
Kenya Country Office HUMANITARIAN SITUATION … Country Office HUMANITARIAN SITUATION REPORT Apr-Jun...
8
Kenya Country Office HUMANITARIAN SITUATION REPORT Apr-Jun 2015 1 Highlights While the overall nutrition situation is showing improvement in coastal, North West and South East Counties with an expected decrease in the acutely malnourished children requiring treatment, the nutrition situation is expected to worsen in Isiolo, Garissa, Mandera and Wajir counties as a result of poor rains. The total caseload for acutely malnourished children requiring treatment in the ASAL and urban areas is expected to decrease from 304,083 as of February 2015 driven by improvements observed across ASAL counties. Humanitarian access and delivery of essential basic social services has been significantly constrained by increased inter-communal conflict and terrorist attacks especially in Northern Kenya, Upper Eastern and Coast regions. Across all conflict-affected counties, 1,600 teachers are not on duty affecting both access and quality of education for approximately 80,000 school pupils. Within this context, a total of 465,000 emergency- affected children continue to remain out of school due to multiple shocks as a result of drought, chronic food insecurity, lack of access to safe water and conflict-related displacement. The Health and Nutrition also continue to be affected by insecurity. The mass exodus of health workers impacted negatively the quality of health and nutrition services provision in most health centers. In several parts of Northern Kenya, Community Health Workers have been left to provide maternal, child health and nutrition services, while a planned Polio campaign in Northern Kenya had to be postponed indefinitely due to insecurity. Since 26 December 2014, a sustained Cholera outbreak has spread to 16 Counties: Nairobi, Migori, Homa Bay, Bomet, Mombasa, Nakuru, Muranga, Kirinyaga, Baringo, Kiambu ,Embu, Machakos, Narok, Kilifi, Trans nzoia and Turkana Counties, with 4,938 cases and 97 deaths (Case Fatality Rate =2 per cent) reported by 29 June 2015 1 . UNICEF is supporting Health, WASH and C4D interventions, and has received ECHO funding to support ongoing preparedness and response efforts, through expanding prevention measures to bring the outbreak under control before the next rainy season starts in October, especially in high risk areas where children are particularly vulnerable. Of the $25,000,000 humanitarian funding appeal for 2015, UNICEF has received a total of $11,427,389 (46 per cent) as at 30 June 2015 (this includes funding carried forward from 2014). However, the HIV/AIDS, Health and Child Protection sectors remained grossly underfunded. In 2015, UNICEF has received humanitarian funding from Government of Japan Supplementary funding, USAID/Food For Peace and European Commission/ECHO. Humanitarian Situation Report April-June, 2015 1.6 million # of food insecure population in Kenya (Kenya Short Rains Assessment, February 2015) Kakuma 46,235 # of newly arrived South Sudanese Refugees in Kakuma Refugee Camp by 25 June 2015 (UNHCR) Kakuma 878# of newly arrived unaccompanied South Sudanese children in Kakuma camp as of 25 June 2015 (UNHCR) Kakuma 5,655 # of newly arrived separated South Sudanese children in Kakuma camp as of 25 June 2015 (UNHCR) 25,000,000 funding requirements Funding Gap: 13.5 M Funding Received: 11.4 M Highlights: The Humanitarian Situation in Figures: Children in Wajir IDP Camp, South Sudanese refugees crossing boarder and in Tana Delta inter communal conflict affected regions. Photo Credit: Minu Limbu/Unicef Kenya
Transcript of Kenya Country Office HUMANITARIAN SITUATION … Country Office HUMANITARIAN SITUATION REPORT Apr-Jun...

Kenya Country Office HUMANITARIAN SITUATION REPORT Apr-Jun 2015
1
Highlights
While the overall nutrition situation is showing improvement in coastal, North West and South East Counties with an expected decrease in the acutely malnourished children requiring treatment, the nutrition situation is expected to worsen in Isiolo, Garissa, Mandera and Wajir counties as a result of poor rains. The total caseload for acutely malnourished children requiring treatment in the ASAL and urban areas is expected to decrease from 304,083 as of February 2015 driven by improvements observed across ASAL counties.
Humanitarian access and delivery of essential basic social services has
been significantly constrained by increased inter-communal conflict and
terrorist attacks especially in Northern Kenya, Upper Eastern and Coast
regions. Across all conflict-affected counties, 1,600 teachers are not on
duty affecting both access and quality of education for approximately
80,000 school pupils. Within this context, a total of 465,000 emergency-
affected children continue to remain out of school due to multiple
shocks as a result of drought, chronic food insecurity, lack of access to
safe water and conflict-related displacement.
The Health and Nutrition also continue to be affected by insecurity. The
mass exodus of health workers impacted negatively the quality of health
and nutrition services provision in most health centers. In several parts
of Northern Kenya, Community Health Workers have been left to
provide maternal, child health and nutrition services, while a planned
Polio campaign in Northern Kenya had to be postponed indefinitely due
to insecurity.
Since 26 December 2014, a sustained Cholera outbreak has spread to 16 Counties: Nairobi, Migori, Homa Bay, Bomet, Mombasa, Nakuru, Muranga, Kirinyaga, Baringo, Kiambu ,Embu, Machakos, Narok, Kilifi, Trans nzoia and Turkana Counties, with 4,938 cases and 97 deaths (Case Fatality Rate =2 per cent) reported by 29 June 20151. UNICEF is supporting Health, WASH and C4D interventions, and has received ECHO funding to support ongoing preparedness and response efforts, through expanding prevention measures to bring the outbreak under control before the next rainy season starts in October, especially in high risk areas where children are particularly vulnerable.
Of the $25,000,000 humanitarian funding appeal for 2015, UNICEF has
received a total of $11,427,389 (46 per cent) as at 30 June 2015 (this
includes funding carried forward from 2014). However, the HIV/AIDS,
Health and Child Protection sectors remained grossly underfunded.
In 2015, UNICEF has received humanitarian funding from Government
of Japan Supplementary funding, USAID/Food For Peace and European
Commission/ECHO.
Humanitarian Situation Report
April-June, 2015
1.6 million # of food insecure population in Kenya (Kenya Short Rains Assessment, February 2015)
Kakuma
46,235 # of newly
arrived South Sudanese Refugees in Kakuma Refugee Camp by 25 June 2015 (UNHCR)
Kakuma
878# of newly arrived
unaccompanied South Sudanese children in Kakuma camp as of 25 June 2015 (UNHCR)
Kakuma
5,655 # of newly arrived
separated South Sudanese children in Kakuma camp as of 25 June 2015 (UNHCR)
25,000,000 funding
requirements
Funding Gap: 13.5 M
Funding Received:11.4 M
Highlights:
The Humanitarian Situation in Figures:
Children in Wajir IDP Camp, South Sudanese refugees crossing boarder and in Tana Delta inter communal conflict affected regions. Ph
oto
Cre
dit
: Min
u L
imb
u/U
nic
ef
Ken
ya
Kenya Country Office HUMANITARIAN SITUATION REPORT Apr-Jun 2015
2
Situation Overview & Humanitarian Needs:
The overall nutrition situation is stable and showing improvements in coastal (Kwale and Kilifi), south-east marginal
(Kitui and Makueni), agro-pastoral (West Pokot, Kieni and Laikipia) and pastoral North West (Turkana, Samburu and
Marsabit) counties. However pastoral North East cluster namely; Isiolo, Garissa, Manderaand Wajir counties, the
nutrition situation is expected to worsen attributed to poor performance of both short and long rain seasons. In
Mandera, Isiolo and Baringo Counties centralized incidences of insecurity and resource based conflicts was reported
within the season (March-May 2015). Nutrition surveys conducted in June 2015 in Turkana and Mandera Counties
indicated GAM estimates of 21.6% and 24.7% respectively, above critical levels of WHO classification on acute
malnutrition though stable when compared to similar rates in June 2014. Nutrition Surveillance updates based on
admissions trend for MAM have shown improving and fairly stable trend in Turkana, Samburu, Baringo, West
Pokot, Marsabit, Kitui, Kwale, Kilifi, Laikipia, Makueni, Kajiado, Narok and Tana River Counties as of May,
2015.However, this is not the case for Wajir, Mandera, Isiolo and Garissa Counties where MAM admissions are
showing increased trend. The total caseload for acutely malnourished children requiring treatment in the ASAL and
urban areas is expected to decrease from 304,083 as of February 2015 driven by improvements observed across
ASAL counties.
In the first half of 2015, humanitarian access and delivery of essential basic social services has been significantly
constrained by increased inter-communal conflict and terrorist attacks especially in Northern Kenya, Upper Eastern
and Coast regions, with the Education Sector being the most affected, leading to an ‘Education in Crisis’. Across
all conflict-affected counties, 1,600 teachers are not on duty, out of which 1,200 have continue to desert their
duties in Northern Kenya citing insecurity, with the support of the Teachers’ Union. This combination of factors is
affecting both access and quality of education for approximately 80,000 school pupils. This result in the closure of
of 122 schools and consequently, approximately 32,000 pupils are unable to access schooling especially in Northern
Kenya, Upper Eastern and Coast regions.
Within this context, a total of 465,000 emergency-affected children continue to remain out of school due to
multiple shocks as a result of drought, chronic food insecurity, lack of access to safe water and conflict-related
displacement.
The Health and Nutrition also continue to be affected by insecurity. The mass exodus of health workers impacted
negatively the quality of health and nutrition services provision in most health centers. In several parts of Northern
Kenya, Community Health Workers have been left to provide maternal, child health and nutrition services, while a
planned Polio campaign in Northern Kenya had to be postponed indefinitely due to insecurity.
Since 26 December 2014, a sustained Cholera outbreak has spread to 16 Counties: Nairobi, Migori, Homa Bay,
Bomet, Mombasa, Nakuru, Muranga, Kirinyaga, Baringo, Kiambu ,Embu, Machakos, Narok, Kilifi ,Trans nzoia and
Turkana Counties, with 4,938 cases and 97 deaths (Case Fatality Rate =2 per cent) reported by 29 June 20152. The
outbreak first started in Nairobi County on 26th December 2014. Later the outbreak was reported in Migori County
on 30th January 2015, Homa Bay County on 2nd February 2015, Bomet County on 12th March 2015, Mombasa
County on 6th April 2015, Nakuru 8th April , Muranga county on 18th April 2015, Kirinyaga county 21st April 2015,
Embu on 26th April 2015, Baringo county on 7th May 2015 ,Kiambu county 7th May 2015,Machakos county 4th
may 2015,Narok county 23rd may 2015 ,Kilifi county on 28th may 2015, Trans Nzoia County on 1/6/2015 and
Turkana county the latest to report a confirmed outbreak on 13/6/2015. Nairobi County has so far reported the
highest number of cases (1090), followed by Migori (915). Trans Nzoia County has the highest case fatality rate
(14.3%), followed by Machakos County 6.3%. Migori and Bomet Cholera outbreaks have been successfully
controlled. Active case search is ongoing in all the affected counties aimed at rapid detection, case management
and follow up of cases. Laboratory specimens are being collected and tested to determine and isolate the species
causing the outbreak. The main circulating serotype so far is Ogawa. UNICEF is supporting Health, WASH and C4D
interventions, and has received ECHO funding to support ongoing preparedness and response efforts to bring the
outbreak under control before the next rainy season starts in October. UNICEF has also used CERF funding and
Government of Japan funding to support the response.
The influx of refugees from South Sudan continues, with 46,235 new arrivals recorded/registered (67 per cent
children) as of 25 June 20153, up from 43,940 in October 2014. Of these, 878 are unaccompanied minors (UAMs)
and 5,655 are separated children.
Kenya Country Office HUMANITARIAN SITUATION REPORT Apr-Jun 2015
3
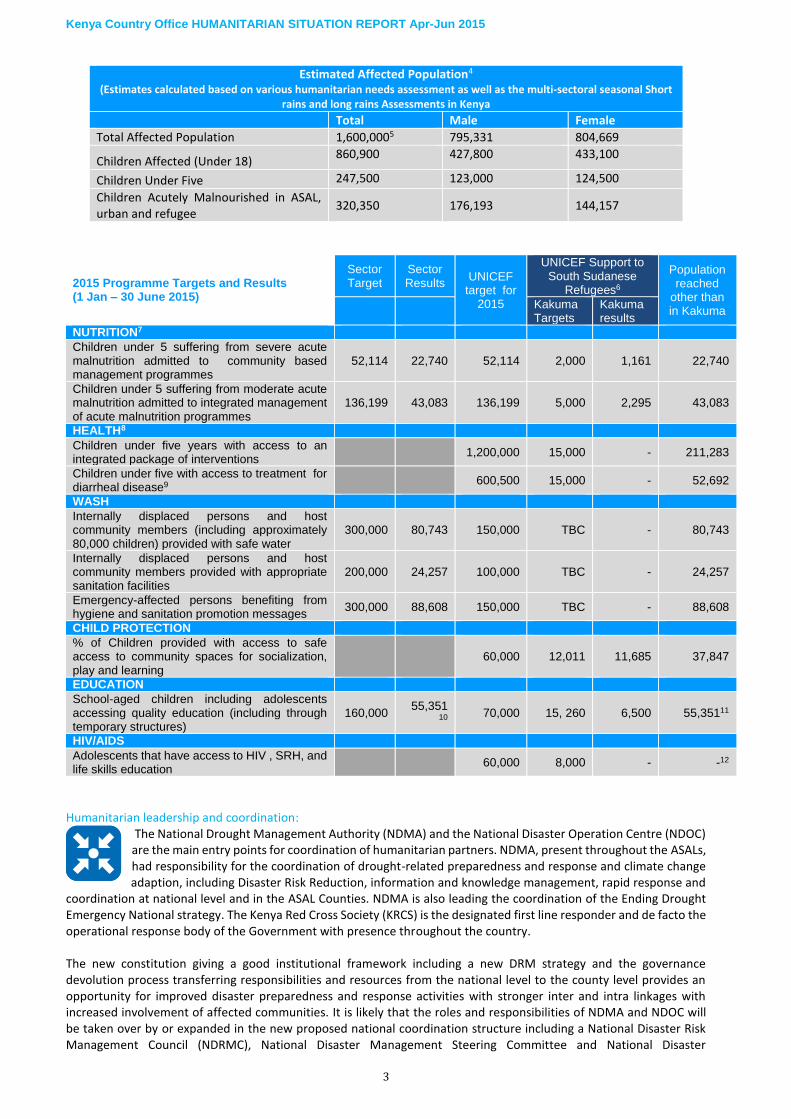
Estimated Affected Population4 (Estimates calculated based on various humanitarian needs assessment as well as the multi-sectoral seasonal Short
rains and long rains Assessments in Kenya
Total Male Female
Total Affected Population 1,600,0005 795,331 804,669
Children Affected (Under 18) 860,900 427,800 433,100
Children Under Five 247,500 123,000 124,500
Children Acutely Malnourished in ASAL, urban and refugee
320,350 176,193 144,157
2015 Programme Targets and Results (1 Jan – 30 June 2015)
Sector Target
Sector Results
UNICEF target for
2015
UNICEF Support to South Sudanese
Refugees6
Population reached
other than in Kakuma
Kakuma Targets
Kakuma results
NUTRITION7
Children under 5 suffering from severe acute malnutrition admitted to community based management programmes
52,114 22,740 52,114 2,000 1,161 22,740
Children under 5 suffering from moderate acute malnutrition admitted to integrated management of acute malnutrition programmes
136,199 43,083 136,199 5,000 2,295 43,083
HEALTH8
Children under five years with access to an integrated package of interventions
1,200,000 15,000 - 211,283
Children under five with access to treatment for diarrheal disease9
600,500 15,000 - 52,692
WASH
Internally displaced persons and host community members (including approximately 80,000 children) provided with safe water
300,000 80,743 150,000 TBC - 80,743
Internally displaced persons and host community members provided with appropriate sanitation facilities
200,000 24,257 100,000 TBC - 24,257
Emergency-affected persons benefiting from hygiene and sanitation promotion messages
300,000 88,608 150,000 TBC - 88,608
CHILD PROTECTION
% of Children provided with access to safe access to community spaces for socialization, play and learning
60,000 12,011 11,685 37,847
EDUCATION
School-aged children including adolescents accessing quality education (including through temporary structures)
160,000 55,351
10 70,000 15, 260 6,500 55,35111
HIV/AIDS
Adolescents that have access to HIV , SRH, and life skills education
60,000 8,000 - -12
Humanitarian leadership and coordination:
The National Drought Management Authority (NDMA) and the National Disaster Operation Centre (NDOC) are the main entry points for coordination of humanitarian partners. NDMA, present throughout the ASALs, had responsibility for the coordination of drought-related preparedness and response and climate change adaption, including Disaster Risk Reduction, information and knowledge management, rapid response and
coordination at national level and in the ASAL Counties. NDMA is also leading the coordination of the Ending Drought Emergency National strategy. The Kenya Red Cross Society (KRCS) is the designated first line responder and de facto the operational response body of the Government with presence throughout the country. The new constitution giving a good institutional framework including a new DRM strategy and the governance devolution process transferring responsibilities and resources from the national level to the county level provides an opportunity for improved disaster preparedness and response activities with stronger inter and intra linkages with increased involvement of affected communities. It is likely that the roles and responsibilities of NDMA and NDOC will be taken over by or expanded in the new proposed national coordination structure including a National Disaster Risk Management Council (NDRMC), National Disaster Management Steering Committee and National Disaster

Kenya Country Office HUMANITARIAN SITUATION REPORT Apr-Jun 2015
4
Management Authority (NADIMA) supervising and coordinating sectoral thematic working groups. However, no progress has been made in the first half of 2015 in the passing of the DRM bill that can enable this change. The capacity of the County Steering Groups and/or County Disaster Management Committees to the County Governments as the main coordination body at County level for disaster preparedness and response are variable. The Ministry of environment and Ministry of Interior with UN support has put in place a proposed joint humanitarian, peace building and DRR coordination mechanism to be implemented in 2015 under the UNDAF Outcome result 4.2, with the first task being to review the humanitarian strategy. But no progress has been made in the first half of 2015 to implement this joint coordination mechanism and the Kenya Humanitarian Partnership Team (KHPT) is still lead exclusively by the Resident Coordinator as the Inter-sector Coordination Group led by UNOCHA There are nine technical sectors led by Government Ministries with technical support from UN agencies. In addition, UNHCR has been supporting the Department of Refugee Affairs in coordinating and leading refugee assistance. Under the new proposed coordination structure, the Government has proposed the following 11 sectoral working groups, with other sectors such as Gender based violence (GBV) and Camp Coordination Camp Management (CCCM) to be created during emergencies. UNICEF co-leads the Nutrition, Education, WASH and Child Protection sectors; and plays a strong role in Non-Food Items and health coordination. UNICEF also co- leads Government of Kenya Ending Drought Emergency (EDE) Human Capital pillar which comprise of Education, Health and Nutrition. UNICEF provides EDE technical support to inter-governmental body on knowledge management, coordination to cross fertilize innovative approaches on EDE. UNHCR and Government Department of Refugee Affairs (DRA) coordinate the refugee operations. UNICEF works closely with UNHCR to support coordination for the refugee operations, and co-chairs some of the sectoral arrangements in Kakuma and Dadaab Refugee Camps. The UNICEF Country Management Team has Emergency Preparedness and Response as a standing agenda, and meets on a monthly basis. The Emergency Management Team aims to ensure that the appropriate systems, policies and strategies are in place to allow UNICEF Kenya to meet the Core Commitments for Children in Emergencies, fulfill its responsibilities for supporting sectoral coordination. As and when needed the EMT meets regularly as convened by the Representative in response to a rapid onset emergency or to review the status of preparedness/response or an anticipated or protracted emergency. During the reporting period, UNICEF KCO with the support of ESARO has organized an internal simulation for Ebola response and reviewed in overall preparedness mechanism through the participation of the validation workshop of the Emergency preparedness platform. Humanitarian Strategy
UNICEF will continue to support the Government of Kenya and partners’ response13 to the humanitarian needs of more than 1.23 million children affected by food insecurity, malnutrition, disease outbreaks, displacement14 and Gender based violence, including support to refugee populations from Somalia in Dadaab refugee camps and South Sudan refugee influx in Kakuma refugee camp.
Technical and financial assistance will be provided to support the coordination of key sectors (nutrition, health, WASH, child protection, education and HIV/AIDS). UNICEF will maintain optimum programme coverage, humanitarian response and capacity building for devolved governance, while advocating for children’s rights in inter-agency rapid assessments and contingency planning. However, accessibility to targeted populations and monitoring of interventions continues to be affected by insecurity, especially in Northern Kenya. To address this, UNICEF will reach the most vulnerable through remote programming and partnering with local partners. High Impact nutrition interventions15 including treatment of acute malnutrition will be scaled up in the Arid and Semi-Arid counties, urban informal settlements, Kakuma and Dadaab refugee camps and immediate host communities. UNICEF will support the coordination and information systems at national and county level in the nutrition sector, to ensure the development of timely contingency plans, response planning, gap analysis, capacity building and enhanced community resilience programmes. In partnership with WFP, UNICEF will provide anthropometric equipment and technical support for quality programme delivery of moderate acute malnutrition (MAM). Cholera outbreak will be monitored in non-endemic areas, systems strengthening and building of new partnerships across priority counties will be carried out to enhance advocacy and behaviour change communication. UNICEF will support the dissemination of integrated Ebola and Cholera messages, and the roll-out of the Emergency and Disaster Risk Management Strategic Plan to contribute to the health response including the current Cholera outbreak.
Kenya Country Office HUMANITARIAN SITUATION REPORT Apr-Jun 2015
5
Communities will be empowered through recruitment and training of community health workers to deliver key health interventions. Delivery of an integrated health interventions package will ensure cost-effectiveness, optimal utilization and ensure minimal loss of life. Using an integrated approach, UNICEF will combine high impact interventions in health, such as mass immunizations, with Vitamin A supplementation and preventing mother to child transmission (PMTCT) services as part of maternal and newborn child health (MNCH). UNICEF will support children and adolescents on HIV prevention knowledge and skills, HIV/AIDS treatment and care services and strengthening data management in Kakuma refugee camp, Turkana host community and priority Arid and Semi-Arid Counties. Child Protection and GBV interventions will involve scaling up child- friendly spaces, case management, psychosocial support and referral mechanisms for unaccompanied or separated and other vulnerable children and adolescents. Partnerships with relevant organisations will scale up child- friendly spaces, capacity development of duty bearers, child participation, case management, psycho-social support, access to GBV and dignity kits and referral mechanisms for unaccompanied or separated and other vulnerable children and adolescents to these communities. Building on County Government emergency response efforts to conflict and drought-affected communities, UNICEF will support timely protection of women and children against violence, abuse, neglect and exploitation in Turkana, Wajir, Garissa and Mandera Counties. An additional 124 temporary learning spaces (including school tents) and 22 Alternative Basic Education centres will be provided to incorporate in-service teacher training, psychosocial support, peace education, and provision of teaching and learning materials and WASH facilities for boys and girls in targeted counties and in the refugee camps. Summary Analysis of Programme response (Jan 01 –Jun 30, 2015) Nutrition:
Drought response: Despite humanitarian access challenges, children accessed life-saving nutrition interventions and preventive high impact nutrition services, of which more than 22,740 were treated for severe acute malnutrition (SAM) and more than 43,083 were admitted to integrated management of acute malnutrition programmes across ASAL areas and in urban informal settlements.
Refugee response: Through CERF funding, a total of 1,802 (81.5%) severely malnourished boys and girls, 3,600 (61.4%) moderately malnourished boys and girls and 7,549 (75.1%) malnourished women in Kakuma refugee camp were reached by 30th June 2015. In addition, 980 pregnant and lactating women received education through 49 mother-to-mother support groups (MTMSGs) and 42 men through two father-to-father support groups (FTFSGs). A total of 85 sessions were held (20 sessions on maternal nutrition, ANC and the importance of hospital delivery, 20 sessions on initiation of breastfeeding and the importance of exclusive breastfeeding, 25 sessions on complementary feeding for children ages six to 24 months, and 20 sessions on position and attachment of the child during breastfeeding.
Health:
Drought response: UNICEF is continuing to provide technical oversight in coordination at the national level for Cholera and Acute Watery Diarrhea (AWD) response. The Cholera response coordination committee continues to meet every two weeks. At County Level, Outbreak coordination teams are meeting regularly with
stakeholders in the Counties with active outbreaks. UNICEF-Procured medical supplies (Ringers Lactate, ORS and antibiotics) have been used in treatment of more than 52,000 children, and procurement of more supplies for distribution to counties is underway. Health education is ongoing in schools, public places and communities and through the local media, and with ECHO funding, C4D interventions are being up-scaled in 23 priority counties. Refugee response: With CERF funding, UNICEF supported refugees in Kakuma and host communities in Turkana West sub-county through procurement of measles and polio vaccines, related devices, cold chain equipment, assorted drugs, and orientation of community health volunteers, who offered sessions of ante-natal care, prevention of mother to child transmission of HIV/AIDS, dissemination of key messaging on epidemic diseases and need to access key lifesaving interventions. The result was increased awareness of community on key epidemics, key lifesaving interventions and consequent increased access and utilization of key interventions by communities and reduced mortality and mortality, reaching 67,100 beneficiaries (44,957children).
Water, Hygiene and Sanitation (WASH):
Drought response: Women, girls, boys and men continue to access essential WASH and health supplies, appropriate sanitation, hygiene and health-seeking behavior messages to prevent diarrheal disease and curb the spread of the cholera outbreak in priority counties. UNICEF continues to support WASH coordination (WESCOORD) structures through convening monthly coordination fora, as well as quality assurance of
projects implemented by various partners through field monitoring of activities. County Stakeholder WASH Forums

Kenya Country Office HUMANITARIAN SITUATION REPORT Apr-Jun 2015
6
further support county-level project monitoring to ensure timely interventions by partners. Information management has been strengthened through regular updating and sharing of 4W matrixes of activities by sector partners, which has improved the quality of preparedness and response as well as enhanced inter- sectoral coordination with Health and Education in the ongoing Cholera response.
Child Protection:
Drought response: A total of 37,487 beneficiaries (Female 21,742 and male 15,745) were reached in Turkana,
Garissa, Wajir and Mandera Counties through psychosocial support, case management, access to SGBV
support services, family reunification and dignity kits. Capacity development and training of duty bearers
including health practitioners, counsellors, police, community leaders and care givers was achieved through
partnerships with Government and partners. In Turkana County, a strategy to strengthen existing child protection
structures including informal and formal systems within the community was developed with UNICEF support.
Refugee response: In Kakuma Refugee Camp, via case management systems a total of 20,685 children (8,738 girls and
11, 947 boys) were reached. Out this 11,685 new children were identified with protection concerns and the follow-up
of 9,000 children. These includes Unaccompanied and Separated Children 1307 (873 boys, 434 girls) who received Best
Interest Assessments at the reception centre and at the community, 18,335 children (10404 boys 7931 girls) were visited
and their protection concerns promptly addressed/referred for medical, psychosocial, and legal support, monthly Foster
parents meeting were done to 483 foster parents (301 males 182 females) and 560 children (369 boys, 191 girls) were
placed under foster care arrangement.
Education:
Drought: With CERF funding, a total of 24 (50% female) teachers were trained on peace education and
education in emergencies and they have reached 600 (250 female) children with peace education in schools.
Psychosocial needs assessment tools were jointly developed by World Vision and ROAD with support from
MoEST and UNICEF and assessments conducted in Baringo, Turkana, Marsabit, Mandera and Wajir counties. Four
education stakeholders meetings were held in Baringo, Marsabit, Turkana and Mandera Counties. Rapid assessments
on the number of out-of-school children and their education needs was conducted in Baringo, Mandera, Wajir and
Turkana Counties. Nine sites for the temporary learning centres have been identified and confirmed by county
education stakeholders in Baringo, Turkana and Marsabit counties. In Mandera and Wajir, they have been identified
but not yet confirmed by the stakeholders. The implementing partners, World Vision and ROAD, have already agreed
and the type of temporary structures and procurement of the same is underway.
Refugee response: An additional 6,500 children benefited from teaching and learning materials in Kakuma refugee
camp. In Dadaab Refugee Camp and within the host community, the Alternative and Peace Education Programmes
benefitted 4,954 children (56 per cent female).
HIV/AIDS There has been improved traction on Adolescents and HIV following the global launch of All in campaign officiated by Kenya’s president, and supported by UNICEF. Ministry of Health’s Health Information
Systems HIV and SRH tools have now been age and sex disaggregated for adolescents. UNICEF is providing technical assistance on HIV information and data systems. Mechanisms have been put in place for real time data, feedback, opinions and suggestions from adolescents, including those who are HIV positive and those in vulnerable and emergency contexts.
Security: Terrorism related threats remain a serious challenge in the country especially in Nairobi, the Coast and
North Eastern areas. There has been a recent escalation in terror group Al-Shabaab (AS) related operations
in north eastern areas of Kenya. Security installations near the Kenya Somali border have been particularly
targeted. Ongoing conflicts between the various communities in the remote North and Eastern parts of the country
have escalated, mainly attributable to competition over scarce natural resources and County administrative boundaries.
The escalation of the Turkana / Pokot intercommunal conflict left 67 reported dead on 4th of May.
Despite a 65% drop in violent crime against UN in the first half of 2015 as opposed to 2014, the operation environment
require a high sense of security awareness and preparedness amongst UN staff members. Subsequently, UNICEF
Kenya Country Office HUMANITARIAN SITUATION REPORT Apr-Jun 2015
7
embarked on a series of trainings over the period, which include First Aid, Emergency Trauma Bags Training and active
shooter training. Following the April attack on Garissa University with 147 reported deaths, UNICEF security team
conducted security risk assessments on UNICEF offices in Dadaab and Garissa. The resultant recommendations are being
implemented to improve staff safety and security.
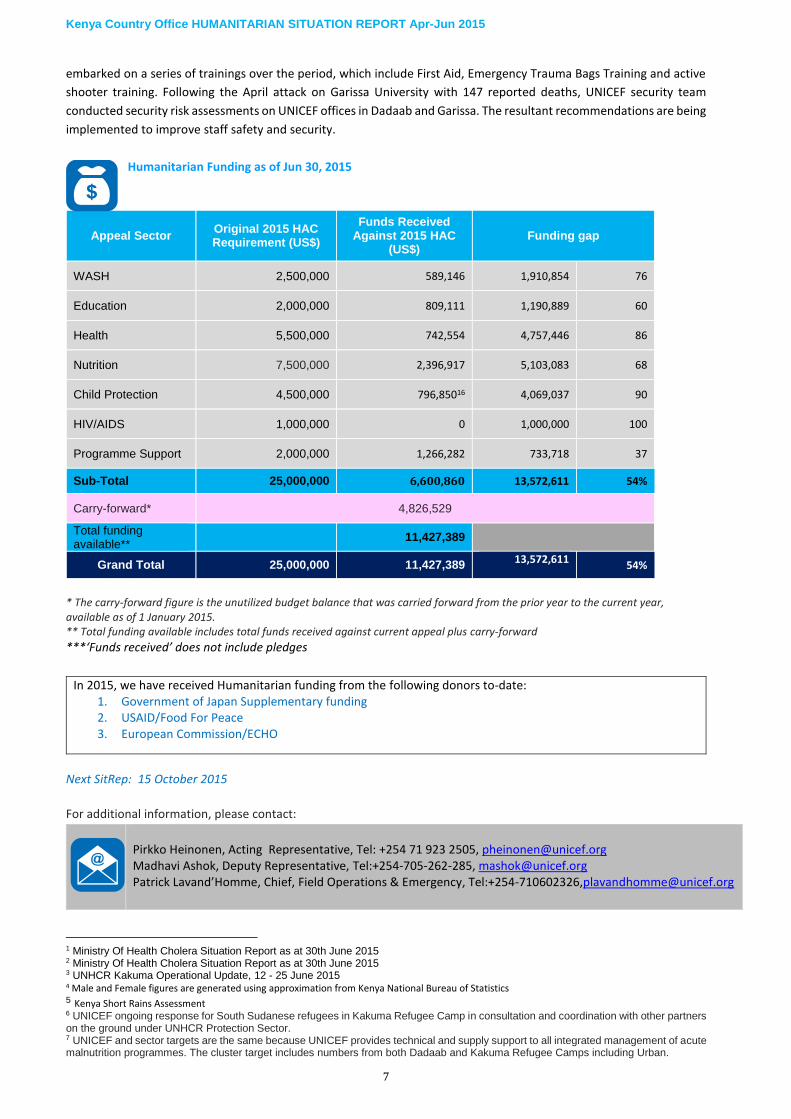
Humanitarian Funding as of Jun 30, 2015
Appeal Sector Original 2015 HAC Requirement (US$)
Funds Received Against 2015 HAC
(US$) Funding gap
WASH 2,500,000 589,146 1,910,854 76
Education 2,000,000 809,111 1,190,889 60
Health 5,500,000 742,554 4,757,446 86
Nutrition 7,500,000 2,396,917 5,103,083 68
Child Protection 4,500,000 796,85016 4,069,037 90
HIV/AIDS 1,000,000 0 1,000,000 100
Programme Support 2,000,000 1,266,282 733,718 37
Sub-Total 25,000,000 6,600,860 13,572,611 54%
Carry-forward* 4,826,529
Total funding available**
11,427,389
Grand Total 25,000,000 11,427,389 13,572,611
54%
* The carry-forward figure is the unutilized budget balance that was carried forward from the prior year to the current year, available as of 1 January 2015. ** Total funding available includes total funds received against current appeal plus carry-forward ***‘Funds received’ does not include pledges
In 2015, we have received Humanitarian funding from the following donors to-date: 1. Government of Japan Supplementary funding 2. USAID/Food For Peace 3. European Commission/ECHO
Next SitRep: 15 October 2015
For additional information, please contact:
Pirkko Heinonen, Acting Representative, Tel: +254 71 923 2505, [email protected] Madhavi Ashok, Deputy Representative, Tel:+254-705-262-285, [email protected] Patrick Lavand’Homme, Chief, Field Operations & Emergency, Tel:+254-710602326,[email protected]
1 Ministry Of Health Cholera Situation Report as at 30th June 2015 2 Ministry Of Health Cholera Situation Report as at 30th June 2015 3 UNHCR Kakuma Operational Update, 12 - 25 June 2015 4 Male and Female figures are generated using approximation from Kenya National Bureau of Statistics 5 Kenya Short Rains Assessment 6 UNICEF ongoing response for South Sudanese refugees in Kakuma Refugee Camp in consultation and coordination with other partners on the ground under UNHCR Protection Sector. 7 UNICEF and sector targets are the same because UNICEF provides technical and supply support to all integrated management of acute malnutrition programmes. The cluster target includes numbers from both Dadaab and Kakuma Refugee Camps including Urban.

Kenya Country Office HUMANITARIAN SITUATION REPORT Apr-Jun 2015
8
8 Data awaited from Ministry of Health for population reached through activities implemented by the Ministry with UNICEF support 9 Target for children under five accessing treatment for diarrheal disease remains the same in spite of the Cholera outbreak, because the same number of children targeted for management of diarrheal diseases (600,500), are within the Cholera-affected population 10 Additional data inputs to be received from Education Cluster Partners 11 Includes 4,954 children (56% female) in Dadaab 12 Interventions are going, and partners will report in July 2015 13 The country’s ongoing transition to decentralized governance structures provides both opportunities and challenges for humanitarian response and resilience-building. The Government of Kenya has made a commitment to end the worst of the suffering caused by drought by 2022. The actions needed to achieve this are set out in the Drought Risk Management and Ending Drought Emergencies Medium Term Plan (MTP) for 2013-17, which is part of the Kenya Vision 2030 MTP2. With the Government of Kenya, UNICEF is currently co-chairing the pillar on Human Capital (Education, Health, Nutrition, hygiene and sanitation) and contributes to all the other pillars including institutional development and knowledge management. URL: http://www.dmikenya.or.ke/home/18-newitem/34-drm-and-ede-common-programming-process.html 14 According to OCHA estimates, a total of 309,000 persons are presently displaced due to inter-communal conflict. According to the DTM for Kenya, recently launched by IOM across 59 displacement sites in seven Counties, the basic needs of the internally displaced remain grossly unmet, especially for the most vulnerable including pregnant/lactating women 15 Promotion of Exclusive Breastfeeding for the first six months of life 2) Promotion of optimal complementary feeding for infants after the age of six months
3) Vitamin A Supplementation (2 doses per year for children 6-59 months) 4. Zinc supplementation for diarrhea management 5. Multiple-micronutrients for children under five years 6. De-worming for children (2 doses per year for children 12-59 months) 7. Iron-folic acid supplementation for pregnant mothers 8. Prevention or treatment of: a) Severe Acute Malnutrition b) Moderate Acute Malnutrition 9. Promotion of improved hygiene practices including hand washing 10. Salt Iodization 11. Iron fortification of staple foods 16 Includes USD 365,887 received from European Commission/ECHO on 1 July 2015


















