KENYA FINAL trans · Measuring Transparency to Improve Good Governance in the Public Pharmaceutical...
80
Transcript of KENYA FINAL trans · Measuring Transparency to Improve Good Governance in the Public Pharmaceutical...



WHO/AFR/EDM/EDP/12.04
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector
KENYA

‐‐ ii ‐‐
© World Health Organization. Regional Office for Africa, 2012
Publications of the World Health Organization enjoy copyright protection in accordance with the
provisions of Protocol.2 of the Universal Copyright Convention. All rights reserved.
The designations employed and the presentation of the material in this publication do not imply the
expression of any opinion whatsoever on the part of the World Health Organization concerning the
legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of
its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there
may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are
endorsed or recommended by the World Health Organization in preference to others of a similar
nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are
distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the
information contained in this publication. However, the published material is being distributed
without warranty of any kind, either express or implied. The responsibility for the interpretation and
use of the material lies with the reader. In no event shall the World Health Organization or its
Regional Office for Africa be liable for damages arising from its use.
Printed by the WHO Document Production Services, Geneva, Switzerland

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ iii ‐‐
CONTENTS
ABBREVIATIONS ................................................................................................................................................................ V
KENYA GGM ASSESSMENT TEAM ............................................................................................................................. VI
FOREWORD ........................................................................................................................................................................ VII
EXECUTIVE SUMMARY .................................................................................................................................................... IX
BACKGROUND ...................................................................................................................................................................... ix
METHODOLOGY .................................................................................................................................................................... ix
RESULTS ................................................................................................................................................................................ ix
GENERAL RECOMMENDATIONS ........................................................................................................................................... xi
SPECIFIC RECOMMENDATIONS ............................................................................................................................................ xi
1. INTRODUCTION ..................................................................................................................................................... 1
1.1. BACKGROUND .......................................................................................................................................................... 1
1.2. OVERVIEW OF THE PHARMACEUTICAL SECTOR IN KENYA ................................................................................... 1
1.2.1. Country socio‐economic and health profile ................................................................................................. 1
1.2.2. Pharmaceutical sector profile ....................................................................................................................... 2
1.3. OBJECTIVES ............................................................................................................................................................... 3
2. METHODOLOGY .................................................................................................................................................... 4
2.1. STUDY PERIOD AND AREA ....................................................................................................................................... 4
2.2. NATIONAL ASSESSORS ............................................................................................................................................. 4
2.3. SELECTION OF KEY INFORMANTS ........................................................................................................................... 4
2.4. DATA COLLECTION .................................................................................................................................................. 5
2.5. DATA SCORING AND ANALYSIS .............................................................................................................................. 6
3. RESULTS .................................................................................................................................................................... 6
3.1. REGISTRATION OF MEDICINES ................................................................................................................................. 8
3.2. LICENSING OF PHARMACEUTICAL ESTABLISHMENTS ........................................................................................ 12
3.3. INSPECTION AND MARKET CONTROL OF MEDICINES .......................................................................................... 16
3.4. MEDICINES PROMOTION CONTROL ..................................................................................................................... 19
3.5. CONTROL OF CLINICAL TRIALS ............................................................................................................................ 24
3.6. SELECTION OF MEDICINES .................................................................................................................................... 28
3.7. PROCUREMENT OF MEDICINES ............................................................................................................................. 31
3.8. DISTRIBUTION OF MEDICINES ............................................................................................................................... 35

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ iv ‐‐
4. DISCUSSION ......................................................................................................................................................... 40
4.1. REGISTRATION OF MEDICINES .............................................................................................................................. 40
4.2. LICENSING OF PHARMACEUTICAL ESTABLISHMENTS ......................................................................................... 40
4.3. INSPECTION AND MARKET CONTROL OF MEDICINES .......................................................................................... 41
4.4. MEDICINES PROMOTION CONTROL ..................................................................................................................... 41
4.5. CONTROL OF CLINICAL TRIALS ............................................................................................................................ 42
4.6. SELECTION OF MEDICINES .................................................................................................................................... 43
4.7. PROCUREMENT OF MEDICINES ............................................................................................................................. 43
4.8. DISTRIBUTION OF MEDICINES ............................................................................................................................... 44
5. CONCLUSIONS ..................................................................................................................................................... 45
6. RECOMMENDATIONS ...................................................................................................................................... 48
6.1. GENERAL RECOMMENDATIONS .......................................................................................................................... 48
6.2. SPECIFIC RECOMMENDATIONS ............................................................................................................................ 48
6.2.1. Registration of medicines .......................................................................................................................... 48
6.2.2. Licensing of pharmaceutical establishments ............................................................................................ 48
6.2.3. Inspection and market control of medicines ............................................................................................. 49
6.2.4. Medicines promotion control .................................................................................................................... 49
6.2.5. Control of clinical trials ............................................................................................................................ 50
6.2.6. Selection of medicines ............................................................................................................................... 50
6.2.7. Procurement of medicines ......................................................................................................................... 51
6.2.8. Distribution of medicines ......................................................................................................................... 51
7. GLOSSARY ............................................................................................................................................................. 52
8. REFERENCES ......................................................................................................................................................... 54
9. ANNEXES ................................................................................................................................................................ 55
ANNEX 1: SCORE SHEETS ............................................................................................................................................... 56
ANNEX 2: LIST OF DOCUMENTARY EVIDENCE OBTAINED ............................................................................. 65
ANNEX 3: ORGANIZATIONAL STRUCTURE OF THE PHARMACY AND POISONS BOARD .................. 66
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ v ‐‐
ABBREVIATIONS
AIDS Acquired Immunodeficiency Syndrome
CCT Committee for Clinical Trials
CDR Committee for Drug Registration
CMS Central Medical Stores
COI Conflict of Interest
EML Essential Medicines List
ERC Ethics and Research Committee
GCP Good Clinical Practices
GDP Good Distribution Practices
GGM Good Governance for Medicines
GMP Good Manufacturing Practices
HIV Human Immunodeficiency Virus
IEC Independent Ethics Committee
INN International Nonproprietary Name
KEMRI Kenya Medical Research Institute
KEMSA Kenya Medical Supplies Agency
KI Key Informant
KNDP Kenya National Drug Policy (1994)
KNH Kenyatta National Hospital
KNPP Kenya National Pharmaceutical Policy (2007)
MDGs Millennium Development Goals
MEDS Mission for Essential Drugs and Supplies
MoH Ministry of Health
MOMS Ministry of Medical Services
MRA Medicines Regulatory Authority
NCST National Council of Science and Technology
NGO Nongovernmental Organization
NHSSP National Health Sector Strategic Plan
NMTC National Medicines and Therapeutics Committee
NQCL National Quality Control Laboratory for Drugs and Medical Devices
PPB Pharmacy and Poisons Board
PPOA Public Procurement and Oversight Authority
QA Quality Assurance
SOP Standard Operating Procedure
TB Tuberculosis
TOR Terms of Reference
UoN University of Nairobi
WHO World Health Organization
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ vi ‐‐
KENYA GGM ASSESSMENT TEAM
COORDINATORS
Fred Siyoi Deputy Chief Pharmacist/Deputy Registrar, MOMS
Njeri Mucheru Deputy Chief Pharmacist, Division of Pharmaceutical Policy, MOMS
Regina Mbindyo National Medicines Adviser, World Health Organization, Kenya
NATIONAL ASSESSORS
Grace N. Thoithi Dean, School of Pharmacy, University of Nairobi
James Mwenda Customer Services Manager, Mission for Essential Drugs & Supplies (MEDS)

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ vii ‐‐
FOREWORD
This report is a national assessment of transparency and potential vulnerability to corruption and
unethical practices in eight key pharmaceutical system functions in Kenya, namely: medicines
registration, licensing, inspection, promotion, clinical trials, selection, procurement and distribution.
It was conducted using an assessment tool and model framework developed by the World Health
Organization, which focuses on structures and mechanisms to prevent unethical practices in decision‐
making in the public pharmaceutical sector.
Kenya is in the process of implementing its development blueprint ‐ Vision 2030 – which is anchored
on economic, social and political pillars, some key aspects being governance reforms as well as
public sector reforms. In this regard, the Government continues to intensify efforts to bring about an
attitudinal change in public service that values transparency and accountability to the citizens of
Kenya. Health sector reform is in progress under the National Health Sector Strategic Plan (NHSSP
II) and mechanisms for health sector governance and coordination are actively being strengthened.
To guide the much‐needed reforms in the pharmaceutical sector, the Government has developed the
Kenya National Pharmaceutical Policy (KNPP) which enshrines ‘good governance’ as one of its core
principles. The Pharmaceutical Strategy will provide a framework for coordinated planning,
monitoring and evaluation.
Promoting good governance in the pharmaceutical sector requires a long‐term strategy through
which best practices and evidence‐based decision‐making are actively assimilated into
pharmaceutical systems. To achieve significant impact, efforts to address corruption must include the
application of two basic strategies: i) discipline‐based strategy – establishing comprehensive laws
and regulations with adequate sanctions for non‐compliance; and ii) values‐based strategy – building
institutional integrity through the promotion of moral values and ethical principles. This assessment
is therefore timely, and the findings and recommendations will inform strategies for entrenching
transparency and best practices in all aspects of pharmaceutical services.
I wish to gratefully acknowledge the efforts of the national assessors and coordinators who were
involved in all technical aspects of this assessment; and to the key informants who readily provided
the information analysed in this report. In addition, we acknowledge the technical support from
WHO, which enabled the necessary training of national assessors, adaptation of the tools and
development of the assessment report.
It is my sincere hope this report promotes awareness among health stakeholders and the general
public on the basic components necessary for promoting good governance in the management of the
national pharmaceutical system. I urge all stakeholders to participate in defining and supporting
strategies for sustaining good governance in the pharmaceutical system.
____________________________
Dr Francis Kimani
Director of Medical Services

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ viii ‐‐

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ ix ‐‐
EXECUTIVE SUMMARY
Background
A study was undertaken in Kenya to collect the perceptions of pharmaceutical policy‐makers and
other stakeholders on the transparency and vulnerability to corruption in the pharmaceutical sector.
It covered procedures and structures for medicines registration, licensing of pharmaceutical
establishments, medicines inspection and market control, medicines promotion control, control of
clinical trials, medicines selection, procurement and distribution. The findings will be used in the
development of a national good governance for medicines (GGM) framework and in the
implementation of a national GGM programme.
Methodology
Two trained national assessors carried out the study between May and July 2008 using a
standardized World Health Organization (WHO) assessment tool. A total of 113 key informants (KIs)
were interviewed. Interviewees were from the Medicines Regulatory Authority (MRA) (Pharmacy
and Poisons Board (PPB)), Government procurement and distribution department, other
Government ministries, universities, community pharmacies, the private pharmaceutical industry,
national and international nongovernmental organizations (NGOs), media and legal institutions. The
quantitative indicators used were scored and a rating system was used to represent the degrees of
vulnerability to corruption.
Results
Registration of medicines: The average final score for registration was 4.36, indicating moderate
vulnerability to corruption. The requirements for applicants are fairly well documented, including a
standard application form for submission of applications for registration, guidelines on how to
submit the application and a list of registered medicines. There is a committee which meets regularly
to assess applications, and applicants who have their applications rejected by the committee can
make formal appeals to the PPB. However, there are no written guidelines on selection criteria for
members of this committee, on the committee’s composition and terms of reference, procedures on
how to assess applications, how and where medicines registration officers meet with applicants and
on conflict of interest (COI) with regard to registration activities.
Licensing of pharmaceutical establishments: The average final score for licensing was 5.21,
indicating moderate vulnerability to corruption. There is provision in the law for licensing of
pharmaceutical establishments and the MRA has a unit and a committee for licensing activities.
There are written procedures on how to submit applications for licensing and how to assess
applications. Although a pre‐licensing inspection report is required before issuing a licence, post‐
licensing inspection of establishments is not regular. There is a list of licensed pharmaceutical
establishments, but it is neither comprehensive nor up‐to‐date. There are no written guidelines on
selection criteria for members of the committee for licensing or on its composition and terms of
reference. There is no independent appeals system for applicants who have their applications for
licensing rejected.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ x ‐‐
Inspection and market control of medicines: Inspection and market control of medicines is very
vulnerable to corruption, having an average final score of 3.95. There is comprehensive provision in
the medicines legislation covering inspection of pharmaceutical establishments and written standard
operating procedures (SOPs) for conducting inspections. There are written guidelines for Good
Manufacturing Practices (GMP) and also for Good Distribution Practices (GDP) for pharmaceutical
products in Kenya, but these guidelines do not classify non‐compliance with GMP or GDP. No
written criteria for selection and recruitment of inspectors and no guidelines on COI exist. Written
procedures to prevent regulatory capture between inspectors and the manufacturing and
distributing companies inspected are also non‐existent.
Drug promotion control: The average final score for licensing was 4.53, indicating moderate
vulnerability to corruption. There is provision within the pharmacy legislation covering promotion
and advertising of medicines, with clear penalties for anyone who breaches the law. Pre‐approval of
promotional material is required and there is a promotions service that vets medicines promotion
advertisements, but monitoring and enforcing the provisions on this promotion are very weak. SOPs
for the service for medicines promotion are being developed. However, there are no written
guidelines on selection criteria for members of the promotion service unit, nor on the composition
and terms of reference of the committee. There are no written procedures to report unethical
promotional practices and none for COI.
Control of clinical trials: The average final score for control of clinical trials was 6.25 which indicates
marginal vulnerability to corruption. There is provision for the regulation of clinical trials in the
Science and Technology Act. The PPB has a committee which is responsible for reviewing
applications and it also has requirements for the manufacture, importation, exportation and use of
investigational products. There are guidelines on the submission of applications to the PPB to
conduct clinical trials and to the various institutional ethics and research committees. There is no
system for inspection of clinical trials and no written guidelines on selection criteria for members of
the PPB and Ethics and Research Committees (ERCs) nor on COI. There are no national guidelines on
principles of Good Clinical Practice and none for the establishment of an independent ethics
committee.
Selection of medicines: Selection of medicines had the lowest average final score of 2.95, showing that
this function is very vulnerable to corruption. The essential medicines list (EML) is in line with WHO
procedures, but it was last updated in 2002. There are no written criteria for the selection process for
including or deleting medicines from the national EML. A National Medicines and Therapeutics
Committee (NMTC) was constituted in 2007, but it is not yet operational. There are clear criteria for
the selection of NMTC members, and terms of reference describing the role and responsibilities of
the NMTC have been developed, but most stakeholders are not aware of their existence. There are no
written guidelines on COI and the NMTC has no SOPs for their decision‐making.
Procurement of medicines: The average final score for procurement of medicines was 7.01, which
indicates marginal vulnerability to corruption. Transparent and explicit procedures for procurement
exist and are heavily informed by the Public Procurement and Disposal Act. A description of the
internal procedures to be followed by procurement staff when processing bids is available to the
staff. The Procurement Office monitors supplier performance for compliance with the contract terms
and it is also audited on a regular basis. There is a Tender Committee whose functions are clearly
separated from the functions of the Procurement Office. There is a formal appeals process for

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ xi ‐‐
applicants who have their bids rejected. There are no written guidelines on COI with regard to the
procurement of medicines.
Distribution of medicines: Distribution of medicines had the highest of all scores, 7.82, indicating
marginal vulnerability to corruption. All procured commodities are delivered from the suppliers
directly to the central warehouses where they are verified. Most medicines carry a Government
identification inscription on both the primary and secondary packaging. A “master map” showing
the location of medicines does not exist, but products are arranged taking into account their expiry
dates. A security management system, procedure for requesting medicines, SOPs for stock
management, computerized and manual information systems, a monitoring and evaluation system,
and a communication system between distributions points are all in place. The warehouses are
subject to regular internal and external auditing. Sanctions to be imposed on individuals for theft or
corrupt practices are set out in the Public Procurement Act.
General recommendations
1. Create a formal appeals system in each function.
2. Improve communication between all players in the pharmaceutical sector: the Ministry, the
PPB and the pharmaceutical industry.
3. Regularly update and publicize all documents and improve data management systems to
provide instant information.
4. Build the human resource capacity in each of the functions.
5. Institutionalize the declaration of COI for all activities.
Specific recommendations
Registration: The development of guidelines for the selection of committees and decision‐making
processes, control of the number of registered products, pre‐registration analysis of all medicines and
sharing of information between drug registration, inspection and importation departments within
the PPB should be embarked on.
Licensing: A review of the Food and Chemical Substances Act (Cap 254), enforcement of annual
renewal of licences, and guidelines for selection and the decision‐making processes of the licensing
committees are required.
Inspection and market control: There is a need to develop documents for selecting and guiding the
decisions of committee members and inspectors, to have regular schedules of inspections, to enforce
the law, and to improve information sharing between the drug registration, pharmacovigilance and
inspection departments within the PPB.
Drug promotion control: The law should be enforced and amended to include control of
complementary medicines’ promotion. Guidelines and SOPs should be strengthened and public
awareness on the regulation of promotion of medicines should be created.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ xii ‐‐
Control of clinical trials: There is a need to review legislation and enforce it, to develop all the
necessary documents, increase the capacity of reviewers, establish an inspection system and improve
interaction between researchers, the National Council of Science and Technology (NCST), ERCs, the
Ministry of Medical Services and the PPB.
Selection: The selection process should be publicized, the NMTC should be operationalized and
documentation on the selection process should be developed.
Procurement: Procurement of all medicines should be done centrally by the Kenya Medical Supply
Agency (KEMSA), the procurement function should be independent and the Public Procurement and
Oversight Authority (PPOA) should be operationalized.
Distribution: A performance monitoring system for the supply chain should be set up, GDP enforced
and regional depots strengthened.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 1 ‐‐
1. INTRODUCTION
1.1. Background
Medicines complement other types of health‐care services in reducing morbidity and
mortality rates and enhancing the quality of life. Therefore, access to health‐care and
essential medicines is increasingly being viewed as a fundamental human right1. The ability
of medicines to save lives, reduce suffering and improve health depends on their being of
good quality, safe, available, affordable and properly used. In many countries these
conditions are far from being met and it is estimated that today almost two billion people
(one third of the global population) do not have regular access to essential medicines. In
some of the lowest‐income countries in Africa and Asia more than half of the population has
no regular access. Furthermore, one third of countries have either no regulatory authority or
only limited capacity to regulate the medicines market. Unreliable supply systems persist,
and irrational use of medicines is a major problem worldwide2.
Poverty, market failures and Government failures, among others, contribute to these urgent
challenges in the pharmaceutical sector. The latter often results, at least in part, from a lack
of transparency in the pharmaceutical system, which is one of the possible reasons for the
medicines gap described above. Lack of transparency in the pharmaceutical system is
increasingly becoming an issue of concern because bad practices can waste resources, which
in turn reduces the availability of essential medicines and so threatens the well‐being of
populations.
1.2. Overview of the pharmaceutical sector in Kenya
1.2.1. Country socio-economic and health profile
Kenya’s population stands at about 34 million people (2005 census), 56% of which lives
below the poverty line and depends on less than US$ 1 per day. Substantial resource inputs
to the health sector by the Government and development partners have resulted in specific
gains and various improvements, however, some key health indicators have been on the
decline and a significant number of Kenyans cannot reliably access the medicines they need3.
Malaria, HIV/AIDS, tuberculosis (TB), diarrhoea and respiratory diseases are the main
threats to health. An estimated 1.5 million Kenyans are living with HIV/AIDS. Malaria is the
main contributor to morbidity and mortality in Kenya, causing 34,000 deaths annually in
children below 5 years of age. Medicines, medical devices and diagnostics to manage these
and other diseases are expensive, and present great challenges for access, monitoring and
regulation. This has put a significant demand on the health system in general and
specifically on the pharmaceutical sector.
The public health‐care system remains the major provider of health services, accounting for
58% of health facilities, 52% of hospital beds and 70% of health personnel. The private for‐
profit sector and the private not‐for‐profit providers complement the public sector health
services3.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 2 ‐‐
Public financing of the health sector through the Exchequer is about US$ 6.2 per capita, or
5% of Gross Domestic Product4, which falls below the WHO recommended level of US$ 34
per capita5 and far short of the Government’s commitment to spend 15% of the national
budget on health, as agreed in the Abuja Declarations (2001 and 2006)6. This under‐funding
has reduced the sector’s ability to ensure an adequate level of service provision to the
population, and has led to significant out‐of‐pocket payments, thus contributing to inequity
in access to health care for poor and disadvantaged groups. These factors put Kenya at risk
of not achieving the Millennium Development Goals (MDGs). Kenya’s Health Policy
Framework (1994)7 outlines health sector reforms, among them strengthening the policy role
of the central Ministry of Health (MoH); decentralization and capacity strengthening of
provincial and district levels; reorientation, retraining and redeployment of health human
resources; and adoption and implementation of the Kenya National Drug Policy (1994)8 as
the guide for legislative reforms, staff development and management improvements in
pharmaceutical services3.
1.2.2. Pharmaceutical sector profile
The growth of the Kenyan population from about 27 million in 1994 when the KNDP was
adopted to about 34 million (2005), coupled with the ongoing burden of HIV, TB and
malaria have created a lot of pressure on the health system. Although the number of public
and private health facilities has also increased, the health system remains overburdened,
and the pharmaceutical sector has experienced the same challenges affecting the health
sector generally. Public sector pharmaceutical services are provided by the MoH through the
Department of Pharmacy, headed by the Chief Pharmacist who is also the Registrar of the
MRA, PPB. The Government has established the Kenya Medicines Supply Agency (KEMSA)
for pharmaceutical supply and the National Quality Control Laboratory (NQCL) for analysis
of medicines. However, the current MoH structure and the dual roles of some MoH officers
are not conducive to effective pharmaceutical sub‐sector management and do not facilitate
effective delivery of services.
The ratio of pharmaceutical personnel (pharmacists and pharmaceutical technologists) to the
population is insufficient, with approximately 1 to 10,000 (Table 1)3. Moreover, these
personnel are inequitably distributed across the country, with the majority concentrated in
the private sector and in urban areas, and there are notable skills gaps in key areas, such as
management, procurement and supply. As a result, the quality of pharmaceutical services is
compromised.
The Government and its bilateral partners contribute significantly to health sector
strengthening and financing but currently this is insufficient to ensure equitable access to
essential medicines for all Kenyans. Factors such as national debt, inflation, economic
growth, unpredictable donor support and lack of required budget‐planning information
make concrete budget projections difficult. This contributes to major gaps in funding and
consequently, access to medicines and resources for the pharmaceutical sector and
medicines supply remain grossly inadequate.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 3 ‐‐
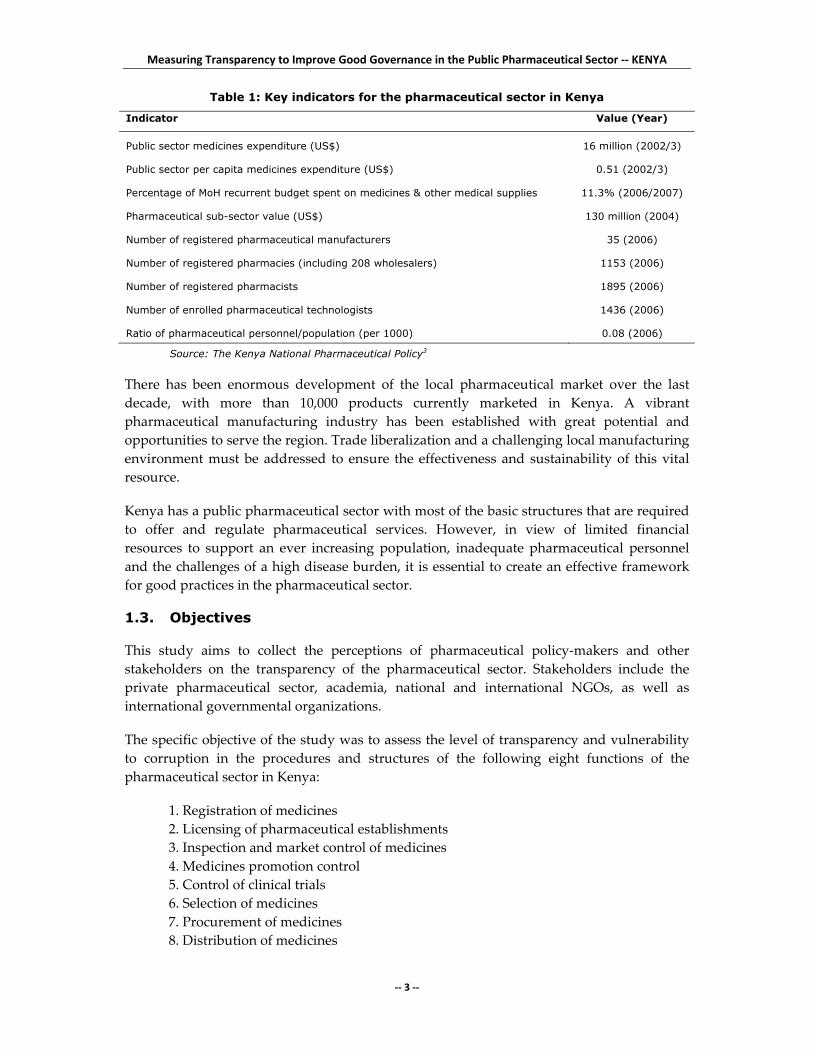
Table 1: Key indicators for the pharmaceutical sector in Kenya
Indicator Value (Year)
Public sector medicines expenditure (US$) 16 million (2002/3)
Public sector per capita medicines expenditure (US$) 0.51 (2002/3)
Percentage of MoH recurrent budget spent on medicines & other medical supplies 11.3% (2006/2007)
Pharmaceutical sub-sector value (US$) 130 million (2004)
Number of registered pharmaceutical manufacturers 35 (2006)
Number of registered pharmacies (including 208 wholesalers) 1153 (2006)
Number of registered pharmacists 1895 (2006)
Number of enrolled pharmaceutical technologists 1436 (2006)
Ratio of pharmaceutical personnel/population (per 1000) 0.08 (2006)
Source: The Kenya National Pharmaceutical Policy3
There has been enormous development of the local pharmaceutical market over the last
decade, with more than 10,000 products currently marketed in Kenya. A vibrant
pharmaceutical manufacturing industry has been established with great potential and
opportunities to serve the region. Trade liberalization and a challenging local manufacturing
environment must be addressed to ensure the effectiveness and sustainability of this vital
resource.
Kenya has a public pharmaceutical sector with most of the basic structures that are required
to offer and regulate pharmaceutical services. However, in view of limited financial
resources to support an ever increasing population, inadequate pharmaceutical personnel
and the challenges of a high disease burden, it is essential to create an effective framework
for good practices in the pharmaceutical sector.
1.3. Objectives
This study aims to collect the perceptions of pharmaceutical policy‐makers and other
stakeholders on the transparency of the pharmaceutical sector. Stakeholders include the
private pharmaceutical sector, academia, national and international NGOs, as well as
international governmental organizations.
The specific objective of the study was to assess the level of transparency and vulnerability
to corruption in the procedures and structures of the following eight functions of the
pharmaceutical sector in Kenya:
1. Registration of medicines
2. Licensing of pharmaceutical establishments
3. Inspection and market control of medicines
4. Medicines promotion control
5. Control of clinical trials
6. Selection of medicines
7. Procurement of medicines
8. Distribution of medicines

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 4 ‐‐
The findings of the study will be used in the development of a national good governance for
medicines (GGM) framework and in the implementation of a national GGM programme.
2. METHODOLOGY
2.1. Study period and area
The study was carried out between May and July 2008. Most of the KIs interviewed were
from Kenya’s capital city, Nairobi, where the regulators and policy‐makers are and where
most of the activities take place. However, to corroborate the information obtained, some
KIs from other parts of the country were interviewed, especially with respect to
procurement and distribution of medicines.
2.2. National assessors
The two national assessors who carried out the study were trained for three days on the
GGM programme and on how to conduct the study. The training took place in Lusaka,
Zambia, on 8‐10 April 2008. The assessors co‐opted one co‐assessor to help in data collection,
whom they trained on the use of the assessment tools.
2.3. Selection of key informants
For each of the eight pharmaceutical functions studied, 13‐15 KIs were interviewed to give a
total of 114 informants. Their selection was carefully made based on knowledge and level of
involvement in the pharmaceutical sector. The KIs were a mix of senior‐, middle‐ and junior‐
level pharmaceutical sector personnel and they represented various institutions, such as the
MRA, the Government procurement and distribution departments, Government ministries,
universities, private community pharmacies (chemists), the private pharmaceutical industry,
and national and international NGOs. In addition, some KIs from other sectors, such as
finance, media and legal (lawyers) were also interviewed.
Table 2 shows the distribution of KIs for each of the pharmaceutical functions studied
among the different sectors.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 5 ‐‐
Table 2: Affiliation of key informants interviewed for each pharmaceutical function
Registration Licensing Inspection Promotion Clinical trials
Selection Procurement Distribution
Government
PPB Dirs - 1 - 2 - 1 - -
PPB Depts 7 1 5 2 1 - - -
MoH 1 - 1 - 1 7 a 2 1
NQCL - - 3 - - - 2 -
KEMSA - - - - - - 4 6
Hospital - - - - - 5 3 2
Private
Chemist 1 3 1 2 - - - -
Industry 2 2 - 6 2 - 1 1
Consultant - - 1 - 1 - - -
NGO (Int) - - - 1 - - 1 1
NGO - - 2 1 - - 1 2
Other
Academia 3 b 6 c 1 1 8d 2 - -
Lawyer - - - - 1 - - -
Media - - - - 1 - - -
KEMRI - - 1 - - - - -
Total 14 13 15 15 15 15 14 13
a: Three people were from MoH Pharmacy Department, two were from the MoH Malaria Division and two from the HIV/AIDS Division. b: All were members of the PPB Committee on Drug Registration. c: Four of these people own chemists. d: Four were researchers in clinical trials, three were members of an institutional ethics and research committee, while one was a member of the PPB committee for clinical trials. Int: International. KEMRI: Kenya Medical Research Institute. KEMSA: Kenya Medical Supplies Agency. MoH: Ministry of Health. NGO: Nongovernmental Organization. NQCL: National Quality Control Laboratory. PPB Dirs: Pharmacy and Poisons Board of Directors. PPB Dept: Pharmacy and Poisons Technical Departments.
2.4. Data collection
To collect information, the national assessors used a set of structured questionnaires that
were developed by WHO’s GGM programme for assessment of each of the eight
pharmaceutical functions. KIs were interviewed at a place of their choice, which in most
cases was in their offices. The assessors assured the KIs of the confidentiality of the
information given. Four methods were used to determine the level of transparency. Only
Methods 1 and 2 were used to score the vulnerability to corruption for each function.
Method 3 allowed the perception of the KI to be compared with the existing procedures and
structures, while Method 4 questions were open‐ended to capture additional information.
To validate and support the information obtained through the questionnaires, the assessors
collected supporting documents from the informants (Annex 2).

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 6 ‐‐
2.5. Data scoring and analysis
Only answers to Method 1 and Method 2 questions were included in the scores. For both
Method 1 and 2 questions, each indicator required a “yes” or “no” response from the KIs,
determining the presence or absence of the existing practice at the Department of Health.
For Method 1, which required a binary answer (yes/no, a “yes” answer was given a value of
“1”, only if there was evidence of a supporting document. A “no” answer was given a value
of “0” irrespective of whether a supporting document was available or not. Method 2
questions had a series of sub‐criteria questions. Each criteria was answered by (yes/no/don’t
know); a “yes” answer was given a value of “1” and a “no” answer was given a value of “0”.
All the “don’t know” answers were considered invalid and were not scored. The overall
score for the question was obtained by dividing the total “yes” answers by the total of valid
answers (yes and no). Each question was scored between 0 and 1. A value of “1” represented
low vulnerability to corruption, while the value of “0” represented high vulnerability to
corruption.
Using Microsoft Excel, the sum of scores for all indicators for each function was then
divided by the number of indicators, and multiplied by 10 to give the final score for each
function on a scale of zero to 10. The 10‐point rating system represented the degrees of
vulnerability to corruption shown in Table 3.
Table 3: Scale of vulnerability to corruption for pharmaceutical functions
3. RESULTS
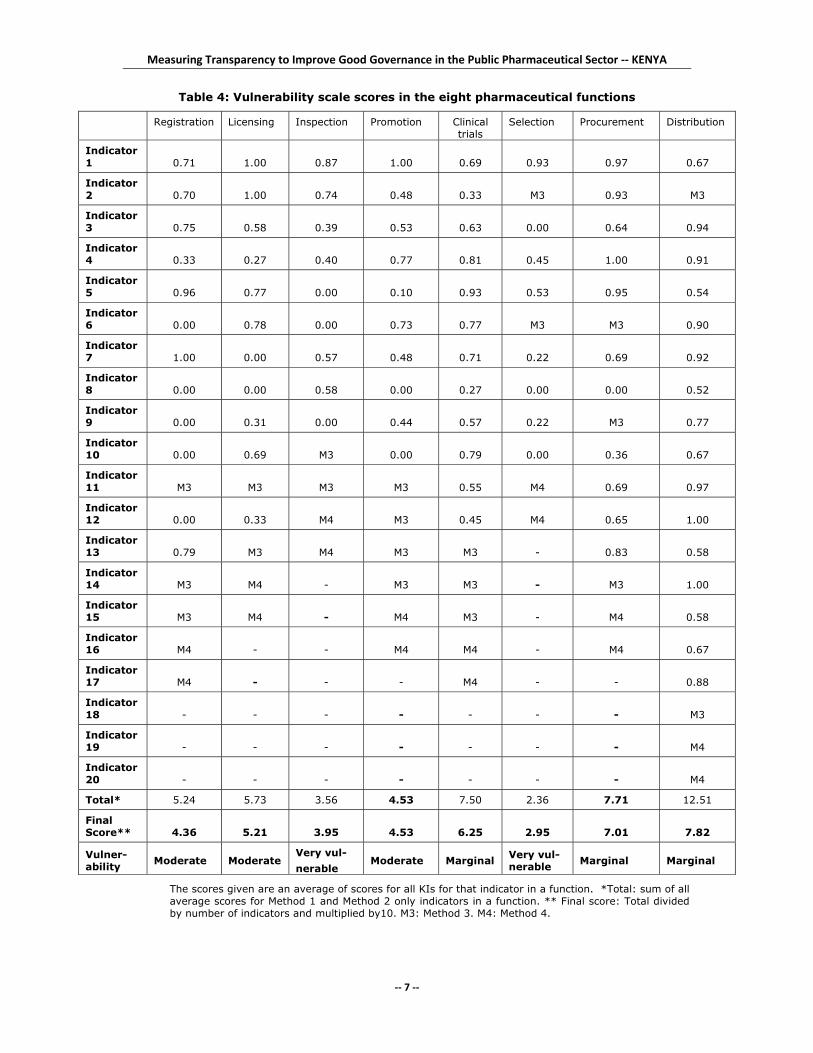
The overall final scores for each function of the assessment are summarized in Table 4.
Selection of medicines was found to be very vulnerable to corruption, while control of
clinical trials, procurement and distribution were only marginally vulnerable. The functions
that were moderately vulnerable were registration of medicines, licensing of pharmaceutical
establishments, inspection and market control, and promotion of medicines.
0.0 – 2.0 2.1 – 4.0 4.1 – 6.0 6.1 – 8.0 8.1 – 10.0
Extremely vulnerable
Very vulnerable
Moderately vulnerable
Marginally vulnerable
Minimally vulnerable
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 7 ‐‐
Table 4: Vulnerability scale scores in the eight pharmaceutical functions
Registration Licensing Inspection Promotion Clinical trials
Selection Procurement Distribution
Indicator 1 0.71 1.00 0.87 1.00 0.69 0.93 0.97 0.67
Indicator 2 0.70 1.00 0.74 0.48 0.33 M3 0.93 M3
Indicator 3 0.75 0.58 0.39 0.53 0.63 0.00 0.64 0.94
Indicator 4 0.33 0.27 0.40 0.77 0.81 0.45 1.00 0.91
Indicator 5 0.96 0.77 0.00 0.10 0.93 0.53 0.95 0.54
Indicator 6 0.00 0.78 0.00 0.73 0.77 M3 M3 0.90
Indicator 7 1.00 0.00 0.57 0.48 0.71 0.22 0.69 0.92
Indicator 8 0.00 0.00 0.58 0.00 0.27 0.00 0.00 0.52
Indicator 9 0.00 0.31 0.00 0.44 0.57 0.22 M3 0.77
Indicator10 0.00 0.69 M3 0.00 0.79 0.00 0.36 0.67
Indicator11 M3 M3 M3 M3 0.55 M4 0.69 0.97
Indicator12 0.00 0.33 M4 M3 0.45 M4 0.65 1.00
Indicator13 0.79 M3 M4 M3 M3 - 0.83 0.58
Indicator14 M3 M4 - M3 M3 - M3 1.00
Indicator15 M3 M4 - M4 M3 - M4 0.58
Indicator16 M4 - - M4 M4 - M4 0.67
Indicator17 M4 - - - M4 - - 0.88
Indicator18 - - - - - - - M3
Indicator19 - - - - - - - M4
Indicator20 - - - - - - - M4
Total* 5.24 5.73 3.56 4.53 7.50 2.36 7.71 12.51
Final Score** 4.36 5.21 3.95 4.53 6.25 2.95 7.01 7.82
Vulner-ability Moderate Moderate
Very vul- nerable
Moderate Marginal Very vul-nerable Marginal Marginal
The scores given are an average of scores for all KIs for that indicator in a function. *Total: sum of all average scores for Method 1 and Method 2 only indicators in a function. ** Final score: Total divided by number of indicators and multiplied by10. M3: Method 3. M4: Method 4.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 8 ‐‐
3.1. Registration of medicines
The Registration Department of the PPB has guidelines for applicants on how to submit an
application for registration of medicinal products, an application form for submission of
applications for registration of medicines and an up‐to‐date list of all registered
pharmaceutical products. There is a Committee for Drug Registration (CDR) that assesses
applications for registration of medicines, but no written evidence of procedures for
assessing applications was found. Appeals can be made to the PPB by applicants who have
their applications rejected.
Indicator I.1: Up-to-date list of all registered pharmaceutical products
Ten of the 14 KIs said there was an up‐to‐date list of pharmaceutical products. Two
Government and two private KIs answered this question in the negative because their
perception was that the list is not up‐to date.
Indicator I.2: Minimum level of information on list of registered pharmaceutical products
The majority of the KIs said that the list includes the name of the product (100% of the KIs),
date of registration (100%), name of the manufacturer (92.9%), country of manufacture
(71.4%) and validity of registration (57.1%). However, fewer of them said that the list
included packaging and identifying marks (28.6%), date of registration (42.9%) and
conditions for registration, such as prescription only or over‐the‐counter (50.0%).
Indicator I.3: Procedures on how to submit applications for registration of medicines
Thirteen of the 14 KIs indicated that there were written procedures on how to submit
applications for registration of medicines. The procedures are written, publicly accessible
and they describe the process to follow in submitting an application. In addition, they
mention the fees to be paid, the data to be submitted and the criteria for registration. All 13
KIs said the procedures make no mention of the time frame for processing. The KI who
indicated that there were no procedures for submitting applications was from the private
sector.
Indicator I.4: Procedures for assessing applications for registration
Five KIs (three CDR members, one from the PPB and one from the private sector) said there
were no procedures for evaluators to assess applications for registration of medicines. Three
(one from the MoH and two from the private sector) did not know if the procedures existed.
One of the KIs (PPB) said only a checklist, and not procedures, existed while five
respondents (all from the PPB) said the procedures existed. These five KIs all said the
procedures were written, described the process to follow in assessing submissions and that
they provided guidance on report writing. However, only one of the five KIs said that the
procedures were publicly accessible and that they mentioned the time frame for processing
the applications.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 9 ‐‐
Indicator I.5: Application form for registration of medicinal products
All KIs agreed that there is a standard application form publicly available for the submission
of applications for registration of medicinal products. More than 95% of them said that the
form is publicly accessible and available at a Government office, that it required descriptions
of the product (brand name and international nonproprietary name (INN)), composition per
unit dose, a summary of the method of manufacture, specifications for the active ingredients
and excipients, a summary of product characteristics (such as pharmacological action,
therapeutic classification, indications, contraindications), packaging materials, inserts and
labelling.
Indicator I.6: Guidelines on how and where medicines registration officers meet with applicants
All KIs responded that there were no guidelines setting limits on how and where medicines
registration officers meet with applicants.
Indicator I.7: Committee for assessing applications for registration of medicines
All respondents indicated that there was a functioning formal committee responsible for
assessing applications for registration of pharmaceutical products.
Indicator I.8: Criteria for selecting the members of the committee
Only two KIs, both from the PPB, said that there were written criteria for selecting the
members of two of the registration committees. However there was no written evidence of
such criteria.
Indicator I.9: Composition and terms of reference of the committee
Only one KI, who was from the PPB, said that there was a written and publicly accessible
document that describes the composition and terms of reference of the committee. There
was no evidence of such a document.
Indicator I.10: Guidelines on conflicts of interest with regard to registration activities
There were no written guidelines on COI and no COI declaration form with regard to
registration activities.
Indicator I.11: Systematic, objective selection of Registration Committee members (see also I.8)
As shown in Table 5 below, one KI strongly agreed, four agreed and another four disagreed
with the statement “the members of the Registration Committee are systemically and
objectively selected based on the written criteria in force in Kenya”. Four respondents said
the question was not applicable and one did not know.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 10 ‐‐
Table 5: Perception of key informants on the selection criteria of Registration Committee members
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 0 2 0 3 1 1 1 8
Private 0 1 0 0 0 2 0 3
Academia 1 0 1 0 1 0 3
Total 0 4 0 4 1 4 1 14
DK: Don’t know, NA: Not applicable
Indicator I.12: Guidelines for the Committee's decision-making process
Three KIs, one from the PPB and two from academia, said there were clear and
comprehensive guidelines for the Committee’s decision‐making process, but there was no
evidence of such documents.
Indicator I.13: Formal appeals system for rejected applications
The majority (78.6%) of the respondents said that there was a formal appeals system for
applicants who had their registration applications rejected and that this involved appealing
to the PPB when the Committee for Drug Registration rejected their applications.
Indicator I.14: Influence of gifts on the final decisions of officials of medicines registration
Table 6 shows that three (23.1%) KIs strongly agreed, two (15.4%) agreed, four (30.8%)
disagreed and 15.4% strongly disagreed with the statement “Gifts and other benefits given
to the officials in charge of medicines registration have no influence at all on their final
decisions”. Two of the respondents were undecided.
Table 6: Perception of key informants on the influence of gifts on the decisions of officials
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 1 1 2 2 2 0 0 8
Private 1 2 0 0 0 0 0 3
Academia 0 1 0 0 1 0 1 3
Total 2 4 2 2 3 0 1 14
DK: Don’t know, NA: Not applicable
Indicator I.15: Frequency of meetings and minutes of the Registration Committee
Ten (71.4%) of the KIs strongly agreed and the remaining four just agreed with the statement
“the Registration Committee meets on a regular basis and keeps minutes of its meetings”.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 11 ‐‐
Indicator I.16: Unethical behaviour in the registration system
Below is a list of what the KIs gave as their perceptions of unethical behaviour common in
the registration area in Kenya:
a. Frequent change of authorized importers and/or agents
b. Substandard drugs: Presence of counterfeit and unregistered medicines in the market
c. Many products are registered without undergoing analysis
d. Data submitted: Incomplete stability protocols and data; plagiarism of data from
innovator products by applicants of generic products; and infringement of patent
rights by some applicants using similar names/presentation of their products as
existing products
e. Influence of registration officers: Officers are influenced by applicants by being given
dinners and gifts, there is lobbying by applicants to have registration of their
products fast‐tracked; some products are registered without going through
evaluation; and some registration officers have obvious vested interest in registration
of certain products
f. Disappearance of registration dossiers from the secretariat
g. In some cases the PPB overrules expert decisions of the Registration Committee
without any good explanation.
Indicator I.17: Actions to improve the medicines registration process
Below is a list of suggestions by KIs on how to improve the medicines registration process:
a. Make the PPB autonomous.
b. Establish a clear appeals system for applicants whose applications for medicines
registration have been rejected.
c. Limit the number of generics that can be registered for any molecule. Fewer generics
would result in more effective pharmacovigilance, control of counterfeit medicines
and facilitate education of the public on rational use of medicines.
d. Improve documentation for medicines registration, including: SOPs for the drug
registration process; time frames for assessment; methods of arbitration when any
two members of the Registration Committee disagree; updated list of rejected and
approved medicines; and declaration of COI for registration activities.
e. Improve the capacity for internal evaluation of generics by using the PPB secretariat
pharmacists, leaving the CDR experts to evaluate only innovator products.
f. Improve interaction and sharing of information between: drug registration, GMP
and importation departments; Registration Committees and applicants; and the PPB
and the Registration Committees.
g. Put in place effective and comprehensive post‐ marketing surveillance to ensure the
quality of subsequent batches of registered products; enforce the withdrawal of all
rejected and unregistered products in the market; and strengthen surveillance at
ports of entry.
h. Draw up a Memorandum of Understanding between the PPB and the NQCL to
ensure that all medicines are analysed before registration, and specify the time
within which analysis should be completed, among other things.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 12 ‐‐
i. Create data management systems to provide instant information to clients and make
available information/literature/internet searches for evaluators as they are meeting.
j. Harmonize: the three Drug Registration Committees (human, veterinary and
complementary medicines), and regional guidelines on medicines registration.
3.2. Licensing of pharmaceutical establishments
The Inspectorate Department of the PPB is responsible for licensing pharmaceutical
establishments. There are two formal committees that assess applications for licensing of a
pharmaceutical establishment at the PPB, one assesses applications for licence renewals (PPB
Management Committee) and the other assesses applications for new licences (PPB Practice
Committee). The guidelines for submission of applications for licensing were published in
June 2006. The process is also clearly spelt out in the service charter, which is publicly
available and covers administrative criteria to be met by applicants, and description of the
requirements to be met in terms of premises, facilities and personnel. Application fee
structure and the time frame for processing applications are also indicated. A list of
establishments (2007) exists, but it mainly includes the names of wholesalers and
manufacturers.
Indicator II.1: Requirement for a licence in order to operate a pharmaceutical establishment in Kenya
All 13 KIs indicated that it was a legal requirement to have a licence in order to operate a
pharmaceutical establishment in Kenya.
Indicator II.2: Issuance of pharmaceutical establishment licences at the medicines regulatory authority
All 13 indicated that there is a unit for issuing pharmaceutical establishment licences at the
PPB. The unit is established under the Inspectorate Department of the PPB.
Indicator II.3: Procedures for submission of applications for licensing
Ten (76.9%) of the KIs indicated that there were written procedures for submission of
applications for licensing. Three KIs, two from the private sector and one from academia,
were unaware of the existence of these procedures, which were published in 2006. Indeed,
most KIs who do not work at the PPB were not very knowledgeable about the contents of
the guidelines and the PPB service charter.
Indicator II.4: Guidelines for assessing applications for a licence
Eight (61.5%) of the KIs indicated that there were no written guidelines for assessing
applications for a licence. Only three (two from the MRA and one from academia) were
aware of the written guidelines. Two from the private sector did not know whether
guidelines existed or not. The procedure for processing of applications is published in the
guidelines.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 13 ‐‐
Indicator II.5: Submission of a pre-licensing inspection report
Ten of the KIs indicated that submission of a pre‐licensing inspection report is required for
making decisions on whether to issue a licence or not. Three from the private sector said it
was not a requirement. One KI from the private sector indicated that sometimes you can get
provisional licence from the PPB or District Pharmacist.
Indicator II.6: Committee that assesses applications for licensing of pharmaceutical establishments
Seven KIs (53.8%) indicated that there was a functioning formal committee that assesses
applications for licensing of a pharmaceutical establishment. Two, both from the private
sector, said that no such committee existed, while four others did not know if it existed or
not.
Indicator II.7: Criteria for selecting members of the committee
Only two KIs (15.4%) out of 13 indicated that criteria for selecting members of the
committees that assess licences existed. The KI from the PPB said criteria exist, but they are
not publicly available. No evidence was offered. The other KI from academia thought that
the criteria existed. Four KIs (30.8%) said that no such criteria existed and another four did
not know whether there were any criteria or not.
Indicator II.8: Composition and terms of reference of the committee
Five KIs indicated that there was no written document that describes the composition and
terms of reference of the committee and the other eight KIs (61.5%) did not know whether
the document existed or not.
Indicator II.9: Post-licensing inspection of licensed pharmaceutical establishments
Only four of the KIs indicated that post‐licensing inspection of licensed pharmaceutical
establishments is carried out at least every two years for all licensed establishments. Two of
the four were from the PPB, one from academia and the other one from the private sector.
All the other nine KIs (69.2%) disagreed and said that post‐licensing inspection of licensed
pharmaceutical establishments is erratic and done on an ad hoc basis. The reason given is
inadequate financial and human resources capacity.
Indicator II.10: List of all licensed pharmaceutical establishments available in the country
Eleven (84.6%) KIs indicated that there is an up‐to‐date list of all licensed pharmaceutical
establishments available in Kenya. One from academia said that no such list existed, while
one from the private sector did not know whether it existed or not. A list of licensed
pharmaceutical establishments (2007) was obtained, however, it mainly listed names of
wholesalers and manufacturers, and was incomplete on retail pharmacies.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 14 ‐‐
Indicator II.11: Opinion about the process of licensing of pharmaceutical establishments
Seven (53.8%) of the KIs disagreed or strongly disagreed with the statement “the licensing of
pharmaceutical establishments is systematically carried out according to policies and
procedures”, two were undecided and four either agreed or strongly agreed with the
statement (Table 7).
Table 7: Perception of key informants on the process of licensing of pharmaceutical establishments
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 0 0 0 0 2 0 0 2
Private 1 2 2 1 0 0 0 6
Academic 2 2 0 1 0 0 0 5
Total 3 4 2 2 2 0 0 13
DK: Don’t know, NA: Not applicable
Indicator II.12: Appeals system for applicants who have their applications for licensing rejected
Six (46.2%) KIs, including two from the PPB, said there was no independent appeals system
for applicants who have their applications for licensing rejected. Four did not know whether
it existed or not, while three (23.1%) said it exists but is not independent. An independent
appeals system for applicants who have their applications for licensing rejected does not
exist. However, the guidelines indicate that in the case of an unsuccessful application, the
applicant will be given further opportunity to revise and comply.
Indicator II.13: Operations and meetings of the committee that assesses applications for licensing
Mixed responses were received from the KIs to the statement “The formal committee that
assesses applications for licensing of pharmaceutical establishments is fully operational and
meets on a regular basisʺ. Two were undecided, three did not know, while four disagreed or
strongly disagreed with the statement. The two KIs from the PPB strongly agreed and two
other KIs from academia just agreed with the statement (Table 8).
Table 8: Perception of key informants on how operational the committee that assesses applications for licensing of pharmaceutical establishments is
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 0 0 0 0 2 0 0 2
Private 1 1 1 0 0 0 3 6
Academic 1 1 1 2 0 0 0 5
Total 2 2 2 2 2 0 3 13
DK: Don’t know, NA: Not applicable
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 15 ‐‐
Indicator II.14: Unethical behaviour in the licensing of pharmaceutical establishments
Below is a list of what the KIs perceived as the unethical practices that commonly occur in
the process of licensing pharmaceutical establishments in Kenya:
a. Subjectivity of the licensing officers: There is subjectivity in licensing so that the outcome depends on which officer handled it; there is bribery; some establishments
are licensed without full compliance with the basic requirements or without pre‐
licensing inspection; and there is manipulation of the pre‐licensing report.
b. Licensing of unqualified persons: There is licensing of unqualified people to operate pharmacies and manufacturing establishments; medical doctors and other
non‐pharmacists being allowed to operate a pharmacy within their clinics without a
pharmacist; and some pharmacists sell their licences to businessmen to operate
pharmaceutical establishments without the pharmacist being in charge.
c. Unethical behaviour: Unfriendly inspectors intimidate applicants in order to obtain
bribes; and lethargy within the PPB secretariat causes unnecessary delays in
licensing.
d. Unethical licensing: Some establishments are licensed for both retail and wholesale
business thus undercutting those that are licensed for retail business only; and there
is licensing of retail pharmacies situated too close to one another, hence promoting
unethical competition.
Indicator II.15: Actions that should be taken to improve the licensing process
The following are suggestions from KIs on how to improve licensing of pharmaceutical
establishments in Kenya:
a. Autonomy: Make the PPB autonomous from the MoH and establish an independent
licensing unit with a clear mandate, terms of reference and performance indicators.
b. Develop new documents and improve existing documentation for licensing, and make them easily accessible: These should include a checklist for inspectors;
guidelines for the composition, selection criteria and terms of reference for licensing
committees; and guidelines on COI with regard to licensing activities.
c. Improve the human resource capacity to carry out regular inspections and improve
on the ethical standards of inspectors.
d. Law enforcement: Carry out audits of licensed and unlicensed establishments; close
all the unlicensed ones; adhere to licensing guidelines; enforce annual renewal of
licences; enforce regular (biannual) inspection of establishments; encourage self‐
inspection of establishments; and have regular rotation of inspectors.
e. Application process: Establish on‐line application for licensing; shorten the time
taken to process and approve applications for licensing; and decentralize licensing to
provinces and districts.
f. Database: Establish an up‐to‐date database of all the licensed establishments.
g. Establish a well defined appeals system for applicants whose applications are
rejected.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 16 ‐‐
3.3. Inspection and market control of medicines
There is a comprehensive provision in the Pharmacy and Poisons Act (Cap. 244)9 covering
inspection of pharmaceutical establishments. There are written guidelines for GMP and also
for GDP for pharmaceutical products in Kenya. There are written SOPs for inspectors on
how to conduct inspections.
Indicator III.1: Legislation/regulation covering inspection of pharmaceutical establishments
Thirteen of the 15 KIs said there was provision in the medicines legislation that covered
inspection of pharmaceutical establishments. Two respondents, one from an NGO and the
other from the private sector, said that there was no provision.
Indicator III.2: Minimum level of information on inspection
All 13 respondents who said that there is provision for inspection of pharmaceutical
establishments in the legislation thought that the provision is comprehensive and that it
provides power to inspectors to enter, at any reasonable time, any place where medicines
are being produced, packaged, stored, distributed or tested. Many (92.3%) said that the
provision provides the PPB with the power to inspect, and 69.2% said the provision defines
the inspector’s duties and responsibilities. Another 76.9% said that the provision is available
to companies being inspected and that, although inspectors do not have identification
documents, they are provided with special identification tags or badges.
Indicator III.3: Guidelines classifying non-compliance with good manufacturing practices
Five KIs said that there were no written guidelines classifying non‐compliance with GMP
that describe the types of deficiencies and the corresponding measures to be taken by the
PPB. Nine KIs said that such guidelines existed in writing. Out of these nine, six (66.6%) said
that the guidelines define corresponding measures to be taken in case of non‐compliance
and that they were easily accessible to all stakeholders, while five (55.5%) said the guidelines
provide classification of GMP deficiencies. A minority of them (33.3%) said that the
guidelines provide an appeals mechanism for companies, but no one was aware of an
appeals system independent of the body making the original decision. Results from one KI
were invalid (too many “don’t knows”).
Indicator III.4: Guidelines classifying non-compliance with good distribution practices
Five KIs said that there were no written guidelines classifying non‐compliance with GDP
that describe the types of deficiencies and the corresponding measures to be taken by the
PPB and two did not know. Eight KIs said that such guidelines existed in writing. Out of
these eight, 87.5% said that they were easily accessible to all stakeholders, while 62.5% said
that the guidelines define corresponding measures to be taken in case of non‐compliance.
Four of them said the guidelines provide classification of GMP deficiencies. Three of them
(37.5%) said that the guidelines provide an appeals mechanism for companies and 12.5%
were not aware of an appeals system that is independent of the body making the original
decision.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 17 ‐‐
Indicator III.5: Procedures and mechanisms to prevent regulatory capture
Eleven KIs responded that there were no written procedures to prevent regulatory capture
between inspectors and the manufacturers or distributors, and one KI did not know.
Although three respondents said that such procedures exist, there was no evidence of
written procedures. However, some KIs (four from Government and one from the private
sector) added that although there were no written procedures, regulatory capture is
prevented as a matter of practice.
Indicator III.6: Guidelines on conflict of interest
All KIs responded that there were no written guidelines on COI with regard to inspection
activities. Some respondents said that the WHO guidelines on COI are followed, but that
they had not been domesticated.
Indicator III.7: Internal review of inspection findings
Eight KIs said that inspection findings and conclusions are subject to an internal review, one
answered that he did not know whether they are or not and six said there was no internal
review of inspection.
Indicator III.8: Standard operating procedures for conducting inspections
The majority (12) of the KIs thought that there were SOPs for inspectors on how to conduct
inspections, but three of them (NGO, government and private sector) said there were no
SOPs. All of the 12 KIs said there was an inspection checklist, but only seven said that there
were procedures detailing requirements for pre‐inspection activities. Eight respondents said
that there were procedures detailing requirements for post‐inspection activities, a
scheduling system identifying companies due for inspection within a set time frame and that
there was a format and content specified for inspection reports.
Indicator III.9: Criteria for the selection and recruitment of inspectors
Only three KIs, who were all from the Government, said that there were written criteria for
the selection and recruitment of inspectors. One responded that he did not know and 11 said
there were no criteria.
Indicator III.10: Influence of personal gain on the integrity of inspectors
Table 9 shows that the majority (11) of the respondents either strongly disagreed (40.0%) or
disagreed (33.3%) with the statement “The integrity of inspectors is in no way influenced by
personal gain, such as bribes, gifts, material or any other benefits”, while two agreed and
one strongly agreed. Those who either strongly disagreed or disagreed came from
Government (seven), private sector (2), academia (1) and an NGO (1). One respondent was
undecided.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 18 ‐‐
Table 9: Perception of key informants on the influence of personal gain on the integrity of inspectors
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 4 3 0 2 1 0 0 10
Private 1 1 0 0 0 0 0 2
Academia 0 1 0 0 0 0 0 1
NGO 1 0 1 0 0 0 0 2
Total 6 5 1 2 1 0 0 15
DK: Don’t know, NA: Not applicable
Indicator III.11: The use of guidelines and procedures in inspection activities
While about half of the respondents either strongly disagreed (3) or disagreed (5) with the
statement “Inspection activities are systematically carried out in accordance with the
guidelines and procedures to prevent bias”, the other half either strongly agreed (4) or
agreed (3) with the statement (Table 10).
Table 10: Perception of key informants on the influence of gifts on officials’ decisions
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 2 2 0 2 4 0 0 10
Private 0 2 0 0 0 0 0 2
Academia 1 0 0 0 0 0 0 1
NGO 0 1 0 1 0 0 0 2
Total 3 5 0 3 4 0 0 15
DK: Don’t know, NA: Not applicable
Indicator III.12: Types of unethical behaviour common in the inspection area
Below is a list of what the KIs perceived as the unethical practices common in the inspection
function in Kenya:
a. Unethical behaviour of the inspection officers: Inspectors are influenced by personal gain, either monetary or elevation of status; there is subjectivity of
inspectors who benefit from sponsored trips by proprietors of establishments;
inspectors do not introduce and identify themselves properly; and inspectors do not
help the companies to improve on their weak areas.
b. Unethical behaviour of proprietors: Proprietors of establishments try to bribe
inspectors; there is stocking of unregistered drugs; pharmacists play the role of
clinicians; during inspections the inspectees try to block inspectors from entering
some areas of the establishment; and some establishments fund inspectors’ travel on
trips.
c. Regulatory processes: There is regulatory capture because there is no rotation of inspectors; reports of inspectors are sometimes not acted on by the PPB; there is slow
feedback to establishments about the inspection report; and those inspected do not
have sufficient knowledge of the powers of the inspectors.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 19 ‐‐
d. Law enforcement: There are no regular inspections and when they are carried out,
there are few sanctions for non‐compliance; inspection guidelines are poor and so
enforcement is left to the discretion of the inspectors; and there are fake inspectors in
the country who harass owners of establishments.
Indicator III.13: Actions to improve the inspection area
The following were the actions suggested by the KIs to improve the inspection function in
Kenya:
a. There were contradictory suggestions on the organizational structure as follows: that
the PPB should be overhauled; the inspectorate should be made independent of the
PPB; the inspectorate should be under the MoH and not the PPB; the inspectorate in
the MoH and that in the PPB should be merged.
b. Documentation: Develop new and improve existing documentation for inspection,
especially guidelines and checklists.
c. Increase the capacity of inspection personnel in numbers and by training; and instil
ethical behaviour in inspectors.
d. Motivation and remuneration of inspectors: Remunerate inspectors well to decrease
the temptation to take bribes and give them confidence, by the PPB acting on their
reports.
e. Improve communication and interaction between the drug registration,
pharmacovigilance and inspection departments of the PPB; encourage benchmarking
for current Good Manufacturing Practices (cGMP) among pharmaceutical
establishments; work closely with the establishments to train personnel, discourage
bribes and show them the benefit of inspections.
f. Law enforcement: Revise the law regulating medicines, increase penalties for
offences and give clear power to the inspectorate; ensure that only registered
establishments are operating; have inspectors at all ports of entry for medicines.
g. Inspection procedures: Rotate inspectors to prevent capture; use ad hoc committees
to help the regular inspectors; have regular schedules of inspections and also have
impromptu inspections; encourage self‐inspection of establishments; introduce pre‐
shipping inspection of all imported drugs and seal to prevent counterfeiting and
changing drugs; report back to those inspected within two weeks.
3.4. Medicines promotion control
Advertising of medicines is governed by the laws of Kenya Cap 244, which mention the
following areas: advertisement to professionals, advertisement to the public, qualification
and training of medical representatives, restrictions on and monitoring of free samples, and
packaging, labelling and package inserts, plus penalties for breaching the law. At the PPB
there is a Promotions Committee that vets medicines promotion advertisements.
Indicator IV.1: Provision in the medicines legislation/regulations covering drug promotion and advertising
All 15 KIs said that there is a provision within the pharmacy legislation covering promotion
and advertising of medicines.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 20 ‐‐
Indicator IV.2: Forms of promotion explicitly mentioned in the provisions on drug promotion
All 15 indicated that the provisions on promotion of medicines mention the following areas:
advertisement to professionals, advertisement to the public, qualification and training of
medical representatives, restrictions on and monitoring of free samples, and packaging,
labelling and package inserts. However, there is no mention of symposia and scientific
meetings, post‐marketing scientific studies, speaker’s fees and consultancies, promotion of
exported drugs, and restrictions and limits on gifts and gimmicks.
Indicator IV.3: Pre-approval of promotional and advertising materials
Eleven KIs (73.3%) indicated that pre‐approval of promotional and advertising materials is
mandatory in Kenya and must include a summary of key product characteristics, such as
dosage form, company name, major indications for use, brand name and generic name,
medicine interactions and adverse/side‐effects profile. Information about the price of the
medicine is not mandatory for approval of the advertising material. Four KIs (26.7%) said
that pre‐approval of promotional materials is not officially required. Three of these were
from the private sector and one from a local NGO who had previously worked with a
multinational drug firm, however. He said that all materials targeted for clinicians did not
require pre‐approvals.
Indicator IV.4: Enforcement mechanism on promotion and advertisement of medicines
Ten KIs (66.7%) indicated that the provisions foresee an enforcement mechanism on
promotion of medicines and sanctions were clearly stated. Three said there were no
provisions, while two did not know. The provisions enforcement is spelt out in subsection
36‐40 of Chapter 244 of Laws of Kenya, which gives sanctions and indicates the type of
penalties for any person or pharmaceutical companies breaching the law.
Indicator IV.5: Complaints procedure to report unethical promotional practices
Eight (53.3%) of KIs indicated that there is no formal complaints procedure to report
unethical promotional practices, five (33.3%) said they did not know and two said it existed.
There are no written procedures, no evidence that any complaints procedure is used or
results of complaints published. Reporting is usually done informally.
Indicator IV.6: Monitoring and enforcing the provisions on drug promotion
Eight KIs indicated that there was a committee responsible for monitoring and enforcing the
provisions on drug promotion. Four of the KIs said they did not know, while three (20.0%)
indicated that such a committee did not exist. At the PPB there is a committee that vets
medicines promotion advertisements, but there is no Government service or committee
responsible for monitoring and enforcing the provisions on drug promotion.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 21 ‐‐
Indicator IV.7: Criteria for selecting members of service/Committee for Monitoring and Enforcing Provisions on Medicines Promotion
Three KIs indicated that there were no clear criteria for selecting members of the committee,
while five said that criteria existed. Seven (46.7%) indicated that they did not know of any
clear criteria for selecting members of the Committee for Monitoring and Enforcing
Provisions on Medicines Promotion. No criteria are available in writing and neither are there
specifications for the professional qualifications, technical skills or work experience
necessary. Selection of people involved in control of medicines promotion is done by the
Registrar of the PPB.
Indicator IV.8: Composition and terms of reference of the service/committee
Only one KI from the PPB indicated that there was a written document that describes the
composition and terms of reference of the service/committee. He described the document as
a memo from the head of the PPB. Five KIs said that no written document was available.
Nine (60.0%) did not know.
Indicator IV.9: Standard operating procedures guiding the services responsible for pre-approving or monitoring drug promotion and advertising
All the KIs indicated that there were no written SOPs guiding the services responsible for
pre‐approving or monitoring drug promotion and advertising. The KIs from the PPB
indicated that the SOPs were being developed.
Indicator IV.10: Guidelines on conflicts of interest with regard to medicine promotion activities
All KIs indicated that there were no written guidelines on COI with regard to the control of
medicine promotion activities.
Indicator IV.11: How legal provisions on drug promotion have been developed
Ten of the KIs disagreed or strongly disagreed with the statement: “The legal provisions on
drug promotion have been developed in broad consultation with all interested parties”.
Four agreed or strongly agreed (two from the MRA and two from the private sector), while
one did not know (Table 11).
Table 11: Perception of key informants on how legal provisions on drug promotion have been developed
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 0 1 0 1 1 0 0 3
Private 2 3 0 2 0 0 1 8
Academic 1 2 0 0 0 0 0 3
NGO 0 1 0 0 0 0 0 1
Total 3 7 0 3 1 0 1 15
DK: Don’t know, NA: Not applicable

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 22 ‐‐
Indicator IV.12: Pre-approval of promotional and advertising materials before they are made public
Ten KIs disagreed or strongly disagreed with the statement: “Pre‐approval of promotional
and advertising materials is systematically obtained before they are made public”. One was
undecided, and four agreed or strongly agreed (Table 12).
Table 12: Perception of key informants on the requirement for pre-approval of promotional and advertising materials
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 0 1 0 1 1 0 0 3
Private 2 5 0 0 1 0 0 8
Academic 0 1 1 1 0 0 0 3
NGO 0 1 0 0 0 0 0 1
Total 2 8 1 2 2 0 0 15
DK: Don’t know, NA: Not applicable
Indicator IV.13: Civil society/nongovernmental organizations’ influence on improving the control of drug promotion
Table 13 shows that nine KIs disagreed or strongly disagreed with the statement: “Civil
society/nongovernmental organizations have a great influence on improving the control of
drug promotion in Kenya”. One was undecided and five agreed or strongly agreed with the
statement.
Table 13: Perception of key informants on the role of civil society organizations/NGOs in improving control of medicines promotion in Kenya
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 2 0 0 1 0 0 0 3
Private 4 2 0 0 2 0 0 8
Academic 0 1 0 2 0 0 0 3
NGO 0 0 1 0 0 0 0 1
Total 6 3 1 3 2 0 0 15
DK: Don’t know, NA: Not applicable
Indicator IV.14: Application of sanctions when there is a breach in medicines promotion activities
Ten KIs disagreed or strongly disagreed with the statement “Sanctions foreseen in the
provisions on medicine promotion are systematically applied when there is a breach”. Two
were undecided, another two agreed and one did not know (Table 14).
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 23 ‐‐
Table 14: Perception of KIs on application of sanctions when there is a breach in medicines promotion
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 0 2 0 1 1 0 0 4
Private 4 3 1 0 0 0 0 8
Academic 0 0 1 0 0 0 1 2
NGO 0 1 0 0 0 0 0 1
Total 4 6 2 1 1 0 1 15
DK: Don’t know, NA: Not applicable
Indicator IV.15: Types of unethical behaviours common in the medicines promotion area
The following were cited by KIs as the perceived unethical practices common in the
medicines promotion area in Kenya:
a. Pharmaceutical firms induce doctors to prescribe certain products through giving incentives, such as free samples, cash, gifts, sponsoring of tours, holidays and
workshops.
b. Unethical promotion: Promoters make biased and false claims without warning
about side‐effects and interactions; and promotion meant for health practitioners
only are directed to the general public through radio advertisements and talk shows.
c. Regulation: Sometimes unregistered medicines are approved for promotion; and
there is inadequate monitoring of promotion.
d. Law enforcement: Legislation and regulation of promotion is weak; and
interventions to address unethical behaviours often occur too late.
Indicator IV.16: Actions to improve the drug promotion process
The following were the actions suggested by the KIs to improve the promotion area in
Kenya:
a. Legislation: Amend the law to include control of herbal and complementary
medicines.
b. Regulation: Promote only registered products; vet all promotional materials;
emphasize the use of INN names in medicines promotion; constitute a promotions
control committee that includes non‐medical practitioners, such as civil society
groups and consumer organizations.
c. Documentation: Develop and strengthen guidelines and SOPs for the control of medicines promotion.
d. Education and awareness: Introduce a unit in the pharmacy education curriculum
on drug promotion; institute mass media campaigns to educate the public on the
dangers of unethical medicines promotion; ensure medical representatives are well
trained and ethical in medicines promotion.
e. Law enforcement: Introduce strict penalties for unethical behaviour and empower
the PPB to penalize offenders; set up an inspectorate to police the promotion of
medicines in the country.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 24 ‐‐
3.5. Control of clinical trials
There is legal provision for the regulation of clinical trials in Kenya, which is provided in the
Laws of Kenya, the Science and Technology Act10 of 1979. This Act established the creation
of the National Council of Science and Technology (NCST), which has mandated the major
hospitals and institutions doing research to have institutional ethics and research
committees (ERCs). The institutions with ERCs are Kenyatta National Hospital/University of
Nairobi (KNH/UoN), Kenya Medical Resarch Institute (KEMRI), Moi Teaching and Referral
Hospital and the Aga Khan University Hospital. There are written and publicly available
guidelines on the submission of applications to the PPB to conduct clinical trials and there is
also a documented procedure for submission of applications to the various institutional
ERCs. The PPB also has requirements for the manufacture, importation, exportation and use
of investigational products. The PPB has a formal review committee which is responsible for
reviewing applications. According to the service charter of the PPB11, the evaluation of the
application and subsequent approval or rejection must be completed within two months.
Indicator V.1: Legal provision requiring regulation of clinical trials
Nine of the 15 KIs said there was provision for regulation of clinical trials in the legislation,
two did not know and four said that it did not exist.
Indicator V.2: National guidelines on principles of Good Clinical Practice
There are no national guidelines on principles of Good Clinical Practice. Ten KIs were aware
of the non‐existence of national guidelines, but five were not.
Indicator V.3: Guidelines on submission of applications to the Pharmacy and Poisons Board
Four KIs said that there were no written guidelines and one KI did not know. The KIs who
were not aware of these guidelines were from the MoH and from the Ethics and Research
Committees (ERCs). The other 10 KIs were aware of the existence of the guidelines and they
were mainly from the PPB, private pharmaceutical companies and researchers conducting
clinical trials. They said that the guidelines included the trials’ objective and purpose (90.0%
of the 10 KIs), trial design (100%), criteria for inclusion and exclusion of trial subjects
(90.0%), the means of obtaining informed consent (80.0%) and the time frame for assessing
applications (70.0%). Although the time frame for assessing applications is not in the
guidelines, it is in the service charter for the PPB.
Indicator V.4: Procedure for submission of clinical trial applications to an Independent Ethics Review Committee
There is no Independent Ethics Review Committee in Kenya and review of clinical trial
applications is only done by the institutional ERCs. Only one KI responded that the
procedure for submission of clinical trial applications to an Independent Ethics Committee
does not exist. The other 14 said that it existed, but in fact they were referring to procedures
of the ERCs, which exist in writing. In reference to the procedure for submission of
applications to the ERCs, 85.7% of KIs said that the following details were required:
acceptability of the investigator for the proposed trial; suitability of the proposal; means by
which subjects are recruited; completeness of information and provision for compensation
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 25 ‐‐
or treatment in case of death or loss or injury to the subject. Seven of the 14 KIs indicated
that the form of payment or remuneration from the sponsor should be included in the
application.
Indicator V.5: Requirement for the manufacture, importation, exportation and use of investigational products
One KI said there were no requirements for regulation of investigational products and one
KI did not know. The other twelve KIs were all aware of the requirements.
Indicator V.6: Committee for reviewing clinical trials applications and results
The Pharmacy and Poisons Board reviews clinical trials applications through the Committee
for Clinical Trials (CCT). This Committee has been in existence for less than two years and
has so far been evaluating applications but not the results of the clinical trials. Only 10 KIs
were aware of the existence of this Committee, three said it did not exist and two did not
know.
Indicator V.7: Mechanisms to ensure reviewers have expertise
Although there were no written guidelines, 11 KIs were confident that there are working
mechanisms to ensure that those involved in the review of applications and clinical trial
results have sufficient and current expertise in all the required areas. The KIs also believed
that the guidelines covered reviewers’ technical qualification (100% of the 11 KIs), their
experience in research and clinical investigation (100%), declaration of COI (90.1%) and the
time frame for serving as a committee member (81.8%).
Indicator V.8: Established and operational clinical trials inspection system
There is no established and operational clinical trials inspection system in Kenya. The PPB
Committee for Clinical Trials has not yet started inspection. Different ERCs also occasionally
carry out inspections, but these are rare and often prompted by adverse effects reports.
Eleven KIs were aware that there is no inspection system, but four said that an inspection
system existed.
Indicator V.9: Establishment of an Independent Ethics Committee
The national guidelines that cover clinical trials do not require the establishment of an
Independent Ethics Committee, but they recommend independence in the review of clinical
trial applications. Eight KIs said that the national guidelines require the establishment of an
Independent Ethics Committee; six said there is no requirement and one did not know.
Indicator V.10: Time frame for assessing clinical trial applications
Eleven KIs said that there is a time frame for the Review Committee to assess clinical trial
applications; three said there is no time frame and one did not know.
Indicator V.11: Guidelines on conflict of interest
Six KIs said there were written guidelines on COI, three said there were none and five did
not know. Those KIs who said there were no guidelines were from the PPB and the CCT,

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 26 ‐‐
while the ‘Don’t know’ responses were mainly from researchers. The respondents who said
‘yes’ were mostly members of ERCs and they said the guidelines were in the form of SOPs.
Indicator V.12: List of all approved and rejected clinical trial applications
In Kenya, each ERC keeps a list of all approved and rejected clinical trials that it has
assessed. There is no published national list giving all clinical trials in the country. Eight KIs
said there was a list of all approved, amended and rejected clinical trials applications, six
said there was not and one KI did not know. Seven out of the eight said that the list was not
publicly available.
Indicator V.13: Selection criteria for Independent Ethics Committee
Half of the KIs strongly agreed (4) or agreed (3) with the statement “The Independent Ethics
Committee members are systematically selected based on the written selection criteria” and
only about a third of the KIs either strongly disagreed or disagreed (Table 15). Since there is
no IEC in Kenya, the KIs were referring to the ERCs.
Table 15: Perception of KIs on the selection criteria for independent ethics committee
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 0 0 0 0 0 1 1 2
Private 0 2 0 1 0 0 0 3
Academia 1 1 0 1 3 0 1 7
Media 0 0 0 1 0 0 0 1
Lawyer 0 0 0 0 1 0 0 1
Total 1 3 0 3 4 1 2 14
DK: Don’t know, NA: Not applicable
Indicator V.14: Selection criteria for the Pharmacy and Poisons Board Review Committee members
Table 16 shows that the majority of the KIs, including all the ones from the private sector,
did not agree with the statement “The Pharmacy and Poisons Board Review Committee
members are selected systematically based on the written selection criteria”. Three KIs
agreed with the statement and two strongly agreed.
Table16: Perception of KIs on the selection criteria for PPB Review Committee members
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 1 0 0 0 0 0 1 2
Private 0 3 0 0 0 0 0 3
Academia 3 1 0 1 2 0 1 8
Media 0 0 0 1 0 0 0 1
Lawyer 0 0 0 1 0 0 0 1
Total 4 4 0 3 2 0 2 15
DK: Don’t know, NA: Not applicable
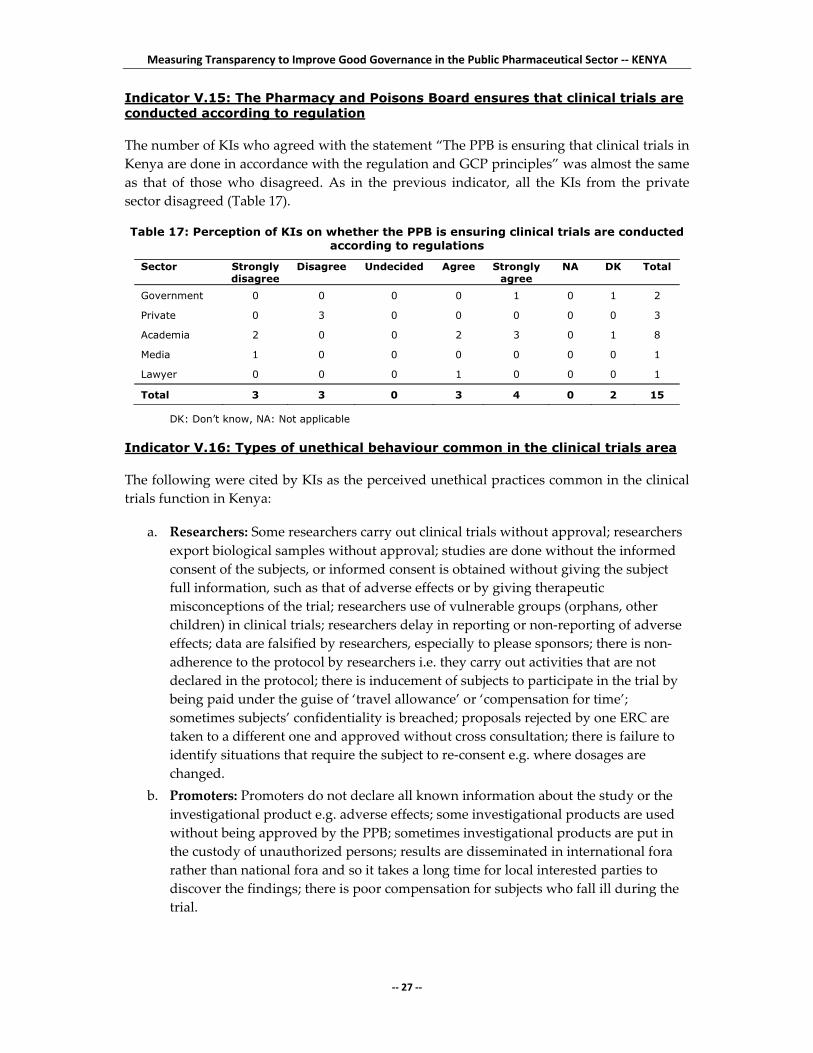
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 27 ‐‐
Indicator V.15: The Pharmacy and Poisons Board ensures that clinical trials are conducted according to regulation
The number of KIs who agreed with the statement “The PPB is ensuring that clinical trials in
Kenya are done in accordance with the regulation and GCP principles” was almost the same
as that of those who disagreed. As in the previous indicator, all the KIs from the private
sector disagreed (Table 17).
Table 17: Perception of KIs on whether the PPB is ensuring clinical trials are conducted according to regulations
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 0 0 0 0 1 0 1 2
Private 0 3 0 0 0 0 0 3
Academia 2 0 0 2 3 0 1 8
Media 1 0 0 0 0 0 0 1
Lawyer 0 0 0 1 0 0 0 1
Total 3 3 0 3 4 0 2 15
DK: Don’t know, NA: Not applicable
Indicator V.16: Types of unethical behaviour common in the clinical trials area
The following were cited by KIs as the perceived unethical practices common in the clinical
trials function in Kenya:
a. Researchers: Some researchers carry out clinical trials without approval; researchers
export biological samples without approval; studies are done without the informed
consent of the subjects, or informed consent is obtained without giving the subject
full information, such as that of adverse effects or by giving therapeutic
misconceptions of the trial; researchers use of vulnerable groups (orphans, other
children) in clinical trials; researchers delay in reporting or non‐reporting of adverse
effects; data are falsified by researchers, especially to please sponsors; there is non‐
adherence to the protocol by researchers i.e. they carry out activities that are not
declared in the protocol; there is inducement of subjects to participate in the trial by
being paid under the guise of ‘travel allowance’ or ‘compensation for time’;
sometimes subjects’ confidentiality is breached; proposals rejected by one ERC are
taken to a different one and approved without cross consultation; there is failure to
identify situations that require the subject to re‐consent e.g. where dosages are
changed.
b. Promoters: Promoters do not declare all known information about the study or the
investigational product e.g. adverse effects; some investigational products are used
without being approved by the PPB; sometimes investigational products are put in
the custody of unauthorized persons; results are disseminated in international fora
rather than national fora and so it takes a long time for local interested parties to
discover the findings; there is poor compensation for subjects who fall ill during the
trial.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 28 ‐‐
c. Regulators: Some studies have been stopped without sound scientific basis;
sometimes there is no independence of review; there is no mechanism to ensure that
applications rejected by one ERC are not approved by another; there is hardly any
inspection of on‐going trials.
d. Ethics and research committees: Sometimes the committee approving the studies is
made up of members who are researchers in the clinical trial being evaluated; the
relationship between applicants and the ERCs is not cordial and is often hostile
towards applicants; the term of office of ERC members is not defined.
Indicator V.17: Actions to improve the clinical trials area
KIs gave the following suggestions for improving clinical trial activities in Kenya
a. Legislation: Review legislation regulating clinical trials as a stand alone law on clinical trials instead of the current law which clusters clinical trials under biomedical
research; include new types of clinical trials such as those on genetic products in the
law; and specify penalties for errant researchers and promoters in the law.
b. Regulation: Enforce coordination and regulation of clinical trials at national level and involve NCST, MoH and the PPB; set up an independent ethics committee;
establish an inspectorate for clinical trials; ensure all investigational products are
registered; publish a list of all clinical trials applications and their status; expedite the
review process to make it shorter; enforce disciplinary measures for errant
researchers.
c. Documentation: Put in place well established processes and publicize them. These
include documents for recruitment, applications, reporting and COI.
d. Education and capacity building: Give technical support and capacity building for the PPB and train staff through other regulatory bodies like the U.S. Food and Drug
Administration; source expertise for review of applications beyond Kenya; educate
and sensitize regulators, subjects, ERC members and researchers through
workshops; strengthen data safety and monitoring boards.
3.6. Selection of medicines
There is a National Essential Medicines List which is in line with WHO procedures, but it
was last updated in 2002. A National Medicines and Therapeutics Committee (NMTC) was
constituted in 2007 with the mandate of selection of medicines, but it is not yet operational.
There are clear criteria for the selection of members of the NMTC and terms of reference that
describe the role and responsibilities of the NMTC that have been developed over the last
year, but they are not yet in use.
Indicator VI.1: National Essential Drugs List
The Government has an officially adopted national essential medicines list that is publicly
available and all the KIs affirmed this. The list was last reviewed in 2002. However, some of
the KIs said that this list is not widely disseminated because there is no system for
distribution and only small quantities are published.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 29 ‐‐
Indicator VI.2: Consultation during the development of the National Essential Drugs List
The number of KIs who agreed with the statement “The national essential medicines list has
been developed in consultation with all interested parties and using an evidence‐based
approach” was almost the same as that of those who disagreed (Table 18). Most of those
who disagreed were the older professionals who have been working in the MoH and were
involved in the last review of the EDL. Some emphasized that major stakeholders were not
consulted in the development of the EML, while others said the approach used was not
evidence based.
Table 18: Perception of key informants on the extent of consultations with interested parties in the development of the National Essential Drugs List
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 1 6 0 5 0 0 1 13
Academia 0 0 0 1 0 1 0 2
Total 1 6 0 6 0 1 1 15
DK: Don’t know, NA: Not applicable
Indicator VI.3: Guidelines for selection of medicines in the essential medicines list
There are no written guidelines for the selection process for including or deleting medicines
from the national EML. Eleven KIs said there were no guidelines, but four said that there
were guidelines. Since no evidence was available, the score for this indicator was therefore
zero.
Indicator VI.4: Essential medicines list and WHO procedures
Eleven KIs said that the EML was in line with WHO procedures, three said ‘No’ and one did
not know. The majority said that the EML was published but not easily accessible (63.6% of
the 11 KIs), not widely disseminated to relevant health professionals (90.9) and had not been
revised in the last five years (72.7%). The KIs said that theEML gives drugs by their generic
names (100%), is listed by levels of health care (72.7%) and is linked to national standard
treatment guidelines (90.9%).
Indicator VI.5: Committee for selection of the national essential medicines list
The National Medicines and Therapeutics Committee is responsible for the selection of the
EML. Eight KIs said that this committee exists but four said there is no such committee.
IndicatorVI.6: Influences on the committee for the selection of the national essential medicines list
Five KIs agreed or strongly agreed with the statement “The committee responsible for the
selection of the national EML is operating free from external influence”, four disagreed and
five said that the question is ‘not applicable because the committee does not exist’. One KI
responded “Don’t know” (Table 19).
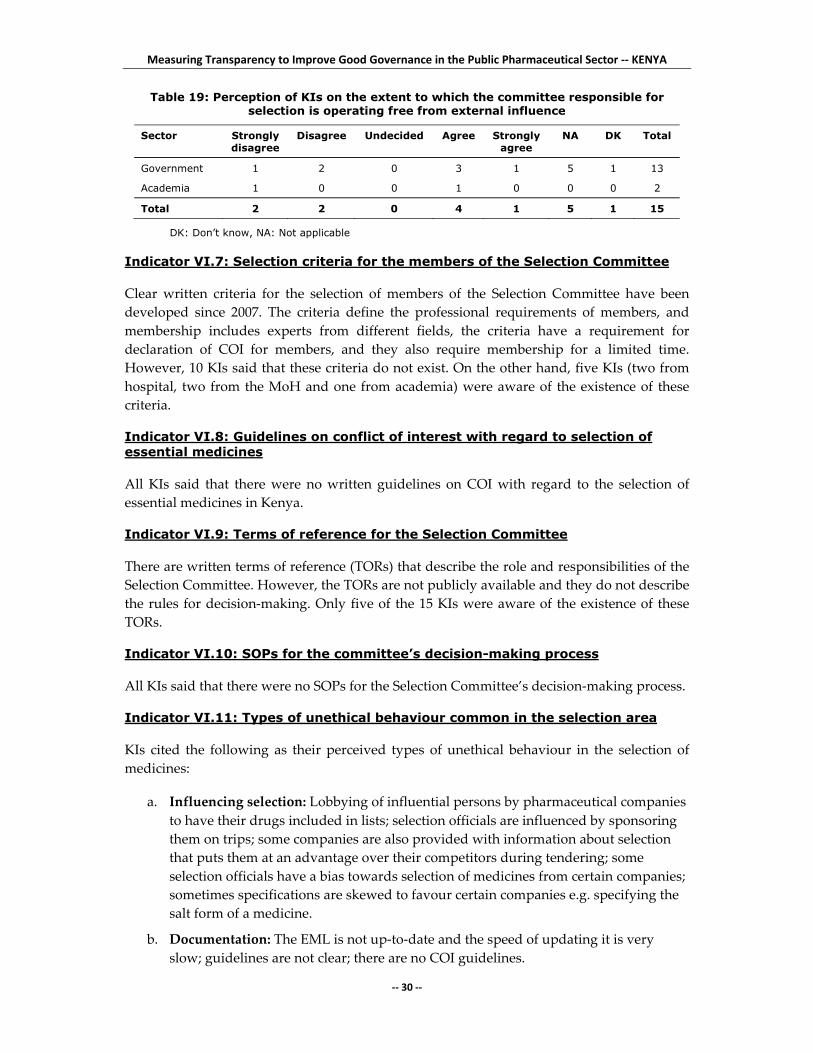
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 30 ‐‐
Table 19: Perception of KIs on the extent to which the committee responsible for selection is operating free from external influence
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 1 2 0 3 1 5 1 13
Academia 1 0 0 1 0 0 0 2
Total 2 2 0 4 1 5 1 15
DK: Don’t know, NA: Not applicable
Indicator VI.7: Selection criteria for the members of the Selection Committee
Clear written criteria for the selection of members of the Selection Committee have been
developed since 2007. The criteria define the professional requirements of members, and
membership includes experts from different fields, the criteria have a requirement for
declaration of COI for members, and they also require membership for a limited time.
However, 10 KIs said that these criteria do not exist. On the other hand, five KIs (two from
hospital, two from the MoH and one from academia) were aware of the existence of these
criteria.
Indicator VI.8: Guidelines on conflict of interest with regard to selection of essential medicines
All KIs said that there were no written guidelines on COI with regard to the selection of
essential medicines in Kenya.
Indicator VI.9: Terms of reference for the Selection Committee
There are written terms of reference (TORs) that describe the role and responsibilities of the
Selection Committee. However, the TORs are not publicly available and they do not describe
the rules for decision‐making. Only five of the 15 KIs were aware of the existence of these
TORs.
Indicator VI.10: SOPs for the committee’s decision-making process
All KIs said that there were no SOPs for the Selection Committee’s decision‐making process.
Indicator VI.11: Types of unethical behaviour common in the selection area
KIs cited the following as their perceived types of unethical behaviour in the selection of
medicines:
a. Influencing selection: Lobbying of influential persons by pharmaceutical companies
to have their drugs included in lists; selection officials are influenced by sponsoring
them on trips; some companies are also provided with information about selection
that puts them at an advantage over their competitors during tendering; some
selection officials have a bias towards selection of medicines from certain companies;
sometimes specifications are skewed to favour certain companies e.g. specifying the
salt form of a medicine.
b. Documentation: The EML is not up‐to‐date and the speed of updating it is very
slow; guidelines are not clear; there are no COI guidelines.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 31 ‐‐
c. Selection process: The annual selection is based on institutional prescribing and practices, more than on the EML, which is not frequently updated; there is confusion
between medicines recommended in the EML and those in the treatment guidelines,
which are often more up‐to‐date; decisions are sometimes made by incompetent
people, leading to irrational decisions; there is lack of objectivity in selection, e.g.
inclusion of too many antimalarial drugs in the list or inclusion of expensive and
rarely used medicines; and selection is influenced by the cost of medicines.
d. There is inappropriate representation in Selection Committees.
e. Higher authorities sometimes overrule the expert opinion given.
f. There is leniency in disciplining errant selection officials.
Indicator VI.12: Actions to improve the selection area
The following suggestions were made by KIs to improve medicines selection in Kenya:
a. Selection Committee: Operationalize the NMTC and decrease the number of MoH
officials in this Committee; speed up the Committee’s work; give it support at the
highest level (minister, permanent secretary, director of medical services); and
introduce rotation and time limits for members.
b. Documentation: develop clear guidelines for the Committee’s work; develop
regional lists to address different disease patterns; and set up a national drug
formulary.
c. Selection process: Carry out a survey to establish which drugs would cater for the
bulk (90%) of health needs; involve wide consultation in the selection process and
include all stakeholders; increase transparency of the procurement process; provide
enough time for the selection and procurement process.
d. Awareness: Publicize the selection process and educate both the public and professionals on selection.
e. Set up a coordination committee to implement decisions.
f. Increase budgetary allocation for selection.
g. Ensure that only prequalified drugs are in the market.
3.7. Procurement of medicines
Public sector procurement of medicines is done by Kenya Medical Supplies Agency
(KEMSA). Procedures for procurement exist and are heavily informed by the newly
published Public Procurement and Disposal Act12. This document is publicly available and
requires: the use of generic names; the advertisement of tenders; that contract specifications
be publicly available to all bidders; that criteria for adjudication of tenders be included as
part of the tender package and all bidders informed in advance; and that the information on
the tender process and results be made public. The Procurement Office monitors supplier
performance during every tender for compliance with the contract terms; the monitoring
system tracks supplier’s lead‐time, delivery status, shelf life and packaging of products.
Product quality is also tracked, and suppliers with poor performance are barred from future
tenders.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 32 ‐‐
Indicator VII.1: Procedures for procurement of pharmaceutical products
All of the 14 KIs indicated that Government uses explicit procedures for procurement of
pharmaceutical products.
Indicator VII.2: Guidance for Procurement Office staff on the type of procurement method to be used for different types of products
Thirteen (92.8%) KIs indicated that a written in‐house guideline existed and is used to guide
the procurement staff on the method to use for different types of products. One KI from the
MoH indicated that no guidelines existed.
Indicator VII.3: Quantification method to determine the amounts to be purchased
Nine (64.3%) of the KIs indicated that procurement was done with an objective
quantification method to determine the quantity of pharmaceuticals to be purchased, but
five (35.7%) said it did not.
Indicator VII.4: Appeals process for applicants who have their bids rejected
Twelve (85.7%) of the KIs said that there was a formal appeals process for applicants who
have their bids rejected and it was clearly defined in the Procurement Act. Two KIs did not
know about the appeals system.
Indicator VII.5: Separation of key functions of the Procurement Office and those of the Tender Committee
All 14 KIs indicated that a Tender Committee was formally established, was responsible for
suppliers’ selection for all tenders and for contract decisions and that the functions of the
Procurement Office and those of the Tender Committee were clearly separated.
Indicator VII.6: Decisions of the Tender Committee
Ten (71.4%) of KIs agreed or strongly agreed with the statement that “Decisions of the
Tender Committee are always taken into account in the procurement process” as shown in
Table 20.
Table 20: Perception of KIs regarding the extent to which decisions of the Tender Committee are taken into account in the procurement process
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 0 2 0 3 5 0 1 11
Private 0 0 0 0 2 0 0 2
Academic 0 1 0 0 0 0 0 1
Total 0 3 0 3 7 0 1 14
DK: Don’t know, NA: Not applicable
Indicator VII.7: Criteria for Tender Committee membership
Thirteen KIs indicated that the criteria for Tender Committee membership are written and
publicly available. One did not know.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 33 ‐‐
Indicator VII.8: Guidelines on conflicts of interest
The law requires members to declare COI. However, 11 (78.6%) of the KIs said they did not
know of any written guidelines on COI with regard to the procurement process. Three
(21.4%) indicated that written guidelines were in place. Forms for members to sign do not
exist and rules on acceptance of gifts are generally covered in the law. The law requires
members to declare COI but there was no evidence of enforcement of this.
Indicator VII.9: Criteria for selection of members of the Tender Committee
Ten KIs agreed with the statement “The members of the Tender Committee are systemically
selected based on specific criteria” (Table 21).
Table 21: Perception of KIs about selection of members of the Tender Committee
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 0 1 1 3 5 0 1 11
Private 0 0 0 1 1 0 0 2
Academic 1 0 0 0 0 0 0 1
Total 1 1 1 4 6 0 1 14
DK: Don’t know, NA: Not applicable
Indicator VII.10: Computerized management information system to report product problems
Seven of the 14 KIs indicated that there was no computerized management information
system used to report product problems in procurement. Four (28.6%) indicted that the
system existed and two did not know. Responses from MoH were mixed with some saying
that the system existed and others saying it did not. The KIs from central medical stores
(KEMSA) procurement department indicated that the management information system is
computerized and it includes product records, and monitors supplier performance and
tracks the status for each order. It does not, however, record quality assurance information
for the products purchased, nor client performance nor does the system track quantities
actually purchased compared with the original estimates made.
Indicator VII.11: Standard operating procedures for routine inspection of consignments
Thirteen KIs indicated that SOPs for routine inspection existed and that each shipment of
medicines should be physically inspected. One KI from the private sector did not know
whether SOPs existed or not. The procedures in place involve checking adherence to
contract specifications. Samples are sent to an in‐house quality control laboratory. Random
sampling is done for regular suppliers and systematic sampling for new ones. All
documents (inspection reports and laboratory testing results) are archived in the
Procurement Office. Only one KI from MoH headquarters was unaware of the existence of
the SOPs.
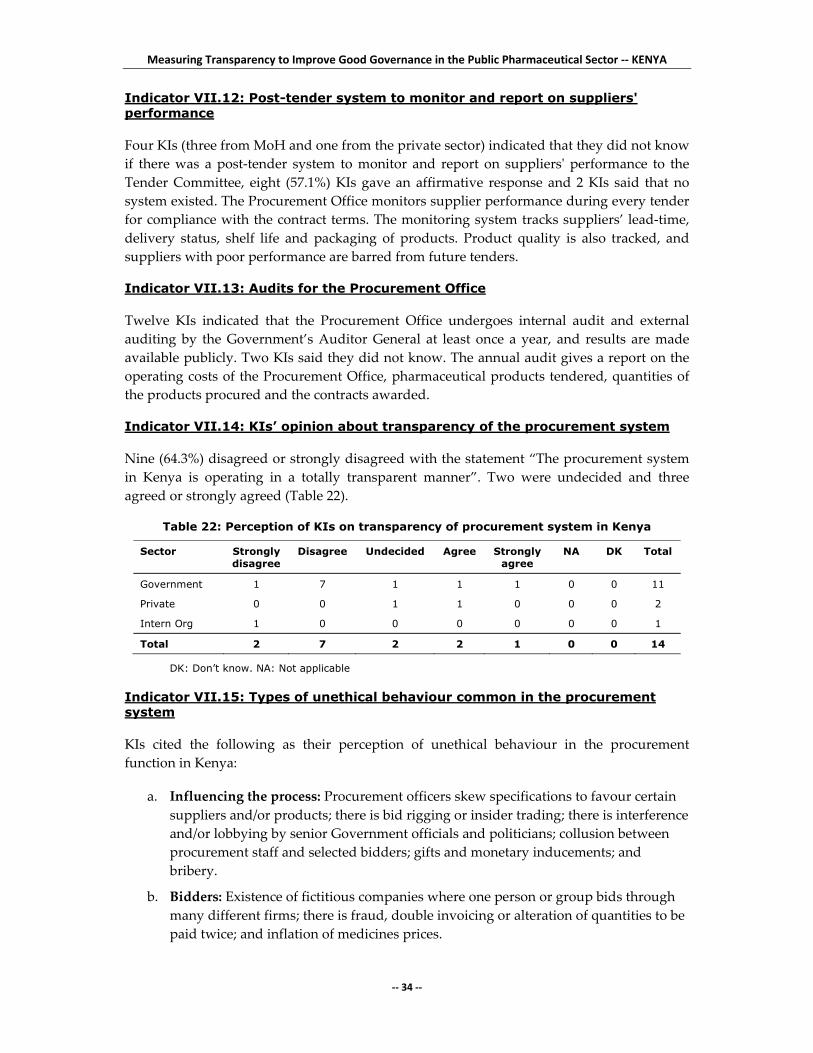
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 34 ‐‐
Indicator VII.12: Post-tender system to monitor and report on suppliers' performance
Four KIs (three from MoH and one from the private sector) indicated that they did not know
if there was a post‐tender system to monitor and report on suppliersʹ performance to the
Tender Committee, eight (57.1%) KIs gave an affirmative response and 2 KIs said that no
system existed. The Procurement Office monitors supplier performance during every tender
for compliance with the contract terms. The monitoring system tracks suppliers’ lead‐time,
delivery status, shelf life and packaging of products. Product quality is also tracked, and
suppliers with poor performance are barred from future tenders.
Indicator VII.13: Audits for the Procurement Office
Twelve KIs indicated that the Procurement Office undergoes internal audit and external
auditing by the Government’s Auditor General at least once a year, and results are made
available publicly. Two KIs said they did not know. The annual audit gives a report on the
operating costs of the Procurement Office, pharmaceutical products tendered, quantities of
the products procured and the contracts awarded.
Indicator VII.14: KIs’ opinion about transparency of the procurement system
Nine (64.3%) disagreed or strongly disagreed with the statement “The procurement system
in Kenya is operating in a totally transparent manner”. Two were undecided and three
agreed or strongly agreed (Table 22).
Table 22: Perception of KIs on transparency of procurement system in Kenya
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 1 7 1 1 1 0 0 11
Private 0 0 1 1 0 0 0 2
Intern Org 1 0 0 0 0 0 0 1
Total 2 7 2 2 1 0 0 14
DK: Don’t know. NA: Not applicable
Indicator VII.15: Types of unethical behaviour common in the procurement system
KIs cited the following as their perception of unethical behaviour in the procurement
function in Kenya:
a. Influencing the process: Procurement officers skew specifications to favour certain
suppliers and/or products; there is bid rigging or insider trading; there is interference
and/or lobbying by senior Government officials and politicians; collusion between
procurement staff and selected bidders; gifts and monetary inducements; and
bribery.
b. Bidders: Existence of fictitious companies where one person or group bids through
many different firms; there is fraud, double invoicing or alteration of quantities to be
paid twice; and inflation of medicines prices.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 35 ‐‐
Indicator VII.16: Actions to improve the public procurement process
The following actions were proposed by KIs to improve the systems and processes of public
sector procurement in Kenya:
a. Autonomy: Make the procurement function independent to avoid political
interference and avoid corruption; ensure that procurement of both pharmaceuticals
and non‐pharmaceuticals is centrally done from the central medical stores (KEMSA).
b. Procurement process: Review procurement operations in line with the law and
ensure strict follow up; avoid procurement from middlemen where it is possible to
get the commodities from the manufacturers or appointed agents; ensure accurate
and reliable quantification; strengthen supervision of the procurement function; and
ensure accurate and reliable quantification.
c. Capacity building: Train procurement staff and build capacity to apply and adhere
to procurement laws.
d. Quality control: Require that all bidders supply samples for prior analysis;
emphasize quality over price to reduce dumping of substandard products in the
country.
e. Audit: Strengthen and operationalize the Public Procurement and Oversight
Authority (PPOA); strengthen procurement audit.
f. Enforce principles of good governance, a system that works starting from the tender
committee membership.
3.8. Distribution of medicines
Distribution of pharmaceuticals is done by KEMSA. Both quality assurance staff and
warehouse staff are involved in receiving and verifying medicines received from suppliers.
Partial consignments are usually accompanied by a delivery note. Products are arranged
taking into account their expiry and there is a security management system. SOPs for stock
management exist at each level of the distribution system. There are inventory records and
procedures in the warehouses at the various levels of the distribution system. The KEMSA
warehouses are subjected to both internal and external auditing by the national audit office
and other independent auditors at regular intervals. Both computerized and manual
systems exist and provide information on medicines that have left the warehouse to go to
health facilities. An elaborate procedure for requesting medicines, a communication system
between distributions points and a monitoring and evaluation programme all exist.
Sanctions to be imposed on individuals for theft or corrupt practices are as spelt out in the
Public Procurement Act.
Indicator VIII.1: Systems to expedite port clearing
Four (30.8%) KIs indicated that a system is in place to expedite port clearing. Five (38.5%)
said the indicator was not applicable since goods are delivered directly to the warehouse
and there is no need for port clearing. Two KIs from NGOs said a system is in place to
expedite port clearing. Two other KIs did not know. All medicines are delivered at the
central medical stores and hence the MoH procurement agency is not involved with clearing
from the port. The question was thus not applicable to KIs from KEMSA.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 36 ‐‐
Indicator VIII.2: Opinion about transparency of port clearing process
Table 23 shows that three KIs agree with the statement that the “Port clearing process is
done smoothly and there is no need for bribery or gift‐giving to expedite the process”. Four
disagreed. Five KIs said the question on port clearing was not applicable to their
procurement process. Indeed, the question was not applicable to the MoH distribution
system.
Table 23: Perception of key informants on transparency of port clearing in Kenya
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 1 1 0 2 0 5 1 10
Private 0 0 0 1 0 0 0 1
NGO 0 2 0 0 0 0 0 2
Total 1 3 0 3 0 5 1 13
DK: Don’t know. NA: Not applicable
Indicator VIII.3: Inspection system to verify that the medicines delivered match those shipped
All the KIs indicated that an inspection system exists to verify that the medicines delivered
from the port or directly from a supplier match those that were shipped from the supplier.
The receiving staff verifies the medicines received against the delivery note and copy of
purchase order issued to supplier. Both quality assurance staff and warehouse staff are
involved in receiving and verifying medicines received from suppliers. Partial consignments
are accompanied by a delivery note.
Indicator VIII.4: Coding system used to identify Government medicines
Ten KIs (76.9%) indicated that Government medicines carry the inscription “GOK
(Government of Kenya)/MoH: NOT FOR SALE” on both primary and secondary packaging.
Two from the NGOs did not know, while one from the private sector indicated that a coding
system does not exist. The KIs from MoH/KEMSA said that there are plans to print the code
on the tablets/capsules.
Indicator VIII.5: Shelving of products in warehouses or store rooms
Eleven (84.6%) KIs indicated that there is systematic and orderly shelving of products in
warehouses. Two (15%) indicated that there is no systematic and orderly shelving.
Medicines in warehouses are organized systematically according to dosage forms, such as
tablets and capsules, injections, syrups and suspensions, creams and ointments. Overall
arrangement is based on therapeutic action. A master map showing the location of
medicines does not exist. However products are arranged taking into account the expiry
dates to ensure FEFO (“first expiry, first out”).
Indicator VIII.6: Security management system to oversee storage and distribution
All the KIs indicated that there is a security management system in place to oversee storage
and distribution. Indeed, a security management system is in place and consists of

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 37 ‐‐
monitoring of entry and exit to and from warehouses as well as searches by security
personnel of those leaving the warehouse. There is limited access to unauthorized persons
and there are locks with controlled key distribution. Controlled substances such as narcotics
are separated and secured. However, alarm system for security is yet to be installed at the
central medical stores. Panic buttons are currently in use.
Indicator VIII.7: Standard operating procedures for stock management
Twelve KIs indicated that there are SOPs for stock management at each level of the
distribution system. Only one KI from a district hospital indicated that there are no SOPs in
place. SOPs for stock management exist at each level of the distribution system, but the
extent to which they are followed has not been determined.
Indicator VIII.8: Inventory management system
All the KIs indicated that there is an inventory management system at each level of the
distribution system. There are inventory records and procedures in the warehouses at the
various levels of the distribution system. The inventory management system is however
inefficient and does not provide information on the following elements: the average working
stock; the amount of safety stock; the frequency of reordering; the quantity of reordering and
the average inventory. Only the expiry date and lead time are readily available from the
system. They also indicated that a system exists, but it is not regularly updated.
Indicator VIII.9: Reconciliation of stock records with physical counts
Ten KIs indicated that stock records are reconciled with physical counts at least every three
months by internal staff. Three (23.1%) said reconciliation is not done. The practice is such
that the warehouse staff carries out weekly cycle counts, monthly and annual stock counts
and reconciles the stock records with physical counts.
Indicator VIII.10: Independent audits of warehouses
Nine (69.2%) KIs indicated that there are independent audits of warehouses by external
inspectors or auditors, in particular the Government’s Auditor General every year. Four,
two from MoH and two from NGOs, did not think that independent audits are carried out.
The KEMSA warehouses are subject to both internal and external auditing by the national
audit office and other independent auditors at regular intervals. Annual audits are
mandatory and audit records are documented.
Indicator VIII.11: System to track the movement of pharmaceuticals from a warehouse to a health facility
Twelve of the 13 KIs indicated that there is a system in place to track the movement of
pharmaceuticals from a warehouse to health facilities. One KI from MoH did not know if a
system exists. Both computerized and manual systems exist and provide information on
medicines that have left the warehouse to health facilities, including: type of medicines that
have left the warehouse; quantity of medicines that have left the warehouse; the person who
verified the amounts; and the intended recipients of the medicines. The date when the
medicines arrived at the designated health facility is determined from the receipt stamp on
the delivery notes.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 38 ‐‐
Indicator VIII.12: Procedure for requesting medicines
All the KIs indicated that the health facilities have an appropriate procedure for requesting
medicines. An elaborate procedure for requesting medicines exists and involves filling of
requisition forms with name of medicine, dosage form, strength and quantity required. The
requisition is then checked by the responsible person, dated and signed and then forwarded
to the central medical stores.
Indicator VIII.13: Guidelines on transportation and delivery of medicines from and to warehouses
Four KIs indicated that there are no appropriately written guidelines on transportation and
delivery of medicines from and to warehouses. The other nine KIs explained that the
guidelines on transportation of medicines are provided in the service level agreement and
provide guidance on measures to take in case of adverse weather conditions, theft during
transportation, and how to protect against this. Measures to prevent swapping of
consignment during transportation are in place. The person responsible for transportation is
required to sign a receipt for the consignment.
Indicator VIII.14: Communication system between distribution points
All the KIs indicated that there is a well‐functioning communication system between
distribution points., which includes a manual/document exchange system between
distribution points at all levels and also telephone contact between all levels of the
distribution points. A computerized network system does not exist, but communication is
enhanced by regional and field liaison officers who make regular visits to the facilities.
Indicator VIII.15: Monitoring and evaluation of the performance of the medicine distribution system
Ten KIs indicated that a programme exists for monitoring and evaluating the performance
of the medicine distribution system. Two KIs from NGOs and one from MoH said that no
system exists. A programme exists for monitoring and evaluation of the performance of the
medicine distribution system, but the reports are not publicly available. Monitoring and
evaluation is done by the MoH, external auditors and through customer satisfaction surveys.
Indicator VIII.16: Sanctions for theft or other corrupt practices associated with distribution
Ten KIs indicated that sanctions are imposed on individuals or agencies/companies for theft
or other corrupt practices associated with distribution. Three (23.1%) thought otherwise.
However, there was no evidence that any individuals have been sanctioned for corrupt
behaviour. Sanctions to be imposed on individuals for theft or corrupt practices are as spelt
out in the Public Procurement Act. Procedures foreseeing the application of sanctions for
corrupt behaviour exist and include the type of sanctions to be applied depending on the
nature and gravity of the act of corruption. However there is no evidence of any individuals
sanctioned for corrupt behaviour.
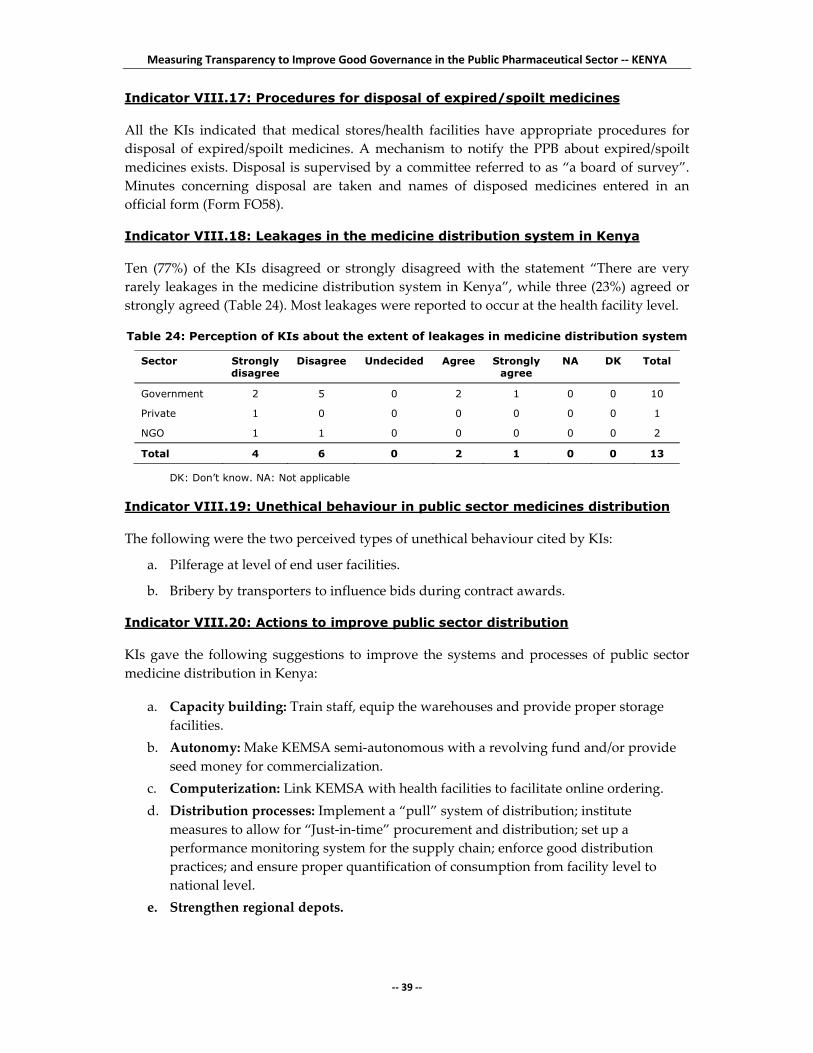
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 39 ‐‐
Indicator VIII.17: Procedures for disposal of expired/spoilt medicines
All the KIs indicated that medical stores/health facilities have appropriate procedures for
disposal of expired/spoilt medicines. A mechanism to notify the PPB about expired/spoilt
medicines exists. Disposal is supervised by a committee referred to as “a board of survey”.
Minutes concerning disposal are taken and names of disposed medicines entered in an
official form (Form FO58).
Indicator VIII.18: Leakages in the medicine distribution system in Kenya
Ten (77%) of the KIs disagreed or strongly disagreed with the statement “There are very
rarely leakages in the medicine distribution system in Kenya”, while three (23%) agreed or
strongly agreed (Table 24). Most leakages were reported to occur at the health facility level.
Table 24: Perception of KIs about the extent of leakages in medicine distribution system
Sector Strongly disagree
Disagree Undecided Agree Strongly agree
NA DK Total
Government 2 5 0 2 1 0 0 10
Private 1 0 0 0 0 0 0 1
NGO 1 1 0 0 0 0 0 2
Total 4 6 0 2 1 0 0 13
DK: Don’t know. NA: Not applicable
Indicator VIII.19: Unethical behaviour in public sector medicines distribution
The following were the two perceived types of unethical behaviour cited by KIs:
a. Pilferage at level of end user facilities.
b. Bribery by transporters to influence bids during contract awards.
Indicator VIII.20: Actions to improve public sector distribution
KIs gave the following suggestions to improve the systems and processes of public sector
medicine distribution in Kenya:
a. Capacity building: Train staff, equip the warehouses and provide proper storage
facilities.
b. Autonomy: Make KEMSA semi‐autonomous with a revolving fund and/or provide
seed money for commercialization.
c. Computerization: Link KEMSA with health facilities to facilitate online ordering.
d. Distribution processes: Implement a “pull” system of distribution; institute
measures to allow for “Just‐in‐time” procurement and distribution; set up a
performance monitoring system for the supply chain; enforce good distribution
practices; and ensure proper quantification of consumption from facility level to
national level.
e. Strengthen regional depots.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 40 ‐‐
4. DISCUSSION
4.1. Registration of medicines
The average final score for registration was 4.36 indicating moderate vulnerability to
corruption. The requirements for those applying are fairly well documented. The guidelines
for applicants on how to submit an application for registration of medicinal products are
comprehensive, clearly written and on the web site. There is a standard application form
publicly available for submission of applications, which can be found at the PPB secretariat
and on the web site. In addition, there is an up‐to‐date list of all registered pharmaceutical
products, which provides sufficient information.
There is a functioning formal committee that is responsible for assessing applications for
registration of medicines. The committee meets at least once a week and keeps minutes of its
meetings. However, there are no written criteria for selecting members of this committee,
and there is no document that describes the composition and terms of reference of the
committee. There are no written procedures for assessors on how to assess applications
submitted for registration of medicines and there are no written guidelines for the
committee’s decision‐making process. Also, there are no written guidelines describing how
and where medicines registration officers should meet with applicants, and none on COI
with regard to registration activities. It is assumed that officers with COI will declare them.
Applicants who have their applications rejected by the committee make formal appeals to
the PPB.
The most cited complaints by KIs were the presence of too many generics; and too many
counterfeit/substandard medicines and unregistered medicines in the market. Many also
thought that the registration process is not free from influence.
4.2. Licensing of pharmaceutical establishments
The average final score for licensing was 5.21 indicating moderate vulnerability to
corruption. There is a low level of awareness in the area of licensing in Kenya because
procedures and guidelines are not widely disseminated. The unit responsible for licensing is
established under the Inspectorate Department of the PPB. The guidelines for licensing were
published in June 2006. The process is also clearly spelt out in the service charter, which is
publicly available and covers administrative criteria to be met by applicants; and a
description of the requirements to be met in terms of premises, facilities and personnel. The
application fee structure is also indicated in the guidelines. A time frame for processing
applications is given. There are two formal committees that assess applications for licensing
of a pharmaceutical establishment at the PPB ‐ one assesses applications for licence renewals
(PPB Management Committee) and the other assesses applications for new licences (Practice
Committee). Post‐licensing inspection of licensed pharmaceutical establishments is erratic
and done on an ad hoc basis. The reason given is lack of adequate financial and human
resource capacity. In essence it is supposed to be done annually.
There was no evidence of an up‐to‐date list of all licensed pharmaceutical establishments
available in Kenya. A 2007 list exists, but mainly has the names of wholesalers and
manufacturers. The list available on the PPB web site is not updated. There is no ‘validity
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 41 ‐‐
date’ on the licences issued for the establishments. Once a licence is given, it is assumed to
be on‐going.
There is no independent appeals system for applicants who have their applications for
licensing rejected. However, the guidelines indicate that in the case of an unsuccessful
application, the applicant will be given further opportunity to revise the application and re‐
apply.
The most commonly mentioned unethical behaviour was the subjectivity of the licensing
officers, which was attributed to them being influenced by licensees through various means,
including bribes. Unqualified persons have also been allowed to operate pharmaceutical
establishments and inspectors can be hostile and unethical.
4.3. Inspection and market control of medicines
Inspection and market control of medicines had an average final score of 3.95, which
indicates that the function is very vulnerable to corruption. There is a comprehensive
provision in the medicines legislation covering inspection of pharmaceutical establishments.
There are written guidelines for GMP and also for GDP for pharmaceutical products in
Kenya. However, these guidelines do not classify non‐compliance with GMP or GDP, nor do
they describe types of deficiencies and measures to be taken by the PPB. There are written
SOPs for inspectors on how to conduct inspection and the inspection findings and
conclusions are subject to an internal review. There are, however, no written criteria for
selection and recruitment of inspectors, and there are no written guidelines on COI with
regard to inspection activities. No written procedures exist to prevent regulatory capture
between inspectors and the manufacturing and distributing companies inspected.
KIs frequently indicated that inspectors are unethical and that their decisions are influenced
by personal gain. Proprietors of establishments also try to bribe inspectors, and there is poor
enforcement of the law by the PPB.
4.4. Medicines promotion control
The average final score for medicines promotion control was 4.53 indicating moderate
vulnerability to corruption. Advertising and promotion of medicines is governed by the
Laws of Kenya Cap 244 subsections 36‐409. The provisions mention the following areas:
advertisement to professionals, advertisement to public, qualification and training of
medical representatives, restrictions on and monitoring of free samples, and packaging,
labelling and package inserts. However, it is silent on symposia and scientific meetings,
post‐marketing scientific studies, speaker’s fees and consultancies, promotion of exported
drugs, and restrictions and limits on gifts and gimmicks. The provisions on enforcement
spelt out in subsection 36‐40 of Cap 244 of the Laws of Kenya include sanctions and indicate
the type of penalties to be imposed on any person or pharmaceutical company for breaching
the law.
At management level there is a promotions committee that vets medicines promotion
advertisements. It is done within a department in the PPB, not through a committee per se.
There is thus no Government service or committee responsible for monitoring and enforcing
the provisions on drug promotion.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 42 ‐‐
The unethical behaviour in the promotion area involves influencing doctors to prescribe
certain products through giving incentives, companies making biased and false claims,
approval of promotion for non‐registered medicines, weak regulation of promotions and
late interventions to address unethical behaviours.
4.5. Control of clinical trials
The average final score for control of clinical trials was 6.25, which indicates marginal
vulnerability to corruption. There is legal provision for the regulation of clinical trials in
Kenya which is provided in the Laws of Kenya, the Science and Technology10 Act of 1979.
The documentation for guidelines for control of clinical trials is fairly comprehensive. There
are written and publicly available guidelines on the submission of applications to the PPB to
conduct clinical trials and there is also a documented procedure for submission of
applications to the various institutional ethics and research committees. The PPB also has
requirements for the manufacture, importation, exportation and use of investigational
products.
The PPB has a formal Review Committee which is responsible for reviewing applications.
This Committee was constituted in 2007 and has not yet started reviewing clinical trials
results, although this is within its mandate. There is no established and operational system
for inspection of clinical trials. However, the study Data Monitoring Safety and Committees
monitor the studies and the ERCs have been trying to inspect trials that they have approved.
However, due to limited capacity, this is not comprehensive. According to the service
charter of the PPB, the evaluation of the application and subsequent approval or rejection
must be completed within two months. There are no written guidelines on COI with regard
to clinical trials activities.
Although the PPB selects assessors who have the expertise in the required areas, there is no
documented mechanism to ensure that those involved in the review of applications have
sufficient and current expertise in all the required areas.
There are no national guidelines on principles of GCP and researchers generally apply the
International Conference on Harmonisation of Technical Requirements for Registration of
Pharmaceuticals for Human Use (ICH) guidelines on GCP. The national guidelines from the
National Council of Science and Technology13 recommend that review of clinical trials
should have independence. However, there is no requirement, and no guidelines for the
establishment of an Independent Ethics Committee, and currently there is none in the
country.
In the area of clinical trials, most of the unethical behaviours cited revolved around the
activities of researchers. Anomalies included carrying out trials without approval; exporting
biological samples without approval; doing studies without informed consent; not reporting
adverse effects and falsification of data. Some promoters do not declare all known
information about the study and some investigational products are used without being
approved by the PPB. The regulators do not ensure the independence of reviews nor do they
clear declarations of COI and there is no inspection of on‐going trials.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 43 ‐‐
4.6. Selection of medicines
Selection of medicines had the lowest average final score of 2.95 and this shows that this
function is very vulnerable to corruption. The essential medicines list is in line with WHO
procedures, but it was last updated in 2002. There are no written criteria for the selection
process for including or deleting medicines from the national list.
In the past, the EML has been drawn up by ad hoc committees of experts. A National
Medicines and Therapeutics Committee (NMTC) was constituted in 2007 with the mandate
of selection of medicines, but it is not yet operational. There are clear criteria for the selection
of members of the NMTC and terms of reference that describe the role and responsibilities of
the NMTC, which have been developed over the last year but most stakeholders are not
aware of their existence. There are no written guidelines on COI with regard to selection of
essential medicines and the NMTC has no SOPs for their decision making.
The unethical behaviour in the selection area consists mainly of pharmaceutical companies
influencing officers to have their drugs included in lists, a selection process that is not
evidence‐based, and inappropriate representation in Selection Committees.
4.7. Procurement of medicines
The average final score for procurement of medicines was 7.01 which indicates marginal
vulnerability to corruption. Public sector procurement of medicines is done by Kenya
Medical Supplies Agency (KEMSA). Procedures for procurement exist and are heavily
informed by the newly published Public Procurement and Disposal Act12. This document is
publicly available and requires: the use of generic names; the advertisement of tenders; that
contract specification be publicly available to all bidders; that the criteria for adjudication of
tenders be included as part of the tender package and all bidders informed in advance; and
that the information on the tender process and results be made public. Tender Committee
membership is defined by the Public Procurement Act, which requires professionals with
specific skills. The law requires members to declare COI, it is however silent on how often
the membership is required to change and does not include representation from client
facilities. A description of the internal process to be followed by the procurement staff on
how to process the bids is available to the staff. However interference with decisions of the
Tender Committee by interested parties cannot be ruled out.
The Procurement Office monitors supplier performance during every tender for compliance
with the contract terms, the monitoring system tracks supplier’s lead‐time, delivery status,
shelf life, and the packaging of products. Product quality is also tracked, and suppliers with
poor performance are barred from future tenders.
The most common unethical behaviour in procurement is pharmaceutical companies
lobbying senior Government officials and politicians for procurement of certain products,
using gifts and bribery. Companies that are bidding also indulge in malpractices such as
double invoicing and inflating medicine prices.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 44 ‐‐
4.8. Distribution of medicines
Distribution of medicines had the highest of all scores, 7.82, indicating marginal
vulnerability to corruption. Distribution of pharmaceuticals is done by Kenya Medical
Supplies Agency (KEMSA), which is the central medical stores for the MoH. Most medicines
carry the inscription “GOK (Government of Kenya)/MoH: NOT FOR SALE” on both
primary and secondary packaging. There are plans to print the code on the tablets/capsules
as well. All commodities procured are delivered directly to KEMSA warehouses from the
suppliers. The receiving staff verify the medicines received against the delivery note and a
copy of the purchase order is issued to the supplier. Both quality assurance staff and
warehouse staff are involved in receiving and verifying medicines from suppliers. Partial
consignments are usually accompanied by a delivery note.
A master map showing the location of medicines does not exist. However, products are
arranged taking into account the expiry dates to ensure FEFO (“first expiry, first out”). A
security management system is in place and consists of monitoring warehouse entries and
exits as well as searches of those leaving the warehouse by security personnel. There is
limited access to unauthorized persons and locks with controlled key distribution.
Controlled substances such as narcotics are separated and secured. However, a security
alarm system is yet to be installed at the central medical stores. Panic buttons are currently
in use.
SOPs for stock management exist at each level of the distribution system but the extent to
which they are followed has not been determined. There are inventory records and
procedures in the warehouses at the various levels of the distribution system. The inventory
management system is however inadequate and does not provide information on the
following elements: the average working stock; the amount of safety stock; the frequency of
reordering; the quantity of reordering and the average inventory. Only the expiry date and
lead time are readily available from the system.
The KEMSA warehouses are subjected to both internal and external auditing by the national
audit office and other independent auditors at regular intervals. Audit reports are on file.
Annual audits are mandatory.
Both computerized and manual systems exist and provide information on medicines that
have left the warehouse to health facilities including: type of medicines that have left the
warehouse; quantity of medicines that have left the warehouse; the person who verified the
amounts and the intended recipients of the medicines. The date when the medicines arrived
at the designated health facility is determined from the receipt stamp on the delivery notes.
An elaborate procedure for requesting medicines exists and involves filling in requisition
forms with the name of the medicine, dosage form, strength and quantity required. The
requisition is checked by the responsible person, dated and signed and then forwarded to
the central medical stores. A pull system is used for bi‐monthly deliveries to hospitals and a
push system for rural health facilities which receive supplies on a quarterly basis.
There is a communication system between distributions points, which includes a
manual/document exchange system between distribution points at all levels and telephone

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 45 ‐‐
contact also between all levels of the distribution points. A networked computerized system
does not exist but communication is enhanced by regional and field liaison officers who
make regular visits to the facilities. A programme exists for monitoring and evaluating the
performance of the medicine distribution system but the reports are not publicly available.
Monitoring and evaluation is done by the MoH, external auditors and through customer
satisfaction surveys.
Sanctions to be imposed on individuals for theft or corrupt practices are as spelt out in the
Public Procurement Act. Procedures foreseeing the application of sanctions for corrupt
behaviour exist and include the type of sanctions to be applied depending on the nature and
gravity of the act of corruption. However, there is no evidence of any individuals being
sanctioned for corrupt behaviour.
5. CONCLUSIONS
Registration of medicines: The average final score for registration was 4.36 indicating
moderate vulnerability to corruption. The requirements for applicants are fairly well
documented. They include a standard application form for submission of applications for
registration of medicines, guidelines on how to submit the application and a list of
registered medicines available. There is a committee which meets regularly to assess
applications for registration of medicines, and applicants who have their applications
rejected by the committee can make formal appeals to the PPB. However, there are no
written guidelines on selection criteria for members of this committee, on the composition
and terms of reference of the committee, procedures on how to assess applications, how and
where medicines registration officers meet with applicants and on COI with regard to
registration activities. To improve transparency, procedures used by registration officers and
committee members at the PPB should all be documented and implemented, the number of
registered medicines in the market should be reduced, all medicines should be analysed
before registration, and interaction between various departments of the PPB should be
enhanced.
Licensing of pharmaceutical establishments: The average final score for licensing was 5.21
indicating moderate vulnerability to corruption. There is provision in the law for licensing of
pharmaceutical establishments, and the Medicines Regulatory Authority has a unit and a
committee for licensing activities. There are written procedures on how to submit
applications for licensing and to assess applications. Although a pre‐licensing inspection
report is required before issuing of a licence, post‐licensing inspection of establishments is
erratic and done on an ad hoc basis. There is a list of licensed pharmaceutical
establishments, but it is neither comprehensive nor up‐to‐date. There are no written
guidelines on selection criteria for members of this committee, or on its composition and
terms of reference. No independent appeals system for applicants who have their
applications for licensing rejected exists. In order to reduce the level of vulnerability of the
licensing function, the Food and Chemical Substances Act should be reviewed. The PPB
should build capacity to carry out regular inspection of all establishments and close down
all unlicensed ones. Procedures used by the licensing unit at the PPB should all be
documented and implemented, and a well defined appeals system should be put in place.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 46 ‐‐
Inspection and market control of medicines: Inspection and market control of medicines had
an average final score of 3.95, which indicates that the function is very vulnerable to
corruption. There is a comprehensive provision in the medicines legislation covering
inspection of pharmaceutical establishments and written SOPs for conducting inspections.
There are written guidelines for GMP and also for GDP for pharmaceutical products in
Kenya, but these guidelines do not classify non‐compliance with GMP or GDP. There are,
however, no written criteria for the selection and recruitment of inspectors and there are no
written guidelines on COI with regard to inspection activities. No written procedures exist
to prevent regulatory capture between inspectors and the manufacturing and distributing
companies inspected. Procedures used by the inspection unit of the PPB should all be
documented and implemented, the capacity of the inspectorate should be increased to
enable regular inspections and the law should be enforced for errant establishments. The
interaction and sharing of information between the drug registration, pharmacovigilance
and inspection departments within the PPB should be strengthened.
Drug promotion control: The average final score for medicines promotion was 4.53
indicating moderate vulnerability to corruption. There is a provision within the pharmacy
legislation covering promotion and advertising of medicines with clear penalties for any
person who breaches the law. Pre‐approval of promotional material is required. There is a
promotions service that vets medicines promotion advertisements, but monitoring and
enforcing the provisions on drug promotion are very weak. SOPs for the service for
medicines promotion are being developed. However, there are no written guidelines on
selection criteria for members of the promotion service unit, the composition and terms of
reference of the committee and on COI with regard to promotion activities. There is no
written procedure to report unethical promotional practices. To decrease vulnerability to
corruption, the law should be amended to include control of promotion of herbal and
complimentary medicines, and strict penalties for unethical behaviour. Comprehensive
guidelines for control of medicines promotion should be developed and used to vet all
promotional materials. The PPB should create awareness in the public about the process of
regulation of promotion materials.
Control of clinical trials: The average final score for control of clinical trials was 6.25 which
indicates marginal vulnerability to corruption. There is legal provision for the regulation of
clinical trials in the Science and Technology Act. There are guidelines on the submission of
applications to the PPB to conduct clinical trials and to the various institutional ethics and
research committees. The PPB has a committee which is responsible for reviewing
applications. It also has requirements for the manufacture, importation, exportation and use
of investigational products. There is no system for inspection of clinical trials and no written
guidelines on selection criteria for members of the PPB and ERC committees and on COI
with regard to control of trials. There are no national guidelines on principles of GCP and
none for the establishment of an Independent Ethics Committee. Transparency can be
enhanced by review of the law, building capacity of the ERCs and PPB clinical trials
committees, developing guidelines for all the committees’ decision‐making process,
establishing an independent clinical trials’ inspection system and making a list of all
approved and rejected clinical trial applications. An Independent Ethics Committee should
be created and interaction between researchers, NCST, ERCs, MoH and the PPB needs to be
encouraged.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 47 ‐‐
Selection of medicines: Selection of medicines had the lowest average final score of 2.95,
showing that this function is very vulnerable to corruption. The essential medicines list is in
line with WHO procedures, but it was last updated in 2002. There are no written criteria for
the selection process for including or deleting medicines from the national EML. An NMTC
was constituted in 2007, but it is not yet operational. There are clear criteria for the selection
of members of the NMTC and terms of reference that describe the role and responsibilities of
the NMTC, which were developed over the previous year, but most stakeholders are not
aware of their existence. There are no written guidelines on COI with regard to selection of
essential medicines and the NMTC has no SOPs for their decision making. Operationalizing
the NMTC, implementing the use of existing documents and publicizing the selection
process will improve the selection function. An evidence‐based survey to establish which
medicines would cater for the bulk of health needs should be carried out.
Procurement of medicines: The average final score for procurement of medicines was 7.01,
which indicates marginal vulnerability to corruption. Transparent and explicit procedures
for procurement exist and are heavily informed by the Public Procurement and Disposal
Act. A description of the internal process to be followed by the procurement staff on how to
process the bids is available to the staff. The Procurement Office monitors supplier
performance during every tender for compliance with the contract terms and it is also
audited on a regular basis. Product quality is also tracked, and suppliers with poor
performance are barred from future tenders. There is a Tender Committee whose functions
are clearly separated from the functions of the Procurement Office. However interference
with decisions of the Tender Committee by interested parties cannot be ruled out. There is a
formal appeals process for applicants who have their bids rejected. There are no written
guidelines on COI with regard to procurement of medicines. To enhance transparency,
procurement should be independent of political interference and operations should adhere
to the law. Procurement staff should get regular training, audit should be strengthened and
the Public Procurement and Oversight Authority should be operationalized.
Distribution of medicines: Distribution of medicines had the highest of all scores, 7.82,
indicating marginal vulnerability to corruption. All procured commodities are delivered
from the suppliers directly to the central warehouses where they are verified. Most
medicines carry a Government identification inscription on both primary and secondary
packaging. A master map showing the location of medicines does not exist, but products are
arranged taking into account their expiry dates. A security management system, procedure
for requesting medicines, SOPs for stock management, computerized and manual
information systems, a monitoring and evaluation system, and a communication system
between distributions points are all in place. The warehouses are subject to regular internal
and external auditing. Sanctions to be imposed on individuals for theft or corrupt practices
are as spelt out in the Public Procurement Act. However, there is no evidence of any
individuals being sanctioned for corrupt behaviour. To strengthen procurement, KEMSA
should be made semi‐autonomous and be linked with health facilities to facilitate online
ordering based on proper quantification and GDP. There is a need to strengthen regional
depots and staff capacity building, and to construct and equip warehouses. A performance
monitoring system should be set up.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 48 ‐‐
6. RECOMMENDATIONS
6.1. General recommendations
1. Create a formal appeals system in each function
2. Improve communication between all players in the pharmaceutical sector:
MoH, PPB and the pharmaceutical industry
3. Improve data management systems to provide instant information and
regularly update and publicize all documents
4. Build the human resource capacity in each of the sectors
5. Institutionalize declaration of COI for each of the functions.
6.2. Specific recommendations
6.2.1. Registration of medicines
a. Develop the following documents and implement their use, review them
regularly and widely disseminate them:
guidelines setting limits on how and where medicines registration
officers meet with applicants
criteria for selecting the members of the Registration Committee
guidelines on the composition and terms of reference of the Registration
Committee
guidelines for the Committeeʹs decision‐making process
b. Reduce the number of registered products in the market through:
limiting the number of generics registerable for any molecule
enforcing the withdrawal of all rejected and unregistered products in
the market
c. Improve interaction and sharing of information between the drug registration,
inspection and importation departments within the PPB
d. Ensure that all medicines are analysed before registration and strengthen
market surveillance.
6.2.2. Licensing of pharmaceutical establishments
a. Review of the Food and Chemical Substances Act (Cap 254). Public Health
Officers use this Act to issue Food and Drugs Certificates to shopkeepers. This
has been misused as a legal instrument for opening illegal drug outlets
b. Develop licensing guidelines and make them easily and publicly available
c. The PPB should establish an on‐line system for application for licensing,
shorten the time taken to process and approve applications, and decentralize
licensing to provinces and districts
d. De‐link the PPB from the MoH to enhance its independence as a national
medicines regulator
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 49 ‐‐
e. The PPB should carry out an audit of licensed and unlicensed establishments,
maintain an up‐to‐date database and close all the unlicensed establishments
f. The PPB should improve human resource capacity to carry out regular
inspections and enforce annual renewal of licences. Enforce adherence to
licensing guidelines, regular rotation of inspectors and regular inspections of
establishments
g. Establish guidelines for the composition and selection criteria for the Licensing
Committee and develop TORs for the Practice Committee.
6.2.3. Inspection and market control of medicines
a. Develop the following documents and implement their use, review them
regularly and widely disseminate them:
procedures to prevent regulatory capture between inspectors and the
manufacturers or distributors
SOPs for conducting inspections
criteria for the selection and recruitment of inspectors
guidelines on COI with regard to inspection activities
guidelines for the internal review of inspection findings
b. Increase the capacity of the inspectorate:
in personnel numbers, and have inspectors at all ports of entry
by training
c. Enforce the law with regard to inspection activities:
by acting on the findings of inspectors, including closing down non‐
conforming establishments
disciplining unethical inspectors
d. Have regular schedules of inspections and also have impromptu inspections
e. Improve interaction and sharing of information between drug registration,
pharmacovigilance and inspection departments within the PPB.
6.2.4. Medicines promotion control
To improve medicines promotion, the following recommendations should be
considered:
a. The PPB and MoH should explore strategies to create public awareness of the
process of regulation of promotion materials by instituting mass media
campaigns to educate the public on the dangers of unethical medicines
promotion
b. The law should be amended to include control of herbal and complementary
medicines, and also introduce strict penalties for unethical behaviour and
empower the PPB to penalize the offenders. All promotional materials should
be vetted to ensure that only registered products are promoted
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 50 ‐‐
c. Set up an inspectorate to police promotion of medicines in the country and
ensure medical representatives are well trained and ethical in medicines
promotion
d. Constitute a promotions control committee that includes non‐medical
practitioners such as civil society groups and consumer organizations
e. Develop and strengthen guidelines and SOPs for control of medicines
promotion.
6.2.5. Control of clinical trials
a. Review legislation regulating clinical trials as a stand alone law on clinical
trials instead of the current law which clusters clinical trials under biomedical
research
b. Develop the following documents and implement their use, review them
regularly and widely disseminate them:
national guidelines on principles of Good Clinical Practice
guidelines on composition and criteria for selecting the members of the
PPB clinical trials committee and the ethics and research committees
guidelines on COI with regard to clinical trials activities
guidelines for the committeeʹs decision‐making process
a list of all approved and rejected clinical trial applications in the
country.
c. Establish:
an operational clinical trials inspection system
an Independent Ethics Committee.
d. Increase the capacity of ERCs and PPB Clinical Trials Committee:
by training them to attain international standards
to expedite the review process to make it shorter
supplement the capacity by sourcing for review expertise beyond
Kenya.
e. Enforce the law with regard to inspection activities:
by ensuring all investigational products are registered
by disciplining errant researchers and sponsors.
f. Improve interaction and sharing of information between researchers, NSCT,
ERCs, MoH and the PPB.
6.2.6. Selection of medicines
a. Operationalize the NMTC
give support at the highest level
implement and publicize the guidelines that have been developed on
the criteria for selection of members, and terms of reference that
describe the role and responsibilities of the NMTC members

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 51 ‐‐
b. Develop the following documents and implement their use, review them
regularly and widely disseminate them:
guidelines for the selection process for including or deleting medicines
from the national EML
guidelines for the Committeeʹs decision‐making process.
c. Do a survey to establish which drugs would cater for the bulk (90%) of health
needs. This would require data from practice. The survey should also establish
the quality, safety and efficacy of drugs
d. Publicize the selection process and involve all stakeholders.
6.2.7. Procurement of medicines
a. Ensure that procurement of both pharmaceuticals and non‐pharmaceuticals is
done centrally from KEMSA to ensure proper controls for the process and cut
out unnecessary bureaucratic procedures
b. Make the procurement function independent to avoid political interference
c. Review procurement operations in line with the law and ensure strict follow
up
d. Train procurement staff and build capacity to apply and adhere to
procurement laws
e. Strengthen and operationalize the Public Procurement and Oversight
Authority (PPOA). This will facilitate the enforcement of principles of good
governance
f. Strengthen procurement audit.
6.2.8. Distribution of medicines
a. Invest more in capacity building through staff training, equipping the
warehouses and provision of proper storage facilities
b. Make KEMSA semi‐autonomous with a revolving fund or through provision of
seed money for commercialization
c. Link CMS with health facilities to facilitate online communication
d. Set up a performance monitoring system for the supply chain and enforce GDP
e. Ensure proper quantification of consumption from facility level to national
level
f. Strengthen regional depots for faster and more cost effective service delivery.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 52 ‐‐
7. GLOSSARY
Auditing: Official examination of an organization or institutionʹs accounts to make sure
money has been spent correctly.
Bribery: Bribery is the act of offering someone money or other valuables, in order to
persuade him/her to do something for you. By definition bribery is corruption.
Conflict of interest: Conflict of interest means that the expert or his/her partner, or the
administrative unit with which the expert has an employment relationship, has a financial or
other interest that could unduly influence the expert’s position with respect to the subject‐
matter being considered.
Corruption: Behaviour on the part of officials in the public and private sectors, in which
they improperly and unlawfully enrich themselves and/or those close to them, or induce
others to do so, by misusing the position in which they are placed.
Easily accessible document: A document which is obtainable effortlessly when needed,
without delays or any bureaucratic obstacle.
Essential medicines: Medicines that satisfy the priority health‐care needs of the population.
They are selected with due regard to public health relevance, evidence on efficacy and
safety, and comparative cost‐effectiveness. Essential medicines are intended to be available
within the context of functioning health systems at all times in adequate amounts, in the
appropriate dosage forms, with assured quality and adequate information, and at a price the
individual and the community can afford.
Generic medicine: A pharmaceutical product usually intended to be interchangeable with
the innovator brand product, manufactured without a licence from the innovator
manufacturer and marketed after the expiry of patent or other exclusivity rights. Generic
medicines are marketed either under a nonproprietary name (INN), or occasionally another
approved name, rather than under a proprietary or brand name.
Governance: The traditions and institutions by which authority in a country is exercised for
the common good. In WHOʹs Good Governance for Medicines programme, good
governance refers to the formulation and implementation of appropriate policies and
procedures that ensure the effective, efficient and ethical management of pharmaceutical
systems, in particular medicine regulatory systems and medicine supply systems, in a
manner that is transparent, accountable, follows the rule of law and minimizes corruption.
Inspection: Entry by staff of the regulatory authority into premises where medicines are
manufactured stored and distributed to ensure that processes are carried out in accordance
with norms and standards, as well as the national legislation/regulation.
International Nonproprietary Name (INN): A common generic name selected by
designated experts, using procedures and guiding principles adopted by the WHO World
Health Assembly, for the unambiguous identification of a new pharmaceutical substance.
This name is often identical to the generic name.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 53 ‐‐
Licensing: Authorization by an official body to an individual, an institution or a company to
carry out a certain activity or business operation.
Marketing authorization: An official document issued by the competent medicine
regulatory authority for the purpose of the marketing or free distribution of a product after
evaluation for safety, efficacy and quality.
Medicine: Any dosage form containing a substance approved for the prevention and
treatment of disease. The term ʺmedicineʺ is increasingly used to distinguish it from a
medicine as a substance that is misused.
Medicine Regulatory Authority (MRA): A national agency which is established by
legislation to administer the full spectrum of medicine regulatory functions.
Pharmaceutical sector: Refers to the various actors (government, nongovernmental
organizations, private‐for‐profit organizations, private not‐for–profit organizations etc.)
engaged in activities such as the research, manufacture, import, export, distribution and sale
of medicines.
Pharmaceutical system: Refers to the relationship/interactions between the various actors of
the pharmaceutical sector and the way decisions are made in particular in the government.
Promotion: All informational and persuasive activities by manufacturers and distributors,
the effect of which is to induce the prescription, supply, purchase and/or use of medicinal
products.
Publicly available document: A document which is found openly, widely, with no
restrictions and usually in more than one media (i.e. soft copy; website; hard copies; at a
Governmental office, documentation centre or in a national gazette).
Registration: Any statutory system of approval required at national level as a pre‐condition
for introducing a pharmaceutical product on the market.
State capture: The phenomenon in which outside interests (often the private sector, mafia
networks, etc.) are able to bend state laws, policies and regulations to their (mainly financial)
benefit through corrupt transactions with public officers and politicians.
Transparency: Transparency means clearness, honesty and openness. Transparency is the
principle that those affected by administrative decisions should be informed, and the duty of
civil servants, managers and trustees is to act visibly, predictably and understandably.
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 54 ‐‐
8. REFERENCES
1. Hogerzeil HV. Access to Essential Medicines as a Human Right. Essential Medicines
Monitor, 2003; 33:26‐27. (http://apps.who.int/medicinedocs/pdf/s4941e/s4941e.pdf
http://apps.who.int/medicinedocs/en/d/Js5416e/)
2. WHO Medicines Strategy 2004 ‐ 2007: Countries at the Core. Geneva, World Health
Organization, 2004 (http://apps.who.int/medicinedocs/en/d/Js5416e/)
3. Kenya National Pharmaceutical Policy, 2007.
4. Ministry of Health National Health Accounts, 2003.
5. WHO Statistical Information System (WHOSIS), February 2007.
6. The Abuja Declarations 2001 and 2006, Abuja, Nigeria.
(http://www.rbm.who.int/docs/Abuja_declaration.pdf)
7. Kenya Health Policy Framework. Nairobi, Ministry of Health, 1994.
8. Kenya National Drug Policy. Nairobi, Ministry of Health, 1994.
9. Laws of Kenya, The Pharmacy and Poisons Act, Chapter 244.
10. Laws of Kenya, The Science and Technology Act, 1979
11. Pharmacy and Poisons Board; Customer Service Charter, 2008.
12. Kenya Gazette. The Public Procurement and Disposal Regulations, 2006 – Legal notice
No. 174.
13. Guidelines for Ethical Conduct of Biomedical Research Involving Human Subjects in
Kenya. NCST No. 45. 2005. National Council of Science and Technology, Nairobi, Kenya.

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 55 ‐‐
9. ANNEXES

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 56 ‐‐
Annex 1: Score sheets
Key to score sheets 1-8
* Profession:
G = Government or public official
P = Private sector (national or international)
N = Nongovernmental organization (national or international)
IO = International governmental organization
M = Media
O = Other
** The average for each question is calculated only on valid responses and all DK and NA answers are discarded *** score = total average/number of indicators x 10
M ethod 3
SD = Strongly disagree
DI = Disagree Note:
Method 3 and Method 4 questions (M3, M4) are not part of the quantitative aspect of the assessment because they are not expressed with numbers/quantities. They are the base for the qualitative part of the assessment. For this reason M3 and M4 questions are not calculated in the totals and/or averages present in this consolidation table.
UD = Undecided
AG = Agree
SA = Strongly agree
DK = Do not know
NA = Not applicable

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 57 ‐‐
Score Sheet 1
Country name: Period assessment carried out:
Registration
Kenya
June-July 2008
Method
KI 1 KI 2 KI 3 KI 4 KI 5 KI 6 KI 7 KI 8 KI 9 KI 10 KI 11 KI 12 KI 13 KI 14 KI 15 Total Average per question**
Profession* --- G G G G G G O O O P G G P P
Indicator I.1 M1 1 1 1 0 1 1 1 1 1 0 1 0 1 0 10 0.71
Indicator I.2 M2 1 0.5 0.63 0.63 0.88 0.88 0.63 1 DK 0.8 0.5 0.38 0.86 0.38 9.07 0.70
Indicator I.3 M2 0.86 0.86 0.86 0.86 0.86 0.86 0.86 0.71 1 0.86 0.86 0.19 0.86 0 10.5 0.75
Indicator I.4 M2 0.67 0.67 0.67 0.17 0.67 0.83 0 0 0 DK 0 DK DK 0 3.68 0.33
Indicator I.5 M2 1 1 0.88 0.88 1 1 1 1 1 1 1 0.86 1 0.75 13.37 0.96
Indicator I.6 M1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0.00
Indicator I.7 M1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 14 1.00
Indicator I.8 M2 0 0 0 0 0 0 0 0 0 DK 0 DK DK DK 0 0.00
Indicator I.9 M2 0 0 0 0 0 0 0 0 0 DK 0 DK DK 0 0 0.00
Indicator I.10 M2 0 0 0 0 0 0 0 0 0 DK DK DK DK 0 0 0.00
Indicator I.11 M3 DK NA AG DI AG SA AG NA DI NA AG DI NA DI
Indicator I.12 M2 0 0 - 0 0 0 0 0 0 DK 0 DK DK 0 0 0.00
Indicator I.13 M1 1 0 1 1 1 1 1 1 1 0 1 1 1 0 11 0.79
Indicator I.14 M3 UD SA SA AG AG UD DI DK SA DI DI SD SD DI
Indicator I.15 M3 SA SA SA SA SA SA SA SA SA AG SA AG AG AG
Indicator I.16 M4 see text in narrative report
Indicator I.17 M4 see text in narrative report
Total 5.24
***Final score Registration 4.36

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 58 ‐‐
Score Sheet 2
Country name: Period assessment carried out:
Licensing
Kenya
June-July 2008
Method
KI 1 KI 2 KI 3 KI 4 KI 5 KI 6 KI 7 KI 8 KI 9 KI 10 KI 11 KI 12 KI 13 KI 14 KI 15 Total Average per question**
Profession* --- G P O G P P P P P P P P O
Indicator II.1 M1 1 1 1 1 1 1 1 1 1 1 1 1 1 13 1.00
Indicator II.2 M1 1 1 1 1 1 1 1 1 1 1 1 1 1 13 1.00
Indicator II.3 M2 0.83 0 1 1 0.67 0.67 0 0.83 0 0.33 0.83 0.8 0.6 7.56 0.58
Indicator II.4 M1 1 0 1 1 0 0 0 DK 0 0 0 DK 0 3 0.27
Indicator II.5 M2 1 0 1 1 1 1 1 1 1 1 0 0 1 10 0.77
Indicator II.6 M2 1 0 1 1 1 1 1 DK 0 DK DK DK 1 7 0.78
Indicator II.7 M2 0 NA 0 0 0 0 DK NA DK DK DK NA 0 0 0.00
Indicator II.8 M2 0 NA DK 0 0 0 DK NA DK DK DK NA 0 0 0.00
Indicator II.9 M1 1 0 0 1 0 0 1 0 0 1 0 0 0 4 0.31
Indicator II.10 M2 0.6 0.4 0 1 0.8 1 1 1 DK 0.8 0.4 0.75 0.5 8.25 0.69
Indicator II.11 M3 SA D SD SA D A SD UN SD AG D UN D
Indicator II.12 M1 1 0 0 0 1 0 1 0 0 DK DK DK DK 3 0.33
Indicator II.13 M3 SA SD SD SA D A UN UN D DK DK DK A
Indicator II.14 M4 see text in narrative report
Indicator II.15 M4 see text in narrative report
Total 5.73
***Final score Licensing 5.21
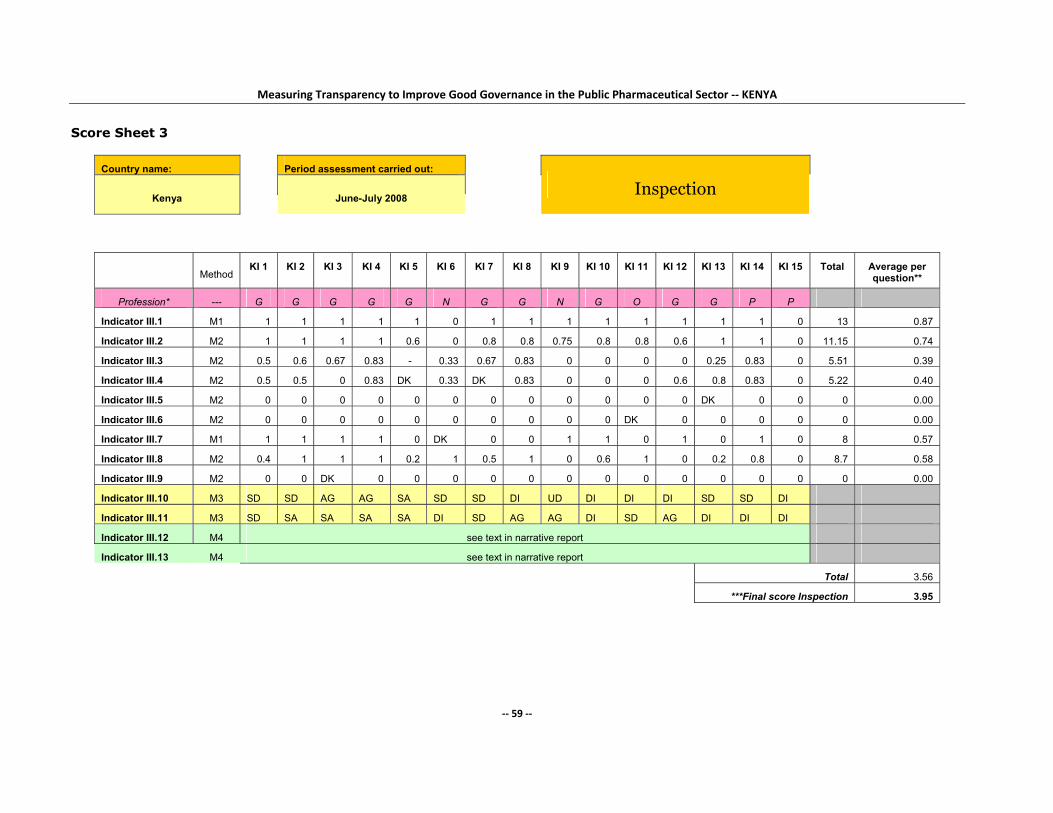
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 59 ‐‐
Score Sheet 3
Country name: Period assessment carried out:
Inspection
Kenya
June-July 2008
Method
KI 1 KI 2 KI 3 KI 4 KI 5 KI 6 KI 7 KI 8 KI 9 KI 10 KI 11 KI 12 KI 13 KI 14 KI 15 Total Average per question**
Profession* --- G G G G G N G G N G O G G P P
Indicator III.1 M1 1 1 1 1 1 0 1 1 1 1 1 1 1 1 0 13 0.87
Indicator III.2 M2 1 1 1 1 0.6 0 0.8 0.8 0.75 0.8 0.8 0.6 1 1 0 11.15 0.74
Indicator III.3 M2 0.5 0.6 0.67 0.83 - 0.33 0.67 0.83 0 0 0 0 0.25 0.83 0 5.51 0.39
Indicator III.4 M2 0.5 0.5 0 0.83 DK 0.33 DK 0.83 0 0 0 0.6 0.8 0.83 0 5.22 0.40
Indicator III.5 M2 0 0 0 0 0 0 0 0 0 0 0 0 DK 0 0 0 0.00
Indicator III.6 M2 0 0 0 0 0 0 0 0 0 0 DK 0 0 0 0 0 0.00
Indicator III.7 M1 1 1 1 1 0 DK 0 0 1 1 0 1 0 1 0 8 0.57
Indicator III.8 M2 0.4 1 1 1 0.2 1 0.5 1 0 0.6 1 0 0.2 0.8 0 8.7 0.58
Indicator III.9 M2 0 0 DK 0 0 0 0 0 0 0 0 0 0 0 0 0 0.00
Indicator III.10 M3 SD SD AG AG SA SD SD DI UD DI DI DI SD SD DI
Indicator III.11 M3 SD SA SA SA SA DI SD AG AG DI SD AG DI DI DI
Indicator III.12 M4 see text in narrative report
Indicator III.13 M4 see text in narrative report
Total 3.56
***Final score Inspection 3.95
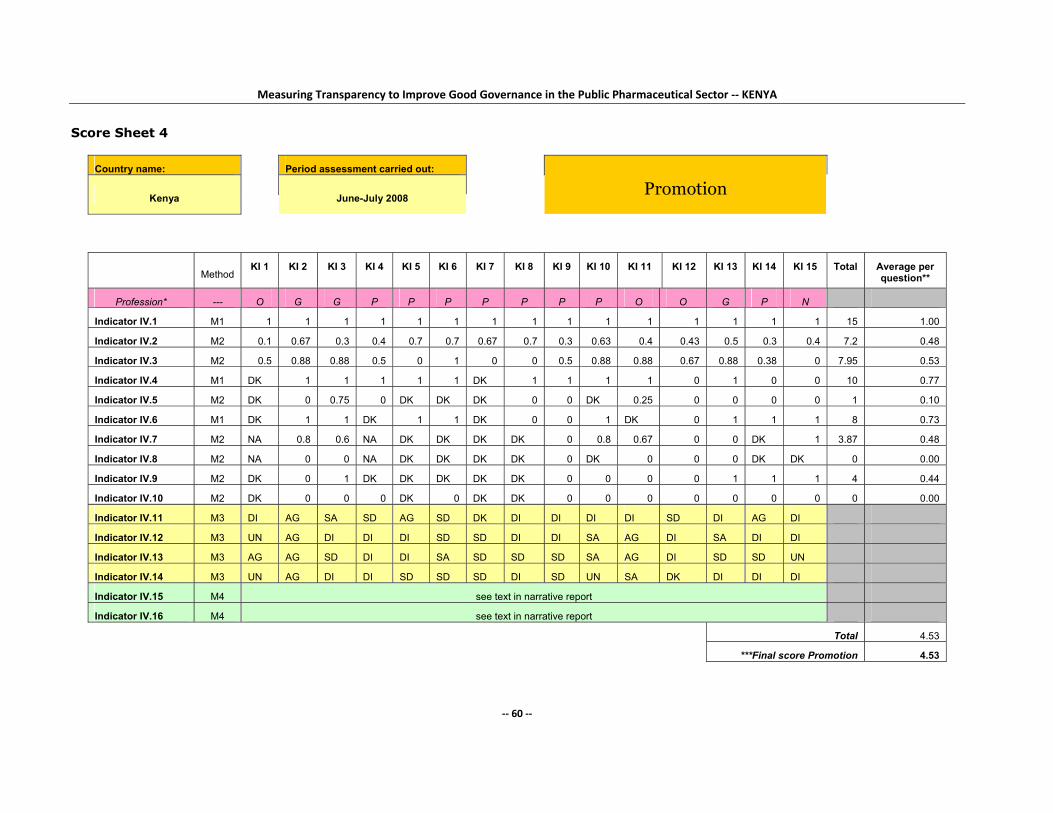
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 60 ‐‐
Score Sheet 4
Country name: Period assessment carried out:
Promotion
Kenya
June-July 2008
Method
KI 1 KI 2 KI 3 KI 4 KI 5 KI 6 KI 7 KI 8 KI 9 KI 10 KI 11 KI 12 KI 13 KI 14 KI 15 Total Average per question**
Profession* --- O G G P P P P P P P O O G P N
Indicator IV.1 M1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 15 1.00
Indicator IV.2 M2 0.1 0.67 0.3 0.4 0.7 0.7 0.67 0.7 0.3 0.63 0.4 0.43 0.5 0.3 0.4 7.2 0.48
Indicator IV.3 M2 0.5 0.88 0.88 0.5 0 1 0 0 0.5 0.88 0.88 0.67 0.88 0.38 0 7.95 0.53
Indicator IV.4 M1 DK 1 1 1 1 1 DK 1 1 1 1 0 1 0 0 10 0.77
Indicator IV.5 M2 DK 0 0.75 0 DK DK DK 0 0 DK 0.25 0 0 0 0 1 0.10
Indicator IV.6 M1 DK 1 1 DK 1 1 DK 0 0 1 DK 0 1 1 1 8 0.73
Indicator IV.7 M2 NA 0.8 0.6 NA DK DK DK DK 0 0.8 0.67 0 0 DK 1 3.87 0.48
Indicator IV.8 M2 NA 0 0 NA DK DK DK DK 0 DK 0 0 0 DK DK 0 0.00
Indicator IV.9 M2 DK 0 1 DK DK DK DK DK 0 0 0 0 1 1 1 4 0.44
Indicator IV.10 M2 DK 0 0 0 DK 0 DK DK 0 0 0 0 0 0 0 0 0.00
Indicator IV.11 M3 DI AG SA SD AG SD DK DI DI DI DI SD DI AG DI
Indicator IV.12 M3 UN AG DI DI DI SD SD DI DI SA AG DI SA DI DI
Indicator IV.13 M3 AG AG SD DI DI SA SD SD SD SA AG DI SD SD UN
Indicator IV.14 M3 UN AG DI DI SD SD SD DI SD UN SA DK DI DI DI
Indicator IV.15 M4 see text in narrative report
Indicator IV.16 M4 see text in narrative report
Total 4.53
***Final score Promotion 4.53

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 61 ‐‐
Score Sheet 5
Country name: Period assessment carried out:
Clinical trials
Kenya June-July 2008
Method KI 1 KI 2 KI 3 KI 4 KI 5 KI 6 KI 7 KI 8 KI 9 KI 10 KI 11 KI 12 KI 13 KI 14 KI 15 Total Average per question**
ACA
CTC
Profession* --- G O P O G O M O O O P O O P P
Indicator V.1 M1 1 1 0 DK 0 1 1 1 1 DK 1 1 1 0 0 9 0.69
Indicator V.2 M1 0 0 0 0 1 1 1 0 0 0 0 1 0 1 0 5 0.33
Indicator V.3 M2 0.8 1 0 0.4 0 0 1 1 1 0 1 DK 1 1 0.6 8.8 0.63
Indicator V.4 M2 1 1 0 0.83 0 1 0.83 1 0.83 1 0.83 1 0.83 1 1 12.15 0.81
Indicator V.5 M1 1 1 0 1 DK 1 1 1 1 1 1 1 1 1 1 13 0.93
Indicator V.6 M1 1 1 0 1 1 0 DK 1 1 1 0 DK 1 1 1 10 0.77
Indicator V.7 M2 1 1 0 DK 0.5 0 1 0.75 1 1 0 0.75 1 1 1 10 0.71
Indicator V.8 M1 0 0 0 0 1 1 0 0 0 0 0 1 1 0 0 4 0.27
Indicator V.9 M2 1 1 0 1 0 1 0 1 1 0 0 DK 0 1 1 8 0.57
Indicator V.10 M1 1 1 1 1 0 1 1 DK 1 1 0 1 1 0 1 11 0.79
Indicator V.11 M2 0 DK 0 1 DK 1 - DK DK DK 0 0.8 1 0.17 1 4.97 0.55
Indicator V.12 M2 0.75 0 0 0.75 0 0.75 0 0.75 0.75 DK 0 1 0.75 0.75 0 6.25 0.45
Indicator V.13 M3 DK SA DI DK NA SA AG SD DK SA AG AG - SA DI
Indicator V.14 M3 AG AG DK DK DK DK DK SD DK SA DK DK DK AG DI
Indicator V.15 M3 SA SA DI SD DK DK SD SA AG SA DI SD AG AG DI
Indicator V.16 M4 see text in narrative report
Indicator V.17 M4 see text in narrative report
Total 7.50
***Final score Clinical trials 6.25

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 62 ‐‐
Score Sheet 6
Method
KI 1 KI 2 KI 3 KI 4 KI 5 KI 6 KI 7 KI 8 KI 9 KI 10 KI 11 KI 12 KI 13 KI 14 KI 15 Total Average per question**
Profession* --- G G G G G G G G G G G G O O O
Indicator VI.1 M1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 1 14 0.93
Indicator VI.2 M3 DI DI DI DI AG DK AG DI AG AG DI AG AG NA SD
Indicator VI.3 M2 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0.00
Indicator VI.4 M2 0 0.67 0.5 0.5 0.83 0.5 0 DK 0.5 0.4 0.17 0.5 1 0 0.67 6.24 0.45
Indicator VI.5 M1 0 0 0 0 1 0 1 1 0 1 1 1 1 1 0 8 0.53
Indicator VI.6 M3 NA NA NA NA AG DK AG NA SA AG DI DI AG SD AG
Indicator VI.7 M2 0 0.71 0 1 0 0 0 0 0 0.5 0.43 0 0 0.714 0 3.354 0.22
Indicator VI.8 M2 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0.00
Indicator VI.9 M2 0.33 0.33 0 0.67 0 0 0 0 0 1 1 0 0 0 0 3.33 0.22
Indicator VI.10 M2 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0.00
Indicator VI.11 M4 see text in narrative report 0
Indicator VI.12 M4 see text in narrative report
Total 2.36
***Final score Selection 2.95
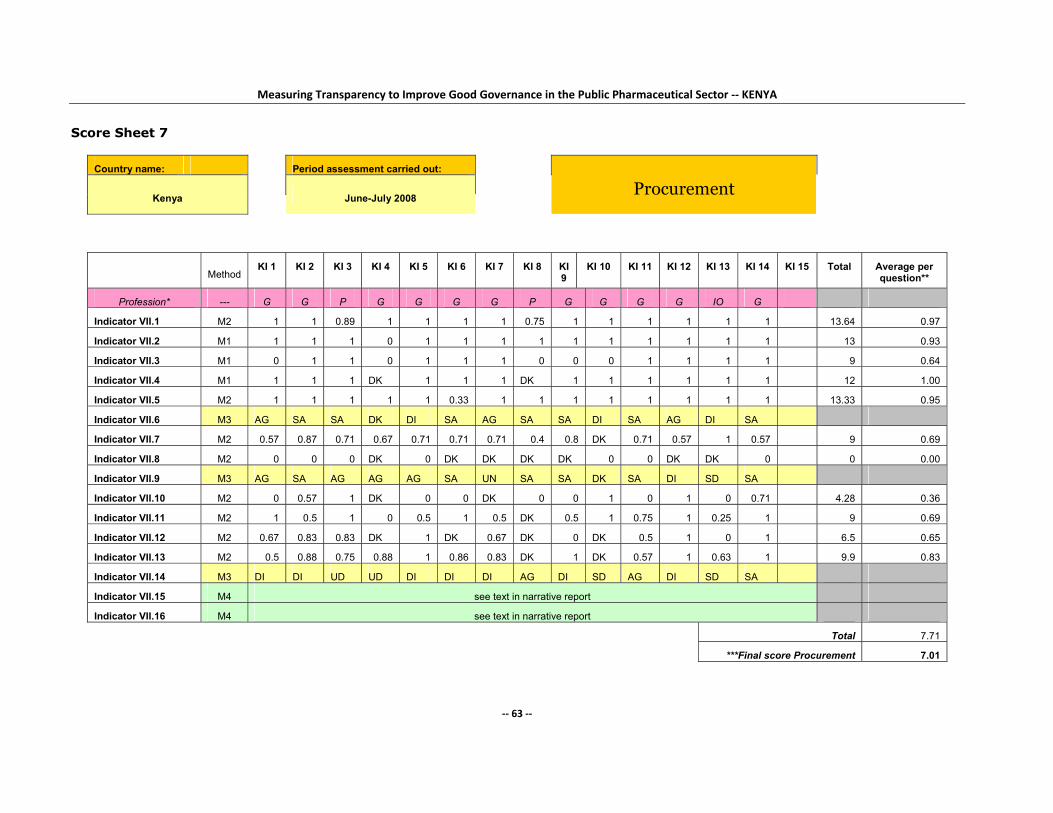
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 63 ‐‐
Score Sheet 7
Country name: Period assessment carried out:
Procurement
Kenya
June-July 2008
Method
KI 1 KI 2 KI 3 KI 4 KI 5 KI 6 KI 7 KI 8 KI 9
KI 10 KI 11 KI 12 KI 13 KI 14 KI 15 Total Average per question**
Profession* --- G G P G G G G P G G G G IO G
Indicator VII.1 M2 1 1 0.89 1 1 1 1 0.75 1 1 1 1 1 1 13.64 0.97
Indicator VII.2 M1 1 1 1 0 1 1 1 1 1 1 1 1 1 1 13 0.93
Indicator VII.3 M1 0 1 1 0 1 1 1 0 0 0 1 1 1 1 9 0.64
Indicator VII.4 M1 1 1 1 DK 1 1 1 DK 1 1 1 1 1 1 12 1.00
Indicator VII.5 M2 1 1 1 1 1 0.33 1 1 1 1 1 1 1 1 13.33 0.95
Indicator VII.6 M3 AG SA SA DK DI SA AG SA SA DI SA AG DI SA
Indicator VII.7 M2 0.57 0.87 0.71 0.67 0.71 0.71 0.71 0.4 0.8 DK 0.71 0.57 1 0.57 9 0.69
Indicator VII.8 M2 0 0 0 DK 0 DK DK DK DK 0 0 DK DK 0 0 0.00
Indicator VII.9 M3 AG SA AG AG AG SA UN SA SA DK SA DI SD SA
Indicator VII.10 M2 0 0.57 1 DK 0 0 DK 0 0 1 0 1 0 0.71 4.28 0.36
Indicator VII.11 M2 1 0.5 1 0 0.5 1 0.5 DK 0.5 1 0.75 1 0.25 1 9 0.69
Indicator VII.12 M2 0.67 0.83 0.83 DK 1 DK 0.67 DK 0 DK 0.5 1 0 1 6.5 0.65
Indicator VII.13 M2 0.5 0.88 0.75 0.88 1 0.86 0.83 DK 1 DK 0.57 1 0.63 1 9.9 0.83
Indicator VII.14 M3 DI DI UD UD DI DI DI AG DI SD AG DI SD SA
Indicator VII.15 M4 see text in narrative report
Indicator VII.16 M4 see text in narrative report
Total 7.71
***Final score Procurement 7.01

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 64 ‐‐
Score Sheet 8 Country name: Period assessment carried out: Distribution
Kenya June-July 2008
Method KI 1 KI 2 KI 3 KI 4 KI 5 KI 6 KI 7 KI 8 KI 9 KI 10 KI 11 KI 12 KI 13 KI 14 KI 15 Total Average/question**
G = Government or public official
G G G G G G G G N N G G P
Indicator VIII.1 M1 0 DK DK DK DK DK 1 1 1 1 DK DK 0 4 0.67
Indicator VIII.2 M3 AG NA NA NA DI NA SD AG DI DI NA DK AG
Indicator VIII.3 M2 1 1 0.75 1 1 1 1 0.75 1 1 1 0.75 1 12.25 0.94
Indicator VIII.4 M1 1 1 1 1 1 1 1 1 DK DK 1 1 0 10 0.91
Indicator VIII.5 M2 0.67 0.67 0.67 0.33 0 1 0.67 0 0.67 0.33 0.67 0.67 0.67 7.02 0.54
Indicator VIII.6 M2 0.83 1 1 0.83 1 0.83 1 0.83 0.83 1 0.83 0.67 1 11.65 0.90
Indicator VIII.7 M1 1 1 1 1 1 1 1 1 1 1 1 0 1 12 0.92
Indicator VIII.8 M2 0.71 0.43 0.43 0.43 0.57 1 0.14 0.57 0.14 1 0.29 0.14 0.86 6.71 0.52
Indicator VIII.9 M1 1 1 1 1 0 1 1 0 1 0 1 1 1 10 0.77
Indicator VIII.10 M2 1 1 0 1 0.67 1 1 0 0 0 1 1 1 8.67 0.67
Indicator VIII.11 M2 1 1 1 1 1 1 1 1 0.83 0.83 1 DK 1 11.66 0.97
Indicator VIII.12 M2 1 1 1 1 1 1 1 1 1 1 1 1 1 13 1.00
Indicator VIII.13 M2 0.75 1 0 1 DK 1 0.75 0 0 0 1 1 0.5 7 0.58
Indicator VIII.14 M1 1 1 1 1 1 1 1 1 1 1 1 1 1 13 1.00
Indicator VIII.15 M2 0.86 0.71 0.71 0.86 0.57 1 0.71 0 0 0 0.86 0.71 0.57 7.56 0.58
Indicator VIII.16 M2 0.33 1 1 0.67 1 1 1 1 0 0 1 0 0.67 8.67 0.67
Indicator VIII.17 M2 1 1 1 1 1 1 0.75 0.75 0.67 0.75 1 1 0.5 11.42 0.88
Indicator VIII.18 M3 DI AG DI SA DI DI SD AG SD DI SD DI SD
Indicator VIII.19
Indicator VIII.20 M4 see text in narrative report
Total 12.51
***Final score Distribution 7.82

Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 65 ‐‐
Annex 2: List of Documentary Evidence Obtained
a. Registration
Checklist for new applications for medicine registration
Requirements for all new manufacturers applying for new drug applications
Guidelines for parallel importation of medicines in Kenya
Guidelines for National Pharmacovigilance system in Kenya
Guidelines for applicants on how to submit an application for registration of
medicinal products
Application form for submission of applications for registration of medicines
List of all registered pharmaceutical products.
b. Licensing
Guidelines for Registration (Licensing) of premises and issuance of wholesale
dealer’s licence
List of licensed pharmaceutical establishments in Kenya (2007). (Not
comprehensive).
c. Inspection
Guidelines for Good Wholesaling and Retail Practice for Pharmaceuticals
Guidelines for Good Manufacturing Practices for medicines in Kenya
Guidelines for product recall and withdrawal
Standard operating procedures for inspectors on how to conduct inspections.
d. Promotion
Code of promotional practices for pharmaceutical representatives in Kenya.
e. Clinical trials
Checklist for submitting documents to the (PPB) committee on clinical trials
Guidelines on the submission of applications to the PPB to conduct clinical
trials
Form for submitting applications to KNH/UoN ERC
Guidelines for protocol development
Forms for reporting adverse effects
Guidelines on the process of protocol review
Standard operating procedures for KNH/UoN ERC.
f. Selection
Kenya Essential Drugs List (KEDL), Third Edition (August 2003)
Criteria for selection of essential medicines (Draft)
Criteria for selection of members of the National Medicines and Therapeutics
Committee (Draft)
Terms of reference for the National Medicines and Therapeutics Committee
(Draft).
g. Procurement
h. Distribution
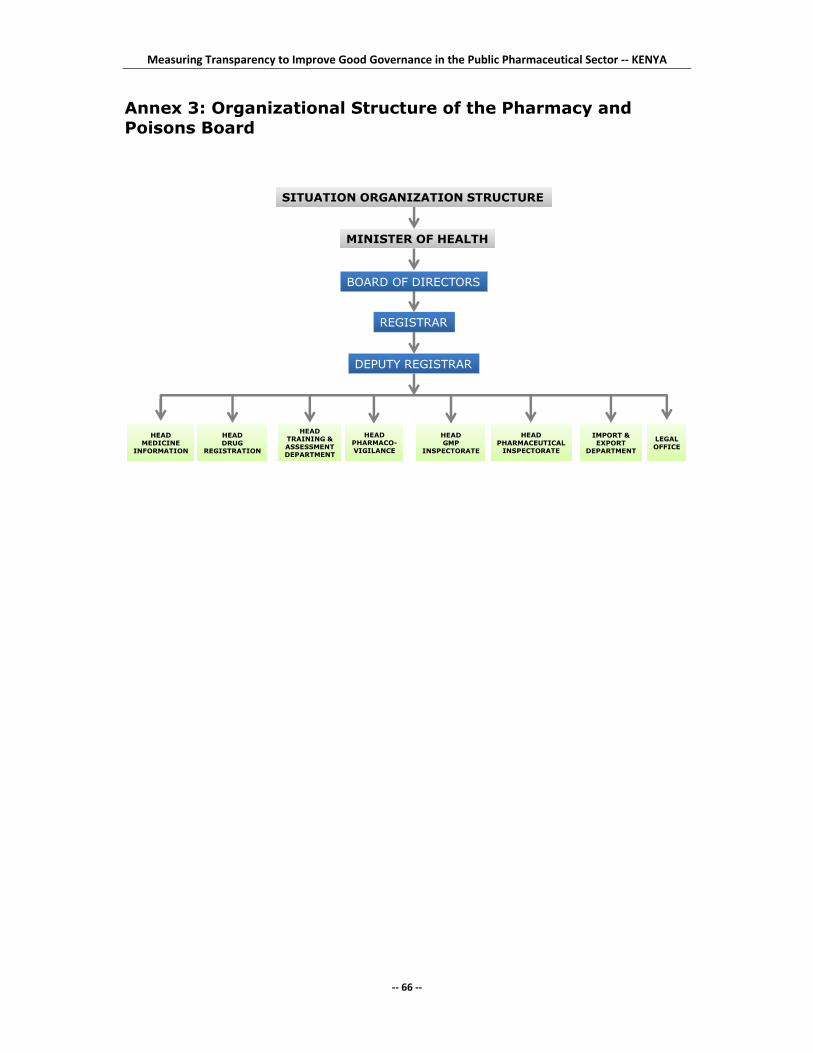
Measuring Transparency to Improve Good Governance in the Public Pharmaceutical Sector ‐‐ KENYA
‐‐ 66 ‐‐
Annex 3: Organizational Structure of the Pharmacy and Poisons Board
HEADMEDICINE
INFORMATION
HEADDRUG
REGISTRATION
HEADPHARMACO-VIGILANCE
HEADPHARMACEUTICAL
INSPECTORATE
LEGALOFFICE
HEADGMP
INSPECTORATE
IMPORT &EXPORT
DEPARTMENT
HEADTRAINING &ASSESSMENTDEPARTMENT
SITUATION ORGANIZATION STRUCTURE
MINISTER OF HEALTH
BOARD OF DIRECTORS
REGISTRAR
DEPUTY REGISTRAR