Keshav word fix.docx

of 16
-
Upload
gerald-harmon -
Category
Documents
-
view
217 -
download
0
Transcript of Keshav word fix.docx
Epidemiological Characteristics of Corneal ulcers in south sharqiya Region
Keshav BR, Zacheria G., Ideculla T., Bhat V., Joseph M.
38Oman Medical Journal 2008, Volume 23, Issue 1, January 2008
39Oman Medical Journal 2008, Volume 23, Issue 1, January 2008Abstract :
Objectives: To understand the epidemiology, predisposing factors, etiology and the outcome of management of corneal ulcers in South Sharqiya region of Oman.Methods: 188 patients who presented to us in eye Ophthalmology Department of Sur regional hospital with corneal ulcers were analyzed retrospectively. The historical aspects including the systemic and local predisposing factors, clinical picture of the ulcer which was noted on slit lamp at the time of presentation, results of culture for which material was taken by scraping of the ulcer, and its sensitivity pattern, type of management, and its outcome, were noted and the results were interpreted.Results: 60.83% were males above the age of 60 years. Severe ulcers were seen in 36.17% of cases. 43.18% of cases showed positive culture of which 88.2% were bacteria and rest were fungal isolates. Of the bacteria 53.84% were pseudomonas, and20% staphylococcus. 83.5% were put on fortified gentamycin and68.61% were on cefuroxime in the initial dual therapy. 37.23% were on ciprofloxacin one time or another during the course of the ulcer. 69.14% of cases recovered fully and 9.57% improved.
introductionCorneal ulcer is a sight threatening disorder presenting in all age groups and either sex world wide. It may resolvewithout any sequelae, progress to perforation and its resultant consequences, or leave behind an opacity which if central may lead to loss of vision. In Oman, corneal opacity is the leading cause of blindness followed by cataract.1 The various risk factors for corneal ulcers and its mode of presentations are rife in literature but they vary from region to region as it depends on the culture, socioeconomic status, occupation, habits, etc, of a particular place/region. The antibiotic sensitivity also varies from region to region. Due to the above stated reasons this study was taken up to evaluate the various risk factors, age and sex predilections, the type of microbes causing the ulcers and the type of antibiotics the organisms are sensitive to so that a systematic approach may be adopted in preventing and treating this sight threatening disorder.The aim of the study is to study the epidemiology of corneal ulcer in South Sharqiya region, the various risk factors and predisposing factors in corneal ulcers, and the bacterial/fungal spectrum causing the ulcers and to determine the best possible empirical therapy and specific therapy for these ulcers please the literature.
54.25% needed hospitalization for less than 1 week and 34% for less than 2 weeks. 58.76% of cases recovered in less than 3 weeks. As local predisposing factors 45 cases (24%) were post surgery, and 29 cases (15.4 %) were having CDK (climatic droplet keratopathy). Diabetes was seen in 8.5% of cases.Conclusion: Corneal ulcer was seen predominantly in males above the age of 60 years, pseudomonas being the main etiological organism. Dual therapy was the commonest empirical therapy. No major systemic risk factor was identified. Post surgical and CDK were the predominant local risk factors.
Keywords: corneal ulcer; pseudomonas; dual therapy.
Received: 3 May 2007Accepted: 28 Oct 2007From the Department of Ophthalmology, Sur Hospital, Sur, Sultanate of Oman. Address correspondence and reprint request to: Dr. Keshav, Head of Department of Ophthalmology, Sur hospital, South Sharqiya Region, Sultanate of OmanP.O. Box 823, P.C. 411e-mail: [email protected]
Method
Patients: One hundred and eighty eight patients treated for corneal ulcers in Sur regional hospital between 14th October2000 and 19 Nov 2006 were included in the study. The catchment area has population of 1: 70000. Almost all cases were advised admission. Corneal ulcer was defined as loss of corneal epithelium with underlying infiltration and suppuration with surrounding inflammation with/without hypopyon.2 In all these patients, symptoms, duration of ulcer, relevant systemic conditions like diabetes, immunosuppression, prolonged hospitalization if any were asked and recorded.Clinical procedures: In most of the cases visual acuity where possible was measured and a detailed slit lamp examination of the anterior segment was performed wherever possible noting the size of ulcer, depth and extent of infiltrations, presence/ absence of hypopyon, scleral extension, corneal thinning and so on and the ulcer was graded as mild, moderate or severe as per the Jones guidelines.3 Local eye conditions predisposing to corneal ulceration like lagophthalmos, dacryocystitis, trichiasis, surgery and corneal opacity/degeneration were noted. Materials were taken from the ulcers with a 23g needle/scalpel from the
Characteristics of Corneal Ulcers ... Keshav et al.
Characteristics of Corneal Ulcers ... Keshav et al.
base and edges of the ulcer and inoculated by linear streaking in blood, chocolate and mcconkeys media and sent to the lab for culture sensitivity. Bacterial cultures were reported after 48 hrs of incubation. In almost all cases, admission was ensured and started on dual (fortified gentamycin+fortified cefuroxime)/monotherapy (ofloxocin) empirically. When a fungal etiology was suspected or in cases not responding to antibacterial treatment, material was taken from such ulcers for KOH smear and inoculation in Sabaorauds medium.Our earlier protocol was to go by the clinical picture and if not suggestive of fungal we would not send the sample in sabaurauds in the first instance. Another reason being that saborauds medium was not routinely available when these samples were sent.Progress of the ulcer was noted every day, when in the hospital by measuring the size of the ulcer, observing the hypopyon if present, infiltrations and patients symptoms. Patients were discharged usually when the ulcer showed signs of regression and if the patient seemed compliant to therapy. The size of the ulcer asvisual acuity is only affected if the ulcer is central.Laboratory: Bacterial growth in culture media was considered significant if it was observed in two solid phase media or confluent growth in one media. Fungal isolation in SDA (sabaurauds dextrose agar) or observation of hyphal filaments in KOH smear was considered sufficient for diagnosis.
Results
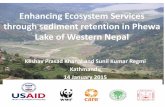
Of the 188 patients, 121 (64.36%) were males and 67 (35.73%) were females. 24 patients (12.76%) were 60 years of age (Figure 1). Thus males and patients above the age of 60 years showed greater frequency of corneal ulcer.
Figure 1: Shows proportion of males and females among the various age groups of patients
With regards to severity of ulcers, the ulcers were graded as per Jones guidelines and we found that 65 cases (34.57%) had mild
ulcers, 55 cases (29.25%) had moderate ulcers and 68 patients(36.17%) had severe ulcers. (Figure 2)
Figure 2: Shows the various grades of severity of corneal ulcers in the studied subjects
Thus severe ulcers were marginally in higher numbers as compared to other types of ulcers.100 patients (53.19%) showed hypopyon while the rest had no hypopyon showing almost the same frequency. Most of the patients in whom visual acuity was elicited showed a vision of< 3/60 (120 patients-65%), 43 patients (22.87%) were blind and 22 patients (11.89%) had a vision of > 3/60. (Table 1)
table 1: Shows the Visual status of patients in the study
NPL3/60
4312022
23.24%64.86%11.89%
NPL: No Perception of Light
When microbiological isolation was evaluated it was found that in 76 patients (43.18%) bacteria/fungi was isolated where material was sent for culture/sensitivity and in 100 patients (56.81%) no isolate was seen.4 Patients (5.1%) showed fungal isolates. In 12 patients scraping could not be done. (Figure 3)
Figure 3: Shows the proportions of patients with positive and negative microbial isolation on culture
Thus 43.18% of patients in the study showed either bacteria/fungus in culture. Among the isolates, 9 cases (11.84%) were fungi
and the rest (88.26%) were bacteria. Of the bacterial isolates, pseudomonas was found in 35 cases (53.84%), staphylococci was found in 13 cases(20%), streptococcus pneumonia was found in12 cases (18.46%), streptococci was found in 2 cases (3%) and klebsiella was found in 5 patients (7.69%). (Figure 4)
Figure 4: Shows the proportion of patients with specific microbial isolates in positive cultures
Thus in over half the cases with bacterial isolates, pseudomonas was seen (53.84%).In so far as treatment is concerned, almost all patients suspected to be bacterial were started on dual treatment of fortified gentamycin (14mgm/ml) and cefuroxime (50mgm/ml) as empirical therapy. 157 patients (83.5%) were given fortified gentamycin and 129 patients (68.61%) were given cefuroxime. 70 patients (37.23%)were given T. Ciprofloxacin, 21 patients (11.17%) were administered ofloxacin eye drops as initial line of therapy. 51 patients (27.12%) were covered with fucidic acid ointment at night.22 patients (11.70%) were changed to ceftazidime (50mgm/ml) based on the c/s report when the ulcer was not responding. 16 patients (8.51%) got ceftriaxone drops (50mgm/ml). Cephradine drops (4 patients) and vancomycin drops (7 patients) were administered in a small proportion of patients. Ketoconazole drops 2 mgm/ml formed by dissolving 200 mgm tab in artificial tears was given to 20 patients (10.63%) who were suspected or proven to have fungal ulcers. Amphotericin drops were started in6 patients (3.19%) with fungal ulcers. (Figure 5)
Figure 5: Shows the various antibiotics that the study patients were put on for treatment of corneal ulcer
When the response to treatment were analyzed it was seen that around 130 (69.14%) patients recovered, 18 (9.57%) patients showed signs of regression but failed to keep up the appointment to assess the course of the ulcer, 10 (5.31%) patients the ulcer remained stationary and left seeking advice elsewhere, 17 (9%) patients left against medical advise and 9 cases (4.78%) worsened. (Figure 6)
Figure 6: Shows the outcome of treatment in patients enrolled in the study
Thus a majority of patients responded to our line of management with only 9 cases showing signs of progression/worsening.When the length of hospitalization was analyzed it was seen that 102 patients (54.25%) stayed for less than a week and 64 patients (34%) stayed for 1-2 weeks and the rest stayed for morethan 2 weeks. (Table 2)
table 2: Shows the length of hospitalization and time taken for recovery in our patients
Less than More than 1 weekMore than 2 weeksMore than 3 weeks1 week& less than 2 week& less than 3 weeks
Length of stay
Time for recovery102(54.25%)
26(19.8%)64(34%)
37(28.2%)13(6.9%)
14(10.68%)9(4.78%)
53(40.45%)
Thus, majority (88%) of patients were discharged within 2 weeks.
With regards to the time of recovery, it was found that 26 patients (19.84%) took less than a week to recover, 37 patients (28.24%) took 1-2 weeks to recover, 14 patients (10.68%) took 2-3 weeks to recover and 53 patients (40.45%) took more than 3 weeks to recover. (Table 2) Thus, around 40% of cases required more than 3 weeks for recovery and 60% took less than 3 weeks.Of the relevant eye conditions predisposing to c.ulcer it was found that about 45 patients (24%) had undergone intraocular surgery one time or other before the development of ulcer. 15 patients (8%) showed trichiasis, 29 patients (15.4%) showed corneal degeneration, 11 cases (5.85%) had h/o trauma, 4 patients (2.12%) gave h/o C.L.wear, 3 patients (1.59%) were on local steroids, glaucoma was present in 27 patients (14.36%) and 5 patients had corneal opacity, 2(1%) patients had proptosis and 7 patients (3.72%) had blepharitis. (Table 3)
is the first study of its kind in this region.In this study males clearly had higher incidence of corneal ulcers (64.36%) than females. This is in conformity with several studies conducted elsewhere like the madurai study by Srinivasan et al,2 wherein the ratio of male to female was 1.6:1 and in a study by Bashir et al,5 males again predominated. This could be explained by the fact that they are more involved in outdoor occupation and hence exposed to unfavorable circumstances like exposure to UV light especially with farmers and fishermen, trauma in agriculturists and date pickers, and so on, leading to corneal ulceration. In a study by Upadhyay et al.6 males and females were found to be equally affected.With regards to age in our study, majority (64.36%) of them were over 60 years of age. The Madurai study also concludes thesame.2 In our study patients above 60 years had many predisposing
table 3: Shows the associated local eye conditions in the patients enrolled in the study
ProptosisPost-operative BlepharitisTrichiasisCorneal. degTrauma CL* DrugsGlaucomaCorneal opacity
021.06%4523.93%73.72%157.97%2915.42%115.85%42.12%31.59%271.43%52.65%
*CL: Contact Lens
Among the systemic diseases diabetes was noted in 16 patients(8.5%) while 1 patient was debilitated.Of the complications perforation at the time of presentation or after starting treatment in the hospital was seen in 33 patients (17.55%), 6 patients (3.19%) developed descemetocele, 4 patients (2.12%) developed endophthalmitis and 12 (6.38%) patients had non-healing ulcers or persistent epithelial defect. (Table 4)
table 4: Shows the proportion of patients with various complications
Perforation Descemetocele Endophthalmitis Recurrent/non healing
3317.5%063.19%042.12%126.38%
Discussion
Corneal ulceration continues to be one of the most important causes of ocular morbidity and blindness worldwide. In a national survey conducted in 1996-97 in Oman, the prevalence of blindness was 1.1% with corneal opacity amounting to 31.6% of cases of which 79% were due to nontrachomatous causes like corneal ulcer.1 This study is a retrospective analysis of data of patients who were treated for corneal ulcers in Sur Regional hospital of South sharqiya region from October 2000 to 19th November 2006. This
factors like CDK, dryness, cataract surgery, glaucomatous patients on medications, and lid deformities due to trachomatous scarring which probably predisposed this age group to corneal ulceration more than the other age groups. In a study by Laspina et al,7 it was found that the greatest frequency was in the age group of 30-59 years, while in our study patients between 30-60 years accounted for 23% of the cases.When the severity of ulcers at presentation was considered, it was found that sever ulcers were marginally higher (36.17%) as compared to moderate (29.25%) and mild ulcers (34.37%). Thus, corneal ulcers occurred almost at equal frequency in so far as severity was concerned.In a study by Mcleod et al.4 it was seen that 33 ulcers (44.59%) were moderate and 41(65.41%) were severe suggesting that severe ulcers were more often seen than moderate ulcer, although the way the severity was classified was not clear. The marginal increase in severe ulcers in our study was partly due to higher incidence of pseudomonas corneal ulcers (53.84%) as compared to other types of microbes which is known to cause severe and rapidly progressive ulcer.Where visual acuity could be recorded on presentation, it was found that around 65% of them had a visual acuity of less than 3/60. The poor VA could be due to the ulcer itself or the predisposing factors like corneal degeneration/opacity or due to cataract. 22.87% had no perception of light at presentation. No
study so far has mentioned Visual acuity at presentation. The significance of this finding is difficult to find out. Patients who were blind were seen in a quarter of our patients who are likely to suffer one type of injury or the other, or may have predisposing factors like corneal degeneration/corneal opacity or corneal edema due to absolute glaucoma.43.18% of all the cases showed either fungus/bacteria in our study while the rest showed no isolates. In 5% of cases fungus was grown in culture. In a study by Srinivasan et al.2 68.4% showed culture positive. Bashir et al.5 showed a bacterial yield of 40% almost similar to our study. fungal growth was found in 12.5% of cases in bashers study,5 and 46.8% in madurai study.2 The low yield of fungus in our cases were probably due to the fact that cases of trauma leading to corneal ulcers were small in number (5.85%) while in madurai study it was of the order of 65.4%.Of the bacterial isolates, 53.84 % was pseudomonas. In the Madurai study,2 the most common isolate was streptococcus pneumoniae and the author has attributed it to the large numbers of chronic dacryocystitis that was seen in his study where pneumococci was the prime isolate. In our study, pneumococci constituted 18.46% of the cases. In several other studies,5,6 pneumococci was the most common isolate. In a study by Laspina et.al,7 coagulase negative staphylococcus was the most common isolate. The reason for the variation could be explained probably due to different climatic conditions, socioeconomic standards, culture and occupation that are seen in these geographical areas. In our study no patients had dacryocystitis while cases with corneal opacities and degenerations were seen more often. In the Madurai study, pseudomonas was seen in 14.4% of isolates. Laspina et al,6 also showed 14% of the isolates to be pseudomonas. In a study by Leck et al,8 pseudomonas was found to be the prime isolate amongst the bacterial ulcers in Ghana and in South India where similar techniques for isolation was used. In the same study the prime bacteria was streptococcus species and the author has attributed it to the changes in bacterial flora within the geographical area as influenced by climate and environment.Majority of our patients who were started on empirical therapy were on Cefuroxime drops (68.61%) and fortified gentamycin (83.5%). Other cephalosporins like ceftriaxone, ceftazidime were administered if culture/sensitivity showed them to be effective against the isolated organism and the empirical therapy was not helping. Fucidic acid ointment was administered in 27.12 % of patients to cover the sleeping time in some cases. Monotherapy with ofloxacin was started in 11.17% of cases. In a study published in ophthalmology (no author listed),9 it was found that treatment with fortified gentamycin and cefuroxime showed equally good response when compared with ofloxcin drops and suggested
monotherapy is less toxic. In our study, monotherapy was less successful than dual therapy as many patients on monotherapy had to be switched over to dual therapy in the course of treatment. This probably is because of varying sensitivity patterns in the two areas tested. In a study by McLeod et al.4 dual therapy was found to be effective in treating most bacterial corneal ulcers. Gentamycin and second to third generation cephalosporin cover a broad spectrum of bacteria and thus was found to be successful as an empirical therapy. Fluoroquinolines (Oflox and Ciprofloxacin) are not so effective against streptococcal species and increasing resistance is noted of late to these antibiotics thus may not be a suitable drug to use in empirical therapy.With the above therapy it was found that about 60% of patients required less than 3 weeks to recover while the rest took more time to recover. In one study (no authors listed),9 it was seen that67.9% on dual therapy were cured within 14 days of treatment. The results between the two studies are nearly comparable.Regarding length of hospitalization, it was found that 88% of the patients were discharged in less than 2 weeks of whom over50% were discharged in 1 week indicating that patients were discharged much before their ulcers were healed thus reducing the cost of hospitalization.Among the patients treated about 80% showed full recovery (69.14%) or improvement following the treatment while a few worsened (4.78%) and a few of them left against medical advise suggesting that our line of treatment was fairly acceptable. This is in conformity with a study by (no authors listed),8 wherein the cure occurred in more than 60% of the cases in the two groups on either dual/monotherapy.In various studies,2, 3, 6 trauma was a major predisposing factor while in our study trauma was seen in 5.85% of patients, a striking difference. This, also, explains the low incidence of fungal ulcers (10.63%) in our study. The number of patients with h/o Contact lens(CL) was also negligible (2%), as compared to a study by Ly CN et al.10 where 36% gave h/o CL use and Keay et al.11 showed33.7% gave h/o CL use. The low incidence in our study was due to the fact that a majority of them were over 60 years and hail from rural areas. In a study by Basak et al.12 the number of CL users were negligible (4/1198 patients) as most of his patients were farmers from rural areas. Intraocular surgery was seen in 24% of cases and this could only be a presumed risk factor as the cornea may be more prone for ulceration than normal as they were on steroids for over a month. this can predispose the cornea to invasion by bacteria/fungi due to lowering of local resistance and to some extent presence of sutures for a long time, which may accumulate mucus and predispose the cornea for ulceration. Basak et al,12 have found only a few cases that were post surgical (8 of 1198 patients).
Other risk factors like trichiasis, corneal degeneration, blepharitis, and proptosis were seen in a few cases. CDK was found in 15% of cases while in madurai study,2 it was seen in 9 of the 434 patients. Climatic droplet keratopathy is presumably caused by exposure to UV light, especially people who work outdoors are more prone for it. Frequent epithelial erosions over the mulberry deposits in CDK renders the cornea more vulnerable to ulceration.Diabetes as a predisposing factor was seen in 8.5% of cases in Madurai study,2 and a study by Basak et al.12 (7.6%) also showed a low incidence of DM among the patients with corneal ulcer.Perforation as a complication was seen in 17% of the cases. Either they presented to us with perforation (7 of 15 cases) or they developed this after admission. The high incidence of pseudomonas ulcer in this study can explain this complication in most of the cases.
Conclusions
The major aetiological agent in our study was bacterial with fungal ulcers forming a small proportion. Pseudomonas species was the major bacteria.Fungal cases were few (5%) in our study. Dual therapy with fortified gentamycin and cefuroxime drops was effective in treating a majority of corneal ulcers.
References
1. Khandekar R, Mohammed AJ, Negrel AD, Riyami AA. The prevalence and causes of blindness in the Sultanate of Oman: the Oman Eye Study (OES). Br J Ophthalmol 2002 Sep;86(9):957-962.2. Srinivasan M, Gonzales CA, George C, Cevallos V, Mascarenhas JM, Ashokan B, et al. Epidemiology and etiological diagnosis of corneal ulceration in Madurai. South India, BJO 1997;81:965-971.
3. Jones DB. Decision-making in the management of microbial keratitis.Ophthalmology 1981 Aug;88(8):814-820.4. McLeod SD, Kolahdouz-Isfahani A, Rostamian K, Flowers CW, Lee PP, McDonnell PJ. The role of smears, cultures, and antibiotic sensitivity testing in the management of suspected infectious keratitis. Ophthalmology 1996Jan;103(1):23-28.5. Bashir G, Shah A, Thokar MA, Rashid S, Shakeel S. Bacterial and fungal profile of corneal ulcersa prospective study. Indian J Pathol Microbiol 2005Apr;48(2):273-277.6. Upadhyay MP, Karmacharya PC, Koirala S, Tuladhar NR, Bryan LE, Smolin G, et al. Epidemiologic characteristics, predisposing factors, and etiologic diagnosis of corneal ulceration in Nepal. Am J Ophthalmol 1991Jan;111(1):92-99.7. Laspina F, Samudio M, Cibilis D, Ta CN, Farina N, Sanabria R, et al.Graefes Epidemiological characteristics of microbiological results on patients with infectious corneal ulcers: A 13 year survey in Paraguay. Arch Clin Exp Ophthalmology 2004;242:204-209 .8. Leck AK, Thomas PA, Hagan M, Kaliamurthy J, Ackuaku E, John M, et al. Etiology of supportive corneal ulcers in Ghana and south India and epidemiology of fungal keratitis. BJO 2002;86:1211-1215 .9. The Ofloxacin Study Group. Ofloxacin monotherapy for the primary treatment of microbial keratitis: a double-masked, randomized, controlled trial with conventional dual therapy. Ophthalmology 1997 Nov;104(11):1902-1909.10. Ly CN, Pham JN, Badenoch PR, Bell SM, Hawkins G, Rafferty DL, et al. Bacteria commonly isolated from keratitis specimens retain antibiotic susceptibility to fluoroquinolones and gentamicin plus cephalothin. Clin Experiment Ophthalmol 2006 Jan-Feb;34(1):44-50.11. Keay L, Edwards K, Naduvilath T, Taylor HR, Snibson GR, Forde K, et al. Microbial keratitis predisposing factors and morbidity. Ophthalmology2006 Jan;113(1):109-116.12. Basak SK, Basak S, Mohanta A, Bhowmick A. Epidemiological and microbiological diagnosis of suppurative keratitis in Gangetic West Bengal, eastern India. Indian J Ophthalmol 2005 Mar;53(1):17-22.
Tujuan: Untuk memahami epidemiologi, faktor-faktor, etiologi dan hasil pengelolaan ulkus kornea di wilayah Selatan Sharqiya Oman predisposisi. Metode: 188 pasien yang disajikan kepada kita di mata Ophthalmology Departemen Sur rumah sakit daerah dengan ulkus kornea dianalisis secara retrospektif. Aspek historis termasuk faktor predisposisi sistemik dan lokal, gambaran klinis dari ulkus yang tercatat pada lampu celah pada saat presentasi, hasil kultur untuk bahan yang diambil oleh gesekan ulkus, dan pola sensitivitas, jenis manajemen , dan hasilnya, dicatat dan hasilnya ditafsirkan. Hasil: 60,83% adalah laki-laki di atas usia 60 tahun. Ulkus parah terlihat pada 36.17% kasus. 43.18% kasus menunjukkan kultur yang positif 88.2% adalah bakteri dan sisanya adalah isolat jamur. Bakteri 53,84% adalah pseudomonas, dan 20% staphylococcus. 83,5% ditempatkan pada gentamisin dan 68,61% berada di cefuroxime dalam terapi ganda awal. 37,23% berada di ciprofloxacin satu waktu atau yang lain selama ulkus. 69.14% kasus sembuh total dan 9,57% meningkat 4.25% diperlukan rawat inap kurang dari 1 minggu dan 34% kurang dari 2 minggu. 58.76% kasus pulih dalam waktu kurang dari 3 minggu. Sebagai predisposisi lokal faktor 45 kasus (24%) adalah pasca operasi, dan 29 kasus (15,4%) sedang CDK (climate droplet keratopathy). Diabetes terlihat pada 8,5% kasus. Kesimpulan: ulkus kornea terlihat terutama pada laki-laki di atas usia 60 tahun, pseudomonas menjadi organisme etiologi utama. Terapi ganda adalah terapi empiris yang paling umum. Tidak ada faktor risiko utama yang teridentifikasi. Posting bedah dan CDK merupakan faktor risiko lokal dominan.
Kata kunci: ulkus kornea; pseudomonas; terapi ganda.
Diterima: 3 Mei 2007 Diterima: 28 Oktober 2007 Dari Departemen Ophthalmology, Sur Rumah Sakit, Sur, Kesultanan Oman. Alamat korespondensi dan permintaan cetak ulang ke: Dr Keshav, Kepala
Departemen Ophthalmology, rumah sakit Sur, South Sharqiya Region, Kesultanan Oman P.O. Box 823, P.C. 411 e-mail: [email protected]
pengantar Ulkus kornea adala gangguan penglihatan yang mengancam pada semua kelompok umur dan jenis kelamin di seluruh dunia. Ini dapat sembuh tanpa gejala sisa apapun, terjadi perforasi dan konsekuensi yang dihasilkannya, atau meninggalkan opacity yang jika pusat dapat menyebabkan kehilangan penglihatan. Di Oman, opacity kornea adalah penyebab utama kebutaan diikuti oleh cataract.(1) Berbagai faktor risiko ulkus kornea dan presentasi yang marak dalam literatur tetapi mereka bervariasi dari daerah ke daerah karena tergantung pada kultur, status sosial ekonomi, pekerjaan , kebiasaan, dll, dari tempat tertentu / wilayah. Sensitivitas antibiotik juga bervariasi dari daerah ke daerah. Karena alasan tersebut di atas penelitian ini diambil untuk mengevaluasi berbagai faktor risiko, usia dan jenis kelamin predileksi, jenis mikroba yang menyebabkan ulkus dan jenis antibiotik organisme yang sensitif terhadap sehingga pendekatan sistematis dapat diadopsi dalam mencegah dan mengobati gangguan penglihatan mengancam ini. Tujuan dari penelitian ini adalah untuk mempelajari epidemiologi ulkus kornea di wilayah Selatan Sharqiya, berbagai faktor risiko dan faktor predisposisi dalam ulkus kornea, dan spektrum bakteri / jamur yang menyebabkan ulkus dan untuk menentukan yang terbaik mungkin terapi empiris dan terapi khusus untuk ulkus ini menyenangkan literatur.
metode
Pasien: Seratus delapan puluh delapan pasien dirawat karena ulkus kornea di rumah sakit daerah Sur antara 14 Oktober 2000 dan 19 Nov 2006 dilibatkan dalam penelitian tersebut. Daerah tangkapan memiliki populasi 1: 70000. masuk Hampir semua kasus disarankan. Ulkus kornea didefinisikan sebagai hilangnya epitel kornea dengan infiltrasi yang mendasari dan nanah dengan sekitarnya peradangan dengan / tanpa hypopyon.2 Pada semua pasien ini, gejala, durasi maag, kondisi sistemik terkait seperti diabetes, imunosupresi, rawat inap berkepanjangan jika ada ditanya dan dicatat . Prosedur klinis: Dalam sebagian besar kasus ketajaman visual mana mungkin diukur dan pemeriksaan lampu celah rinci segmen anterior dilakukan sedapat mungkin mencatat ukuran ulkus, kedalaman dan luasnya infiltrasi, ada / tidaknya hypopyon, ekstensi scleral, kornea menipis dan seterusnya dan ulkus itu
dinilai sebagai ringan, sedang atau berat sesuai kondisi mata lokal Jones guidelines.3 predisposisi ulkus kornea seperti lagophthalmos, dakriosistitis, trichiasis, operasi dan opacity kornea / degenerasi dicatat. Bahan diambil dari ulkus dengan jarum 23g / scalpel dari dasar dan tepi ulkus dan diinokulasi goresan linear dalam darah, cokelat dan media mcconkeys dan dikirim ke laboratorium untuk kultur sensitivitas . Kultur bakteri dilaporkan setelah 48 jam inkubasi. Dalam hampir semua kasus, penerimaan dipastikan dan mulai dual (diperkaya gentamisin + cefuroxime diperkaya) / monoterapi (ofloxocin) secara empiris. Ketika etiologi jamur diduga atau dalam hal tidak menanggapi pengobatan antibakteri, bahan diambil dari ulkus tersebut untuk KOH smear dan inokulasi di media Sabaorauds. Protokol sebelumnya kami adalah untuk pergi dengan gambaran klinis dan jika tidak sugestif dari jamur kami tidak akan mengirim sampel dalam sabaurauds dalam contoh pertama. Alasan lain media saborauds tidak secara rutin tersedia ketika sampel tersebut dikirim. Kemajuan ulkus dicatat setiap hari, ketika di rumah sakit dengan mengukur ukuran ulkus, mengamati hypopyon jika ada, infiltrasi dan pasien gejala. Pasien dipulangkan biasanya ketika ulkus menunjukkan tanda-tanda regresi dan jika pasien tampak sesuai untuk terapi. Ukuran ulkus ketajaman asvisual hanya terpengaruh jika ulkus adalah pusat. Laboratorium: Pertumbuhan bakteri dalam media kultur dianggap signifikan jika diamati dalam dua media yang fase padat atau pertumbuhan konfluen in-one media. Isolasi jamur di SDA (sabaurauds dextrose agar) atau pengamatan filamen hifa di KOH smear dianggap cukup untuk diagnosis.
hasil
Dari 188 pasien, 121 (64,36%) adalah laki-laki dan 67 (35,73%) adalah perempuan. 24 pasien (12.76%) adalah 60 tahun (Gambar 1). Jadi laki-laki dan pasien di atas usia 60 tahun menunjukkan frekuensi yang lebih besar dari ulkus kornea
Gambar 1: Menunjukkan proporsi laki-laki dan perempuan di antara berbagai kelompok usia pasien
Sehubungan dengan keparahan ulkus, borok yang dinilai sesuai pedoman Jones dan kami menemukan bahwa 65 kasus (34,57%) memiliki ulkus ringan, 55
kasus (29.25%) memiliki ulkus moderat dan 68 pasien (36.17%) memiliki ulkus parah. (Gambar 2)
gambar 2: Menunjukkan berbagai nilai keparahan ulkus kornea di bidang studi
Jadi ulkus parah yang sedikit dalam jumlah yang lebih tinggi dibandingkan dengan jenis lain dari ulcers.100 pasien (53,19%) menunjukkan hypopyon sementara sisanya tidak memiliki hypopyon menunjukkan hampir frekuensi yang sama. Sebagian besar pasien yang ketajaman visual menimbulkan menunjukkan visius 3/60. (Tabel 1)
Tabel 1: Menunjukkan status Visual dari pasien dalam penelitian iniNPL3/60
4312022
23.24%64.86%11.89%
Ketika isolasi mikrobiologi dievaluasi ditemukan bahwa pada 76 pasien (43.18%) bakteri / jamur diisolasi di mana bahan dikultur / sensitivitas dan pada 100 pasien (56,81%) tidak ada isolat Pasien
seen.4 (5,1%) menunjukkan jamur isolat. Pada 12 pasien menggores tidak bisa dilakukan. (Gambar 3)
Gambar 3: Menunjukkan proporsi pasien dengan isolasi mikroba positif dan negatif pada kultur
Dengan demikian 43.18% dari pasien dalam penelitian ini menunjukkan baik bakteri / jamur dalam kultur . Di antara isolat, 9 kasus (11.84%) adalah jamur dan sisanya (88,26%) adalah bakteri. Isolat bakteri, pseudomonas ditemukan pada 35 kasus (53,84%), stafilokokus ditemukan pada 13 kasus (20%), streptococcus pneumonia ditemukan pada 12 kasus (18,46%), streptokokus ditemukan pada 2 kasus (3%) dan klebsiella ditemukan pada 5 pasien (7.69%). (Gambar 4)
Gambar 4: Menunjukkan proporsi pasien dengan mikroba tertentu isolat dalam kultur positif dan sisanya (88,26%) adalah bakteri. Isolat bakteri, pseudomonas ditemukan pada 35 kasus (53,84%), stafilokokus ditemukan pada 13 kasus (20%), streptococcus ditemukan dalam 12 kasus (18,46%), streptococcus ditemukan 2 kasus (3%) dan klebsiella ditemukan pada 5 pasien (7,69%) gamba 4: Menunjukkan proporsi pasien dengan mikroba tertentu isolat dalam kultur positif
Jadi di lebih dari setengah kasus dengan isolat bakteri, pseudomonas terlihat (53,84%). Sejauh pengobatan yang bersangkutan, hampir semua pasien yang diduga bakteri memulai pengobatan ganda gentamisin diperkaya (14mgm /ml) dan cefuroxime (50mgm / ml) sebagai terapi empiris. 157 pasien (83,5%) diberi gentamisin diperkaya dan 129 pasien (68,61%) diberi cefuroxime. 70 pasien (37,23%) diberi T. Ciprofloxacin, 21 pasien (11,17%) diberikan ofloksasin tetes mata garis sebagai awal terapi. 51 pasien (27.12%) ditutupi dengan salep asam fucidic di malam hari. 22 pasien (11.70%) diubah menjadi ceftazidime (50mgm / ml) berdasarkan c / s laporan ketika ulkus tidak menanggapi. 16 pasien (8,51%) mendapat tetes ceftriaxone (50mgm / ml). Sefradin tetes (4 pasien) dan vankomisin tetes (7 pasien) diberikan pada sebagian kecil pasien. Ketoconazole turun 2 mgm / ml dibentuk dengan melarutkan 200 mgm tab di air mata buatan diberikan kepada 20 pasien (10.63%) yang diduga atau terbukti memiliki ulkus jamur. Tetes Amfoterisin dimulai pada 6 pasien (3,19%) dengan ulkus jamur. (Gambar 5)
Gambar 5: Menampilkan berbagai antibiotik yang pasien studi ditempatkan di untuk pengobatan ulkus kornea Ketika respon terhadap pengobatan dianalisis terlihat bahwa sekitar 130 (69,14%) pasien sembuh, 18 (9,57%) pasien menunjukkan tanda-tanda regresi tetapi gagal untuk menjaga janji untuk menilai jalannya ulkus, 10 (5,31%) penderita maag tetap diam dan meninggalkan mencari nasihat tempat lain, 17 (9%) pasien yang tersisa terhadap saran medis dan 9 kasus (4,78%) memburuk. (Gambar 6)Dengan demikian mayoritas pasien menanggapi baris kami manajemen dengan hanya 9 kasus yang menunjukkan tanda-tanda perkembangan / memburuk. Ketika lama waktu rawat inap dianalisis terlihat bahwa 102 pasien (54.25%) tinggal selama kurang dari seminggu dan 64 pasien (34%) tinggal selama 1-2 minggu dan sisanya tinggal selama lebih dari 2 minggu.Sehubungan dengan waktu pemulihan, ditemukan bahwa 26 pasien (19.84%) waktu kurang dari satu minggu untuk pulih, 37 pasien (28,24%) mengambil 1-2 minggu untuk pulih, 14 pasien (10.68%) mengambil 2-3 minggu untuk pulih dan 53 pasien (40.45%) membutuhkan waktu lebih dari 3 minggu untuk pulih. (Tabel 2) Dengan demikian, sekitar 40% dari kasus yang dibutuhkan lebih dari 3 minggu untuk pemulihan dan 60% waktu kurang dari 3 minggu.
Dari kondisi mata yang relevan predisposisi untuk c.ulcer ditemukan bahwa sekitar 45 pasien (24%) telah menjalani operasi intraokular satu waktu atau lainnya sebelum pengembangan ulkus. 15 pasien (8%) menunjukkan trichiasis, 29 pasien (15,4%) menunjukkan degenerasi kornea, 11 kasus (5,85%) memiliki h / o trauma, 4 pasien (2,12%) memberi h / o penggunaan lensa kontak, 3 pasien (1,59%) berada di steroid lokal, glaukoma ditemukan pada 27 pasien (14,36%) dan 5 pasien memiliki opacity kornea, 2 (1%) pasien memiliki proptosis dan 7 pasien (3,72%) memiliki blepharitis.Di antara diabetes penyakit sistemik tercatat pada 16 pasien (8,5%) sedangkan 1 pasien lemah. Komplikasi perforasi pada saat presentasi atau setelah memulai pengobatan di rumah sakit terlihat pada 33 pasien (17.55%), 6 pasien (3,19%) mengembangkan descemetocele, 4 pasien (2,12%) mengembangkan endophthalmitis dan 12 (6,38%) pasien memiliki borok non-penyembuhan atau cacat epitel persisten. (Tabel 4)
Tabel 4: Menunjukkan proporsi pasien dengan berbagai komplikasi
Perforation Descemetocele Endophthalmitis Recurrent/non healing
3317.5%063.19%042.12%126.38%
diskusi
Ulserasi kornea terus menjadi salah satu penyebab paling penting dari morbiditas okular dan kebutaan di seluruh dunia. Dalam sebuah survei nasional yang dilakukan pada 1996-1997 di Oman, prevalensi kebutaan sebesar 1,1% dengan opacity kornea sebesar 31,6% dari kasus yang 79% adalah karena penyebab nontrachomatous seperti ulkus . kornea penelitian ini adalah analisis retrospektif data pasien yang dirawat karena ulkus kornea di rumah sakit Sur Regional wilayah Sharqiya Selatan dari Oktober 2000 sampai 19 November 2006 ini adalah studi pertama
dari jenisnya di wilayah ini. Dalam penelitian ini pria jelas memiliki insiden yang lebih tinggi dari ulkus kornea (64,36%) dibandingkan perempuan. Hal ini sesuai dengan beberapa penelitian yang dilakukan di tempat lain seperti studi madurai oleh Srinivasan et al, 2 dimana rasio laki-laki untuk perempuan adalah 1,6: 1 dan dalam sebuah studi oleh Bashir et al, 5 laki-laki lagi didominasi. Hal ini dapat dijelaskan oleh fakta bahwa mereka lebih terlibat dalam pekerjaan luar ruangan dan karenanya terkena keadaan yang tidak menguntungkan seperti paparan sinar UV terutama dengan petani dan nelayan, trauma di agriculturists dan tanggal pemetik, pekerja kasar dan sebagainya, yang menyebabkan ulserasi kornea. Dalam sebuah studi oleh Upadhyay et laki-laki dan perempuan al.6 ditemukan sama-sama terpengaruh. Berkaitan dengan usia dalam penelitian kami, sebagian besar (64,36%) dari mereka lebih dari 60 tahun. Studi Madurai juga menyimpulkan hal yang sama .2 Pada pasien penelitian kami di atas 60 tahun memiliki banyak predisposisi faktor-faktor seperti CDK, kekeringan, operasi katarak, pasien glaukoma pada obat-obatan, dan kelainan bentuk tutup karena jaringan parut trachomatous yang mungkin cenderung kelompok usia ini ulserasi kornea lebih dari kelompok usia lainnya. Dalam sebuah studi oleh Laspina et al, 7 ditemukan bahwa frekuensi terbesar adalah pada kelompok usia 30-59 tahun, sedangkan pada pasien penelitian kami antara 30-60 tahun menyumbang 23% dari kasus. Ketika tingkat keparahan ulkus pada presentasi dianggap, ditemukan bahwa memutuskan borok yang sedikit lebih tinggi (36,17%) dibandingkan dengan sedang (29.25%) dan ulkus ringan (34,37%). Dengan demikian, ulkus kornea terjadi hampir pada frekuensi yang sama sejauh keparahan khawatir. Dalam sebuah studi oleh Mcleod et al.4 terlihat bahwa 33 ulkus (44,59%) yang moderat dan 41 (65,41%) yang parah menunjukkan bahwa ulkus parah lebih sering terlihat dari ulkus moderat, meskipun cara keparahan diklasifikasikan tidak jelas. Peningkatan marginal dalam ulkus parah dalam studi kami adalah sebagian karena insiden yang lebih tinggi dari ulkus kornea pseudomonas (53,84%)
dibandingkan dengan jenis lain dari mikroba yang diketahui menyebabkan ulkus parah dan progresif cepat. Dimana ketajaman visual dapat terekam pada presentasi, ditemukan bahwa sekitar 65% dari mereka memiliki ketajaman visual kurang dari 3/60. Masyarakat miskin VA bisa disebabkan oleh ulkus itu sendiri atau faktor predisposisi seperti kornea degenerasi / opacity atau karena katarak. 22.87% tidak persepsi cahaya pada presentasi. Tidak Penelitian sejauh ini telah disebutkan Visual ketajaman pada presentasi. Arti penting dari temuan ini sulit untuk mencari tahu. Pasien yang buta terlihat pada seperempat pasien kami yang cenderung menderita satu jenis cedera atau yang lain, atau mungkin memiliki faktor predisposisi seperti kornea degenerasi / opacity kornea atau edema kornea karena glaukoma absolut. 43.18% dari semua kasus menunjukkan baik jamur / bakteri dalam penelitian kami sementara sisanya tidak menunjukkan isolat. Pada 5% kasus jamur yang tumbuh dalam kultur. Dalam sebuah studi oleh Srinivasan et al.2 68,4% menunjukkan kultur positif. Bashir et al.5 menunjukkan hasil bakteri dari 40% hampir mirip dengan penelitian kami. pertumbuhan jamur ditemukan pada 12,5% kasus di bashers studi, 5 dan 46,8% di madurai study.2 Rendahnya hasil jamur dalam kasus kami itu mungkin karena fakta bahwa kasus trauma yang mengarah ke ulkus kornea yang kecil jumlahnya (5.85 %) sedangkan dalam penelitian madurai itu dari urutan 65,4%. Isolat bakteri, 53,84% adalah pseudomonas. Dalam studi Madurai, 2 isolat yang paling umum adalah Streptococcus pneumoniae dan penulis telah dikaitkan ke sejumlah besar dakriosistitis kronis yang terlihat di ruang kerjanya di mana pneumokokus adalah isolat utama. Dalam penelitian kami, pneumokokus merupakan 18,46% dari kasus. Dalam beberapa penelitian lain, 5,6 pneumokokus adalah isolat yang paling umum. Dalam sebuah studi oleh Laspina et.al, 7 coagulase staphylococcus negatif adalah isolat yang paling umum. Alasan untuk variasi dapat dijelaskan mungkin karena kondisi yang berbeda iklim, standar sosial ekonomi, kultur dan pekerjaan yang terlihat di daerah-daerah geografis. Dalam penelitian kami tidak
ada pasien yang dakriosistitis sementara kasus dengan kekeruhan kornea dan degenerasi terlihat lebih sering. Dalam studi Madurai, pseudomonas terlihat pada 14,4% dari isolat. Laspina et al, 6 juga menunjukkan 14% dari isolat menjadi pseudomonas. Dalam sebuah studi oleh Leck et al, 8 pseudomonas ditemukan isolat utama antara ulkus bakteri di Ghana dan di India Selatan di mana teknik yang sama untuk isolasi digunakan. Dalam penelitian yang sama bakteri utama adalah spesies streptokokus dan penulis telah menghubungkannya dengan perubahan flora bakteri dalam wilayah geografis yang dipengaruhi oleh iklim dan lingkungan. Mayoritas pasien kami yang memulai terapi empiris berada di Sefuroksim turun (68,61%) dan gentamisin diperkaya (83,5%). Sefalosporin lain seperti ceftriaxone, ceftazidime diberikan jika kultur / sensitivitas menunjukkan mereka untuk menjadi efektif terhadap organisme terisolasi dan terapi empiris tidak membantu. Salep asam Fucidic diberikan pada 27.12% dari pasien untuk menutupi waktu tidur dalam beberapa kasus. Monoterapi dengan ofloksasin dimulai pada 11,17% kasus. Dalam sebuah penelitian yang diterbitkan dalam oftalmologi (tidak ada penulis yang terdaftar), 9 ditemukan bahwa pengobatan dengan gentamisin diperkaya dan cefuroxime menunjukkan respon sama baik bila dibandingkan dengan tetes ofloxcin dan disarankan monoterapi kurang beracun. Dalam penelitian kami, monoterapi kurang berhasil daripada terapi ganda karena banyak pasien dengan monoterapi harus beralih ke terapi ganda dalam pengobatan. Ini mungkin karena dari berbagai pola sensitivitas di dua daerah yang diuji. Dalam sebuah studi oleh McLeod et terapi ganda (4) ditemukan efektif dalam mengobati ulkus kornea bakteri. Gentamycin golongan kedua dan sefalosporin generasi ketiga mencakup spektrum yang luas dari bakteri dan dengan demikian ditemukan untuk menjadi sukses sebagai terapi empiris. Fluoroquinolines (Oflox dan Ciprofloxacin) tidak begitu efektif terhadap spesies streptokokus dan meningkatkan resistensi tercatat akhir-akhir ini terhadap antibiotik sehingga tidak mungkin obat yang cocok untuk digunakan dalam terapi empiris.
Dengan terapi di atas ditemukan bahwa sekitar 60% dari pasien yang diperlukan kurang dari 3 minggu untuk pulih sedangkan sisanya mengambil lebih banyak waktu untuk pulih. Dalam satu studi (tidak ada penulis yang terdaftar), 9 terlihat bahwa 67,9% pada terapi ganda sembuh dalam waktu 14 hari pengobatan. Hasil antara dua studi hampir sebanding. Mengenai panjang rawat inap, ditemukan bahwa 88% dari pasien habis dalam waktu kurang dari 2 minggu di antaranya lebih dari 50% dipulangkan dalam 1 minggu menunjukkan bahwa pasien dipulangkan banyak sebelum ulkus mereka sembuh sehingga mengurangi biaya rawat inap. Di antara pasien yang diobati sekitar 80% menunjukkan pemulihan penuh (69,14%) atau peningkatan setelah pengobatan sementara beberapa memburuk (4,78%) dan beberapa dari mereka meninggalkan melawan nasihat medis menunjukkan bahwa baris kami pengobatan cukup dapat diterima. Hal ini sesuai dengan penelitian yang dilakukan oleh (tidak ada penulis yang terdaftar), 8 dimana obat terjadi di lebih dari 60% kasus dalam dua kelompok di kedua ganda / monoterapi. Dalam berbagai penelitian (2, 3, 6 ) trauma merupakan faktor predisposisi utama, pada saat trauma penelitian kami terlihat pada 5,85% pasien, perbedaan yang mencolok. Ini, juga, menjelaskan insiden rendah ulkus jamur (10.63%) dalam penelitian
kami. Jumlah pasien dengan lensa h / o Kontak (CL)
juga diabaikan (2%), dibandingkan dengan studi oleh Ly CN et al.10 mana 36% memberikan h / o CL menggunakan dan Keay et al.11 menunjukkan 33,7% memberikan h / o menggunakan CL. Insiden rendah dalam studi kami adalah karena fakta bahwa mayoritas dari mereka lebih dari 60 tahun dan berasal dari daerah pedesaan. Dalam sebuah studi oleh Basak et al.12 jumlah pengguna CL yang diabaikan (4/1198 pasien) karena kebanyakan
pasiennya adalah petani dari daerah pedesaan. Operasi intraokular terlihat pada 24% kasus dan ini hanya bisa menjadi faktor risiko dianggap sebagai kornea mungkin lebih rentan untuk ulserasi dari biasanya ketika mereka berada di steroid selama lebih dari sebulan. ini dapat mempengaruhi kornea terhadap invasi oleh bakteri / jamur karena menurunkan resistensi lokal dan beberapa kehadiran batas jahitan untuk waktu yang lama, yang dapat terakumulasi lendir dan mempengaruhi kornea untuk ulserasi. Basak et al, 12 telah menemukan hanya beberapa kasus yang posting bedah (8 dari 1.198 pasien).Faktor risiko lain seperti trichiasis, degenerasi kornea, blepharitis, dan proptosis terlihat dalam beberapa kasus. CDK ditemukan pada 15% kasus sedangkan dalam penelitian madurai, 2 itu dilihat di 9 dari 434 pasien. Climate droplets keratopathy ini agaknya disebabkan oleh paparan sinar UV, terutama orang-orang yang bekerja di luar lebih rentan untuk itu. Erosi epitel Sering atas deposito murbei di CDK membuat kornea lebih rentan terhadap ulserasi. Diabetes sebagai faktor predisposisi terlihat di 8,5% kasus dalam penelitian Madurai, 2 dan studi oleh Basak et al.12 (7,6%) juga menunjukkan rendahnya tingkat insiden DM antara pasien dengan ulkus kornea. Perforasi sebagai komplikasi terlihat pada 17% kasus. Entah mereka disajikan kepada kita dengan perforasi (7 dari 15 kasus) atau mereka mengembangkan ini setelah masuk. Tingginya angka kejadian ulkus pseudomonas dalam penelitian ini dapat menjelaskan komplikasi ini di sebagian besar kasus. kesimpulan
Agen etiologi utama dalam studi kami adalah bakteri dengan ulkus jamur membentuk sebagian kecil. Spesies Pseudomonas adalah bakteri utama. Kasus jamur yang sedikit (5%) dalam penelitian kami. Terapi ganda dengan diperkaya gentamisin dan cefuroxime tetes efektif dalam mengobati sebagian besar ulkus kornea.