Ketamine in The ED - VACEPvacep.org/wp-content/uploads/2017/02/Ketamine-in-The-ED-1.pdf · KETAMINE...
46
Paul Stromberg, MD Carilion Clinic VACEP February 11, 2017 KETAMINE IN THE ED
Transcript of Ketamine in The ED - VACEPvacep.org/wp-content/uploads/2017/02/Ketamine-in-The-ED-1.pdf · KETAMINE...
Paul Stromberg, MD
Carilion Clinic
VACEP
February 11, 2017
KETAMINE IN THE ED

FINANCIAL DISCLOSURES
• NONE

OUTLINE
• History and background
• Pharmacology/Mechanism of action
• Excited delirium
• Analgesia
• Depression
• Wrap-up

• PCP: Park Davis 1956
• 1961 Ketamine
synthesized
• 1/10th the potency
• 1964: First anesthetic
use in humans
• Ketalar approval 1970
KETAMINE

PHARMACOLOGY
• Arylcycloalkamine
• Racemic mixture of R and S isomers
• S (+) ketamine: higher anesthetic potency, decreased
emergence reactions
• R (-) ketamine: more potent antidepressant effects
• CYP 3A4: norketamine (30% the activity)
• Highly fat soluble

Li and Vlisides 2016

Gao et al, 2016

EXCITED DELIRIUM
• Altered mental status
• Often aggressive, “superhuman”
• Hyperthermia, tachycardia, hypertensive
• Danger to self and others
• High mortality, especially when forcibly restrained
• Numerous case reports of Ketamine for transporting
agitated patients



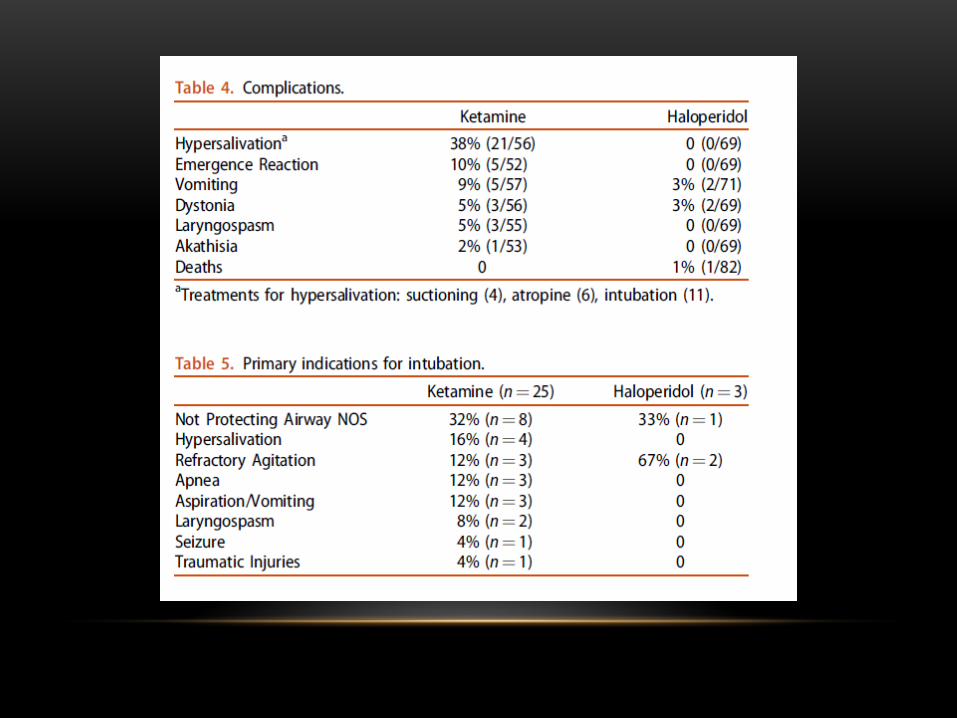
PREHOSPITAL IM KETAMINE
• Jan 2011 – May 2014
• 52 patients, effective in 50 patients
• Time to effective sedation and control approximately 2 mins
• Half the patients got midazolam per protocol
• Three cases of respiratory depression, 2 intubations (all got midazolam)


PREHOSPITAL AND RETRIEVAL
• Retrospective chart review 2013
• 163 encounters, 160 patients (2 repeat patients)
• 153 encounters analyzed in study
• 68% for analgesia, 25% for agitation
• 17% required intubation (most in ED after arrival)
• Mix of IV and IM (nearly 80% for agitation IM)





KETAMINE FOR ANALGESIA
• Prehospital
• In the ED
• Orthopedic injuries, all pain, migraines
• IM, IV, continuous infusions, IN






KETAMINE AND OPIOID SPARING
EFFECTS
• Primary mechanism of action is NMDA
antagonism
• Also binds to spinal mu and delta opioid
receptors
• May block opioid hyperalgesia



LOW DOSE KETAMINE
• Primary outcome: pain relief
• Followed for 2 hours post-ketamine (30, 60, 120)
• Secondary outcome: pain relief at each scoring
• Adverse effects collected
• Greater pain relief in ketamine groups, more sustained at higher dose, dizziness frequent complaint (50%)

Ahern, et al. 2015

KETAMINE INFUSION FOR SEVERE PAIN
• Prospective open-label study June 2013-Feb 2014
• 38 patients
• 15 mg bolus of ketamine, 20 mg/h infusion for 1h
• Offered additional analgesia at 20, 40, 60 min
• Pain assessed every 5-15 min for 120 min
• Primary outcome: change in pain
• Secondary outcomes: adverse effects, acceptability to patients
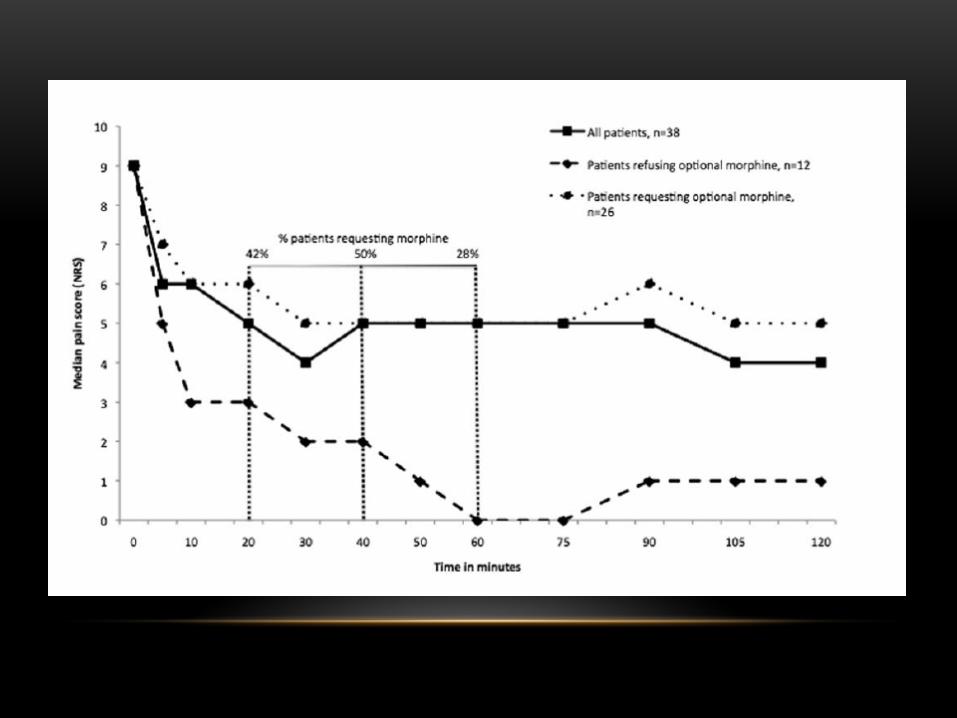

KETAMINE INFUSION
• Minimal sedation noted, no hypoxia
• Transient hypertension and tachycardia
• 85% would use ketamine for pain again


IN KETAMINE
• 1.0 mg/kg IN ketamine; 0.1 mg/kg IV morphine;
0.15 mg/kg IM morphine
• Pain and VS assess every 5 min for 1 hour
• Primary outcome: pain reduction of 15 mm on
VAS
• Adverse effect information collected

IN KETAMINE FOR PAIN RELIEF
• No difference in maximal pain relief or time to
maximal pain relief between groups
• Higher proportion of dizziness and difficulty
concentrating in ketamine group
• No difference in patient satisfaction between
groups

KETAMINE FOR DEPRESSION
• Emerging evidence for effectiveness in
management of severe depression
• Impact on suicidal ideation
• Glucose metabolism alteration in mood centers
• May be related to ketamine’s ability to alter
glutamate in the brain

Han, et al. 2016

KETAMINE FOR DEPRESSION
• Meta-analysis of 9 RCTs
• 368 total patients, 0.5 mg/kg IV ketamine
• Primary end-point of 50% reduction of symptoms
• Screened at 24 hrs, 72 hrs, and 7 days post-infusion
• Significantly more responders at all time points in the ketamine groups compared to placebo

IN KETAMINE, NOT JUST FOR PAIN

IN KETAMINE FOR DEPRESSION
• 18 patient cross-over study
• April 2012-June 2013
• 21-65, failed at least 1 anti-depressant in current episode
• 50 mg of IN ketamine or IN saline, switched 1 week later
• Primary outcome 50% reduction in depression symptoms

IN KETAMINE FOR DEPRESSION
• Significant difference in depressive symptoms as
early as 4 hours post insufflation
• 44% of patients met primary endpoint at 24
hours
• No significant difference at 3 days or 7 days
• No significant difference in adverse effects
compared to placebo


CONCLUSIONS
• Ketamine provides rapid sedation of agitated
patients
• Ketamine control associated with higher rate of
intubation
• May be useful adjunct in pain control
armamentarium
• Stay tuned for role in acute treatment of depression

THANK YOU
REFERENCES• GJ Hollis, et al. Emergency Medicine Australasia (2017) 29, 89-95
• JB Cole, et al. Clinical Toxicology, 2016. Vol. 54, No. 7, 556-562.
• Lovisk, et al. Scandinavian Journal of Trauma, Resuscitation, and Emergency Medicine (2015). 23:94.
• LN Petz, et al. Military Medicine, 180, 3:14, 2015.
• E Wiel, et al. Prehospital Emergency Care. January/March 2015. Volume 19/Number 1
• Lee EN, Lee JH. (2016). PLoS ONE 11(10).
• TL Ahern, et al. Pain Medicine 2015; 16: 1402-1409.
• FL Beaudoin, et al. Academic Emergency Medicine 2014. Vol. 21, No. 11.
• Lauristen, et al. The Journal of Headache and Pain (2016) 17:106.
• L Li, PE Vlisides. Frontiers in Human Neuroscience. November 2016. Vol. 10. Article 612.
• Han, et al. Neuropsychiatric Disease and Treatment 2016:12 2859-2867.
• Shimonovich, et al. BMC Emergency Medicine (2016) 16:43.
• Lapidus, et al. Biol Psychiatry. 2014 December 15; 76(12): 970-976.
• Gao, et al. Acta Pharmacologia Sinica (2016) 37: 865-872.
• D. Reicher. Air Medical Journal 35 (2016) 84-85.
• KA Scheppke, et al. Western Journal of Emergency Medicine. Volume XV, No 7: November, 2014.
• Ch Schultz. West J Emerg Med. 2104; 15(7): 742-743.