Journal of Orthopaedics, Trauma and Rehabilitation
4
Case Report Non-union of Fracture of Distal Radius: A Case Report and Literature Review 橈骨遠端骨折不連合:一個病例報告和文獻回顧 Koo Siu-Cheong Jeffrey Justin * , Ho Sheung-Tung Department of Orthopaedic and Traumatology, Caritus Medical Centre, Hong Kong article info Article history: Accepted January 2010 Keywords: distal radius fracture fracture non-union abstract Non-union of distal radius fracture is uncommon. Promising results in dorsally displaced fractures of distal radius were reported with the use of volar fixed-angle fixation. We report about a 75-year-old woman with non-union of distal radius, treated successfully by using volar locking compression plate. 中 文 摘 要 橈骨遠端骨折不連合並不常見。有文獻敘述利用掌側固定角度接合骨板作內固定術,對於背側移位的橈骨遠 端骨折不連合,治療效果良好。本報告敍述一名 75歲女仕的成功案例,利用鎖定加壓固定角度接骨板作為橈 骨末端骨折不連合之治療方法。 Case Report A 75-year-old right-handed woman sustained a fall that resulted in closed distal radius and ulna fractures of left wrist. She had closed reduction and short arm plaster cast applied in another hospital. However, closed reduction failed (Figure 1), but she refused surgical treatment. Five months later, she had persistent left wrist pain and hand numbness. Physical examination showed severe radial deviation and z- deformity of her left wrist (Figure 2). The fingers were stiff with flexion contracture at the metacarpophalangeal and distal interpha- langeal joints. There was marked shortening of left radius. The left wrist motion was 5 dorsiflexion, 40 palmar flexion, 45 pronation, and 50 supination. The handgrip and pinch grip were 9% (1 kg vs. 11 kg) and 29% (1 kg vs. 3.5 kg) of the contralateral side, respectively. She could not make a fist and hold a bowl with her left hand. X-rays showed that there was non-union of distal radius frac- ture, with distal fragment being radially and dorsally displaced. The distal ulna was mal-united, but the length was preserved, resulting in ulna positive variance with 1-cm difference in length. Open reduction and internal fixation were performed by means of volar approach. Intra-operative findings showed pseudoarthrosis of the distal radius fracture. The distal end of proximal fragment caused compression of median nerve in carpal tunnel. There were also adhesions and attrition rupture of flexor digitorum profundus to middle and ring fingers. Excision of the pseudoarthrosis, shortening of proximal radial fragment by 1 cm, and distraction with small Albeitgemeinshaft fur osteosynthenfragen/Association for the study of internal fixation (AO/ASIF) external fixator were performed to realign the fracture. The fracture was fixed with contoured 3.5-mm locking compression plate (Synthes AG Chur). Distal radio-ulnar joint was realigned by ulnar shortening osteotomy for 1 cm over the mid-shaft of ulna, which was fixed with 3.5-mm dynamic compression plate (Figure 3). Resected bone from both proximal radial fragment and ulnar shortening osteotomy was used as bone graft at the pseudoarthrosis. Lengthening of the brachioradialis and flexor carpi radialis tendon and arthrolysis of dorsal radiocarpal and/or volar distal radio-ulnar joint were not required. Flexor tendon tenolysis was carried out to improve the finger passive movement. Carpal tunnel release was performed to relieve the median nerve compression at carpal tunnel. The rupture of flexor digitorum profundus to middle and ring fingers was not repaired and was planned for later reconstruction after regain of passive range of movement. The external fixator was retained to protect the fixation and was removed 3 weeks later because of pin loosening. Short arm plaster cast was applied for another 4 weeks. The fracture united at 4 months after the operation. At 40 months after operation, the wrist motion was improved with 25 dorsi- flexion, 40 palmar flexion, 90 pronation, 90 supination, 30 radial deviation, and 10 ulnar deviation. The handgrip and pinch grip were 56.5% (13 kg vs. 23 kg) and 80% (4 kg vs. 5 kg) of contralateral side, respectively. Despite rigorous mobilisation, there was only modest improvement in finger stiffness; hence, it was decided not to * Corresponding author. E-mail: [email protected]. Contents lists available at ScienceDirect Journal of Orthopaedics, Trauma and Rehabilitation Journal homepages: www.e-jotr.com & www.ejotr.org 2210-4917/$ e see front matter Copyright Ó 2011, The Hong Kong Orthopaedic Association and Hong Kong College of Orthopaedic Surgeons. Published by Elsevier (Singapore) Pte Ltd. All rights reserved. doi:10.1016/j.jotr.2010.11.004 Journal of Orthopaedics, Trauma and Rehabilitation 15 (2011) 21e24
Transcript of Journal of Orthopaedics, Trauma and Rehabilitation

Case Report
Non-union of Fracture of Distal Radius: A Case Report and Literature Review橈骨遠端骨折不連合:一個病例報告和文獻回顧
Koo Siu-Cheong Jeffrey Justin*, Ho Sheung-TungDepartment of Orthopaedic and Traumatology, Caritus Medical Centre, Hong Kong
a r t i c l e i n f o
Article history:Accepted January 2010
Keywords:distal radius fracturefracturenon-union
a b s t r a c t
Non-union of distal radius fracture is uncommon. Promising results in dorsally displaced fractures ofdistal radius were reported with the use of volar fixed-angle fixation. We report about a 75-year-oldwoman with non-union of distal radius, treated successfully by using volar locking compression plate.
中 文 摘 要
橈骨遠端骨折不連合並不常見。有文獻敘述利用掌側固定角度接合骨板作內固定術,對於背側移位的橈骨遠
端骨折不連合,治療效果良好。本報告敍述一名 75歲女仕的成功案例,利用鎖定加壓固定角度接骨板作為橈
骨末端骨折不連合之治療方法。
Case Report
A 75-year-old right-handedwoman sustained a fall that resultedin closed distal radius and ulna fractures of left wrist. She hadclosed reduction and short arm plaster cast applied in anotherhospital. However, closed reduction failed (Figure 1), but sherefused surgical treatment. Five months later, she had persistentleft wrist pain and hand numbness.
Physical examination showed severe radial deviation and z-deformity of her left wrist (Figure 2). The fingers were stiff withflexion contracture at the metacarpophalangeal and distal interpha-langeal joints. There was marked shortening of left radius. The leftwrist motionwas 5� dorsiflexion, 40� palmar flexion, 45� pronation,and 50� supination. The handgrip and pinch grip were 9% (1 kg vs.11 kg) and 29% (1 kg vs. 3.5 kg) of the contralateral side, respectively.She could not make a fist and hold a bowl with her left hand.
X-rays showed that there was non-union of distal radius frac-ture, with distal fragment being radially and dorsally displaced. Thedistal ulna was mal-united, but the length was preserved, resultingin ulna positive variance with 1-cm difference in length.
Open reduction and internal fixation were performed by meansof volar approach. Intra-operative findings showed pseudoarthrosisof the distal radius fracture. The distal end of proximal fragmentcaused compression of median nerve in carpal tunnel. There werealso adhesions and attrition rupture of flexor digitorum profundusto middle and ring fingers.
Excision of the pseudoarthrosis, shortening of proximal radialfragment by 1 cm, and distraction with small Albeitgemeinshaft furosteosynthenfragen/Association for the study of internal fixation(AO/ASIF) external fixator were performed to realign the fracture.The fracture was fixed with contoured 3.5-mm locking compressionplate (Synthes AG Chur). Distal radio-ulnar joint was realigned byulnar shortening osteotomy for 1 cm over the mid-shaft of ulna,whichwas fixedwith 3.5-mmdynamic compression plate (Figure 3).Resected bone from both proximal radial fragment and ulnarshortening osteotomywas used as bone graft at the pseudoarthrosis.Lengthening of the brachioradialis and flexor carpi radialis tendonand arthrolysis of dorsal radiocarpal and/or volar distal radio-ulnarjoint were not required.
Flexor tendon tenolysis was carried out to improve the fingerpassive movement. Carpal tunnel release was performed to relievethe median nerve compression at carpal tunnel. The rupture offlexor digitorum profundus to middle and ring fingers was notrepaired and was planned for later reconstruction after regain ofpassive range of movement. The external fixator was retained toprotect the fixation and was removed 3 weeks later because of pinloosening. Short arm plaster cast was applied for another 4 weeks.
The fractureunited at 4months after the operation. At 40monthsafter operation, the wrist motion was improved with 25� dorsi-flexion, 40� palmarflexion, 90� pronation, 90� supination, 30� radialdeviation, and 10� ulnar deviation. The handgrip and pinch gripwere 56.5% (13 kg vs. 23 kg) and 80% (4 kg vs. 5 kg) of contralateralside, respectively. Despite rigorous mobilisation, there was onlymodest improvement infinger stiffness; hence, itwasdecidednot to* Corresponding author. E-mail: [email protected].
Contents lists available at ScienceDirect
Journal of Orthopaedics, Trauma and Rehabilitation
Journal homepages: www.e- jotr .com & www.ejotr .org
2210-4917/$ e see front matter Copyright � 2011, The Hong Kong Orthopaedic Association and Hong Kong College of Orthopaedic Surgeons. Published by Elsevier (Singapore) Pte Ltd. All rights reserved.doi:10.1016/j.jotr.2010.11.004
Journal of Orthopaedics, Trauma and Rehabilitation 15 (2011) 21e24

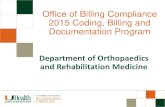
Figure 1. X-ray of left wrist showed extra-articular fracture of distal radius and distal ulna fracture, both in acute injury and non-union.
Figure 2. Clinical photo showing (A) dorsal side and (B) volar side of left wrist. Left wrist was in severe radial deviation and z-deformity. (C) Fingers showing flexion contracture atmetacarpophalangeal and distal interphalangeal joints.
S.-C.J.J. Koo, S.-T. Ho / Journal of Orthopaedics, Trauma and Rehabilitation 15 (2011) 21e2422

reconstruct the flexor tendon rupture. The distal radio-ulnar jointdid functionwell with good forearm painless rotation. According tothe rating of Fernandez et al,1 the patient had good clinical result.There was no wrist or distal radio-ulnar joint pain.
Discussion
For distal radius fracture, non-union is arbitrarily defined as nobony union at 6months after the injury.1e3However, the presence ofpseudoarthrosis confirmed thenon-unionof distal radius fracture asin our patient, though the time interval from injury was 5 months.
The incidence was 0.2% according to New York State Worker’sCompensation Board.4 There were about 60 cases reported in theEnglish literature.1,3,5e10 The low incidence of non-union of distalradius fractures is probably because of the impaction of fracturefragment during the injury, the metaphyseal location, and lesserdegree of soft tissue disruption in low-energy falls.5
Several contributing factors had been elaborated, including thefollowing: concomitant distal ulnar fracture reduces the stability ofthe distal radius fracture and causes increased motion at the frac-ture;5,11 inadequate immobilisation; inadequate fixation or exces-sive distraction during application of external fixator or pins andplaster;11e13 some medical conditions such as heavy smoking,
alcohol abuse6 and peripheral neuropahty in diabetes mellitus alsocontribute to distal radius fracture non-union. In our patient, thenon-union might have been caused by the concomitant distal ulnarshaft fracture, the failure of apposition of the fracture fragments,and an inadequate period of immobilisation.
The results of operation to regainunionof distal radius fracture areunpredictable.11 The aims of treatment for non-union of distal radiusfracture are correction of deformity, providing solid fixation to ach-ieve a solid union and well-aligned wrist with preservation of wristmotion. Operative options included open reduction and internalfixation or wrist arthrodesis. Wrist arthrodesis was advocated forinfirm patients with low functional demand or was used as a salvageprocedure after failed attempts to gain union.10 Some authors advo-cated wrist arthrodesis as a primary procedure for non-union asso-ciated with concomitant distal ulnar fracture.5 Some recommended5-mm subchrondral bone stock in distal radius fragment as a guide-line for choosing between internal fixation and wrist arthrodesis.3
A dorsal approach is used when there was dorsal displacementor angulation of the distal fragment and vice versa.1 Volarapproach is usually preferred as there is less irritation or damageto overlying tendons when compared with that by dorsalapproach.1 A variety of fixation methods were reported withsuccessful results,1,3,6,11,12 such as the volarly placed fixed-angle
Figure 3. X-ray of left forearm immediately after the operation and at 4 months post-operation. Both distal radius fracture and ulna osteotomy site were healed.
S.-C.J.J. Koo, S.-T. Ho / Journal of Orthopaedics, Trauma and Rehabilitation 15 (2011) 21e24 23

device in osteoporotic bone based on biomechanical study andpromising clinical experiences10,14,15 and placement of two platesin orthogonal plane, that is, the ulnar and radial columns of thedistal radius for small distal radius fragments.10,16
The successful union rate for internal fixation in the reportedseries is 90%, with a range from 60% to 100% (Table). The averagerange of motion in flexion-extension arc, pronation-supination arc,radio-ulnar deviation arc, and grip strength, were 91.5�, 139�, 38.7�,and 67.5%, respectively.
In summary, non-union of distal radius fracture is rare. Carefullyplanned open reduction and fixation can help to achieve rapid boneunion with satisfactory functional outcome.
References
1. Fernandez DL, Ring D, Jupiter JB. Surgical management of delayed union andnonunion of distal radius fractures. J Hand Surg 2001;26A:201e9.
2. Chapman MW. Principles of treatment of non-unions and malunions. In:Chapman MW, editor. Chapman’s Orthopedic Surgery. 3rd edition. LippincottWilliams and Wilkins; 2001. p. 847e66.
3. Segalman KA, Clark GL. Un-united fractures of the distal radius. A report of 12cases. J Hand Surg 1998;23A:914e8.
4. Bacorn RW, Kurtzke JF. Colle’s fracture. A study of two thousand cases from theNew York State Workmen’s Compensation Board. J Bone Joint Surg 1953;35A:643e58.
5. McKee MD, Waddell JP. Non-union of distal radial fractures associated withdistal ulnar shaft fractures: a report of four cases. J Orthop Trauma 1997;11:49e53.
6. Smith VA, Wright TW. Nonunion of the distal radius. J Hand Surg 1999;24B:601e3.
7. Eglseder Jr WA, Elliott MJ. Non-union of the distal radius. Am J Orthop 2002;31:259e62.
8. Harper WM, Jones JM. Non-union of Colle’s fracture: report of 2 cases. J HandSurg 1990;15B:121e3.
9. Kwa S, Tonkin MA. Nonunion of a distal radial fracture in a healthy child. J HandSurg 1997;22B:175e7.
10. Ring D, Jupiter JB. Nonunion of the distal radius. Tech Hand Up Extrem Surg2002;6:6e9.
11. Prommersberger KJ, Fernandez DL. Non-union of distal radius fractures. ClinOrthop 2004;419:51e6.
12. Prommersberger KJ, Fernandez DL, Ring D, et al. Open reduction and internalfixation of un-united fractures of the distal radius: does the size of the distalfragment affect the result? Chir Main 2002;21:113e23.
13. Kaempffe FA, Wheeler DR, Peimer CA, et al. Severe fractures of the distalradius: effect of amount and duration of external fixator distraction onoutcome. J Hand Surg 1993;18A:33e47.
14. Orbay JL, Fernandez DL. Volar fixation for dorsally displaced fractures of thedistal radius: a preliminary report. J Hand Surg 2002;27A:205e15.
15. Leung F, Zhu L, Ho H, et al. Palmar plate fixation of AO type C2 fracture of distalradius using a locking plateda biomechanical study in a cadaveric model.J Hand Surg 2003;28B:263e6.
16. Jakob M, Rikli DA, Regazzoni P. Fractures of the distal radius treated by internalfixation and early function. A prospective study of 73 consecutive patients.J Bone Joint Surg 2000;82B:340e4.
TableFunctional results after operation in various studies1,7,11,12
Authors No. of pt. FU length % Fracture union F/E arc P/S arc RD/UD arc Grip % Satisfactory result
Fernandez et al1 10 40 10/10 105 145 34 73 7/10Eglseder and Elliott7 10 19 8/10 88 131 e 71 e
Prommersberg et al12 23 22 22/23 87 139 40.7 62.5 17/23
Pt¼ patients; FU length¼ follow-up length in months; F/E¼ flexion to extension; P/S¼ pronation to supination; RD/UD¼ radial to ulnar deviation; grip %¼ % strength of thenormal side.
S.-C.J.J. Koo, S.-T. Ho / Journal of Orthopaedics, Trauma and Rehabilitation 15 (2011) 21e2424