Kobe University Repository : Kernel · T. Isobe et al. tomegaly 2cm below the right costal margin....
9
Kobe University Repository : Kernel タイトル Title Plasma Cell Leukemia with Acute Renal Failure 著者 Author(s) Isobe, Takasi / Horimatsu, Tohru / Chihara, Kazuo 掲載誌・巻号・ページ Citation Bulletin of allied medical sciences Kobe : BAMS (Kobe),13:177-184 刊行日 Issue date 1997-12-26 資源タイプ Resource Type Departmental Bulletin Paper / 紀要論文 版区分 Resource Version publisher 権利 Rights DOI JaLCDOI URL http://www.lib.kobe-u.ac.jp/handle_kernel/00188186 PDF issue: 2018-10-29
Transcript of Kobe University Repository : Kernel · T. Isobe et al. tomegaly 2cm below the right costal margin....

Kobe University Repository : Kernel
タイトルTit le Plasma Cell Leukemia with Acute Renal Failure
著者Author(s) Isobe, Takasi / Horimatsu, Tohru / Chihara, Kazuo
掲載誌・巻号・ページCitat ion Bullet in of allied medical sciences Kobe : BAMS (Kobe),13:177-184
刊行日Issue date 1997-12-26
資源タイプResource Type Departmental Bullet in Paper / 紀要論文
版区分Resource Version publisher
権利Rights
DOI
JaLCDOI
URL http://www.lib.kobe-u.ac.jp/handle_kernel/00188186
PDF issue: 2018-10-29

Plasma Cell Leukemia with Acute Renal Failure
Takasi Isobe l, Tohru Horimatsu 2 and Kazuo Chihara 2
A 58 year old female had a clinical feature of general fatigue. She had been an occupational background to have been exposed to a strong organic solvent at the leather manufacturing for the last 20 years. She was found to have plasma cell leukemia followed by remission with oral melphalan. A year later a relapsed plasma cell leukemia occurred and another institution of melphalan made again hematological improvement associated with fetal renal failure. Kappa-chain depositions in the epithelial cells of the renal tubules were confirmed by immunoperoxidase. An additional study on measuring the size and shape of tumor cells was done under microscopy, in comparison with abnormal plasma cells in the marrow of non-leukemic and classical type multiple myeloma. Tumor cells in this patient were confirmed to be small in sige and ovoid in shape.
Key words Oral administration of melphalan, Plasma cell in the peripheral blood.
INTRODUCTION
Plasma cell leukemia (peL) is a rare form of plasma cell dyscrsia (peD) i.e, plasma cell malignancy in its true nature.!) The clinical pictures of peL varies from the terminal appearrance of leukemia stage of multiple myeloma to an initial manifestation of fulminating course of acute leukemia. 2-4) In the present paper, one case of peL is described with its features of typieal leukemic stage charactrized firstly by being obtained once remission with an introducing chemotherapy, secondly by terminal acute renal failure occurred just after chemotherapy for a relapred state of
School of Allied Medical Sciences Ii Third Division, Department of Medicine , Kobe University Kobe city, Japan.
peL in the peripheral blood. CASE REPORT
Aka., 58 year old female, had a clinical feature of general fatigue at the age of 57. Her family history was non-contri~utory. However, it is noted that she had· been engaged in an occupation for the last 20 years at shoe-making factory, where a strong organic solvent had been routinely used for manufacturing. She had been exposed ,to that kind of solvent in a daily proces of handling leather material for shoe-making process.
The patient had a record of the first admission at the age of 56, when she was found to have pretibial pitting edema. Increasing edema made her hospitalized a month later on October 26, 1976 at her age of 56. A clinical diagnosis of plasma cell leukemia was made after admission.
Physical examination revealed her conscionsness clear, poorly nourished, body temperature 37.0°C, pulse rate 96/min and regular, venous hum at the cervical regIOn audible, hepa-
Vol.13, 1997 Bulletin of Allied Medical Sciences, Kobe 177

T. Isobe et al.
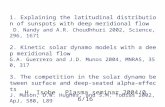
Figure 1. Numbers of plasma cells in the peripheral blood (right upper) and in the bone marrow smear (left upper). May-Giemsa stain X 200. Autopsied kidney specimen with anti kappa immuno stain X 100 with a positive stain in the epithelial cells of the tubules (right lower) and casts formation in the autopsied kiney with anti kappa chin immunostaining (left lower) .
178 Bulletin of Allied Medical Sciences, Kobe

Plasma cell leukemia with acute renal failure
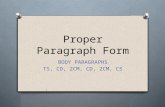
Figure 2. Electron microscopy of plasma cell in the peripheral blood (upper) and in the bone marrow (lower) . Eccentric nucleus and poorly developed rough end plasmic reticulum were observed in each cell Xl 0,000.
Vol.13 , 1997 179

T. Isobe et al.
tomegaly 2cm below the right costal margin. Laboratory exmina~ions included CRP 4.0mg/dl, HB antigen and antibody negative, GOT 251U/l, GPT 171U/l, LDH 4361U/l total cholesterol 107mg/dl, BUN 19.9mg/dl, serum creatinine 1.3mgl dl, serum total protein 9.4g/dl, albumin 4.2g/dl, IgG 6,699mgl dl with a monoclonal protein of IgG (k) type, decreased IgA and IgM undetectable levels in the serum, an aspirated bone marrow with nucleated cell count of 7.9X 104/pl including 44.8% of plasma cells, white cell count of the peripheral blood 15, 400/ml including plasma cells 10%, red blood cell 301 X 1041 pI, hemoglobin 1 O.4mgl dl, hematocrit 33%, platelet count 9.7 X 104 /pl, venous pressure measured at right cubital vein 193mm H20 and left cubital 213 mm H20, respectively. A cardiac echogram showed decreased left ventricular compliance with no evidence of thickened ventricular septum.
As shown in Figure 1 and Figure 2, plasma cells in the peripheral bone marrow aspirate were demonstrated with some charcleristics of plasma cells such as the presence of obvio~s perinuclesr hallo and eccentric location of the nucleus in the cytoplasm. As for measurement of size and shape of tumor cells, one hundred plasma cells were measured by ocular micrometer with oil immersion under light microscopy. The long and short diameters of each cell were determined along two axes at right angles. The size of each cell was expressed as the mean of the long and short diameters; the shape of each cell was expressed as the ratio of the long and short diameters, as published separately.9-10)
Mean value of size was 10.0 + 1.2 microns, and shape of cell was 1.40 + 0.27. In contrast, mean values of sizes of plasma cell from patients with myeloma without leukemia were 20.3 + 2.1 and shapes of cells were 1.10 + 0.00. In short summary of tumor cells in the this patient were confirmed to be small and ovoid.
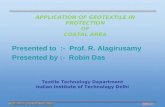
Clinically edema diminished with decresed body weight from 45kg to 39kg was seen during hospitalization. An insititution of chemotherapy of melphalan 2mg daily intake resulted in peripheral leucopenia of 7001 pI including neutrophil 46%, as well as thrombocytopenia 4.6 X 1041 pI. Although oral melphalan was discontinued, infections of acute tonsillitis, and acute cystitis with a urinary sendiment of bacterial casts, renal epithelial cells and white cell casts were noted. Intensive care for neutropenia and acute infections made her back in a stable condition. Figure 3 3howed a serial improvement of cardiac shilhouette during hospitalization. Although an aspirated bone marrow a showed plasma cell proliferation 27.2% out of nucleated cell. She was discharged as in a stable condition without edema from the hospital on April 16, 1977 at her age of 57. She visited our out-patient clinic under a maintenance dose of melphalan Img/day orally with prednisolone 5mgl day. Laboratory examination at the first visit at the out-patient clinic, were as follows ; a monoclonal IgG level of 2,73 Omgl dl in the serum bachground serum immanoglobulin 38mg/dl of IgA and 50mg/dl of IgM a peripheral blood count included white cell 7,5001 pI, with no evidence of increased plasma cells, red blood cell
180 Bulletin of Allied Medical Sciences, Kobe

Plasma cell leukemia with acute renal failure
Figure 3. Edema at the first admission (right upper). Pleural effusion and cardiac shilhouette improved 3 months later (left upper) and at dischange 6 months (right lower). Terminal stage and renal failure (left lower).
VoL13, 1997 181

T. Isobe et al.
Aug 24, 1977 Sep 8 Sep 13
MP Alb MP (MP)
s 4.9 1.0
BJP
u
WBC 30,700 /1J.e 3,800 3,000
PC 12,587 /1J.e 228 0
BMNCC 87,000 /1J.e 13,000
BMPC 35.6 % 0
IgG 6,468 mg/ d.e 1,512
IgA <10 120
IgM <10 86
TP 9.2 g/ d.e 8.6 8.0
MP 4.9 g/ d.e 2.8 1.0
BUN 26 mg/ d.e 108
UA 6.8 mg/ d.e 10.0
Hb 10.8 g/ d.e 8.6
plat x 104 7.3 /~.e 6.7
s - /(, 3.9 mEq/L 6.4
Figure 4. Marked improvement of serum monoclonal protein and urinary B]P, along with decreased number of plasma cells at the terminal stage of the present case.
182 Bulletin of Allied Medical Sciences, Kobe

407 X 104 1 pI, hemoglobin 13.8gml dl, hematocrit 39.1%, platelet 19.2 X 104 /pl; plasma fibrinogen 195mg/dl, erythrocyte sedimentation rate 5mm per hour, blood urea mitrogen 22mg/dl, serum creatinine 1.2mg/dl, GOT 135IU/I, and GPT 279IU/l. Although liver dysfunction without hepatomegaly was still pressent, the check-up at the out-patient clinic appeared almost unchanged for the subseque~t 4 months until August 24, 1977.
On the immediate physical examination at emergency room of the day of August 24, she was found to be distressed and anemic. Edema was obvious on the face and at the bilateral lower legs, presence of hepatomegaly 5cm below the right costal margin, low voltage in the electrocardiogram with sporadic Ventricular premature contractions, tachycardia 120in, cubital venous pressure 400mm H20 (normal adult, below 150mm H20) made a clinical diagnosis of acute right-sided cardiac failure. She was mentally disturbed in a state of somnolence. Further laboratory examinations included 9.8g/dl of total serum protein plasma hyperviscosity 25 seeonds compared with 20 seconds of normal adult plasma and negative eRP. She had a white blood cell count 30,7001 pI with 41 % of plasma cells in the peripheral blood, clearly revealing the relapse of plasma cell leukemia. A red blood cell count of 316 X 104 1 pI, hemoglobin 1 0.8g1 dl, hematocrit 32.0%, platelet count 6.7 X 104 /pl, GOT 182IU/I, and GPT 2571U/I, were also noted.
As shown in Figure 4, numbers of plasma cells in the peripheral blood decreased very rapidly, by means of
Vol.13 , 1997
Plasma cell leukemia with acute renal failure
reinstitution of chemotherapy using melphalan 6mgl day continuously. Other parameters improved such as total white cell count, plasma cells in the bone marrow, decreased monoclonal IgA and IgM levels in the serum as seen in Figure 4. And disappearance of Bence Jones protein in the urine. As noted in the figure 4 that there were rapid improvements of laboratory findings, however, renal functions were disturbed along with the terminal stage of her clinical cource. In fact, blood urea nitrogen from 26 to 1 08mgl dl, with another parameter of uric acid. from 6.8 to 1 O.Omgl dl, and serum creatinine from 2.1 to 5.3mg/dl, serum potassium from 3.8 to 6.4mEq/l, as shown in Figure 4. As examined an aliquot of the patient's urine, PH 5.0, protein 1 OOmgl dl, no Bence Jones protein in the urine with sediments of heavy accumulation of renal epithels and crystals without red blood cells or white cells. These clinical findings led to a clinical diagnosis of an acute renal failure on the basis of relapsed plasma cell leukemia at the terminal stage. She had small amounts of urine after by repeated injections of furosemide 80mg. In a way' to the rapid transfer to hemodialysis room for treatment of oliguria, she had unfortunately apnea and cardiac arrest.
At autopsy, pathological findings included, CD plasma cell leukemia, ® hypoplastic bone marrow, ® myeloma kidneys, and contracted kidney, @ uremia, pericarditis and pulmonary edema, ® hemorrhagic mucous membranes of alimentary tracts, ® lipid deposits in the liver, (j) atrophy of bilateral adrenals, ® bloody pericardial effusion 25 Oml and pleural effusion
183

T. Isobe et al.
(right 500ml, left 450ml), ®a follicular cyst in the left ovary, and ® generalized edema, @ no deposit of amyloid.
An imm unoperoxidase study was performed on the serial sections of paraffin-embedded kidney material, using anti immunoglobulin antibodies such as anti-kappa, anti-lambda, antigamma, anti-alpha, anti-mu, and antialbumin. As shown in Figure 4, there was no evidence of positive immuno-stainings on glomeruli. Tubular casts were seen with a clear result of positive stain for kappa but not for lambda. There were also positive stain of kappa chain on the epithelial cells of proxismal renal fubules with negative stains with antigamma or anti-alpha antiserum. In summary of the renal impairment in the present case acute renal failuren at the terminal stage was one of the direct cause of her death, mainly on the basis of myeloma kidney related to
REFERENCES
her plasma cell leukemia~
DISCUSSION
Plasma cell leukemia has been reported to have such characteristics as thrombocytopenia and bleeding tendency, infiltrations of tumor cells and rapid fatal course, which is expressed as the short survival time 1 .4), compared with ordinary straight multiple myeloma. In the author's experience in our laboratory, there was observed in 7 of 13 cases with a mean survival time less than 2 months from the diagnosis, in our previous study of plasma cell leukemia? Another clinical study on plasma cell leukemia in our laboratory already established that plasmacytic leukemia cells were elongated or ovoid and significantly smaller in size, whereas the myeloma cells were generally more nearly round and larger, as published separately.9)
1. Osserman EF, Isobe T : Plasma cell dyscrasias, in Hematology ed by Williams WJ. et al. New York, Me Graw-Hill, 1972, pp950-956
2. Pedraza MA : Plasma-cell leukemia with unusual immunoglobulin abnormalities. Am J. clin pathol 64 : 410-415, 1975
3. Kyle RA, Maldonado JE, Bayrd ED : Plasma cell leukemia. Arch Intern Med. 133: 813-818, 1974
4. Pruzanski W, Platts ME, Ogrylzo MA : Leukemic form of immunocytic dyscrasia (plasma cell leukemia) : A study of ten caces and a review of the literature. Am J Med 47 : 60-74, 1969
5. Isobe T, Ikeda Y, Imura Hand Ohta H : Plasma cell leukemia-A clinical study of 13 cases, with a demonstration of small-size plasma cells. Acta Haematol Jap. 40: 529-540, 1977
6. Aggressive course of primary plasma cell leukemia with unusual morphological and cytogenic features. Ann Hematol. 71: 307-310, 1996
7. Murayama T et al : Plasma cell leukemia with myelofibrosis. Ann Hematol : 69 : 151-152, 1996
8. Yang CH et al : Autologous bone marrow transplant Proc : 24, 1531-1532, 1996 9. Isobe T, Ikeda Y, Ohta H : Comparison of sizes and shapes of tumor cells in plasma cell
myeloma. Blood: 53 : 1028-1030, 1979 10. Isobe T, Imura H. Ohta H: Plasma cell leukemia. A clinical study of 13 cases, with a demon
stration of small-sized plasma cell. Acta Haem. Jap 40 : 529-540, 1977
184 Bulletin of Allied Medical Sciences, Kobe