Kendra Suder IPPE Assignments SP20
25
1 Kendra Suder PHAR592 IPPE Assignments SP20 2 goals: 1. I will concisely communicate 1 drug-related problem to another healthcare professional. 2. I will effectively use and interpret 2 hospital-specific dosing protocols. Reflection: I completed my final IPPE experience at Southwest General Hospital in Middleburg Heights, Ohio. This site is a fairly busy mid-size hospital with about 350 beds and a residency program. I completed two previous IPPEs at a much smaller hospital, so I knew that this site would give me many opportunities to learn. I set out to accomplish two personal goals. My first goal was to correctly utilize two of the hospital’s site-specific dosing protocols. I was able to accomplish this goal easily as I was using dosing protocols on my very first day. The one I became most acquainted with was the vancomycin protocol. This site’s dosing protocol was very similar to the one I learned in my skills lab course when I practiced writing a vancomycin consult. It utilized weight- and creatinine-clearance based dosing with trough goals, so it was easy for me to interpret and use the protocol. I calculated loading and maintenance doses for many patients using this protocol as well as some dose adjustments. Another dosing guide I used was a heparin protocol. I have never seen a heparin protocol before, but it was easy to follow this one as it was weight-based. While dosing a heparin patient, the pharmacist also showed me how to order the APTT labs in the computer. I also briefly reviewed another dosing protocol for tPA but I did not get a chance to practice it. I enjoyed using the dosing protocols and they served as opportunities to review dosing and monitoring parameters for several medications.
Transcript of Kendra Suder IPPE Assignments SP20

1
Kendra Suder
PHAR592
IPPE Assignments SP20
2 goals:
1. I will concisely communicate 1 drug-related problem to another healthcare professional.
2. I will effectively use and interpret 2 hospital-specific dosing protocols.
Reflection:
I completed my final IPPE experience at Southwest General Hospital in Middleburg
Heights, Ohio. This site is a fairly busy mid-size hospital with about 350 beds and a residency
program. I completed two previous IPPEs at a much smaller hospital, so I knew that this site
would give me many opportunities to learn. I set out to accomplish two personal goals.
My first goal was to correctly utilize two of the hospital’s site-specific dosing protocols. I
was able to accomplish this goal easily as I was using dosing protocols on my very first day. The
one I became most acquainted with was the vancomycin protocol. This site’s dosing protocol
was very similar to the one I learned in my skills lab course when I practiced writing a
vancomycin consult. It utilized weight- and creatinine-clearance based dosing with trough goals,
so it was easy for me to interpret and use the protocol. I calculated loading and maintenance
doses for many patients using this protocol as well as some dose adjustments. Another dosing
guide I used was a heparin protocol. I have never seen a heparin protocol before, but it was easy
to follow this one as it was weight-based. While dosing a heparin patient, the pharmacist also
showed me how to order the APTT labs in the computer. I also briefly reviewed another dosing
protocol for tPA but I did not get a chance to practice it. I enjoyed using the dosing protocols and
they served as opportunities to review dosing and monitoring parameters for several medications.
2
My second goal was to present a problem to a fellow healthcare provider using the SBAR
format. I was able to practice the SBAR format with pharmacists, but I was not able to execute
this communication technique in a real-life scenario. I also observed that many of the
pharmacists I worked with used a more abbreviated SBAR method to communicate with
physicians. Often, the physicians knew the background and history of the patient, so the
pharmacists would simply identify the patient and describe only the present issue or problem
followed by a concise recommendation. The physicians and pharmacists communicated very
efficiently with each other and the dynamic was free of any aggression or hostility for all of the
interactions that I observed. Additionally, the physician almost always asked the pharmacist to
input or change the relevant medication orders. I liked observing interactions such as these
because they serve as examples of how I would like to communicate as a pharmacist. Ideally, I
would have liked to practice more interprofessional communication, but I understand that
logistically this can be difficult to execute at a busy hospital.
I had other beneficial experiences at this site that were unrelated to my goals. I attended
my first P&T committee meeting, which was another good example of interprofessional
communication. I also attended several topic discussion presentations from pharmacists and
residents. These were more casual, usually involved less than eight people, and utilized handouts
and spoken words rather than slideshows. I much prefer this method of presentation to reading
from slides and I chose to do my topic presentation in this format as well. Other activities I did
included observing a cardiac catheterization, assisting the pharmacist in the warfarin clinic,
taking part in a rapid response team for a critically ill patient, and observing a cardioversion.
Many of these experiences were spontaneous and unexpected, and they were some of my
favorite parts of my time at this site.

3
I would definitely recommend this IPPE site to other students. In fact, it is my favorite
institutional IPPE that I have done due to the positive, student-friendly environment and the
focus on learning. I could easily see myself coming back here for a residency in the future if I
choose to do so.

4
Assignment #1:
# Intervention Rationale
1 A patient with type 2 diabetes and COPD
was admitted to the ICU for respiratory
distress. He was placed on
methylprednisolone, and after
approximately 5 days of therapy, his
breathing improved but his blood glucose
readings were consistently above 200
mg/dL. The methylprednisolone was
discontinued.
Steroids such as methylprednisolone are
known to raise blood glucose. Steroids are
appropriate to treat an inflamed airway, but
due to their side effects, treating for the
shortest possible duration is preferred. Since
this patient no longer was experiencing airway
inflammation, it was appropriate to discontinue
the methylprednisolone.
2 A patient with stage 5 CKD was initially
given ampicillin every 6 hours due to an
Enterococcus bloodstream infection. The
patient’s renal function has worsened
over the past 3 days, with most recent
labs being BUN 131, SCr 7.1, and
estimated CrCl 10. The dosing interval
for the ampicillin was changed to every 8
hours.
Ampicillin is a renally cleared antibiotic with
dosage adjustments based on creatinine
clearance. The recommended dosing interval
for a CrCl of 10-50 mL/min is 6-12 hours.
Given the severity of the bloodstream
infection, the pharmacist was reluctant to
change the interval to every 12 hours, so the
pharmacist decided on an 8-hour dosing
interval instead.
3 A 76-year-old male with a history of
heart failure and an MI was on
atorvastatin 20 mg at bedtime, and the
pharmacist increased this to 40 mg at
bedtime.
The patient had an MI, or an acute coronary
syndrome. Acute coronary syndromes are
considered clinical ASCVD, and the presence
of clinical ASCVD means that this patient is in
the first of four statin benefit groups. He is a
candidate for a high-intensity statin, which
would be either 40 or 80 mg of atorvastatin.
Due to his age, the pharmacist opted for 40 mg
of atorvastatin at bedtime. Statins should also
be given at night because the body’s
cholesterol production peaks at night.
4 A 70-year-old patient with a history of
type 2 diabetes and stage 5 CKD was
taking 20 units of insulin glargine SQ
once daily. His blood glucose readings
were consistently in the 200s despite use
of short acting regular insulin before each
meal, so his insulin glargine was
increased to 40 units SQ once daily.
This patient’s poor renal function excludes him
from taking renally cleared oral diabetes
medications such as sulfonylureas. Thus, he
must rely on insulin for glucose control. His
blood glucose has been consistently high while
in the hospital, and since he is already
receiving regular insulin multiple times daily,
increasing his basal insulin dose is appropriate.
5 A patient with a severe foot infection was
initially placed on clindamycin +
vancomycin + cefepime. An incision &
drainage was done on the blister and the
infection improved, so the pharmacist de-
escalated therapy to vancomycin at a
lower dose + piperacillin/tazobactam.
Because the patient showed improvement, de-
escalation was appropriate. The physician
considered vancomycin alone, but anaerobes
are likely to cause diabetic foot infections, the
pharmacist added piperacillin/tazobactam for
anaerobic coverage.

5
6 A patient was placed on ceftriaxone 1 g
IV q24h for community-acquired
pneumonia. 1 of the 2 most recent
cultures have come back positive for a
rare MRSA strain. The patient has
completed 5 days of therapy. She is now
afebrile and her lungs are clear.
The rare strain of MRSA found in the culture
is most likely a colonizer. The patient no
longer has any signs and symptoms of
infection, so discontinuing the ceftriaxone is
appropriate. Antibiotic overuse breeds resistant
organisms and does not benefit the patient.
Assignment #2:
SOAP Note #1 is on pages 5-10
SOAP Note #2 is on pages 11-15
SOAP Note 1 Problem List:
1. Asymptomatic bacteriuria
2. Bilateral pulmonary emboli/ respiratory failure/ Anticoagulation management
3. Hypertension (HTN)/ Chronic Kidney Disease (CKD)
4. Alzheimer’s Dementia
5. Probable osteoporosis/ reduced bone density
6. Depression/ anxiety/ Neuropathy
7. Hypothyroidism
8. Glaucoma
9. Omeprazole use with unknown indication
10. Seasonal allergies
S: HPI: LG is an 88YO Caucasian female with a history of dementia and recurrent urinary tract infections
who was brought to the ED by a family member 3 days ago due to altered mental status, sudden
weakness, and limpness. She has also experienced headaches and decreased appetite. At the ED, the
patient was shown to have dehydration and also complained of shortness of breath. She denied nausea,
vomiting, diarrhea, fever, chills, or chest pain. Approximately 6 months ago, she began taking a 90-day
course of nitrofurantoin for recurrent UTIs, and this medication was stopped in the ED because she was
placed on ceftriaxone empirically for a suspected UTI (and also due to her declining renal function). Due
to the patient’s shortness of breath, the physician ordered a chest CT scan which revealed bilateral
pulmonary emboli, so the patient was also started on anticoagulation therapy. PMH: Alzheimer’s dementia, recurrent UTIs, HTN, neuropathy, depression/ anxiety, glaucoma, vaginal
prolapse, bilateral hip replacements FH: None pertinent. SH: The patient denies smoking, alcohol use, or drug use. She lives with her children. ROS: Altered mental status, weakness, limpness, headaches, and decreased appetite. Negative for nausea,
vomiting, diarrhea, diarrhea, fever, chills, or chest pain. All other systems are normal.
O: Allergies: NKDA Vitals (most recent): Temperature 36.3 C, HR 77, RR 20, BP 102/69, SpO2 96% on oxygen mask,
height=160.02 cm, ABW= 78.5 kg, pain= none reported PE: Appears alert and oriented and in no acute distress. Regular heart rate and rhythm with a 2/6 murmur
indicating tricuspid insufficiency. Lungs are clear to auscultation. Skin is warm, dry, and intact with no
edema and no lymphadenopathy. All other systems normal.
6
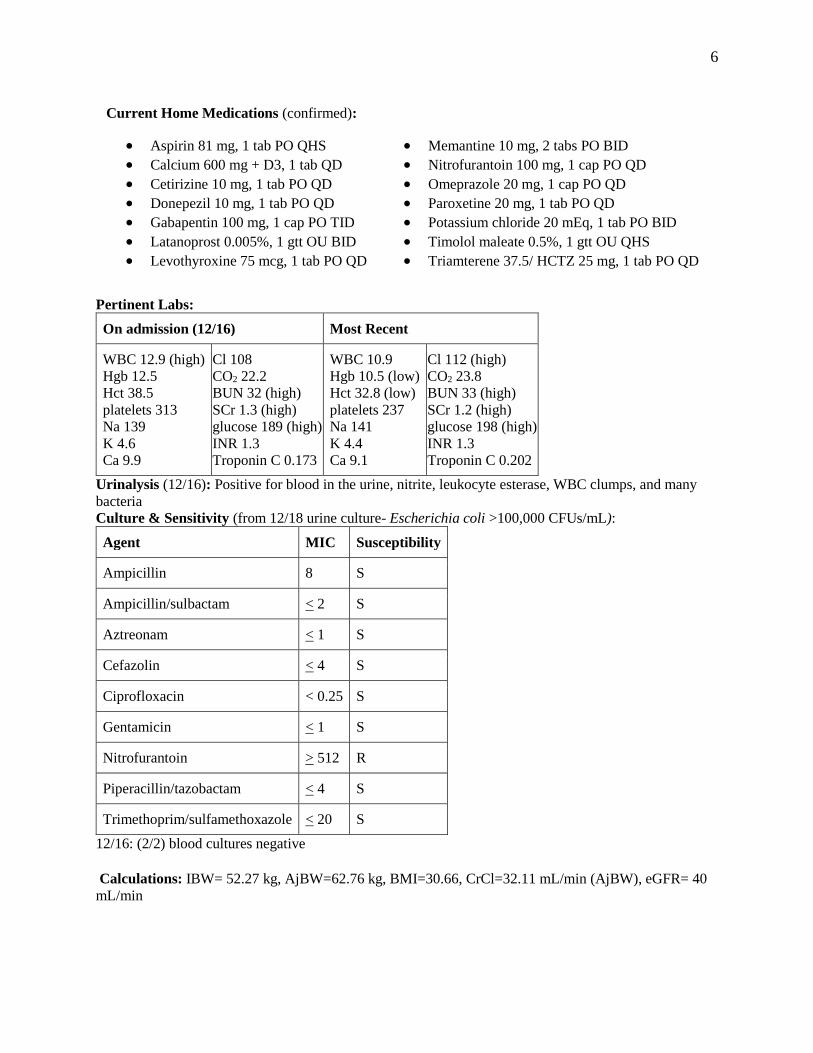
Pertinent Labs:
On admission (12/16) Most Recent
WBC 12.9 (high) Hgb 12.5 Hct 38.5 platelets 313 Na 139 K 4.6 Ca 9.9
Cl 108 CO2 22.2 BUN 32 (high) SCr 1.3 (high) glucose 189 (high) INR 1.3 Troponin C 0.173
WBC 10.9 Hgb 10.5 (low) Hct 32.8 (low) platelets 237 Na 141 K 4.4 Ca 9.1
Cl 112 (high) CO2 23.8 BUN 33 (high) SCr 1.2 (high) glucose 198 (high) INR 1.3 Troponin C 0.202
Urinalysis (12/16): Positive for blood in the urine, nitrite, leukocyte esterase, WBC clumps, and many
bacteria Culture & Sensitivity (from 12/18 urine culture- Escherichia coli >100,000 CFUs/mL):
Agent MIC Susceptibility
Ampicillin 8 S
Ampicillin/sulbactam < 2 S
Aztreonam < 1 S
Cefazolin < 4 S
Ciprofloxacin < 0.25 S
Gentamicin < 1 S
Nitrofurantoin > 512 R
Piperacillin/tazobactam < 4 S
Trimethoprim/sulfamethoxazole < 20 S
12/16: (2/2) blood cultures negative
Calculations: IBW= 52.27 kg, AjBW=62.76 kg, BMI=30.66, CrCl=32.11 mL/min (AjBW), eGFR= 40
mL/min
Current Home Medications (confirmed):
Aspirin 81 mg, 1 tab PO QHS
Calcium 600 mg + D3, 1 tab QD
Cetirizine 10 mg, 1 tab PO QD
Donepezil 10 mg, 1 tab PO QD
Gabapentin 100 mg, 1 cap PO TID
Latanoprost 0.005%, 1 gtt OU BID
Levothyroxine 75 mcg, 1 tab PO QD
Memantine 10 mg, 2 tabs PO BID
Nitrofurantoin 100 mg, 1 cap PO QD
Omeprazole 20 mg, 1 cap PO QD
Paroxetine 20 mg, 1 tab PO QD
Potassium chloride 20 mEq, 1 tab PO BID
Timolol maleate 0.5%, 1 gtt OU QHS
Triamterene 37.5/ HCTZ 25 mg, 1 tab PO QD

7
1. Asymptomatic bacteriuria
A: Assessment statement: The patient has asymptomatic bacteriuria as evidenced by the absence of urinary
symptoms despite a urine culture positive for E. coli (>100,000 CFU/mL) and altered mental status. The
patient also experienced sudden weakness and limpness, elevated WBC (12.9) upon admission, and a
recently decreased appetite, but she is afebrile and has no CVA tenderness, nausea/vomiting, or flank
pain. Urinalysis on 12/16 showed cloudy, yellow urine with albumin 100 mg/dL and positive for blood,
nitrite, leukocyte esterase, WBC clumps, and many bacteria with occasional mucous. The E. coli cultured
in the urine was notably resistant to nitrofurantoin, and 4/4 blood cultures on 12/16 were negative for any
pathogens. The patient has been taking nitrofurantoin 100 mg PO BID since 6/12 for recurrent urinary
tract infections and still takes this medication at home. On 12/16 she received ceftriaxone, 1g IV in the
ED and her nitrofurantoin was not given. Since starting empiric therapy, her WBC decreased to 10.9 (as
of 12/18). P: Goals: 1) Prevent unnecessary antibiotic use, 2) Prevent future infections, 3) Improve patient’s quality of life Pharmacologic: D/C nitrofurantoin. Initiate cephalexin, 250 mg PO QD for 90 days.
Non-pharmacologic: Adequate hydration, reminders to drink Monitoring and Follow-up: Monitor for signs of anaphylaxis after first dose of cephalexin. Monitor daily:
hydration status, side effects and toxicities of cephalexin (diarrhea, vaginal yeast infections) and
resolution of signs/symptoms (dehydration, headache, decreased appetite, weakness). Follow-up with
primary care physician in 2 weeks. At follow-up appointment obtain CBC and assess for signs of liver
toxicity (i.e. jaundice, decreased appetite) and CNS effects (confusion). Follow-up monthly thereafter. At
the 3-month mark assess efficacy and safety again to determine whether therapy should be continued. Rationale: Due to the absence of urinary symptoms which are typical of cystitis and the absence of flank
pain and CVA tenderness usually seen in pyelonephritis, this patient likely has asymptomatic bacteriuria
rather than a true urinary tract infection. In the emergency department, LG was given ceftriaxone 1 g IV,
and this would be appropriate empiric therapy if the patient had a true UTI. In terms of definitive therapy,
Escherichia coli, which is a Gram-negative rod, was cultured from the urine. The organism was shown to
be sensitive to several antibiotics. However, according to the 2005 IDSA guidelines regarding
asymptomatic bacteriuria (and the 2019 update), asymptomatic bacteriuria should only be treated in
pregnant women, those undergoing a urologic intervention, and renal transplant recipients. This patient
does not fall into one of these groups, so the IDSA recommends careful observation and assessment of
other causes of the patient’s altered mental status. Administration of unnecessary antibiotics will place the
patient at risk for infections such as C. difficile, increased drug resistance, and serious or undesirable
adverse effects. Though antibiotics would be inappropriate to treat asymptomatic bacteriuria, this patient
is a candidate for prophylactic antibiotics. According to the 2019 AUA/CUA/SUFU guidelines on the
management of recurrent UTIs in women, antibiotics may be considered for UTI prophylaxis in women
of all ages with recurrent UTIs. Prophylaxis may be continuous or intermittent (post sexual intercourse)
and durations of 3-12 months have been used in practice. Options for continuous prophylaxis include
trimethoprim/sulfamethoxazole (TMP-SMX), cephalexin, nitrofurantoin, fosfomycin, or TMP. The 2019
Beers Criteria recommends avoiding nitrofurantoin in patients > 65 years with a CrCl of <30 mL/min, and
since this patient has a CrCl of approximately 32 mL/min, it is reasonable to stop her nitrofurantoin as her
kidneys will likely continue to decline. Additionally, the E. coli specimen previously mentioned was
resistant to nitrofurantoin, so the medication will likely be of no use in preventing future UTIs. TMP-
SMX and TMP are not good choices for prophylaxis due to adverse effects including nephrotoxicity.
Fosfomycin is high in cost and not commonly used. Therefore, cephalexin 250 mg daily is a reasonable
agent to use for continuous UTI prophylaxis in this patient. Its adverse effects are commonly GI-related,
and other effects such as blood glucose abnormalities can be managed with regularly scheduled meals. It
does have the potential to cause CNS effects such as dizziness and confusion, but because the

8
prophylactic dose is low, these effects are likely to be minimal. After a 90-day course of therapy, the
patient can be re-assessed to determine whether a longer duration would provide further benefits. In terms
of nonpharmacologic therapy, adequate hydration is essential for LG since dementia patients have a
decreased sense of thirst making them prone to dehydration.
Patient Education: -Make sure to stay well hydrated
-The most common side effects of cephalexin are nausea, vomiting, and diarrhea. Take the medication
with food to help minimize stomach upset.
-Get medical help if you notice signs of an allergic reaction such as rash, feeling hot or flushed, or
difficulty breathing, especially with the first dose.
-Cephalexin may affect blood sugar. Caregivers, please make sure that the patient eats meals on a regular
basis.
-Cephalexin may cause vaginal yeast infections in women.
2. Bilateral pulmonary emboli/ Respiratory Failure/ Anticoagulation Management A: Assessment: Patient has had pulmonary emboli (PE) as evidenced by shortness of breath (SOB) and a
chest CT scan on 12/16 revealing bilateral pulmonary emboli and moderate clot burden. Imaging was also
significant for cor pulmonale with right ventricular enlargement. D-dimer level was not obtained. As of
12/19, she is also experiencing acute hypoxic respiratory failure, most likely exacerbated by her PE, and a
second chest CT revealed a small right pleural effusion, infiltrates, and collapsing of the right lung base.
The patient denies chest pain and she is negative for tachypnea, tachycardia, or distended neck veins. She
has been taking nitrofurantoin at home which carries a risk for pulmonary toxicity and may have
contributed to her SOB as well. In the ED, she received anticoagulation therapy, which decreased her
SOB, and is currently receiving enoxaparin 80 mg SQ QHS. For her respiratory failure, she is receiving
oxygen and is set to receive spirometry and bronchodilation. Her most recent INR is 1.3 and she is stable
except for episodes of hypotension/ syncope. At home, she is taking aspirin 81 mg QHS, most likely for
primary prevention. Recommend continue current interventions, obtain thorough family history, and re-
evaluate the patient upon discharge to determine appropriate oral long-term anticoagulation therapy based
on her renal function and insurance coverage. Based on the patient’s current renal function, either
apixaban or rivaroxaban would be appropriate, or warfarin if cost is a concern; to determine duration of
therapy, risk factors (including genetic) should be investigated and taken into consideration.
3. HTN/CKD A: Assessment: The patient has been diagnosed with hypertension as evidenced by statements in her past
medical history, and she also has undiagnosed CKD as evidenced by a calculated GFR of 40 mL/min. She
has been hypotensive (SBP ~100) and experiencing episodes of syncope while in the hospital, most likely
due to her PE. Home BP readings are not available. Her urinalysis showed albumin 100 mg/dL in the
urine, and her most recent BUN and SCr are 33 and 1.2 respectively. ACR and I&Os not completed. She
is currently taking triamterene 37.5 mg/ HCTZ 25 mg, 1 tab PO QD. Recommend monitoring BP daily
once discharged home, continue current therapy, and follow up with physician following resolution of
infection to monitor renal function and determine appropriate course of action for CKD.
4. Alzheimer’s Dementia A: Assessment: LG has been diagnosed with Alzheimer’s dementia as evidenced by statements in her past
medical history; a brain CT scan on 12/16 was notable for brain volume loss, white matter changes, and
small vessel ischemia. The patient presented to the ED with altered mental status but this could be
attributed to her UTI. She is currently taking donepezil 10 mg, 1 tab PO QD, and memantine 10 mg, 2

9
tabs PO BID. Recommend continue current therapy and follow up with physician for regular assessments
such as MMSE. 5. Probable osteoporosis/ reduced bone density A: Assessment: The patient has probable osteoporosis and reduced bone density as evidenced by a history of
falls. T-score was not available. She was seen in the ED on 8/28 for recurrent falls at home, and she has
also had bilateral hip replacements. She has been deemed a fall risk while inpatient for her UTI. At home,
she is taking calcium 600 mg + vitamin D, 1 tab PO QD. Recommend continue current therapy, reduce
fall hazards at home, and follow up with primary care physician to complete DXA scans and other tests as
appropriate if not previously completed.
6. Depression/ Anxiety/ Neuropathy A: Assessment: LG has depression, anxiety, and “questionable” neuropathy as evidenced by statements in
her past medical history. She has not complained of any bothersome symptoms, though her dementia and
mental status does create a communication barrier. She is currently taking gabapentin 100 mg PO TID
and paroxetine 20 mg QD. Because gabapentin has been associated with lung damage and the patient
recently experienced a PE and respiratory failure, the use of this medication should be re-evaluated.
Recommend continue current therapy pending a diagnostic workup for neuropathy. If the patient does not
have neuropathy, recommend discontinuing gabapentin and continuing paroxetine.
7. Hypothyroidism A: Assessment: The patient has been diagnosed with hypothyroidism as evidenced by statements in her past
medical history. TSH values and other information unavailable. She is currently taking levothyroxine 75
mcg, 1 tab PO QD. Recommend continue current therapy and re-evaluate if patient becomes symptomatic
or TSH levels change, and obtain TSH every 6-12 months if stable (obtain 6 weeks after any dosage
adjustments).
8. Glaucoma A: Assessment: The patient has glaucoma as evidenced by statements in her past medical history. No other
information is available. She is currently taking timolol maleate 0.5%, 1 gtt OU QHS. Recommend
continue current therapy and follow-up with physician/ ophthalmologist for eye exams as appropriate.
9. Omeprazole use with unknown indication A: Assessment: LG likely has either GERD or PUD as evidenced by statements in her past medical history
regarding the need for “GI prophylaxis” and her use of omeprazole 20 mg daily at home. Recommend
continue current therapy for now and follow with primary care provider to obtain diagnostic history, but
discontinue therapy if no clear diagnosis is present due to the potential for serious adverse effects.
10. Seasonal Allergies A: Assessment: LG has seasonal allergies as evidenced by statements in her past medical history. No other
information is available. She is currently taking cetirizine 10 mg QD and latanoprost 0.005% 1 gtt OU
BID. Recommend continue current therapy and re-assess if patient becomes symptomatic.

10
References 1. Nicolle LE, Bradley S, Colgan R, et al. Infectious Diseases Society of America guidelines for the
diagnosis and treatment of asymptomatic bacteriuria in adults. Clin Infect Dis. Mar
2005;40(5):643-54. Epub 2005 Feb 4. Available from:
https://academic.oup.com/cid/article/40/5/643/363229
2. Nicolle LE, Gupta K, Bradley SF, et al. Clinical practice guideline for the management of
asymptomatic bacteriuria: 2019 update by the Infectious Diseases Society of America. Clin Infect
Dis [Internet]. 2019 May 2;68(10):e83-e110. Available from: https://www.idsociety.org/practice-
guideline/asymptomatic-bacteriuria/
3. Anger J, Lee U, Ackerman AL. Recurrent uncomplicated urinary tract infections in women:
AUA/CUA/SUFU guideline. J Urol [Internet]. Aug 2019;202(2):282-289. Available from:
https://www.auajournals.org/doi/10.1097/JU.0000000000000296
4. 2019 American Geriatrics Society Beers Criteria Update Expert Panel. AGS Beers Criteria for
Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc. 2019;67(4):674-
694. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/jgs.15767
5. National Kidney Foundation. GFR calculator [Internet]. National Kidney Foundation, Inc. c2019.
Available from: https://www.kidney.org/professionals/kdoqi/gfr_calculator
6. Lexicomp [Internet]. Hudson (OH): Wolters Kluwer. c1978-2019. [updated 2019 Dec 19; cited
2019 Dec 20]; [about 8 screens]. Available from:
http://online.lexi.com.ezproxy.findlay.edu:2048/lco/action/home

11
SOAP Note 2 Problem List:
1. Altered mental status/ Bipolar I Exacerbation/ Dehydration
1. Type 2 Diabetes Mellitus
2. Coronary Artery Disease (CAD)/ Hypercholesterolemia
3. Hypothyroidism
4. Hypertension
5. Resolved Vitamin B12 deficiency
6. Peripheral neuropathy
HPI: HK is a 70YO Caucasian female with a history of bipolar I disorder with psychotic features who
was admitted to the geriatric psychiatry unit for an evaluation due to altered mental status, delirium, and
paranoid behavior as well as dehydration. In September 2019, she spent 2 weeks in the ICU due to
delirium following anesthesia after a carotid endarterectomy. She was stable until last week when she
became delirious again. She has previously been stable on lithium + olanzapine + sertraline, but her
sertraline was discontinued during her ICU stay and restarted on 12/29/19. She has had 4 prior psychiatric
hospitalizations, her first being in 1975 following her first husband’s death, and has undergone several
sessions of ECT. She has a history of two instances of suicidal ideation and one suicide attempt in 2009
which led to her diagnosis of bipolar disorder.
PMH: Bipolar I disorder, type 2 diabetes mellitus x10-12 years, coronary artery disease, hypertension,
hypercholesterolemia, hypothyroidism, vitamin B12 deficiency, peripheral neuropathy
Surgical: Recent carotid endarterectomy, coronary artery bypass graft (CABG) x3, oophorectomy x1 FH: 15 years ago, 2 male cousins died by suicide within 4 years of one another
SH: The patient occasionally has wine. She quit smoking 33 years ago and quit caffeine 6 weeks ago. She
is not currently working and lives with her second husband. ROS: Positive for decreased sensation in the hands, “pocketing food” in the cheeks, and delayed
swallowing. Positive for a history of depressive episodes with psychotic paranoia, paranoid delusions, and
grandiose delusions. Negative for dizziness, weakness, chest pain, SOB, and extrapyramidal symptoms
(EPS).
O: Allergies: Bactrim, penicillins, and sulfa drugs; reactions unknown
Vitals (most recent): Temperature 36.6 C, HR 77, RR 18, BP 149/76, SpO2=94%, height=160 cm,
ABW= 69.5 kg, pain= none reported
PE: Appears alert in no acute distress. Periorbital edema and masked facies. Hearing aids bilaterally.
Normal heart rhythm. Diminished lung sounds anteriorly and posteriorly. All other systems normal.
Current Home Medications (confirmed):
Amlodipine 10 mg, 1 tab PO QD
Aspirin 81 mg, 1 tab PO QD
Clopidogrel 75 mg, 1 tab PO QD
Ezetimibe 10 mg, 1 tab PO QD
Gabapentin 100 mg, 1 cap PO TID
Olanzapine 10 mg, 1 tab PO QHS
Glimepiride 4 mg, 1 tab PO QD
Insulin glargine, 28 units SQ QHS
Levothyroxine 88 mcg, 1 tab PO QD
Lithium 300 mg, 1 tab PO BID
Losartan 50 mg, 1 tab PO QD
Rosuvastatin 40 mg, 1 tab PO QD

12
Pertinent Labs:
On admission (12/29) Most Recent (1/1-1/2)
WBC 13.7 (high) Hgb 11.9 (low) Hct 36.3 platelets 227 Na 141 K 4.4 Ca 9.4 Cl 107 CO2 29.4 BUN 22 (high)
SCr 1.1 (high) glucose 132 (high)
Serum lithium 0.8 total cholesterol 93 mg/dL
HDL 28 mg/dL (low)
LDL 24 mg/dL
TG 204 mg/dL (high) free T4 1.26 ng/dL
free T3 1.6 pg/mL (low)
TSH 2.5 mIU/mL
WBC 18.1 Hgb 12.0 Hct 35.9 (low) platelets 227 Na 136 K 4.5 Ca 10.1
Cl 103 CO2 28.7 BUN 42 (high) SCr 1.2 (high) glucose 79
Serum lithium 1.3 (high)
Urinalysis: negative
Calculations: IBW= 52.4 kg, AjBW=59.24 kg, BMI=27.15, CrCl=40.8 mL/min (AjBW)

13
1. Altered Mental Status/ Bipolar I Exacerbation/ Dehydration A: Assessment statement: The patient has altered mental status secondary to dehydration and a Bipolar I
depressive episode as evidenced by delusional thoughts, paranoid thoughts surrounding her husband, flat
affect, slow responses, poor eye contact, impaired focus and concentration, and poor attention. Her
urinalysis was negative, her most recent BUN is 42, she is not eating or drinking adequately, and her
lithium level was 1.3 mEq/L on 1/2/20.
P: Goals: 1) Remission of symptoms for the current episode, 2) Prevent relapses, 3) Improve psychosocial
functioning, 4) Minimize adverse effects and suicide risk, 5) Maximize adherence Pharmacologic: Continue sertraline at previous dose of 50 mg PO daily. Continue olanzapine 10 mg, 1
tab PO QHS and lithium 300 mg PO BID with meals.
Non-pharmacologic: Psychotherapy, fluid replacement, diet and exercise Monitoring and Follow-up: Monitor adherence on a medication log and monitor for mood episodes using
a mood chart or journal. Continue to manage comorbidities (diabetes, hypothyroidism). For lithium,
obtain serum concentration every 12 hours until dehydration resolves, then every 2 weeks until a
therapeutic level is reached (0.6-1.2 mEq/L and stable mood). Thereafter, monitor lithium levels every 3
months due to the patient’s age and comorbidities. Also monitor sodium levels, A1c, BUN, SCr and
weight every 3 months. Every 6 months, obtain thyroid panel, lipid panel, and ECG.
Rationale: Because this patient’s altered mental status and delirium presented acutely following a
surgery, and because she is not cognitively impaired at baseline per her medical records, she likely does
not have dementia. Rather, her mental status changes are likely due to a combination of dehydration and
her current bipolar depressive episode. CANMAT/ISBD 2018 guidelines list lithium or divalproex + an
SSRI as a first-line option for the acute treatment of bipolar I depression. HK is currently taking lithium
and recently restarted sertraline, so these two agents are a reasonable choice. However, the sertraline will
take approximately 4-6 weeks to exert its full antidepressant effects, so the efficacy of the regimen cannot
be assessed until then.
For maintenance therapy, the patient was previously controlled on a combination of olanzapine + lithium
+ sertraline. Olanzapine is a second-line antipsychotic agent per CANMAT/ISBD due to its adverse
effects. These include weight gain, new-onset type 2 diabetes, metabolic syndrome, and anticholinergic
effects. However, the guidelines do note that olanzapine has level 1 evidence for efficacy, and it has
previously been effective for this patient when used in a combination regimen. HK’s type 2 diabetes
seems to have been well-controlled at home based on her A1C, and her lipids also seem to be well-
controlled. Therefore, continuing olanzapine therapy due to its effectiveness and manageable adverse
effects for HK is reasonable. Though it is first-line for acute therapy as stated above, sertraline is not
specifically recommended for maintenance therapy (alone or in combination with other agents) per the
aforementioned guidelines. However, since HK has no contraindications to its use and is reported to have
done well on her previous regimen, continuing the sertraline after the resolution of her depressive episode
is justifiable. HK is also taking lithium as part of her maintenance regimen. Lithium is a first-line agent
per CANMAT/ISBD for maintenance of bipolar I disorder as monotherapy, but it is not first-line when
combined with olanzapine. However, it does have antidepressant and mood stabilizing effects which
explains its use in this patient. HK has been on lithium for many years, so long-term effects are a concern.
HK has hypothyroidism, which is likely a result of lithium use, and she is overweight, which may be
lithium-related weight gain. The patient did have a recent history of an elevated WBC count which is a
known side effect of lithium. Lithium is also nephrotoxic, and it should be avoided in patients whose CrCl
is less than 30 mL/min. HK’s most recent CrCl is about 40 mL/min. Switching HK to another mood
stabilizer such as divalproex would be beneficial to her in terms of reducing adverse effects. Divalproex
in particular is less nephrotoxic. However, dose adjustments and titrations of mood stabilizers can take
several weeks. Because HK has just restarted sertraline and is currently in a depressive episode, she is at
risk of switching to a manic state. She must be on a mood stabilizer at a therapeutic dose to prevent this.

14
Therefore, it is reasonable to keep her on lithium, her current mood stabilizer. She is currently taking 600
mg total per day, which is a low dose, and this will help mitigate adverse effects. Additionally,
discontinuation of lithium may cause her to experience discontinuation-induced refractoriness, and she
may never again respond to lithium. If her renal function continues to decline and her CrCl approaches 30
mL/min, then discontinuation of lithium (via a slow taper) and starting a different mood stabilizer will be
necessary. Divalproex is ideal as it can be combined with antipsychotics in a similar manner to lithium
per the guidelines. In terms of non-pharmacologic therapy for HK, reminding her of the importance of
eating and drinking when she is depressed are critically important to prevent further dehydration and
lithium toxicity (her serum level is 1.3 mEq/L which is slightly elevated). She particularly cannot be on a
sodium- or fluid-restricted diet. Psychotherapy sessions need to be put into place for her as well, and these
should be continued long-term.
Patient Education: -Make sure to stay well hydrated. This is especially important if you are vomiting, have diarrhea, have a
fever, or are heavily sweating.
-Avoid alcohol or excessive caffeine. These can dehydrate you and affect your sleep and mood.
-Lithium may cause acne, alopecia, worsening psoriasis, decreased libido, dry mouth, or altered taste. Let
your doctor or pharmacist know if these become bothersome for you.
-Some people may gain weight on lithium therapy. Eat a balanced diet and incorporate mild exercise into
your routine. This will help you manage your diabetes as well.
-Take your medication consistently, even if you think you do not need it or your mood is better.
-Get medical help if you suddenly experience symptoms such as hand tremors, muscle twitching, slurred
speech, sleepiness, vertigo, confusion, loss of appetite, incontinence, vomiting or diarrhea.
2. Type 2 Diabetes Mellitus/ Overweight A: Assessment: HK has type 2 diabetes mellitus that was controlled at home as evidenced by an A1c of 7%
and blood glucose readings averaging between 75-136 while inpatient. Her glucose has been as low as 29
due to lack of food and fluid intake recently, so her antidiabetic medications have been held. HK is also
overweight as evidenced by a BMI of 27. At home, she has been taking metformin 1000 mg PO BID,
insulin glargine 28 units SQ daily, and glimepiride 4 mg daily. Recommend close monitoring of blood
glucose (one reading in the morning before breakfast and another reading 2 hours after a meal) at home
upon discharge, and if readings continue to be low, consider discontinuation of glimepiride due to its
propensity to cause severe hypoglycemia per AGS Beers criteria. Otherwise, continue current home
medications, and educate patient on diet and mild exercise to control weight. Also obtain A1c every 3
months.
3. CAD/Dyslipidemia A: Assessment: The patient has coronary artery disease and hypercholesterolemia as evidenced by a history
of CABG x 3 and carotid endarterectomy and labs as follows: total cholesterol 93 mg/dL, HDL 28 mg/dL
(low), LDL 24 mg/dL, TG 204 mg/dL (high). Pretreatment lipid panel not available. The patient is
currently aspirin 81 mg, 1 tab PO QD, clopidogrel 75 mg, 1 tab PO QD, ezetimibe 10 mg, 1 tab PO QD
and rosuvastatin 40 mg (high-intensity statin), 1 tab PO QD. Recommend continue dual antiplatelet
therapy. For dyslipidemia, recommend continue current therapy as long as patient tolerates the high-
intensity statin; also recommend diet and lifestyle modifications. If statin becomes intolerable then
moderate-intensity therapy (e.g., rosuvastatin 5 or 10 mg) can be considered.
4. Hypothyroidism
A: Assessment: HK has hypothyroidism as evidenced by statements in her past medical history and labs as
follows: free T4 1.26 ng/dL, free T3 1.6 pg/mL (low), and TSH 2.5 mIU/mL. She is currently taking

15
levothyroxine 88 mcg, 1 tab PO QD. Recommend continue current therapy, re-evaluate if patient
becomes symptomatic, and obtain TSH every 6-12 months (maintain a goal TSH of 0.4–4.0 mIU/L).
5. HTN
A: Assessment: HK has hypertension as evidenced by statements in her past medical history. Home BP
readings are unavailable. SBP has ranged from ~103-166 while inpatient and the patient has been in poor
health due to hypoglycemia and dehydration predominantly. HK is currently taking amlodipine 10 mg, 1
tab PO QD and losartan 50 mg, 1 tab PO daily. Recommend to keep a log of daily BP readings at home,
continue current medications, and show log to primary care provider at next appointment.
6. Resolved Vitamin B12 Deficiency A: Assessment: The patient has previously had a vitamin B12 deficiency as evidenced by statements in her
past medical history. Her most recent vitamin B12 level was 1290 ng/mL on 12/29 and no supplements
were found in her medication history. Her folate level on 12/29 was 48.4 ng/mL. Metformin use may lead
to B12 deficiency, while kidney and liver dysfunction may lead to elevations in B12 levels, so
recommend obtaining methylmalonic acid (MMA) and homocysteine levels if B12 deficiency is
suspected in the future.
7. Peripheral neuropathy A: Assessment: HK has a history of peripheral neuropathy as evidenced by statements in her past medical
history. Upon admission she complained of decreased sensation in her hands but has not mentioned any
symptoms recently. She currently takes gabapentin 100 mg PO TID for neuropathy. Recommend continue
current therapy and re-evaluate if bothersome symptoms arise.
References 1. Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments
(CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the
management of patients with bipolar disorder. Bipolar Disord [Internet]. Mar 2018;20(2):97-170.
Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5947163/
2. American Geriatrics Society Beers Criteria Update Expert Panel. AGS Beers Criteria for
Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc [Internet].
2019;67(4):674-694. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/jgs.15767
3. Lexicomp [Internet]. Hudson (OH): Wolters Kluwer. c1978-2019. [updated 2020 Jan 1; cited
2020 Jan 3]; [about 8 screens]. Available from:
http://online.lexi.com.ezproxy.findlay.edu:2048/lco/action/home

16
Assignment #3:
1. Vancomycin dosing: Recommend a loading dose and maintenance dose of vancomycin
for a 79 YO female with cellulitis with SCr 1.1, weight 88 kg, and height 5’5”.
Loading dose is 15-20 mg/kg using ABW, and doses are rounded to the nearest 250 mg
per hospital protocol.
15-20 mg/kg * 88 kg= 1320-1760 mg/kg
LD= 1750 mg IV x1
To determine the maintenance dose, the pharmacist needs to calculate the patient’s
creatinine clearance.
ABW= 88 kg. IBW= 45.5 kg + (2.3* 5 inches) = 57 kg
The patient is >30% over her IBW, so AjBW should be used for CrCl:
AjBW= 0.4(88-57) + 57= 69.4 kg
CrCl= [(140-79) (69.4 kg)/ (72*1.1)] * 0.85= 45.43 mL/min
Per the hospital nomogram, an appropriate maintenance dose and interval is 1250
mg IV q 18h. However, the hospital does not utilize 18-hour dosing intervals (and
the patient is elderly), so this was adjusted to 1250 mg q 24 h.
Monitoring parameters:
Obtain a trough before the 4th loading dose (or 5th total dose) of vancomycin and
aim for a trough goal of 10-15 mcg/mL based on infection severity.
Also for efficacy, monitor for resolution of the cellulitis and resolution of
signs/symptoms of infection.
For toxicity, monitor for hypotension, flushing, rash, chills, nephrotoxicity,
ototoxicity, and phlebitis. If Red Man Syndrome occurs (characteristic red rash on
face, neck, and limbs), dilute the antibiotic and/or extend the infusion time to 1.5-
2 hours.
2. Warfarin dosing: A 45 YO female with a goal INR of 2-3 comes in to the clinic with
INR 4.9 today. She has been taking 5 mg warfarin every day. Warfarin will be held for 2
days due to her high INR. Create a new dosing regimen for the patient.
Her INR is supratherapeutic, indicating that her total weekly dose (TWD) of
warfarin needs to be decreased by 10-15%.
TWD= 5 mg * 7 days= 35 mg
10-15% of 35= 3.5-5.25, so her new TWD should be between 29.75-31.5 mg
Considering that the patient has 5 mg tablets at home, a reasonable TWD would
be 30 mg.
Her new dosing regimen should be 5 mg warfarin by mouth daily except 2.5
mg (1/2 tablet) on Monday and Friday.
Monitoring parameters:
Check INR in 2 days, then resume warfarin. Thereafter, come back every 4 weeks to
check INR.
Monitor for signs/symptoms of excessive bleeding such as unusual bruising, pink or
brown urine, frequent nose bleeds, bleeding gums, or cuts that take a long time to stop
bleeding.
Monitor for chest pain, shortness of breath, headaches, dizziness, or falls, and get
medical help for serious or debilitating symptoms.
Inform physician of any diet or medication changes.

17
3. Digoxin Dosing: An elderly female is taking digoxin for atrial fibrillation with rapid
ventricular rate. She does not have heart failure. Her renal function has rapidly declined
due to infection and her estimated GFR is 18 mL/min. Her current digoxin dose is 125
mcg daily and her digoxin level was 3.66 ng/mL taken 6 hours after her last dose. Based
on her current GFR, adjust her digoxin dose.
Her digoxin level is supratherapeutic. The target serum concentration for this
patient is 0.8-2 ng/mL.
Patients with GFR 10-50 mL/min should receive 62.5 mg every 24-36 hours. This
patient’s GFR is nearer to the lower end of this range, so an appropriate dose is
62.5 mg every 36 hours.
Monitoring parameters:
Draw serum concentrations at least 6-8 hours after the last dose.
Monitor for signs and symptoms of digoxin toxicity including confusion, loss of
appetite, nausea/vomiting/diarrhea, irregular pulse, arrhythmias, and vision changes.
Monitor heart rate and rhythm and get periodic ECGs.
Monitor potassium, magnesium, and calcium levels periodically.
Inform physician of any diet or medication changes.
18
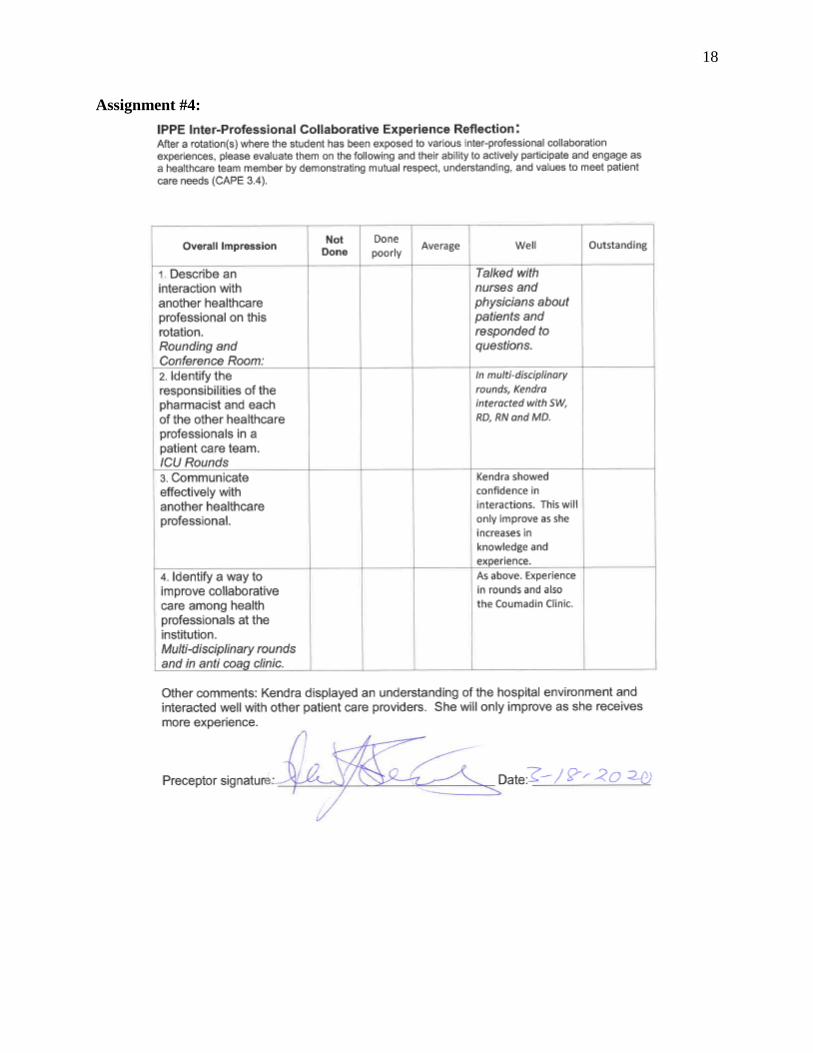
Assignment #4:
19
Assignment #5: Topic presentation is on pages 19-22 CGRP Antagonists: Mechanism, Therapeutics, and Role in Migraine Treatment
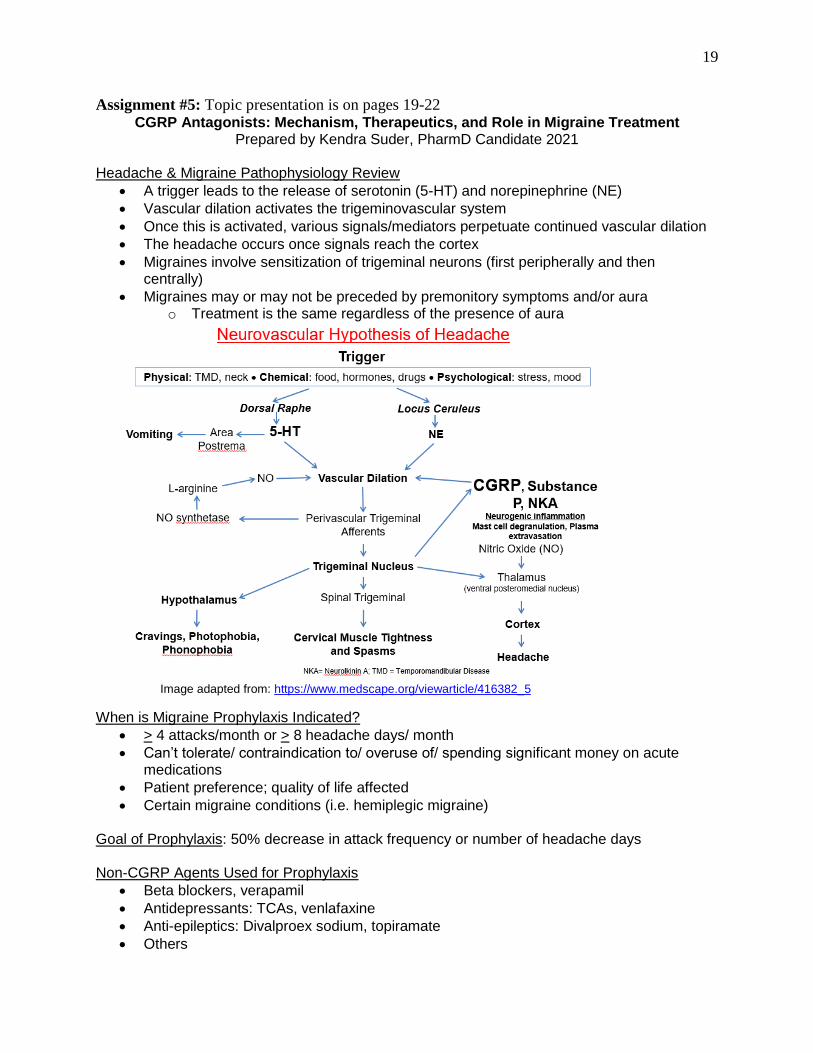
Prepared by Kendra Suder, PharmD Candidate 2021 Headache & Migraine Pathophysiology Review
A trigger leads to the release of serotonin (5-HT) and norepinephrine (NE)
Vascular dilation activates the trigeminovascular system
Once this is activated, various signals/mediators perpetuate continued vascular dilation
The headache occurs once signals reach the cortex
Migraines involve sensitization of trigeminal neurons (first peripherally and then centrally)
Migraines may or may not be preceded by premonitory symptoms and/or aura o Treatment is the same regardless of the presence of aura
When is Migraine Prophylaxis Indicated?
> 4 attacks/month or > 8 headache days/ month
Can’t tolerate/ contraindication to/ overuse of/ spending significant money on acute medications
Patient preference; quality of life affected
Certain migraine conditions (i.e. hemiplegic migraine)
Goal of Prophylaxis: 50% decrease in attack frequency or number of headache days Non-CGRP Agents Used for Prophylaxis
Beta blockers, verapamil
Antidepressants: TCAs, venlafaxine
Anti-epileptics: Divalproex sodium, topiramate
Others
Image adapted from: https://www.medscape.org/viewarticle/416382_5

20
Fig. 5. From: FA Russell, et al. Physiol Rev. Oct 2014;94(4):1099-1142.
What is CGRP?
Calcitonin gene-related peptide, a 37-amino acid neuropeptide
Binds to CLR-RAMP receptors and mediates effects through a variety of GPCRs
Role in other conditions besides migraine o Cardioprotective (protects against hypertension, hypertrophy, inflammation) o Promotes wound healing, protective effect on aging o But pro-inflammatory in arthritis, may promote obesity
In migraine: promotes vasodilation and mast cell degranulation o CGRP antagonists serve to block these effects
CGRP Monoclonal Antibodies (-mabs)
Common administration counseling points: o Inject in abdomen, thigh, or upper arm o Avoid tender, red, bruised, irritated, or infected skin o Refrigerate, protect from light, do not freeze or shake o Allow to come to room temperature for 30 minutes prior to use
Common adverse effects: antibody development, injection site reaction
Hepatic/renal impairment not anticipated to affect pharmacokinetics
Unknowns: Elderly populations, pregnancy/breastfeeding safety

21
Name Target Dosing/ Administration/ t½
Cost (AWP)*
Unique features/ pearls
Erenumab-aooe (Aimovig)
Receptor 70 mg SQ once a month Some patients: 140 mg monthly (half-life 28 days)
$690 -Single-use autoinjector -Do not inject within 2 inches of navel -Stable at room temp. for up to 7 days -Causes constipation
Fremanezumab-vfrm (Ajovy)
Ligand 225 mg SQ once a month OR 675 mg q 3 months (half-life 31 days)
$690 -Prefilled syringe -For the 675 mg dose, give 3 consecutive injections at the same body site (but not the exact same location) -Stable at room temp. for up to 24 hours -Those with cardiovascular disease excluded from clinical trials
Galcanezumab- gnlm (Emgality)
Ligand 240 mg SQ loading dose, followed by 120 mg SQ once a month (half-life 27 days)
100 mg/ml: $575 120 mg/mL: $690
-Auto-injector or prefilled syringe -Also approved for cluster headaches (different dosing)
*average wholesale price
CGRP Antagonists Place in Therapy: Summary
Patients who are a candidate for prophylaxis
Patients who have already tried or cannot take other therapies
Willing to give an adequate trial (at least 2 months)
Able to give injections
Can afford the medication New Agent: Ubrogepant (Ubrelvy)
Approved 12/23/19
Orally administered, small-molecule CGRP antagonist
Indicated for treatment of migraine only (not prophylaxis)
Common side effects: drowsiness, nausea, dry mouth
Metabolism: Substrate of BCRP/ABCG2, CYP3A4 (major), OATP1B1/1B3 (SLCO1B1/1B3), P-glycoprotein/ABCB1
Drug interactions! Contraindicated with use of strong CYP3A4 inhibitors
Thought that it may replace triptans in the treatment of acute migraine
Another oral agent called atogepant is in development

22
References
1. Figure 1. Neurovascular hypothesis of headache. From: Medscape [Internet]. Medscape, c2019. New treatment options in migraine (updated Mar 2001; cited 2019 Dec 30];[about 1 screen]. Available from: https://www.medscape.org/viewarticle/416382_5
2. Silberstein SD. Preventive migraine treatment. Continuum (Minneap Minn) [Internet]. Aug 2015 [cited 2019 Dec 30];21(4 Headache):973-89. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4640499/
3. Russell FA, King R, Smillie SJ, Kodji X, Brain SD. Calcitonin gene-related peptide: physiology and pathophysiology. Physiol Rev [Internet]. Oct 2014;94(4):1099-142. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4187032/
4. Lexicomp [Internet]. Hudson (OH): Wolters Kluwer. c1978-2019. [cited 2019 Dec 30]; [about 12 screens]. Available from: http://online.lexi.com.ezproxy.findlay.edu:2048/lco/action/home
5. Allergan USA [Internet]. Ubrelvy (ubrogepant) [prescribing information]. Madison, NJ: Allergan USA Inc. December 2019. Available from: https://media.allergan.com/products/Ubrelvy_pi.pdf

23
Assignment #6:
The following drug information question comes from a pharmacist:
“We have seen a lot of patients coming in who are on Remodulin. What are some of the common
adverse effects of this drug and how can we help manage them as pharmacists?”
Response:
Remodulin, generic name treprostinil, is a prostacyclin analog used to treat pulmonary
arterial hypertension (PAH). The Remodulin brand can be given via intravenous or subcutaneous
infusion, while other brands have different routes of administration.
Treprostinil has several significant adverse effects. One serious adverse effect is rebound
or worsening PAH. Pharmacists and physicians can help by adjusting doses gradually, especially
in those with renal impairment. Pharmacists should also counsel patients not to stop treprostinil
abruptly and to have back-up medication ready at all times, including a spare pump, tubing, or
inhalation device. If the infusion is interrupted for more than a few hours, re-titration may be
necessary. Another serious adverse effect is the potential for bloodstream infections and sepsis.
This risk is highest with the use of an indwelling central venous catheter, so pharmacists can
recommend switching patients to a continuous subcutaneous undiluted infusion instead. If an IV
infusion must be used, an implantable pump may have a reduced risk of infections compared to
an external pump. Treprostinil can also increase patient’s bleeding risk. Pharmacists can help
manage this by decreasing the dose of drugs that affect coagulation and bleeding such as aspirin,
clopidogrel, and warfarin. They can also counsel patients on signs and symptoms of bleeding
such as bruising, black tarry stools, coughing up blood, or bleeding from the gums. Patients
should seek medical attention for any bleeding that does not stop or for any head injuries.
Infusion site pain, jaw pain, limb pain, and headache are adverse effects that may be bothersome
for patients on treprostinil, and pharmacists can recommend that patients take acetaminophen for

24
their pain. If the pain is severe and debilitating, opioid analgesics may be justifiable. Infusion site
reactions can also occur with treprostinil, and these may manifest as redness, induration, or skin
rash. Pharmacists can recommend changing the infusion site if a reaction occurs or using
antihistamines such as diphenhydramine. Severe infusion reactions may necessitate
discontinuation of treprostinil. Hypotension, flushing, vasodilatation, and syncope can occur with
treprostinil as well, especially in treatment-naïve patients. When initiating treprostinil, patients
need to be under continuous hemodynamic monitoring in an emergency department or other
qualified setting. For patients already on treprostinil, pharmacists should adjust any
antihypertensive medications and recommend that patients monitor their blood pressure daily at
home. Edema and fatigue can also be bothersome for patients, and these can be managed
through increased physical activity and diuretics, similar to a heart failure patient. Nausea,
vomiting, diarrhea, and abdominal distress can be managed by taking oral treprostinil tablets
with a meal containing at least 250 calories and 30-50% fat. Persistent nausea, vomiting or
headache may also indicate that the dose of treprostinil is too high in which case pharmacists can
recommend a dose reduction to the physician. For any restlessness and anxiety that patients
experience, pharmacists can recommend a short-term benzodiazepine or an SSRI such as
escitalopram for long-term management. With inhaled formulations of treprostinil specifically, a
cough or throat irritation may occur. Pharmacists can recommend hydration or throat lubrication
for patients in addition to reviewing proper inhaler technique. A final side effect of treprostinil is
hypokalemia. Pharmacists can recommend that patients have potassium levels drawn prior to
starting and while on treprostinil, and they can also counsel patients on signs and symptoms of
hypokalemia such as fatigue, muscle cramps, and heart palpitations which may indicate the need
for urgent medical attention.

25
There are other less common adverse effects of treprostinil that were not discussed here,
but these can be managed using many of the same techniques. Treprostinil has many significant
adverse effects, and pharmacists are qualified to help patients manage these and improve their
quality of life.
References
1. Treprostinil [package insert on the Internet]. White Oak (MD): U.S. Food and Drug
Administration; 2002 May [updated 2018 Jun; cited 2019 Dec 28]. Available from:
https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/021272s026lbl.pdf
2. Lexicomp [Internet]. Hudson (OH): Wolters Kluwer. c1978-2019. [cited 2019 Dec 30];
[about 12 screens]. Available from:
http://online.lexi.com.ezproxy.findlay.edu:2048/lco/action/home
3. Malone PM, Malone MJ, Park SK. Drug information: a guide for pharmacists. 6th
Edition. New York (NY): McGraw Hill; 30 Dec 2019.