Keep Smiling….! “ It will help you to grow up in greater happiness & Love for each other. Mother...
161
• Keep Smiling….! “ • It will help you to grow up in greater happiness & Love for each other. • Mother Teresa • Roman Catholic Missionary
-
Upload
aubrey-cole -
Category
Documents
-
view
215 -
download
0
Transcript of Keep Smiling….! “ It will help you to grow up in greater happiness & Love for each other. Mother...

• Keep Smiling….! “ • It will help you to grow up in greater
happiness & Love for each other. • Mother Teresa• Roman Catholic Missionary

Chapter 11 Blood vessels

TOPICS• Vascular wall
responses• Congenital
Anomalies• Atherosclerosis• Arteriosclerosis• Hypertension• Aneurysms
• Vasculitides• Raynaud
“phenomenon”• Veins• Lymphatics• Tumors• Interventions

• Taking blood to the tissues and back• Arteries,• Arterioles,• Capillaries,• Venules,• Veins,

• NORMAL VESSELS • Arterial walls are thicker than
veins • To accommodate pulsatile flow
and higher blood pressures.

ARTERIES – WALLS ARE THICKER DUE TO GREATER SMOOTH MUSCLE, HENCE STRONGER & CAN WITHSTAND HIGH PRESSURE

Structure of blood vessels
• Tunica intima–Endothelium and connective tissue
• Tunica media–Smooth muscle and elastic tissue
• Tunica externa or tunica adventitia–Connective, nerve fibers and vasa
vasorum
7


Arteries
• Large arteries or elastic arteries –
• Aorta and its branches, subclavian , common carotid artery, pulmonary artery
• Ileac artery
• Medium arteries are muscular arteries
• Coronary and renal arteries.
• Small arteries and arterioles are
• With in tissue and organs.

•Arterioles are the main unit in regulating the systemic arterial Blood pressure

Capillaries
• Only a single layer of endothelium and a basement membrane and no media
• Connect arterioles and venules• Exchange of diffusible substances between
blood and tissues.• Capillary network of most tissues are high and • Myocardium has highest density of capillaries.
11


Veins
• Relatively thin; less elastic• Larger in diameter than arteries• Have valves to prevent backflow of
blood• Flow to heart is assisted by
contraction of skeletal muscles..
13

• veins are more prone to dilation, compression, and easy penetration by tumors and inflammatory processes.

• Lymphatics are thin-walled, endothelium-lined channels that drain excess interstitial tissue fluid eventually returning it to blood via the thoracic duct. Lymphatic make pathway for the spread of the disease by transporting bacteria and also tumor cells to distant sites.

The main cellular components of the walls of vessels are:
1) endothelial cells 2) smooth muscle cells 3)ECM including elastin, collagen, and glucosamine glycans

1) Endothelial cells:
a)Maintenance of permeability barrier.
b)Elaboration of ,anticoagulant,antithrombotic and fibrinolytic regulators.
c)Elaboration of prothrombotic molecules.,
VWF, Tissue factor,
Plasminogen activator

• d) Regulation of inflammation and immunity
• e) Extracellular matrix production
• f)Regulation of cell growth • Growth stimulators, PDGF,FGF• Growth inhibitors,• TGF beta, heparin

The term endothelial dysfunction is defined as an altered phenotype that impairs vasoreactivity or induces a surface that is thrombbogenic or abnormally adhesive to inflammatory cells, is responsible for initiation of thrombus formation,

Endothelial activation.
The EC responds to various patho physiological stimuli by adjusting their usual functions and expressing newly acquired properties is called as Endothelial activation.

Inducers
• 1.cytokines and bacterial products• 2.advanced glycosylation of end products (involved
in pathogenesis of diabetes)• 3. viruses, • 4.complement components • 5.hypoxia• 6.Lipid products.• 7.Hemodynamic forces.

Activators
Activated endothelial cells also elaborate adhesion molecules, other cytokines and chemokines, growth factors, molecules of the major histocompatibility complex (MHC), procoagulant or anticoagulant factors and vasoactive molecules that are involved either in vasoconstriction or in vasodilatation.

• Smooth muscle cells are capable:
to mediate vasoconstriction,
to mediate vasodilatation, by
to synthesize the collagen, elastin, and proteoglycans,
to elaborate the growth factors and cytokines,
to proliferate, and to migrate to the intima.
• They play important role in normal vascular repair and atherosclerosis.

Smooth muscle cell
• Promoters• PDGF• Endothelin,• Inter ferongama• FGF and thrombin
• Inhibitors,• NO,• TGF beta• Heparn sulfate,• Angiotensin II,• Catecholamines

Diseases of arterias
• A) Congenital anomalies• B) Atherosclerosis• C) Hypertensive vascular disease• D) Inflammatory disease – Vasculitis• E) Raynaud disease• F) Aneurysms a dissections

Congenital anomalies
• AVM (Arterio Venous malformations)
• Abnormal communication between the high pressure arteries and low pressure veins.
• Usually congenital but acquired by trauma or inflammation.
• Most often described in Brain as AVM
• Asymptomatic or hemorrhage or pressure effect.

Berry aneurysm
• They are also called as saccular aneurysm• Most common intracranial aneurysms.• There is increased risk of aneurysms in
Autosomal dominant polycystic kidney disease.
• Rupture aneurysms lead to Subarchanoid hemorrhage and most common during 5th decade and in females.

Subarchanoid hemorrhage
• They present with excruciating or worst headache (They never had such headache in their life) and
• Malignant hypertension• Papilledema• And Neck stiffness.• Vomiting.

• Most common causes of Subarachanoid hemorrhage
• Berry aneurysm rupture.• Extension of traumatic hematoma• hypertensive intracranial
hemorrhage into ventricular system.

Berry aneurysm

Berry Aneurysms
• Severe headache, (Excruciating pain he never had in his life time that severe nature)
• Papilledama,• Hypertension,• Dizzeness• Sometime associated
with Polycystic kidney disease
Berry Aneurysms1.People with
polycytstic kidney,
2.Coarctation of aorta.

• Polycystic kidney


• Fibromuscular dysplasia -leads to
-renal artery stenosisCommon in females and younger age
group. pathogenesis--Fibrous or Fibromuscular
thickening of the media and intimal layers due to hyperplasia and fibrosis.

• The lesions leads to constriction or series of narrowing the middle or distal portion of the renal artery and may be bilateral involvement
• Clinical features-• Essential hypertension• Renal artery bruit in some cases• Lab-elevated level of Plasma Renin• Treatment –Good response to ACE inhibitors



Diseases of arterias
. ARTERIOSCLEROSIS(Hardening of the arteries)
It is a generic term for three patters of vascular disease that have in common thickening and loss of elasticity of arterial walls:
1) Atherosclerosis – characterized by the formation of intimal fibrous plaques that often have a central core rich in lipid (fibrofatty plaques).
.

Monckeberg medial calcific sclerosis
• 2.Monckeberg arteriosclerosis (medial calcific sclerosis) involves the media of medium sized muscular arteries, most typically
• the radial and ulnar arteries, • persons older than 50 years of age. It does not
obstruct arterial flow because the intima is not involved.

This is Monckeberg's medial calcific sclerosis, which is the most insignificant form of arteriosclerosis.
Note the purplish blue calcifications in the media; note that the lumen is unaffected by this process.
Thus, there are usually no real clinical consequences.


• a. Ring-like calcifications in the media of the arteries are characteristic.• b. Stiff, calcific "pipestem"
arteries.• Common in elderly person,

• 3.Arteriolosclerosis• Hardening of the small arteries and arteriols
espescially in the kidneys and usually associated with Hypertension /diabetes mellitus.
• Two variants are• 1.Hyaline arteriolosclerosis• 2.Hyperplastic arteriolosclerosis

Hyaline Arteriolosclerosis
• This vascular lesion consists of a homogeneous pink hyaline thickening of the walls of arterioles with loss of underlying structural detail and with narrowing of the lumen.
• Present in• Elderly patients, whether normo tensive or
hypertensive,• Patients with hypertension. • It is also common as part of the characteristic of
diabetes .(Benign nephrosclerosis)

Benign nephrosclerosis
• Sclerosis of renal arterioles and small arteries.• Vessel wall thickening with narrowing of the
lumen.• Seen mainly in • benign Hypertension and • Diabetics, and • old age individuals.

Benign nephrosclerosis

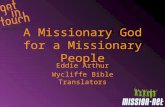
HISTOPATHOLOGY ofESSENTIAL HYPERTENSION
“HYALINE” = BENIGN HTN. “HYPERPLASTIC” = MALIGNANT HTN. SYS>200 1) ONION SKIN 2) “FIBRINOID” NECR.

Hyperplastic Arteriolosclerosis
• Malignant hypertension200/120 mm Hg (typically, diastolic pressures over 120 mm Hg associated with acute cerebral and/or renal injury).
• Hyperplastic arteriolosclerosis is associated with "onion-skin," concentric, laminated thickening of the walls of arterioles with luminal narrowing. The laminations consist of SMCs and thickened, duplicated basement membrane.

• In malignant hypertension, these hyperplastic changes are accompanied by fibrinoid deposits and vessel wall necrosis (necrotizing arteriolitis), particularly prominent in the kidney.


• Malignant hypertension. This slide is a gross specimen showing multiple hemorrhages on the surface of the kidney. This is called a flea-bitten kidney...



HYPERTENSION
• High blood pressure• Elevated blood pressure exceeding 140 over
90 mmHg -- a systolic pressure above 140 or a diastolic pressure above 90.
• Hypertensions is higher among blacks and older persons, especially older women.
•

• Silent Killer – painless – • dizziness, headache, and visual difficulties,• It is the leading risk factor – MI, Stroke and R.F• Responsible for the majority of office visits,• Complications bring to diagnosis but late…• Chronic, end organ & vascular damage

Classification
www.nhlbi.nih.gov

Isolated Systolic Hypertension
• Systolic B.P more than 160 mm Hg and diastolic pressure less than 90 mmHg is called as systolic hypertension.
• SBP should be primarily considered during treatment and not just diastolic BP.
• Systolic BP is more important cardiovascular risk factor after age 50.

• White coat hypertension• BP recording in hospital or clinic is high.• But recording the BP at home will remain
normal.• Labile HT- BP remain high at certain time of the
day and remain normal.• Malignant HT- Systolic BP higher than 200 and
diastolic remain above 110 mm of Hg associated with papilledema, headache,

• Regulation of BP:• BP = Cardiac Output x Peripheral Resistance• Endocrine Factors– Renin, Angiotensin, ANP, ADH, Aldosterone.
• Neural Factors– Sympathetic & Parasympathetic
• Blood Volume– Sodium, Mineralocorticoids, ANP
• Cardiac Factors– Heart rate & Contractility.


ReninAngiotensinAldosteroneAXIS (RAAS)
• If the perfusion of the juxtaglomerular apparatus in the kidneys decreases, then the juxtaglomerular cells release the enzyme renin.
• Renin cleaves an inactive peptide called angiotensinogen, converting it into angiotensin I.
• Angiotensin I is then converted to angiotensin II by angiotensin-converting enzyme (ACE), which is found mainly in lung capillaries.
• Angiotensin II is the major bioactive product of the renin-angiotensin system. Angiotensin II acts as an endocrine, autocrine/ paracrine, and intracrine hormone.

HYPERTENSION• “ESSENTIAL” 95%• “SECONDARY” 5%

Primary hypertension
• Also called essential or idiopathic hypertension
• 92- 95 % of all cases• No specific cause identified• Can happen with retention of sodium and
water → increased blood volume.• Also low dietary potassium, calcium and
magnesium intakes 63

GENETIC vs.ENVIRONMENTAL
• GENETIC UN-CONTROLLABLE• ENVIRONMENTAL CONTROLLABLE– STRESS– OBESITY– SMOKING– PHYSICAL ACTIVITY– NaCl INTAKE

Suspected causes
• Interaction of genetics and environment• Overactivity of sympathetic nervous system• Overactivity of renin / angiotensin/
aldosterone system• Salt and water retention by kidneys• And others
65

SECONDARY• Renal • Acute glomerulonephritis • Chronic renal disease • Polycystic disease • Renal artery stenosis • Renal artery fibromuscular dysplasia• Renal vasculitis • Renin-producing tumors
• Endocrine • Adrenocortical hyperfunction • (Cushing syndrome, primary aldosteronism, congenital adrenal hyperplasia, licorice ingestion)• Exogenous hormones (glucocorticoids, estrogen [including pregnancy-induced and oral
contraceptives], sympathomimetics and tyramine-containing foods, monoamine oxidase inhibitors)• Pheochromocytoma, Acromegaly, Hypothyroidism (myxedema), Hyperthyroidism• Pregnancy-induced
• Cardiovascular: Coarctation of aorta, Polyarteritis nodosa (or other vasculitis)• Increased intravascular volume
• MISC: Increased cardiac output, Rigidity of the aorta, Neurologic, Psychogenic, Increased intracranial pressure, Sleep apnea, Acute stress, including, surgery

GENETIC
ACQUIRED






• Normal Retina
• A: Hemorrhages• B: Exudates (Fatty Deposits)• C: Cotton Wool Spots (Micro Strokes)


ATHEROSCLEROSIS
• Etiology/Risk Factors• Pathogenesis• Morphology• Clinical Expression

ATHEROSCLEROSIS
• Atherosclerosis is characterized by intimal lesions called atheroma or atheromatous plaques, which protrude into and obstruct vascular lumen and weaken the underlying media.

Risk Factors for AtherosclerosisMajor MinorNON-modifiable
Increasing age Obesity
Male gender Physical inactivity
Family history Stress ("type A" personality)
Genetic abnormalities Postmenopausal estrogen deficiency
High carbohydrate intake
Modifiable
Hyperlipidemia Alcohol
Hypertension Lipoprotein Lp(a)
Cigarette smoking Hardened (trans)unsaturated fat intake
Diabetes Chlamydia pneumoniae

• There are a number of other less well-established risk factors for atherosclerosis, including:– High serum homocysteine levels• Homocysteine is derived from the metabolism of
dietary methionine• Homocysteine inhibits elements of the anticoagulant
cascade and is associated with endothelial damage.– Elevated serum C-reactive protein• It may increase the likelihood of thrombus formation;• Inflammation marker;

– Infectious agents• The presence of some organisms (Chlamydia
pneumoniae, herpesvirus hominis, cytomegalovirus) in atheromatous lesions has been demonstrated by immunocytochemistry, but no cause-and-effect relationship has been established. • The organisms may play a role in
atherosclerotic development by initiating and enhancing the inflammatory response

PATHOGENESIS• “atherosclerosis is a chronic inflammatory
response of the arterial wall initiated by injury to the endothelium”. Lesion progression is due to interaction between modified lipoproteins, monocyte derived macrophages, T lymphocytes and normal cellular constituents of arterial wall

Main features of the injury hypothesis:1. Chronic endothelial injury 2. Insudation of lipoproteins into the vessel wall mainly LDL with high cholestrol
content…….then oxidation of lesional lipoprotein3. Adhesion of blood monocytes & other leukocytes to the endothelium , & their
migration into the intima & their transformation into macrophages & foam cells
4. Adhesion of platelets5. Release of factors from activated platelets , macrophages or vascular
endothelial cells that cause migration of SMCs from media into the intima.6. Proliferation of SMCs in the intima , elaboration of extracellular matrix, leading
to accumulation of collagen & proteoglycans.7. Enhanced accumulation of lipids within macrophages & SMCs & extracellularly



Chronic endothelial “injury”
Atheroma
1

Chronic endothelial injury
• Hypertension• Hyperlipedemia• Homocysteine• Smoking• Viruses• Toxins• Hemodynamic factors• Immune reactions

Endothelial dysfunctionMonocyte adhesion and emigration2
Atheroma

Macrophage activationSmooth muscle recruitment3
Atheroma

Macrophages and smooth muscle cells engulf lipid
Atheroma

Accumulation of lipoproteins
• Increase in the level of LDL
• Decrease in the levels of HDL
• Increase in the Lipoprotein (a)
• Other conditions that affect the circulating lipids
• 1.Nephrotic syndrome• Hypothyroidism• Diabetes and
Alcoholism

• The mechanism of Hyperlipidemia contributing to Atherosclerosis
• Endothelial impairment by chronic hyperlipidemia by increasing O2 free radicals production
• Deactivates Nitric oxide• Impair vaso dilation• Impair endothelial function Oxidize the LDL

• Intimal SMC proliferation and ECM deposits convert a fatty streak into atheroma

Oxidative modification of LDL
• 1.Is important in atherogenic process.• 2.Oxidized LDL is toxic to endothelial cells,• 3.Responsible for endothelial injury• 4.It is chemo tactic to monocytes and
immobilizes the macrophges favoring their accumulation at the site.
• 5.It is taken up by macrophages and smooth muscle cells(Through scavenger pathway)

•Fatty streak is the earliest lesion in Atherosclerosis.

1. Fatty dots• not raised , so do not cause obstruction to the flow• Multiple, yellow , flat spots < than 1mm in diameter • composed of lipid laden foam cells
2. Fatty streaks =coalesce of multiple fatty dots• Elongated, 1 cms longer or more • contain T- lymphocytes & extracellular lipid < than plaques• Appear in aorta in some children younger than 1 year & all
children older than 10years ,
3. Fatty streaks may be precursor of plaque but not all fatty streaks are converted into fibrous plaque or more advanced lesions

The white arrow denotes the most prominent fatty streak in the photo, but there are other fatty streaks scattered over the aortic surface. Fatty streaks are the earliest lesions seen with atherosclerosis in arteries.

Fatty streaks

Common sites:
1. Abdominal aorta compared to thorasic aorta & lesions are more common around the ostia of major branches
2. Other common arteries in descending order after aorta is coronaries, popliteal, internal carotid & cicle of Willis
3. Vessels of the upper extremities are usually spared 4. Mesenteric & renal arteries are also spared but
ostias can be involve

COMPONENTS OF ATHEROMATOUS PLAQUE (MP)
1. *Superficial fibrous cap is composed of SMCs & relatively dense collagen
2. *cellular zone containing, SMCs , macrophages, Lymphocytes (T cells)
*Foam cells : are monocytes derived from blood & SMCs can also become foam cells
3. *Deep to the fibrous cap is central necrotic core , containing a disorganized mass of lipids( cholestrol& cholestrol esters) cholestrol clefts, debris from dead cells , foam cells, fibrin

3. *Below & to the sides of cap ( shoulder) is a cellular area consisting of macrophages, SMCs, T lymphocytes
4. At the periphery area of neovascularization is present
Generally plaque undergo remodelling ( degeneration , synthesis of ECM & organization of thrombus.

PLAQUE

American heart association classified ATH into six types or stages
• Type I – Fatty dots - Foam cells• Type II – Fatty streak• Type III – Intermediate stage (Extracellular lipid pool)• Type IV – Atheroma – Core of lipid• Type V – Fibroatheroma – Fibrotic layer• Type VI – Complicated lesion ( Ulcer, Ca+
Hemorrhage, thrombus, embolism, aneurysm).

Atheroma Aorta:

Atheroma Aorta:

Atheroma Coronary Artery:
Calcification

COMPLICATIONS & clinical significance
A) Advanced lesions of atheromas are vulnerable to following pathological changes:

Complications
• MI,• Rupture or ulceration• Erosion or thrombus formation• Aneurysms• Arrhythmias• Cerebral infarct• Renal infarct, Atheroembolism• And Death

1. Thrombosis & calcification 2. Emboli formation , cholestrol emboli or
atheroemboli which are discharged into blood stream.
3. Rupture, ulceration, erosions.4. Hemorrhage: due to rupture of fibrin cap or thin
walled capillaries that vascularize the plaque & contained hematoma expand & rupture the plaque
5. Aneurysmal dilatation: Fusiform, dissecting, or berry etc., due to pressure or ischemic atrophy of media with loss of elastic tissue causing weakness & rupture.

This is severe atherosclerosis of the aorta in which the atheromatous plaques have undergone ulceration along with formation of overlying mural thrombus.

A coronary thrombosis is seen microscopically occluding the remaining small lumen of this coronary artery.
Such an acute coronary thrombosis is often the antecedent to acute myocardial infarction.

The aorta shows a large atheroma. Cholesterol clefts are numerous in this atheroma. The surface shows ulceration and hemorrhage.

Prevention
• Three factors need improvement 1. life style, cigarette smoking2.Reduced consumption of cholestrol &
saturated animal fat & control of hypertension
3. Prevention of recurrences in those who have previously suffered from serious ATH related clinical events


PLAQUE DEPOSITORIGINAL DIAMETER

Mild fibrous plaques

Aneurysm
• An aneurysm is a localized abnormal dilation of a blood vessel or the heart.• There are two types of aneurysm.• 1.Trueaneurysm• 2.False aneurysm

• True Aneurysm• When an aneurysm
involves all three layers of the arterial wall (intima, media, and adventitia) or the attenuated wall of the heart.

False aneurysm
• (pseudoaneurysm) is a breach in the vascular wall leading to an extravascular hematoma that freely communicates with the intravascular space ("pulsating hematoma").

• True Aneurysms
• Atherosclerotic.• Syphilitic• Congenital• Ventricular aneurismal
follow a MI
• False aneurysms• 1.Post myocardial
infarction rupture• 2.Leak at the junction
(anastomosis) of vascular graft with natural artery.

• Fusiform– Spindle-shaped
involving whole circumference
• can involve extensive portions of the aortic arch, abdominal aorta, or even the iliacs
• Saccular– Small segment of
wall ballooning due to localized weakness– they vary from 5
to 20 cm in diameter and often contain thrombi.


• Fusi form • Saccular form

Risk factors
–Smoking, –Hypertension,
Hypercholesterolaemia

•Most common causes of aneurysm
•Atherosclerosis•Hypertension

Rare causes of aneurysms
• Congenital– Marfan’s syndrome, Berry aneurysms
• Post-stenotic– Coarctation of the aorta, Cervical rib, Popliteal
artery entrapment syndrome• Traumatic– Gunshot, stab wounds, arterial punctures
• Inflammatory– Takayaso’s disease, Behcet’s disease

Rare causes of aneurysms
• Mycotic– Bacterial endocarditis, syphilis
• Pregnancy associated– Splenic, cerebral, aortic, renal, iliac & coronary

Aortic Aneurysms
• Laplace’s LawTension varies directly with radius when pressure is
constant
T = P x R
T - TensionP - PressureR - Radius

Aortic Aneurysms
• Decrease in elastin and collagen in arterial wall
• Elastin becomes fragmented-->arterial elongation and dilatation
• Increase in the collagenase and elastase activity.


• Pathogenesis • 1.The intrinsic quality of the vascular wall
connective tissue is poor• Eg. Marfan syndrome• Loeys Deitz syndrome• Ehlers Danlos syndrome

• 2.The balance of collagen synthesis and degradation is altered by inflammatory. Infiltration and destructive proteolytic enzymes.
• Increased production of MMP by macrophages in atherosclerosis or vasculitis
• Also decreased in tissue MMP inhibitors

• 3.The vascular wall weakened through loss of smooth muscle cells.
• Hypoxia due to athermanous plaque and leads to ischemia and HT in turn leads to smooth muscle loss and scarring and decreased synthesis of ECM and increased amount of gycosaminoglycons called as cystic medial degeneration seen in Marfan syndrome and scurvy.

Most abdominal aortic aneurysms (AAA) occur between the renal arteries and the bifurcation of the aorta

Abdominal Aortic Aneurysm
• Atherosclerosis, the most common cause of aneurysms, causes thinning and weakening of the media secondary to inti.mal plaques
• Site-. Atherosclerotic aneurysms occur most frequently in the abdominal aorta (abdominal aortic aneurysm, often abbreviated AAA), but the, Associated with iliac aneurysms in 30%
• Associated with popliteal aneurysms in 10%
• can also be involved

Pathogenesis AAA
• More frequently in men and rarely develops before age 50.Male to female (4:1)
• since the incidence is less than 5% in men older than 60 years,

• Two AAA variants• Inflammatory AAAs are characterized by
dense periaortic fibrosis containing abundant lympho plasmacytic infiltrate with many macrophages and often giant cells. Their cause is uncertain.

• Mycotic AAAs are atherosclerotic lesions infected by lodging of circulating microorganisms in the wall, particularly in the setting of bacteremia from a primary Salmonella gastroenteritis. In such cases, suppuration further destroys the media, potentiating rapid dilation and rupture.

Clinical features of AAA
• Asymptomatic in 75%– Incidentally discovered during clinical exam.or
radiographic investigation • Pain– Central abdominal radiating to the back – Chronic due to stretching the vessel wall or
compression/erosion of surrounding structures– Acute pain due to rupture

Clinical features of AAA
• Asymptomatic in 75%– Incidentally discovered during clinical exam.or
radiographic investigation • Pain– Central abdominal radiating to the back – Chronic due to stretching the vessel wall or
compression/erosion of surrounding structures– Acute pain due to rupture

• Clinical features• The clinical features depend on the
consequences of the AAA• Rupture into peritoneal cavity leads to fatal
hemorrhage• Obstruction into the branch leads to ischemic
injury• Embolism

• Compression of the adjacent structures like ureter or vertebral erosion
The risk of rupture depends upon the sizes a abdominal mass.

• 1.0 to 1%/year if aneurysm size is less than 4 cm in diameter.
• 2.11% /year if aneurysm is 5 to 5.9 cm in diameter.
• 3.25%/year if aneurysm is more than 6 cm.• Most aneurysm expand 0.2 to 0.3 c,/year .

Complications
• 1.Rupture into the peritoneal cavity or retroperitoneal tissues with massive hemorrhage.
• 2.Obstruction of the vessel(Mainly iliac, renal, mesentric)
• 3.Embolism from the atheroma• 4.Pressure effect on adjacent structure (ureter
or erosion of the vertebra)• 5.present as a abdominal mass.

Syphilitic ( luetic) aneurysm
• . This aneurysm is a manifestation of tertiary syphilis, which has become rare with better
• treatment and control of the disease. It is caused by syphilitic aortitis, which is characterized
• by obliterative endarteritis of the vasa vasorum and necrosis of the media.
• Grossly, these changes result in a "tree-bark" appearance


• The narrowing of the lumina of the vasa vasorum causes ischemic injury of the aortic media, with patchy loss of the medial elastic fibers and muscle cells, followed by inflammation and scarring, the aorta loses its elastic recoil producing an aneurysm. Contraction of fibrous scars may lead to wrinkling of intervening segments of aortic intima, grossly reminiscent of "tree bark."

• Unlike atherosclerotic aneurysms, syphilitic aneurysms characteristically involve the
• ascending aorta. Dilation of the ascending aorta may widen the aortic commissures,
• leading to aortic valve insufficiency

FTA –ABS test
• FTA –ABS test reads Syphilis infection,
• Important to remember in a patient with Aortic aneurysm mainly thoracic or ascending aorta involved in Syphilitic aortitis

THORACIC ANEURYSMS–Hypertnesion is common cause –Marfan syndrome and loeys Dietz syndrome–Encroachment–Respiratory difficulties–Dysphagia–Cough–Pain–Aortic valve dilatation–Rupture

DISSECTION

Aortic Dissection
• Blood splays apart the laminar planes of the media to form a blood-filled channel within the aortic wall this channel often ruptures through the adventitia and into various spaces, where it causes either massive hemorrhage or cardiac tamponade


• (1) men aged 40 to 60 years, with antecedent hypertension (more than 90% of cases of dissection), and
• (2) younger patients with systemic or localized abnormalities of connective tissue affecting the aorta.
• 3.Iatrogenic following catheterization or bypass surgery.
• 4.During and after pregnancy.

• Hypertension is the major risk factor.• There is medial hypertrophy of the vasa
vasorum.• Degenerative changes in the aortic media• Loss of smooth muscle cells• The medial weakness trigger the intimal tear.• There is cystic medial degeneration.

Level of the aorta affected
• The more common (and dangerous) proximal lesions (called type A dissections), involving either the ascending aorta only or both the ascending and descending aorta.
• Distal lesions not involving the ascending part and usually beginning distal to the subclavian artery Type B.


. Stanford classification
• type A - A affects ascending aorta and arch– accounts for ~60% of aortic dissections– surgical management–may result in:–Aortic incompetence• coronary artery occlusion• rupture into pericardial sac with resulting
cardiac tamponade

• TYPE B - begins beyond brachiocephalic vessels– accounts for ~ 40% of aortic dissections–dissection commences distal to the left sub-
clavian artery–medical management with blood pressure
control.


CLINICAL FEATURES
• The classic clinical symptoms of aortic dissection are the sudden onset of excruciating pain, usually beginning in the anterior chest, radiating to the back between the scapulae, and moving downward as the dissection progresses; the pain can be confused with that of myocardial infarction.

• The most common cause of death is rupture of the dissection into body cavities (i.e., pericardial, pleural, or peritoneal). Retrograde dissection into the aortic root can cause disruption of the aortic valvular apparatus. cardiac tamponade,
• aortic insufficiency,• myocardial infarction

• Extension of the dissection into the great arteries of the neck or
• Into the coronary,• Renal, • Mesenteric, or• Iliac arteries




![Mansfield Ukulele Group When You’re Smiling Fisher ......Mansfield Ukulele Group When You’re Smiling –Fisher, Goodwin and Shay When you're [G] smiling, when you're smiling The](https://static.fdocuments.in/doc/165x107/60e04689944378331c32ff9f/mansfield-ukulele-group-when-youare-smiling-fisher-mansfield-ukulele-group.jpg)