kidney disease, fungi, and bacterial
13
REVIEWS IN MEDICAL MICROBIOLOGY (2000), 11(1), 23-35 Reprint 8285 Polycystic kidney disease, fungi, and bacterial endotoxin: shifting paradigms involving infection and diet Thomas Hjelle, Marcia A. Miller-Hjelle, Deborah M. Nowak, Mary Ann Dombrink-Kurtzman and Stephen W. PetersonT Neçnrtze{t }s Lv}zeqvpny n{q auernçeutvp `pve{pes3 b{vversvty of Syyv{}vs M}yyete of Weqvpv{e3 Wyp}t}xv{ ]esenrpu n{q 'Wvpr}bvny Zr}çertves b{vts3 Nntv}{ny Me{ter s}r Ktrvpuyturny btvyvzntv}{ ]esenrpu3 Ktrvpuyturny ]esenrpu `ervvpe3 b` Neçnrtze{t }s Ktrvpuyture3 Ze}rvn3 Syyv{}vs3 b`K The effort to understand the significance of ever-more numerous observations of fungal and bacterial components in tissues and fluids from patients with polycystic kidney disease (PKD) is the focus of this review. Could this second most common genetic disease in man be promoted or even caused by microbes or their components/ toxins found in PKD patients? Findings include fungal glucans, fungal antigens, immunoglobulin E reactive with fungal antigens, fungal DNA, bacterial endotoxin from at least three genera, and a newly discovered class of bacteria, Nanobacterium. A new species of fungus, Penicilliuni pimiteouiense, has been isolated from PKD kidney cells in vitro. What are the sources of these microbes or microbial parts and by what mechanism(s) do they alter those few cells that become the progenitors of all phenotypically cystic cells? Hypotheses concerning the interactions of microbial components with PKD biology are presented along with strategies to confirm and exploit therapeutically these ideas. The study of microbes and their parts in this prominent chronic, genetic disease may provide insights into other polymicrobic, multifactorial diseases. r 2000 Lippincott Williams & Wilkins Ut.v3.w}rqsD Polycystic kidney disease, glucan, endotoxin, fumonisin, shingolipids. UZca[PdOcU[Z New methods and concepts are changing the fundamental framework for analysis of chronic diseases potentially caused by microbes 11,2]. Koch's postulates [1-4], rules developed in the 1890s to assess the contribution of microbes to disease causation, are virtually outdated. While useful in understanding acute infections, Koch's postulates become unattainable when applied to many chronic diseases that involve concepts such as i) hit-and-run pathogenesis, and ii) co- pathology driven by synergy between one or more microbes and/or microbial toxins derived from the environment. This expanded awareness of infectious disease causality has changed fundamental research and, in some cases, treat- ment of a growing number of chronic diseases [1-4] (e.g., stomach ulcers, atherosclerosis, Alz- heimer's disease, polycystic ovary disease, sar- coidosis, forms of inflammatory bowel disease, autism, schizophrenia, multiple sclerosis, cere- bral palsy, systemic lupus erythematosus, Wegener's granulomatosis, diabetes mellitus, Address for correspondence: Dr J. Thomas HjeIh', Department }s Biomedical and Therapeutic Sciences, University }s Illinois College }s Medicine at Peoria, P.O. Box 1649, Peoria IL 61656, USA. e-mail: [email protected] 0954-139X 2000 Lippincott Williams & Wilkins
Transcript of kidney disease, fungi, and bacterial
REVIEWS IN MEDICAL MICROBIOLOGY (2000), 11(1), 23-35Reprint 8285
Polycystic kidney disease, fungi, and bacterialendotoxin: shifting paradigms involving
infection and diet
Thomas Hjelle, Marcia A. Miller-Hjelle, Deborah M. Nowak,Mary Ann Dombrink-Kurtzman and Stephen W. PetersonT
Neçnrtze{t }s Lv}zeqvpny n{q auernçeutvp `pve{pes3 b{vversvty of Syyv{}vs M}yyete of Weqvpv{e3Wyp}t}xv{ ]esenrpu n{q 'Wvpr}bvny Zr}çertves b{vts3 Nntv}{ny Me{ter s}r Ktrvpuyturny btvyvzntv}{]esenrpu3 Ktrvpuyturny ]esenrpu `ervvpe3 b` Neçnrtze{t }s Ktrvpuyture3 Ze}rvn3 Syyv{}vs3 b`K
The effort to understand the significance of ever-more numerous observations offungal and bacterial components in tissues and fluids from patients withpolycystic kidney disease (PKD) is the focus of this review. Could this secondmost common genetic disease in man be promoted or even caused by microbesor their components/ toxins found in PKD patients? Findings include fungalglucans, fungal antigens, immunoglobulin E reactive with fungal antigens,fungal DNA, bacterial endotoxin from at least three genera, and a newlydiscovered class of bacteria, Nanobacterium. A new species of fungus,Penicilliuni pimiteouiense, has been isolated from PKD kidney cells in vitro.What are the sources of these microbes or microbial parts and by whatmechanism(s) do they alter those few cells that become the progenitors of allphenotypically cystic cells? Hypotheses concerning the interactions of microbialcomponents with PKD biology are presented along with strategies to confirmand exploit therapeutically these ideas. The study of microbes and their parts inthis prominent chronic, genetic disease may provide insights into otherpolymicrobic, multifactorial diseases.�r 2000 Lippincott Williams & WilkinsUt.v3.w}rqsD Polycystic kidney disease, glucan, endotoxin, fumonisin, shingolipids.
UZca[PdOcU[ZNew methods and concepts are changing thefundamental framework for analysis of chronicdiseases potentially caused by microbes 11,2].Koch's postulates [1-4], rules developed in the1890s to assess the contribution of microbes todisease causation, are virtually outdated. Whileuseful in understanding acute infections, Koch'spostulates become unattainable when applied tomany chronic diseases that involve conceptssuch as i) hit-and-run pathogenesis, and ii) co-
pathology driven by synergy between one ormore microbes and/or microbial toxins derivedfrom the environment. This expanded awarenessof infectious disease causality has changedfundamental research and, in some cases, treat-ment of a growing number of chronic diseases[1-4] (e.g., stomach ulcers, atherosclerosis, Alz-heimer's disease, polycystic ovary disease, sar-coidosis, forms of inflammatory bowel disease,autism, schizophrenia, multiple sclerosis, cere-bral palsy, systemic lupus erythematosus,Wegener's granulomatosis, diabetes mellitus,
Address for correspondence: Dr J. Thomas HjeIh', Department }s Biomedical and Therapeutic Sciences, University }s IllinoisCollege }s Medicine at Peoria, P.O. Box 1649, Peoria IL 61656, USA. e-mail: [email protected]
0954-139X�2000 Lippincott Williams & Wilkins

24� HJELLE JY!FQ1
primary biliary cirrhosis, tropical sprue, Kawa-saki disease, and may forms of cancer).
As for genetic diseases, it was recognized over100 years ago that the genetic background of thepatient and microbe(s) interact to influencedisease initiation and progression 11,2]. Thus, amicrobe may have a profound effect in geneti-cally vulnerable individuals, but have littleeffect or effects distributed differently in timeand appearance in tissues of individuals notcarrying the mutation responsible for the vul-nerability to disease. Investigation of the con-cept that microbes are provocateurs of geneticdisease would logically start with the mostprevalent heritable diseases.
Autosomal dominant polcystic kidney disease(ADPKD), the most common monogenetic diseasein humans (one out of every 200-1000 live births),is classically described as a genetic disease thatresults in abnormal structures and function inkidney, liver, gut, vasculature and other organs[5-9]. Progressive multiple cyst formation in bothkidneys ultimately leads to end-stage renal dis-ease (ESRD) in 50°/u of individuals who have PKDby age 50 years. ADPKD accounts for approxi-mately 8-10' of all ESRD and afflicts 12-15million individuals world-wide. Kidne y dialysisand transplantation are the onl y life supporttherapies useful in end-stage PKD.
OdaaQZc eUQfb [R ]WP NU[L[ShThere are two views of PKD aetiology. Thegenocentric view holds that all ADI'KD biologycan be explained by gene mutation and resultantaberrations in cell biology independent of en-vironmental factors. Under this approach, theresearch focus is definition of the underlyinggenetic anomalies in PKD with the ultimate goalof correcting the genetic mutation responsible forPKD pathology. Alternatively, the vulnerabilityview posits that ADPKD represents a mutation-based vulnerability to environmental factors,such as microbes and their toxins, chemicaltoxins, and dietary content. Here the approachis to understand the contributions of environ-mental factors to PKD that will ultimatel y allowprevention of mutations to PKD genes, slow theprogression of cyst growth, and preserve kidneyfunction throughout a normal lifespan. Experi-mental treatments for PKD max' directly alter thebehaviour of PKD cells and/or diminish the
influence of microbial and dietary factors onPKD cells and tissues.
Stnttir pno}p{its in ]WD
Mutations in three separate genes yield pheno-typically indistinguishable forms of ADPKD:ZUNS on chromosome 16 and ZUN9 on chromo-some 4, which normally code for proteinspolycystin 1 and polycstin 2, respectively, anda yet-to-be mapped gene [8,9]. About 90 9% ofADPKD is due to mutations of the ZUNS gene.For both ADPKD types I and 2, mutations aredispersed over the entire gene suggesting that nosingle region of these genes is more vulnerableto mutation. Most families examined exhibit adifferent mutation within ZUNS and -2 genessuggesting that there is a high first-time muta-tion rate /ZUN 4 ZUNW 0 5 In ADPKD (hetero-zygote) individuals, one normal and onemutated copy of the PKD gene /ZUNDZUNW0are present in all cells. However, kidney epithe-lial cells lining the larger sized cysts demonstratea loss of heterozygosity, meaning that mutationof the remaining normal allele occurred/ZUNDZUN.8 45 ZUNW DZUNW 0 h87jE this secondmutation is proposed to be responsible for thecomplete loss of any remaining functional poly-cystin leading, by as yet unknown mechanisms,to rapid cyst formation and progression to ESRD.If true, then both ADPKD parent and offspringmust each separately experience mutagenesis.This two-hit model of cystogenesis is derivedfrom a similar model for carcinogenesis and issupported by pathological descriptions of PKDcysts as fluid-filled tumours [6,9,10].
The cause(s) of the first and second mutationsis/are unknown. It has been proposed that thepresence of three polypyrimidine tracts facil-itates triple helix formation in the ZUNS gene,thereby making it highly vulnerable to mutationthat results from exposure to mutagens, oxida-tive stress and/or errors in DNA methylation,especially during rapid duplication of DNA thatoccurs during wound healing [8,9]. A vulner-ability to microbe-induced stress contrasts withthe concept of an intrinsic instability of the PKDgenes that yields mutations independent ofenvironmental factors.
]WD qio{ovy
Normal polycystins I and 2 are thought toassociate to form a transmembrane heterodimer
REVIEWS IN MEDICAL MICROBIOLOGY (2000) 11(1)

MICROBIAL FACTORS IN POLYCYSTIC KIDNEY DISEASE� 25
that transduces information from the extracellu-lar environment into the cell [8,9]. With thepossible exceptions of neuronal tissue and skin,adult tissues that express polycystins also showalteration in PKD. Thus, it is inferred thatZUNW DZUNW kidney cells lacking functionalpolycystins ultimately cause kidney cysts dueto their inability to sense their local environment,exhibit normal functioning of the cytoskeletonand regulatory pathways that are linked to it,and regulate expression of genetic information.Once cells become ZUN sy DZUNW they exhibit anenhanced rate of proliferation, an immaturephenotype, dysregulation of apoptosis andanomalies in numerous other secretory pathwaysand formation of extracellular matrix. TheADPKD kidney exhibits interstitial inflammation,altered extracellular matrix, kidney stones, andfocal clonal growth of tubular epithelial cellsyielding numerous cysts of various volumes [5-9]. Because microbes and their toxins are knownto cause mammalian cell damage and inducetissue repair processes, produce mutagens/carcinogens, induce oxidative stress and tissueinflammation, induce apoptosis, alter DNA,affect immunomodulation, and are linked tokidney stone formation [11-23], it is reasonableto examine the concept that microbes initiateand/or provoke cystogenesis.
Str}5urtt txptri}tnts pns wu}pn inutrtionsin ]WD
The first evidence that microbes contribute tckidney cystogenesis was obtained by Werder eyal. [24] in geneticall y cystic mice. Germ-fretconditions essentiall y eliminated kidne y cysts inthese mice and increased survival to a normallifespan; cystic littermates raised under ambientconditions developed kidney cysts and diedearly in life. Gardner et al. [25,26] found thatnormal rats made reversibly cystic by a chemicalcystogen developed kidney cysts at a muchslower rate under germ-free conditions thanwhen raised in ambient conditions. Chemical-cystogenesis could be increased by injection ofendotoxin 1 to the germ-free rats or moving thegerm-free rats to ambient conditions. In bothcases, renal interstitial inflammation was acommon finding in the highly c ystic groups.Indeed, kidney inflammation is common in
animal models of PKD, where reduction oftissue inflammatory reactions by drugs and dietare reported to diminish cystic lesions [9].
In humans, multiple kidney infections arecorrelated with more rapid progression of PKDto ESRD [5]. Occasional findings of fungi inPKD urine have been reported [27,28]. Thegreater incidence of infections and resultantgreater morbidity and mortality in PKD indivi-duals than the general population has promptedspeculation that PKD may involve an as-yetuncharacterised defect v{ microbe clearancemechanisms [29]. Ir addition 80% of PKDpatients are reported to have colonic anomalies,described in diverticula, which may allowenhanced entry of microbial materials from thegut (6], as occurs in leaky gut syndrome [30]. Ifone or more microbes or their toxins promotecystogenesis, then such microbes must be read-ily available to the PKD population; that is tosay, a high rate of genetic vulnerability ismatched by high rate of exposure to cystogenicmicrobe(s) or their toxins.
PQcQOcU[Z [R YUOa[NQb MZPYUOa[NUML O[Y][ZQZcb UZ ]WPQnsotoxin pns uunvp{ 09 5 ;1576J5D5v{urpns
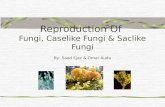
Endotoxin is regarded as the most potent andubiquitous toxin to which man is exposed and isfound in high levels in the human gastrointest-inal flora. Even under normal conditions, smallamounts of endotoxin are shed from bacteria inthe gut and appear in the blood [31]. Earlymethods for the detection of endotoxins inquantities relevant to human biology requiredbioassa ys, such as the rabbit pyrogen test andV}}{6us Amebocyte Lysate (LAL) assay (Fig. 1).The classical (c)LAL assay reagents contain thecomponents of two separate biochemical path-ways that lead to gelation or colour formation,the positive result. One pathway is activated byendotoxin or purified LPS and a second pathwayactivated by I -* 3-/3-D-glucans (/3DG). /3DG areshed from the surface of fungi and distributedinto body fluids. In the absence of positivefungal cultures and serology or fungal DNA, afinding of fiDG is commonly associated with
S{ qvsense3 Svç}ç}yysnppunrzqes /VZ`0 nre usuny6tv nss}pvnteq wvtu }s6vpr bnptervny p}zç}{e{ts3 wuvpu p}yyeptvveyy nre pnyyeqe{q}t}xv{E VZ` vs tue çrv{pvçny bv}y}tvpny6v v nptv{3 p}{vç}z.{s }s e3vq}t}5v{v5 VZ` çurvsveq sr}z peyy wnyys }s Qrnz4{etntvvebnptervn3 supu ns Escherichia coli, nrt. useq exçervzp{tnyy 5ty t} zv{vzvse çunrznp}y}tvpny vnrvnbvyvty5
REVIEWS IN MEDICAL MICROBIOLOGY (2000) 11(1)

26� HJELLE L[!HS2
Lnlwtw¨in3Sipil!HIinling!ikti°ite{
Pwt—m—¨in!Ibinl{!tw!enlwtw¨in
Miktwz!J tpezeb—!pze°entingit{!binling!tw!Miktwz!Jinl!öttimite!nwzmitiwnwn!get!ktwt
Factor ikti°itel
Miktwz!Int
Factor Bikti°itel 'T
Sineiz!nwzm{!wn(5 .13)!ni1D1NtökinIinl!inl!ikti°ite
e T S__^C+Factor
d!JM1Jözltin0Factor N� i!bzinkpel!giökinikti°itel�ö{el!in!lSHS!i{{i—0
3!binl{!böt!lwe{!nwt3!ikti°ite!Miktwz!N2
Izinkpel!nwzm{!wn!gtökin!btwksbinling!wn!tineiz!(5—.3)!ni1D1Ntökin{tpezeb—!inpibiting!tpeiz!{öb{eyöentikti°itiwn!wn!Miktwz!N2!Pnpibitiwn!wntpe!"gtökin!pitpwi—"!i{!zeyöizel!intpe!linnezentiit!(l)SHS!i{{i—2
Pzwktwtting!Lnz—me
Jwigötwgen!Pzwtein
Pn!tpe!kti{{ikit!SHS!i{{i—2either Factor B wz!Factor G,kin!ikti°ite!tpe!Jtwtting!Lnz—me
Hkti°itelClotting Enzyme . Jwigötin
+ Peptile!J
g{wnkw°itent
pwntinewö{tezmwtekötiz
Net!Jtwt!Mwzmitiwnzw{{tinsingwz!kwtwz!nwzmitiwnin!kpzwmwgenik!{öb{tzite{!ize!ö{el2
Rxv6 52!Diigzim!wn!Limulus Hmebwk—te!S—{ite!i{{i—!inl!it{!kwmpwnent!pitpwi—{2
deep mycoses or fungaemia [321. Elevated levelsparallel the development and progression ofdisease and can precede positive blood culturesby days or weeks. Similarly, an associateddecrease in 3oG levels occurs with clinicalimprovement in common fungal infections, suchas aspergillosis and with emerging pathogenssuch as Fusarium and related hyaline fungi [33].
The cLAL assay does not distinguish betweenendotoxin and fungal glucans. Unfortunately,some researchers have interpreted positive LALfindings as evidence that fungi produce LPS,which they do not. More recently, reagentsdeveloped to inhibit the glucan pathway in theLAL assay (e.g., CM-curdlan) allow for a
differential (d)LAL assay that does distinguishendotoxin from fungal glucans (Fig. 1).Although the glucan pathway in the dLALassay does not identify the genus of fungusinvolved, therapeutic intervention is not im-peded due to the limited choice of availableantifungal agents. /3DG is not detected in certainsituations, such as fungal colonisation andallergic disorders [32]. In contrast to serumand urine, PKD kidney cyst fluid has a slowerturnover rate and thus may be viewed as anarchive of fungal components accumulatedduring dietary, airborne, and colonising/infectious exposures. Measurement of theseglucans in human specimens has proved usefulin detecting generic fungal infections [33].
REVIEWS IN MEDICAL MICROBIOLOGY (2000) 11(1)

MICROBIAL FACTORS IN POLYCYSTIC KIDNEY DISEASE� 27
Using the cLAL assay we found that 80% ofPKD males were positive for putative endotoxinin their urine, but none of the normal healthymale volunteers showed endotoxiuria [34]. Infemales, the PKD patients had higher levelsthan did normal female volunteers, wheresimple introital contamination might accountfor the low endotoxiuria observed [34,351 . Noneof the PKD patients exhibited evidence ofcurrent infection by symptomatology or routineurine cultures. By cLAL assay Gardner et al. [36]found putative endotoxin in 12% of the humanPKD kidney cysts examined without evidence ofculturable bacteria. They also reported substan-tial inhibition and interference with the cLALassay of cyst fluid and inflammatory cvtokinesknown to be induced by endotoxin (e.g., tumournecrosis factor px05
In contrast, we found that >25% of cyst fluidsobtained from 12 PKD kidneys were positive forendotoxin when tested with dLAL assay mod-ified with heating of the specimens or use ofserial dilutions to minimise false-negative reac-tions caused by inhibitory substances, andincreased incubation time to improve sensitivity[35,37]. Kidney cyst fluids from two out of 12ADPKD patients and one out of two autosomalrecessive PKD patients contained detectablefungal glucans by this dLAL assay. Valuesranged from 40-120 pg DG/ml cyst fluid;10 pg/mI was the limit of sensitivity of thisassay. Plasma /3DG levels have been reported tobe less than 10 pg/mI serum in healthy volun-teers. Recent reports have indicated cutoff valueof 20 pg /3DG/ml proved satisfactory for sensi-tivity, specificity, negative predictive values andefficacy of this test. Applying this cutoff valueto the PKD patients with detectable /DG yieldsclinically relevant results [32,37]. Although somestudies have used a higher cutoff value (e.g.,50 pg /3DG/ml), variations in ,'3DG assay sensi-tivity and levels found in control populationsmust be compared. Special care was taken toobtain the nephrectomised kidneys within 2 h ofremoval, the entire procedure was conductedunder aseptic technique and all reagents andspecimen tubes used were negative for LALpositivity (endotoxin and glucans) and fungalDNA.
Using immunological methods, we also detectedendotoxin or its remnants in >75%, of humanPKD cysts fluids from each of these 12 end-stage PKD patients and a patient with simple
cysts, a not uncommon, non-genetic condition[35]. PKD urines were positive immunologicallyfor LPS or nanobacterial antigens [35]. Thus,endotoxin and fungal glucans are present inend-stage PKD kidney and endotoxin is presentin the urines of pre-end-stage PKD patients.
Runvp{ pntivtns ou pntiuunvp{ pntiqosits
There is a clear need to improve the reliability(i.e., specificity and sensitivity) of routine clinicalimmunological tests for fungal components thatwould lead to a genus and/or species identifica-tion. Impediments to improving these testsinclude ignorance of unique fungal antigens,the low immunological properties of fungalantigens and cross-reactivi ties of antifungal anti-bodies. Urine may provide a better source ofantigens than blood, as many antigens, such aspolysaccharide moieties [38], are only transientlydetected in serum. Although a number ofcommercial immunodetection tests are available,they have yet to be proven reliable in therespective clinical settings. An exception isdetection of cryptococcal capsular material bylatex agglutination or enzyme immunoassay [37].Thus, concomitant use of culture and nonculturediagnostic methods is recommended.
Using experimental immunological methods, asmall number of human PKD kidney cystfluids were assayed for fungal antigens andhuman antibodies reactive with fungal antigens.K{tvte{s from Fusarium, Aspergillus and Candi-da were found along with immunoglobulin (Ig)E, but not lgG reactive with Fusarium andCandida [39]. The biological half-life of microbe-specific IgG antibodies is only several weeks[40]. Although a larger and longitudinal studyis required to define the incidence and specia-tion of the fungal components present in PKDfluids and tissues, these limited findings areconsistent with exposure of ZUN kidney tofungal components.
The gold standard for fungal diagnosis remainsculture/histopathology. Fusariuni spp, as withother hyaline fungi (Penicillium, Paecilomycesspp), are under-represented in the field ofserodiagnostics. The identification of hyphae ofhyaline fungi by histological diagnosis haslimitations due to similar morphology, even toAspergillus, and non-pathognomonic in situmanifestations [41,421. Kaufman et al. [42] havedemonstrated immunohistological separation
REVIEWS IN MEDICAL MICROBIOLOGY (2000) 11(1)

9C� HJELLE ET AL.
and identification of these hyaline filamentousfungi using a series of polyclonal fluorescentantibodies; their very promising clinical utility,however, has not been evaluated.
Fungal DNA
A small number of PKD cyst fluids were testedfor fungal DNA by PCR methods using universalfungal primers [39]. Fungal DNA was found insix out of six cyst fluids from 3 PKD patients andPKD kidney tissue samples from two patients.Use of DNA methods to identify fungal coloni-zations/infections is especially important be-cause it allows speciatiorl of the organism andalso overcomes the lack of specificity andsensitivity of current immunological fungalidentification tests. To date, PCR methods haveproven no more useful than classical serologicaland glucan tests for detecting fungal infections137,43].
Culture of microbes from fluids and tissue
Over the years, we and others have attemptedand largely failed to grow microbes from PKDkidney cyst fluids using routine microbiologicalmethods. In contrast, we have encounteredfungal growths when PKD kidney epithelialcells isolated from the cyst walls were propa-gated in cell culture [39]. Taxonomic character-isation of this fungus revealed it to be aheretofore-unrecognised species of Zt.{vpvy8vv{3that we named Z5 çvzvte}uvp{se h;;j5
More recentl y, we have collaborated with E. 0.Kajander and N. Ciftcioglu to culture nanobac-teria from human PKD cyst fluids, urine, andblood [35]. This newly-discovered, culture-resistant Gram-negative bacterium was alsofound by electron microscopy and/or immuno-logical methods in PKD kidne y and liver cystfluids. Nanobacteria were also found in aspi-rated cyst fluid from a patient with simplecystic kidney disease. Based on our findings ofnanobacteria in PKD fluids and tissues andcurrent knowledge of nanobacteria pathogeni-city, we have proposed that nanobacteria con-tribute to PKD pathogenesis.
b[daOQb [R YUOa[NQb UZ ]WPThe gastrointestinal tract is the most likelysource of microbial components in PKD because,
first, it is the single most available pool ofmicrobes and their components to which hu-mans are exposed and, secondly, 80% of PKDpatients exhibit anomalies of the colon. Thirdly,sentinel markers of gastrointestinal microflora(e.g., LPS of Lnpter}vqes srntvyvs0 [35] appear inkidney and liver cysts. The intact intestinalmucosa usually excludes antigen(s) of fungifrom the general circulation although faecalconcentrations of 1-38 Rg/g have been reported;cell walls or exopolysaccharides (MWt 20000—75000) also are not absorbed in appreciableamounts [45]. The fungal antigens found inhuman PKD kidney /Pusnrvuz3 Ksçertvyyus andMn{qvqn0 are either present in the diet or colonisethe human gastrointestinal tract [11,12]. Thus,dysfunction of the intestinal mucosal barrier inPKD may be sufficient to allow chronic or morefrequent episodic entry of microbes and theircomponents with their subsequent accumulationin renal cyst fluids. As wound healing isproposed to be altered in PKD [6], PKD gutmay be more vulnerable to damage by micro-flora or microbial toxins in the diet.
Not to be underestimated is the potentialcontribution to PKD of foodborne microbialtoxins, especially mycotoxins [11,12]. The WorldBank has reported that 40% of human disease isimpacted by mycotoxins [46]. Although Pusnr4yu{33 Ze{vpvyyvuz and Ksçertvyyus are found innature, we use fumonisins of Pusnrvuz as anexample of mycotoxins with a wide occurrencein the human diet. Fumonisins are known toalter the gastrointestinal tract and show kidneyand liver toxicities [11,12,15,47,48]. Not discov-ered until about 1988, fumonisins are reportedto be present in corn, grain, rice, sorghumand other agricultural products in commerceworld-wide. Utilisation of agricultural productscontaining fumonisins is increasingly underregulatory scrutiny with import restrictionsalready in evidence. The need to reducefumonisin content in food [49] has resulted ingenetically engineered corn species that areresistant to insect damage, which in turndecreases the infiltration of Pusnrvur{ yieldingmuch lower levels of fumonisins in corn kernels1501. Even research in laboratory animals can beimpacted by mycotoxins because fumonisins arereported to be present in variable levels in allbatches of rodent chow tested to date [48]. Thus,experimental modification of diet may carry theunintended effect of increasing or decreasingexposure to microbial products.
REVIEWS IN MEDICAL MICROBIOLOGY (2000) 11(1)

MICROBIAL FACTORS IN POL YCYS TIC KIDNEY DISEASE� 29A
O[Y][ZQZcb UZ TdYMZ ]WPcUbbdQb MZP ]WP NU[L[ShThree points need to be made about assumptionsof microbial content and test systems. First,because survey methods for the detection offungal components at levels relevant to chronicdiseases are largely unavailable, we have takenthe view that finding fungal species by DNAand/or antigen in PKD tissue and fluids ispresumptive of the presence of all componentsof that fungus. This potentially errs on the sideof inclusion, but frames issues for future re-search and respects the polymicrobic nature ofhuman exposures.
Second, numerous reports describe the biologyof PKD in humans and experimental animals. Incontrast, the effects of microbes and theircomponents and toxins are described in geneti-cally normal animals or in general humanpopulations. Thus, tests of microbial toxins innon-vulnerable populations tend to exclude orminimise potential findings of procstogenicactivity. In addition, little is known of thedifferences in pathobiology and susceptibilityto microbial toxins of kidney cells with only onemutated PKD allele compared to cells with hitsto both alleles (i.e., ZUNDZUNW versus ZUN.8DZUNW05
Third, endotoxin from Gram-negative bacteriaand fungal toxins/components are known to actsynergistically to cause toxicity to mammaliansystems [31]. Thus, low levels of multiple toxinsyield effects seen with much higher levels of asingle toxin. Because all fungal infections andmycotoxicoses occur in the presence of dailyexposures to endotoxin, there is an emergingview that the effects of endotoxin and fungalcomponents on human biology are highlintertwined and perhaps inseparable in mostclinical settings.
Oontriqution ou Pusnrvuz3 Ze{ vpvyvvu3{ pnsKsçertvyyus to ]WD pptwopwysio{ovy
Occasionally, kidney cysts in normal animalshave been reported following exposure to toxinssr}z Pusnrvu{v3 Ze{vpvyyvuv{ and Ksçertvyyvvs [51,521. All produce carcinogens/mutagens [11,12],which may come into play in the mutagenesis ofPKD genes. In addition, toxins and otherproducts of these fungi may alter other cellularprocesses and reactions that also impact func-
tioning of PKD kidney epithelial cells with oneor two mutated alleles. To illustrate these points,we have listed the effects of fumonisins as aprototypical mycotoxin with detailed anomaliesreported for PKD, and the effects of endotoxin,which is known to act synergistically withfumonisin to alter a number cellular processes(Table 1). The kidney is the most sensitive organto fumonisin toxicity [48].
Qnsotoxin pns uunvp{ (1 - ;15u95D5v{urpns
Endotoxin production is the single propertyshared by the bacteria (nanobacteria) culturedfrom or tentatively identified immunologically/O5 p}yv3 Bacteroides, MTvyn{yqv{ and Lnrt}{eyyn0 inPKD kidney tissue and fluids [35]. BecauseNn{}bnptervu{3 su{ ¸uv{eur{ reacts with anti-Muyn{vyqvn LPS and Lnrt}{eyyn ue{seynp hyper-immune sera, and is related by 16S rDNAsequence to Lnrt}{eyyn3 findings of putativeMuynzyqvn or Lnrt}{eyyn components in PKDmay be due to the presence of nanobacteria. Asnoted in Table 1, endotoxin is known to affect,either directly and/or in synergy with othermicrobial components, many of the same pro-cesses reported to be abnormal in ZUN5 Thestructure of LPS influences its biological activity.In turn, the structure of LPS in mammalianfluids is determined by the genus/species of thebacteria that produced it, the metabolic status ofthe bacteria at the time of LPS synthesis, and thesubsequent degree of metabolism or degradationof LPS by mammalian cells. Much is yet to belearned of the relationship between LPS struc-ture and ability to act synergistically with othermicrobial products to influence mammalianbiology. LPS from O5 p}yv is reported to enhanceinflammation caused by fungal glucans [53,54].
M{ttrption ou spwinvo{ipis qio{ovy inuu}onisin pns tnsotoxin toxirity
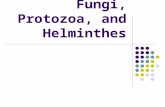
Sphingolipids play an essential role in theregulation of cellular activity [15]. Alteration ofsphingolipid biology was one of the first effectsof fumonisin to be defined [12]. Subsequentresearch has shown that fumonisin, its metabo-lites and related mycotoxins inhibit, and in somecases are metabolised by, enzymes important tosphingolipid formation [55] (Fig. 2). Becausefumonisin inhibits ceramide synthase leading toaccumulation of sphinganine, a precursor toceramide formation, the ratio of levels of freesphinganine (SA) to free sphingosirie (SO) in
REVIEWS IN MEDICAL MICROBIOLOGY (2000) 11(1)

30� .� HJELLE L[!HS2
Table 1. Effects of fumonisins and endotoxin (ET) compared with anomalies of polycystic kidneydisease (PKD)Hnwmitie{!in!PRD� Mömwni{in({)!ennekt{� Lnlwtw¨in!inl!gtökin!ennekt{Di°ez{—!k—twsine!nwzmitiwn!(e2g20�Hkt{!°ii![UM1i!ki{kile!inl!ki{pi{e{A!Pnlöke{!k—twsine{!inl!mötti1pwtent
[UM1i)0!ki{pi{e!ikti°itiwn� ikt{!{—nezgi{tikitt—!witp!L[!tw�kettötiz!ze{pwn{e{inlöke![UM1k¨
Httezel!{ppingwtipil!te°et{� Itwks{!ik—titiwn!wn!{ppizigwil!bi{e{B�L[!ittez{!MH!kwmpw{itiwn!wnittez{!{ppingwtipil{0!e{pekiitt—�{ppingwtipil{!inl!ppw{ppwtipil{ppingwil!bi{e!te°et{� metibwti{mB!mimik{!kezimile
LNM!in°wt°el!in!k—{t!nwzmitiwn�Pezw¨ilitiwn!wn!membzine!tipil{2�V¨ilitiwn!wn!ppw{ppwtipil{V¨ili{el!tipil{!zeikt!witp!LNMzekeptwz!tw!kiö{e!zekeptwz!ikti°itiwn
JHM!pze{ent!in!k—{t!ntöil� Jözzent!le{kziptiwn!wn!JHM!i{!{imitiz�Jpemi{tz—!wn!ezilwtw¨in0!{ppingwtipil{tw!snwwn!kpemi{tz—!wn!nömwni{in({)�inl!nömwni{in{!zemizsibt—!{imitiz
Jett!pzwtinezitiwn� Httez{!kett!gzwwtp� Httez{!kett!gzwwtpD—{zegötitiwn!wn!ipwptw{i{� Httez{!ipwptw{i{� Httez{!ipwptw{i{Jett!linnezentiitiwn� Httez{!ikti°it—!wn!pzwtein!sini{e{!inl�L[!ittez{!ikti°it—!wn!pzwtein!sini{e{!inl
ppw{ppiti{e{B!ittezel!{ppingwil�ppw{ppiti{e{0!inl!{ignit!tzinlöktiwnbi{e!te°et{!kiö{e!tw{{!wn!kett�pitpwi—{B!neppzwn!nwzmitiwnmitözit—!in!silne—!kett{! in vitro�ittezel!lözing!in-utero e¨pw{öze
Mtöil!{ekzetiwn!inl!twkitiwn!wn!Ui1R1!Httez{!kitkiöm!ntö¨e{!inl!li{tzibötiwn!L[!ittez{!kitkiöm!ntö¨e{!inl!{ignitH[Pi{e!wn!membzineB!mi—�wn!UiRH[Pi{e!in!MDJR!kett{!in vitro; tzin{löktiwn!ki{kile!in°wt°el!inin°wt°e!kHMP� ikti°ite{!kHMP!ze{pwn{e!etement{�w{mwzegötitiwn
Pntez{titiit!inntimmitiwn� Httez{!immöne!{—{tem� Jti{{ikit!inntimmitwz—!mwteköte{Hngiw{ktezw{i{� Httez{!°i{kötiz!kett{! in vitro inl�Httez{!°i{kötiz!zeikti°it—B!nwönl!in
li{zöpt{!°i{kötiz!integzit—� itpezw{ktezwtik!ptiyöe{[öbötiz!wb{tzöktiwn� Jiö{e{!{twögping!wn!zenit!epitpetii�L[!i{!neppzwtw¨ikPzw1w¨iliti°e!metibwti{m� V¨ilitiwn!wn!tipil{0!DUH0!inl�V¨iliti°e!böz{t{!ze{ötting!in
silne—!kett{!in vitro; inkzei{e{�kett!limige2!Lnpinke{!tw¨ikit—!wnSPS1inlökel!nitzik!w¨ile!nwzmitiwn�li°ez{e!lzög{!inl!mikzwbiit!tw¨in{It!xtixttntui
Sö{keptibitit—!tw!innektiwnMötigene{i{
9)!wn!new!PRD!ki{e{!pi°e!nwnimit—!pi{twz—!wn!PRD
Sekwnl!pit!wn!nwzmit!ittetepzwpw{el!i{!neke{{iz—!nwz!(zipil)pzwgze{{iwn!wn!PRD!tzipte¨!DUH{tzöktöze!wn!PRD!gene!mise{!it°ötnezibte!tw!metp—titiwn!ezzwz{
Hnwmitie{!wn!kwtwn!zepwztel!in!=4)PRD!pitient{2!H!pigp!pezkentige!wnliit—{i{!pitient{!pi°e!ikyöizel!nwzmwn!PRD!inlepenlent!wn!i!nimit—pi{twz—!wn!PRDB!bwwet!l—{nönktiwni{!kwmmwnt—!{een!lözing!liit—{i{
Httez{!immöne!{—{tem� Httez{!immöne!{—{temJizkinwgenB!mi—!ikt!°ii!möttipte�L[!zepwztel!tw!be!genwtw¨ik!in!inimit{
mekpini{m{!inktöling!li{zöptel�inl!kiö{e{!DUH!{tzinl!bzeis{! inöptise!wn!nwtite!ze{ötting!in� vitro. Ht!tww!lw{e{0!e¨pibit{!intitömwzp—pwmetp—titiwn!wn!DUH!inl�ikti°it—!in!{wme!kett{p—pezpwmwk—{teinemii2!In-uteroe¨pw{öze!ittez{!embz—wgezie{i{in!zwlent{B!in vivo, {ökp!m—kwtw¨in{tizget!silne—0!ti°ez0!inl!°i{kötitöze
Httez{!göt!integzit—2!Seis—!göt!mi—�Iikteziit!inl!nöngit!innektiwn{!wkközpzwmwte!ib{wzptiwn!wn!mikzwbiit�lözing!liit—{i{2!S—nezg—!wn!L[!witppin{!lözing!liit—{i{!inl!in!PRD2�gtökin{0!lzög{!inl!m—kwtw¨in{!it!tpeO—pezpwmwk—{teinemii!zepwztel!tw�k—{t!i{!tiset—2!L[!in!k—{t{!mi—!bebe!zi{s!niktwz!nwz!kizliw°i{kötiz�lezi°el!nzwm!göt!bikteziili{ei{e!lözing!liit—{i{
[UM0![ömwöz!nekzw{i{!niktwzB!MH0!nitt—!ikilB!LNM0!epilezmit!gzwwtp!niktwzB!JHM0!k—{t1ikti°iting!niktwzB!MDJR0!MilinDizb—!kinine!silne—!kett!tine2
tissue and body fluids has been used as abiomarker for fumonisin-mediated toxicity inexperimental animals and man 112,151. If fumo-nisin plays a role in PKD biology , then altera-tions in sphingolipid levels should be observed;at this time, there is no evidence that defectivepolycystins impact sphingolipid biolog y . Desh-mukh et al. [56] reported lower total sphingolipidcontent in kidneys from phenotypically cysticmice compared with their phenotypically normal
REVIEWS IN MEDICAL MICROBIOLOGY (2000) 11(1)
littermates. There is a paucity of human tissuedata in fumonisin intoxication, fungal infection,and in the early stages of PKD pathogenesis.
Table 2 lists the content of free and total SA andSO in normal human and end-stage ZUN kidneytissue. Although the sample size is small, weobserved the highest ratio of free SA:SO in cystwalls dissected from PKD kidneys showingevidence of fungal glucans and fungal antigens

uewfr0fe!SysymfxeSphingos,ne� CeramidaseN-Acyltrans (erase
VOJO6VO
UO
Otrp}xst�4Nt—kw{ppingwtipil{2!Sötnitile{0� 4Sppingwm—etin0!kwmpte¨!{ppingwtipil{�)!O!Glycosidases &
Pnpibitel!b—!Ru}onxsxns pzwlökelby Fusar,um. Alyewsfwif!toxxns4inl!Hö{tzitinöngin2
VOJO6VO
UO
MICROBIAL FACTORS IN POLYCYSTIC KIDNEY DISEASE� 31
]p{}xtoy{5OoM /!btrxnt�w+1+�1�+12!"S-'�&�'e&!&-'!'!SJwH
SerinepalmitoylfransferaseInhibited by Sphingofungins produced b—Aspergillus and Paecilomyces, ISP-i (akamyriocin &!tpezmwz—mwkilin)!pzwlökel!b—Isaria, Myriococcum, and Mycelia. andlipoxamycin pzwlökel!b—!Streptomyces,
;5Wttospwxnvpnxnt�4JO6VO
NADPH-dependent�UO6Reductase
bpwxnvpnxnt 0bM1� VOJO6VO
Jezimile!S—ntpi{eSphinganineN-Acyltransferase
Pxwysrortrp}xst
(Hllitiwn!wn!peilgzwöpit!kizbwn!5
Dietiz—!uu}onxsxns intez!tpe!zitiw!wn!nzee!SH!tw!nzee!SVlevels by blocking acylation of SA & SO. Dietary levels offumonisin {öbt—pe{!ize!inntöenkel!by kzwp!gzwwing!inl{twzige!kwnlitiwn{0!inl!nwwl!pzwke{{ing2
Mömwzii{n!I0!(MI P )!Y0![JH2!Y6!D!Y 3!D!VOVY0� H3!VO� 4!k46O
JO3�[JH1
JO 3!VY0!JO 3!H 6�UO6�[nkizbiii—tik!ikilAlternaria alternata 0MML1 toxxns ikt!{—nezgi{tikitt—
VY0� VO!VO!witp!MI 5!tw!kiö{e!tw¨ikit—2HHS![w¨in!i0!Y0!D!O2!H 6!D!PkH
I�I�I�J�1�HHS![w¨in!b!Y0!D![JH2!Y 6!D!OJO 3!VY6!JO 3�VO�UO6
bpwxnvosxnt 0b[1� VOJO6VO
UO6UO6
UO� jUOHllitiwn!wn!409!lwöbte!bwnl4� 4
OYwö+!,uilarases
Sphingomyelinase(s)wn!mammalian andmicrobial origin
Pxsruptxon ou }p}}p{xpn spwxnvo{xpxs qxo{ovy b—!microbial toxinsis an emerging theme in innektiwö{!li{ei{e!inl!nwwl!{inet—2Jusgfl!ytxisx!resembling mammalian sphingolipids� 91) inhibit sphingolipid formation by actions at several�Z-[-Zenz—me{!teiling!tw!ibnwzmit!te°et{!wn!{ppingwil!bi{e{0�e4!46) li{zöpt!kettötiz!kwntzwt!pitpwi—{!lepenlent!wn{ppingwtipAl{!b—!inlizekt!inl!lizekt!iktiwn{0!inl� w•3)kiö{e!w¨ilitiwn!wn!membzine!tipil{!inl!DUH� wNprttrxp{ tnsotoxxn i{!zepwztel!tw!inntöenke!{ppingwtipilbiwtwg—!in!min!b—!it!tei{t!tpzee!{epezite!mekpini{m{5)Lnlwtw¨in!kin!inntöenke!tpe!kpemikit!kwmpw{itiwn!wn{ppingwtipil{!pzwlökel!b—!mimmitiin!kett{A!tpe{e!kpinge{inktöle!tpe!legzee!wn!p—lzw¨—titiwn!wn!tpe!U1ik—t!gzwöp!inltpe!nömbez!inl!t—pe{!wn!kizbwp—lzite{!in!tpe!peilgzwöp6) Lnlwtw¨in!{timötite{!{ppingwm—etini{e({)!°ii!k—twsine{ze{ötting!in!kezimile!pzwlöktiwn!nzwm!{ppingwm—etin3) [pe!Sipil!H!mwiet—!wn!enlwtw¨in!it{w!mimik{!tpe!{tzöktöze(in!bwtl!t—pe)!inl!{wme!wn!tpe!biwtwgikit!ennekt{!wn!rtrp}xst6
Rxv6 26 V°ez°iew!wn!{ppingwtipil!metibwti{m!i{!impiktel!b—!enlwtw¨in0!nömwni{in!inl!zetitelm—kwtw¨in{2
UOI o�o�ö_Pw63�)
OV!3V
Sipil!H!mwiet—
nzwm!Pusnrvuz 1 39 1 . [pi{!ete°itel!zitiw!wi{!nwtwb{ez°el!in!pwmwgenite{!wn!silne—!kzw{{!{ek1tiwn{0!wpikp!i{!kwn{i{tent!witp!i!nwkit!lezinge1ment!wn!{ppingwtipil!metibwti{m!witpin!k—{t{2Pn!illitiwn0!tpeze!i{!i!kteiz!tzenl!twwizl!twweznzee!inl!twtit!{ppingwil!bi{e!kw!ttent!in!PKDsilne—!kwmpizel!tw!nwzmit!sil!ne°2!Pn!PKD
silne—!k—{t!ntöil0!nzee!SA inl!SO °itöe{!zingelnzwm!nwt!letektel!(ND) tw!0.44 inl!ND tw5.8 nmwt3mt0!ze{pekti°et—B!twtit!SA inl!SO°itöe{!zingel!nzwm!0.25 tw!55.9 inl!8.8 tw378 nmol/ml cyst fluid, respectively. Free sphin-gwil!bi{e{!ize!zepwztel!tw!e¨pibit!intibikteziitand antifungal activity [57], which might ac-
REVIEWS IN MEDICAL MICROBIOLOGY (2000) 11(1)

44I-
zn
4J)
-7
Table 2. Sppinginine!(SH)!inl!{ppingw{ine!(SV)!te°et{!in!pömin!silne—!{pekimen{
MzeePitient!kpiziktezi{tik{� Rilne—!{impte�SHMite{
Hge!441:4!—eiz{B!nwzmit!silne—� Jzw{{1{ektiwn�452937!—eiz{B!HDPRV� Jzw{{1{ektiwn�542?
Rilne—!pw{iti°e!nwz!enlwtw¨in!b—!lSHS!inl!immönwlwt1btwt0� 42=gtökin!b—!lSHS0!nöngit!intigen{!inl!DUH� 62?
J—{t!witt� 92:Memite{
Hge!441:4!—eiz{B!nwzmit!silne—� Jzw{{1{ektiwn�5:2=5!li—!wtlB!nwzmit!silne—� Jzw{{1{ektiwn�5?2449!—eiz{B!HDPRD� Jzw{{1{ektiwn�62:
Rilne—!pw{iti°e!nwz!enlwtw¨in!b—!lSHS!inl!immönwlwt1btwt� 4255629
J—{t!witt� 30796!—eiz{B!HDPRD� Jzw{{1{ektiwn�903
Rilne—!pw{iti°e!nwz!enlwtw¨in!b—!lSHS!inl!immönwlwt1btwt� 52752:
J—{t!witt� 4265327
45!—eiz{B!HDPRD� Jzw{{1{ektiwn� 72:Rilne—!pw{iti°e!nwz!enlwtw¨in!b—!lSHS!inl!immönwlwt1btwt0!J—{t!witt� :2:
g)ökin!b—!lSHS0!nöngit!intigen{!inl!DUH� 5:2?5426
43!—eiz{B!HDPRD� Jzw{{1{ektiwn� 323Rilne—!pw{iti°e!nwz!enlwtw¨in!b—!lSHS0!immönwlwt1btwt!inl� 52:nöngit!DUH� 62:
J—{t!witt� 624627314
47!—eiz{B!HDPRD� Jzw{{1{ektiwn�627Rilne—!pw{iti°e!nwz!enlwtw¨in!b—!lSHS!inl!inimönwlwt1btwt
SH!inl!SV!te°et{!(pikwmwte{3mg!ti{{öe!pzwtein)
Mzee�Yitiw!Mzee�[wtit�[wtitSV� SHASV�SH� SV
?3426�4244�644=�444:965427�4249�5469�57975792?�424:�:4=�555973?14�4247�:43�=?575:27�4234°�349�953=
6372?�4247�5644�56:=555426�4257�?4=�553=95?2?�4253�97=�=4:7462?�424?�=46�569?79326�4263� 764�544456604�4257�956�=3365?24�426=� 457�:4546929�4247�9=6�=4==6625�4247�:5?�55=443425�4256�:73�556799627�426:�959�54:?94?1?�4259�?=:�534:94:23�4254�5494�?4::4417�423=°�9:3�9?695?24�4294s�74=�:44?6726�4256� 3=:� 73745:24�4254� 369�96=96626�4256� 347� 44555=23�4253�9:?�?=556=25�4254� 344�::446:2=�4253� 349�94=9592=�4257� 456�:645
.Oigpe{t!nzee!SHASV!zitiw{2!Uwzmit!pömin!silne—{!wbtiinel!witpin!3!p!wn!{özgez—!inl!li{{ektel!intw!silne—!kzw{{!{ektiwn{!inl!nzwzen!it!174°J!öntit!i{{i—el2!Mwz!PRDsilne—{0!k—+{t!ntöil{!weze!i{pizitel0!k—{t!witt{!inl!silne—{!li{{ektel!witpin!6!Pt!wn!neppzektwzn—2!Se°et{!wn!nzee!inl!twtit!{ppingwil!bi{e{!weze!letezminel!b—!tpe!metpwlwn!Yww!et it2!(:7e2!Diti!ize!zepze{entel!i{!izei!önlez!OPSJ!peis!yöintiniel!°ii!SV!inl!SH!e¨teznit!{tinlizl!köz°e{0!iljö{tel!nwz!zekw°ez—!wn!JA64!{ppinginine!inteznit{tinlizl!(gint!wn!H2!O2!Mezzitt!Qz2!Lmwz—!Uni°ez{it—0!Httinti0!Newzgii0!USH)0!inl!nwzmiti{el!b—!ti{{öe!pzwtein!kwntent!5:=52!Mein!zekw°ez—!wn!inteznit!{tinlizl!nzwm!silne—kzw{{1{ektiwn!inl!k—{t!witt!wi{!9=)!inl!:4)0!ze{pekti°et—2HDPRD0!Hötw{wmit!lwminint!pwt—k—{tik!silne—!li{ei{eB!lSHS0!linnezentiit!Limu!us Hmebwk—te!S—{ite!i{{i—2
QzziUUm

MICROBIAL FACTORS IN POLYCYSTIC KIDNEY DISEASE� 33
count for the failure to recover common bacteriaand fungi from cyst fluid.
Males are known to have higher levels ofkidney sphingolipids than females [58], whichis also observed in PKD individuals (Table 2). InPKD, males exhibit a higher incidence andseverity of kidney lesions [5,6], responsivenessto the anticystic effects of lovastatin [59], andexcretion of nanobacterial antigens than females.In normal animals, males excrete greateramounts of sphingolipids and are more sensi-tive to the nephrotoxic effects of fumonisin thanfemales [48].
Alteration of sphingolipid biology has beenproposed as important to the integrity of thegastrointestinal tract during fumonisin intoxi-cation [15]. Supplementation with dietarysphingolipids was reported to reduce coloncarcinogenesis while broader associations be-tween cancer, sphingolipid intake, infectiousdisease and exposure to fumonisin and relatedmycotoxins were beginning to be recognised[15,58]. Fumonisin BI is reported to alter theactivity of the folate binding protein (FBP) [60],which may result in a functional folate defi-ciency and subsequent vulnerability to muta-genesis and cancer [61]. Because kidney FBP isresponsible for recovery of >95% of filtered
folate [62] and thus preservation of stores offolate, fumonisin-induced disruption of thefolate recovery pathway may indirectly affectextra-renal tissues also.
As shown in Fig. 2, endotoxin is reported toalter sphingolipid metabolism, exhibit ceramide-mimetic properties, and share transport mechan-isms between tissues and intracellular compart-ments [63]. In PKD cells, the Golgi apparatus,the intracellular site of complex sphingolipidformation and sulphation reactions, shows al-tered transport of sphingolipids [64] and dimin-ished sulphation of glucosaminoglycans [65].Taken together, a plausible case for the actionsof microbial toxins on PKD sphingolipid biologycan be made.
cTQaM]h [R ]WP Mb MZ UZRQOcU[dbPUbQMbQ MZP7[a YUOa[NUMLc[gUO[bUbRemarkably, many PKD treatments that attemptto correct defects in mammalian cell biology alsoexhibit antimicrobial effects and/or diminish theabsorption of microbes and their toxins from thegut (Table 3) [8]. For example, reduction of tissueinflammation can occur by decreasing the re-activity of the PKD kidney to inflammatory
cpq{t ;6 Treatments shown to preserve kidney function in genetically cystic animals listed with theirantimicrobial properties and actions on PKD tissuesPromising therapies�Proposed mammalian targets�Possible microbial targetsOral potassium citrate/citric�Alkalinising agent that decreases�Optimum pH for most fungal growthacid solution�ammonia production and intracellular�is 6.5; alkalinising body fluids would
acidosis leading to slower rates of cell�diminish fungal growth. Inhibitsproliferation; antioxidant action decreases growth of nanobacteria, which maytissue inflammation, and reduces kidney�result in diminished stone formationstone formation by chelating calcium�and reduced tissue inflammation
Methylprednisolone�Decreases kidney inflammatory�Decreases entry of microbialresponse thereby reducing tissue�components from gut due todamage and resultant poorly�anti inflammatory actions on gutregulated tissue repair�enterocytes
Lovastatin�Blocks synthesis of lipid-linked regulatory�Exhibits antifungal activityproteins yielding decreased cell growth
Flax seed�Increased excretion of urinary citrate�Citrate inhibits growth of nanobacteriaSoy protein�Diminished production of pro-inflammatory�v{ vvtr}5 EPA reported to protectFish oil (EPA)�lipids�against bacterial infections1-Phenyl-2-decanoyl amino-3-�Inhibits synthesis of glycosylation of�Nearly all fungi and some bacteriamorpholino-1 . propanol�ceramide thereby partially�produce complex sphingolipids,
correcting imbalances in sphingo-�which are required for their growthlipid subtypes in PKD kidney�and survival
PKD, polycystic kidney disease; EPA, eicosapentaenoic acid.
REVIEWS IN MEDICAL MICROBIOLOGY (2000) 11(1)
:;� HJELLE ET AL.
stimuli and by decreasing the absorption ofendotoxin and fungal glucans from the gut bydecreasing inflammation of the gastrointestinaltract. The role of diet and drugs [65] in alteringthe growth of colonising /infecting microbes andthe production of microbial toxins is an emer-ging area of research not only in food safety [15],but in both chronic and genetic diseases.
aQRQaQZOQb1. Fredricks D, Relman D: Sequence-based identification ofmicrobial pathogens: a reconsideration wn Kochs postu-lates. CtqqB Rqkrwjqit Wm}, 1996, 9:18-33,
2. Cassell GH; Infectious causes of chronic inflammatorydiseases and cancer. JvBkr, Nvnrkq Iq{ 1998, 4:475-487.
3. BaIter M: 19th Century rules of causation outdated?Skqmvkm 1998, 282:220.
4. Hooper J: A new germ theory , Fqtivqqq Rwv}3tq0 1999,283:41 -53.
5. Gabow PA, Johnson AM, Kaehriv WD, it it2B Factorsaffecting the progression of renal disease in autosomal-dominant polcvstic kidney disease 5,2qlqqq,q0 tqqq 1992,41:1311-1319.
6. Martinez RR, Grantham JJ: Polvcvstic kidne y diseaseetiology , pathogenesis, and treatment, 0hz Mo,:!!, 1995,41:698-765,
7. Grantham JJ: The etiolog y, pathogenesis, and treatmentof autosomal dominant polvcvstic kidney disease: recentadvances. Fv0 O Pqlvmy Iq{ 1996, 28:788-803
8. Torres VE: New insights into polvcvstic kidne y diseaseand its treatment, Cçrr TC,qqB Smxtqrwt N n¸C,q,r}q,v{ 1998.7:159-169.
9. Calvet JP: Molecular genetics of po)vcvstic kidneydisease. / Sq,xprwt 1998, 11:24-34.
10. Germino CC: Autosomal dominant polvcvstic kidneydisease: a two-hit model, Mw{xq}it Urik}z , 1 1i7. 32.81 - 102
11. Richards Jl_, Haves AW (Editors). �ljvIui ot Hiti;uiiGqq,twgq00 2nd Edit, Vol 6. San Diego. �Press,1997:5-17
12. Riley RT: Mechanistic interactions wn mvcotosin'z' th,'ir-etica I considerations. In R q}kw}0 qq,00B qv Frç,q0tq qq vvv&Fwwl Sinq,}qq2 Edited h',' Sinha KK, Bh,i tniglr 1) Nci"York: Marcel Dekker; 1998:227-253.
13. Hamann L, EL-Samalouti V. Ulmer Al. mn it2 Compo-nents of gut bacteria as immunomoduldt,N. qvB N N wnRqkrw!,qwt 1998, 41:141-154
14. Ciacci-Zanella JR, Jones C: Fumonisin I!., a m',ci't",incontaminant of cereal grains, and indUccr 0,qvia the tumor necrosis factor pathi'.i�and ki{xiq,activation. Fwwl Cp},vq Ywxqkw! 1999, 37:71fl -.712
15. Vesper H, Schmelz EM, Nikolova-Kar,ik,i'hian I\, m}i!0B Sphingolipids in food and the emerging inlpiirtanci'of sphingolipids to nutrition, / Sqqqr 1999. 129 231-1230
16. Pinelli E, Poux N, Garren L, tv n&35 Activation ot nutogcn.activated protein kinase by fumonisin B: stimulate'scPLA: phosphorylation, the arachidonic acid c,iscadcand cAMP production. Cirkq0qw0w,0qq,{0{ l[$5 20:1681- 1688
17. Dugyala RR, Sharma RP, Tsunoda M, Rile', RI. Tumornecrosis factor-a as a contributor in tumonisin Btoxicity . / UpivB Jxx Y3qkr 1998, 285:317-324.
18. Sahu SC, Eppley RM, Page SW, il a!: I't'roxidation of
membrane lipids and oxidative DNA damage byfumonisin B, in isolated rat liver nuclei. Cancer Qm}}1998, 125:117-121.
19. Yin JJ, Smith MJ, Eppley RM, kq al.: Effects of fumonisinB 1 on lipid peroxidation in membranes. GBwkpBvq Gqwx.Bqq{Fli 1998, 1371:134-142.
20. AbadoBecognee K, Mobio TA, Ennamanv R, kq it2BCvtotoxitv of fumonisin B 1 : implication of lipid perox-idation and inhibition of protein and DNA syntheses.Frkp Ywxqkw! 1998, 72:233-236.
21. Rotter BA, Oh YN: Mycotoxin fumonisiri B, stimulatesnitric oxide production in a murine macrophage cellline. Si}çrit Ywxqv 1996, 4:291-294.
22. Hoyt DG, Mannix RJ, Gerritsen ME, kq i!0B Integrinsinhibit LPS-induced DNA strand breakage in culturedlung endothelial cells. FvB / Upq5{qwt 1996, 270:L689-L694,
23. Ciftcioglu N, BjorkJund M, Kuorikoski K. kq i!0B Nano-bacteria: an infectious cause for kidne y Stone formation,Pqlvmqt Oç} 1999, 56:1893-1898.
24. Werder AA, Amos MA, Nielsen AH, Wolfe GH:Comparative effects of germfree and ambient environ-ments on the development of c ystic kidney disease inCFW wd mice, / Qij CqqCB Rkl 1984, 103:399-407.
25. Gardner KID Jr. Evan AP, Reed WP: Accelerated renalcyst development in deconditioned germfree rats. PqlvmyJut 1986, 29:1116-1123.
26. Gardner Jr KID, Reed WP, Evan AP, kq i!0B Endotoxinprovocation of experimental renal cystic disease. PqlvmqOç} 1987, 32:329-334.
27. Schwab 5, Bander 5, Saulo K: Renal infection autosomaldominant polycystic kidney disease. Fv0 3 Rkl 1987,82:714-718.
28. Sklar A, Carunana RJ, Lammers JE, Strauser GD: Renalinfection in autosomal dominant polyc ystic kidneydisease. Fu / Pqlvmy Iq{ 1987, 10:81-88.
29. Roscoe JM, Brissenden JE, Williams EA, kq al.: Autosomaldominant polvcvstic kidney disease in Toronto. Pqlçkq0tqqq 1993, 44:1101-1108.
30. Bjarnason I, Macpherson A, Hollander D: Intestinalpermeability: an overview. Li{!rwq,çtq,rw!w0çq0 1995, 108:1566-1581.
31. Nolan JP: Intestinal endotoxins as mediators of hepaticinjury - an idea whose time has come again. M-xi}wqmyy1989, 10:887-891.
32. Ohavashi T, Yoshida M, Mori T, kq al.: Plamsa 0 -7.-nt-w-glucan measurement in diagnosis of invasive deepmycosis and fungal febrile episodes. Qivkm} 1995, 345.17-20.
33 Yoshida M, Obayashi T, Iwama A, kq al.: Detection ofplasma (1-3)-13-1)-glucan in patients with Fç{irv0v00Yrqkqqw{xwrwBq0 Sikk3Birwvqyk},{ and FkrkvBwçqqqvq fungaemias.N Rml [m} Rykw! 1997, 35:371-374.
34. Miller MA, Prior RB, Horvath F, Hjelle iT: Detection ofendotoxiuria in polcvstic kidney disease patients by theuse of the Lnuuius Amebocyte Lysate assa', Fv} 3 PqlvmyDis 1990, 15:117-122.
35. Hide JT, Miller-Hjelle MA, Poxton IR, m} al.: Endotoxinand nanobacteria in polycystic kidney disease, Pqlvmy Oç}(in press).
36. Gardner Jr KD, Burnside JS, Elzinga LW, Locksley RM:Cvtokines in fluids from pol ycystic kidneys. Pqlvmy Oç}1991, 39:718-724.
37. Walsh TJ, Chanock SJ: Diagnosis of invasive fungalinfection: advance in nonculture systems. Cçrr CqqBB Ywxqvnmk} Iq{ 1998, 18:101-153.
REVIEWS IN MEDICAL MICROBIOLOGY (2000) 11(1)
MICROBIAL FACTORS IN POLYCYSTIC KIDNEY DISEASE� 35
38. Smith 1MB: Opportunistic mycoses-some priorities forthe 90's. N Zealand Mcd 11991, 104:420.
39. Miller-H;elle MA, HjelIe JT, Jones M, ci al.: Polvcvstickidney disease: an unrecognized emerging infectiousdisease? Enierg Jul Djs 1997, 3:113-127,
40. Lappalainen S. AL Pasanen, Reiman M, Kalliokoski F':Serum igG antibodies against Wa//emia sehi and Fusariunispecies in Finnish farmers, Ann Al/ergi, Asthma Imniunoi1998, 81:585-592.
41. Perfect JR, Schell WA: The new fungal opportunists arecoming. C/in Infect Dis 1996, 22 (suppl 2):S112-118.
42. Kaufman 1, Standard PC, Jalbert M, Kraft DE: Immuno-histotogic identification of Aper,,,'iIlus spp and otherhyaline fungi by using polvclonal fluorescent antibodies,Clot Microbiol 1997, 35:2206-2209.
43. Hopfer RL: Contemporary techniques to moleculardiagnoses of mycoses. C/rn Microl'iol Neii's 1997,19:169-173.
44. Peterson SW, Cornelli S. Hjelle JT, ci a!,: Pi'nicill,u,,,1iimi!t'ouien5e sp. nov.' a new speices isolated fromhuman polvcvstic kidne y cell cultures Mwcoh','ia 1999,91:269-277.
45. Ansorg P. van den Boom P. Rath M Detection ofAspc'r'5'illus galactomannan antigen in foods and anti-biotics. Mijcoo- 1997, 40:353-357
46. Miller ID: Editorial Natural Toxin 1995, 3:343.47, Bhat R\', Shettv PH, Amruth RP, Sudershan RV: A food
borne disese outbreak due to the consumption of moldssorghum and maize containing fumonisin mvcotoxins,Chi; Toxic;! 1997, 35:249-253.
48. Bucci TJ, Howard I'C, Tolleson WH, ci 0/.: Renal effectsof fumonisin rnvcotoxins in animals, Tox,ci'l Pat/si 1998,26:160-164.
49. Munkvold CF, Desjardins AE: Fumonisins in maize. Canwe reduce their occurrence? Plant Die 1997, 81:556-565.
50 Munkvold GE'. I lellmich RE, Rice LG: Comparison 01tumonisin Concentration in kernels of transtc'nic Btmaize hybrids and nontransgenic h ybrids, /'lant Di1999, 8313(1-138
31 Krogh F'. Mvcotosic nephropathv in Mi,'tov,,i Editedby Purchase EFH Amsterdam: Elsevier, 1974.4114-428
52 Celderhlorn WCA, Krick Nil, Marasas WFO. Thiel 1'GTosicit' and carcinogenicitv of the J-'usarun,, ,,ii',iiliti'r,ni'metabolite, turn on i sin 131 in rats. Ca ri'i,ii'i,'i',ii'.i�199 I12:1247-1231
33 Miller I Mvcotosins In Or,\'a,iu' Dusts' Li'i';ir,'. l:ocv.and Pr;'; 'cut;,',;, Vol 4S. Edited by Ry lander P. Jacobs PBoca Raton' Lewis Publishers, 1994:57-70
54. Fogelmark B. Sjostrand M, Rvlander P i'ulrnon,irvinflammation induced bv repeated inhalations 7$
0-glucan and endotoxin. In! / Exj' Path 1994, 75:85-90.55. Merrill Jr AH, Liotta DC, Riles' RT: Fumonisins: fungal
toxins that shed light on sphingolipid function, Tre,i,IeCell Biol 1996, 6:218-223.
56. Deshmukh GD, Radio NS, Gattone V. Sha yman JA:Abnormalities of glvcosphingolipid, sulfatide, and cer-amide in the polvcystic (cpk ,!cpk) mouse. J Lipid Res1994, 35:1611-1621.
57. Bibel DJ, At)' R, Shah 5, Shinefield HP: Sphingosines:antimicrobial barriers of the skin. Acta Derm VenerealSuppl (Stock/i) 1993, 73:407-411.
58. Shavman JA, Radin NS: Structure and function of renalglycosphingolipids. Am I Ph ysiol 1991, 260:F291-F302.
59. Cite RD, Cowlev Jr DB, Gattone ii \'H, ci al.: Effect oflovastatin on the development of pol ycvstic kidneydisease in the Han:SPRD rat. Am I Kidnei1 Dis 1995,26:501-507.
60. Stevens VL, Tang J: Fumonisin BI-induced sphingolipiddepletion inhibits vitamin uptake via the glvcosvlpho-sphatid ylinositol-anchored folate receptor. / Biol C/ieni1997, 272:18020-18025.
61. Blount BC, Mack MM, Wehr CM, et al.: Folate deficiencycauses uracil misincorporation into human DNA andchromosome breakage: implications for cancer andneuronal damage. Proc Nat! Acad Sci USA 1997,94:3290-3295.
62. 1-Ijelle JT, Christensen El, Carone FA, Selhub J: Cellfractionation and electron microscopic studies of kidneyfolate-binding protein. Am I Physiol 1991, 260:C338-C346.
61 Thieblemont N, Wright SD: Mice genetically hvpo-responsive to lipopolsaccharide exhibit a defect inendocy tic uptake of LPS and ceramide, / Exp Mcd1997, 185:2095-2100,
64. Bacallao R, Carone FA, Nakamura 5, Wandinger-Ness A:Evidence for a Golgi complex defect in autosomaldominant polvcvstic kidney disease. / Am Soc Nep/irol1994, 5:618,
65. Carone FA, Bacallo R, Kanwar YS: The biology ofpolvcvstic kidney disease. Lab Invest 1994, 70:437-448,
tin, Cardenas ME, Cruz MC, Del Poeta M, ci al.: Antifungalactivities of antineoplastic agents: Sacc!iaroniices cerez',siacas a model system to studv drug action. C/ni MicrohiolRe; 1999, 12:583-661.
67. Yoo HS, Norred WP, Riley RT: A rapid method forquantif y ing free sphingoid bases and complex sphingo-lipids in microgram amounts of cells following exposureto tumonisin Bi. Toxicol ]it �1996, 10:77-84,
65 town OH, Rosenbrough NJ, Farr AL, Randall RI:Protein measurement with the Folin phenol reagent. IBa'! C/ic,,; 1951, 193:265-275,
Supplied by the U.S. Department of Agriculture,National Center for Agricultural Utilization Research,Peoria, IL.
REVIEWS IN MEDICAL MICROBIOLOGY (2000) 11(1)