KETAMINE: AN OPTION FOR YOUR PAIN … Conference Documents... · 1 KETAMINE: AN OPTION FOR YOUR...
19
1 KETAMINE: AN OPTION FOR YOUR PAIN MANAGEMENT TOOLBOX Cindy Klaess, MSN, RN, ACNS-BC, CCM CONFLICT OF INTEREST DISCLOSURE No conflicts of interest OBJECTIVES Describe mechanism of action and side effects of Ketamine. Discuss the use of Ketamine in multi-modal strategies of pain management. Apply knowledge of Ketamine’s mechanism of action and benefits to case scenarios
Transcript of KETAMINE: AN OPTION FOR YOUR PAIN … Conference Documents... · 1 KETAMINE: AN OPTION FOR YOUR...

1
KETAMINE: AN OPTION FOR YOURPAIN MANAGEMENT TOOLBOXCindy Klaess, MSN, RN, ACNS-BC, CCM
CONFLICT OF INTEREST DISCLOSURE
No conflicts of interest
OBJECTIVES
Describe mechanism of action and side effects of
Ketamine.
Discuss the use of Ketamine in multi-modal strategies
of pain management.
Apply knowledge of Ketamine’s mechanism of action
and benefits to case scenarios
2
Duke University Hospital
KETAMINEMechanism of ActionSide EffectsPatient Selection
3
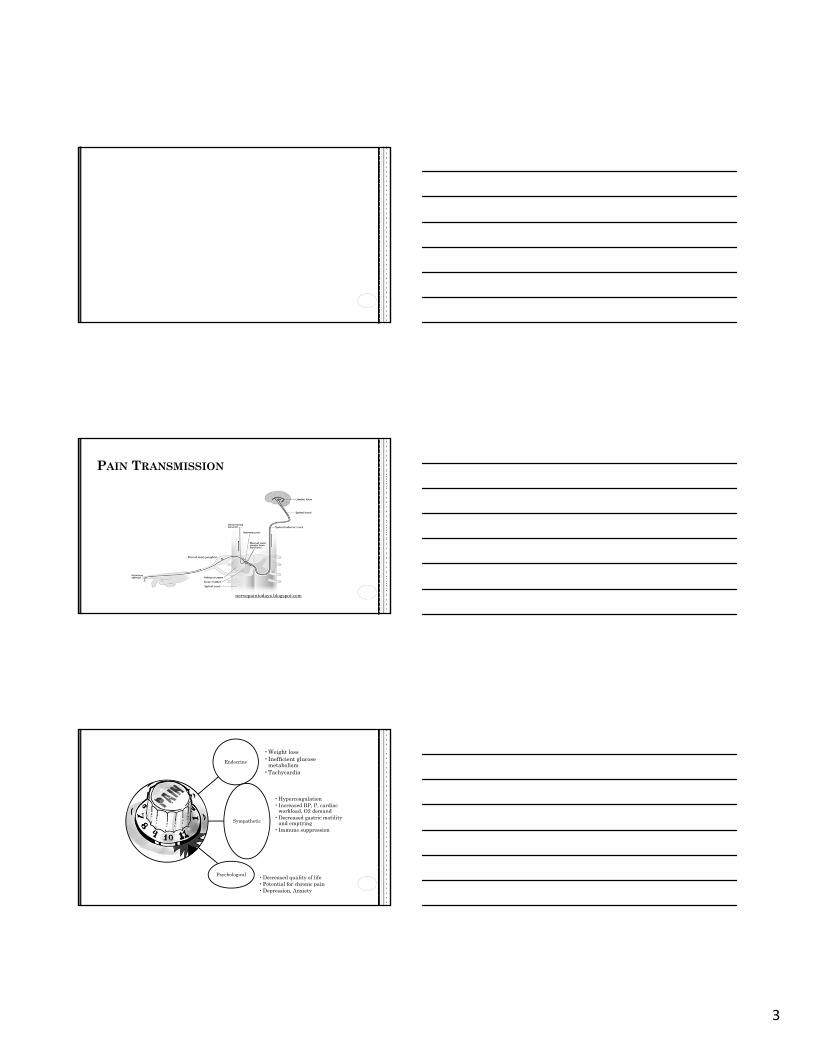
PAIN TRANSMISSION
nervepaintodays.blogspot.com
Endocrine
•Weight loss•Inefficient glucose
metabolism•Tachycardia
Sympathetic
•Hypercoagulation•Increased BP, P, cardiac
workload, O2 demand•Decreased gastric motility
and emptying•Immune suppression
Psychological •Decreased quality of life•Potential for chronic pain•Depression, Anxiety
4
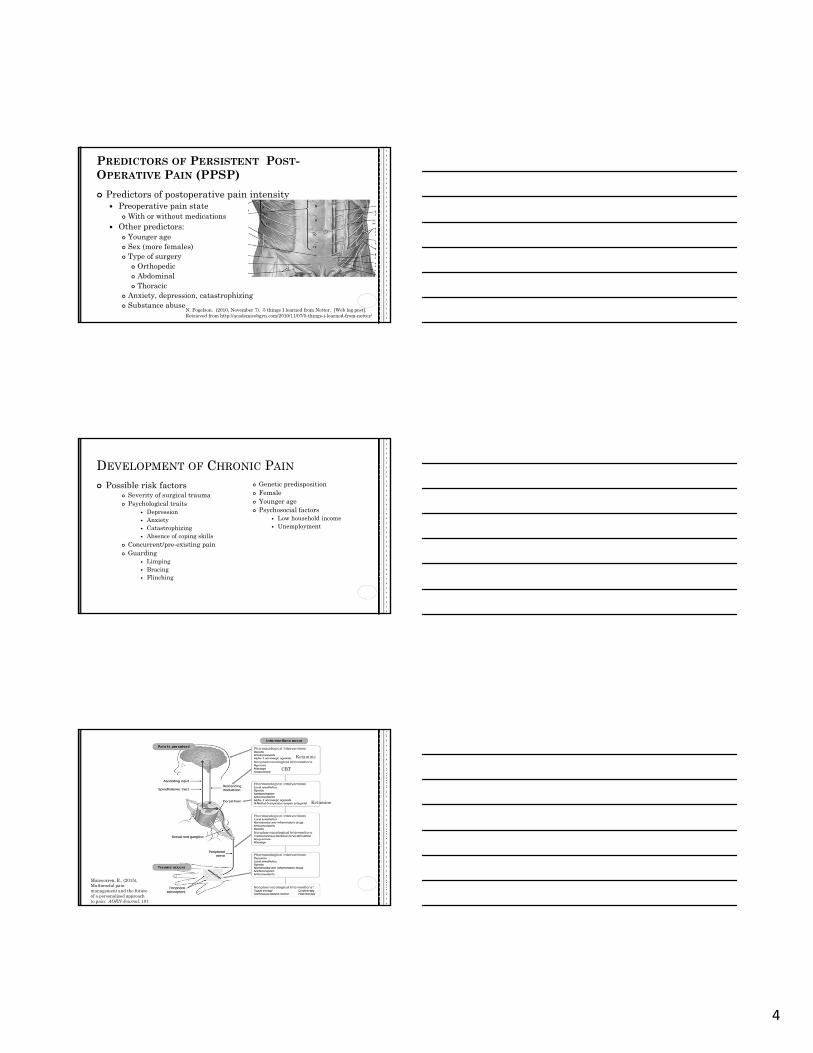
PREDICTORS OF PERSISTENT POST-OPERATIVE PAIN (PPSP)
Predictors of postoperative pain intensity Preoperative pain state
With or without medications Other predictors:
Younger age Sex (more females) Type of surgery
Orthopedic Abdominal Thoracic
Anxiety, depression, catastrophizing Substance abuse
N. Fogelson. (2010, November 7). 5 things I learned from Netter. [Web log post].Retrieved from http://academicobgyn.com/2010/11/07/5-things-i-learned-from-netter/
DEVELOPMENT OF CHRONIC PAIN
Possible risk factors Severity of surgical trauma Psychological traits
Depression Anxiety Catastrophizing Absence of coping skills
Concurrent/pre-existing pain Guarding
Limping Bracing Flinching
Genetic predisposition Female Younger age Psychosocial factors
Low household income Unemployment
Manworren, R., (2015), Multimodal pain management and the future of a personalized approach to pain. AORN Journal, 101 (3) 307 318
Ketamine
CBT
Ketamine
5
NON-PHARMACOLOGIC
Heat Cold Repositioning Distraction
Music
Meditation Massage Touch Therapy Active Listening
TENS Referral to
interdisciplinary services: Chaplain, Social worker, Stress management, Psychiatry Cognitive Behavioral
Therapy (CBT)
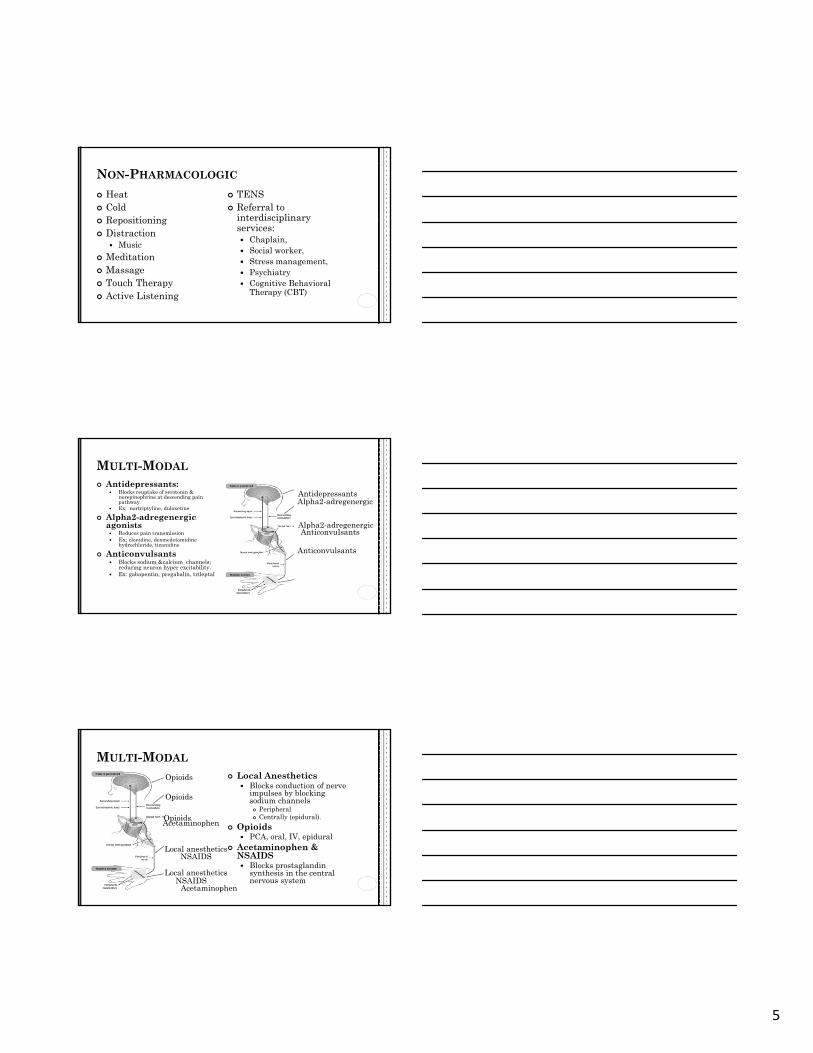
MULTI-MODAL
Antidepressants: Blocks reuptake of serotonin &
norepinephrine at descending pain pathway.
Ex: nortriptyline, duloxetine
Alpha2-adregenergic agonists Reduces pain transmission Ex: clonidine, dexmedetomidine
hydrochloride, tizanidine
Anticonvulsants Blocks sodium &calcium channels;
reducing neuron hyper excitability. Ex: gabapentin, pregabalin, trileptal
Antidepressants
Alpha2-adregenergic
Anticonvulsants
Alpha2-adregenergic
Anticonvulsants
MULTI-MODAL
Local Anesthetics Blocks conduction of nerve
impulses by blocking sodium channels Peripheral Centrally (epidural).
Opioids PCA, oral, IV, epidural
Acetaminophen & NSAIDS Blocks prostaglandin
synthesis in the central nervous system
Local anesthetics
Local anesthetics
Opioids
Opioids
Opioids
NSAIDS
NSAIDS
Acetaminophen
Acetaminophen
6
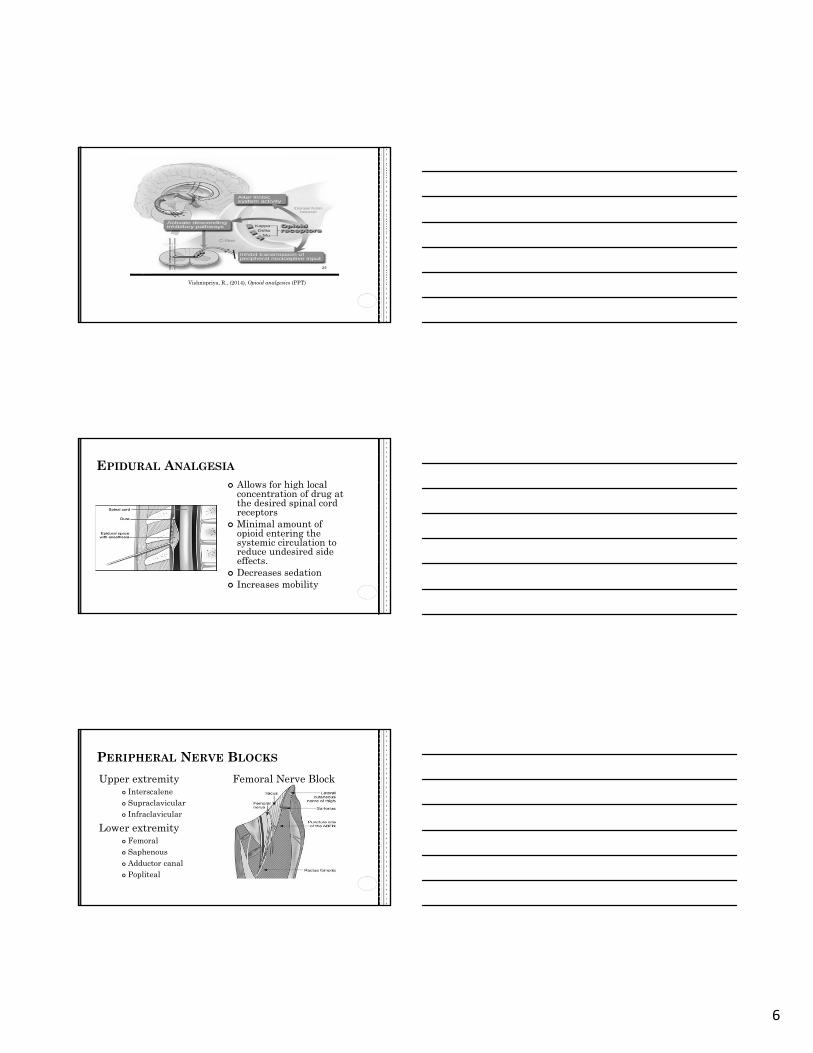
Vishnupriya, R., (2014), Opioid analgesics (PPT)
EPIDURAL ANALGESIA
Allows for high local concentration of drug at the desired spinal cord receptors
Minimal amount of opioid entering the systemic circulation to reduce undesired side effects.
Decreases sedation Increases mobility
PERIPHERAL NERVE BLOCKS
Upper extremity Interscalene Supraclavicular Infraclavicular
Lower extremity Femoral Saphenous Adductor canal Popliteal
Femoral Nerve Block
7
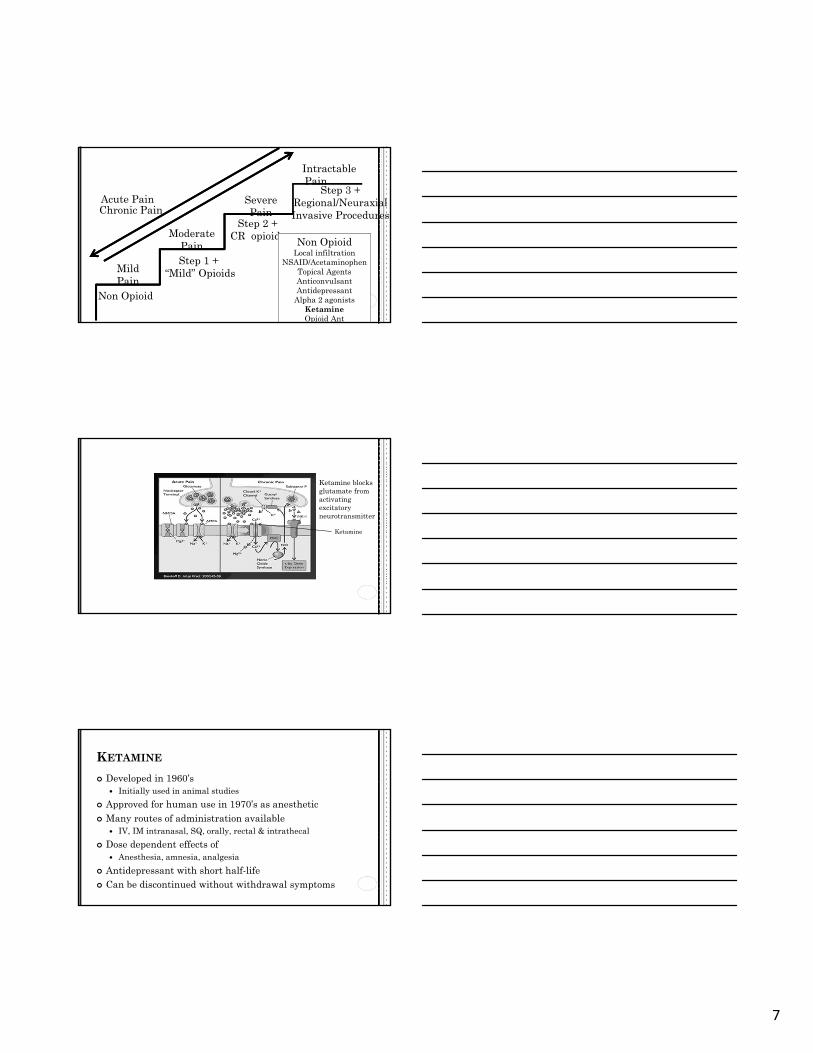
Mild Pain
Severe Pain
ModeratePain
Non Opioid
Step 1 + “Mild” Opioids
Step 2 +CR opioids Non Opioid
Local infiltrationNSAID/Acetaminophen
Topical AgentsAnticonvulsantAntidepressant
Alpha 2 agonistsKetamineOpioid Ant
Step 3 +Regional/NeuraxialInvasive ProceduresChronic Pain
Acute Pain
IntractablePain
Ketamine blocks glutamate from activating excitatory neurotransmitter
Ketamine
KETAMINE
Developed in 1960’s Initially used in animal studies
Approved for human use in 1970’s as anesthetic Many routes of administration available
IV, IM intranasal, SQ, orally, rectal & intrathecal
Dose dependent effects of Anesthesia, amnesia, analgesia
Antidepressant with short half-life Can be discontinued without withdrawal symptoms
8
PHARMACOKINETICS
Metabolized in liver Highly lipid soluble
Crosses blood brain barrier rapidly Binds to NMDA receptor
Inhibits glutamate from activating the NMDA Creates dissociative effect between the thalamus & limbic regions of the
brain Rapid onset
IV effects in 30 seconds with full effect in 1 minute Duration of 60 minutes Elimination half-life 2-3 hours
Immediate effects Analgesia, sedation, pupil dilation, nystagmus, lacrimation, salivation,
antidepressant, and increased muscle tone
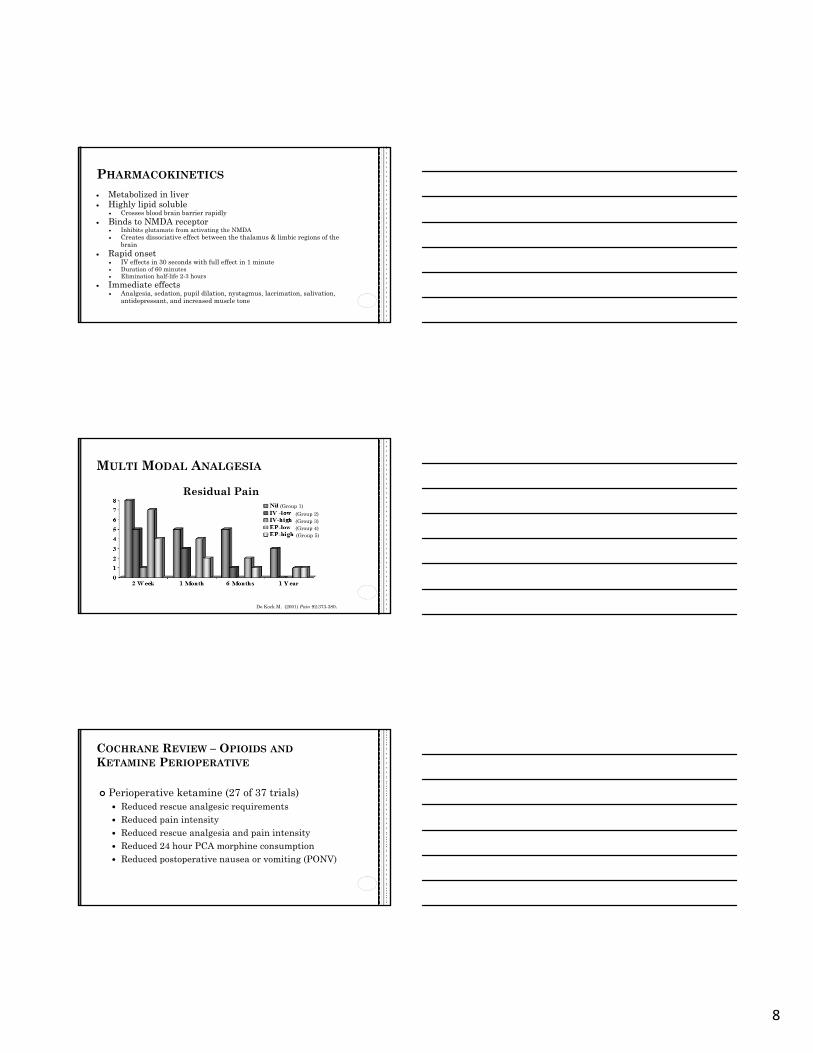
MULTI MODAL ANALGESIA
De Kock M. (2001) Pain 92:373-380.
Residual Pain(Group 1)
(Group 2)(Group 3)(Group 4)(Group 5)
COCHRANE REVIEW – OPIOIDS ANDKETAMINE PERIOPERATIVE
Perioperative ketamine (27 of 37 trials) Reduced rescue analgesic requirements Reduced pain intensity Reduced rescue analgesia and pain intensity Reduced 24 hour PCA morphine consumption Reduced postoperative nausea or vomiting (PONV)

9
POST OPERATIVE ANALGESIA
Randomized, double blind (n=1088)Evaluated effect of Ketamine & Morphine on
pain intensity Study criteria
VAS > 6/10 (> 100 mcg/kg morphine in 30 mins)
2 Groups ( < 3 doses aim of VAS <4/10) Morphine 30 mcg/kg + saline Morphine 15 mcg/kg + ketamine 250 mcg/kg
Weinbroum , AA. (2003) Anesthesia Analg.96(3):789-95.
POST OPERATIVE ANALGESIA
Pa
in
Lev
els
Time in MinutesWeinbroum, AA (2003).Anesthesia Analg.9 6(3):789-95.
POST OPERATIVE ANALGESIA
PACU Side Effects
Weinbroum, A.A. (2003).Anesthesia Analg.96(3):789-95:
10
KETAMINE: REDUCED ANALGESICCONSUMPTION
Total Hip Arthroplasty ( n= 154) IV ketamine before incision (0.5 mg/kg), and a 24-h
infusion (2 mcg /kg/ min) Placebo
Postoperative for 48 hours IV acetaminophen Ketoprofen PCA morphine/droperidol
Reduced total morphine consumption up to 7 days post-op
Remerand F. (2009), Anesthesia Analg;109:1963–71.
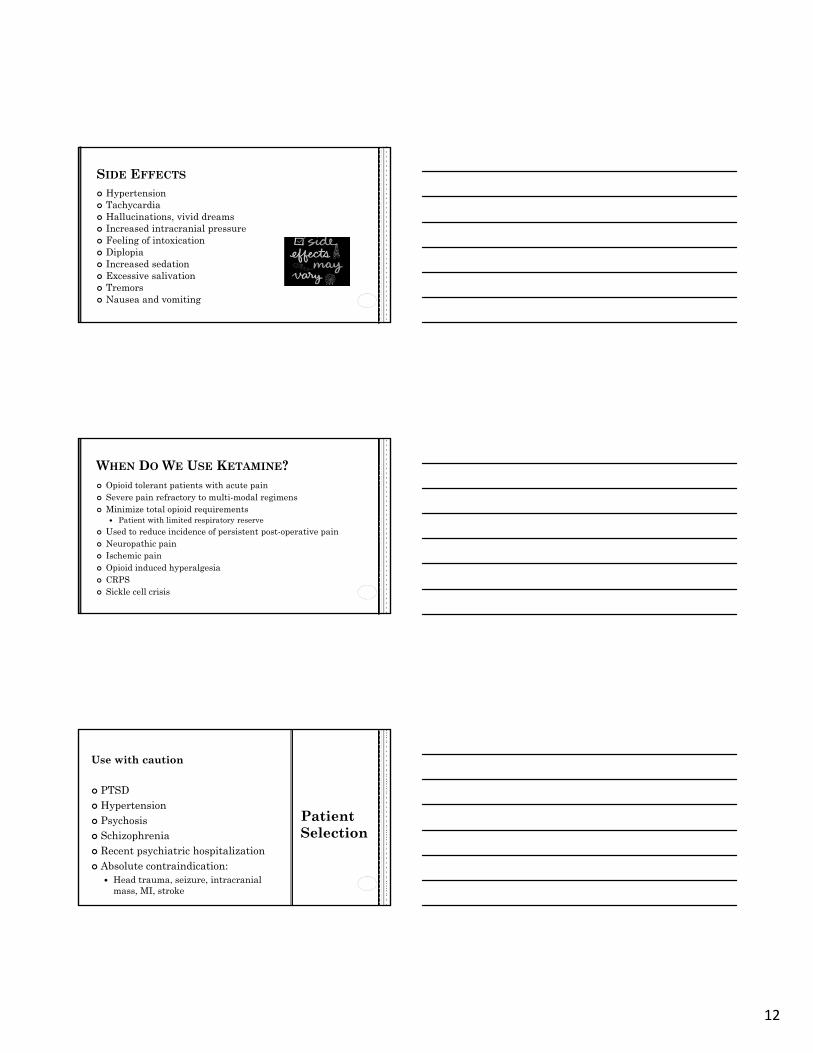
0
5
10
15
20
25
30
35
Day 30 Day 90 Day 180
Placebo
Pain at rest
Pe
rce
nta
ge
Remerand F. , (2009), Anesth Analg;109:1963–71.
24-H IV INFUSION OF KETAMINE DECREASES REST PAIN BY 67% AT 6 MONTHS
Ketamine: Reduced Long Term Pain Scores
KETAMINE
As a singular agent→ analgesia With other agents
Synergistic Dose sparing
Minimal effect on respiratory drive Bronchodilator effects
Uses Anesthesia induction Sedation maintenance Pre-hospital stabilization & transportation Acute & chronic pain Procedural sedation

11
CARDIOVASCULAR EFFECTS
Sympathomimetic effect Brain stem stimulation with catecholamine release Blocks reuptake of catecholamines Heart rate, cardiac output, blood pressure
Direct depression of myocardium Increase coronary blood flow Heart rhythm
Direct anti arrhythmic Indirect arrhythmogenic – catecholamines
Acts on cholinergic, muscarinic and adenosine receptors
CENTRAL NERVOUS SYSTEM SIDE EFFECTS
Auditory and visual hallucinations
Paranoid ideas Anxious feelings (panic attacks) Inability to control thoughts
(internal perception) Change in concept of time &
space Increased awareness of sound
and color (external perception)
Intense sense of drug high or euphoria
Nightmares or vivid dreams, Dizziness, Blurred vision, Vertigo, Nausea/vomiting, Dysphasia, Nystagmus, Impaired motor function Memory deficits
CNS SIDE EFFECTS
Psychedelic effects Decrease rapidly after termination of ketamine
administration Unpleasant dreams
Significantly increased compared with placebo for 3 nights
Effects can be managed Benzodiazepines Alpha 2-adrenergic
receptor agonists
12
SIDE EFFECTS
Hypertension Tachycardia Hallucinations, vivid dreams Increased intracranial pressure Feeling of intoxication Diplopia Increased sedation Excessive salivation Tremors Nausea and vomiting
WHEN DO WE USE KETAMINE? Opioid tolerant patients with acute pain Severe pain refractory to multi-modal regimens Minimize total opioid requirements
Patient with limited respiratory reserve
Used to reduce incidence of persistent post-operative pain Neuropathic pain Ischemic pain Opioid induced hyperalgesia CRPS Sickle cell crisis
Patient Selection
Use with caution
PTSD Hypertension Psychosis Schizophrenia Recent psychiatric hospitalization Absolute contraindication:
Head trauma, seizure, intracranial mass, MI, stroke

13
Start low: 0.15-0.25 mcg/kg/hr Monitoring:
Within 60 minutes of initiation Every 2 hours x 24 hours then q 4
hours. For an increase in dose, monitor q2 hours x 24 hours
Opioid requirements will decrease once Ketamine initiated Decrease opioid by 25-50%
Consider low dose benzodiazepine for agitation
MONITORING
MONITORING Assessment:
Respiratory rate Oxygenation saturation, Level of pain and Sedation (using RASS)
Notify Medical team and ordering MD if any of the following occur: RASS ≤-2 or ≥ 2. Psychological side effects i.e.
hallucinations, vivid dreams, aggressive behavior.
Sustained hypertension (>20% increase in blood pressure).
Increased pain level or unrelievedpain
DISCONTINUING KETAMINE
Limit infusion to 48-72 hours if possible Risk of hemorrhagic cystitis
Maximize multi-modal Avoid discontinuation of all IV pain management
at the same time Have a plan for transition to orals
14
CA
SE
ST
UD
Y#1
Patient not meeting patient selection criteria
62 yo male admitted following traumatic BKA of right lower extremity History of diabetes, prior right
transmetatarsal amputation, prior lumbar surgery
Preoperative medications: Gabapentin 300mg every 8 hours Morphine Sulfate (MS Contin) 30 mg
every 8 hours Oxycodone 5-10 mg every 4 hours PRN Sertraline 75 mg every morning.
Patient reports history of PTSD
TAKEAWAYS FOR YOUR TOOLBOX
Opioid requirements will decrease once Ketamine initiated Decrease opioid dose by
25-50% Consider low dose benzo
for agitation Maximize multi-
modal Start low (0.15-0.25
mcg/kg/hr)
INSTITUTIONAL INITIATIVESAdult Roll OutKetamine Lock BoxesPediatric Ketamine Order Sets
15
Acute Pain Service
Interdisciplinary team Attending anesthesiologist 3 Clinical Nurse Specialists 2 Nurse Clinicians 2 Nurse Practitioners Anesthesia residents Pain fellow
Provide 24/7 coverage for epidural & peripheral nerve catheter patients
Consult service Complex pain patients Ketamine & Lidocaine infusions Intrathecal
KETAMINE USE
Data available from 2008 ~ 70 patients first year
Average 4-5 patients daily on Ketamine. Daily peak: 12 patients
2015: over 350 patients projected
INSTITUTIONAL INITIATIVES
Roll out to all adult acute care areas
Revision of policies
Education for nursing staff
In-services
Just-In-Time Training
On-line training modules
Ketamine order sets
Consultation with Pain Service attending required
Bundles orders with monitoring and reporting criteria

16
PEDIATRIC ROLLOUT
Previously only in ICU
Pediatric Roll Out Stepdown, high acuity
& ICU
Number of pediatric cases since April 2015 4
Revision of ketamine policy
Nursing education Ketamine order set
Orders based on age Convert to pediatric
dosing (mcg/kg/min)
KETAMINE ABUSE
Dissociative & hallucinogenic effects Recreational drug of abuse Street names
Special K Vitamin K Lady K
K-Hole Ketamine dissociative state

17
CASE STUDIESPediatricOpioid TolerantGeriatricAddiction History
CA
SE
ST
UD
Y# 2
Pediatric Case Study
10 yo female admitted with abdominal tumors Lengthy hospitalization On hydromorphone PCA Opioid requirements increasing
Management Possibilities:
CA
SE
ST
UD
Y# 3
Geriatric Case Study
72 yo male admitted following spinal fusion; C2-T6. Chronic left upper extremity shoulder
& arm pain Home medications:
Hydromorphone (Dilaudid )2-4 mg every 4 PRN
Oxycodone (OxyContin®) 60 mg every 12 hours
Clonazepam 0.5 mg twice daily PRN Pregabalin 100mg twice daily
Management Possibilities:
18
CA
SE
ST
UD
Y# 4
Sickle Cell Disease:
Acute on Chronic
32 yo female History of sickle cell disease Avascular necrosis of hips Admitted following total hip
arthroplasty
Management Possibilities:
CA
SE
ST
UD
Y# 5
Opioid Tolerant
30 yo male with metastatic cancer Requiring thoracotomy Home medications:
Morphine Sulfate (MS Contin) 60 mg every 12 hours
10/10 post-operative pain
Management Possibilities:
CA
SE
ST
UD
Y# 6
Substance AbuseHistory
35 yo female MVC
Traumatic amputation of left lower extremitybelow the knee
Drug screen positive Cocaine, opiates, THC
Management Possibilities:

19
REFERENCES American society for pain management nursing guidelines on monitoring for opioid-induced sedation and respiratory
depression, (2011). Pain management nursing, 12 (3) 118-145.
Anesthesiology, 2012. Second Edition. Ed. Brown, D., Newman, M., & Zapol, W.. McGraw Hill.
Bell, R.F., Dahl, J.B., & Kalso, E., (2006), Perioperative ketamine for acute post operative pain. Cochrane database review, Jan 25;(1):CD004603.
Brookoff, D., (2000), Chronic pain: 1. a new disease? Hospital Practice, 35(7); page 45-59. Posted: 2003-11-16; Modified: 2007-05-10.
Chen, L., & Malek, T., (2015), Follow me down the k-hole; ketamine and its modern application. Critical care nursing quarterly, 38 (2) 211-216.
Constantini, R., Affaitati, A., & Giamberadino, M.A., (2011), Controlling pain in the post-operative setting. International journal of clinical pharmacology and therapeutics, 49 (2) 116-27.
De Kock, M., Lavand’homme, P., & Waterloos, H., (2001), Balanced analgesia in the perioperative period: is there a place forketamine?. Pain, 92 (3) 373-80.
Mazzeffi M, Johnson K, Paciullo C., (2015) Ketamine in adult cardiac surgery and the cardiac surgery intensive care unit: an evidence-based clinical review. Ann card anaesthesia 18:202-9.
Manworren, R., (2015), Multimodal pain management and the future of a personalized approach to pain. AORN Journal, 101 (3) 307-318.
Pasero, C. & McCaffery, M., (2011). Pain assessment and pharmacologic management. Mosby-Elseiver. St. Louis, MO.
Weinbroum, A., (2003), A single dose of postoperative ketamine provides rapid and sustained improvement in morphine analgesia in the presence of morphine-resistant pain. Anesthesia analg, 96; 789-95.
Cindy Klaess, MSN, RN, ACNS-BC, [email protected]