jurnal NGT komplitt

of 31
-
Upload
allen-renaldo -
Category
Documents
-
view
251 -
download
3
Transcript of jurnal NGT komplitt
-
7/25/2019 jurnal NGT komplitt
1/31
Guidance on the insertion ofNasogastric (NG) tubes,
management of feeds andadministration of medicines via
an NG tube or via aPercutaneous Endoscopic Gastric
tube (PEG) in adults
-
7/25/2019 jurnal NGT komplitt
2/31
Guidance on the insertion of Nasogastric (NG) tubes, management offeeds and administration of medicines via an NG tube or via a
Percutaneous Endoscopic Gastric tube (PEG) in adults
Document Type Clinical Guideline
Uniue !dentifier CL-035
Document Purpose To set out evidence based practice for the insertion andmanagement of NG tubes and care of patients receiving feeds via anNG tube.
Document "uthor Vic! "reece# $eput! $irector of Nursing
Target "udience %ll health care professionals responsible for the care of patients &ith
an NG tube and receiving feeds via an NG ' "(G tube.
#esponsible Group Clinical "olicies Group
Date #atified %pril )0*)
E$piry Date %pril )0*5
This validit! of this polic! is onl! assured &hen vie&ed via the +orcestershire ,ealth andCare N, Trust &ebsite hac&.nhs.u./. f this document is printed into hard cop! or savedto another location# its validit! must be checed against the uni1ue identifier number onthe internet version. The internet version is the definitive version.
f !ou &ould lie this document in other languages or formats i.e. large print/# pleasecontact the Communications Team on 0*205 400)0 or email atcommunicationshac&.nhs.u.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
mailto:[email protected]:[email protected]:[email protected]:[email protected] -
7/25/2019 jurnal NGT komplitt
3/31
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age %of &'
-
7/25/2019 jurnal NGT komplitt
4/31
ersion istory
VersionCirculation Job Title of PersonName of Group circulated to !rief
"ate#ummar$of
Change
% %%&%% Communit! ,ospital 6atronsLocalit! 6anagers
Chief "harmacist
"atient afet! 6anager
Consultant Nurse nfection "revention 7 Control
Clinical ervices 8perational Lead outh+orcestershire/
Clinical ervices 8perational Lead 9edditch 7:romsgrove/
Clinical ervices 8perational Lead +!re ;orest/
Governance 6anager
"rofessional tandards 6anager
Training 7 $evelopment 6anager
CN "alliative Care
Learning $isabilit! 6anager
peech 7 Language Therapist Lead
troe Team Lead
6edical $irector
"rofessional "ractice ;acilitator $istrict Nursing
Trust $ietician
' &*%& Clinical "olicies Group +inor
"ccessibility
+orcestershire ,ealth and Care N, Trust has a contract &ith %pplied Language olutions tohandle all interpreting and translation needs. This service is available to all staff in the trust via a
free-phone number 0
-
7/25/2019 jurnal NGT komplitt
5/31
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age &of &'
-
7/25/2019 jurnal NGT komplitt
6/31
*ontents
*. ntroduction "age =
). "urpose of document "age 5
3. $efinitions "age 5
=. cope "age 5
5. Training ' Competencies "age 5
4. 9esponsibilities and $uties "age 4
. Contraindications for inserting an NG tube "age 4
-
7/25/2019 jurnal NGT komplitt
7/31
1. !ntroduction
1. 6alnutrition is both a cause and a conse1uence of ill-health. The conse1uences ofmalnutrition include vulnerabilit! to infection# dela!ed &ound healing# impaired functionof heart and lungs# decreased muscle strength and depression. urgical patients# &hohave malnutrition for e@ample# have around three times as man! postoperativecomplications and four times greater ris of death than &ell nourished patients havingsimilar operations. f poor dietar! intae or complete inabilit! to eat persists for &ees#the resulting malnutrition can be life-threatening in itself NC(# )004/.
2. %ll patients &ho are unable to tae ade1uate food and fluids orall! should beconsidered for an alternative route for feeding (nteral ;eeding/. This ma! benecessar! both on a short term or long term basis. Nasogastric feeding is usuall!considered as a first line in artificial nutritional support and therefore should onl! beconsidered as a short term method of feeding# normall! no more than si@ &ees 9o!al6arsden# )00
-
7/25/2019 jurnal NGT komplitt
8/31
2. Purpose of document
1. The National "atient afet! %genc! N"%/ has issued guidance indicating thatfeeding patients through a misplaced NG feeding tube is largely preventable with
potentially serious and harmful effect, and the! have therefore l(ventA.
2. The purpose of this guideline is to ensure that patients receive safe and effectivenutritional support. The guideline sets out clear evidence based practice guidelines forthe>
insertion of NG tubes?
management of feeds via an NG tube'"(G tube? and
administration of medicines via an NG tube'"(G tube.
3. Definitions
% Never Eventis a serious and largel! preventable patient safet! incident that should
not occur if the available preventable measures have been implemented.
Enteral feeding refers to the deliver! of a nutritionall! complete feed# containingprotein# carboh!drate# fat# &ater# minerals and vitamins# directl! into the stomach#duodenum or DeDunum.
4. cope
1. "atients covered are those primaril! &ithin +orcestershire ,ealth and Care N, Trust+,CT/ inpatient areas. N- nsulin dependent diabetic patients should have theestablishment of NG feeding in an acute hospital setting onl!.
2. This guideline applies to all members of the healthcare team &ho have a responsibilit!for deciding &hether an NG tube is appropriate for the patient and for the insertion of anNG tube and administration of feeds and medicines via an NG tube. t ma! includemedical staff# registered nurses# dieticians# pharmacists and speech and languagetherapists according to individual roles and responsibilities.
3. This guideline ma! also be used for patients receiving care from &ithin communit!nursing teams &ho re1uire enteral feeding'h!dration.
4. ;or the purposes of the guideline,C"/ the&illbe term referred to throughout.
5. Training.*ompetencies
%ll staff re1uired to insert NG tubes must receive theoretical and practical instruction
on ho& to safel! and competentl! insert an NG tube.
%ll staff re1uired to administer feeds and medication via an NG'"(G tube mustreceive theoretical and practical instruction on ho& to safel! and competentl! carr!out this tas.
Training ma! be delivered either as theoretical instruction via e-learning or on sitetraining and competenc! assessment. % record should be ept of the trainingreceived and the competenc! obtained b! the individual.
1. "lease refer to %ppendi@ ) for the appropriate competenc! assessment sheet for theinsertion of an NG tube.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age /of &'
-
7/25/2019 jurnal NGT komplitt
9/31
6. #esponsibilities and duties
1. 6edical staff - are responsible# in conDunction &ith other members of the healthcareteam# for decisions to commence feeding via an NG'"(G tube and for the appropriatefeeding regime and if appropriate# medication.
2. 9egistered nurses are responsible for the safe insertion of NG tubes# the checing ofongoing patenc! of NG'"(G tubes and administration of prescribed feeds andmedication as per the prescribed regime.
3. "harmacists are responsible for ensuring correct feeds and medications are in thecorrect formulation to be administered safel! via an NG'"(G tube. n the communit!setting# this &ill involve liaison &ith communit! pharmacists and clinical nursespecialists.
4. $ieticians are responsible for providing an individual regime of feeds and forarranging a home deliver! service for feeds if relevant.
7. *ontra0indications for insertion of an NG tube
1. n some clinical conditions the insertion of an NG tube must be ver! carefull!considered as there ma! be contra-indications. These ma! include>
,ead inDur! nasal intubation ma! be contra-indicated in patients &ith a fractured
base of sull because of the ris of intra-cranial insertion?
%bnormal oesophageal tract due to possible stricture# tumour or trauma?
Gastric outflo& obstruction or intestinal obstruction? or
ntestinal perforation.
2. ,C"s should also be a&are of potential difficulties of NG insertion in patients &ho>
have e@perienced previous difficulties in attempts at NG tube insertion?
have had recent surger! to the face# head and nec?
have oesophageal reflu@? or
have neurological problems that can cause an increased ris of aspiration.
3. !n all these cases, medical advice should be ta1en before proceeding2
8. afety considerations
1. 6ost patients &ho are fed via an NG tube receive this care safel! and effectivel!. f anNG tube is &rongl! placed into the lungs instead of the stomach# severe harm or evendeath can result.
2. n )005 the N"% issued guidance to help &ith the safe placement of NG tubes &iththe aim of reducing the occurrence of tube misplacement.
3. The N"% guidance highlighted the unreliabilit! of previous methods for confirming the
correc t plac emen t of the NG tube # such sh A tesas
4. t also recommended that checing the NG tube placement via chest @-ra!s should bereserved for second line checking only because of the potential for misinterpretingposition chec imaging N"%# )005/. ince that time# the N"% have reported thatincidents continue to occur due to misinterpretation of E-ra!s.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age 3of &'
-
7/25/2019 jurnal NGT komplitt
10/31
5. %s a result in )0**# the N"% issued a further safet! alert and guidance on ho& tochec for correct placement of NG tubes N"%# )0**/ recommending that the firstline testing for correct tube placement should be by pH testing. This guideline full!supports the N"% guidance.
9. Gaining informed consent
1. This guideline should be read in conDunction &ith the Consent to Treatment "olic!. The
,ealthcare "rofessional ,C"/ should aim to reduce the patientsA an@i the patientAsfearsbeforecarr!ing out the procedure. The! should e@plain full! and
clearl! the reasons for nasogastric tube placement in terms the patient &ill understand#and if receiving feeds or medicines via the NG tube# the! should ensure that the patientunderstands the reasons for this. The ,C" must consider the most appropriate andinclusive format for this communication.
2.The ,C" should invite and encourage 1uestions from the patient and obtain thepatients consent before going ahead &ith the procedure and mae a record of this inthe patients care record.
3. n the case of patients &ith receptive and'or e@pressive speech or language difficulties#it is liel! that the patient is under the care of a peech and Language Therapist# but foran! communication issues it is advisable to contact a peech and Language Therapistto obtain general advice on communication issues.
4. n the case of patients &ho lac mental capacit! to consent# the appropriate proceduresshould be follo&ed in line &ith the 6ental Capacit! %ct )005.
5.imilar consideration must also be given to the decision to insert a "(G tube.
10. #e0feeding syndrome
1. 9e-feeding s!ndrome is an important# !et commonl! overlooed condition affectingpatients and occurs &hen feeding is re-commenced after a prolonged period ofstarvation e.g. Nil b! 6outh# or in patients suffering from severe malnutrition.%ggressive introduction of nutritional support can lead to fluid and electrol!te imbalance&hich can cause life threatening complications including heart failure# convulsions andin e@treme cases coma and death.
2.9e-feeding should not be aggressive and should begin &ith a high protein# lo&carboh!drate diet and increased graduall! &hile monitoring electrol!tes and ph!sicalstatus. n these circumstances# earl! input from a dietician is advisable so that there iseffective case management.
11. Procedure or insertion of an NG tube and ongoing care
1. :efore commencing the procedure# the ,C" should have obtained the consent of thepatient and be sure that the patient full! understands &hat &ill happen during theprocedure. The! should ensure that the! have all necessar! e1uipment to hand andthat the! have the necessar! documentation read! to mae appropriate records.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age 4of &'
-
7/25/2019 jurnal NGT komplitt
11/31
%%2% Euipment needed
;ine bore nasogastric feeding tube &ith radio-opa1ue line and guide &ire such as
;locare/.
p, indicator paper.Non-sterile gloves N-$ependent upon techni1ue# sterile gloves should be used&ith immuno-compromised patients if a non touch techni1ue can not be adopted/.
40ml purple s!ringe for enteral feeding under no circumstances should an V
s!ringe be used/.
terile &ater and galipot.
Clinicall! clean receiver.
Tissues.
$rining &ater and stra& for the patient to drin unless contra-indicated/.
;i@ative tape.
ingle use disposable plastic apron.
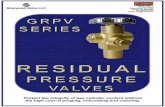
%%2& !llustration of correct tube positioning in nasogastric tract
%%2+ Procedure for passing the nasogastric feeding tube
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
-
7/25/2019 jurnal NGT komplitt
12/31
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age 5of &'
-
7/25/2019 jurnal NGT komplitt
13/31
"*T!6N #"T!6N"7E
*. (@plain the procedure to the patient. 9educe an! an@ieties# ensure the patientunderstands the procedure and consents.
). "lace the patient in an upright To improve the chance of oesophagealposition &ith head fle@ed slightl! intubation.for&ards. f patient unable to sit
upright lie on one side.
Diagram on the left sho8s correct position forpassing NG tube 8ith head slightly fle$edfor8ard
3. %gree &ith the patient a signal b! To enable the patient to stop the procedure if&hich he or she can indicate to stop the! &ish.the procedure e.g. b! raising a hand.
=. Cleanse hands and put on gloves. 9educe the ris of introducing infection.
5. 6easure the distance from the To ensure that the correct length of tube ispatientAs ear lob
passed into the stomach. f too much tube is
nose# plus the distance from the passed this riss ining or coiling in thebridge of the nose to the bottom of stomach# this ma! cause problems &henthe @iphisternum, using the mar1 on removing the guide &ire or the tube ma!the NG tube using the closest mar become bloced or notted. f too little tube
on the tube. is passed# then the tube could be l!ing in theoesophagus and aspiration of feed ma!ensue.
4. Lubricate the tip of the tube &ith To assist the passage of the tube.sterile &ater.
. Chec thepatien
To ensure there is no obstruction.
deviated septum or nasal pol!ps.
-
7/25/2019 jurnal NGT komplitt
14/31
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age 9of &'
-
7/25/2019 jurnal NGT komplitt
15/31
soap and &ater. securing the tube later.
**.(nsure guide &ire is firml! placed To mae sure the guide &ire does not slipinside the tube. out &hile passing the tube.
*). %dvance the tube into the nostril# aim To facilitate the passage of the tube follo&ingthe tube horiFontall! and posteriorl! the natural anatom! of the nose and avoidingalong the floor of the nasal cavit!. f trauma to the nasal turbinates.obstruction is felt &ithdra& the tubeand tr! again at a slightl! differentangle.
13.%s the tube approaches the naso- To help the tip of the tube pass into the phar!n@as the patient to s&allo& oesophagus.
&ater unless contra-indicated/ andadvance the tube as the patient
s&allo&s. N- f the patient startscoughing or gagging &hen the tubereaches the orophar!n@# stopadvancing the tube until the coughingstops# then continue.
*=. f the patient becomes distressed or 9educe patient distress.agitated# &ithdra& the tube andpostpone the procedure. nform6edical taff and $ietician.
*5. f the patient becomes short of The tube ma! have passed into the trachea
breath# c!anosed or e@periences and caused trauma to the lung.chest pain# &ithdra& the NG tube andsee medical help.
*4. +hen the limiting mar on the tube is The tip of the tube should no& have reachedreached stop advancing the tube. the stomach.
*. Lightl! tape the tube to the chee. To hold the tube in place &hile position of the
tube is confirmed.
*
-
7/25/2019 jurnal NGT komplitt
16/31
Tr! again b! repositioning thepatient on their left side f the stomach is empt!# b! allo&ing the
patient to drin &ill increase the volume of
f the patient is able to safel! gastric contents thus maing aspiration
s&allo as them to tae a easier.small drin of &ater and tr!again.
)0. 8nce positioning is confirmed# This facilitates easier removal of the guideactivate the internal lubricant of the &ire.tube b! flushing *0ml of freshl! dra&n
drining tap &ater through the guide&ire port unless patient is immune-compromised# in &hich case# cooledboiled or sterile &ater can be
considered/ .
)*. 9emove the guide &ire b! using The guide &ire should be removable &ithgentle traction. gentle traction. N- once removed the guide
8ire must never be reinserted2 f despiteusing this techni1ue for removal# the guide&ire &ill not come out# proceed to removethe &hole tube and the procedure &ill needto be repeated &ith a ne& NG tube.
)). ecure tube to patientAsfaceusinga To ensure NG tube remains firml! in positionfi@ative tape such as 6icropore# thus reducing the ris of pulmonar!
ensuring itAs ep aspiration and ma@imise patient comfortfield of vision. The tape should be N- Chec that the pat
secured in such a &a! that provides a fi@ation tape.bridge bet&een the tube and the sin
to reduce friction.
)3. % thin piece of ,!drocolloid dressing# To ensure sin integrit! in the area.such as Granufle@# can be placedunder the tubing and attached to the
patientAs chee#
reduce sin irritation especiall! if thetube is in place for some time.
)=. $ocument the insertion details in the To optimise communication bet&een thepatient records on the NG tube healthcare team and for checing purposes.
patenc! sheet see %ppendi@ *.
)5. 6aintain nasal h!giene and To ensure patient comfort.mouthcare.
)4. "erform ongoing checs for pressure To maintain sin integrit! and patientdamage. comfort.
). Commence fluid balance chart. To ensure accurate documentation.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
-
7/25/2019 jurnal NGT komplitt
17/31
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age %%of &'
-
7/25/2019 jurnal NGT komplitt
18/31
11.4 "ctions to be ta1en if difficulty e$perienced in obtaining aspirate
1. There are a number of reasons &h! aspirate ma! not be immediatel! obtainable after
insertion of the NG tube. The ,C" should not immediatel! arrange @-ra! confirmationbut should consider the follo&ing reasons and actions?
%ir in s!ringe but no aspirate the NG tube ma! not !et have reached the level ofgastric secretions therefore - slo&l! advance the NG tube ma@imum of anadditional *0 cm/ and repeat the aspiration.
No air or aspirate obtainable the NG tube can sometimes be occluded b! beingplaced up against the gastric mucosa therefore - gentl! &ithdra& the NG tube asmall amount and attempt aspiration.
No air or aspirate obtainable - the NG tube ma! have been advanced too far andinto the duodenum therefore ver! slo&l! pull bac on the NG tube and attempt to
aspirate.%spirate amount obtained is less than 0.5 ml this could be due to lo& levels ofgastric secretions therefore position the patient onto left lateral side and ifpossible at 30 degrees# and attempt aspiration again.
%%2/ ;0#ay confirmation of tube placement
a. E-9a! confirmation should onl! be considered &hen the p, test has been tried andfailed and then clearl! documented in patientsA reco
2. %rrange the E-ra! and ensure that the patient records are sent &ith the patient to the @-
ra! department. 8nce the @-ra! has been completed# the radiolog! staff should &rite inthe patientsA records &hether the NG tube i the @-ra!.
3. N- nder no circumstances should the guide &ire be reinserted into the tube if it hasalread! been removed. The @-ra! can be taen &ith or &ithout the guide &ire in placeas the tube itself is radio-opa1ue.
4. 8n return to the clinical area# if the tube coughing or retching# then feeding via the NG tube cancommence. ,o&ever# furtherattempts at aspirating should still be carried out.
5. N- f there is an! continuing doubt as to the positioning of the tube# then advice mustbe sought from medical staff or other clinical specialists before proceeding &ith feeding.
11.6
"rior to an! substance being administered such as feeds# &ater or medication.
f there is an! doubt of the tube not being in the correct position.
f the patient is coughing# retching or vomiting.
f the recorded mared length of the tube has changed this ma! mean that the tube
has migrated in or out of the nostril.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age %&of &'
-
7/25/2019 jurnal NGT komplitt
19/31
f the patient displa!s signs of respirator! distress such as shortness of breath#&heeFing# change of colour in the face.
f there has been a decrease in 8)%Ts readings.
11.7 =anagement of a bloc1ed tube
1. 8ccasionall! fine bore NG tubes can become bloced. The follo&ing actions should betaen>
f attached to a feeding giving set chec the clamp is open.
%ttach an empt! 40 ml purple s!ringe and pull the plunger bac to tr! and unblocthe tube.
6assage the tube b! rolling it gentl! bet&een !our fingers using small movements
onl!. tart from the end furthest a&a! from the bod! and &or to&ards the nose.
Tr! flushing &ith 30 ml of &arm &ater# &ait 30 minutes then tr! again.
D6 N6T use force and do not use any sharp ob>ects to try and unbloc1 tube
D6 N6T try to reinsert the guide 8ire in an attempt to dislodge the bloc1age
2. f the tube &ill not unbloc remove the tube and reinsert a ne& NG tube.
12. afety and appropriate chec1s of patients 8ith NG tubes
1. This guideline sets out the procedures to follo& to ensure that patients receive safe andeffective care &hen having an NG tube inserted# and feeds and medicines via thenasogastric route. ,C"s should remain vigilant to the potential complications of enteralfeeding and be a&are of the follo&ing>
,C"s involved in carr!ing out the procedures contained in this guideline should
have received appropriate training and assessment of competence.
9ecord eeping of all procedures should be accuratel! recorded.
E-ra! confirmation of tube placement should not be the *stline confirmation method
and onl! used if all other methods have failed# or specificall! indicated.
%ll NG tubes re1uire regular flushing to prevent blocage before starting a feed#&hen the feed is stopped# and before and after the administration of medicines. Thetube must be flushed &ith 30 ml of freshl! dra&n drining tap &ater unless thepatient is immunocompromised# in &hich case# cooled boiled or sterile &ater can beconsidered.
+herever possible# patients should be positioned sitting up at an angle of at least 30
degrees during nasogastric feeding and for at least an hour after feeding.
%ll s!ringes used for enteral use should be those designed specificall! for enteral
feeding N"%# )00/.
Three-&a! taps and s!ringe tip adaptors should not be used in enteral feed s!stems
N"%# )00/.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age %+of &'
-
7/25/2019 jurnal NGT komplitt
20/31
%ll used giving sets should be discarded after )= hours# and all bottled feeds shouldbe used &ithin a )= hour period once removed from the fridge.
The patient should be &eighed if possible at the start of a feeding regime and then
&eel!# maing recordings on the appropriate chart.
%ssess ris of re-feeding s!ndrome.
%+2 "dministration of feeds via an NG.PEG tube
a. The feeding regime should have been discussed and agreed b! the dietician'nutritionist
to ensure it meets ntsthe. patientsA re1uireme
2. Continuous feeding using a feeding pump is the method of choice and should be givenover a ma@imum on )0 hours. This allo&s the feed to be administered at a stead! rate.
3. "atents should be &eighed at the beginning of a feeding regime &ith the &eight
recorded in the patient record and then &eighed &eel! if possible.
4. f a decision is made to stop the feeding regime# this should be discussed &ith thepatient if appropriate and their famil!'carers and form part of a multi-disciplinar! teamdiscussion.
5. f a decision to stop a feeding regime is made because it is felt the patient has recovered theirs&allo&ing abilit!# the pa monitored dail! and their &eight closel! monitored.
6. %n! &eight loss or changes in the patientAs conditionbediscussedshould&iththedietician'clinical nurse specialist'speech and language therapist to agree a treatment
plan.
%+2% Euipment needed
"rescribed feed.
%ppropriate giving set.
40 ml purple s!ringe.
;reshl! dra&n drining tap &ater for flushing.
;eeding pump.
ingle use disposable gloves and apron.
13.2 The feeding procedure
a. The feeding procedure should be carried out as follo&s>
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age %'of &'
-
7/25/2019 jurnal NGT komplitt
21/31
"*T!6N
1. (@plain the procedure to the patient and gain their consent - ensures the! areat ease and understand &hat is about to be carried out.
2. Tae the feed and necessar! e1uipment to the patient.
3. (ncourage the patient to assist if the! are able to do so as this &ill assist intraining the patient in becoming self caring if appropriate.
4. ndertae hand h!giene including the patient if assisting/ and put single usedisposable gloves and apron.
5. %ssist the patient into sitting position.
6. Chec placement of the NG tube prior to food'drug administration to ensurepatient safet!
7. ;lush the tube &ith 30 ml freshl! dra&n drining tap &ater unless patient isimmuno-compromised# &hen cooled boiled'sterile &ater should be used.
8. hae the feed if re1uired and open the bottle of feed. cre& onto the givingset &ith the clamp closed
9. $ecant the feed into the reservoir and scre& on the cap of the giving set
10. "rime the giving set as per manufacturers instructions to ensure there are no
air bubbles
11. %ttach the bottle to the enteral instructions.
12. Connect the end of the giving set to the end of the tube.
13. et the rate on the pump to the re1uired rate and s&itch the pump on.
14. Chec that the pump alarm is on b! referring to manufacturerAsinstructions.
15. 8nce the feed has run through# turn off the pump.
16. ;lush the tube &ith 30 ml of freshl! dra&n drining tap &ater as soon as thefeed has finished.
17. deall! the patient should remain sitting up for at least an hour after the feedhas stopped.
18. $ispose of all e1uipment and discard the giving set and all otherconsumables. 9emove personal protective e1uipment and undertae handh!giene.
19.$ocument as appropriate on relevant sheet.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age %/of &'
-
7/25/2019 jurnal NGT komplitt
22/31
14. "dministration of medicines via an NG tube
1. % maDor safet! concern relates to the inappropriate administration of drugs intended fororal'enteral administration via the intravenous route in error. The National "atientafet! %genc! published an alert N"% "atient afet! %lert *2 ssued 6arch )00/and recommended the follo&ing>
1. To ensure that the riss are reduced to a minimum# the follo&ing points should beadhered to at all times>
8nl! use labelled oral'enteral s!ringes that cannot be connected to intravenous
catheters or ports to measure and administer oral li1uid medicines.
$o not use intravenous s!ringes to measure and administer oral li1uid medicines.
(nsure stocs available are of the correct t!pe of oral'enteral s!ringes.
(nsure patients or carers are supplied &ith the correct t!pe of oral'enteral
s!ringes.
(nteral feeding s!stems should not contain ports that can be connected tointravenous s!ringes or that have end connectors that can be connected tointravenous or other parenteral lines.
Three-&a! taps and s!ringe tip adaptors should not be used in enteral feeding
s!stems because connection design safeguards can be b!passed.
2. "atients &ho need to have medicines administered via NG'"(G tube should have their
prescriptions revie&ed and their regime simplified &here possible. Considerationshould be given to using other routes and'or once-dail! regimes &here possible. Thepharmacist ma! suggest alternative medicines'routes if there is doubt about thesuitabilit! of a medicine to be given via an NG'"(G tube.
3. The prescriber must change the route on the prescription chart to mae it clear that themedicines are to be given via the NG tube or via a "(G tube.
4. +here possible all medicines should be prescribed in li1uid or soluble tablet form toavoid blocage of tube. ome tablets that are not mareted as soluble &ill neverthelessdisperse in &ater. The ,C" should discuss an! medicine &hich does not come in li1uidor soluble form &ith the medical team or the pharmacist.
5. ome li1uid medicine preparations can be ver! thic and should be diluted &ith ane1ual volume of &ater before administration but specific guidance should be soughtfrom the pharmacist.
6. ,o&ever# administration of medicines b! unlicensed methodsis sometimes necessar!to ensure that patients receive appropriate treatment. uch unlicensed methods &ouldinclude>
Crushing tablets.
8pened capsules to access contents.
The administration of a particular medicine via an NG tube.ome li1uid preparations chec :N;.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age %3of &'
-
7/25/2019 jurnal NGT komplitt
23/31
7. nlicensed methods means that the medicine manufacturer &ill assume no liabilit! foran! harm that ma! occur to the patient or the person administering the medicine.%l&a!s see pharmacistAsadvice for the avoidance of doubt. "atients should also beadvised that an unlicensed product is being prescribed and the reasons for doing andtheir consent should be documented.
8. "t all times, the method chosen should minimise any potential for harm so thatthe benefits of giving treatment in an unlicensed 8ay, out8eighs any potentialris1s2
9. The pharmacist 8ill advise of the appropriateness and suitability ofadministering medicines in an unlicensed 8ay ?*Ps should not crush tablets oropen capsules for administration through an NG.PEG tube unless this has beendiscussed and agreed 8ith the pharmacists first and this is recorded on theadministration chart2
14.1 =edicines that must N6T be crushed or opened
1. The table belo& indicates the oral preparations that must notbe crushed or capsulesopened.
Type of =edication E$ample #eason
(nteric Coated Tablets 6ared $iclofenac# odium 6edicine designed not to be released(C'(N Valproate# in stomach.
ulfasalaFine
lo& 9elease "reparations 6ared $iltiaFem# Nifedipine# 6edicine designed to be releasedL% ' % ' C9' EL ' 9 Verapamil# 6orphine over prolonged period
C!toto@ics 6ethotre@ate 9is to practitioner ' carer
%nitibiotics ;luclo@acillin 9is to practitioner ' carer
"rostaglandin %nalogues 6isoprostol 9is to practitioner ' carer
,ormone "reparations C!proterone 9is to practitioner ' carer
;ilm Coated ugar Coated tablets Huinine ulphate ' 9is to practitioner ' carer
mared f'c s'c bisulphate "oor tasting medicinebuprofen 9apid degradation of drug
:uccal'sublingual tablets "rochlorperaFine buccal 9educed drug absorptionoft gelatine capsules Ciclosporin "oor?! soluble in &ater
14.2 Procedure for administration of medicines via an NG.PEG tube
1. top the feed if one is in process.
2. Chec if a time dela! is re1uired bet&een the feed and administration ofmedicines# before administrating the medication.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age %4of &'
-
7/25/2019 jurnal NGT komplitt
24/31
3. ;lush the tube &ith 30ml of freshl! dra&n tap &ater via a 40ml purple enterals!ringe.
4. (ach medicine should be administered separatel!. f it is all administered togetherand the tube becomes bloced# it &ould not be possible to evaluate ho& much ofeach drug &as given.
5. %ll medicines must be administered as soon as the! are prepared.
6. Liquid medicines should be dra&n up in a 40ml purple enteral s!ringe.
7. Injectable formulations given enterally should be diluted &ith 30ml freshl! dra&ntap &ater before administration.
8. Effervescent tablets should be added to a beaer of freshl! dra&n tap &ater# andonce the reaction has finished# the solution should be dra&n up &ith a 40ml purpleenteral s!ringe.
9. :et&een each medicine flush the tube &ith at least *0ml of freshl! dra&n tap &aterusing a 40ml purple enteral s!ringe. ;lush again &ith 30ml once all medicineshave been administered.
10.8nce all medicines have been administered# enter the total amount of &ater used
onto fluid balance chart.11.9e-start feed if necessar!.
N- :e a&are that in fluid restricted patients# the total amount of &ater used for tubeflushing ma! have to be reduced.
Tablets some tablets &ill disperse &hich is preferable to crushing# but ifcrushing is necessar!# crush using a tablet crusher or bet&een ) metal spoonsif not available/ and add to &ater before dra&ing up into enteral s!ringe.
*apsulesgentl! pull apart the capsule shell and empt! the po&der contents
into &ater before dra&ing up into enteral s!ringe.
%/2 6ther measures in support of safe practice
15.1 !nfection prevention and control
1. ,and h!giene should be carried out before the insertion of an NG tube and beforeadministration of feeds. Non-sterile gloves should be &orn and a ne& plastic apronshould be &orn before each procedure.
2. %ll s!ringes and giving sets used must be single use onl!.
3. The use of freshl! dra&n tap &ater is appropriate in individuals &ho are not immuno-compromised. Cool boiled or sterile &ater can be considered as an alternative option inthose &ho are immuno-compromised. The &ater must not be shared &ith other patientsand must be discarded after )= hours. f sterile &ater is used for flushing the tube itma! be decanted from a one litre bottle of sterile &ater# ho&ever the bottle must belabelled &ith the patient name and date and time of opening. t must not be shared &ithother patients and must be discarded after )= hours.
15.2 #ecord 1eeping
1. %s &ith an! clinical intervention# accurate record eeping is essential. "lease refer to
%ppendi@ * and ) for the appropriate form to be used in support of these guidelines.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age %5of &'
-
7/25/2019 jurnal NGT komplitt
25/31
15.3 Discharge planning for patients 8ith NG tubes from inpatient areas
1. f the patient is being discharged from an inpatient area into the communit! &ith an NGtube in position# and is to receive feeds via the tube# this should onl! be considered ifthe patient or carer is assessed as being competent to manage the feeding at home to
ensure patient safet! and compliance &ith the N"% )005 guidance.
2. The potential riss of poor management of an ind&elling NG tube are serious andpotentiall! life threatening and are>
"spiration of feeds, 8ater or medication into the lungs this can be due tomisplacement of the tube &hich can occur on initial insertion or due to the patientcoughing or retching after the NG tube is placed.
The tube falling out or the tube becoming bloc1ed ?this could lead to theinabilit!to administer the full nutritional re1uirements# fluids or medication that the patientre1uires.
3.
Therefore all appropriate measures must be in place for successful patient dischargeas follo&s>
f appropriate# the communit! nursing team should also be contacted to chec on the
patientsA abilit!. to manage at home
Training has been provided to the patient or carer if appropriate/ in all aspects offeeding to include managing the e1uipment# management of the tube and simpleproblem solving before the discharge is planned.
The discharging nurse should inform the $ietician and pharmacist of the dischargedate 5- da!s prior to patient discharge This is to ensure that the $ietician has timeto arrange home deliver!# and to contact the G" regarding feed prescriptions#arrange pump training for patient'carers and the pharmacist to organise the
appropriate medicines and medication leaflet.
%rrangements are in place to enable the patient to be seen b! an appropriate ,C" if
there are an! problems &ith the tube placement or abilit! to administer the feeds.
The patient is provided &ith the contact details of &ho to contact if there are an!
problems &ith appropriate )= hour support.
"rior to discharge the nurse must ensure that the patient is given a da! suppl! of
40ml purple s!ringes provided b! the &ard/ and a da! suppl! of giving sets.
6edications must have been ordered and a da! suppl! of feed is sent home.
%rrangements must be in place for an (nteral feeding pump to be supplied Do not
send 8ard pump)2
%n enteral feed regimen has been agreed and a medications leaflet supplied.
The $ietician has put plans in place for ongoing supplies of s!ringes and giving setsfor the patient in the Communit!.
% discharge checlist has been full! completed.
16. =onitoring implementation
1. 6onitoring implementation# compliance and effectiveness of this guideline &ill becarried out via the respective governance groups in the Trust. %n! incidents relevant tothis guideline &ill be monitored via governance meetings and lessons learned across
relevant clinical areas.2. Compliance &ith documentation &ill be monitored as part of ongoing clinical audit of
records.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age %9of &'
-
7/25/2019 jurnal NGT komplitt
26/31
17. #eferences
%nderton# % )000/ 6icrobial contamination of enteral tube feeds ho& e can reduce theris. Nutricia Clinical Care
:%"(N )00=/ %dministring $rugs Via (nteral ;eeding Tubes % "ractical Guide# :ritish%ssociation for "arenteral 7 (nteral Nutrition &&&.bapen.org.u'pdfs'drugsI)4enteral'practical-guide-poster.pdf
Cannab! %# (vans L# ;reeman % )00)/ Nursing care of patients with nasogastric feedingtubes :ritish Journal of Nursing Vol **# No 4
Clare J# Crans&ic G# $ennis 6 # ;laig 9 et al )005/ Effect of timing and method ofenteral feeding for dysphagic stroe patients !"##$% & a multicentre randomisedcontrolled trial The Lancet# Vol 345# ;eb )4# )005
Colgiovanni L *222/ 'aing the tubeNursing Times 25 )*/ 43-
,uman 9ights %ct *22
-
7/25/2019 jurnal NGT komplitt
27/31
"ppendi$ %
N"6G"T#!* TU-E (NG) "atient ticer
*are Plan
Problem The patient is unable to meet their o&n ade1uate nutritional needs #evie8orall!.
Date.Time.ig
Goal To meet the patients nutritional needs b! using a fine borenasogastric tube
"ction (nsure the enteral feeding process is e@plained to the patient andfamil!'carers# &ith consent sought and documented
(nsure correct tube position prior to each feed or medicationadministration b! testing aspirate &ith p paperand that tube issecured appropriatel!. 9ecord gastric aspirate p, level on NG tubepatenc! sheet at each feed.
$ocument the tube lot number and e@pir! date and repeat if tube isreplaced
Change adhesive tape or patch ever! )=-=< hours and chec sin
integrit!
%dminister feeds at rate and times as prescribed
The tube mustbe flushed &ith 30 ml of freshl! dra&n drining tap&ater# using a 40ml purple enteral s!ringe before and after each feedthe s!ringe mustbe single use onl! in inpatient settings
f tube becomes bloced flush &ith a further 30 ml of &arm &ater or ifnecessar!# replace the tube
Giving set must be changed ever! )= hours
6aintain fluid balance chart and monitor and record bo&el actions. fno bo&el action for 3 or more monitoring periods# inform medicalteam. f the patient suffers from diarrhoea on commencement offeed# half the rate and contact dietician.
9ecord patients &eight &eel!.
"atients head and shoulders should be elevated appro@ 30oto
reduce ris of aspiration &hilst feeding is in under&a!.
6aintain nasal h!giene and mouthcare.
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age &%of &'
-
7/25/2019 jurnal NGT komplitt
28/31
"ppendi$ &
N"6G"T#!* TU-E P"TEN*@ *E*A EET"atient sticer
Practice notef p, M 5.5 do not use tube%spirate again 30 minutes laterf p, remains M5.5# inform medical team and refer to Trust NG tube guidelines
D"TEB . .
T6( 00- 0*- 0)- 03- 0=- 05- 04- 0- 0
-
7/25/2019 jurnal NGT komplitt
29/31
"ppendi$ & cont
Euipment #ecord
Date.Time pecific euipment Date euipment ignaturereuired and ordered received
EvaluationDate.Time Evaluation ignature
-
7/25/2019 jurnal NGT komplitt
30/31
The insertion of Nasogastric NG/ tubes# management of feeds and administration of medicines
via an NG tube or via a "ercutaneous (ndoscopic Gastric tube "(G/ in adults "age &+of &'
-
7/25/2019 jurnal NGT komplitt
31/31
"ppendi$ +
*ompetency assessment sheet for registered health care practitionersfor the insertion of a fine bore Nasogastric (NG) tube
Name of practitionerB 0000000000000000000000000000 Cor1 locationB 000000000000000000000000000000
"imB To ensure that all practitioners are competent to pass a fine bore NG tube as per the Trustguidelines.
7earning ob>ectives are as follo8snderstanding of the legal and ethical issues of NG feeding
nderstand the procedure in detail$emonstrate the safe insertion and placement of an NG tube
Training reuiredB attendance at a training session or via e-learning on subDect area
"ssessmentB abilit! to full! meet obDectives and complete an observed successful NG tubeinsertion
Underpinning 1no8ledge
To discuss and understand the legal and ethical issues related to NG tube feedingTo discuss and understand the Nutritional guidelines
To e@plain the factors &hich need consideration before undertaing the procedureTo identif! all necessar! e1uipment re1uired for the procedure
To discuss and understand the importance of establishing correct tube placement prior to andduring feedingTo demonstrate correct techni1ues to aspirate the tubeTo identif! ris factors and to the appropriate action to be taen to maintain patient safet!
! confirm that the above named healthcare practitioner has successfully completed theassessment of competence reuired for this procedure as detailed above
ignedB Print nameB
DateB DesignationB
NB:A registered healthcare practitioner who has already achieved competence in thisarea of practice is able to confirm the competence of another healthcare practitioner in thisskill or a specialist practitioner in nutritional care or another suitably qualified individual in
an educational field.