
JOURNAL OF OCCUPATIONAL SAFETY AND HEALTH€¦ · By Gan Chun Chet, MSc (UK), BSc (Hons) (UK), Peng...
72
JOURNAL OF OCCUPATIONAL SAFETY AND HEALTH National Institute of Occupational Safety and Health National Institute of Occupational Safety and Health (NIOSH) Ministry of Human Resources Malaysia December 2013, Vol 10, No. 2 ISSN 1675-5456 PP13199/12/2012(032005)
Transcript of JOURNAL OF OCCUPATIONAL SAFETY AND HEALTH€¦ · By Gan Chun Chet, MSc (UK), BSc (Hons) (UK), Peng...
-
JOURNAL OFOCCUPATIONALSAFETY AND HEALTH
National Institute of Occupational Safety and Health
National Institute of Occupational Safety and Health (NIOSH)Ministry of Human Resources Malaysia
December 2013, Vol 10, No. 2ISSN 1675-5456PP13199/12/2012(032005)
-
Journal of OccupationalSafety and Health
Editor-in-chiefIr. Haji Rosli bin Hussin
Executive DirectorNIOSH, Malaysia
Secretariat
Editorial Board
Prof. Dr. Krishna Gopal RampalUniversiti Kebangsaan Malaysia
NIOSH, MalaysiaIr. Daud Sulaiman
Fadzil OsmanNIOSH, MalaysiaRaemy Md. ZeinNIOSH, Malaysia
The Journal
- Aims to serve as a forum for the sharing of research findings and information across broad areas in Occupational Safety and Health. - Publishes original research reports, topical article reviews, book reviews, case reports, short communications, invited editorial and letters to editor. - Welcomes articles in Occupational Safety and Health related fields.
Associate Editors
Prof. Dr. Ismail BahriUniversiti Kebangsaan MalaysiaDr. Jeffereli Shamsul BahrinBASF East Asia Regional Headquartes Ltd.Dr. Abu Hasan SamadPrince Court Medical Centre
Mohd Rashidi RohmadRoslina Md HusinNor Akmar Yussuf
-
i
December 2013 Vol.10 No.2
Contents
Journal of Occupational Safety and Health
1. The Origin of Workers Hearing Level – A Finding Based on Chances of OccurrenceBy Gan Chun Chet, MSc (UK), BSc (Hons) (UK), Peng
2. Occupational Lung Carcinogens and Factors in Relation to Lung Cancer RiskFauziah Nordin1,3, Richard Booton2, Paul O’Donnell2, Philip Barber2, Andrew Povey1 1Centre for Occupational & Environmental Health, Faculty of Medical & Human Sciences, The University of Manchester, United Kingdom 2North West Lung Centre, Wythenshawe Hospital, Manchester, United Kingdom 3Institute for Public Health, Ministry of Health Malaysia, WP Kuala Lumpur, MalaysiaCorresponding author:Dr Fauziah Nordin,Institute for Public Health,Ministry of Health Malaysia,Jalan Bangsar, 50590 WP Kuala Lumpur,Malaysia(Tel: +60322979400, Fax: +60322823114, email: [email protected])
3. OHSAS 18001 and MS 1722 Certification Initiatives Prove the Commitment to SustainabilityWai Onn HongProcessing Department, Genting Plantations Berhad,10th Floor, Wisma Genting, Jalan Sultan Ismail, Kuala Lumpur, MalaysiaTel: +60 3 2333 6506 Fax: + 60 3 2161 9689 Email: [email protected]
4. The Extent of Predictability of Noise-Induced Problems – A Cross-Over from the Healthy Limit to Off-Limit ConditionsBy Ir. Gan Chun ChetMSc (UK), BSc (Hons) (UK), PEng
5. Prevalence Of Work Related Musculoskeletal Disorder Among Port Workers: Quantitative Analysis At The Physiotherapy Centre Of Malaysian Shipping Industry, SelangorIzham Zain¹, Azrul Anuar¹, Asrina Asri¹, Shamsul Azhar²¹ KPJ Healthcare University College² Physiotherapy Department, Malaysia Shipping Industry, SelangorCorresponding author: [email protected]
1 - 11
13 - 25
27 - 36
37 - 50
51 - 66
-
This page has been intentionally left blank
-
Journal of Occupational Safety and Health
1 1
The Origin of Workers Hearing Level – A Finding Based on
Chances of Occurrence
By Gan Chun Chet, MSc (UK), BSc (Hons) (UK), Peng
_____________________________________________________________________
Abstract
The paper writes on the possible origin of off-limit cases found in a noise
project conducted internally in a factory in Malaysia. Out of 691 sampled workers’
that attended audiometric test results (some repeated), it was found that the mode of
hearing ability is between 20 to 30 dB depending on individual worker’s age ranging
from 20 to 55 years. Out of the total results, approximately 100 workers are above a
limit defined here in this paper as the off-limit condition. The chance of a worker
originating from a good condition to an unhealthy condition is about 1 percent. The
data are tabulated to show that a sway pattern could be an explanation of workers’
origin. Although the data is profound, there is no evidence of a trace due to a short
test period. Possibilities are highlight here to outline the severity of a cross over to the
unhealthy condition (here defined as the off-limit condition). Some advises are
mentioned here with individual susceptibility on the matter though there is no data to
substantiate. Further findings are required to show a trace. In conclusion, the severity
is highlight. A chart, developed to know the limits of hearing ability, is illustrated
based the findings.
_____________________________________________________________________
Introduction
Scientific data induced to formulate a theory or depicted from an observation
and subsequently utilizing an existing theory to explain a fact, are used as a base for
an answer or a comparison. However, scientific disillusionment exists, drawing from
the base of data in question where different views exist from the same set of
observations. While scientific breakthroughs are remarkable yet a theory is falsifiable
if other research is concluded differently. This leave a myth to the underlying truth
based on the truth of facts due to a possible change in a hypothetical assumption or a
change in a theory, etc. Is this possible?
The following are findings of a real case on noise induced problems in a
factory. The trace of historical origin of these workers’ hearing ability is unknown.
The data is profound because it shows the actual truth but unknown to others. After
going through the analysis, my personal opinion is that the truth lies within these
individuals. Here defined the off limit cases (red line) as shown in the diagram below,
-
Journal of Occupational Safety and Health
2 2
grids with utterly puzzled and astonished findings. A possible explanation to the
situation is that sway pattern might had happened and a possible origin based on the
possibilities might be the explanation. This article tries to uncover the origin of their
hearing abilities based on the chances of occurrence in each of the sway pattern are
illustrated in the sections.
Background of the Research Data
The total number of workers attended the test, including repeated cases,
amounts to 691 in number. The hearing abilities of the workers are checked using an
audiogram by an independent test company. The workers average hearing abilities at
500, 1000, 2000 and 3000Hz were plotted against age; regardless of the number of
year of service with the company. This is shown in graph 1 (Right Ear). This article
investigates the possible origin of hearing ability of Right Ear when they are at the
age of 16 to 20 years old (started and joined the industry). Some of these workers
discovered at later age that they had hearing problem. The findings found that about
10 – 16 percent of the workers are able to hear loud noises (possibly with hearing
impaired). Regardless of the area noise in this factory or area noise in previous
company, the graph below shows their hearing abilities.
Graph 1 : Workers Hearing
Abilities (Right Ear Only)
-
Journal of Occupational Safety and Health
3 3
Methodology
The method is based on possible sway patterns of a worker that might not have
eluded noisy area. However, a worker might be employed with a noise problem.
Unfortunately nearing to the end of employment, between the age of 40 to 55,
problems were noticed. This is shown in the graph. It is thoughtful to know but the
actual origin (occurrence) cannot be traced. Possibly these patterns exists, as shown in
the graph below (2 to 6). The possible path called the “sway patterns”. In the diagram
below, the ability either started off from a healthy condition or an off limit condition.
Both these conditions are the possible origin. At the end of employment is here called
the “end destination” of a sway pattern. The numbers of off limit cases were counted
to calculate the possible occurrences shown in a grid matrix below. The findings are
as shown in the next section.
2
grids with utterly puzzled and astonished findings. A possible explanation to the
situation is that sway pattern might had happened and a possible origin based on the
possibilities might be the explanation. This article tries to uncover the origin of their
hearing abilities based on the chances of occurrence in each of the sway pattern are
illustrated in the sections.
Background of the Research Data
The total number of workers attended the test, including repeated cases,
amounts to 691 in number. The hearing abilities of the workers are checked using an
audiogram by an independent test company. The workers average hearing abilities at
500, 1000, 2000 and 3000Hz were plotted against age; regardless of the number of
year of service with the company. This is shown in graph 1 (Right Ear). This article
investigates the possible origin of hearing ability of Right Ear when they are at the
age of 16 to 20 years old (started and joined the industry). Some of these workers
discovered at later age that they had hearing problem. The findings found that about
10 – 16 percent of the workers are able to hear loud noises (possibly with hearing
impaired). Regardless of the area noise in this factory or area noise in previous
company, the graph below shows their hearing abilities.
Graph 1 : Workers Hearing
Abilities (Right Ear Only)
-
Journal of Occupational Safety and Health
4
4
Category 3
Category 2
Category 1
A B C
2
Graph 3 : From Category 3 (Sheet 2)
Category 3
Category 2
Category 1
A B C
1
Very rare Graph 2 : From Individual Categories (Category 1, 2 or 3) (Sheet 1)
Category 3 : Caution Level Category 2 : Healthy Level Category 1 : Very Good Level
Category 3 : Caution Level Category 2 : Healthy Level Category 1 : Very Good Level
-
Journal of Occupational Safety and Health
5
5
Category 3
Category 2
Category 1
A B C
3
Graph 4 : From Category 2 (Sheet 3)
Category 3 : Caution Level Category 2 : Healthy Level Category 1 : Very Good Level
Category 3 : Caution Level Category 2 : Healthy Level Category 1 : Very Good Level
A B C
4
Graph 5 : From Category 1 (Sheet 4)
-
Journal of Occupational Safety and Health
6
6
Findings
The following are the findings from graph 2 to 6. The numbers of hearing
ability in each of the possible pattern are counted. This is tabulated in table 1 below.
Separated by “below 10 counts”, “10 to 19 counts” and “above or equal to 20 counts”,
most of these workers are in the two circles shown the table below.
The most probable occurrence is 40 cases as defined here by the count of
occurrences above the limit (red line), could originated from Category 2 and swayed
to C. The second most probable occurrence is 38, with the origin from Category 1 and
the end destination is C. The probable occurrences are tabulate in table 2 together
Category 3
Category 2
Category 1
Very low level Graph 6: From Off Limit (Sheet 5)
-
Journal of Occupational Safety and Health
7 7
with the number of occurrences in descending order. The high chances of origin
shown in the table might have originated from Category 1 or 2 defined here applicable
to this situation.
Discussion
The numbers shows the count in each of the pattern. It does not tell that a
person hearing ability originated from a point above the off limit condition or from
any point on the Y-axis of the graphs (2 to 6). In addition, it is not possible to say that
a person will move to a point with certainty after exposure to noise years later. It is to
note that a sway of a possible situation might have originated from these defined
limits, with the possibility that each of the condition is considered independent from
each other.
The pattern cannot compute specifically which employee has a good hearing
ability and later have a problem at the age of 40 to 50. Neither does the pattern shows
that a person in a good condition, as defined, ended up with a problem due to noise
problem in the plant. The patterns are the possibilities of an origin by the count of
occurrence in the sway pattern.
By counting the possibility of an occurrence, out of an estimate off limit cases
with reference to the mode occurrence, the chance on one person originated from
either side of the limit is approximately 1 percent. Out of the number of workers (691
records), about 109 records a fifty fifty chance on either sides. Half of which might be
healthy, with an increment of approximately 1 percent on an addition case.
The Development of A Chart Defining the Possibilities of An Origin
The chart as shown below represents and shows the origin in a graphical form.
It could be used as to explain a point of reference origin in this situation.
6
Findings
The following are the findings from graph 2 to 6. The numbers of hearing
ability in each of the possible pattern are counted. This is tabulated in table 1 below.
Separated by “below 10 counts”, “10 to 19 counts” and “above or equal to 20 counts”,
most of these workers are in the two circles shown the table below.
The most probable occurrence is 40 cases as defined here by the count of
occurrences above the limit (red line), could originated from Category 2 and swayed
to C. The second most probable occurrence is 38, with the origin from Category 1 and
the end destination is C. The probable occurrences are tabulate in table 2 together
Category 3
Category 2
Category 1
Very low level Graph 6: From Off Limit (Sheet 5)
-
Journal of Occupational Safety and Health
8 8
Category Possibly From The Following Sound Limit
Off Limit 21 and 40 dB
Category 3 17 to 20 dB
Category 2 13 to 16 dB
Category 1 9 to 12 dB
Low Level Less than 8dB!
Category of age range
[O] – 16 to 20 years old
[A] – 30 to 40 years old
[B] – 40 to 50 years old
[C] – 50 to 60 years old
[D] – More than 60
Diagram 1: A Pattern that is to Be Avoided
From
Category 3
Category 2
Category 1 10
20
View 1
Off Limit
A
Age
40
0
10
20
0
30 40
0
50 60
B C D O Noise, dB
See View
1
To
Limit
-
Journal of Occupational Safety and Health
9 9
The shaded area, as shown in the graphic above, shows the sway pattern of a
worker from healthy condition (below the red line) to either [A], [B] or [C]. This is to
be avoided. The [O]s are unknown condition as the problem occurs at a very early
age. The [D] end destination are old or elderly people.
The hearing level should be below the limit by avoiding exposure to unwanted
sound.
• Some Advises regarding Noise Problem Based on this Situation
Different factory conditions will have different impact on the workers. The
hearing ability of every worker is different, whether they are new or an existing
worker. A few advises as listed below.
Opinion alone not substantiated by data is not real. A change in theory is a
change of a hypothetical question forming a paradox. In this case, the origin of
workers noise level, based by factual data by the count of workers falling in the sub-
diagram, is in fact forming a set of suggestions and fitting it into the box.
In this article, it is only to suggest that there might be possibilities that the off
limit workers might have came from an off limit condition or a healthy condition
(whether Category 1 then Category 2, etc) in the order. It is difficult to conclude that
this is where the workers condition came from.
Disclaiming the facts, that workers are from healthy condition and the cause of
their hearing disability is from the plant, the point of origin cannot be traced exactly.
In fact, in my opinion, it can only be know of possible origins. This is only one plant
that encountered this problem. What about others? The truth lies in the workers
themselves.
8
Category Possibly From The Following Sound Limit
Off Limit 21 and 40 dB
Category 3 17 to 20 dB
Category 2 13 to 16 dB
Category 1 9 to 12 dB
Low Level Less than 8dB!
Category of age range
[O] – 16 to 20 years old
[A] – 30 to 40 years old
[B] – 40 to 50 years old
[C] – 50 to 60 years old
[D] – More than 60
Diagram 1: A Pattern that is to Be Avoided
From
Category 3
Category 2
Category 1 10
20
View 1
Off Limit
A
Age
40
0
10
20
0
30 40
0
50 60
B C D O Noise, dB
See View
1
To
Limit
-
Journal of Occupational Safety and Health
10 10
The Line below the Limit (Red Line)
The conditions below the limit are healthy conditions. This line is drawn based
on the majority of the workers being below this limit in clusters due to employment
years shown in graph 1. The general view shows that the workers are healthy below
the red line in the diagram below. The equation to this line is calculated. With this
line, different factors to categorize healthy workers are possible, with a caution region
to warn the workers that the condition might cross above the limit. If this happens,
then the group will be in the possible pattern of origin as highlighted in this article.
Ideally, workers should come in healthy and maintain a healthy condition at
later stage of their employment. Noise induced problems are caused by prolong
exposure of unwanted sound into the ear. Age related losses might be the reason for
the increased in hearing ability of the workers at later age. The problem about noise is
that if it is detected will cause a failure in hearing ability. If it is purely due to age
related reasons, as already known, then the reason of workers moving up to a new
level of hearing ability is due to an over exposure can be identify, assuming that there
is no disease to the ears or other medical reasons linked to this, which requires
qualified medical practitioner to inform and a cure.
The plot of audiometric results shows the location of a person hearing level.
The results from the workers in the graph above (graph 1) show remarkable truth in it.
Worker’s Age (Year)
20
dB
30
dB
20 60
10
dB
30 40 50
Normal Hearing
Ability
Category 3
Category 2
Category 1
Category 1 : Very Good
Category 2 : Good
Category 3 : Caution
Chart 1: A Noise Chart of Healthy Workers
-
Journal of Occupational Safety and Health
11 11
The inadequacy of health information might be the reason to a high number of off
limit cases. It is might be only known at that instant of time that the ears have been
affected that medical examiners are only able to comfort these patience. It might be
that the workers are not aware of the problem and have caused a shift in hearing.
How is it possible to trace the point of origin at a test or a series of test within
the short time frame? If an earlier test was conducted, there might be able to locate the
origin, subject also to age related losses and other unknown factors like susceptibility,
etc. In this article, it is stated by rough approximation that the count of numbers in the
pattern of possible sway from the start of employment might have happened.
Otherwise, without the count, it is just a guess.
In Conclusion
The purpose of the article is to highlight the severity of the problem. Noise
induced problem should be avoided. From a layman point of view, it is advised to
consult an expert in this area or an ear specialist should problem arise.
Please note that the off limit in this article is based on the general mode limit
of a plant. It does not mean that it is applicable to other situations. Please refer to an
ear consultant for medical advice for the permissible levels.
(Note : The data is also key in by the author to analyze the problem)
The author expresses his personal opinions on the above out of interest to the topic and
indemnifies himself from the readers for any charges. It is not to depict any information from
this article and is only to be referred to a qualified medical practitioner for expert advice if a
problem is encountered. The article writes on the possible origin based on data collected to
help other to avoid a hearing problem.
Author Contact:
Info to Reviewer:
Qualifications:
MSc (UK), University of Manchester Institute of Science and Technology in Operations
Management
BSc (Hons) (UK), University of Manchester in Mechanical Engineering
Professional Registration:
PEng Registration, Board of Engineers Malaysia, Mechanical Branch (Registration No.
12539)
10
The Line below the Limit (Red Line)
The conditions below the limit are healthy conditions. This line is drawn based
on the majority of the workers being below this limit in clusters due to employment
years shown in graph 1. The general view shows that the workers are healthy below
the red line in the diagram below. The equation to this line is calculated. With this
line, different factors to categorize healthy workers are possible, with a caution region
to warn the workers that the condition might cross above the limit. If this happens,
then the group will be in the possible pattern of origin as highlighted in this article.
Ideally, workers should come in healthy and maintain a healthy condition at
later stage of their employment. Noise induced problems are caused by prolong
exposure of unwanted sound into the ear. Age related losses might be the reason for
the increased in hearing ability of the workers at later age. The problem about noise is
that if it is detected will cause a failure in hearing ability. If it is purely due to age
related reasons, as already known, then the reason of workers moving up to a new
level of hearing ability is due to an over exposure can be identify, assuming that there
is no disease to the ears or other medical reasons linked to this, which requires
qualified medical practitioner to inform and a cure.
The plot of audiometric results shows the location of a person hearing level.
The results from the workers in the graph above (graph 1) show remarkable truth in it.
Worker’s Age (Year)
20
dB
30
dB
20 60
10
dB
30 40 50
Normal Hearing
Ability
Category 3
Category 2
Category 1
Category 1 : Very Good
Category 2 : Good
Category 3 : Caution
Chart 1: A Noise Chart of Healthy Workers
-
This page has been intentionally left blank
-
Journal of Occupational Safety and Health
13
Occupational Lung Carcinogens and Factors in Relation to Lung
Cancer Risk
Fauziah Nordin
1,3, Richard Booton
2, Paul O’Donnell
2, Philip Barber
2, Andrew Povey
1
1Centre for Occupational & Environmental Health, Faculty of Medical & Human Sciences, The
University of Manchester, United Kingdom 2North West Lung Centre, Wythenshawe Hospital,
Manchester, United Kingdom 3Institute for Public Health, Ministry of Health Malaysia, WP Kuala
Lumpur, Malaysia
Corresponding author:
Dr Fauziah Nordin,
Institute for Public Health,
Ministry of Health Malaysia,
Jalan Bangsar, 50590 WP Kuala Lumpur,
Malaysia
(Tel: +60322979400, Fax: +60322823114, email: [email protected] )
_______________________________________________________________________________
Abstract
Introduction:
Although smoking is the most important cause of lung cancer, occupational factors can also play
an important role. Worldwide, approximately 10% of lung cancer deaths in men (88,000 deaths)
and 5% in women (14,300 deaths) were attributable to exposure to occupational carcinogens,
referred to the report on the global burden of disease due to occupational carcinogens
Methods:
We examined the risks associated with occupational exposures in a case-referent study of lung
cancer that was carried out between November 1998 to March 2000. Cases were patients attended
a bronchoscopy clinic at the North West Lung Centre, Wythenshawe Hospital in Manchester
during that period who were subsequently found to have lung cancer. Referents were patients
found not to have lung cancer at bronchoscopy.
Results:
There were 121 subjects in the study (39 cases, 82 referents). Smoking status was significantly
associated with lung cancer risk: the odds ratio of having lung cancer in ever smokers (vs never
smokers) was 3.21 (95% CI: 1.02 - 10.07). There were also significant association between
number of cigarettes smoked (p = 0.01) and years smoked (p = 0.04) with lung cancer risk.
-
Journal of Occupational Safety and Health
14 2
Years of exposure to occupational carcinogens was also associated with the development of lung
cancer (p = 0.02). Workers who were exposed for 45 years or more, had an increase risk when
compared to those who had worked for less than 17 years (OR, 95% CI = 2.54, 1.12 – 6.34). Job
category was found to be borderline significant with lung cancer risk. The adjusted odds ratio of
having lung cancer among unskilled manual job worker (vs management, professional & associate
professional) was 4.75 (95% CI: 1.06 - 21.4).
Conclusion:
This study shows an exposure to occupational carcinogens was associated with an elevated lung
cancer risk. Unskilled manual job workers had a higher lung cancer risk compared with other
categories, such as management, professional & associate professional.
Keywords:
Occupational Lung Carcinogens, Lung Cancer, Smoking
_______________________________________________________________________________
1. INTRODUCTION
1.1. Occupational exposure to known lung carcinogens
Lung cancer is the second ranked after bladder cancer among all occupational cancers worldwide
(Hansen, 2008). The risk of occupational substances causing lung cancer depends on certain
occupational characteristics, including the nature of work or job category (direct or indirect
exposure), how much exposure (the quantities), for how long (age of employment, length of
exposure, frequency been exposed), types of the substance (gas or mist form, individual or mixed
form) and whether the substance is organic or non-organic (Hansen, 2008).
The carcinogen list based on IARC category (“Lists of IARC evaluations according to IARC
monographs - International occupational safety & health information centre,” n.d.) such as list A
(confirmed human carcinogen) and list B (suspected human carcinogen), is still being updated
periodically to uncover the harmful effects particularly for those where there are still substantial
uncertainties. A recent population-based study found an increased risk of lung cancer in list A
occupation category with OR 1.74 (95% CI 1.27 – 2.38) compared with list B category. Lung
cancer risk in increased in several industrial sectors; the ceramic and refractory brick sector (OR,
95% CI = 2.64, 1.13– 6.19) and nonferrous metals industry (OR, 95% CI = 2.45, 1.31– 4.60)
(Consonni et al., 2010). They estimated that 4.9 % (95% CI 2.0 – 7.8) of lung cancers in men were
attributable to occupation (Consonni et al., 2010).
-
Journal of Occupational Safety and Health
15 3
1.2. Risk factors and specific occupational lung carcinogen
Based on a recent number of occupations or occupational exposures listed by IARC (“Lists of
IARC evaluations according to IARC monographs - International occupational safety & health
information centre,” n.d.) studies have reported on the magnitude of the association between
specific occupational carcinogen and lung cancer risk. As reported in the IARC and the National
Toxicology Program (NTP) (“Lists of IARC evaluations according to IARC monographs -
International occupational safety & health information centre,” n.d.), workers in a specific job
category and particular type of industry are often at an increased risk of lung cancer. For example,
workers in shoe manufacturing are exposed to a group of carcinogenic substances such as organic
solvents (toluene, xylene, methyl ethyl ketone, formaldehyde), chromium, nickel, arsenic, vinyl
chloride or others (Galán Dávila, Romero Candeira, Sánchez Payá, Orts Giménez, & Llorca
Martínez, 2005).
A cohort study of 7828 workers in a shoe manufacturing plant in USA found a significant excess
of lung cancer deaths with a SMR = 1.36 (95% CI 1.19-1.54)(Lehman & Hein, 2006). This was
associated with exposure to chronic, low levels of organic solvents and the finding has persisted
with increasing years of follow up of the cohort. The evidence regarding the risk of lung cancer
related to solvents continues to emerge. Another study with 6000 subjects in European countries
looking at the exposure to specific organic solvents (acrylnitrile, vinyl chloride and styrene)
reported a significant increase in the risk of lung cancer for ever exposure to acrylnitrile (OR, 95%
CI = 2.20, 1.11 – 4.36) and vinyl chloride (OR, 95% CI = 1.05, 0.68– 1.62). There was a positive
dose-response relationship although not significant, between estimated cumulative exposure
(maximum cumulative exposure compared to non-exposed) and lung cancer risk for both
acrylnitrile (OR, 95% CI = 2.87, 0.85 – 9.66) and vinyl chloride (OR, 95% CI = 1.51, 0.65– 3.47)
(“Lists of IARC evaluations according to IARC monographs - International occupational safety &
health information centre,” n.d.)
Two occupations met the criteria of having sufficient evidence of carcinogenicity for the human
lung, namely painters and welders (“Lists of IARC evaluations according to IARC monographs -
International occupational safety & health information centre,” n.d.). A significant association
between risk of lung cancer and occupational exposure to paint dust (RR, 95% CI = 2.48, 0.88-
6.97) and welding fumes (RR, 95% CI = 1.73, 1.05 – 2.85) has been reported in a large cohort
study in the Netherlands with 58,279 participants (van Loon et al., 1997). The same finding was
2
Years of exposure to occupational carcinogens was also associated with the development of lung
cancer (p = 0.02). Workers who were exposed for 45 years or more, had an increase risk when
compared to those who had worked for less than 17 years (OR, 95% CI = 2.54, 1.12 – 6.34). Job
category was found to be borderline significant with lung cancer risk. The adjusted odds ratio of
having lung cancer among unskilled manual job worker (vs management, professional & associate
professional) was 4.75 (95% CI: 1.06 - 21.4).
Conclusion:
This study shows an exposure to occupational carcinogens was associated with an elevated lung
cancer risk. Unskilled manual job workers had a higher lung cancer risk compared with other
categories, such as management, professional & associate professional.
Keywords:
Occupational Lung Carcinogens, Lung Cancer, Smoking
_______________________________________________________________________________
1. INTRODUCTION
1.1. Occupational exposure to known lung carcinogens
Lung cancer is the second ranked after bladder cancer among all occupational cancers worldwide
(Hansen, 2008). The risk of occupational substances causing lung cancer depends on certain
occupational characteristics, including the nature of work or job category (direct or indirect
exposure), how much exposure (the quantities), for how long (age of employment, length of
exposure, frequency been exposed), types of the substance (gas or mist form, individual or mixed
form) and whether the substance is organic or non-organic (Hansen, 2008).
The carcinogen list based on IARC category (“Lists of IARC evaluations according to IARC
monographs - International occupational safety & health information centre,” n.d.) such as list A
(confirmed human carcinogen) and list B (suspected human carcinogen), is still being updated
periodically to uncover the harmful effects particularly for those where there are still substantial
uncertainties. A recent population-based study found an increased risk of lung cancer in list A
occupation category with OR 1.74 (95% CI 1.27 – 2.38) compared with list B category. Lung
cancer risk in increased in several industrial sectors; the ceramic and refractory brick sector (OR,
95% CI = 2.64, 1.13– 6.19) and nonferrous metals industry (OR, 95% CI = 2.45, 1.31– 4.60)
(Consonni et al., 2010). They estimated that 4.9 % (95% CI 2.0 – 7.8) of lung cancers in men were
attributable to occupation (Consonni et al., 2010).
-
Journal of Occupational Safety and Health
16 4
reported in a recent meta-analysis study on lung cancer and welding with 60 studies of welders of
shipyard, mild steel and stainless steel. The combined relative risks (CRR) for lung cancer in all
the welders as compared with non-welders was 1.26 (95% CI 1.20 – 1.32) (Ambroise, Wild, &
Moulin, 2006).
Figure 1: Forest plot of lung cancer risk with occupational exposure
(van Loon et al., 1997),(Ambroise et al., 2006),(Berry, 2004),(Cassidy et al., 2007),(Olsson et
al., 2010),(Scélo et al., 2004)
However the study failed to detect any dose-response relationship between lung cancer incidence
and cumulative exposure to chromium and nickel in welders (Ambroise et al., 2006). The
magnitude of association between occupational exposure and lung cancer risk from previous
studies is summarized in figure 1.
In another study in the Netherlands an increased risk of lung cancer was reported for employment
of 15 years and more in blue collar jobs in the “electronics and optical instruments” industry (RR,
5.0
2.0
_________________
Asbestos (OR, 95% CI = 1.85, 1.07-3.21)
Vinyl chloride (OR, 95% CI = 1.05, 0.68– 1.62)
Acrylnitrile (OR, 95% CI = 2.20, 1.11 – 4.36)
PAHs (OR, 95% CI = 1.97, 1.16 – 3.35)
Silica (OR, 95% CI = 1.37, 1.14-1.65)
Welding fumes (RR, 95% CI = 1.73, 1.05 – 2.85)
Paint dust (RR, 95% CI = 2.48, 0.88-6.97)
Occupational Exposure
Magnitude of association
____________________
_______________________
____________
____________________________
_______________
1.0
-
Journal of Occupational Safety and Health
17 5
95% CI = 1.99, 1.18 – 3.35), “construction and homebuilding business” industry (RR, 95% CI =
1.64, 1.21 – 2.22) and “railway company” (RR, 95% CI = 2.40, 1.00 – 5.73) (Preller, Balder,
Tielemans, Brandt, & Goldbohm, 2008). The risk of lung cancer was observed for lengthy
employment in certain high-risk industries and research on specific occupational category is
needed to further investigate causative factors.
The aim of this study was to examine occupational exposures and lung cancer risk in a North West
population. The ultimate aim of this work is to compare the occupational exposure and the
development of lung cancer in previous studies carried out in Wythenshawe, which have been
looking at the factors and determinants for lung cancer risk and susceptibility.
2. METHODOLOGY
2.1. Study population
Self-reported occupational histories and exposures were collected in a case-referent study that was
carried out between November 1998 to March 2000. Cases were patients attended a bronchoscopy
clinic at the North West Lung Centre, Wythenshawe Hospital who were subsequently found to
have lung cancer. Referents were patients found not to have lung cancer at bronchoscopy.
2.2. Occupational exposure analysis
The occupational history was assessed by questions on the employment status, the title of the job,
period of employment and working duration (hours) per week. For each person, information of a
maximum of five occupations was registered, starting with the current or most recent job first and
working backwards. In the few cases where more than five occupations were mentioned, similar
consecutive jobs for different employers were deleted. If more than five jobs still remained, the job
with the least information provided was omitted unless it lasted for a very long time.
The information on occupational exposure was obtained by asking the participants whether they
were exposed to smoke, dust, fumes or asbestos. The type of industry was coded according to the
UK Standard Industrial Classification (2003) and occupation was coded according to the Standard
Occupational Classification (2000), both from the UK Office for National Statistics (ONS) (Office
for National Statistics, 2010).
4
reported in a recent meta-analysis study on lung cancer and welding with 60 studies of welders of
shipyard, mild steel and stainless steel. The combined relative risks (CRR) for lung cancer in all
the welders as compared with non-welders was 1.26 (95% CI 1.20 – 1.32) (Ambroise, Wild, &
Moulin, 2006).
Figure 1: Forest plot of lung cancer risk with occupational exposure
(van Loon et al., 1997),(Ambroise et al., 2006),(Berry, 2004),(Cassidy et al., 2007),(Olsson et
al., 2010),(Scélo et al., 2004)
However the study failed to detect any dose-response relationship between lung cancer incidence
and cumulative exposure to chromium and nickel in welders (Ambroise et al., 2006). The
magnitude of association between occupational exposure and lung cancer risk from previous
studies is summarized in figure 1.
In another study in the Netherlands an increased risk of lung cancer was reported for employment
of 15 years and more in blue collar jobs in the “electronics and optical instruments” industry (RR,
5.0
2.0
_________________
Asbestos (OR, 95% CI = 1.85, 1.07-3.21)
Vinyl chloride (OR, 95% CI = 1.05, 0.68– 1.62)
Acrylnitrile (OR, 95% CI = 2.20, 1.11 – 4.36)
PAHs (OR, 95% CI = 1.97, 1.16 – 3.35)
Silica (OR, 95% CI = 1.37, 1.14-1.65)
Welding fumes (RR, 95% CI = 1.73, 1.05 – 2.85)
Paint dust (RR, 95% CI = 2.48, 0.88-6.97)
Occupational Exposure
Magnitude of association
____________________
_______________________
____________
____________________________
_______________
1.0
-
Journal of Occupational Safety and Health
18 6
2.3. Statistical analysis
Frequencies are presented for categorical data and means with standard deviations for continuous
data. All statistical analysis was carried out in SPSS (version 15.0). Comparisons were made
between two groups (e.g. cases and referents) to determine the risk of lung cancer. χ2-test was
used for 2 X 2 table and binary logistic regression was used for variable with 2 or more categorical
groups. Odds Ratio (OR) and its 95% confidence interval (96% CI) was measured to determine the
magnitude of association for occupational and other factors (smoking, alcohol consumption and
family history of lung cancer) with lung cancer risk. The variables were further stratified for
smoking status to control for confounding factor and adjusted odds ratio were then measured.
3. RESULTS
3.1. Study population
There are 121 subjects in the study (39 cases, 82 referents), which 74 (61.2%) of them were men
with a mean age of total study population was 61.1 + 13.7 years old. (Table 1)
Table 1.Frequency distribution of lung cancer incidence by gender and age group
Variable
Lung Cancer
Yes No n (%) n (%)
Total n (%)
Gender
Male
Female
Age group (years)
< 55
55 - 64
65 - 74
≥ 75
(mean + SD)
29 (74.4)
10 (25.6)
6 (17.1)
10 (28.6)
14 (40.0)
5 (14.3)
64.6 + 10.7
45 (54.9)
37 (45.1)
32 (40.5)
15 (19.0)
18 (22.8)
14 (17.7)
59.7 + 14.6
74 (61.2)
47 (38.8)
38 (33.3)
25 (21.9)
32 (28.1)
19 (16.7)
61.1 + 13.7
3.2. Smoking characteristics and alcohol intake with lung cancer
Smoking status was significantly associated with lung cancer risk: the odds ratio (OR) of having
lung cancer in ever smokers (vs. never smokers) were 3.21 (95% CI: 1.02 - 10.07). The duration of
years cigarette smoked was longer in the lung cancer group with mean of 42.7 + 13.1 years
compared with mean of 32.1 + 16.0 for referents, and was significantly associated with lung cancer
risk. Other characteristics were not significantly associated with lung cancer risk (Table 2)
-
Journal of Occupational Safety and Health
19 7
Table 2. Smoking characteristics and alcohol intake in cases and referents
Variable
Lung Cancer
Yes No n (%) n (%)
Crude Odds Ratio
(95% CI)a
Ever smoking
Yes
Nob
Smoking status
Current smoker
Ex-smokerb
Age smoking began
(years)
< 15b
15 - 19
20 - 24
≥ 25
(mean + SD)
Cigarettes smoked
(per day)
1 - 9
10 - 19
20 - 39
≥ 40 b
(mean + SD)
Years smoked
1 - 9
10 - 29
30 - 49
≥ 50b
(mean + SD)
Passive smoker
Yes
Nob
Ever drink alcohol
Yes
Nob
Alcohol intake
(units per week)
0b
1 - 13
14 - 27
≥ 28
(mean + SD)
35 (89.7)
4 (10.3)
17 (48.6)
18 (51.4)
22 (62.9)
10 (28.6)
3 (8.6)
0 (0)
15.2 + 2.9
0 (0)
10 (28.6)
18 (51.4)
7 (20.0)
24.0 + 12.6
0 (0)
5 (14.7)
17 (50.0)
12 (35.3)
42.7 + 13.1
17 (43.6)
22 (56.4)
29 (74.4)
10 (25.6)
10 (25.6)
17 (43.6)
6 (15.4)
6 (15.4)
14.5 + 16.1
60 (73.2)
22 (26.8)
23 (38.3)
37 (61.7)
28 (46.7)
23 (38.3)
7 (11.7)
2 (3.3)
16.4 + 3.3
8 (13.6)
11 (18.6)
34 (57.6)
6 (10.2)
21.0 + 12.4
3 (5.9)
19 (37.3)
19 (37.3)
10 (19.6)
32.1 + 16.0
34 (41.5)
48 (58.5)
66 (80.5)
16 (19.5)
17 (21.0)
39 (48.1)
17 (21.0)
8 (9.9)
12.3 + 12.2
3.21 (1.02-10.07)
1*
1.52 (0.65-3.53)
1
1
0.55 (0.22-1.40)
0.54 (0.13-2.36)
0.78 (0.19-3.11)
0.45 (0.13-1.55)
1
0.22 (0.60-0.80)
0.75 (0.26-2.16)
1*
1.09 (0.50-2.36)
1
0.70 (0.29-1.73)
1
1
0.74 (0.28-1.94)
0.60 (0.18-2.02)
1.23 (0.34-4.75)
* significant difference p
-
Journal of Occupational Safety and Health
20 8
3.3. Occupational exposure and lung cancer risk
The variables of occupational characteristic were stratified for smoking status to control for
confounding factor and adjusted odds ratio (aOR) are tabulated in Table 3. Lung cancer risk varied
with job category with an aOR among unskilled manual job workers (vs. management,
professional & associate professional) of 4.75 (95% CI: 1.06-21.36). Exposure to occupational
carcinogens was associated with an elevated but non-significant lung cancer risk: the aOR in ever
exposed (vs never exposed) was 1.93 (95% CI: 0.77-4.82). There was no association with duration
of exposure. Workers who were exposed to smoke or asbestos, had an increased risk when
compared to those who had no exposure: aOR = 3.56 (95% CI: 0.96-13.13) for smoke and aOR =
4.00 (95% CI: 1.10-14.47) for asbestos.
Table 3. Occupational characteristics in cases and referents
Variable
Lung Cancer
Yes No n (%) n (%)
Crude Odds Ratio
(95% CI)a
Adjusted Odds Ratio
(95% CI)c
Employment status
Employed
Not employedb
Job category
Management, professional &
associate professionalb
Clerical and secretarial
Sales and service
Skilled manual
Unskilled manual
Exposure to carcinogen
Yes
Nob
Years of exposure
1 - 17b
18 - 32
33 - 44
≥ 45
(mean + SD)
Exposure to specific carcinogen
No exposureb
Exposed to smoke
Exposed to dust
Exposed to fumes
Exposed to asbestos
5 (12.8)
34 (87.2)
8 (20.5)
7 (17.9)
8 (20.5)
8 (20.5)
8 (20.5)
30 (76.9)
9 (23.1)
13 (43.3)
11 (36.7)
4 (13.3)
2 (6.7)
20.6 + 13.7
9 (23.1)
9 (23.1)
6 (15.4)
6 (15.4)
9 (23.1)
27 (31.7)
55 (68.3)
26 (32.1)
12 (14.8)
24 (29.6)
15 (18.5)
4 (4.9)
46 (56.1)
36 (43.9)
26 (56.5)
10 (21.7)
9 (19.6)
1 (2.2)
18.1 + 13.3
36 (43.9)
9 (11.0)
15 (18.3)
14 (17.1)
8 ( 9.8)
0.30 (0.10-0.85)
1*
1
1.89 (0.56-6.44)
1.08 (0.35-3.34)
1.73 (0.54-5.57)
6.50(1.54-27.4)
2.61 (1.10-6.18)
1*
1
2.20 (0.74-6.51)
0.89 (0.23-3.44)
4.00 (0.33-48.3)
1
4.00 (1.23-13.0)
1.60 (0.48-5.29)
1.71 (0.51-5.71)
4.50 (1.35-14.9)
0.33 (0.11-0.99)
1*
1
2.38 (0.63-9.02)
0.96 (0.27-3.42)
1.97 (0.56-6.94)
4.75 (1.06-21.4)
1.93 (0.77-4.82)
1
1
2.73 (0.81-9.15)
1.09 (0.26-4.55)
1.91 (0.11-33.5)
1
3.56 (0.96-13.1)
0.89 (0.23-3.49)
1.11 (0.30-4.05)
4.00 (1.10-14.5)
* significant difference p
-
Journal of Occupational Safety and Health
21 9
3.4. Family history of lung cancer and lung cancer risk
Table 4 shows the number of patients with a family history of lung cancer. The majority of the
lung cancer patients had no family history of lung cancer (94.9%) and there was no significant
association with lung cancer risk.
Table 4. Family history of lung cancer in cases and referents
Variable
Lung Cancer
Yes No n (%) n (%)
Odds Ratio
(95% CI)a
Relatives with lung cancer
No
Yesb
Unknown
37 (94.9)
2 (5.1)
0 (0)
75 (91.5)
6 (7.3)
1 (1.2)
1
0.68 (0.13-3.51)
aOdds ratio is for incidence of lung cancer in each group versus incidence in patients in groupb
4. DISCUSSION
In this study, we examined the risks associated with occupational exposures in a case-referent
study of lung cancer. The completed self-reported occupational histories and exposures were
analysed. This is a small pilot study using general job questionnaires to assess the occupational
exposure and the findings will be used as part of the reference for the main study that will be
undertaken in the same population.
From this study, smoking status was significantly associated with lung cancer risk, with three-fold
higher risk to get lung cancer. The risk also associated with the duration of years smoked. The
findings were consistent with the other studies (Doll & Hill, 1950), (Peto, Lopez, Boreham, Thun,
& Heath, 1992) which indicating the duration of smoking is one of the strongest determinants of
lung cancer risk in smokers. The risk increases with the number of years a person has smoked and
also the number of cigarettes smoked (Lubin & Caporaso, 2006).
Different job category having different types of exposure to occupational hazards particularly
occupational carcinogens. In this study, unskilled manual job workers had a higher lung cancer
risk compared with other categories, such as management, professional & associate professional. It
is suggested that those who worked in the unskilled manual workers are prone to be more exposed
to different kind of occupational carcinogens.
8
3.3. Occupational exposure and lung cancer risk
The variables of occupational characteristic were stratified for smoking status to control for
confounding factor and adjusted odds ratio (aOR) are tabulated in Table 3. Lung cancer risk varied
with job category with an aOR among unskilled manual job workers (vs. management,
professional & associate professional) of 4.75 (95% CI: 1.06-21.36). Exposure to occupational
carcinogens was associated with an elevated but non-significant lung cancer risk: the aOR in ever
exposed (vs never exposed) was 1.93 (95% CI: 0.77-4.82). There was no association with duration
of exposure. Workers who were exposed to smoke or asbestos, had an increased risk when
compared to those who had no exposure: aOR = 3.56 (95% CI: 0.96-13.13) for smoke and aOR =
4.00 (95% CI: 1.10-14.47) for asbestos.
Table 3. Occupational characteristics in cases and referents
Variable
Lung Cancer
Yes No n (%) n (%)
Crude Odds Ratio
(95% CI)a
Adjusted Odds Ratio
(95% CI)c
Employment status
Employed
Not employedb
Job category
Management, professional &
associate professionalb
Clerical and secretarial
Sales and service
Skilled manual
Unskilled manual
Exposure to carcinogen
Yes
Nob
Years of exposure
1 - 17b
18 - 32
33 - 44
≥ 45
(mean + SD)
Exposure to specific carcinogen
No exposureb
Exposed to smoke
Exposed to dust
Exposed to fumes
Exposed to asbestos
5 (12.8)
34 (87.2)
8 (20.5)
7 (17.9)
8 (20.5)
8 (20.5)
8 (20.5)
30 (76.9)
9 (23.1)
13 (43.3)
11 (36.7)
4 (13.3)
2 (6.7)
20.6 + 13.7
9 (23.1)
9 (23.1)
6 (15.4)
6 (15.4)
9 (23.1)
27 (31.7)
55 (68.3)
26 (32.1)
12 (14.8)
24 (29.6)
15 (18.5)
4 (4.9)
46 (56.1)
36 (43.9)
26 (56.5)
10 (21.7)
9 (19.6)
1 (2.2)
18.1 + 13.3
36 (43.9)
9 (11.0)
15 (18.3)
14 (17.1)
8 ( 9.8)
0.30 (0.10-0.85)
1*
1
1.89 (0.56-6.44)
1.08 (0.35-3.34)
1.73 (0.54-5.57)
6.50(1.54-27.4)
2.61 (1.10-6.18)
1*
1
2.20 (0.74-6.51)
0.89 (0.23-3.44)
4.00 (0.33-48.3)
1
4.00 (1.23-13.0)
1.60 (0.48-5.29)
1.71 (0.51-5.71)
4.50 (1.35-14.9)
0.33 (0.11-0.99)
1*
1
2.38 (0.63-9.02)
0.96 (0.27-3.42)
1.97 (0.56-6.94)
4.75 (1.06-21.4)
1.93 (0.77-4.82)
1
1
2.73 (0.81-9.15)
1.09 (0.26-4.55)
1.91 (0.11-33.5)
1
3.56 (0.96-13.1)
0.89 (0.23-3.49)
1.11 (0.30-4.05)
4.00 (1.10-14.5)
* significant difference p
-
Journal of Occupational Safety and Health
22 10
Exposure to occupational carcinogens was associated with an elevated lung cancer risk; however
there was no association with duration of exposure. Workers who were exposed to smoke or
asbestos had an increased risk when compared to those who had no exposure. It is consistent with
other studies which showed workers who are exposed to smoke or asbestos, which include in the
list A IARC list are in the higher risk to get the occupational lung cancer (Driscoll et al., 2005),
(Berry, 2004).
5. CONCLUSION
This study shows an exposure to occupational carcinogens was associated with an elevated lung
cancer risk. Unskilled manual job workers had a higher lung cancer risk compared with other
categories, such as management, professional & associate professional.
-
Journal of Occupational Safety and Health
23 11
6. REFERENCES
Ambroise, D., Wild, P., & Moulin, J.-J. (2006). Update of a meta-analysis on lung cancer and
welding. Scandinavian Journal of Work, Environment & Health, 32(1), 22–31.
doi:10.5271/sjweh.973
Berry, G. (2004). The Interaction of Asbestos and Smoking in Lung Cancer: A Modified Measure
of Effect. Annals of Occupational Hygiene, 48(5), 459–462. doi:10.1093/annhyg/meh023
Cassidy, A., ’t Mannetje, A., van Tongeren, M., Field, J. K., Zaridze, D., Szeszenia-Dabrowska,
N., Boffetta, P. (2007). Occupational exposure to crystalline silica and risk of lung cancer: a
multicenter case-control study in Europe. Epidemiology (Cambridge, Mass.), 18(1), 36–43.
doi:10.1097/01.ede.0000248515.28903.3c
Consonni, D., De Matteis, S., Lubin, J. H., Wacholder, S., Tucker, M., Pesatori, A. C., … Landi,
M. T. (2010). Lung cancer and occupation in a population-based case-control study. American
Journal of Epidemiology, 171(3), 323–333. doi:10.1093/aje/kwp391
Doll, R., & Hill, A. B. (1950). Smoking and Carcinoma of the Lung. British Medical Journal,
2(4682), 739–748.
Driscoll, T., Nelson, D. I., Steenland, K., Leigh, J., Concha-Barrientos, M., Fingerhut, M., &
Prüss-Ustün, A. (2005). The global burden of disease due to occupational carcinogens.
American Journal of Industrial Medicine, 48(6), 419–431. doi:10.1002/ajim.20209
Galán Dávila, A., Romero Candeira, S., Sánchez Payá, J., Orts Giménez, D., & Llorca Martínez, E.
(2005). Lung Cancer Risk in Shoe Manufacturing. Archivos de Bronconeumología ((English
Edition)), 41(4), 202–205. doi:10.1016/S1579-2129(06)60426-6
10
Exposure to occupational carcinogens was associated with an elevated lung cancer risk; however
there was no association with duration of exposure. Workers who were exposed to smoke or
asbestos had an increased risk when compared to those who had no exposure. It is consistent with
other studies which showed workers who are exposed to smoke or asbestos, which include in the
list A IARC list are in the higher risk to get the occupational lung cancer (Driscoll et al., 2005),
(Berry, 2004).
5. CONCLUSION
This study shows an exposure to occupational carcinogens was associated with an elevated lung
cancer risk. Unskilled manual job workers had a higher lung cancer risk compared with other
categories, such as management, professional & associate professional.
-
Journal of Occupational Safety and Health
24 12
Hansen, H. (Ed.). (2008). Textbook of Lung Cancer, Second Edition (2nd ed.). Informa
Healthcare.
Lehman, E. J., & Hein, M. J. (2006). Mortality of workers employed in shoe manufacturing: an
update. American Journal of Industrial Medicine, 49(7), 535–546.
Lists of IARC evaluations according to IARC monographs - International occupational safety &
health information centre. (n.d.). Retrieved May 1, 2012, from
http://www.ilo.org/legacy/english/protection/safework/cis/products/safetytm/iarclist.htm
Lubin, J. H., & Caporaso, N. E. (2006). Cigarette smoking and lung cancer: modeling total
exposure and intensity. Cancer Epidemiology, Biomarkers & Prevention: A Publication of the
American Association for Cancer Research, Cosponsored by the American Society of
Preventive Oncology, 15(3), 517–523. doi:10.1158/1055-9965.EPI-05-0863
Office for National Statistics, E. L. and S. A. (2010, June 23). Standard Occupational
Classification 2010 (SOC2010). Office for National Statistics. Text. Retrieved July 29, 2013,
from http://www.ons.gov.uk/ons/guide-method/classifications/current-standard-
classifications/soc2010/index.html
Olsson, A. C., Fevotte, J., Fletcher, T., Cassidy, A., ’t Mannetje, A., Zaridze, D., Boffetta, P.
(2010). Occupational exposure to polycyclic aromatic hydrocarbons and lung cancer risk: a
multicenter study in Europe. Occupational and Environmental Medicine, 67(2), 98–103.
doi:10.1136/oem.2009.046680
Peto, R., Lopez, A. D., Boreham, J., Thun, M., & Heath, C., Jr. (1992). Mortality from tobacco in
developed countries: indirect estimation from national vital statistics. Lancet, 339(8804),
1268–1278.
-
Journal of Occupational Safety and Health
25
13
Preller, L., Balder, H. F., Tielemans, E., Brandt, P. A. van den, & Goldbohm, R. A. (2008).
Occupational lung cancer risk among men in the Netherlands. Occupational and
Environmental Medicine, 65(4), 249–254. doi:10.1136/oem.2006.030353
Scélo, G., Constantinescu, V., Csiki, I., Zaridze, D., Szeszenia-Dabrowska, N., Rudnai, P., …
Boffetta, P. (2004). Occupational Exposure to Vinyl Chloride, Acrylonitrile and Styrene and
Lung Cancer Risk (Europe). Cancer Causes & Control, 15(5), 445–452.
Van Loon, A. J., Kant, I. J., Swaen, G. M., Goldbohm, R. A., Kremer, A. M., & van den Brandt, P.
A. (1997). Occupational exposure to carcinogens and risk of lung cancer: results from The
Netherlands cohort study. Occupational and Environmental Medicine, 54(11), 817–824.
12
Hansen, H. (Ed.). (2008). Textbook of Lung Cancer, Second Edition (2nd ed.). Informa
Healthcare.
Lehman, E. J., & Hein, M. J. (2006). Mortality of workers employed in shoe manufacturing: an
update. American Journal of Industrial Medicine, 49(7), 535–546.
Lists of IARC evaluations according to IARC monographs - International occupational safety &
health information centre. (n.d.). Retrieved May 1, 2012, from
http://www.ilo.org/legacy/english/protection/safework/cis/products/safetytm/iarclist.htm
Lubin, J. H., & Caporaso, N. E. (2006). Cigarette smoking and lung cancer: modeling total
exposure and intensity. Cancer Epidemiology, Biomarkers & Prevention: A Publication of the
American Association for Cancer Research, Cosponsored by the American Society of
Preventive Oncology, 15(3), 517–523. doi:10.1158/1055-9965.EPI-05-0863
Office for National Statistics, E. L. and S. A. (2010, June 23). Standard Occupational
Classification 2010 (SOC2010). Office for National Statistics. Text. Retrieved July 29, 2013,
from http://www.ons.gov.uk/ons/guide-method/classifications/current-standard-
classifications/soc2010/index.html
Olsson, A. C., Fevotte, J., Fletcher, T., Cassidy, A., ’t Mannetje, A., Zaridze, D., Boffetta, P.
(2010). Occupational exposure to polycyclic aromatic hydrocarbons and lung cancer risk: a
multicenter study in Europe. Occupational and Environmental Medicine, 67(2), 98–103.
doi:10.1136/oem.2009.046680
Peto, R., Lopez, A. D., Boreham, J., Thun, M., & Heath, C., Jr. (1992). Mortality from tobacco in
developed countries: indirect estimation from national vital statistics. Lancet, 339(8804),
1268–1278.
-
This page has been intentionally left blank
-
Journal of Occupational Safety and Health
27 1
OHSAS 18001 and MS 1722 Certification Initiatives Prove the
Commitment to Sustainability
Wai Onn Hong
Processing Department, Genting Plantations Berhad,
10th
Floor, Wisma Genting, Jalan Sultan Ismail, Kuala Lumpur, Malaysia
Tel: +60 3 2333 6506 Fax: + 60 3 2161 9689 Email: [email protected]
__________________________________________________________________________________
Abstract
Malaysia’s palm oil industry is growing in complexity and successively to succeed on the global
level by accounts for about 36% of the word production of palm oil [1]. But, Occupational Health
and Safety (OHS) issues are still problematic areas that need to be addressed by all parties
concerned in this industry. In the olden days, unlike construction or manufacturing industry, palm
oil industry was green in OHS management system. However, due to stringent in the legislative
enforcement in the past few years, it has lead some of the plantation companies to develop OHS
management system, which are based on Occupational Health and Safety Assessment Series
(OHSAS), towards corporate sustainability. Sustainability is not about paying lip-service to the
latest corporate buzzword; neither is it about superficially meeting minimum requirements for the
sake of compliance. Rather, sustainability is a core value that lies at the heart of the companies’
business conduct. In practical terms, this means strive to operate with due consideration for the
interest of all stakeholders by making the health and safety of all workers a priority. This paper
describes the certification of OHSAS 18001 and MS 1722 in Genting Plantations Berhad (GENP)
prove the commitment to sustainability by forming guiding principle on safety management.
Further, this paper also demonstrates that the implementation of safety management can help to
reduce the accident rate, especially fatal accident.
Keywords: palm oil industry, OHSAS 18001, MS 1722, safety management, sustainability
_________________________________________________________________________________
Introduction
The working population is a valuable asset to our nation especially palm oil industry, therefore we
cannot afford to have many accidents which will eventually jeopardize our valued human resources.
Workers involved in palm oil industry can be divided into two broad categories: those working in
the plantations and those employed to work in the palm oil mill. The former are mainly the
harvesters who harvest the fresh fruit bunches while the second category includes the workers
employed to operate and maintain machineries in palm oil mills. Accidents involving both of these
categories are not rare in Malaysia. Statistic of occupational accidents in the country published by
-
Journal of Occupational Safety and Health
28 2
Department of Occupational Safety and Health (DOSH) show that the total number of accidents as
well as the number of fatalities has not much improvement between 2007 and 2011 (Figure 1).
In view of OHS issues still remain an important matter in palm oil industry throughout the decade,
government has in fact stringent in the legislative enforcement since recent years. It is at a time like
this that the palm oil industry needs to consolidate and be proactive in meeting upcoming
challenges. The palm oil industry also needs to meet challenges with more evidence of sustainable
safety management system throughout the implementation.
This paper not only describes the certification of OHSAS 18001 and MS 1722 in Genting
Plantations Berhad proves the commitment to sustainability by forming guiding principle on safety
management, but also demonstrates that the implementation of safety management can help to
reduce the accident rate, especially fatal accident.
The OHSAS 18001 and the MS 1722 standard enable an organization to manage its OHS risks and
improve its OHS performance. The requirements of the standard are intended to address OHS for
employees, temporary employees, contractors and other personnel on site rather than the safety of
products and services. The standards provide a more effective method of protecting employees and
others from workplace injuries and illnesses and demonstrate management commitment in meeting
OHS requirements [2, 3, 4].
-
Journal of Occupational Safety and Health
29 3
Figure 1: National accident rate per 1,000 workers and fatality rate per 100,000 workers from year 2007 – 2011
GENP’s Response and Initiative
In Malaysia, legislation concerning OHS for palm oil industry comprises the following Acts and
Regulations:
a) Occupational Safety and Health Act 1994
b) Factories and Machineries Act 1967
c) Electricity Supply Act 1990
d) Fire Services Act 1994
Although with all these Acts and Regulations in placed, it is always an argument that who should
responsible and accountable for accident prevention, employers, employees or relevant authorities.
GENP’s commitment to these areas, which are of paramount importance to the Group’s overall
sustainability agenda, was displayed clearly through important certification initiatives undertaken at
the palm oil mill level. As part of the palm oil mill improvement efforts, GENP’s palm oil mills
embarked on a third party, independent verification exercise of their OHS Management System,
guided by a road map began in year 2010. Under the standards subscribes, OHS management
system composed of standards, procedures and monitoring arrangement that aim at promoting the
OHS of people at workplace and to protect the public from accident shall be established and
implemented.
2
Department of Occupational Safety and Health (DOSH) show that the total number of accidents as
well as the number of fatalities has not much improvement between 2007 and 2011 (Figure 1).
In view of OHS issues still remain an important matter in palm oil industry throughout the decade,
government has in fact stringent in the legislative enforcement since recent years. It is at a time like
this that the palm oil industry needs to consolidate and be proactive in meeting upcoming
challenges. The palm oil industry also needs to meet challenges with more evidence of sustainable
safety management system throughout the implementation.
This paper not only describes the certification of OHSAS 18001 and MS 1722 in Genting
Plantations Berhad proves the commitment to sustainability by forming guiding principle on safety
management, but also demonstrates that the implementation of safety management can help to
reduce the accident rate, especially fatal accident.
The OHSAS 18001 and the MS 1722 standard enable an organization to manage its OHS risks and
improve its OHS performance. The requirements of the standard are intended to address OHS for
employees, temporary employees, contractors and other personnel on site rather than the safety of
products and services. The standards provide a more effective method of protecting employees and
others from workplace injuries and illnesses and demonstrate management commitment in meeting
OHS requirements [2, 3, 4].
-
Journal of Occupational Safety and Health
30 4
Implementation of OHSAS 18001 and MS 1722
The initiatives on certification of OHSAS 18001 and MS 1722 started with gap analysis at GENP’s
oil mills to determine the status of existing OHS processes and controls in place. Recommendations
were provided to bridge the gaps in that analysis. Having completed the gap analysis, a series of
training were held to cover variety of topics, including ISO Awareness, Hazard Identification, Risk
Assessment and Risk Control, Safe Operating Procedure and Emergency Preparedness. This was
followed by the challenging task of preparing documentations in accordance with the unique
features of each palm oil mill and these have been structured into four levels as follows:
• Level 1 - Manual. This document gives an overview of the OHS Management Systems, includes
the policies and all the non-operations procedures. It also outlines the structure of the
documentation used in the OHS Management System.
• Level 2 – System Procedure. These documents specify principles, strategies and the general
procedures of operations related actions (system process).
• Level 3 – Operations Procedure Documents. These documents specify in details the current
practices or processes in any operations related action (core process).
• Level 4 – Records, forms and checklists. These documents further specify the manner of
processes in an action. They also demonstrate conformance to specified OHS Management
Systems.
The pyramid of OHS management system documentation is shown in Figure 2.
Figure 2: The pyramid of OHS management system documentation
-
Journal of Occupational Safety and Health
31 5
Meanwhile, at the operation sites, proactive measures were taken to improve the safety and health
performances. At the same time, safety and health awareness was also actively promoted at the
palm oil mills during daily morning muster and periodically training. Last stage of this project is to
conduct internal auditing of OHS performance. The internal auditors aim to ensure compliance with
OHSAS 18001 and MS 1722 standards thereby ensuring the success of OHS programs through the
implementation of safety management system. In additional, internal audit also serves as a platform
to identify OHS opportunities for continual improvement. After about one year implementation
period, SIRIM QAS International Sdn Bhd, the country’s leading and internationally-recognized
certification, inspection and testing body, was engaged to carry out a series of audits, culminate in
all palm oil mills successfully securing recommendation for certification of their Health and Safety
Management System under OHSAS 18001 and MS 1722 by the end of January 2011.
Implementation stages of OHSAS 18001 and MS 1722 was summarized in Figure 3.
Figure 3: Road map for implementation of OHSAS 18001 and MS 1722
Guiding Principle on Safety Management
OHSAS 18001 and MS 1722 implemented by GENP is applicable company-wide and information
is disseminated to all employees in order to ensure successful implementation. A generic safety
management system has been established in order to sustain OHSAS 18001 and MS 1722. In this
management system, a number of important elements are specified and these are related to the
setting of policy and creation of plans and organizational capacity to realize that policy (Plan), the
analysis of hazards and effects leading to planning and implementation of those plans in order to
manage the risks (Do) and the control on the effective performance of those steps (Check). A
4
Implementation of OHSAS 18001 and MS 1722
The initiatives on certification of OHSAS 18001 and MS 1722 started with gap analysis at GENP’s
oil mills to determine the status of existing OHS processes and controls in place. Recommendations
were provided to bridge the gaps in that analysis. Having completed the gap analysis, a series of
training were held to cover variety of topics, including ISO Awareness, Hazard Identification, Risk
Assessment and Risk Control, Safe Operating Procedure and Emergency Preparedness. This was
followed by the challenging task of preparing documentations in accordance with the unique
features of each palm oil mill and these have been structured into four levels as follows:
• Level 1 - Manual. This document gives an overview of the OHS Management Systems, includes
the policies and all the non-operations procedures. It also outlines the structure of the
documentation used in the OHS Management System.
• Level 2 – System Procedure. These documents specify principles, strategies and the general
procedures of operations related actions (system process).
• Level 3 – Operations Procedure Documents. These documents specify in details the current
practices or processes in any operations related action (core process).
• Level 4 – Records, forms and checklists. These documents further specify the manner of
processes in an action. They also demonstrate conformance to specified OHS Management
Systems.
The pyramid of OHS management system documentation is shown in Figure 2.
Figure 2: The pyramid of OHS management system documentation
-
Journal of Occupational Safety and Health
32 6
feedback loop is in placed to enable all the information gained are sent to management for their
respond (Act/Feedback). [2, 3, 4, 5]. Further, there is an element extended out of the loop where
the organization has to establish an OHS management system with continual improvement activities
in order to ensure the sustainability of OHSAS 18001 and MS 1722 subscribes. This safety
management system is simplified in Figure 4.
Figure 4: Generic OHS management system with elements of Plan-Do-Check-Act
Evolution of Safety Culture
The systematic approach to safety management in OHSMS is not the end the journey as
management system is a primarily rational inventions, defined on paper in offices and capable of
objective in audits. The next stage is to build generative safety culture. As the premier level in safety
cultures, generative safety culture is the situation where people carry out what they know has to be
done not because they have to, but they want to. In other words, it is where the safe behavior is fully
integrated into everything the organization does [5].
-
Journal of Occupational Safety and Health
33 7
In order to promote generative safety culture, GENP encouraging to have combination of a top-
down commitment to improve and the realization that the workforce is where that improvement has
to take place. To have this premier safety culture implant, information is actively sought and
responsibilities are shared among employees and employers. Furthermore, new ideas are welcomed
in generative safety culture regardless it is from which level of employees, workers, staffs or
executives.
Figure 5 shows the evolution of safety culture in GENP. Initial stage of safety culture at individual
oil mill might vary from reactive to proactive due to different level of safety awareness.
Nevertheless, all have successfully built and implant premier level of generative safety culture after
implementation of OHSMS.
Figure 5: Evolution of safety culture in GENP after implementing safety management
The effect of Implementing OHSAS 18001 and MS 1722
The most important and measurable benefit resulting from safety management system and evolution
to generative safety culture is decrease in occupational accident rate and fatality rate. Figure 6
summarizes the statistic of occupational accidents recorded during last five years in GENP oil mills.
2007 2008 2009 2010 2011 2012*
Number of
accidents 5 9 13 6 4 3
Number of
fatalities 2 2 1 0 0 0
6
feedback loop is in placed to enable all the information gained are sent to management for their
respond (Act/Feedback). [2, 3, 4, 5]. Further, there is an element extended out of the loop where
the organization has to establish an OHS management system with continual improvement activities
in order to ensure the sustainability of OHSAS 18001 and MS 1722 subscribes. This safety
management system is simplified in Figure 4.
Figure 4: Generic OHS management system with elements of Plan-Do-Check-Act
Evolution of Safety Culture
The systematic approach to safety management in OHSMS is not the end the journey as
management system is a primarily rational inventions, defined on paper in offices and capable of
objective in audits. The next stage is to build generative safety culture. As the premier level in safety
cultures, generative safety culture is the situation where people carry out what they know has to be
done not because they have to, but they want to. In other words, it is where the safe behavior is fully
integrated into everything the organization does [5].
-
Journal of Occupational Safety and Health
34 8
Accident rate
per 100
workers
0.35 0.62 0.85 0.38 0.25 0.19
Fatality rate
per 100
workers
0.14 0.14 0.07 0.00 0.00 0.00
Remark: Data updated as at June 2012.
Figure 6: Statistic of occupational accidents recorded during last five years in GENP oil mills
Figure 7 clearly shows that there was significant decrease in accident rate since year 2009 after
implementation of Occupational Health and Safety Management System. Furthermore, the accident
rate of 0.38 and 0.25 per 100 workers recorded in year 2010 and 2011 were greatly lower than
national accident rate for the same period, 0.65 and 0.62 per 100 workers respectively.
Figure 8 shows the fatality rate per 100 workers from year 2007 to 2012 (June). It was clearly shows
that implementation of OHSMS proves the commitment to sustainability as GENP oil mills
continuously recorded zero fatal accident since year 2009.
Figure 7: Accident rate per 100 workers from year 2007 – 2012 (June)
-
Journal of Occupational Safety and Health
35 9
Figure 8: Fatality rate per 100 workers from year 2007 – 2012 (June)
Conclusion
Owing to increase in complexity of operations, the palm oil industry has become more challenging
than ever before. Plantation companies are faced with the challenge of having to close monitor their
business to minimize occupational hazards, while simultaneously trying to sustain profits in a
competitive marketplace. In Malaysia, government agencies such as DOSH have done their part to
promote safety awareness in the industry in order to reduce accidents rate in workplace. However,
the key to proper safety execution is neither through strict guidelines nor stringent in enforcement,
but through an effective safety management initiative, first approved by an organization’s top
management, then integrated via specific safety management implementation tools and system, and
finally by continuous follow up and monitoring to ensure quality and continuous improvement. In
order to prove the commitment to sustainability, GENP has to ensure consistency in the adoption
and implementation of the OHSMS among Group operating units as only those companies that take
on aggressive safety management will prove the commitment to sustainability and guarantee the
improvement of work conditions, the decrease of occupational accident rate as well as lowering of
the occupational fatality rate.
Acknowledgement
The writer would like to thank the Senior Vice President – Group Processing, Genting plantations
Berhad for permission to present this paper...
8
Accident rate
per 100
workers
0.35 0.62 0.85 0.38 0.25 0.19
Fatality rate
per 100
workers
0.14 0.14 0.07 0.00 0.00 0.00
Remark: Data updated as at June 2012.
Figure 6: Statistic of occupational accidents recorded during last five years in GENP oil mills
Figure 7 clearly shows that there was significant decrease in accident rate since year 2009 after
implementation of Occupational Health and Safety Management System. Furthermore, the accident
rate of 0.38 and 0.25 per 100 workers recorded in year 2010 and 2011 were greatly lower than
national accident rate for the same period, 0.65 and 0.62 per 100 workers respectively.
Figure 8 shows the fatality rate per 100 workers from year 2007 to 2012 (June). It was clearly shows
that implementation of OHSMS proves the commitment to sustainability as GENP oil mills
continuously recorded zero fatal accident since year 2009.
Figure 7: Accident rate per 100 workers from year 2007 – 2012 (June)
-
Journal of Occupational Safety and Health
36 10
References
[1] Foreign Agricultural Service, United States Department of Agriculture, 2012, Oilseeds: World
Markets and Trade.
[2] Department of Standards Malaysia, 2005, Occupational Safety and Health Management Systems,
Part 1: Requirements.
[3] Department of Standards Malaysia, 2003, Occupational Safety and Health Management Systems,
Part 2: Guidelines.
[4] OHSAS Project Group, 2007, Occupational Health and Safety Management Systems –
Requirements.
[5] Patrick Hudson, 2001, Safety Management and Safety Culture The Long, Hard and Winding Road
(Edited by Warwick Pearse, Clare Gallagher and Liz Bluff). Occupational Health & Safety
Management Systems, 3-32.
-
Journal of Occupational Safety and Health
37 10
References
[1] Foreign Agricultural Service, United States Department of Agriculture, 2012, Oilseeds: World
Markets and Trade.
[2] Department of Standards Malaysia, 2005, Occupational Safety and Health Management Systems,
Part 1: Requirements.
[3] Department of Standards Malaysia, 2003, Occupational Safety and Health Management Systems,
Part 2: Guidelines.
[4] OHSAS Project Group, 2007, Occupational Health and Safety Management Systems –
Requirements.
[5] Patrick Hudson, 2001, Safety Management and Safety Culture The Long, Hard and Winding Road
(Edited by Warwick Pearse, Clare Gallagher and Liz Bluff). Occupational Health & Safety
Management Sy






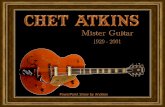

![CAN WING CHUN STUDENTS DEAL WITH BOXERS?€¦ · [1] MASTER JAMES SINCLAIR Founder of the UK Wing Chun Kung Fu Assoc. Began his martial art journey in 1972. June 2014 8th Edition](https://static.fdocuments.in/doc/165x107/5b350b297f8b9a3a6d8cb7a1/can-wing-chun-students-deal-with-boxers-1-master-james-sinclair-founder-of.jpg)





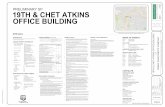
![INTERVIEW WITH JAMES SINCLAIR - UK Wing Chun · PDF file[1] MASTER JAMES SINCLAIR Founder of the UK Wing Chun Kung Fu Assoc. Began his martial art journey in 1972. September 2012 First](https://static.fdocuments.in/doc/165x107/5a7b9a027f8b9a2e358c04a7/interview-with-james-sinclair-uk-wing-chun-1-master-james-sinclair-founder.jpg)

