Kanika Bagai, MD, MS Assistant Professor Department … · Kanika Bagai, MD, MS . Assistant...
75
Kanika Bagai, MD, MS Assistant Professor Department of Neurology Vanderbilt University Medical Center Nashville, TN
Transcript of Kanika Bagai, MD, MS Assistant Professor Department … · Kanika Bagai, MD, MS . Assistant...

Kanika Bagai, MD, MS Assistant Professor Department of Neurology Vanderbilt University Medical Center Nashville, TN
I have no financial disclosures for this talk.
Discuss the interrelationship of sleep apnea and stroke. Emphasize the importance of recognizing and
treating sleep apnea in patients with stroke/TIA. Treatment options for sleep apnea
75 year old man with chief complaints of : loud snoring witnessed apneas frequent nocturnal awakenings daytime sleepiness in sedentary situations.
Past Medical History HTN Pontine stroke on MRI Glucose intolerance with FBS up to 131 Paroxysmal atrial fibrillation CAD, s/p CABG in 1992,s/p stent placement to RCA Echocardiogram: nml wall motion, dilated LA/LV, EF > 55% Examination BMI = 31.5, Friedman palate position of 4
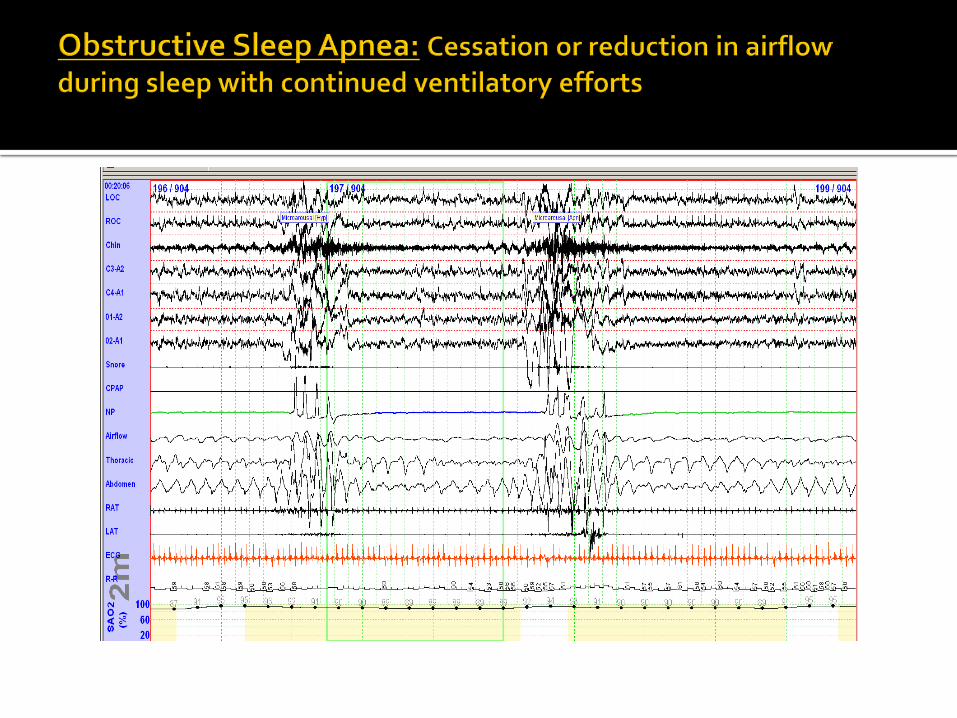
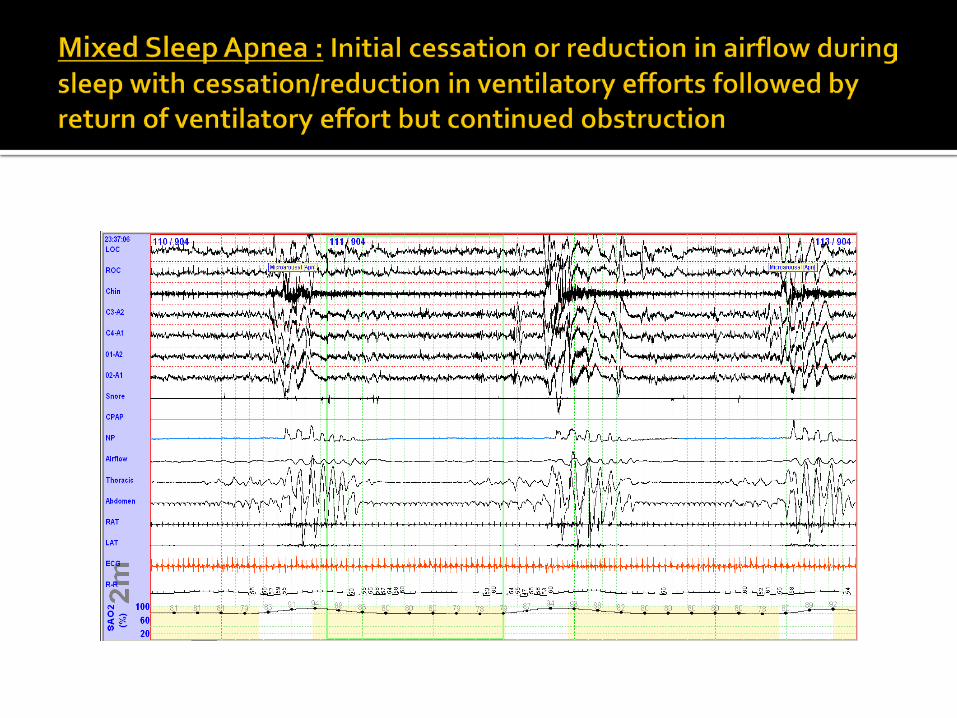
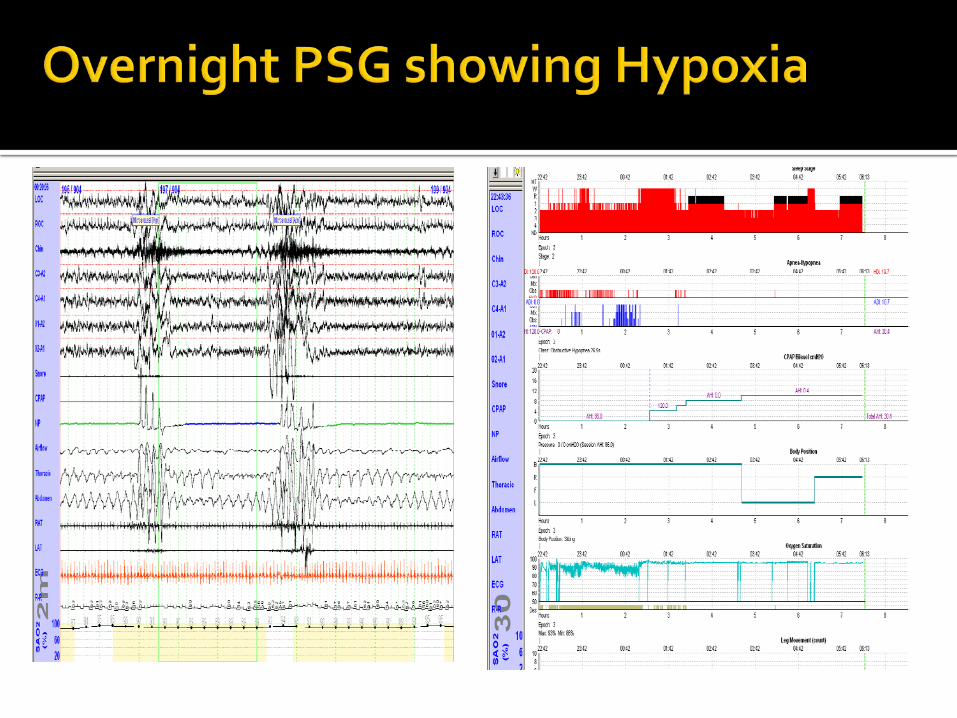
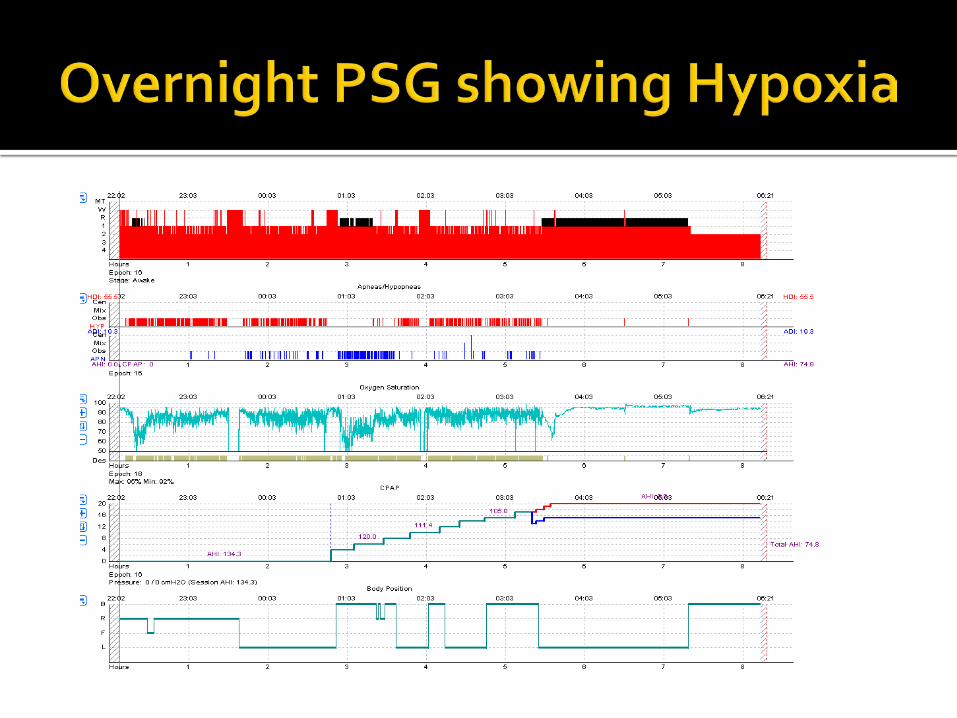
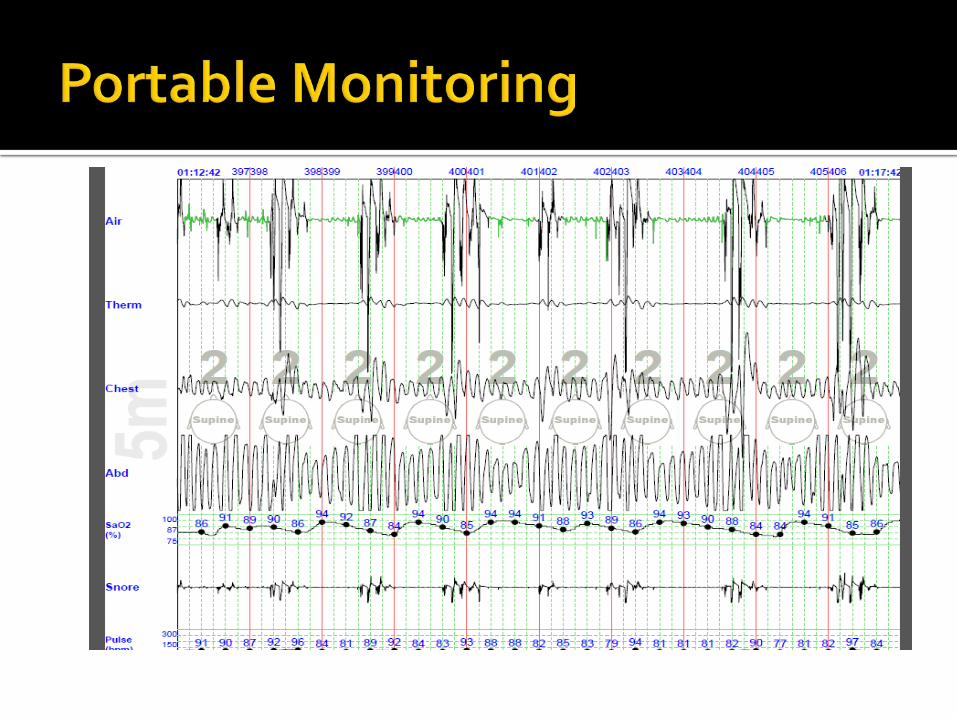
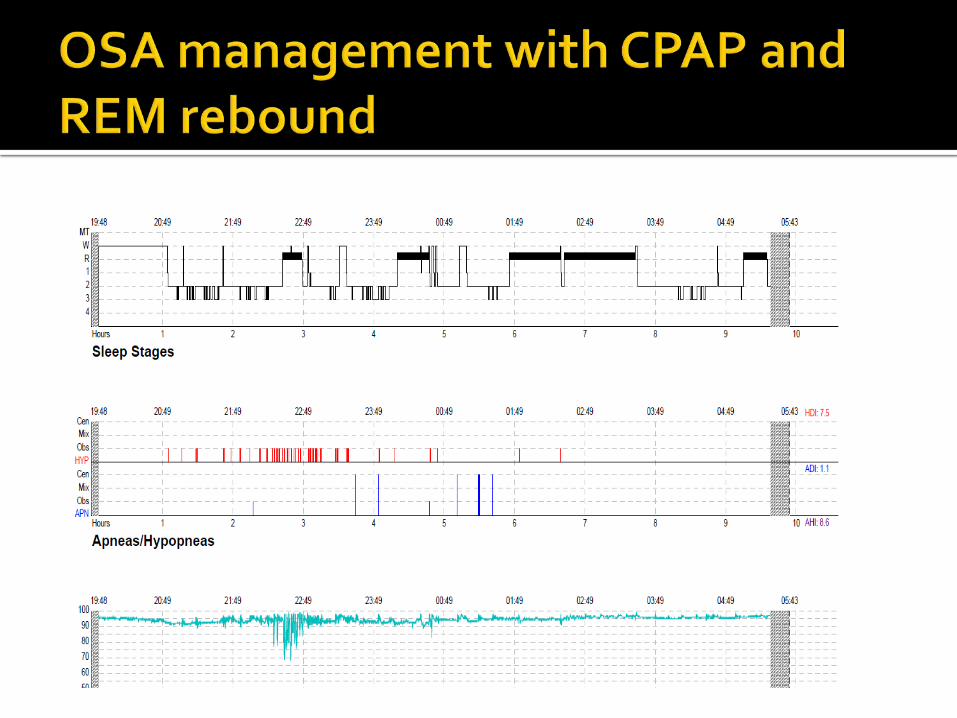
Apneas- >90% decrement in the thermistor, for at
least 10 seconds.
Hypopneas- 30-90% decrement in the nasal pressure transducer for at least 10 seconds, with concurrent oxyhemoglobin desaturation of 3% or greater or an EEG arousal, as defined by the American Sleep Disorders Association arousal criteria .
Presenter
Presentation Notes
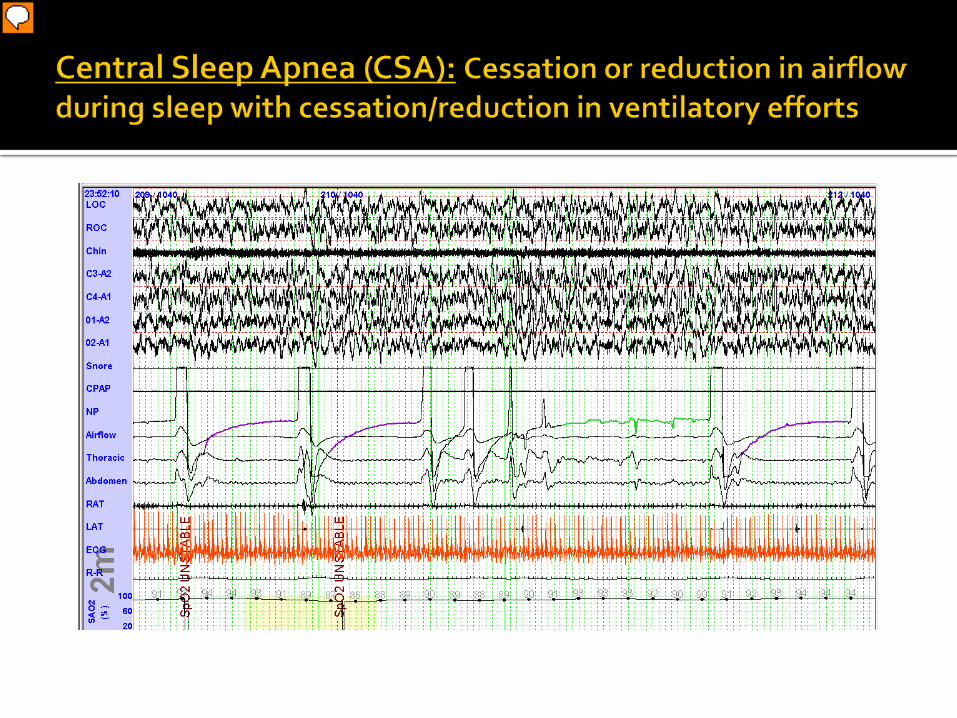
Etiology of CSR-CSA is believed to be secondary to increased sensitivity of chemoreceptors, with resulting hyperventilation. Increased circulation time plays a role in modeling cycle length.
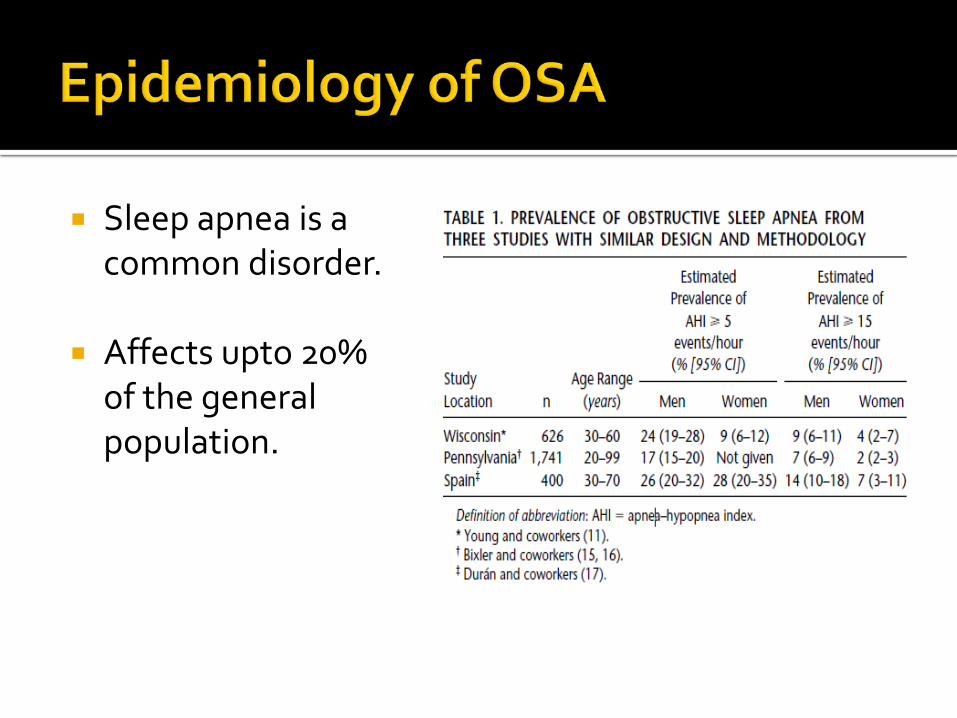
Sleep apnea is a common disorder.
Affects upto 20% of the general population.
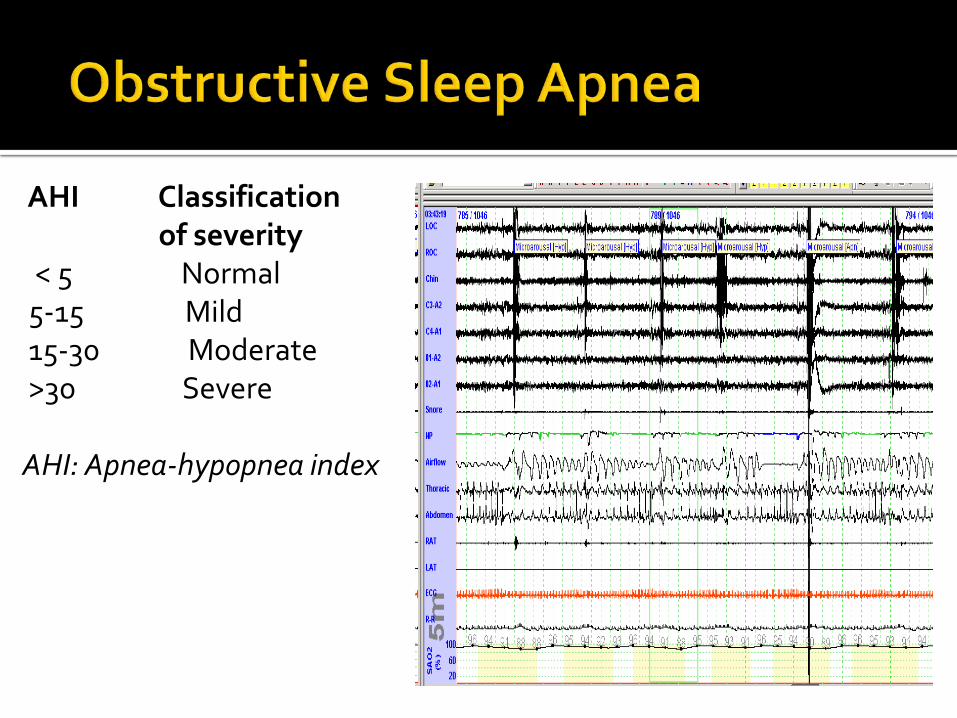
AHI Classification of severity
< 5 Normal 5-15 Mild 15-30 Moderate >30 Severe AHI: Apnea-hypopnea index
Date of download: 10/16/2013 Copyright © 2012 American Medical Association. All rights reserved.
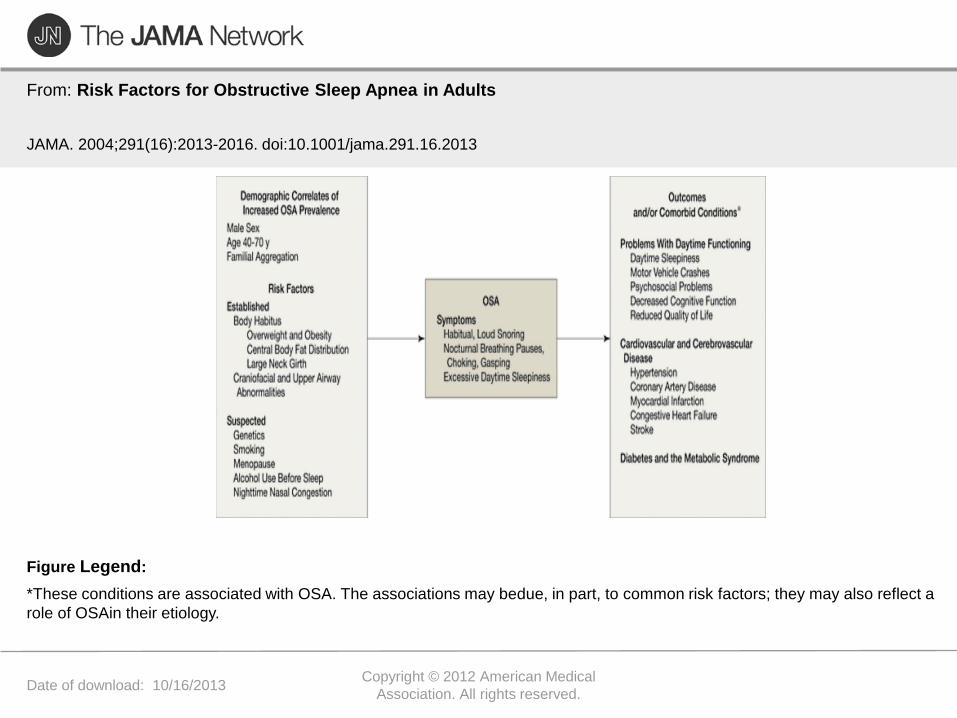
From: Risk Factors for Obstructive Sleep Apnea in Adults
JAMA. 2004;291(16):2013-2016. doi:10.1001/jama.291.16.2013
*These conditions are associated with OSA. The associations may bedue, in part, to common risk factors; they may also reflect a role of OSAin their etiology.
Figure Legend:
The prevalence of sleep apnea is high is stroke patients-estimated to be between 50-70%.
It may predate the stroke, worsen during the acute stage, and persist after the acute phase.
1991: Retrospective study1 found that 72% of patients with stroke (n = 47) had AHIs ≥10
1996: Prospective study2 on 24 consecutive patients admitted with recent stroke (mostly ischemic) found AHIs ≥ 10 in: 77% of men and 64% of women with strokes 23% of men and 14% of women
(age and gender-matched controls)
1 Kapen et al, 1991, Neurology 41 (suppl 1):125 2 Mohensin and Valor, 1995, Arch Phys Med Rehabil 1995;76:71-76
1996: Comparison of sleep apnea in three groups1
Acute Stroke (n = 48) TIA (n = 32) Age/gender-matched controls (n = 25) Stroke and TIA did not significantly differ in AHI.
This result suggested that sleep apnea is a cause of
stroke, rather than its consequence 1 Bassetti et al, 1996; Neurology, 27:401-407
AHI = 32 (0-140)
AHI = 23 (0-81)
AHI = 5 (0-24)
Presenter
Presentation Notes
Independent predictors of AHI included: Age Diabetes Obesity Severity of Stroke
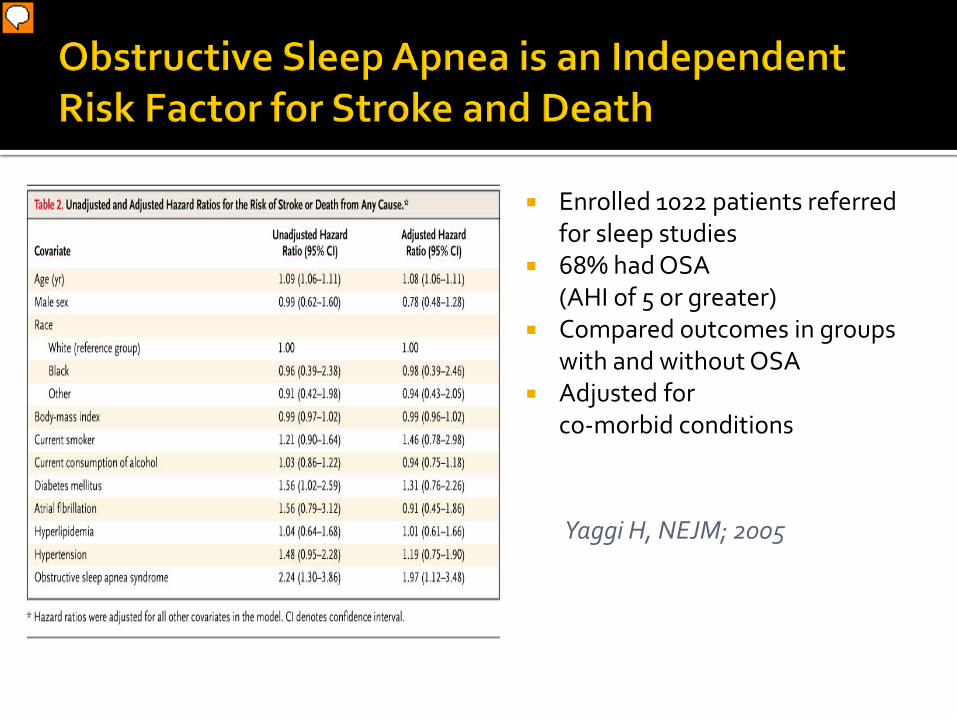
Enrolled 1022 patients referred for sleep studies
68% had OSA (AHI of 5 or greater)
Compared outcomes in groups with and without OSA
Adjusted for co-morbid conditions
Yaggi H, NEJM; 2005
Presenter
Presentation Notes
Prevalence of OSA amongst 1022 patients referred for sleep studies was 68%. HR for death or stroke in OSA patients, adjusted for co-morbid conditions (age, sex, race, BMI, smoking, alcohol, DM, HTN, atrial fibrillation) was 1.97 (1.12-3.48, p=0.01) A stepwise increase in risk of death or stroke with increasing AHI was noted. Hazard ratios 1.75, 1.74, and 3.30 respectively for AHI 4-12, 13-36, and > 36 events/hour (p=0.005 for linear trend).
Am J Respir Crit Care Med Vol 182. pp 269–277, 2010
Presenter
Presentation Notes
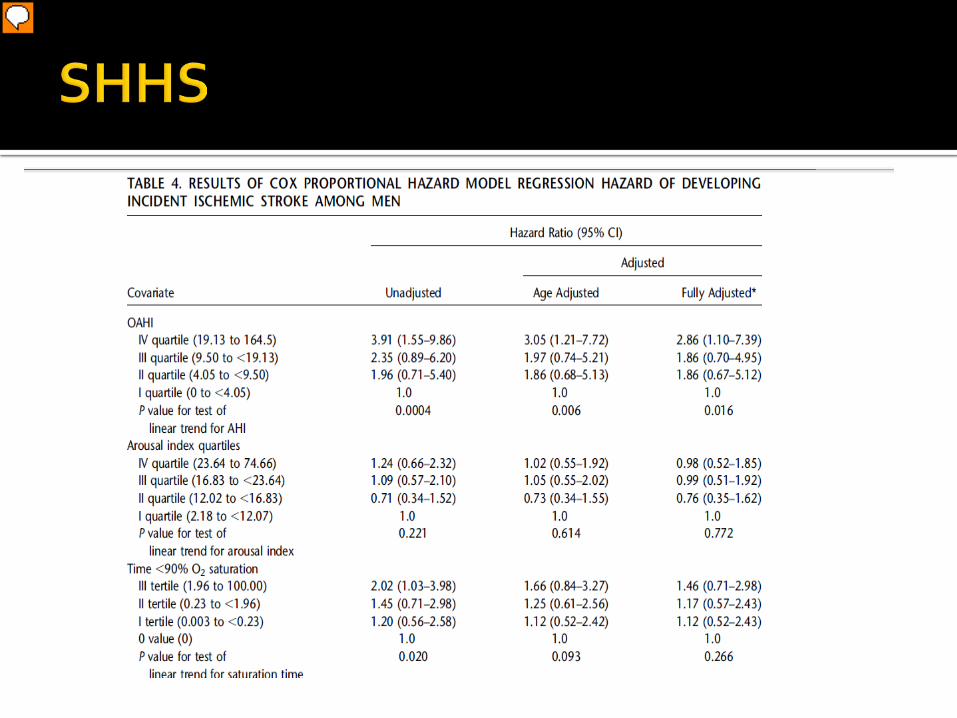
Addresses whether sleep apnea is associated with an increased risk of ischemic stroke in men and women recruited from the community. 8 years of prospective data from a large, geographically diverse community-based cohort of middle-aged and older adults, that modest to severe levels Sleep apnea are associated with an approximately threefold increase risk of ischemic stroke in men
Presenter
Presentation Notes
Adjusted for age, BMI, smoking status, Systolic BP, use of anti-hypertensive medications, DM, race
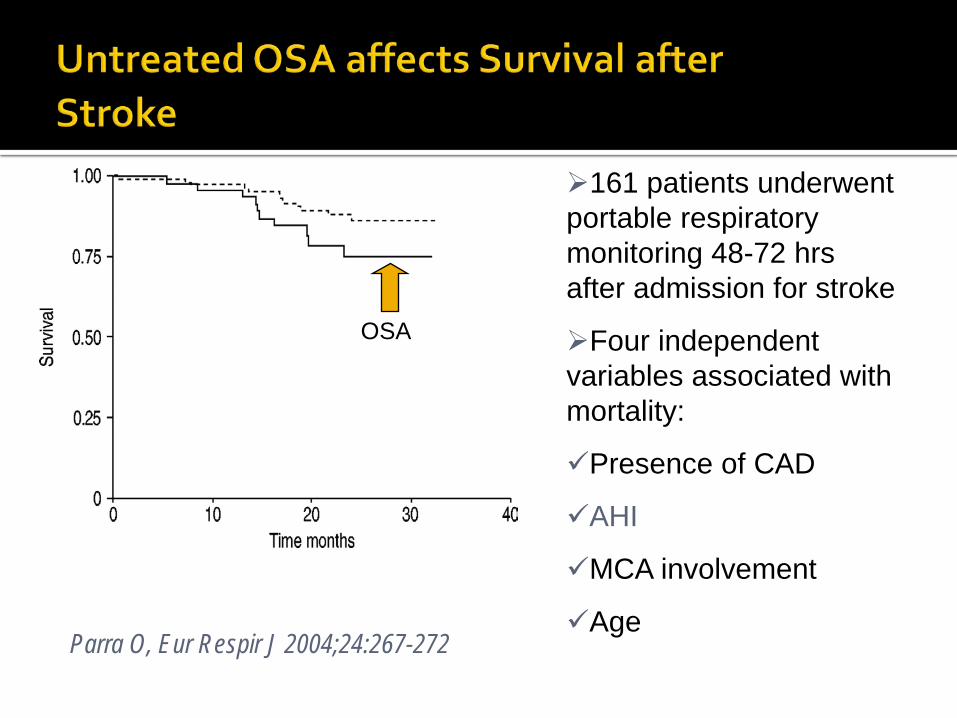
Parra O, Eur Respir J 2004;24:267-272
161 patients underwent portable respiratory monitoring 48-72 hrs after admission for stroke
Four independent variables associated with mortality:
Presence of CAD
AHI
MCA involvement
Age
OSA
Sleep apnea Drug-induced or drug-related
Chronic kidney disease Primary aldosteronism Renovascular disease
Chronic steroid therapy and Cushing syndrome
Pheochromocytoma Coarctation of the aorta
Thyroid or parathyroid disease Chobanian A, JAMA, 2003:The Seventh Report of the Joint National Committee on
Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 Report
Small (5 mm Hg) improvements in mean blood pressure seen in
normotensive cohort, driven by those with more frequent oxyhemoglobin desaturation episodes.
Pepperell J, Lancet, 2002 Larger reductions in mean blood pressure (9.9 ± 11.4 mm Hg)
were seen in those with severe OSA treated for 60 days . Becker H, Circulation, 2003
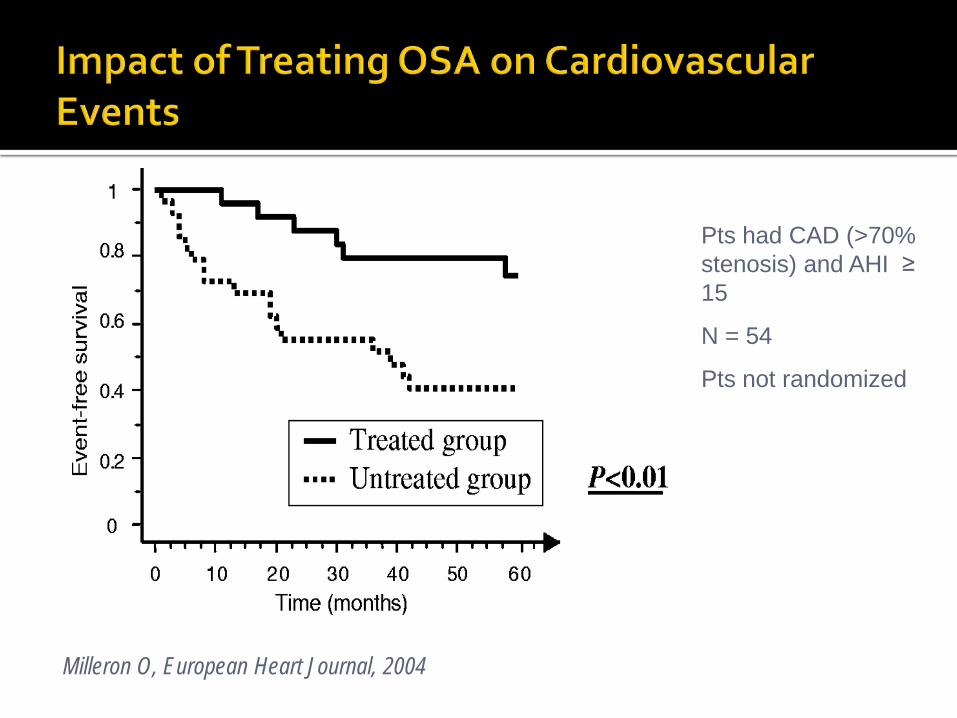
Milleron O, European Heart Journal, 2004
Pts had CAD (>70% stenosis) and AHI ≥ 15
N = 54
Pts not randomized
The entire spectrum of arrhythmias is increased in sleep apnea.
About half of patients undergoing elective cardioversion for atrial fibrillation had significant sleep disordered breathing
Gami A, Circulation, 2004
Patients with both atrial fibrillation and sleep disordered breathing are more likely to remain in sinus rhythm after cardioversion if treated with CPAP.
Kanagala R, Circulation, 2003
Presenter
Presentation Notes
New slide
AHI and minimum oxygen saturation are independent determinants of insulin resistance, even after controlling for obesity
Ip, Am J Respir Crit Care Med, 2002 CPAP improves insulin sensitivity in patients with OSA and Type 2 DM Harsch I, Respiration, 2004
Sympathetic nervous system overactivity and RAAS.
Impaired glucose tolerance, increased insulin resistance.
Endothelial dysfunction Blood coagulation abnormalities, such as
elevated PAI-1. Altered systemic inflammatory markers that
promote atherosclerosis, such as C-reactive protein and tumor necrosis factor
Oxidative stress.
Presenter
Presentation Notes
New slide
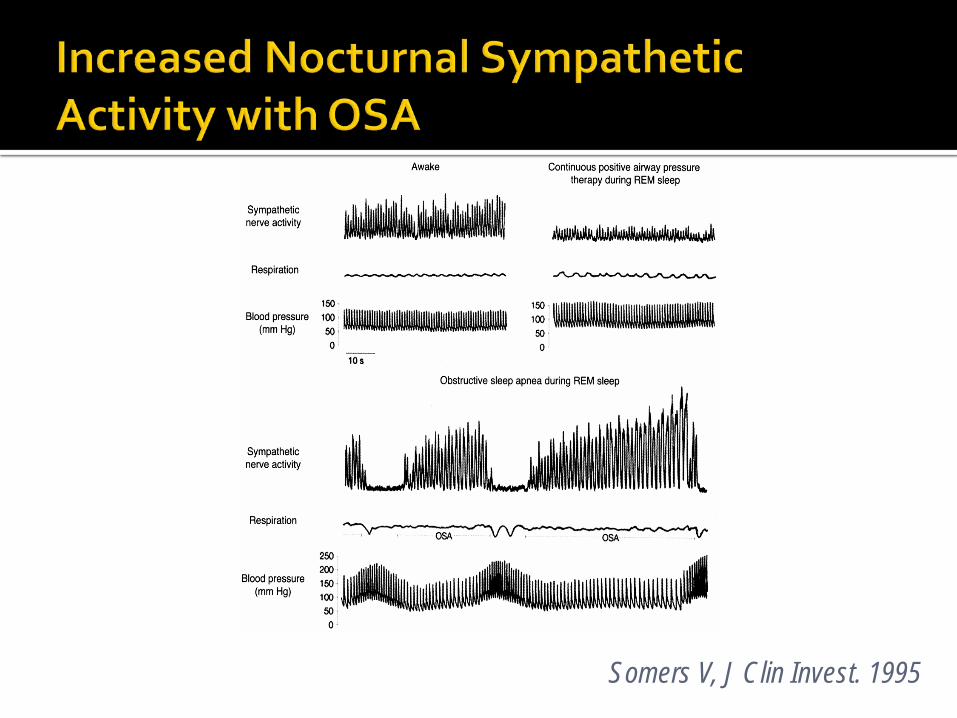
Somers V, J Clin Invest. 1995
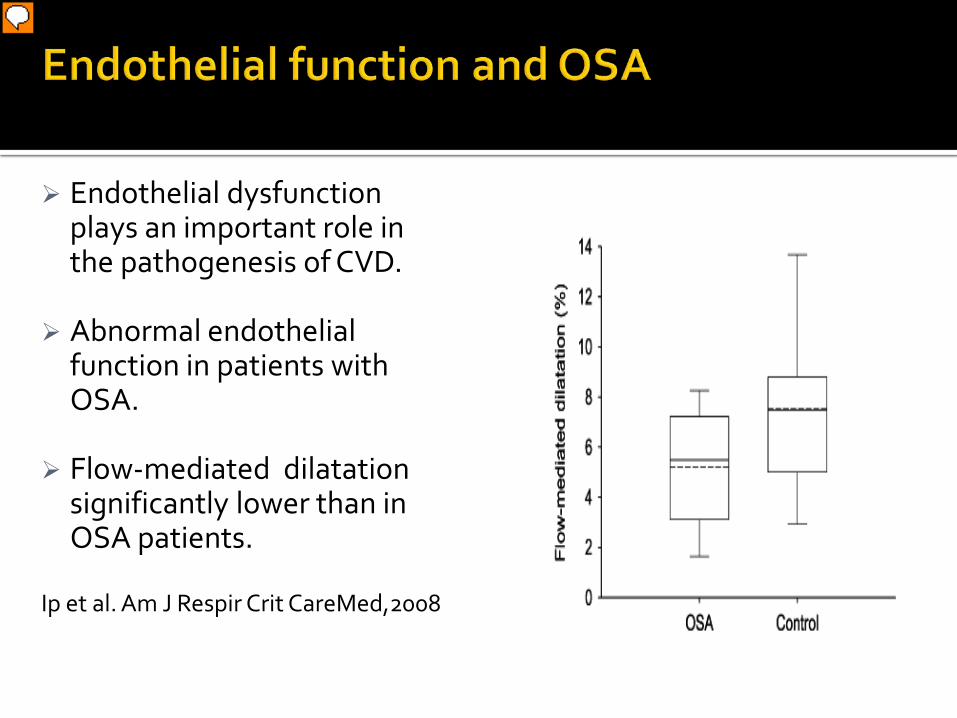
Endothelial dysfunction plays an important role in the pathogenesis of CVD.
Abnormal endothelial function in patients with OSA.
Flow-mediated dilatation significantly lower than in OSA patients.
Ip et al. Am J Respir Crit CareMed,2008
Presenter
Presentation Notes
FMD- Is an endothelium dependent function measured in the brachial artery. The stimulus provokes release of No with subsequent dilation which can be imaged and quantitated as an index of vasomotor function. Non-invasive and allows repeated measures.
Endothelium-derived nitric oxide (NO) NO is a major mediator of endothelium-dependent
vasodilatation.
Anti-inflammatory and antithrombotic properties.
Lower levels of NO in patients with OSA and an increase in levels following treatment with CPAP.
Lavie L, J Mol Neurosci 2003
Reactive oxygen species (ROS) Intermittent hypoxia in OSA patients may alter
endothelial function by promoting the formation of reactive oxygen species.
Inflict injury to surrounding tissues.
Activate signaling pathways that can initiate adaptive responses to hypoxia, such as hypoxia inducible factor-1alpha (HIF-1 alpha) or inflammatory pathways via NFkB.
Presenter
Presentation Notes
Hypoxia induces endothelial cell IL-1, IL-6, and IL-8 synthesis, similar to cytokine induction seen in sepsis.53 There is also evidence to support activation of inflammatory transcriptional factors such as nuclear factor-kB (NF-kB) and HIF-1 in conditions with hypoxia as seen in OSA.
TNF-a: Serum TNF-a is the downstream product of activation of the NF-kB pathway
TNF-a levels are reported to be elevated in OSA and fall with CPAP.
Ryan S. Circulation. 2005;112:2660–2667.
CRP: CRP is a marker of inflammation and a strong predictor of future CVD.
In patients with OSA, CRP levels are reported to be elevated and decrease with CPAP treatment.
Yokoe et al,Circulation. 2003
Majority of strokes and MIs are due to atherothrombotic events, with impaired fibrinolytic activity increasing the propensity for these events.
Plasminogen Activator Inhibitor-1 (PAI-1) is the major physiologic inhibitor of the body’s fibrinolytic system.
PAI-1 is released from platelets and endothelial cells in response to thrombin.
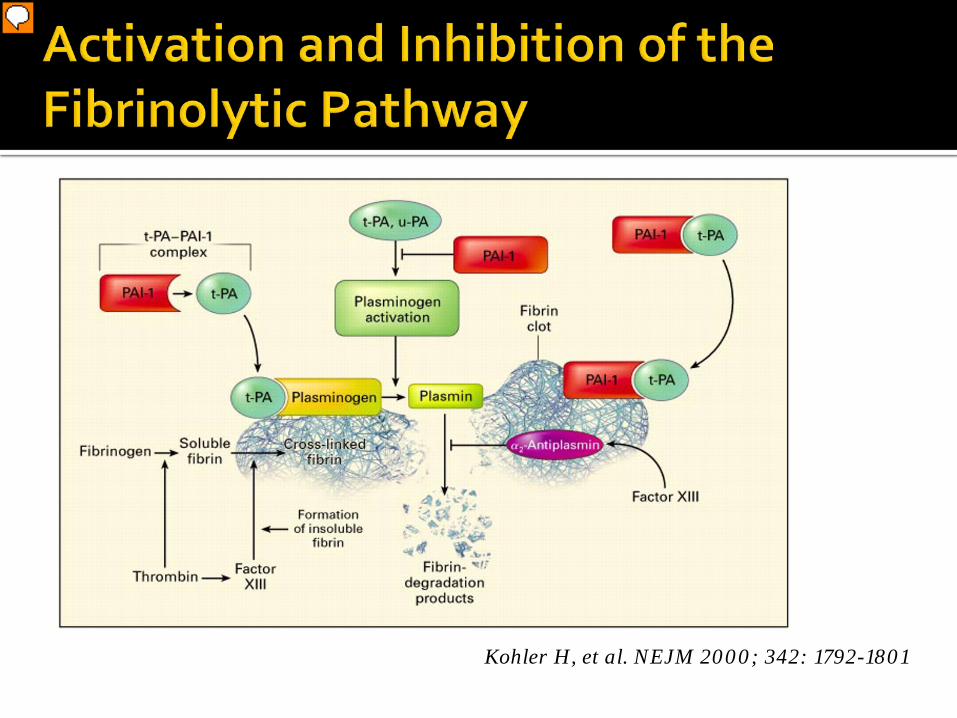
Kohler H, et al. NEJM 2000; 342: 1792-1801
Presenter
Presentation Notes
Figure 2. Activation and Inhibition of the Fibrinolytic Pathway. Tissue plasminogen activator (t-PA) circulates in plasma as a complex with plasminogen-activator inhibitor type 1 (PAI-1) in a 1:1 ratio. PAI-1 binds to fibrin, within a clot and inhibits t-PA, thereby increasing the clot’s resistance to lysis. The fibrin clot also provides the surface on which other reactions occur. Plasminogen is activated by t-PA or urinary-type plasminogen activator (u-PA). Plasminogen, t-PA, and fibrin form a ternary complex that promotes the formation of plasmin and the subsequent lysis of cross-linked fibrin into low-molecular-weight fragments (fibrin-degradation products). PAI-1 also binds to fibrin and, when bound, retains its inhibitory activity against t-PA. {alpha}2-Antiplasmin is cross-linked to fibrin by factor XIII.
PAI-1 expression has been observed in atherosclerotic
plaques in humans and may contribute to the progression of vascular disease.
PAI-1 levels are elevated in patients with cardiovascular events such as myocardial infarction (MI) and stroke
Elevated PAI-1 appears to be a risk factor for recurrent MI.
Extent of PAI-1 elevation independently correlates with mortality in acute MI.
PAI-1 and CVD
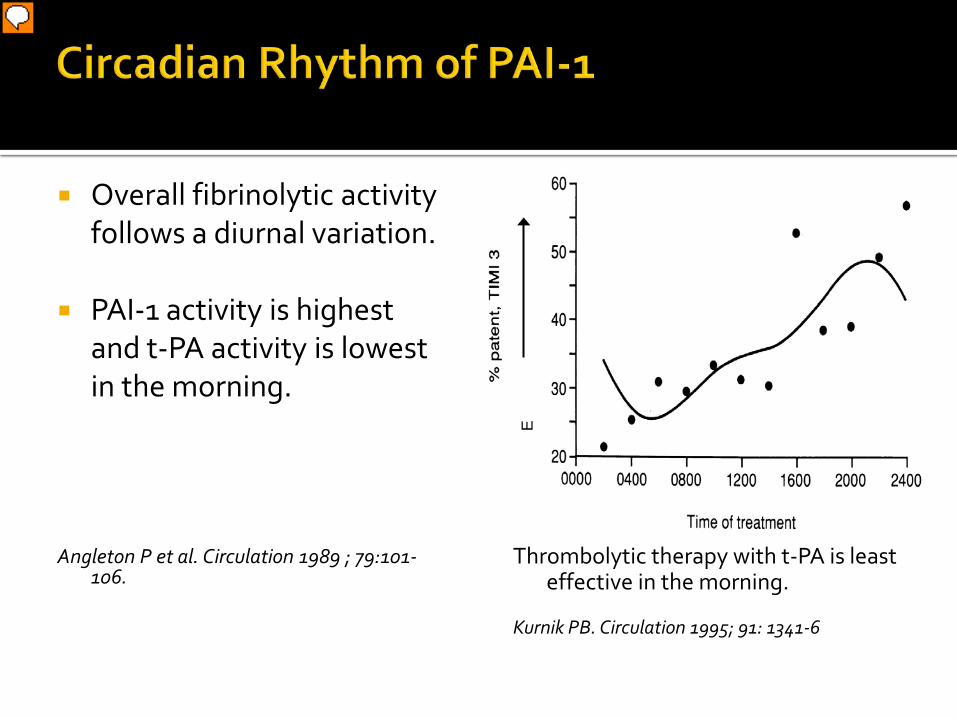
Overall fibrinolytic activity follows a diurnal variation.
PAI-1 activity is highest and t-PA activity is lowest in the morning.
Angleton P et al. Circulation 1989 ; 79:101-
106.
Thrombolytic therapy with t-PA is least effective in the morning.
Kurnik PB. Circulation 1995; 91: 1341-6
E
Presenter
Presentation Notes
There is a well recognized circadian variation in PAI-1 levels, which results in a
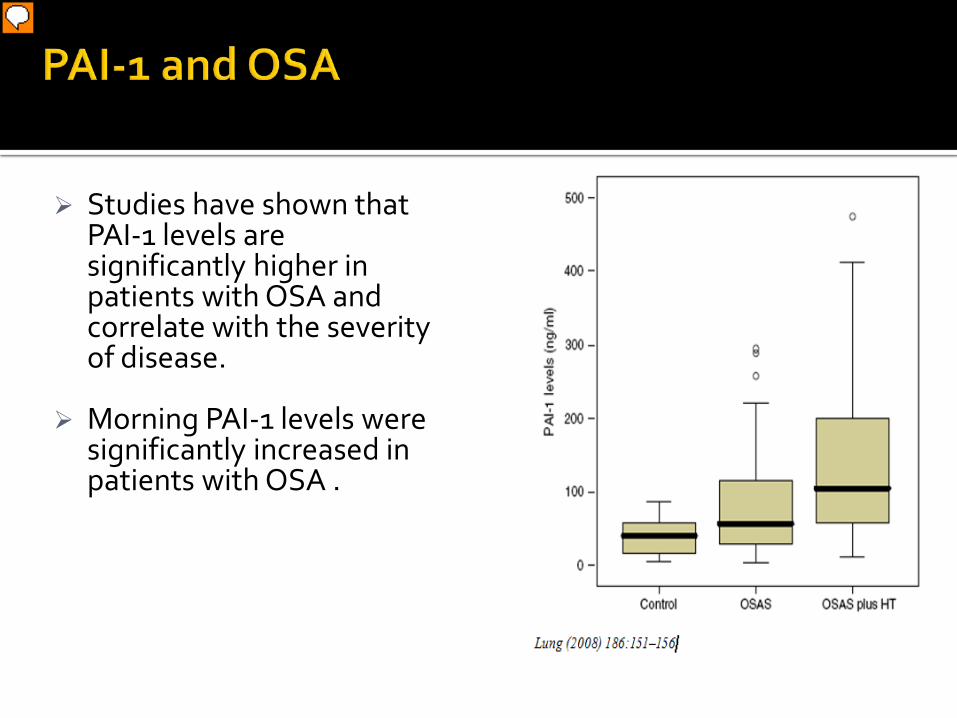
Studies have shown that
PAI-1 levels are significantly higher in patients with OSA and correlate with the severity of disease.
Morning PAI-1 levels were significantly increased in patients with OSA .
Presenter
Presentation Notes
N= 32 in each gp, Pai1 levels normal – 39, osa 59, osa and htn 105
Circadian Clock Genes Hypoxia
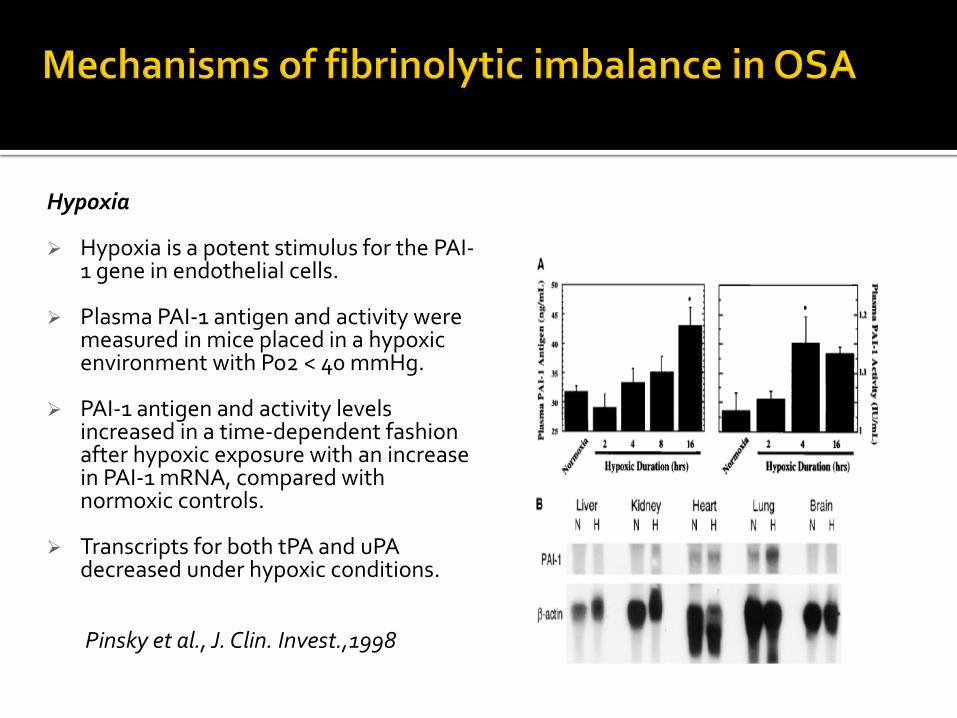
Hypoxia Hypoxia is a potent stimulus for the PAI-
1 gene in endothelial cells.
Plasma PAI-1 antigen and activity were measured in mice placed in a hypoxic environment with Po2 < 40 mmHg.
PAI-1 antigen and activity levels increased in a time-dependent fashion after hypoxic exposure with an increase in PAI-1 mRNA, compared with normoxic controls.
Transcripts for both tPA and uPA decreased under hypoxic conditions.
Pinsky et al., J. Clin. Invest.,1998
Circadian clock genes Studies have implicated the molecular components of the
body’s endogenous circadian clock as a key determinant of PAI-1 rhythmicity.
These include the transcriptional activators- BMAL1, BMAL2 and CLOCK, which directly regulate PAI-1 gene expression.
Changes in sleep-wake cycles are known to alter the amplitude of PAI-1’s oscillations .
The heightened circadian variation in PAI-1 levels noted in patients with OSA may be mediated via an effect on the circadian clock genes.
Specific Aims Assess the relationship between endothelial
dysfunction and OSA.
Characterize the relationship between circadian variation of fibrinolytic markers and OSA, to determine the circadian rhythm of PAI-1 and t-PA in patients with OSA and normal controls.
To determine the correlation between severity of OSA and fibrinolytic balance and the correlation between severity of OSA and endothelial function.
History of MI, stroke, TIA or peripheral vascular disease. History of DM, uncontrolled HTN (SBP >160, DBP > 120), ESRD on dialysis,
cancer, autoimmune or liver disease. Significant medical or psychiatric disease that may impair participation in
the trial. Evidence of medical instability (cardiac arrhythmias, CHF, pulmonary
disease) that requires expedited evaluation and treatment of OSA. History of alcohol or drug abuse during the one-year period prior to trial
participation. Current use of tobacco products. Current treatment with ACE-Inhibitors and or chronic NSAID use. Another primary sleep disorder that can cause disrupted sleep. Patients with unusual sleep or wake habits, including shift work. Trans meridian travel in the previous 3 months. Patients with OSA who have already received treatment with CPAP, surgery
or oral appliance. Pregnancy; as hormonal changes affect sleep disordered breathing.
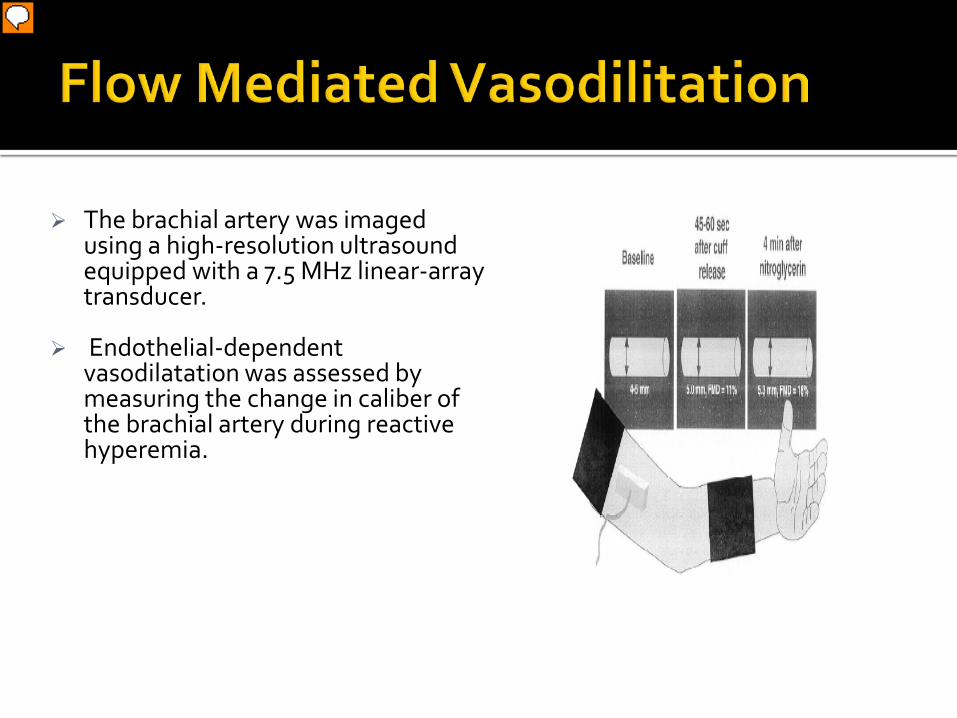
The brachial artery was imaged using a high-resolution ultrasound equipped with a 7.5 MHz linear-array transducer.
Endothelial-dependent vasodilatation was assessed by measuring the change in caliber of the brachial artery during reactive hyperemia.
Presenter
Presentation Notes
Reactive hyperemia was produced by placing a cuff on the upper arm and inflating it to suprasystolic pressure for 5 minutes, occluding flow to the forearm, resulting in dilation of downstream forearm resistance vessels.
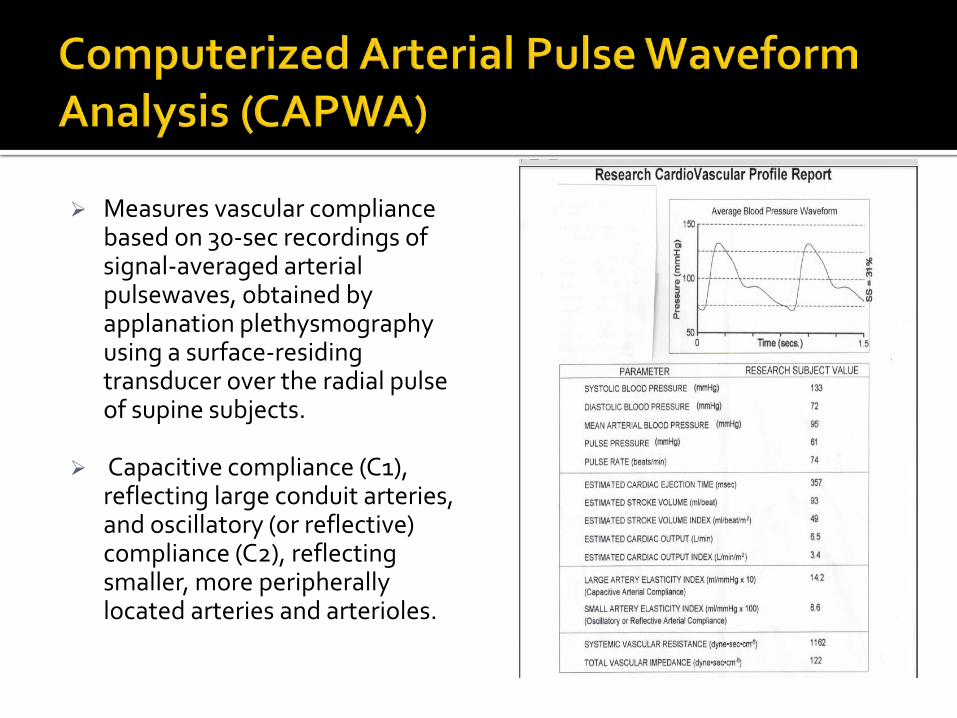
Measures vascular compliance based on 30-sec recordings of signal-averaged arterial pulsewaves, obtained by applanation plethysmography using a surface-residing transducer over the radial pulse of supine subjects.
Capacitive compliance (C1), reflecting large conduit arteries, and oscillatory (or reflective) compliance (C2), reflecting smaller, more peripherally located arteries and arterioles.
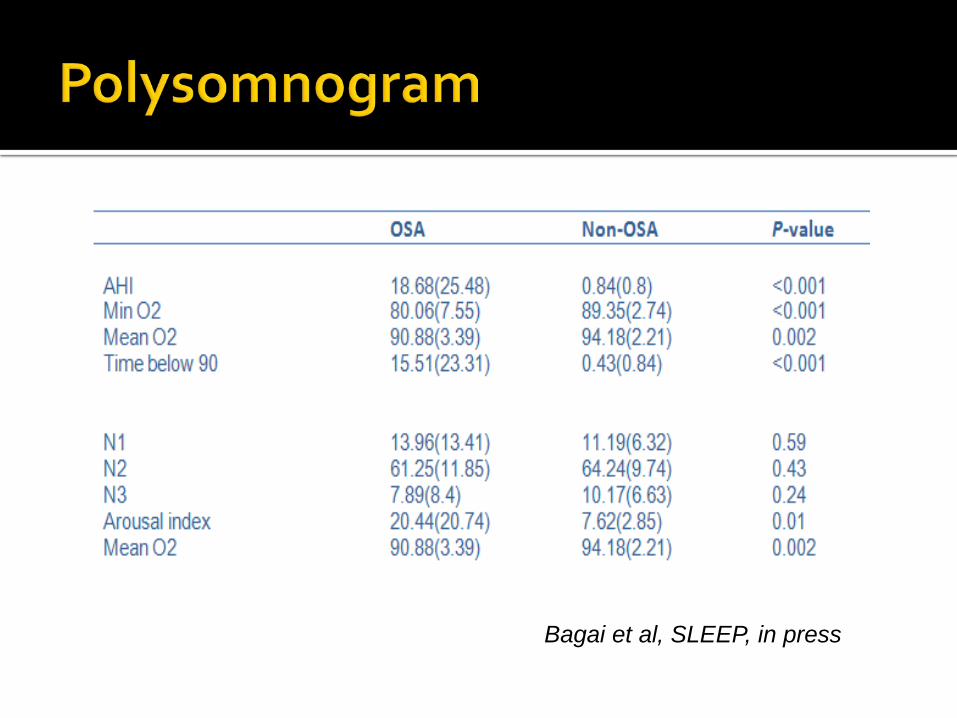
Bagai et al, SLEEP, in press
Presenter
Presentation Notes
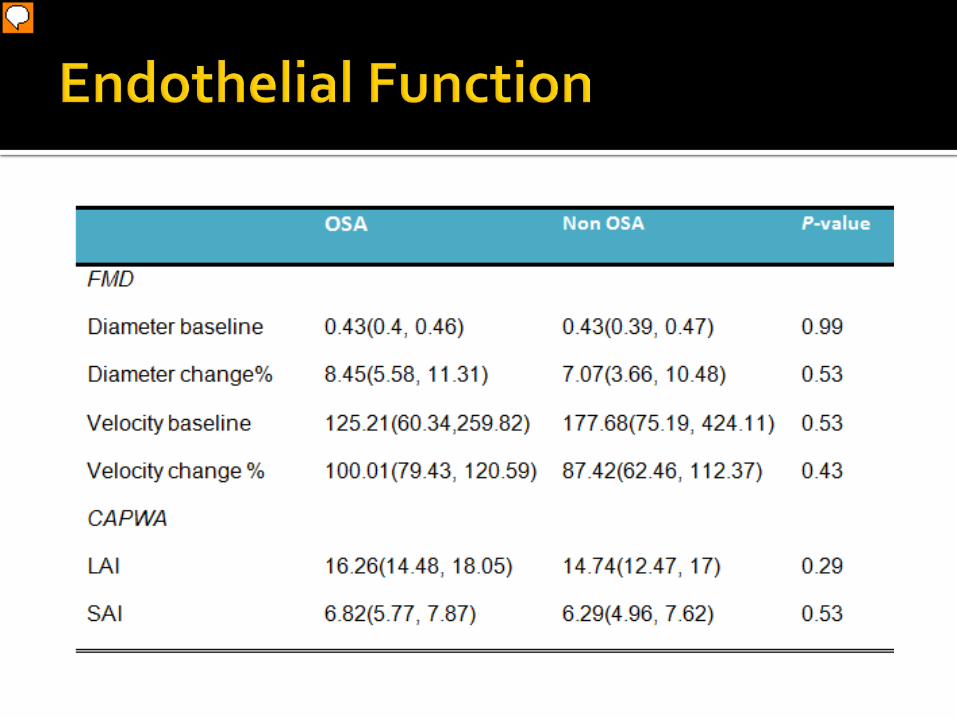
No significant difference in the markers of endothelial function. One reason for the less dramatic difference noted in our study may be due to the fact that we included patients with mild OSA , as compared with other studies which included patients with moderate to severe OSA. A further subgroup analysis based on severity of OSA may help answer this question.
Bagai et al, SLEEP, in press
Presenter
Presentation Notes
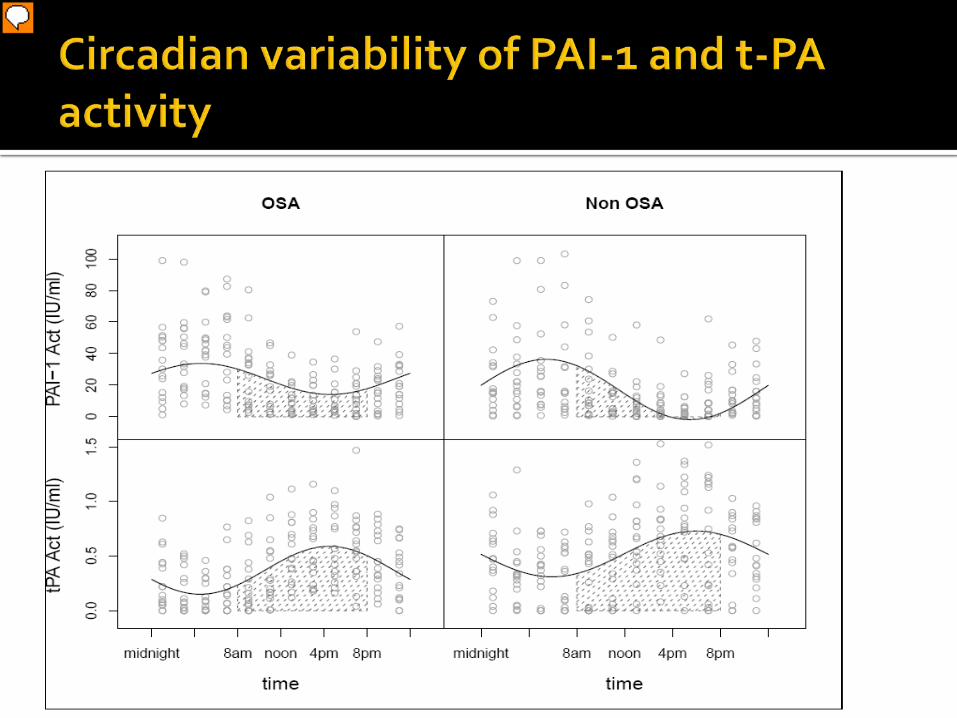
24-hour variability of PAI-1 and t-PA antigen in OSA patients and normal controls. PAI-1 and t-PA circadian variations (oscillations) were evaluated by fitting non linear mixed effect models y = (M+u1) + (A+u2) sin (2π÷24hr×t+ B), where M was the rhythm-adjusted mean, A was the amplitude, and B was the acrophase. In the above formula, the peak time (time of the day at which the maximum level of the variable was reached) was calculated by setting sin [(2*pi/24hr) * time + B] = sin [0.5 pi] = > 1. The solid line is based on the model and it is an estimator of population mean PAI-1 or t-PA antigen along the time. The mean amplitude of PAI-1 antigen in the OSA group was 5.16 (95% CI, -0.46 to 10.78) units higher than that of the non OSA group, p value =0.069.
Bagai et al, SLEEP, in press
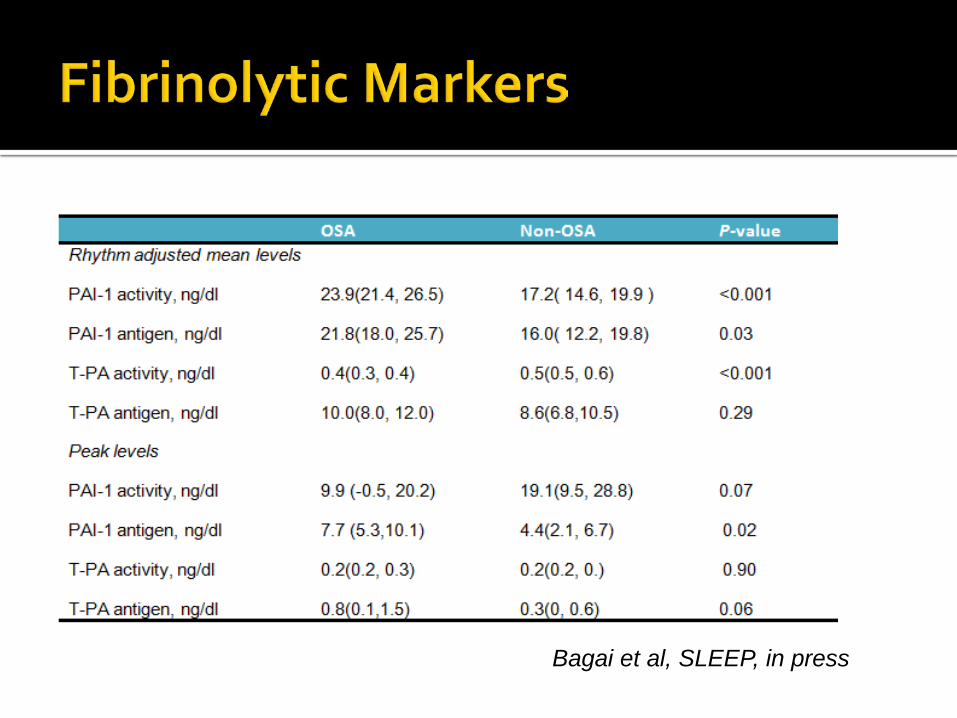
The rhythm adjusted mean levels of PAI-1 activity and antigen in the OSA group was significantly higher and t-PA activity levels were significantly lower than the non-OSA group.
The mean peak time of the PA1-1 antigen and activity and t-PA antigen and activity did not differ significantly between the two groups.
Results indicate an alteration of the circadian rhythm of fibrinolytic markers in OSA patients as compared with control subjects confirmed by overnight polysomnography.
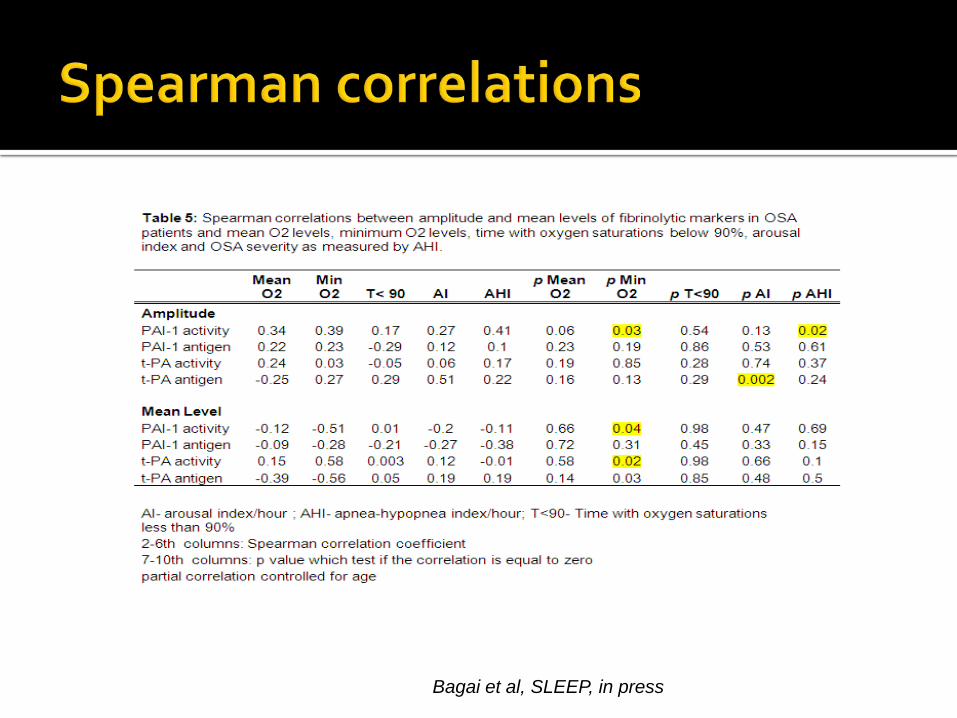
Using Spearman correlation, PAI-1 activity was strongly correlated to the minimum oxygen levels and the severity of OSA ( as measured by AHI).
Presenter
Presentation Notes
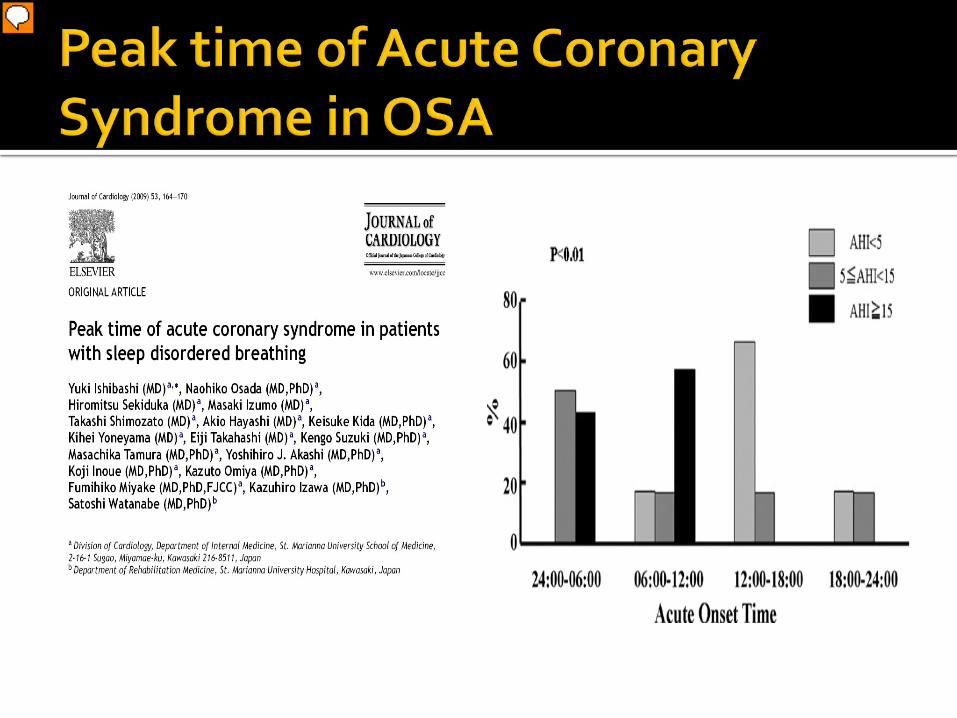
Ishibashi et al (35) recently reported that the peak onset time of acute coronary syndromes in moderate OSA patients (AHI> 15/hour) was shifted with a tendency to observe ACS between midnight and morning as the severity of OSA increased making OSA patients vulnerable to ACS in both the first part of the night and the early morning hours (between 24:00h and 12:00h). This, coupled with the known circadian variation in the efficacy of t-PA poses OSA patients to acute CVD throughout the night.(36) In addition to altered timing of fibrinolytic markers, patients with OSA experience repeated hypoxia, arousals or sympathetic activation which could trigger plaque instability and therefore influence the timing of CVD.
Alteration in fibrinolytic balance, mediated by PAI-1, may be one of the key links between OSA and CVD.
No significant differences in the markers of endothelial function were noted.
Based on the results of this study, treatment strategies to favorably shift the fibrinolytic balance can be expected to result in primary and secondary prevention of CVD in OSA.
PSG/Ambulatory PSG confirming OSA CPAP/Follow up program Alternative Therapy- Provent - Oral
Appliance - Surgery - Weight loss
PM for the diagnosis of OSA should be performed only in conjunction with a comprehensive sleep evaluation.
May be used as an alternative to polysomnography (PSG) for the diagnosis of OSA in patients with a high pretest
probability of moderate to severe OSA.
PM is not appropriate for the diagnosis of OSA in patients with significant comorbid medical conditions that may degrade the accuracy of PM, including, but not limited to, moderate to severe pulmonary disease, neuromuscular disease, or congestive heart failure.
J Clin Sleep Med 2007 ;3(7):737-747
Height _____ inches/cm Weight _____ lb/kg Age _____ Male/Female BMI _____ Collar size of shirt: S, M, L, XL, or _____ inches/cm ,Neck circumference*
_____ cm
1. Snoring 2. Tired 3. Observed Apneas 4. Blood pressure 5. BMI > 35 kg/m2? 6. Age > 50 yr old? 7. Neck circumference > 40 cm? 8. Gender male? * Neck circumference is measured by staff High risk of OSA: answering yes to three or more items Low risk of OSA: answering yes to less than three items
Adapted from: STOP Questionnaire A Tool to Screen Patients for Obstructive Sleep Apnea Frances Chung, F.R.C.P.C.,* Balaji Yegneswaran, M.B.B.S.,† Pu Liao, M.D.,‡ Sharon A. Chung, Ph.D.,§ Santhira Vairavanathan, M.B.B.S.,_ Sazzadul Islam, M.Sc.,_ Ali Khajehdehi, M.D.,† Colin M. Shapiro,
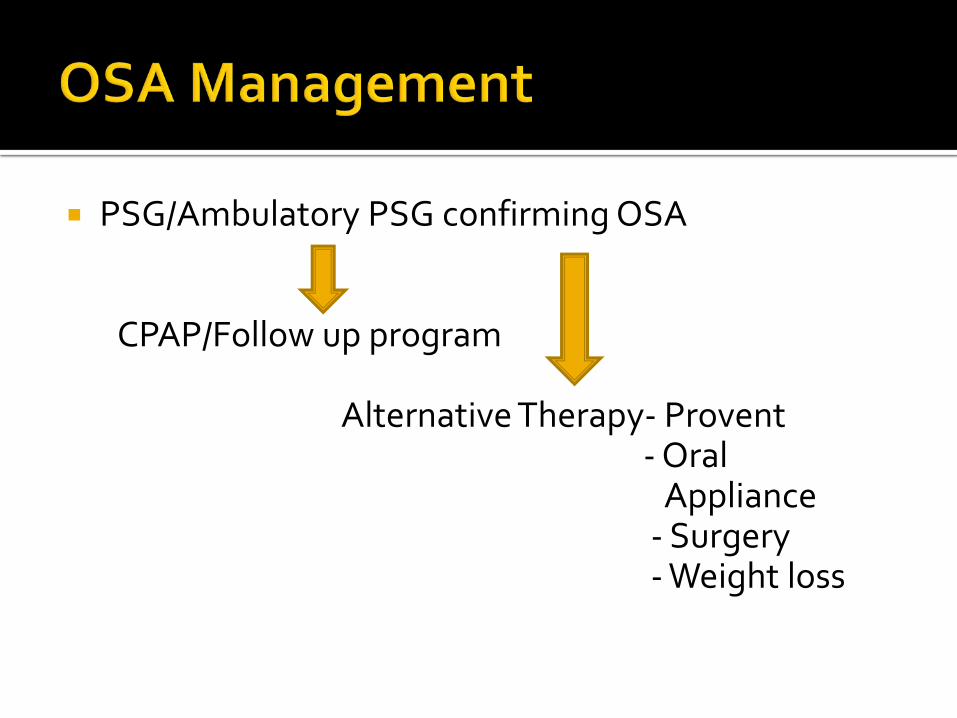
PSG/Ambulatory PSG confirming OSA CPAP/Follow up program Alternative Therapy- Provent - Oral
Appliance - Surgery - Weight loss
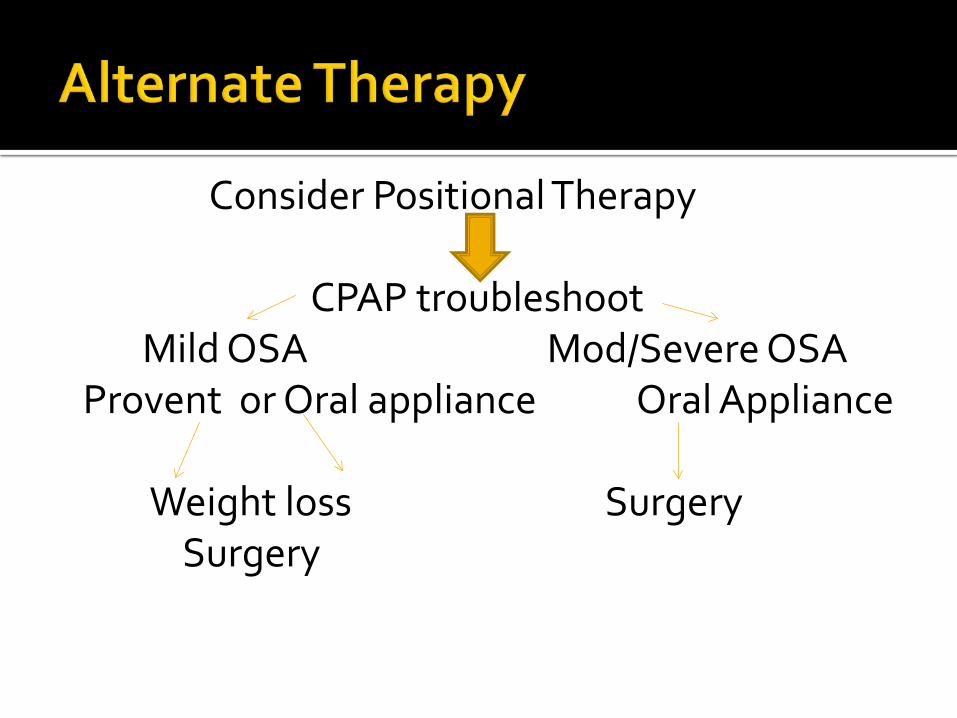
Consider Positional Therapy CPAP troubleshoot Mild OSA Mod/Severe OSA Provent or Oral appliance Oral Appliance Weight loss Surgery
Surgery

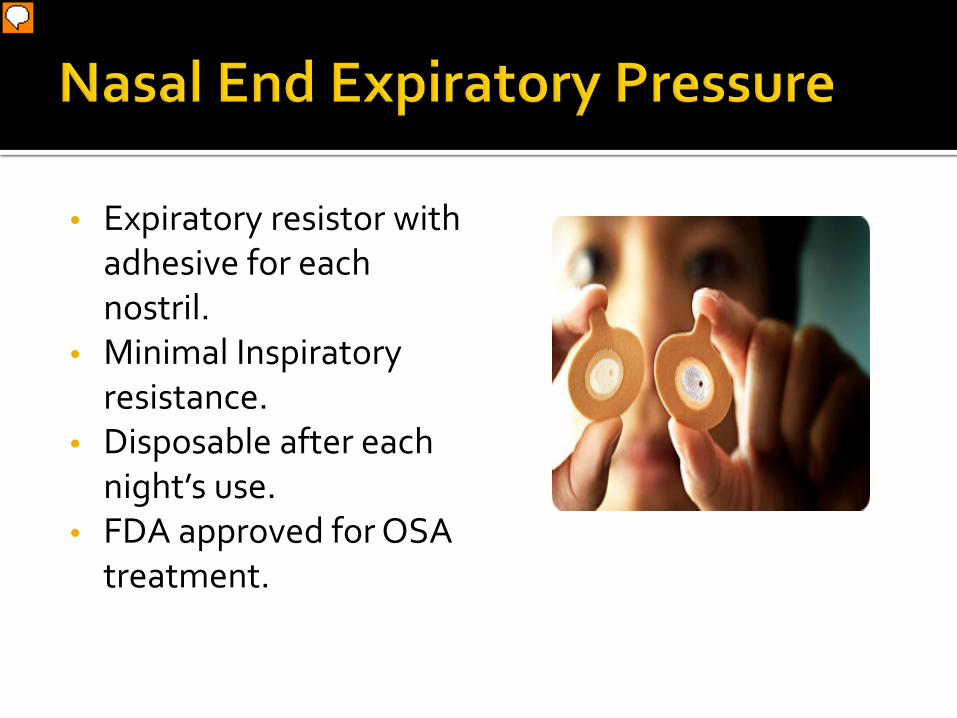
• Expiratory resistor with adhesive for each nostril.
• Minimal Inspiratory resistance.
• Disposable after each night’s use.
• FDA approved for OSA treatment.
Presenter
Presentation Notes
Works by increasing FRC during expiration. Provent acclimatization with trial pack In lab efficacy confirmation recommended Patients with demonstrated efficacy should be given prescription. May use adjunctive therapy to achieve optimal efficacy ( chin strap, positional therapy) Response rate higher in women and in patients with mild sleep apnea. EPAP could dilate the upper airway with carrover benefit to inspiration, may increase the cross-sectional area during early inspiration, results in less resistance.
Presenter
Presentation Notes
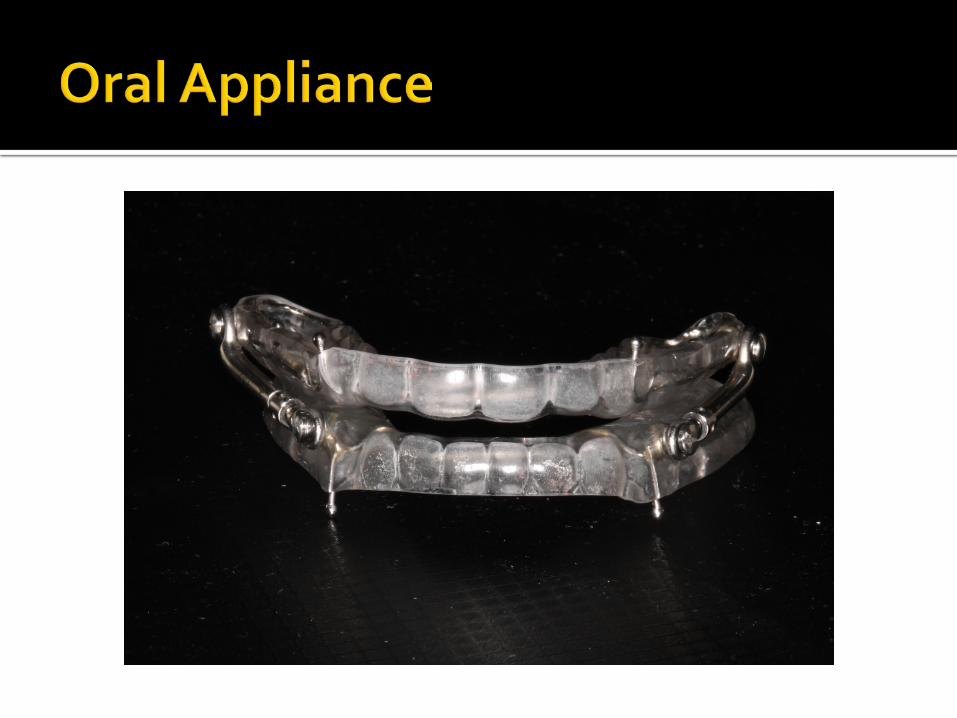
Oral appliances (OA)are indicated for use in patients with mild to moderate OSA who : Prefer OAs to CPAP Do not respond to CPAP, or are not appropriate candidates for CPAP. Fail treatment attempts with CPAP or treatment with behavioral measures such as weight loss or sleep position change. To ensure satisfactory therapeutic benefit from OAs, patients with OSA should undergo polysomnography or an attended cardiorespiratory (Type 3) sleep study with the oral appliance in place after final adjustments of fit have been performed. (Guideline)
Nasal surgery: Correction of nasal problems such as a deviated septum.
Uvulopalatopharyngoplasty (UPPP): A procedure that removes soft tissue on the back of the throat and palate, increasing the width of the airway at the opening of throat.
Tonsillectomy Mandibular maxillar advancement surgery: Surgery to
correct certain facial problems or throat obstructions that contribute to sleep apnea.
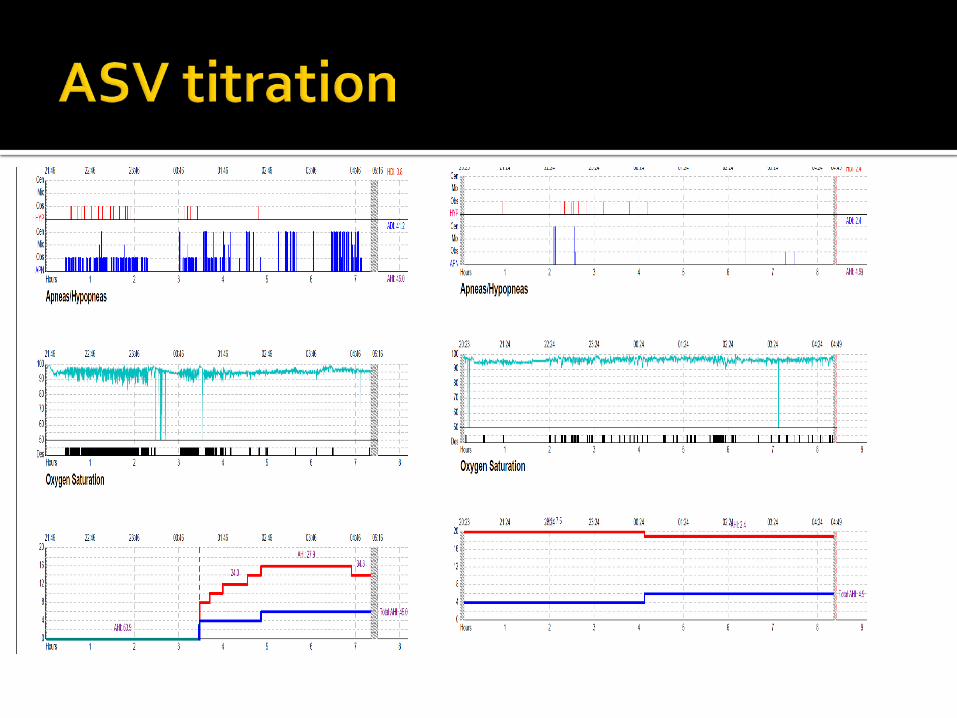
75 year old man with loud snoring, witnessed apneas, frequent nocturnal awakenings, and daytime sleepiness in sedentary situations.
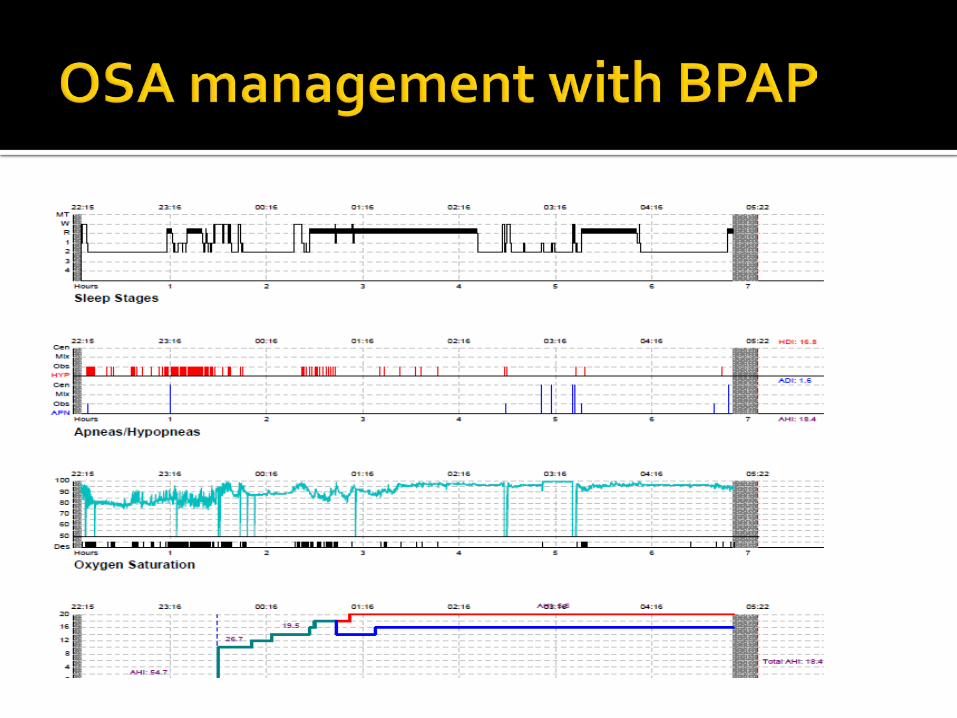
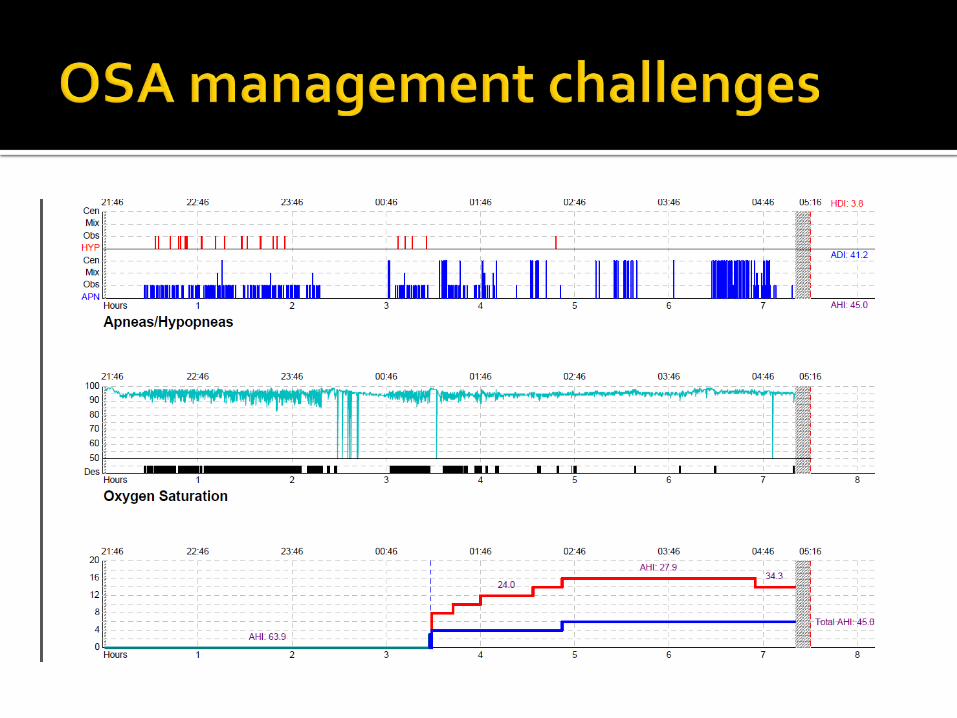
Begun on BIPAP but felt like he was “fighting machine” to breathe.
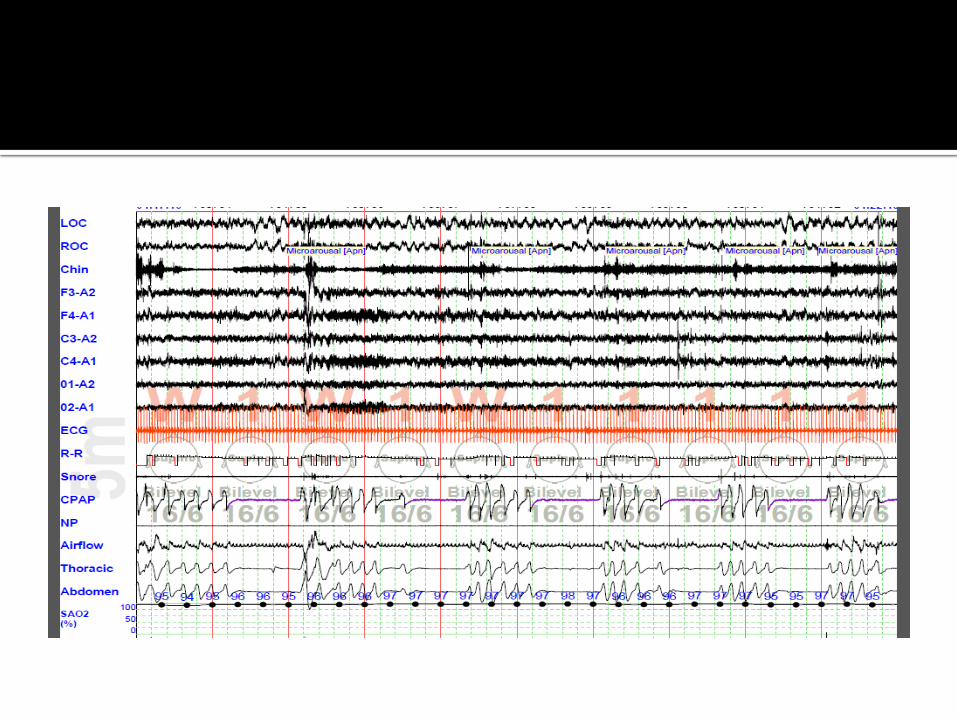
Came back for a trial of adaptive servo ventilation (ASV) and did very well.
Using ASV device every night with improved alertness and more consolidated sleep.
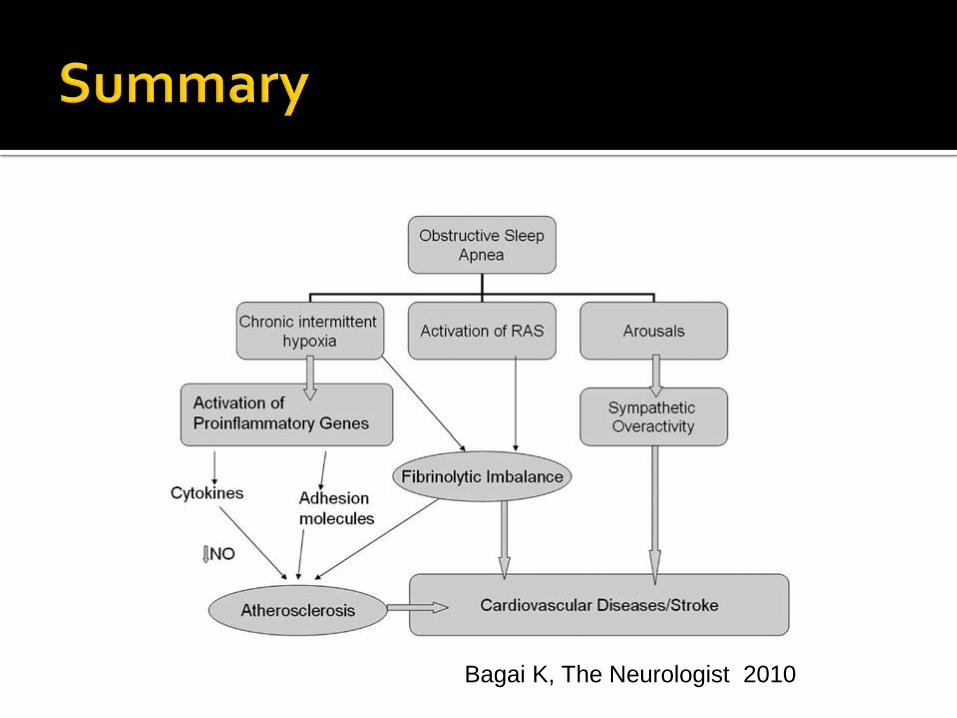
Bagai K, The Neurologist 2010
Sleep apnea and stroke are interrelated, with shared risk factors as well as plausible mechanisms that await further research
Treatment of sleep apnea may impact favorably on management of their condition and prevention of cardiovascular events
Presenter
Presentation Notes
New slide