Kevin Gallagher MRC/KRUK/GSK PhD fellow RIP 1 kinase ...
25
RIP 1 kinase inhibition for acute ischemic kidney injury Kevin Gallagher MRC/KRUK/GSK PhD fellow University of Edinburgh Supervisors: Ewen Harrison, Jeremy Hughes, Jim Ross, Lorna Marson, Stephen Wigmore, Allison Beal
Transcript of Kevin Gallagher MRC/KRUK/GSK PhD fellow RIP 1 kinase ...

RIP 1 kinase inhibition for acute ischemic kidney injury
Kevin Gallagher MRC/KRUK/GSK PhD fellow University of Edinburgh Supervisors: Ewen Harrison, Jeremy Hughes, Jim Ross, Lorna Marson, Stephen Wigmore, Allison Beal

DCD transplantation
40% get delayed graft
function
Increased rate of graft loss

Healthy Tubular necrosis
Fibrosis leading to
graft loss
92% of DCD grafts show evidence of ATN on day 10 protocol biopsies
Bank et al Nephrology Dialysis Transplantation, December 2017

How do cells die and can we stop them?
NECROSIS APOPTOSIS
PROGRAMMED NECROSIS?
Can we stop tubular cells from necrosing with a drug?
NECROPTOSIS
Programmed cell suicide:

Definition? Caspase independent cell death dependent on RIPK1
IRI
RIPK1 MLKL
Stimulus: Many
MLKL
Necrostatin-1
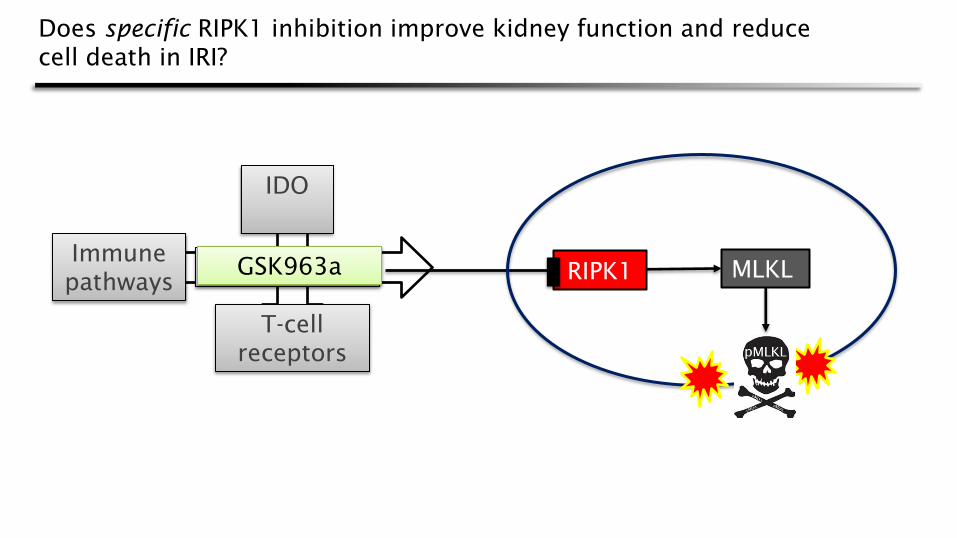
IDO
T-cell
receptors
Immune
pathways
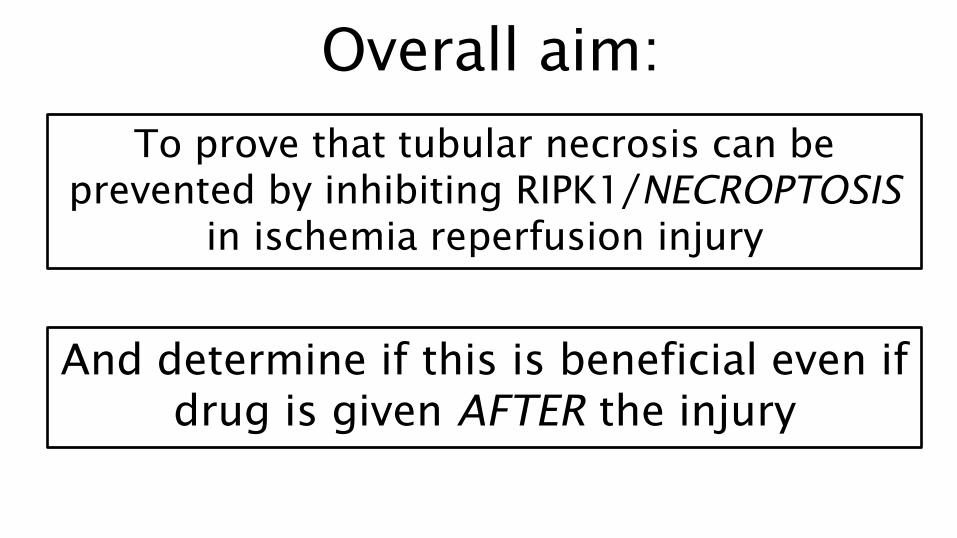
Overall aim:
To prove that tubular necrosis can be
prevented by inhibiting RIPK1/NECROPTOSIS
in ischemia reperfusion injury
And determine if this is beneficial even if
drug is given AFTER the injury
Left kidney Left renal
blood
vessels
Micro-
clamp
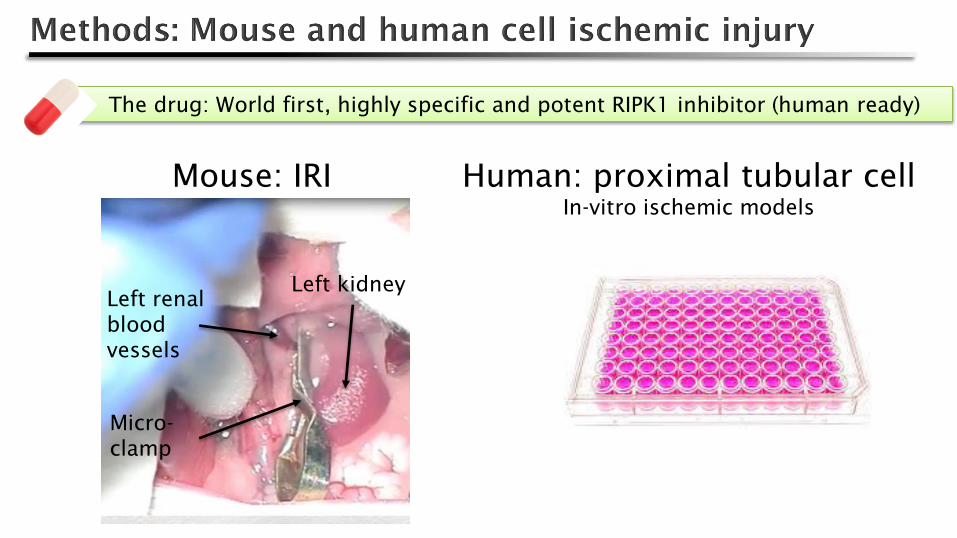
The drug: World first, highly specific and potent RIPK1 inhibitor (human ready)
Human: proximal tubular cell
In-vitro ischemic models
Mouse: IRI
RIPK1 Necrostatin-1
IDO
T-cell
receptors
Immune
pathways MLKL GSK963a
Does specific RIPK1 inhibition improve kidney function and reduce
cell death in IRI?

N=8 Mean and SD shown
Sh
am
Veh
icle
Co
mm
erc
ial R
IPK
1 in
hib
ito
r
Hig
hly
sp
ecif
ic R
IPK
1 in
hib
ito
r
0
2 5
5 0
7 5
1 0 0
1 2 5
1 5 0
1 7 5
2 0 0
Cre
ati
nin
e (
um
ol/
L)
p = 0 .0 0 6
Moderate IRI Severe IRI
Sh
am
Veh
icle
Co
mm
erc
ial R
IPK
1 in
hib
ito
r
Hig
hly
sp
ecif
ic R
IPK
1 in
hib
ito
r
0
2 5
5 0
7 5
1 0 0
1 2 5
1 5 0
1 7 5
2 0 0
Cre
ati
nin
e (
um
ol/
L)
p = 0 .0 1

VEHICLE RIPK1 inhibitor
x200
Moderate
injury
50-60%
CMJ
tubular
necrosis
Severe
injury 80-
90% CMJ
tubular
necrosis

Tubular necrosis scores:
Veh
icle
RIP
K1 in
hib
ito
r
0
1
2
3
4
Sc
ore
1 = 0 - 2 4 %
2 = 2 5 - 4 9 %
3 = 5 0 - 7 4 %
4 = > 7 5 %
p = 0 .0 1
Veh
icle
RIP
K1 in
hib
ito
r
0
1
2
3
4
Sc
ore
p = 0 .0 0 8
Median (25th
, 75th
) shown
Moderate IRI Severe IRI

RIPK1
MLKL
Stimulus:
Ischemia
reperfusion
?
Improves
renal
function
Reduces
necrosis

Green: Activated MLKL
(phosphorylated)
Red: Dead cells (TUNEL)
Healthy kidney (sham): No dead cells (red), no phosphorylated MLKL (green)
x100

Moderate
injury
Severe
injury
Vehicle RIPK1 inhibition
x100
Green: Activated MLKL
(phosphorylated)
Red: Dead cells (TUNEL)
Renal ischemic
injury is associated
with MLKL
phosphorylation

Activated MLKL is found on the apical boarder of IRI injured tubules:
Green: Activated
MLKL
(phosphorylated)
Red: Brightfield
pseudocolour
Blue: DAPI (nuclei)
X400 magnification

Moderate IRI
pMLKL quantification TUNEL positive cells
Moderate IRI Severe IRI N=6
Sh
am
Veh
icle
RIP
K1 in
hib
ito
r
0
2
4
6
8
1 0
1 2
1 4
1 6
1 8
2 0
To
tal
pM
LK
L s
tain
ing
pe
r l
ow
po
we
r f
ield
(ra
win
tde
n i
n m
illi
on
s)
p = 0 .0 0 4
Sh
am
Veh
icle
RIP
K1 in
hib
itio
r
Veh
icle
RIP
K1 in
hib
ito
r
0
5 0
1 0 0
1 5 0
2 0 0
2 5 0
3 0 0
3 5 0
4 0 0
4 5 0
Nu
mb
er o
f T
UN
EL
po
sit
ive
nu
cle
i p
er l
ow
po
we
r f
ield
p = 0 .0 3
p = 0 .0 3

T=0 T=24
pMLKL
RIP inhibitor

N=8
P=0.03 P=0.01
Creatinine 48 hours after injury Urea 48 hours after injury
Drug first given after 4 hours of reperfusion
IRI+
Veh
icle
IRI+
RIP
K1 in
hib
itio
n
0
5 0
1 0 0
1 5 0
2 0 0
2 5 0
Se
ru
m c
re
ati
nin
e (
um
ol/
L)
IRI+
Veh
icle
IRI+
RIP
K1 in
hib
itio
n
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
Se
ru
m u
re
a (
mm
ol/
L)
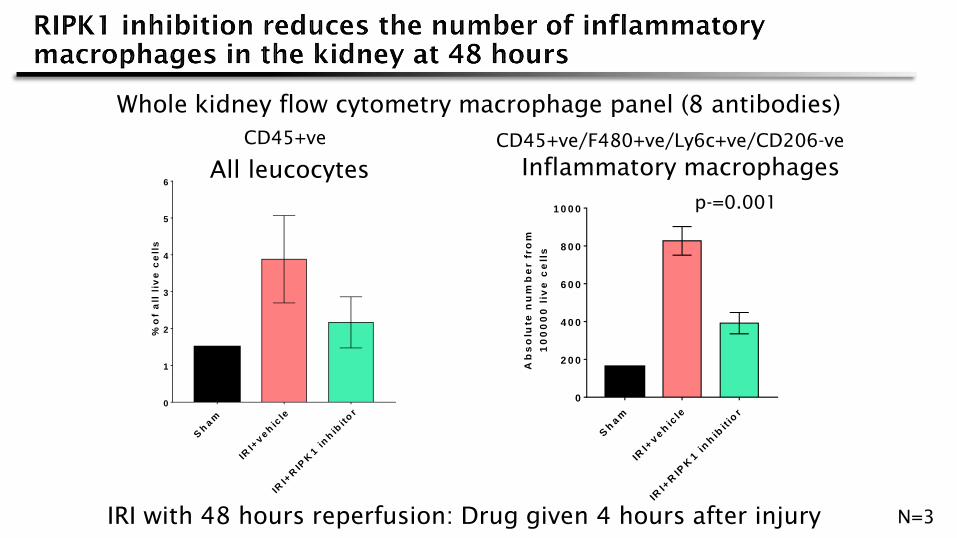
IRI with 48 hours reperfusion: Drug given 4 hours after injury
Whole kidney flow cytometry macrophage panel (8 antibodies)
N=3
Sh
am
IRI+
veh
icle
IRI+
RIP
K1 in
hib
itio
r
0
2 0 0
4 0 0
6 0 0
8 0 0
1 0 0 0
Ab
so
lute
nu
mb
er f
ro
m
10
00
00
liv
e c
ell
s
Inflammatory macrophages
p-=0.001
CD45+ve/F480+ve/Ly6c+ve/CD206-ve
Sh
am
IRI+
veh
icle
IRI+
RIP
K1 in
hib
ito
r0
1
2
3
4
5
6
%o
f a
ll l
ive
ce
lls
All leucocytes
CD45+ve
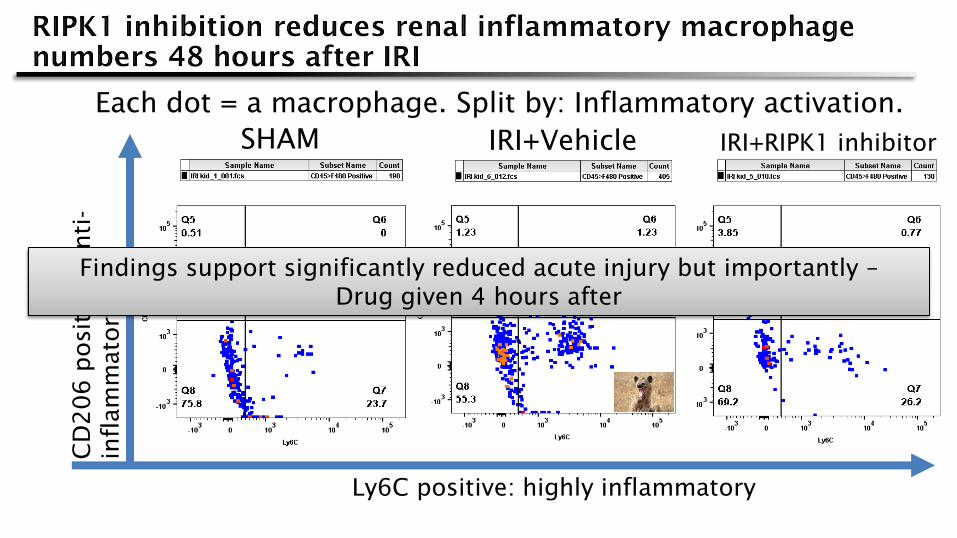
SHAM IRI+Vehicle IRI+RIPK1 inhibitor
Ly6C positive: highly inflammatory
CD
206 positive: A
nti-
inflam
matory
Each dot = a macrophage. Split by: Inflammatory activation.
Findings support significantly reduced acute injury but importantly –
Drug given 4 hours after
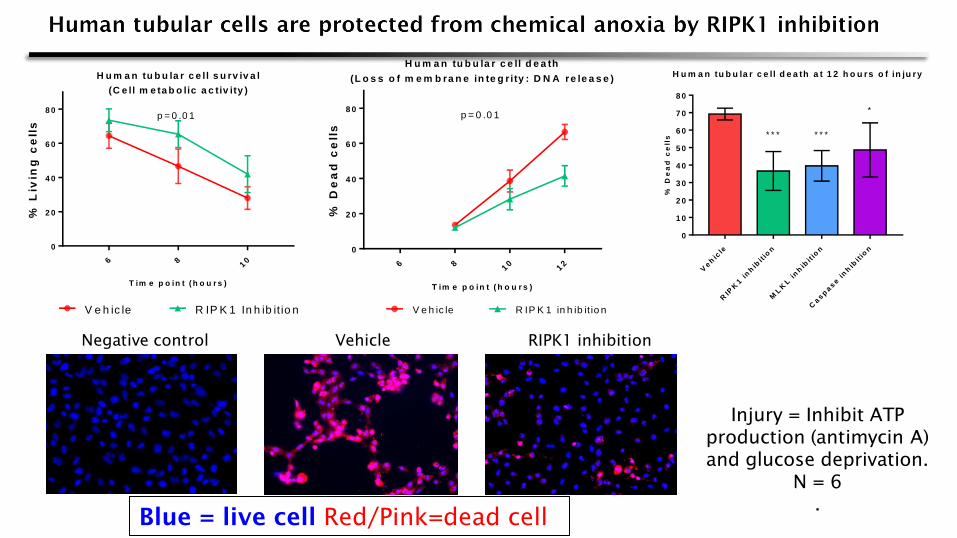
Negative control Vehicle RIPK1 inhibition
Injury = Inhibit ATP
production (antimycin A)
and glucose deprivation.
N = 6
.
Blue = live cell Red/Pink=dead cell
Veh
icle
RIP
K1 in
hib
itio
n
ML
KL
in
hib
itio
n
Casp
ase in
hib
itio
n
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
H u m a n tu b u la r c e ll d e a th a t 1 2 h o u rs o f in ju ry
% D
ea
d c
ell
s * * * * * *
*
6 810
12
0
2 0
4 0
6 0
8 0
H u m a n tu b u la r c e ll d e a th
(L o s s o f m e m b ra n e in te g r ity : D N A re le a s e )
T im e p o in t ( h o u r s )
% D
ea
d c
ell
s
p = 0 .0 1
V e h ic le R IP K 1 in h ib it io n
6 810
0
2 0
4 0
6 0
8 0
H u m a n tu b u la r c e ll s u rv iv a l
(C e ll m e ta b o lic a c tiv ity )
T im e p o in t ( h o u r s )
% L
ivin
g c
ell
s
V e h ic le R IP K 1 In h ib it io n
p = 0 .0 1

1. Is beneficial in
mouse IRI even when
given AFTER injury
2. Reduces mouse
tubular cell death by
necroptosis
3. Reduces HUMAN ischemic tubular cell
death by necroptosis in-vitro
?
The first evidence
that specific RIPK1
inhibition is
beneficial in IRI
The first evidence
that necroptosis
occurs in IRI and that
RIPK1 inhibition
reduces this
Early evidence
That this process may
be relevant in human
kidney cells

• MRC, KRUK and GSK
• My supervisors
• Jim Black, Kathryn Sangster, Jyoti
Nanda, Anwar Palakka , Gary
Borthwick, Laura Denby, Carolynn
Cairns