
DISCUSSIONThis study sought to correlate atypical PHE muscle firing patterns with symp-toms of lower back pain. There was not a statistically significant relationship between LBP and atypical firing patterns (B-X from Table 1) on either the right or left side.
Multiple firing patterns were seen in subjects without LBP (16/24 possible) and had variable predominant patterns bilaterally. A limited number of patterns were seen in subjects with LBP (5/24). Data argues against a single typical PHE muscle firing pattern in healthy adults. This supports other authors who have shown a lack of consistent firing pattern in prone hip extension. These findings suggests that the firing pattern order may not be as important with re-gards to LBP. Lack of muscle strength or lack of firing in theory could be more pathological in regards to LBP.
It has been theorized that low back and sacroiliac pain may be caused at least in part due to muscular imbalance. These imbalances result in a phenomenon known by Janda called pseudoparesis.
This study was limited by a small sample size (n=28). All patients were already under going OMT resulting in likely over representation of musculoskeletal dysfunction even in the absence of low back pain symptoms. Additionally, limi-tations including reliance on the palpatory skills of the investigators, which are inherintly subjective, and may have become more sensitive over time.
CONCLUSIONThis observational study did not show any significance with regards to prone hip extension muscle firing patterns and low back pain.
Future research should aim to include a more in depth study on the etiology of low back pain, as well as further investigation of the validitity in muscle firing patterns.
ACKNOWLEDGEMENTSThe NMM/OMM department at Western University, the staff, patients and providers of Crossroads PHC, and special thanks to Dr’s Janice Blumer and Michael Seffinger
MUSCULAR FIRING PATTERN AND LOWER BACK PAIN IRB APPROVAL 16/RFD/002
Kraig Wasik OMS V¹; Carly Ann Crider OMS IV¹; Tobin Rummel DO²; Sandra Sleszynski DO, FAAO²
¹ Western University of Health Sciences, College of Osteopathic Medicine of the Pacific - Northwest, 200 Mullins Ave, Lebanon, OR 97355.
² Crossroads Premiere Health Care, 1760 SW Third St, Corvallis, OR 97333.
METHODSData was collected over 1 week at Crossroads Premiere Health Care. The 28 study participants were asked about current symptoms of LBP on a researcher generated questionnaire. The evaluating researcher was blinded from this information.
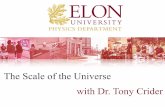
Patients were positioned prone with feet off the end of the treatment table. They were then instructed to extend at the hip. Set up for palpation of PHE:Stand on ipsilateral leg with hand placement as follows:
• Caudal 5th digit: Ipsilateral hamstring (1)• Caudal 1st digit: Ipsilateral gluteus maximus (2)• Cephalad 1st digit: Ipsilateral erector spinae (4)• Cephalad 2nd-4th digit: Contralateral erector spinae (3)
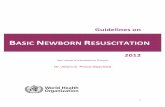
Typical Atypical
2
7
3
16
FIGURE 2: FREQUENCY OF LEFT SIDED PRONE HIP
EXTENSION FIRING PATTERN AND RELATIONSHIP TO LBP
Back Pain No Back Pain
Figure 2: Left sided PHE typical vs atypical mus-cle firing patterns and relation to LBP. Typical fir-ing pattern is defined in Table 1 as “A.”
Figure 1: Right sided PHE typical vs atypical mus-cle firing patterns and relation to LBP. Typical fir-ing patterns defined in Table 1 as “A.”
Typical Atypical
5 43
16
FIGURE 1: FREQUENCY OF RIGHT SIDED PRONE HIP
EXTENSION FIRING PATTERN AND RELATIONSHIP TO LBP
Back Pain No Back Pain
Table 1 : Firing Pattern SequenceThe following short-hand was used for each muscle: (1) hamstring, (2) gluteus maxi- mus, (3) contra-lateral erector spinae, and (4) ip-silateral erector spinae. The firing
Table 1: Firing Pattern Sequences
REFRENCES1. Manchikanti L, Singh V, Falco FJE, Benyamin RM, Hirsch JA. Epidemiology of low back pain in Adults. Neuromodulation. 2014;17(S2):3-10. doi:10.1111/ner.12018.2. Becker A, Held H, Redaelli M, et al. Low back pain in primary care: costs of care and prediction of future health care utilization. Spine (Phila Pa 1976). 2010;35(18):1714-1720. doi:10.1097/BRS.0b013e3181cd656f.3. Chou R, Qaseem A, Snow V, et al. Diagnosis and Treatment of Low Back Pain : A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147(July):478-494. doi:10.7326/0003-4819-147-7-200710020-00006.4. Ma VY, Chan L, Carruthers KJ. Incidence, prevalence, costs, and impact on disability of common conditions requiring rehabilitation in the united states: Stroke, spinal cord injury, traumatic brain injury, multiple sclerosis, osteoarthritis, rheumatoid arthritis, limb loss, and back pa. Arch Phys Med Rehabil. 2014;95(5):986-995.e1. doi:10.1016/j.apmr.2013.10.032.5. Murray CJL. The State of US Health, 1990-2010. JAMA J Am Med Assoc. 2013;310(6):591-608. doi:10.1001/jama.2013.13805.Dagenais S, Caro J, Haldeman S. A system-atic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008;8(1):8-20. doi:10.1016/j.spinee.2007.10.005.6. Greenman PE. Principles of Manual Medicine. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2003.Janda V, Frank CC, Liebenson C. Evaluation of Muscular Imbalance. In: Rehabilitation of the Spine: A Practitioner’s Manual. 2nd ed. Baltimore: Lippincott Williams & Wilkins; 2006:97-112.7. Janda V. On the concept of postural muscles and posture in man. Aust J Physiother. 1983;29(3):83-84. doi:10.1016/S0004-9514(14)60665-6.8. Singer KP. A new musculoskeletal assessment in a student population. J Orthop Sports Phys Ther. 1986;8:34-41.9. Sakamoto ACL, Teixeira-Salmela LF, Paula-Goulart FR, Faria CDCM, Guimarães CQ. Muscular activation patterns during active prone hip extension exercises. J Eletcro-myography Kinesiol. 2009;19:105-112. doi:10.1016/j.jelekin.2007.07.00410. Nygren Pierce M, Lee W a. Muscle firing order during active prone hip extension. J Orthop Sports Phys Ther. 1990;12(July):2-9.11. Lehman GJ, Lennon D, Tresidder B, Rayfield B, Poschar M. Muscle recruitment patterns during the prone leg extension. BMC Musculoskelet Disord. 2004;5:3. doi:10.1186/1471-2474-5-3
Letter OrderA 1234B 1243C 1324D 1342E 1432F 1423G 2134H 2143I 2341J 2314K 2413L 2431M 3124N 3142O 3214P 3241Q 3412R 3421S 4123T 4132U 4213V 4231W 4312X 4321