Kidney and vasculitis part 1 General approach and interactive cases
87
Ahmed Yehia Ismaeel Ass. Lecturer Bani-Sweif Nephrologists & Vasculitis
-
Upload
- -
Category
Health & Medicine
-
view
414 -
download
0
Transcript of Kidney and vasculitis part 1 General approach and interactive cases
Ahmed Yehia Ismaeel
Ass. Lecturer
Bani-Sweif
Nephrologists
&
Vasculitis

BLOOD VESSELS

Pathology in blood vessels
Congenital Anomalies
Arteriosclerosis
HTN
Vasculitides ( inflammations)
Aneurysms & Dissections
Veins & Lymphatics
Tumors
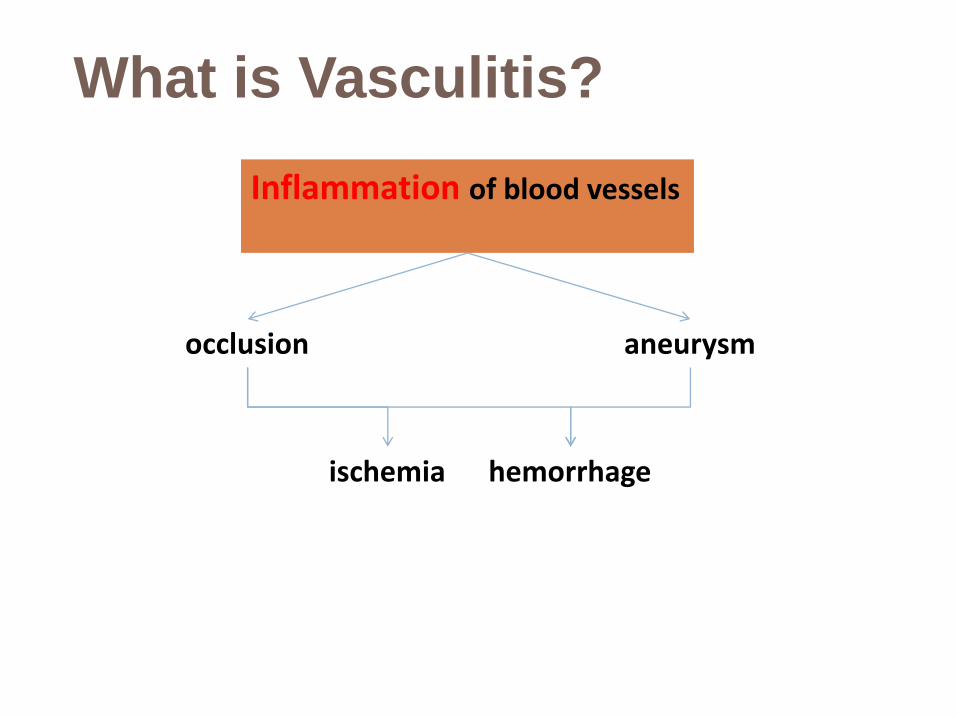
What is Vasculitis?
Inflammation of blood vessels
occlusion aneurysm
ischemia hemorrhage

WHICH BLOOD VESSELS
ARE AFFECTED?
ANY BLOOD VESSEL CAN BE AFFECTED:
ARTERIES
ATERIOLES
CAPILLARIES
VENULES
VEINS
CAN DAMAGE VIRTUALLY ANY ORGAN OR
TISSUE.

Vasculitis classification
According to:
Size of Vessels involved
Site of involvement
Characteristic Features



CLASSIFICATION OF
VASCULITIS1990- American College of Rheumatology
(ACR) Classification Criteria
1994- Chapel Hill Consensus Conference (CHCC)
European Medicines Agency developed a stepwise algorithm for vasculitis in 2007
CHCC definitions were revised in 2012
•ANCA testing not
included
•PAN and MPA put
togather
•Size of blood vessel (tissue
Bx)
•PAN and MPA seperated
•ANCA suggested
•AAV- WG, CSS, MPA
•ACR
•Lanham crietria for
CSS
•ANCA
•CHCC defination


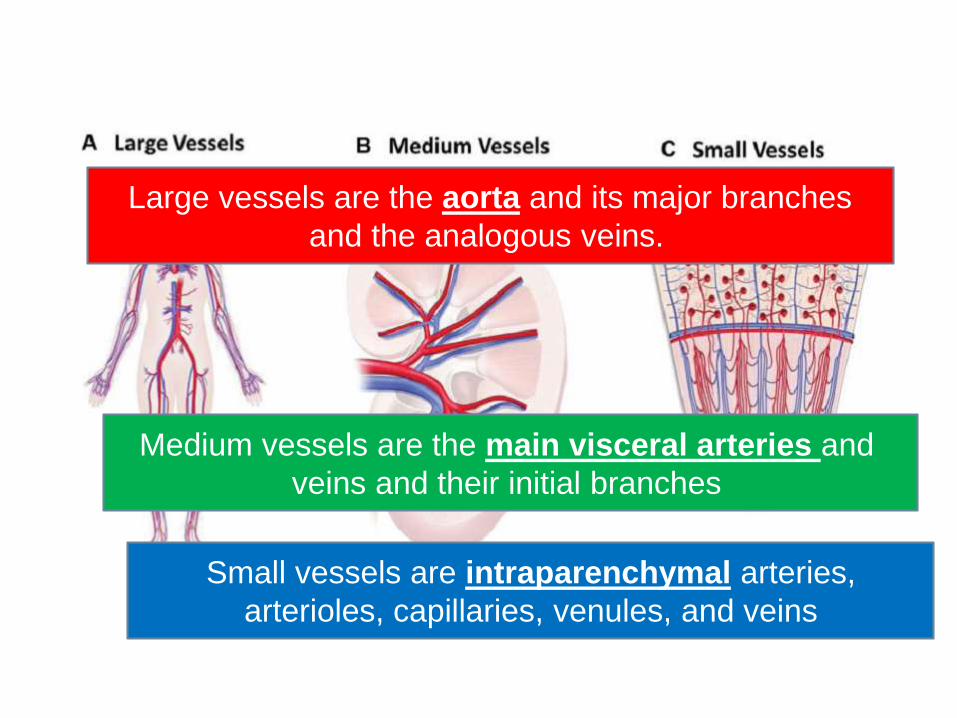
Large vessels are the aorta and its major branches
and the analogous veins.
Medium vessels are the main visceral arteries and
veins and their initial branches
Small vessels are intraparenchymal arteries,
arterioles, capillaries, venules, and veins



Case
A-57-year old male was admitted to
nephrology unit because of renal dysfunction
and severe anemia. One month before
admission, he was in a relatively good health.
Physical examination on admission revealed
BP 140/100, temperature: 37.3ºC and apical
systolic murmur was found.
Caspian J Intern Med 2012; 3(3): 496-499

Early laboratory examination revealed
s.creatinine: 2.8 mg/dl, BUN: 94 mg/dl,
urinalysis; 2+ proteinuria / hematuria,
WBC: 8700/µl, hemoglobin: 7.3 g/dl,
ESR: 110 mm/h, CRP:+ve
24 hours urine :800 mg/day proteinuria.
Negative results for hepatitis B and hepatitis
C infections.

S. complement C3: 53 mg/dl (90-180),
C4: 15 mg/dl (10-40), CH50: <50 (70-150U)
Anti-GBM antibody: 5.8 U/ml (< 15)
PR3-ANCA: 45 U/ml (<0.4),
MPO- ANCA: 0.1 U/ml (<3.1U/ml),
Rheumatoid factor (RF): 2+ positive,
(ANA):1+ positive,
(anti-dsDNA) and anti-cardiolipine antibodies : -
ve.
Ultrasound :increased renal parenchymal
echogenicity, RT kidney size :112mm & LT :

Renal biopsy revealed focal and segmental
glomerular necrosis with an increase in
mesangial matrix, capillary lumen narrowing
and closure without hypercellularity.
An immunofluorescent study showed IgG, IgM,
and C3 deposit in the mesangial regions.

What is the first line of
treatment?

Renal biopsy was performed and with the
suspicion of renal limited ANCA associated
(RPGN),
methylprednisolone pulse therapy, 500 mg
daily for two consecutive days was started.

3 days after receiving steroid therapy the
patient’s general condition worsened and
started chilling with high grade fever.
Blood culture was performed and empiric
antibiotic therapy with 3rd generation
cephalosporin and vancomycin were started.
Echocardiography: multiple large vegetations
on the aortic valve, severe aortic
regurgitation with pseudoaneurysm
formation with systolic bulging.
TEE confirmed the findings.

The patient became afebrile after the start of IV
antibiotic therapy with ceftriaxone, gentamicin and vancomycin. His fever dropped within 72 hours, then he underwent cardiac surgery and aortic valve replacement.
After 2 months, the patient’s general condition improved dramatically and his serum creatininelevel was1.7 mg/dl hemoglobin reached 12 mg/dl.
The results of PR3-ANCA, RF and ANA negative and C3 serum level level returned to normal.
Message from the case
Sub-acute bacterial endocarditis
(SBE) can rarely manifest with
features of SVV.
It is usually attributed to
microembolism and the effects
of circulating immune
complexes on the vascular
endothelium.

The differentiation
The differentiation between SBE induced
vasculitis and primary SVV can be difficult
sometimes especially if the heart murmur is
absent.
The minor criteria for SBE including fever,
GN and purpura are similar to the manifestations
of primary AAV.
Osler's nodes, Janeway lesions and splinter
hemorrhages typical for SBE may mimic
cutaneous vasculitis .

Non-infectious endocarditis sometimes is a part
of a clinical spectrum of systemic vasculitis.
The D.D. is much more difficult when a culture-
negative SBE has positive laboratory test results for
ANCA.
Misdiagnosis of SBE as AAV and an inappropriate
immunosuppressive therapy can have
catastrophic consequences.


AKI can complicate the course of SBE as :
1. infection induced interstitial nephritis,
2. acute tubular necrosis,
3. glomerulonephritis and
4. antibiotic related interstitial nephritis.
Clues for secondary
vasculistis??
Double ANCA positivity.
Low levels of serum complement.
Multiple antibody positivities: e.g.RF, ANA,
cryoglobulins and anticardiolipin antibodies.
The patients with primary ANCA associated
vasculitis have higher rate of nasal and sinus
involvement.
The biopsy

The common denominator in all types of RPGN is severe glomerular injury
SUMMARY OF CLASSIFICATION
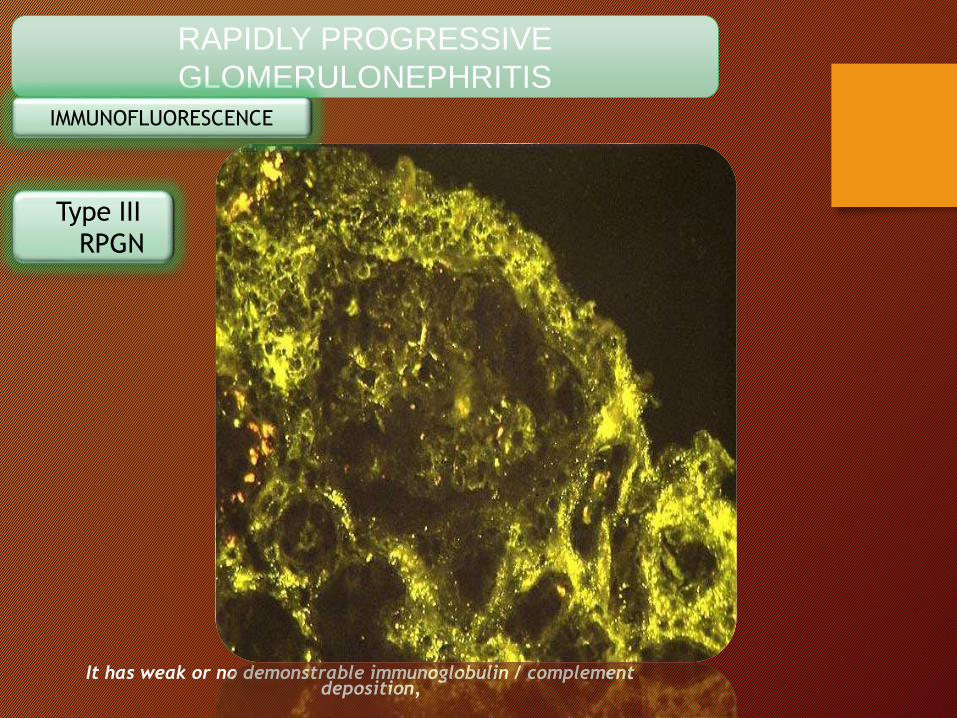
It has weak or no demonstrable immunoglobulin / complement deposition,
RAPIDLY PROGRESSIVE
GLOMERULONEPHRITIS
Type III
RPGN
IMMUNOFLUORESCENCE
Abstract
Objective: Chronic infections tend to induce the production of ANCA.Infective
endocarditis (IE) has been reported to exhibit positive ANCA tests and to mimic ANCA-
associated vasculitis, which may lead to a misdiagnosis and inappropriate treatment.
The aim of this study was to clarify whether there is any difference in the clinical features
between ANCA-positive IE and ANCA-negative IE.
Methods: A retrospective study was carried out on 39 IE patients whose (PR3)-ANCA
and (MPO)-ANCA levels were measured. After dividing the patients into ANCA-positive
and ANCA-negative IE, we compared their clinical features.
Results: we compared 13 ANCA-positive IE patients with 26 ANCA-negative IE
patients. All 13 ANCA-positive IE patients were PR3-ANCA positive. The prevalence of
lower limb edema, LDH level and positive blood cultures rate were higher in ANCA-
positive IE group, but there was no significant difference in other clinical features.
Conclusion: if a patient presents with fever, arthralgia, skin rash and
is ANCA-positive, appropriate steps should be taken to
exclude infection (especially IE) before confirming the diagnosis
of ANCA-associated vasculitis and embarking on long-term
immunosuppressive therapy.Ying C-M, Yao D-T, Ding H-H, Yang C-D (2014) Infective Endocarditis with Antineutrophil Cytoplasmic Antibody: Report of 13 Cases and Literature
Review. PLoS ONE 9(2): e89777. doi:10.1371/journal.pone.0089777

Hepatitis B virus
PAN
Hepatitis C virus
Cryoglobulinemic vasculitis

A case from Bani-Sweif (our
department)
A 28 year old male patient, complaining of shortness of
breath for 3 months duration.
**3 months prior to admission:
Dyspnea on moderate exertion progressing to dyspnea at rest with orthopnea and P.N.D.
**2 months later:
Periorbital puffiness, associated with bilateral lower limb swelling & abdominal distension.
Throughout illness: constitutional manifestations, recurrent epistaxis & occipital headache .

On Examination
• Radial Pulse: 88/min, regular, of big pulse
• Blood Pressure:
(230/140 mmHg) • Respiratory Rate: 30/min.

Investigations
Laboratory work up:Na: 139 mEq/L.K: 4.5 mEq/L.Blood urea: 65 250 mg/ dL. Serum creatinine: 1.9 6.8 mg/dLCRP: +ve (48 mg/L). ESR: 45 mm / 1st hour.Serum albumin: 3.4 gm %. Total proteins: 6.4 gm %.Urine analysis: Granular casts (++) & albuminuria (++). 24-hours urine collection for albumin: 465 mg / day. CBC: Normocytic&normochromic anemia.Lipogram: Normal
Viral markers: -HBs Ag: -ve HBc Ab: - ve-HCV Ab: -ve-HIV Ab: -ve

Abdominal Ultrasound:
-Rt. kidney is small in size (7.5 x 2.5 cm) with grade II echogenic parenchyma.
Colour duplex of both renal arteries:
Rt. renal artery is attenuated distally .
DTPA Scintigraphy (split renal function):
17% residual contribution of Rt kidney.

Next step?

Is it fibromuscular
dysplasia?

Is it atherosclerotic?

So, MRA of the aorta & its main branches:
Stenosed Lt. subclavian and Lt common carotid arteries.
• Angiography of the aorta & its main branches:
-Attenuated Rt. renal artery.
-Aortic arch shows normal origin and caliber of both the innominate and Lt. common & carotid arteries.
-The origin of the Lt. subclavian artery is obliterated.
-The Lt. subclavian fills from the vertebral artery.

Diagnosis?

Diagnosis
TAKAYASU
ARTERITIS
(The occlusive
thromboaortopathy or
pulseless disease)

Clues not to be missed
From history : Marked constitutional
symptoms.
From investigations : ++ acute phase reactants
Abdominal Ultrasound:
-Rt. kidney is small in size (7.5 x 2.5 cm) with grade II echogenic parenchyma.
Colour duplex of both renal arteries:
Rt. renal artery is attenuated distally

The most important & easiest
clue
which is usually missed:•Radial Pulse: 88/min, regular, of big pulse volume on the Rt side but absent on the Lt side, all other peripheral pulses were felt with no radio-femoral delay.
•Blood Pressure:Rt. arm (230/140 mmHg) Lt. arm (150/100 mmHg).

AHA recommendations
The AHA recommends that at least two readings be taken, with a one-minute interval between them, and the average of the measurements recorded. The firstreading in a series is usually the highest. Additional readings should be taken if the difference between the first two is greater than 5 mm Hg
At the first visit, blood pressure should be measured in both arms, which may be useful for identifying coarctation of the aorta and upper-extremity arterial obstruction. If there is a consistent difference in measurement between the arms, the highest pressure should be recorded. In children, the right arm is always preferable for consistency and comparison with reference tables.
Am Fam Physician. 2005 Oct 1;72(7):1391-1398.

European Society of Hypertension
recommendations
The recommendation is that bilateralmeasurement should be made on
first consultation and, if reproducible
differences greater than 20 mmHg for
systolic or 10 mmHg for diastolic pressure
are present on consecutive readings, the
patient should be referred to a
cardiovascular centre for further evaluation
with simultaneous bilateral measurement
and the exclusion of arterial disease .Journal of Hypertension 2003, 21:821–848

Diagnostic pathway
1.Suspect
2.Investigate:
systematic,
serology,
biopsy
3.Exclude mimics
and identify
drivers

Step one: When to suspect
vasculitis?
Step two: The diagnostic strategy
Having considered the possibility of primary vasculitis we suggest you try to answer the following questions in
succession:
Is this a condition that could mimic the presentation of vasculitis?
Is this a secondary vasculitis?
How do I confirm the diagnosis of vasculitis and what is the extent of the disease?
What specific type of vasculitis is this?

1.When to suspect vasculitis?
1.Constitutional features:fatigue,
weight loss, night sweats and low grade fever (the B-symptoms), weakness & anorexia.
2.Musculoskeletal :
Myalgias , arthralgia & arthritis.
3.Skin:
Palpable purpura , digital infarction , punched out ulcers & livido reticularis.
4.Multisystem involvement(according to the type of vasculitis)

When to suspect vasculitis
Presence of following findings alone or in combination or other bizarre systemic manifestations should raise the suspicion of vasculitis - – Occlusive arterial disease or hypertension in young adults.
– Unexplained fever, weight loss.
– Unexplained proteinuria with or without casts.
– Splinter haemorrhages in nails
– cutaneous lesions - palpable purpura, erythema, subcutaneous nodules or urticaria.
– Sudden retinal vascular disease without hypertension or diabetes.

2.Rule out vasculitis mimickers (they cause vessel
occlusion without true inflammation):
1.Cholesterol embolization.
2.antiphospholipid syndrome.
3.infective endocarditis embolism.
4.chronic egotism.
5.atrial myxoma with emboli

•Persistent headache with sudden visual impairment (monocular blindness) in elderly.
•J aw claudication
•Sudden appearance of peripheral neuropathy - wrist drop, foot drop.
•C erebrovascular/cardiovascular events in young.
•Unexplained finding of pulmonary nodular/cavitatory lesions.
Mimicks of vasculitis
Mimicks of vasculitis

Challenging mimickers of
primary systemic vasculitisThe need to distinguish true primary systemic vasculitis from its
multiple potential mimickers is one of the most challenging diagnostic conundrums in clinical medicine. This article reviews 9 challenging vasculitis mimickers:1. fibromuscular dysplasia, 2. calciphylaxis, 3. segmental arterial mediolysis,
4. antiphospholipid syndrome,
5. hypereosinophilic syndrome,
6. lymphomatoid granulomatosis,
7. malignant atrophic papulosis,
8. livedoid vasculopathy, and
9. immunoglobulin G4-related disease.
Rheum Dis Clin North Am. 2015;41(1):141-60,

In particular, infections deserve careful attention, as they are major mimics of vasculitis and would be
aggravated by medication aimed to suppress vascular inflammation. Infective endocarditis should always be
considered. It is known to mimic vasculitis. Although the endocardium is the primary site of infection, it often
results in multisystem manifestations, involving several organs. Bacteraemia and peripheral embolic events
are common. Circulating immune complexes may lead to immune responses most often affecting the skin, the
kidney and the central nervous system.
Differential diagnosis is not always simple.
EULAR on-line course on Rheumatic Diseases
Diagnostic strategies in rheumatology – In-depth discussion 1 – Module 1
©2007-2014 EULAR

Clinical and laboratory
similarities between infection
and vasculitis Clinical findings:
• B-symptoms (fatigue, weight-loss, fever)
• myalgia
• arthralgia
Laboratory findings:
• normocytic normochromic anaemia
• lymphocytosis
• thrombocytosis
• elevated ESR
• raised CRP

Laboratory work up for the evaluation of suspected
vasculitis and for determining systemic involvement:

-DIRECTED:
1.blood cultures.
2.Infection serologies
3.ANA, RF
4.Antiphosphlipid antibodies.
5.C3 / C4 / CH50
6.Cryoglobulins.

-Other diagnostic studies.
1.chest X-ray or CT scan
2.Sinus X-ray or CT scan.
3.Brain CT or MRI
4.EMG, NC studies.
5.ECHOcardiography

3.Exclude Secondary vasculitis
(Exclude underlying cause)
1. Infection related vasculitis ( HB&CV-IE)
2. Connective tissue diseases : RA ,SLE Sjögren's
syndrome, inflammatory myopathies
3. Inflammatory bowel disease.
4. Malignancy related vasculitis: Lymphom, leukemia,
myeloproliferative or myelodysplastic syndromes.
5. Drugs


• These lists pose an important practical problem: immediate onset of immunosuppressive treatment might be
• lifesaving in primary vasculitis – but it could be fatal for one of the other conditions.
• A structured diagnostic approach is indispensable.
EULAR on-line course on Rheumatic Diseases
Diagnostic strategies in rheumatology – In-depth discussion 1 – Module 1
©2007-2014 EULAR

4.Determine the size of the vessel
affected:
*Palpable purpura ,superficial ulceration ,
mononeuritis multiplex & RBCs casts in urine
small vessel vasculitis
* Cutaneous nodules , livido reticularis ,
papulonecrotic lesions & digital infarction
medium vessel vasculitis
*Pulse deficit or bruit large vessel vasculitis
*Organ failure is not specific for any size e.g AKI
(RPGN or acute renal infarction)

Clinical finding according to
vessel involvement

5.Determine the specific type of
vasculitis within the vessel size group:
e.g. GPA &MPA are pauci-immune.
(IgAv) HSP is characterized by IgA-dominant
immune complex deposition.









GPA classically involves upper airways,
lungs and kidneys.
Cogan’s syndrome involves eyes, inner
ears and large arteries (in 10 -15 % of
cases)
IgAv typically affect skin, joints, kidneys and
gut.
ORGAN
TROPISMS

The epidemiologic features features of
individual forms of systemic vasculitis vary
by
Behcet’s disease more common in countries
bordering the ancient Silk road …
Takayasu’s arteries is the most common
cause of renal artery stenosis in India…
Geographic location

is an important
considerations in
epidemiology of vasculitis.
80% of patients with Kawasaki’s disease are younger than 5 years of age.
Giant cell arteries never occurs in patients younger than 50years old.
HSP (IgAv) in children have self-limited courses.
In adult HSP has a higher likelihood of chronicityand poor renal outcome
Age

Buerger’s disease is the only form of vasculitis
with striking male predominance.
TA has great tendency to occur in female (9-1).
Gender

Forms of vasculitis associated with
inflammation
Giant – cell arteritis.
Takayasu’s arteritis.
Cogan’s syndrome.
GPA.
Primary angiitis of CNS.
EGPA.
Granulomutous

Eosenophilic infiltrate
Leukocytoclastic angiitis…
with fragmented neutrophils
infltration of the wall of cutaneous
vessels differes from MPA …
It does not involve internal organs
ANCA -ve

FAST FACTS
Vasculitides affect multiple organ systems
and have highly variable presentations often
without classic findings.

FAST FACTS
Conventional angiography,
Computed Tomographic Angiography
(CTA) Magnitic Resonance
Angiography (MRA) are useful
diagnostic modalities.

•New imaging modalities such as colour
Doppler ultrasound and positron-emission
tomography are providing insights into the
extent and pathogenesis of large vessel
vasculitis.
•But have not yet replaced temporal artery
biopsy and angiography as the gold standards
for diagnosis
FAST FACTS

The mainstay of treatment for most of systemic
vasculitides is corticosteroids ,,, additional
Immunosuppressives may be necessary
in severe diseases.
FAST FACTS

• Details on AAV
• Pitfalls in ANCA testing
• Guidelines & updates in management
Is our next topic in shaa ALLah