Ketamine: After Fifty Year Reign – from Pre-op to...
42
Transcript of Ketamine: After Fifty Year Reign – from Pre-op to...
Objectives
1) Review the history of ketamine
2) Revisit the mechanism of action of ketamine
3) Discuss the pharmacokinetics,
pharmacodynamics, and adverse effects of
ketamine
4) Examine the pain pathway and role of NMDA
receptor in acute and chronic pain
5) Describe use of ketamine in various pain
syndromes

The History of Ketamine
1956
Phencyclidine discovered
1958
Park-Davis (MI) developing
phencyclidine surgical
anesthetic
1960s
Phencyclidine (Sernyl) for
human surgical anesthesia
1967
Phencyclidine (Sernylan) enters US veterinary medicine
market
1970
Ketamine (Ketalar) for human and animal use
Domino EF. Anesthesiology 2010;113:678-86. Olmedo RE. Chapter 85. Phencyclidine and Ketamine. Goldfrank's
Toxicologic Emergencies, 9e (2011).

Ketamine: Quick Facts
0 Rapid-acting general anesthetic
0 Commercial preparation of racemic mixture of
two enantiomers, S(+) ketamine and R(–)
ketamine.
0 S(+) ketamine has four times the affinity of R(–)
ketamine for the NMDA receptor
0 S(+) ketamine also binds to mu and kappa opioid
receptors.

Ketamine in Practice

Mechanism of Action
G
G G
AC
Decrease cAMP
Decrease neurotransmitter
release
Decrease intracellular Ca2+
Increase K+
efflux

Mechanism of Action
G
G G
AC
Decrease neurotransmitter release
Decrease intracellular Ca2+
Decrease Ca2+ entry

Ketamine Effects Central Nervous
System
Sympathetic
System
0 NMDA receptor
antagonism
0 Anesthesia
0 Sedation
0 Analgesia
0 Antidepressant
effects
0 Cholinergic
activation
0 Hemodynamic
changes
0 Bronchodilation
0 Sialorrhea

Ketamine Drug Properties
Pharmacology and Adverse Effects

Absorption and Distribution 0 Absorption
0 Distribution 0 Low protein binding 0 Large volume of distribution (3L/kg)
0 Highly lipophilic
0 T ½ α (distribution): 10-15 minutes
Ketamine. Pediatric and Neonatal Lexi-Drugs Online. 2014.
Ketamine. MICROMEDEX Healthcare Series. 2014. Ketamine. FDA drug label. Available at http://dailymed.nlm.nih.gov
Route Bioavailability Comments
Oral 20% Extensive first-pass effect Mix oral solution in cola to disguise taste Rectal 25%
Intranasal 50% pH 3.5-5.5 Intravenous product contains preservative (benzethonium chloride
0.1mg/mL)
Intramuscular 90%
Intravenous 90%
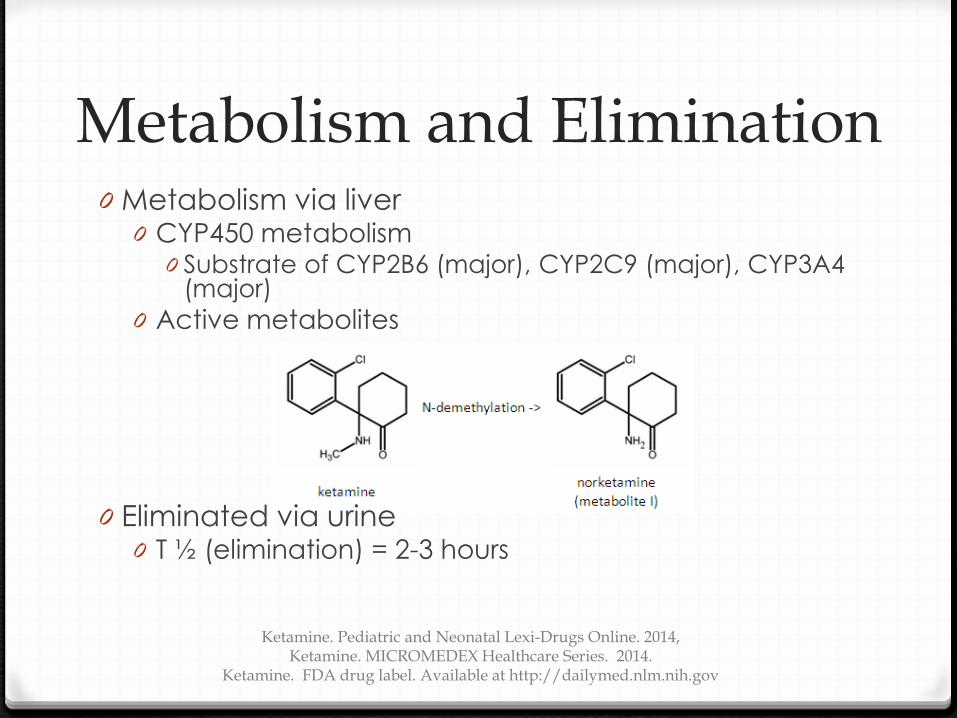
Metabolism and Elimination 0 Metabolism via liver
0 CYP450 metabolism 0 Substrate of CYP2B6 (major), CYP2C9 (major), CYP3A4
(major)
0 Active metabolites
0 Eliminated via urine 0 T ½ (elimination) = 2-3 hours
Ketamine. Pediatric and Neonatal Lexi-Drugs Online. 2014, Ketamine. MICROMEDEX Healthcare Series. 2014.
Ketamine. FDA drug label. Available at http://dailymed.nlm.nih.gov

Ketamine Pharmacodynamics
Ketamine. Pediatric and Neonatal Lexi –Drugs Online. 2014.
Anesthesia Analgesia
Onset of Action
PO < 30 minutes
IM 3-4 minutes 10-15 minutes
IV < 30 seconds
Duration of action
IM 12-25 minutes 15-30 minutes
IV 5-10 minutes 1-2 hours
Recovery
IM 3-4 hours
IV 1-2 hours

Ketamine Adverse Effects: Brain
0 Dissociative analgesia
0 Catalepsy
0 Amnesia
0 Emergence delirium
0 Hallucinations
Olmedo RE. Chapter 85. Phencyclidine and Ketamine. In: Nelson LS. Goldfrank's Toxicologic Emergencies, 9e (2011). Accessed October 10, 2014.
Patel PM. Chapter 19. General Anesthetics and Therapeutic Gases. In: Brunton LL. Goodman & Gilman's The Pharmacological Basis of Therapeutics, 12e (2011). Accessed October 10, 2014.
Eilers H. Chapter 25. General Anesthetics. In: Katzung BG. Basic & Clinical Pharmacology, 12e (2012). Accessed October 10, 2014.

Ketamine Adverse Effects: Cardiovascular
0 Hemodynamic changes
0 Increases blood pressure
0 Increases stroke volume
0 Increases heart rate
0 Increases myocardial oxygen demand
Olmedo RE. Chapter 85. Phencyclidine and Ketamine. In: Nelson LS. Goldfrank's Toxicologic Emergencies, 9e (2011). Accessed October 10, 2014.
Patel PM. Chapter 19. General Anesthetics and Therapeutic Gases. In: Brunton LL. Goodman & Gilman's The Pharmacological Basis of Therapeutics, 12e (2011). Accessed October 10, 2014.
Eilers H. Chapter 25. General Anesthetics. In: Katzung BG. Basic & Clinical Pharmacology, 12e (2012). Accessed October 10, 2014.

Ketamine Adverse Effects: Respiratory
0 Transient apnea
0 Occurs with rapid IV injection (<60 seconds)
0 Bronchodilation
Olmedo RE. Chapter 85. Phencyclidine and Ketamine. In: Nelson LS. Goldfrank's Toxicologic Emergencies, 9e (2011). Accessed October 10, 2014. Patel PM. Chapter 19. General Anesthetics and Therapeutic Gases. In: Brunton LL. Goodman & Gilman's The Pharmacological Basis of
Therapeutics, 12e (2011). Accessed October 10, 2014. Eilers H. Chapter 25. General Anesthetics. In: Katzung BG. Basic & Clinical Pharmacology, 12e (2012). Accessed October 10, 2014.

Ketamine Adverse Effects: Miscellaneous
0 Increased skeletal muscle tone
0 Improves with benzodiazepine administration
0 Increased salivation and secretions
0 Mixed evidence of treatment with
anticholinergics
0 Increased intra-ocular pressure
0 Nystagmus and blurred vision
0 Decreases with physostigmine
0 Crosses placenta
Olmedo RE. Chapter 85. Phencyclidine and Ketamine. In: Nelson LS. Goldfrank's Toxicologic Emergencies, 9e (2011). Accessed October 10, 2014. Patel PM. Chapter 19. General Anesthetics and Therapeutic Gases. In: Brunton LL. Goodman & Gilman's The Pharmacological Basis of
Therapeutics, 12e (2011). Accessed October 10, 2014. Eilers H. Chapter 25. General Anesthetics. In: Katzung BG. Basic & Clinical Pharmacology, 12e (2012). Accessed October 10, 2014.

Ketamine for Treatment of Pain Review of pain pathways

http://www.physioprescription.com/2014/01/06/chronic-pain-all-in-my-head-1/

Types of Pain
Pain
Acute Chronic
Nocicoceptive Neuropathic
Central Peripheral
Visceral Mixed
Adapted from Figure 1. Pain classification and representative indications. Melnikova, I. Nature Reviews Drug Discovery 2010;9:,589-
590.

Biology of Acute versus Chronic Pain
Brookoff D. Hospital Practice. 2000;45-49.

Ketamine for Treatment of Pain
Acute and Chronic Pain: Evidence-based medicine

Ketamine IV Single Dose + IV Opioids Study Surgery
Group (N) KET Dose Opioid Pain
Scores TFA TSD Side
Effects
Menigaux 2001
Adult, Athroscopic menisectomy (50)
0.15 mg/kg preop
Alfentanil P<0.05 - P<0.05 NS
Kudoh 2002
Adult, Orthopedic (70)
1 mg/kg preop
Fentanyl P<0.05 @ 8, 16hr
- - NS
Weinbroum 2003
Adult, Thoracic, Orthopedic
(245)
0.25 – 0.75 mg/kg post
Fentanyl intra, Morphine
post
P<0.001 - P<0.001 ↓ PONV, ↑ central side
effects in KET
Xie 2003
Adult, Gastrectomy (28)
0.5 mg/kg preop
Fentanyl P<0.05 P<0.05 P<0.05 NS
*All studies are randomized double-blind controlled trials. KET=ketamine group; Morph=morphine; NS=not statistically significant; PONV=post-operative nausea and vomiting; Sufent=sufentanil; TFA=time to first request for analgesia; TSD=total supplemental analgesic requirement
Adapted from Table 4 in Subramaniam K. Anesth Analg 2004;99:482-95.
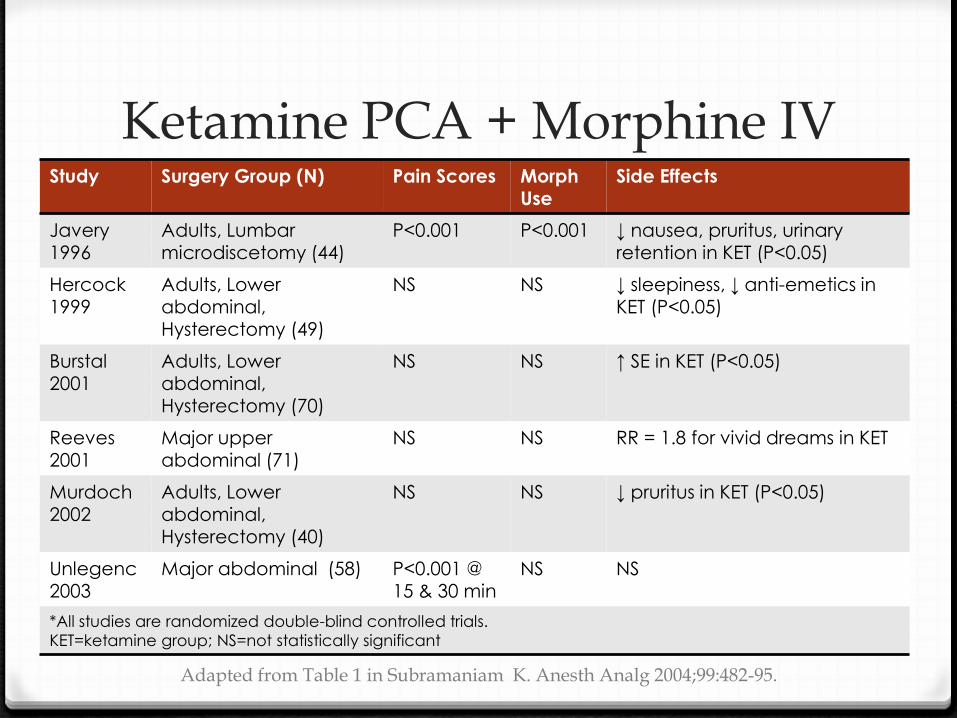
Ketamine PCA + Morphine IV Study Surgery Group (N) Pain Scores Morph
Use Side Effects
Javery 1996
Adults, Lumbar microdiscetomy (44)
P<0.001 P<0.001 ↓ nausea, pruritus, urinary retention in KET (P<0.05)
Hercock 1999
Adults, Lower abdominal,
Hysterectomy (49)
NS NS ↓ sleepiness, ↓ anti-emetics in KET (P<0.05)
Burstal 2001
Adults, Lower abdominal, Hysterectomy (70)
NS NS ↑ SE in KET (P<0.05)
Reeves
2001 Major upper
abdominal (71) NS NS RR = 1.8 for vivid dreams in KET
Murdoch 2002
Adults, Lower abdominal, Hysterectomy (40)
NS NS ↓ pruritus in KET (P<0.05)
Unlegenc
2003 Major abdominal (58) P<0.001 @
15 & 30 min NS NS
*All studies are randomized double-blind controlled trials.
KET=ketamine group; NS=not statistically significant
Adapted from Table 1 in Subramaniam K. Anesth Analg 2004;99:482-95.
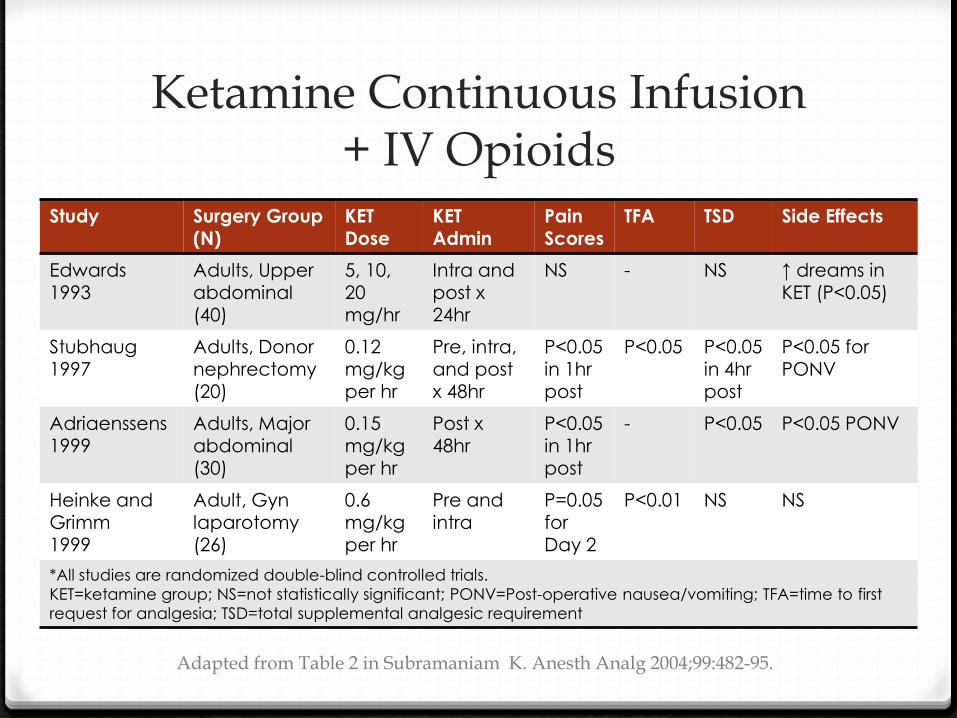
Ketamine Continuous Infusion + IV Opioids
Study Surgery Group (N)
KET Dose
KET Admin
Pain Scores
TFA TSD Side Effects
Edwards 1993
Adults, Upper abdominal (40)
5, 10, 20 mg/hr
Intra and post x 24hr
NS - NS ↑ dreams in KET (P<0.05)
Stubhaug 1997
Adults, Donor nephrectomy (20)
0.12 mg/kg per hr
Pre, intra, and post x 48hr
P<0.05 in 1hr post
P<0.05 P<0.05 in 4hr post
P<0.05 for PONV
Adriaenssens
1999 Adults, Major
abdominal (30)
0.15
mg/kg per hr
Post x
48hr P<0.05
in 1hr post
- P<0.05 P<0.05 PONV
Heinke and Grimm 1999
Adult, Gyn laparotomy (26)
0.6 mg/kg per hr
Pre and intra
P=0.05 for Day 2
P<0.01 NS NS
*All studies are randomized double-blind controlled trials.
KET=ketamine group; NS=not statistically significant; PONV=Post-operative nausea/vomiting; TFA=time to first
request for analgesia; TSD=total supplemental analgesic requirement
Adapted from Table 2 in Subramaniam K. Anesth Analg 2004;99:482-95.

Ketamine Continuous Infusion + IV Opioids
Study Surgery Group (N)
KET Dose
KET Admin
Pain Scores
TFA TSD Side Effects
Jaksch 2002
Adult, Knee arthroscopy
(30)
0.12 mg/kg
per hr
Pre, intra, post x 2hr
NS NS NS NS
Guignard 2002
Adult, Open colorectal (50)
0.12 mg/kg per hr
Pre and Intra
P<0.05 in 15 min
P<0.01 P<0.01 NS
Guillou
2003 Adult, Major
abdominal (93)
0.12
mg/kg per hr
Post x
48hr P<0.05
at 16, 2, 40, and 44hr
- P<0.05 NS
*All studies are randomized double-blind controlled trials. KET=ketamine group; NS=not statistically significant; TFA=time to first request for analgesia;
TSD=total supplemental analgesic requirement
Adapted from Table 2 in Subramaniam K. Anesth Analg 2004;99:482-95.

Ketamine Continuous Infusion + Epidural Opioids
Study Surgery Group (N)
KET Dose KET Admin Opioid Pain Scores
TSD Side Effects
Ilkjaer 1998
Adults, Nephrectomy (52)
10 mg/hr Pre, intra, post
Morph NS NS ↑ sedation wit KET
Aida 2000
Adults, Gastrectomy (61)
0.5 mg/kg per hr
Pre, intra Morph P<0.05 P<0.05 -
De Kock 2001
Adults, Rectal surgery (60)
0.125 – 0.25
mg/kg per hr
Pre, intra Sufent NS NS NS
Kararmaz 2003
Adults, Renal (40)
0.5 mg/kg per hr
Pre, intra Morph P<0.01 P<0.01 ↓ nausea and pruritus in
KET (P<0.05)
*All studies are randomized double-blind controlled trials. KET=ketamine group; Morph=morphine; NS=not statistically significant; Sufent=sufentanil; TSD=total supplemental analgesic requirement
Adapted from Table 3 in Subramaniam K. Anesth Analg 2004;99:482-95.

Epidural Ketamine + Epidural Opioids Study Surgery Group
(N) KET Dose and
Admin
Opioid Pain Scores
TFA TSD Side Effects
Subramaniam 2001
Adult, Upper abdominal (40)
1 mg/kg postop
Morphine - P<0.05 P<0.05 ↑ sedation in KET
Santawat
2002
Adult,
Gynecology (80)
30mg
pre and postop
Morphine NS NS NS NS
Taura 2003
Adult, Hepatectomy (104)
20mg, 30mg postop
Morphine P<0.05 P<0.05 P<0.05 NS
Xie 2003
Adult, Gastrectomy (28)
0.5 mg/kg preop
Fentanyl, PCEA morphine
P<0.05 P<0.05 P<0.05 NS
*All studies are randomized double-blind controlled trials.
KET=ketamine group; Morph=morphine; NS=not statistically significant; PCEA=patient controlled epidural
analgesia; PONV=post-operative nausea and vomiting; Sufent=sufentanil; TSD=total supplemental analgesic
requirement
Adapted from Table 4 in Subramaniam K. Anesth Analg 2004;99:482-95.

Ketamine for Acute Pain in Children
Adapted from Table 4 in Subramaniam K. Anesth Analg 2004;99:482-95.
Study Surgery Group
(N) KET Dose
and Admin Opioid
used Pain
Score TFA TSD
Side
Effects
Ozbek 2002
1-9yrs, Hypospadias repair (109)
0.5 mg/kg caudal preop
Alfentanil NS P=0.001
P<0.01 NS
Dix 2003
7-16yrs, Appendectomy (75)
0.5 mg/kg preop ± 4
mcg/kg per
min postop
Fentanyl NS - NS ↑ in CI KET
Elhakim 2003
5-12yrs, Tonsillectomy (50)
0.1 mg/kg IM preop
Fentanyl P<0.05 P<0.01 P<0.05 NS
O’Flaherty 2003
3-12yrs, Tonsillectomy (80)
0.15 mg/kg IV preop
Fentanyl NS - NS NS
*All studies are randomized double-blind controlled trials.
CI=continuous infusion; KET=ketamine group; NS=not statistically significant; TSD=total supplemental analgesic
requirement

Summary: Ketamine for Acute Pain
0 Ketamine is viable option for addition to
standard practice opioid analgesia in children
and adults
0 Showed greatest utility in abdominal surgery
patients as continuous infusion

Summary: Opioid-sparing Effects of Ketamine
0 Statistically significant decrease in opioid use
with single dose, continuous infusion, and
epidural ketamine
0 No reduction in PONV, pruritus, or respiratory
depression
0 Little to no increase hallucinations and sedation

Ketamine for Cancer Pain
Yang 1996
Methods Randomized, blinded, placebo-controlled,
crossover
Study Group Hospitalized patients with terminal cancer
N=20
Intervention Intrathecal morphine vs. KET 1mg intrathecal +
morphine intrathecal
Outcomes Total morphine dose: Low-dose IT KET reduces
amount of morphine needed
Adverse effects: Frequency not statistically
different between groups. Pruritus, constipation,
urinary retention, N/V, hallucinations noted.
Bell RF, Cochrane Database Syst Rev. 2012 Nov 14
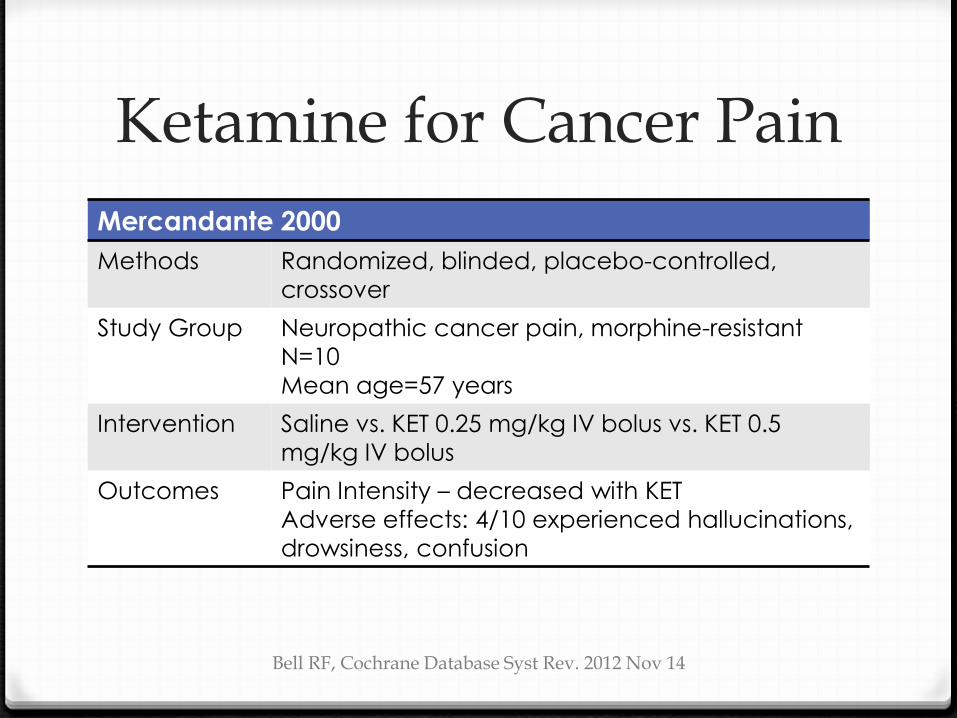
Ketamine for Cancer Pain
Mercandante 2000
Methods Randomized, blinded, placebo-controlled,
crossover
Study Group Neuropathic cancer pain, morphine-resistant
N=10
Mean age=57 years
Intervention Saline vs. KET 0.25 mg/kg IV bolus vs. KET 0.5
mg/kg IV bolus
Outcomes Pain Intensity – decreased with KET
Adverse effects: 4/10 experienced hallucinations,
drowsiness, confusion
Bell RF, Cochrane Database Syst Rev. 2012 Nov 14

Ketamine for Cancer Pain Hardy 2012
Methods Randomized, double-blinded, placebo-
controlled
Study Group Multi-center, palliative care patients with
refractory chronic pain secondary to cancer or its
treatment
N=185
Mean age=63 years
Intervention Subcutaneous saline infusion or subcutaneous KET
infusion (100, 300, 500mg) x 5 days
Outcomes Pain improvement – no difference between
groups
Adverse effects: Double the adverse effects in
KET arm compared to baseline
NNT=25; NNH=6
Hardy J. J Clin Oncol. 2012;30:3611-17.

Summary: Ketamine for Cancer Pain
0 Limited evidence available
0 Small sample sizes
0 Heterogeneous groups
0 Many unanswered questions
0 Optimal dose?
0 Optimal route?
0 Optimal duration?

Ketamine for Chronic Pain Syndromes Patil 2012 CRPS
(N=18)
Non-CRPS
(N=31)
Total
(N=49)
Age (years) Median, (Range)
46 (21-55) 42 (18-68) 45 (18-68)
Gender
n (%) F: 11 (61.1)
M: 7 (38.9) F: 20 (64.5)
M: 11 (35.5) F: 31 (63.3)
M: 18 (36.7)
Number of Infusions Median, (Range)
5.5 (1-36) 3 (1-34) 4 (1-36)
Baseline VAS Mean (SD)
8.2 (1.7) 6.7 (1.9) 7.2 (2)
Infusion Dose (mg/kg) Median, (SD)
1 (0.5) 0.9 (0.4) 0.9 (0.4)
Infusion Duration (minutes) Median, (Range)
43.8 (30-60) 34.7 (30-165) 38.3 (30-165)
Post-Infusion VAS Median, (Range)
0.8 (0-6) 1 (0-9) 0.9 (0-9)
CRPS=complex regional pain syndrome; SD=standard deviation; VAS=visual analog scale
Patil S. Pain Medicine. 2012;13:263-9.
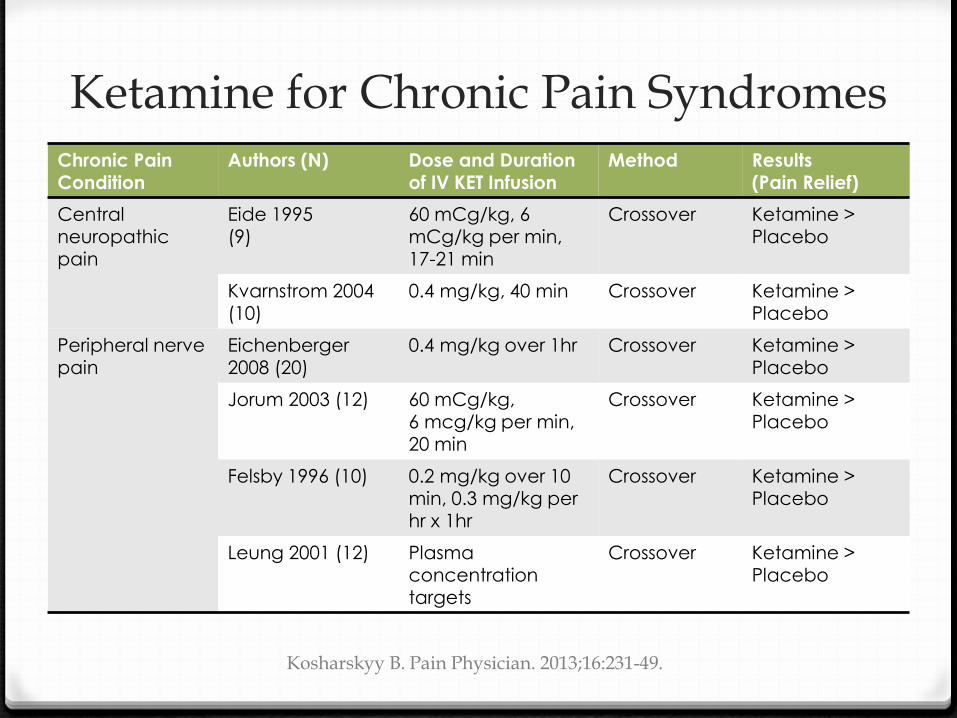
Ketamine for Chronic Pain Syndromes Chronic Pain
Condition Authors (N) Dose and Duration
of IV KET Infusion Method Results
(Pain Relief)
Central neuropathic pain
Eide 1995 (9)
60 mCg/kg, 6 mCg/kg per min, 17-21 min
Crossover Ketamine > Placebo
Kvarnstrom 2004 (10)
0.4 mg/kg, 40 min Crossover Ketamine > Placebo
Peripheral nerve pain
Eichenberger 2008 (20)
0.4 mg/kg over 1hr Crossover Ketamine > Placebo
Jorum 2003 (12) 60 mCg/kg, 6 mcg/kg per min, 20 min
Crossover Ketamine > Placebo
Felsby 1996 (10) 0.2 mg/kg over 10 min, 0.3 mg/kg per hr x 1hr
Crossover Ketamine > Placebo
Leung 2001 (12) Plasma concentration
targets
Crossover Ketamine > Placebo
Kosharskyy B. Pain Physician. 2013;16:231-49.

Ketamine for Chronic Pain Syndromes Chronic Pain
Condition Authors (N) Dose and Duration of IV
KET Infusion Method Results
(Pain Relief)
Post-herpatic neuralgia
Eide 1994 (8) 0.15 mg/kg, 10 min Crossover Ketamine > Placebo
Gottrup 2006 (20)
0.24 mg/kg, 30 min Crossover Ketamine > Placebo
CRPS Sigtermans 2009 (60)
5 – 30 mg/hr x 4.2 days Parallel Ketamine > Placebo
Schwarztman 2009 (19)
25 mg/hr x 4hrs x 10 days Parallel Ketamine > Placebo
Fibromyalgia Graven-
Nielsen 2000 (29)
0.3 mg/kg, 30 min Crossover Ketamine >
Placebo
Sorensen 1995 (11)
0.3 mg/kg, 10 min Crossover Ketamine > Placebo
Noppers 2011
(24) 0.5 mg/kg, 30 min Parallel Ketamine >
Placebo
Kosharskyy B. Pain Physician. 2013;16:231-49

Summary: Ketamine for Chronic Pain Syndromes
0 Ketamine performs better than placebo for
chronic pain syndromes
0 Downfalls:
0 Many small studies, many indications
0 No standard dosing approach (bolus vs.
continuous infusion vs bolus + continuous infusion)
0 No standard duration of ketamine exposure

Final Synopsis: Ketamine for Treatment of Acute and Chronic Pain
0 Ketamine for treatment of acute pain well
established
0 Ketamine for treatment of chronic pain shows
promise
0 Many gaps in chronic pain treatment evidence
0 Necessary to study ketamine further in special
populations
Future Direction
0 Creation of ideal dosage form for both
inpatient and outpatient use
0 Investigate ketamine for treatment of pain in
special populations
0 Cancer
0 Sickle cell crisis
0 Opioid-resistant populations (substance abusers,
back pain patients, chronic pain sufferers)