Journal of Hand Therapy v-15 N-2 2002
81
Transcript of Journal of Hand Therapy v-15 N-2 2002


1. The splinting issuePages 95-96Caroline W. Stegink Jansen, Gail N. Groth
Preview PDF (121 K) | Related Articles
2. A History of splinting: To understand the present, view the past,Pages 97-132Elaine Ewing Fess
Preview PDF (3870 K) | Related Articles
3. Lessons from hot feet: A note on tissue remodelingPages 133-135Paul Brand
Preview PDF (42 K) | Related Articles
4. Outcomes, treatment effectiveness, efficacy, and evidence-based practice: Examples fromthe world of splintingPages 136-143Caroline W. Stegink Jansen
Preview PDF (106 K) | Related Articles
5. Plaster of Paris: The forgotten hand splinting materialPages 144-157Judy C. Colditz
Preview PDF (1644 K) | Related Articles
6. A proposed decision hierarchy for splinting the stiff joint, with an emphasis on forceapplication parametersPages 158-162Kenneth R. Flowers
Preview PDF (81 K) | Related Articles
7. Static progressive splinting,
Pages 163-178Karen Schultz-Johnson
Preview PDF (3007 K) | Related Articles
8. The effect of the forearm support band on forces at the origin of the extensor carpi radialisbrevis: A cadaveric study and review of literature, , ,Pages 179-184Nicholas J. Meyer, William Pennington, Barb Haines, Roger Daley
Preview PDF (100 K) | Related Articles
9. The effect of corrective splinting on flexion contracture of rheumatoid fingers, ,
Pages 185-191Cecilia W. P. Li-Tsang, Leung Kim Hung, Arthur F. T. Mak
Preview PDF (101 K) | Related Articles
10. Minimalistic splint design: A rationale told in a personal style,
Pages 192-201Paul Van Lede
Preview PDF (1772 K) | Related Articles
11. Splinting materials old and new, , : Origins and application of bark cloth in upper extremitysplintingPages 202-204Gail N. Groth, Julius Kamwesiga
Preview PDF (571 K) | Related Articles
12. Introduction to a new method for inelastic mobilization,
Pages 205-209Nelson Vazquez
Preview PDF (806 K) | Related Articles
ScienceDirect - Journal of Hand Therapy, Volume 15, Issue 2, Pages 95-2... http://www.sciencedirect.com.lp.hscl.ufl.edu/science?_ob=Publication...
1 of 1 5/7/2009 11:54 AM

Splints have been in use for millen-nia. Medical workers in Egypt werecrafting them during the reign of thePharaohs. Even so, to catch a glimpseof a splint in public is, even now,always a little startling. It may evokeempathy and curiosity from a friendor cool appraisal and valuation from ahealth professional. What is itdesigned to do? Is it holding up well?Does it look comfortable, even artistic,or is it strictly functional and not at allattractive?
Even if a splint has great artisticappeal, its creation, utilization, andanticipated effectiveness must bebased on evidence. The topics selectedfor inclusion in this special issue areintended to advance the artistry ofsplinting toward an evidence-basedpractice approach.
Therapists have been charged withthe “responsibility . . . to examine thetheoretical grounding and evidenceunderlying” the techniques we use.1
Working to establish an evidence-based approach will not smother ourartistic creativity and freedom. Rather,increasing our base of evidence willensure that the utilitarian objects wecreate and prescribe will gain greaterappreciation.
The illustration on this page ex-presses our commitment to an evi-dence-based path, to an underlyingscience and theory of splinting, andforemost to improving the well-beingof our individual patients. The intentof the artwork becomes clear with a bitof interpretation.
The picture in the lower left cornerof the triangle represents the path toevidence-based practice. The verticalline represents the neutral dividingline between a positive and a nega-tive outcome of treatment. The hori-zontal lines represent individual pub-
lications that attempt to provide evi-dence of the effectiveness of the treat-ment. The judgment involved in evi-dence-based practice lies in the rela-tionship between the horizontal linesand the vertical line. The farther thehorizontal lines fall away from thevertical line, the more certain one canbe of a statistically significant effectof the treatment, either positive ornegative. If the horizontal line bisectsthe vertical line, the effect is not greatenough to be of statistical signifi-cance. The starred line at the bottomof all horizontal lines depicts theeffectiveness of all the horizontallines combined.
Figuratively, the left hand pictureshows that our goal in delivering this
issue to you is to increase the avail-able number of effective horizontallines at your disposal. The picture inthe lower right corner represents theunderlying science of splinting, be itbiomechanics, tissue response, or theoretic models of clinical reasoning.
The triangle indicates that all ele-ments are connected and that, ulti-mately, the rational base componentsserve the individual patient -- repre-sented in the top corner by the photo-graph of the young man. Dr. PaulBrand exemplifies these triangularlinkages in his description of the les-sons he learned in India from hot littlefeet!
Eleven authors volunteered to con-tribute their work to this issue of the
The Splinting Issue
April–June 2002 95
EDITORIAL
*
Edited by Caroline W. Stegink Jansen, PT, PhD, and Gail N. Groth, MHS, OTR, CHT

96 JOURNAL OF HAND THERAPY
Journal. This enormous wealth of tal-ent has provided a true potpourri ofsplint articles. Elaine Fess gives us athorough review of the history anddevelopment of splinting. CarolineJansen seeks to stimulate debate onthe evidence for splinting. Theoreticalgorithms for splinting choices areproposed in separate papers by KenFlowers and Karen Schultz-Johnson.
Clinical practice is also well repre-sented. Cecilia Li and her colleaguesprovide experimental evidence for theefficacy of splinting for patients withfinger contractures. Nicholas Meyerand colleagues present a study of theefficacy of the mechanism of thecounter-force braces used for patientswith lateral epicondylitis.
The practice of splinting is furtherenriched by Judy Colditz, who des-cribes the use of plaster of Paris, andGail Groth, who shows how barkcloth is used. Nelson Vasquez des-cribes a new technique to provide ameasured static stretch in a splint
design. Paul van Lede introduces analgorithm that promotes the conceptof “minimal” splint design.
The flow of the articles is such thatpapers with a theoretical orientationalternate with papers that have amore direct practical orientation, sothat the reader can see clearly theclose links between clinical practiceand theory. As guest editors, weclaim no special honors as splintmakers. We feel humbled and privi-leged to have been given this chanceto stimulate the creation of this spe-cial issue of the Journal. Ken Flowers’foresight and gentle persistence haveprovided vital support in the compo-sition and completion of the issue.We also want to thank RebeccaRobinson, ELS, at Hanley & Belfus,for her skillful and dedicated work.
We hope that this issue will stimulate therapists in clinical andresearch capacities to apply the theory, evidence, and art of splintingto the care of current and future
patients entrusted to us. An evidence-based approach will only support ourartistic creativity and freedom!—CAROLINE W. STEGINK JANSEN, PT, PHD,AND GAIL N. GROTH, MHS, OTR, CHT
The editors thank Alex McLaughlin, OTR,Lewis Milutin, and Josue Andrade, fromShriners Hospitals for Children, Galveston,Texas, and Hollie Hackett, University ofTexas Medical Branch, also in Galveston,for their contributions to the illustrationthat appears on the previous page.
References
1. Harris SR. How should treatments becritiqued for scientific method? PhysTher. 1996;76:175–81.
2. Fess EE, Philips CA. Hand Splinting:Principles and Methods. 2nd ed. St.Louis, Mo.: Mosby, 1987.
Correspondence and reprint requests toCaroline W. Stegink Jansen, PT, PhD, Uni-versity of Texas Medical Branch, School ofAllied Health Sciences, Dept. of PhysicalTherapy, 301 University Blvd., Galveston, TX77555-1144; e-mail: <[email protected]>.

April–June 2002 133
Few persons have contributed more to our understanding of biomechanics and soft tissue response to stress thanDr. Paul Brand. Historically, enlightened physicians and bracemakers have, for centuries, advocated slow, gentle tension toeffect change in soft tissue, but their opinions were based on indi-vidual trial-and-error observations. This lack of organization andscientific validation made their teachings vulnerable to contra-dictory, opposing practices that promoted harsh manipulation toeffect soft tissue change. Confusion flourished for centuries. Incontrast to early practitioners, Dr. Brand transferred his vastclinical experience and empirical understanding of soft tissueresponse to stress to the biomechanics laboratory to provide afoundation of knowledge based on scientific inquiry.
His subsequent work has served as a foundation for expandingunderstanding and investigation into the histologic and bio-mechanical basis for soft tissue response to stress. Dr. Brand’swork is closely entwined with contemporary splinting theory andpractice. His straightforward teaching style and exceptional abil-ity to translate difficult biomechanical and physiologic constructsinto easily understood concepts facilitate learning for surgeonsand therapists alike.
Innovators often are able to identify watershed experiences thatforever changed their thinking. Distinguishing the insights thatsuch events bring has two-fold importance, in that both truth andprocess are better appreciated. I had heard Dr. Brand describe thesequence of events that altered his understanding of soft tissueremodeling and asked him if he would write about these experi-ences for my article on the history of splinting (see p. 113). Hewillingly agreed, and I soon received a beautifully written narra-tive. On reflection, I realized that it would be a great disservice tobury this important account in the middle of my history article.
This letter is not exclusively about correcting clubfoot problems.It is relevant to all those who work with healing tissues and seekto influence the soft tissue remodeling process. It is the base onwhich splinting endeavors are founded. With Dr. Brand’s per-mission, Caroline Jansen’s support, and the creativity of theHanley and Belfus editor, Rebecca Robinson, Dr. Brand’s letteris presented here as a stand-alone piece in this special issue of theJournal. Read, enjoy, contemplate!—ELAINE EWING FESS, MS, OTR, FAOTA, CHT
DR. BRAND WRITES:—In 1944, I worked as FirstAssistant to Sir Denis Browne at the Great OrmondStreet Children’s Hospital in London. Denis Brownehad become quite famous for his management of club-foot, particularly talipes equinovarus, so we got a verylarge number of these cases. I was responsible for thefollow-up clinic.
Denis Browne was a large man with large hands,and most of the patients he saw were within days ofbeing newborn. His idea was that if the child wasseen early, he would correct the deformity complete-ly the very first time the child was seen. His methodwas to correct the three deformities of each foot, onedeformity at a time. First he would correct themetatarsus varus at the level of the mid-foot. Then,when the foot was straight in a length-wise direction,he would correct the varus deformity of the hind footto bring the os calcis directly under the ankle. Finally,he would correct the equines deformity, and for thiscorrection it was important not to use the foot as alever to stretch the tendo achilles, for fear he wouldbreak the mid-foot. So Denis Browne would put hislarge thumb under the full length of the sole of thefoot to preserve the arch of the foot while he pushedthe foot up into a right angle position or higher.
In all these maneuvers, as I watched him, it wasobvious that he was breaking little ligaments andcausing at least minor cracks in bones like the talus.The skin on the medial side of the foot had to bestretched, and sometimes little cracks appeared inthe skin. I did not like watching this manipulation,because it seemed to me that it was just too violent.However, it did finish up with a foot in a normal rela-tionship to the leg and the sole of the foot in the rightposition for walking in shoes.
However, at that early stage we did not put shoeson the foot, but we used the Denis Browne splint—which, as you know, has an aluminum soleplate and,at right angles to that, an aluminum sidepiece that
Paul Brand, MDClinical Professor EmeritusDepartment of OrthopaedicsUniversity of WashingtonSeattle, Washington
Lessons from Hot Feet:A Note on Tissue Remodeling
Correspondence and reprint requests to Paul Brand, MD, 1026California Lane SW, Seattle, WA 98116.

goes up to a little above the ankle. The newly manip-ulated foot was strapped onto the soleplate withadhesive strapping, and then to the lateral uprightplate. When both feet had been strapped to their ownsection of the Denis Browne splint, then the two feetwere each attached separately to the crossbar thatheld the two feet parallel to each other.
Within a week, I had to see the baby at the follow-up clinic and take off the old strapping and reapply itin the same position. The reason for doing the strap-ping over again was that the foot had swollen gross-ly inside the first adhesive strapping, and any partthat was not covered bulged out.
Anyway, we went on reattaching the splint withfresh strapping every week for a few weeks and thenevery two weeks until the swelling had gone down.
All this time, the baby had been kicking its legs, asany baby will do, and as one foot kicked downward,the other foot was being withdrawn, and the DenisBrowne splint thrust the feet into inversion and eversion because of the bar that connected the twofeet. This undoubtedly kept the subtalar joint and theankle joints in congruity with each other, but thesewere the only joints that kept moving. The mid-tarsaljoints were constantly kept in the same relationshipto each other by the soleplate of the splint.
I had to follow these babies up to the stage whenthey were ready to begin standing and walking, andthen they had to be fitted with little boots.
As these young children grew and as they learnedto walk freely, they were able to move a little at theankle joints and some at the subtalar joint, but thefoot as a whole remained straight and rather rigidindefinitely.
I was required to keep track of these feet until thechildren were 12 years old, at which stage I would beseeing them about every 6 months.
Having become very accustomed to observinghundreds and hundreds of these baby clubfeet at allstages of development, my hands became very accus-tomed to feeling the feet and became aware of thosewho were doing well and of those who perhaps didnot do so well.
When I went to India in 1946 and started a clubfootclinic, I taught my assistants to do the manipulationand correction just as I had been taught by DenisBrowne. I was able to get plenty of aluminum sheath-ing from the wings of an airplane that had crashed afew miles away from Vellore. I hired a mechanic touse this aluminum sheathing to make Denis Brownesplints, and everything seemed to be going well.
However, among the patients who came to myclinic in India (and unlike the patients whom I saw inLondon), there were several teenagers who had beenborn with clubfoot, but no attempt had ever beenmade to correct them. They came to me walkingeither on the lateral side of the foot or even on thedorsum of the foot. I was interested to know whether
one could do manipulation on these late older casesor whether one would have to operate on them.
I began by trying to manipulate the feet, at leastpart way toward full correction. This meant that Ihad to handle these feet and feel them and feel themobility. To my astonishment, I found that theseuntreated clubfeet of the older children felt cool tothe touch and had surprising range of motion of allthe joints, even though the range of motion was froma deformed position and was not enough to correctthe deformity. I remember being astonished at thecontrast between the texture and temperature of thefeet I was now seeing in children aged 10 or 12, com-pared with the feet of children who had been throughDenis Browne’s treatment, which were corrected inposition but so stiff and so hot compared with theuntreated feet I was seeing in India.
I felt at once that the Indian feet were better feet thanthe ones we had treated in England, even though theones in England were straight and in a better shape. Ifelt convinced that there was something fundamental-ly wrong about all those patients in London. I won-dered whether we could treat the Indian patients in away that would not cause the inflammation and thedamage to ligaments and to some bones that had beenthrust upon the babies in London.
I felt that we had to be slow, and we also had to begentle. I hoped that we could achieve this by a gentlecontact manipulation keeping within the limitsimposed by pain, and then by using total contactplaster casts to hold the partially corrected positionfor a week or so. Then we would remove the cast,manipulate a little more, and apply a new cast. Ihoped that the improvement gained by moderatecorrection at the beginning of the week would loosenup and allow further improvement that would bemaintained by the next cast.
Now, I had several doctors to assist me at the club-foot clinic, and I taught each of them the technique oflittle-by-little manipulation and plaster casts, but Ifound it very difficult to explain exactly what I meantwhen I said they had to be gentle. How do you meas-ure gentleness? We were not using anesthetics for themanipulation and plaster casting. So we tried sayingthat if the baby cried, that meant the manipulationwas too strong. However, some babies cried for noreason other than the strange atmosphere of the clin-ic and the white coats of the doctors. We had todevelop an answer for that as well.
We told the mothers not to feed their babies in themorning before coming to the clinic. So the waitingroom where the mothers and the babies were waitingfor their turns for treatment was full of screamingbabies feeling hungry and not being allowed to gothe breast. As soon as each baby’s name was called,the mother would take it to the treatment room andsit herself on a stool opposite the doctor. The oldplaster casts had been taken off, and now the baby
134 JOURNAL OF HAND THERAPY

was allowed to go to the breast and start sucking. Fora time the baby’s whole interest was to satisfy itshunger. This allowed the doctors to begin feeling thefoot and moving it gently into its best new position.
I told the doctors that if the baby remained happyhaving its meal, that meant that they hadn’t pushedhard enough on the foot to correct the position. Onthe other hand, if they pushed much harder, the babymight let go of the nipple and start to scream, andthat meant that they had used too much force. Theideal moment for the manipulation was when thebaby showed it recognized that something unpleas-ant was happening to its foot, and it turned its eyesand looked at the doctor without letting go of thenipple. At that moment, the doctor should hold theposition and apply the plaster cast.
This resulted in some teasing among the doctors,because when a baby yells, everybody can hear it,and the other doctors would know that the doctordealing with that baby had gone too far and used toomuch force.
We used Denis Browne’s methods of correcting thethree deformities in sequence, and we switched fromplaster casts to Denis Browne splints as soon as a fullcorrection had been achieved by serial casting. Butthe real joy and satisfaction came after a few years,when I was able to compare the feel of the 6-year-oldand the 10-year-old feet with my memories of the feelof same-age feet in London. Not only were our feet inIndia in a normal position (as the London feet hadbeen), but they were mobile and they felt cool and softto the touch.
April–June 2002 135

The movements of outcome research and outcome-based management of health care and the cry to armsfor evidence-based practice arose in the 1990s,1,2 whenaccountability for treatment procedures was advocat-ed in an effort to stem rising health care costs.Urbaniak, in his presidential address to the AmericanSociety for Surgery of the Hand, urged members of thesociety to present outcome studies to demonstratephysician accountability to the public and support thehistorical trust between the patient and treating physi-cian in a contemporary way.3 However, calls for out-come studies and evidence-based practice leave manytherapists bewildered. What constitutes the evidencefor evidence-based practice? How do such terms as“evidence-based practice,” “treatment efficacy,”“treatment effectiveness,” and “treatment outcomes”relate to one another? Is evidence-based practice evenuseful for practicing clinicians, or is it just an addition-al administrative burden?
The purpose of this paper is to review terms relatedto outcome research and evidence-based practice inthe context of the practice of splinting used in handrehabilitation. The objectives of the paper are to 1)review the structure of outcome reports and research;2) describe the background and discuss the terms
“treatment efficacy,” “effectiveness,” and “evidence-based practice”; 3) discuss these concepts as theyapply to selected studies found in the literature thatreport the use of splints for patients with ailments thataffect the use of their hands; and 4) provide somereflections that place these terms in the context of sci-entific inquiry and clinical practice. The splint exam-ples were chosen as illustrations, not to provide a com-prehensive review of the current state-of-the-art of theeffectiveness of splinting for hand rehabilitation.
STRUCTURES OF OUTCOMERESEARCH
In their simplest form, outcomes are results meas-ured after an intervention.4 The outcome approachaims to describe the outcomes of everyday practice,but it encompasses more than just the gathering of allpossible data that may affect a patient’s response tointerventions.5 An outcome approach is a prospec-tive activity of data collection. The goal is to isolatethe relationship between the outcomes of interest andthe treatment provided, by controlling for the effectsof other relevant material.5
Investigations may include topics of quality assur-ance, such as contrasting the outcomes when differentdevices are used, contrasting outcomes in differenttreatment settings, different health care disciplines, oreven different health care providers.
Outcomes, Treatment Effectiveness, Efficacy,and Evidence-based Practice:
Examples from the World of Splinting
Caroline W. Stegink Jansen, PT, PhDUniversity of Texas Medical BranchSchool of Allied Health SciencesGalveston, Texas
ABSTRACT: Calls for outcome studies and evidence-based prac-tice leave many therapists bewildered as to the meaning of varioustypes of terminology. The objectives of this paper are to 1) reviewthe structure of outcome reports and research; 2) describe the back-ground and discuss the terms “treatment efficacy,” “effectiveness,”and “evidence-based practice”; 3) discuss these concepts as theyapply to selected studies found in the literature that report the useof splints for patients with ailments that affect the use of theirhands; and 4) provide some reflections that place these terms in thecontext of scientific inquiry and clinical practice. It is concludedthat health care is being reviewed on an increasingly more system-atic and grand scale. While studies that include large numbers ofsubjects are needed to substantiate the effectiveness of splinting,studies involving smaller numbers of subjects can contribute great-ly as well, so long as they are performed with the highest level ofstudy design and use standardized outcome measures that arevalid for answering the designated research questions. J HAND THER. 2002;15:136–143.
136 JOURNAL OF HAND THERAPY
Correspondence and reprint requests to Caroline W. SteginkJansen, PT, PhD, University of Texas Medical Branch, School ofAllied Health Sciences, Dept. of Physical Therapy, 301 UniversityBlvd., Galveston, TX 77555-1144; e-mail: <[email protected]>.

During the outcome approach, participating par-ties proactively reach a consensus about the concep-tual model of the data gathering, including how toanalyze and use the acquired data.5,6 The partiesfocus on the data collection and decide what dataamong a myriad possible data points are crucial fordescribing the outcomes.
The question arises about what outcome measuresto use to conduct an outcome study. The OutcomeIssue of this Journal, published last year (April/June2001), elegantly describes the various forms thatmeasured outcomes may take. Following the modelof disablement described by the World HealthOrganization, outcome measures may include suchmeasures as grip strength and range of motion(impairment) and measures that reflect the opinionsof patients, such as perceived symptom severity.7
The organization of outcome studies can be adaunting task, because many outcome studiesinclude large numbers of subjects. MacDermid et al.8
included 250 subjects in their outcome reports ofpatients with distal radius fractures. The Mainecarpal tunnel outcome study9 included 467 subjectseligible for surgical treatment and 240 subjects eligi-ble for non-surgical treatment. Twenty-six surgeonsperformed the carpal tunnel releases. With the orga-nizational challenges of completing a study of thisnature, it is crucial that only pertinent data are select-ed. Because of the proactive nature of outcomeresearch, less effort is wasted on the collection of datathat will not be used later.
An informative study that was performed prior tothe outcome movement shows what opportunitiesmay be missed if outcomes are collected without aplan for analyzing contributing factors. This prospec-tive outcome study, performed in South Africa byEdinburg et al.,10 reports results for patients whowere treated by a program of protective range ofmotion after flexor tendon surgery in zone II of thehand.
The 42 participating patients were manual laborers,living far from the hospital. The surgical repairs wereperformed by junior surgeons. For the mobilizationprogram, the authors used a cast rather than a thermo-plastic orthosis. The hands of the patients were placedin dorsal plaster splints, with the wrist in 60° of flex-ion, the metacarpophalangeal joints in 40° to 60° offlexion, and the interphalangeal joints in a neutralposition. A Steinmann pin was embedded in the castto serve as a palmar bar for the achievement of full fin-ger flexion when rubber-band traction was applied.
Unfortunately, no control group or other compari-son group was included in the study. The authorsconcluded that their results were similar to those ofpublished studies, despite the fact that the patientslived in rural areas and had limited access to follow-up care. The authors praised this treatment programbecause it allowed the patients to be more independ-
ent, requiring fewer hospital visits and less supervi-sion by therapists.
All these conclusions were opinions of the authorsbased on their empirical judgment. Had the authorsprospectively planned to address these issues in theirstudy and planned statistical analysis of their data,they could have reported the effects of the servicedelivery in a more scientific way. Would it not havebeen useful if we had evidence that an early motionprogram not only improves motion of the injuredhand but also makes the patient less dependent on thecare delivery system?
Kane5 describes the basic model of an outcomestudy as a mathematical formula, namely:
Outcomes = function of (baseline, patient clinicalcharacteristics, patient demographiccharacteristics, treatment, setting of care)
Statistically, a regression analysis can be performed toanalyze the contributions of each factor. But the avail-able number of patients limits the number of factorsthat can be included in the model if the statistical analy-sis is to be meaningful. This is the reason a consensus isneeded to determine the conceptual model that is validto describe the outcomes in the most efficient way.
Kane categorizes contributing factors, in their sim-plest form, as clinical factors (severity of disease,duration, etiology, comorbidity, and baseline status),patient factors (age, gender, occupation), treatmentfactors (which may include a combination of treat-ments and treatment setting), and outcomes (symp-toms, function, quality of life, complications). Treat-ments may be applied in randomized clinical trialsbut are often delivered in a more natural, scientifical-ly less well controlled study design.
Tarlov et al.6 include characteristics of the patientand the caregiver alike. These authors divide themodel into three categories—structure of the care(delivery system characteristics, provider characteris-tics, and patient characteristics), process of the care(technical style, including the provided treatmentand interpersonal style), and outcomes of care (clini-cal end point, functional status, general well-being,and patient satisfaction with the care).
An example of structured outcome research is theMaine carpal tunnel study by Katz et al.9 This studycompares outcomes after open and closed carpal tun-nel release surgeries and compares surgical and non-surgical treatments of carpal tunnel syndrome. Thenonsurgical treatments included medical treatmentwith anti-inflammatory medications, corticosteroidinjections, and wrist splints (93% of patients). The out-come measures included patient self-reports in sur-vey format, the symptom severity and functional sta-tus scale,11 and measures of quality of life, patientsatisfaction, scar tenderness, and work status.
Scientific controls, such as proactive randomassignment of study subjects, could not be applied in
April–June 2002 137

this case, and existing groups of patients were used.The study elaborated descriptions of patient charac-teristics to indicate the equivalence of surgical andnonsurgical groups.
The study concluded that surgical treatment result-ed in optimal patient outcomes. However, the modelmay have been biased against nonsurgical treatments,because all forms of nonsurgical treatment werelumped together, and no analysis was performed toanalyze the interactions between the nonsurgicaltreatments and the methods by which they were pro-vided. For instance, the position of the wrist in thesplints was not described, even though wrist anglemay significantly affect intracarpal canal pressure.12,13
This example illustrates the strength of outcomeresearch in reporting many patient characteristics, butit also shows the limitations. Because of the broaddescription and possible variability in the technicalperformance of treatments by the many participatinghealth care professionals, as well as the interaction ofvarious splint designs and medical treatments, noconclusive evidence could be provided to support theeffectiveness of the use of splints.
EFFICACY AND EFFECTIVENESS OF TREATMENT
How, then, does a practicing clinician gather evi-dence that a chosen treatment is the best currentoption available for a specific patient and that it iswithin the realm of the skills of the therapist? Twoissues play a role—the efficacy of treatment and theeffectiveness of treatment.
The efficacy of an intervention is its effects in thebest possible circumstances.14 In a study of efficacy,all conditions are optimal, from the randomizedstudy design to the skills of the therapists and thecharacteristics of the subject sample. The aim of sucha study is to demonstrate the capability of the inter-vention to benefit the described patients, in compari-son with a control group of patients who receive notreatment or standard treatment.
The potential of an intervention to benefit a patientunder ideal conditions should be tested before theeffectiveness of the treatment is tested under a varietyof treatment conditions, because the effects in real-life studies may be less dramatic than those in ideal-condition efficacy studies. In real life, increased vari-ability among subjects, the skills of clinicians, andother confounding factors may make it more difficultto reach statistical significance to substantiate thebenefits of the intervention.
Studies of the effectiveness of treatment look at theeffects of an intervention on measured outcomes inordinary clinical practice, and may include the effectsof the treatment, the effects of clinicians’ skills, thequality of service delivery, cost effectiveness, andpatient characteristics.2
An example of an efficacy study is the study byStrickland and Glocovac15 on the efficacy of a passiveearly mobilization program for patients after surgicalrepair of flexor tendons in zone II of the hand. Thesubjects were 37 patients with 50 injured fingers. Theselection criteria for the subjects were stringent, sothat the study would include only patients withclean-cut flexor tendons and no concomitant injuries,such as fractures. The same experienced surgeon per-formed all the surgeries.
The postoperative treatment and the positioning ofthe Orthoplast splint were described in detail, as wasthe passive motion program. The authors stated thatthe groups were the same at the beginning, but theydid not describe how the patients were assigned tothe two treatment groups (immobilization and earlycontrolled mobilization). Random assignment wouldhave meant that other, uncontrolled patient charac-teristics could have been similar between the twogroups.
The results showed that, under the ideal treatmentconditions, the patients in the early motion groupregained better active range of motion than did thepatients who were treated with immobilization.
An example of an effectiveness study on the sametopic is the retrospective cohort study by Jansen andMinerbo in which the effectiveness of early mobiliza-tion using the Kleinert and Duran technique wascompared with the effectiveness of treatment withimmobilization in a cast or splint for patients withsurgical repairs in zone II of the hand.16
Existing groups of subjects were included over2 years. A variety of treating physicians, who referredpatients to a private clinic, made the treatment choiceaccording to their clinical preferences, and a variety oftreating therapists chose the manner of splint fabrica-tion and the rehabilitative treatment. The rater wasnot blinded to the treatment group.
In this real-life context, the range of motionattained by patients treated with early mobilizationwas found to be better than the range of motionattained by the immobilized patients.
The data were collected in the 1980s. At that time,quite a few physicians still preferred treatment withimmobilization to early mobilization, so no systemicdifference in patient characteristics was observed.Because of the lack of random assignment, factors thatwere not under the control of the therapist or thephysician may have contributed to the results.
EVIDENCE-BASED PRACTICE
Justification and Definitions
Evidence-based medicine is a movement that start-ed in Canada at McMaster University. Sackett et al.,1
early leading authors in the field, defined evidence-based medicine as the conscientious, explicit, and
138 JOURNAL OF HAND THERAPY

judicious use of current best evidence for makingdecisions about the care of individual patients. In thesecond edition of their book Evidence-based Medicine:How To Practice and Teach EBM, the definition retainsits simplicity but adds an important dimension:Evidence-based medicine is the integration of bestresearch evidence with clinical expertise and patientvalues.17
The concept of evidence-based practice has beenexpanded to include “evidence-based health care,”2
with components such as evidence-based policy, pur-chasing, management, practice, and patient choice.
Sackett et al.1 justify the need for evidence-basedmedicine on the following basis: The growth of newevidence for treatment effectiveness (beneficial orharmful) is exponential in our time, so that we cannotsafely base our practice on our old knowledge.Sackett et al.1 report results of a survey of partici-pants in medical rounds, which showed that manyfailed to read clinical scientific materials, and thosewho did read them spent less than an hour a daydoing so.
Our current knowledge and practice patterns thusdeteriorate with years of practice. Traditional contin-uing education models may not been able to stemthis tide. The constant effort by clinicians to obtainthe best available evidence and incorporate this evi-dence into daily practice is a preferred mechanism toensure that the advances in health care will reach thepatient through clinicians who use the best currenttreatment.
An important feature of evidence-based practice isthat systems exist18,19 to grade the quality of evidenceand the strength of treatments recommended on thebasis of that evidence. The strategy for seeking evi-dence to support a treatment is to find the highestlevel of evidence, the gold standard being the double-blind randomized clinical trial. If that type ofevidence is not available, the health care provider willcontinue down the path of available evidence to findthe best current external evidence for the treatment.1
All levels of clinical study designs can provide evi-dence for a clinician, but not all carry the same weightin the ranking system. For instance, a well-designedsingle-case study can provide evidence about treat-ment effectiveness, but its evidence is not as strong asthe evidence provided by a double-blind randomizedtrial.
What if evidence cannot be found? This does notmean that the treatment cannot be efficacious, but itdoes mean that work still needs to be done to provideevidence of the benefit of the treatment. Some practi-tioners fear that third-party payers may misuse evidence-based practice by equating lack of evidencewith ineffectiveness of treatment.1,2
Definitions vary for ranking the quality of treat-ment evidence and, consequently, for ranking thestrength of recommendations to support treatmentfor clinical practice. Tables 1, 2, and 3 show rankorder definitions of the quality of research and thestrength of treatment recommendations. The lowerthe ranking number, or the earlier in the alphabet theranking letter, the more confidently the study resultscan be included as evidence.
Most systems rank the findings of the double-blind randomized clinical trial as the highest evi-dence. However, some systems require more thanone double-blind randomized trial and, as highestevidence, a number of such studies all in agreementin support of a treatment.
April–June 2002 139
TABLE 1. Relationship Between Rank Order of theLevel of Evidence and Grade of Treatment
Recommendation18
Level of Evidence Grade of Recommendation
Level I: Large randomized trial Grade Awith clear results (low risk of error/high power)
Level II: Small randomized trial Grade Bwith uncertain results (high risk of error/low power)
Level III: Non-randomized, Grade Ccontemporary controls; non-randomized, historical controls; no controls, case series only
TABLE 2. Quality of Evidence*
Level I: Properly randomized controlled trial
Level II.1: Well-designed controlled trial without randomization
Level II.2: Well-designed cohort or case control analyticalstudy
Level II.3: Time series with or without the intervention or dramatic results in an uncontrolled experiment
Level III: Opinion of respected authority, descriptive study or case report, or report of expert committee
*The lower the number of the study level, the stronger the quality of the evidence19; level I evidence is strongest.
TABLE 3. Grading the Strength of the TreatmentRecommendation*,19
A: Good evidence to support recommendation for the use of the intervention
B: Fair evidence to support recommendation for the use of the intervention
C: Insufficient evidence to support recommendation for the use of the intervention
D: Fair evidence to support recommendation against the use of the intervention
E: Good evidence to support recommendation against theuse of the intervention
*The closer the letter grade to the start of the alphabet, the strongerthe recommendation for use of the intervention (e.g., A is strongerthan B, B is stronger than C, and so on).

In the ranking provided by Pinsky et al.,19 the opin-ion of experts is included in the ranking. These authorsalso recognize that, on investigation, treatment may befound to be harmful, and they provide the ranking fora recommendation system that includes the beneficialand harmful effects of treatments.
Dissemination of the Evidence
For a clinician, the issue of the demands of dailypractice comes to mind. With the enormous amountof information available in published form, both inprint and on the Internet, how can a clinician stayabreast of current evidence?
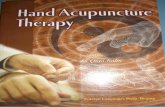
Archie Cochrane, MD, realized the need for profes-sionally performed reviews to collect evidence, pre-vent the loss of evidence, and convey the evidence inthe most time-efficient way to clinicians. The firstadvantage of a systematic review is that the effec-tiveness of a treatment as expressed in multiple stud-ies is summarized in one manuscript. Second,Chalmers et al.20 found that pooling the effects ofmany studies in a systematic review can statisticallysupport treatments, even when not all participatingstudies reach the level of statistical significance.14 Theofficial logo of the Cochrane Collaboration expressesthe advantage of pooling the effects of many studiesin systematic reviews of treatment effectiveness(Figure 1).
Many review databases now exist, including theCochrane Library and the Database of Abstracts ofReviews and Effectiveness.14 In 1989, the U.S. gov-ernment established the Agency for Health Care
Policy and Research, with the Forum for Quality andEffectiveness in Health Care operating under itswing.21 Evidence-based journal clubs, like that pub-lished by the American College of Physicians, alsofacilitate the sharing of results.22
Study results may be systematically reviewed in aqualitative, narrative way, but they are often describedin a mathematical, quantitative way, in a meta-analy-sis study. Systematic reviews may be performed byindividual authors, but organizations like the CochranCollaboration have established teams of reviewerswho collaborate to complete systematic reviews.
A nice example of a systematic review is a meta-analysis study published by Lacasse et al.,23 whichevaluates the pooled effects of 11 studies of respirato-ry rehabilitation for patients with chronic obstructivepulmonary disease. Each study had a small numberof subjects, ranging from 7 to 32. The combined stud-ies, however, included 309 subjects! All but one studyhad a concealed randomized design. Six studies usedblinded assessment of all outcomes, three appliedblinding for most outcomes, and two did not blind therater from the group assignment. Three studiesshowed statistical benefit of the intervention, and ineight studies findings did not reach statistical signifi-cance. The studies in which findings did not reach sta-tistical significance did, however, show a mathemati-cal effect, and when the results of all 11 studies werepooled, statistically significant support for the treat-ment was substantiated.
This illustrates the strength of pooling results whenmultiple studies ask the same research question, evenwhen each study by itself does not have a large sam-ple size. The pooling of results does require, though,that studies be performed at the highest possibledesign level, in formats that are acceptable for inclu-sion in a systematic review, and that standardized,uniformly accepted outcome measures are used thatare valid for answering the research question.
Performing a systematic review is a labor-intensivetask, because an effort must be made to locate all liter-ature that investigates the topic, rank the studies, andidentify those studies with the most scientific strengthfor the review. Many studies are performed in waysthat are not scientifically controlled, or they use non-standardized outcome measures, making review diffi-cult and the pooling of results impossible.
Only one completed systematic review was foundthat involved the use of splints. The study is entitled“Orthotic Devices for Tennis Elbow.”24 Of 788 studiesaddressing the treatment of tennis elbow, obtainedby a variety of computer searches of medical andallied health databases as well as by hand searching,only 17 eligible studies were found that met theinclusion criteria for the systematic review and only5 randomized clinical trials were found. Variousquestions were addressed, such as comparison of dif-ferent types splints, including a wrist splint, forearm
140 JOURNAL OF HAND THERAPY
FIGURE 1. Official logo of the Cochrane Collaboration. Resultsdisplayed are based on a study by Chalmers et al.20 Each hori-zontal line represents the results of one trial (the shorter the line,the more certain the results), and the diamond represents thecombined results of all seven studies. The vertical line indicatesthe position around which the horizontal lines would cluster ifthe two treatments had similar effects. Where the horizontal linetouches the vertical line, it means that that particular trial foundno clear difference between treatments. The position of the dia-mond to the left of the vertical line indicates that the treatmentstudied is beneficial. (Courtesy of The Cochrane Collaboration.)

band, and lateral epicondylitis clasp. Different out-come measures were included in the review, such aspain-free grip strength. The authors stated that theycould not pool the effects of the studies because of theheterogeneity of study designs and outcome meas-ures. In the end, despite the enormous number ofpublications about the treatment of tennis elbow, nodecision could be made on the effectiveness of splint-ing as a treatment for it. The authors suggested morewell-designed clinical trials and the developmentand acceptance of standardized outcome measures.
DISCUSSION
This paper reviews outcome studies—studies ofefficacy, effectiveness, and evidence-based practice—and provides examples from the world of splinting toillustrate the topics. The definitions and the practice ofevidence-based health care are still developing.25
Outcome research and evidence-based practice, as thephrases imply, are concerned with the end results ofinterventions and do not emphasize significant devel-opmental hallmarks along the way.
How results from the entire field of research areincorporated in the ranking of evidence is not clear.Where, for example, can rankings be found for infor-mation gleaned from animal studies that investigatemechanisms of disease or treatment?26,27 Even thoughSackett18 indicates that our best evidence may bederived from animal studies, the subsequent defini-tions of the quality and the strength of evidence donot include animal studies and rely solely on clinicalstudies of patients. Where is the unifying conceptfrom the disablement model of the World HealthOrganization, which shows that micro-occurrences ona cellular level as well as issues of societal impact,such as access to health care, all contribute to thehealth and well-being of the world’s population?Where is the place for theory development28 in a pub-lished format, or for projects that demonstrate themechanism of an intervention?29,30
An example of this predicament is the elegant lineof research that runs through the history of the treat-ment of flexor tendon injuries in zone II of the hand.In 1948, Bunnell31 dramatically stated the problemthat plagues the field of tendon repair in the hand.He reported failures of surgical repairs in the areabetween the distal crease of the palm and a line justpast the middle crease of the finger. The failuresoccurred not because the tendon was not solidlyrepaired but because adhesions formed around therepair and surrounding tissues. As a result, no ten-don excursion took place and finger movement failedto occur.
Duran and Houser32 hypothesized that a gliding ofthe repaired tendon between 3 and 5 mm would be suf-ficient to prevent formation of these adhesions. Howwould this early motion best be applied, and howmuch load should be placed on the healing tendon?
The use of a cast or splint regimen in postoperativeearly motion treatment has been an ongoing focus ofstudy since then. To review the entire rich develop-ment in detail would go beyond the scope of thispaper, but the line of research includes basic scienceby Gelberman et al.26,27 showing the superior qualityof healing of the tendon in dogs after application ofan early motion program; electromyelographic test-ing of the finger flexor and extensor musculatureduring the splint regimen30 and placement of metalmarkers in the repaired tendons of patients to meas-ure actual achieved tendon excursion33 to support themechanism of the treatment; and various descrip-tions of results.34,35 However, from this rich researchline, only a few studies use control or comparisongroups15,36 in patient reports. Thus, few studies maybe eligible for inclusion in a systematic review, butcan we say that the other authors did not seek evi-dence for their practice?
Figure 2 shows an organization model of the rela-tionships between clinical expertise and scientificefforts to form the basis for treatment interventions.Science, clinical expertise, and patient values and pref-
April–June 2002 141
FIGURE 2. A model of relationships between clin-ical practice where it all happens, and the scientificapproaches that help make it all happen.

erences are mutually influential factors, as indicatedby the double arrows in the model. Future debates willdecide how the clinicians, scientists, legislators, pay-ing communities, and well-informed patients delin-eate the roles and importance of all aspects of scientif-ic, applied inquiries and clinical practice.
CONCLUSION
Health care is being reviewed on an increasinglygrand and more systematic scale. Our work is beingreviewed systematically even if we are not aware ofit, so taking the lead by conducting high-qualitystudies and disseminating the results of our studiesto the world of health care at large is crucial. We stillhave work to do to substantiate our interventionsand to publish results so that they can easily be foundon computer searches, as in the Journal of HandTherapy, the Journal of Hand Surgery, our AOTA andAPTA scientific publications, and others.
Studies that include large numbers of subjects arehelpful. But studies involving smaller numbers ofsubjects can also contribute greatly so long as theyare performed with the highest level of study designand use standardized outcome measures that arevalid for answering the designated research ques-tions. Great contributions to standardization of meas-urements have been made by the ASHT in publica-tions like their Clinical Assessment Recommendations37
and the Journal of Hand Therapy. The inclusion of hand therapists in review teams,
such as those of the Cochrane Collaboration, is ofgreat importance for posing questions relevant to thefield of rehabilitation of the upper extremity and formaking a team of reviewers aware of the state of theart of outcome measures in our field. Our hand ther-apy community includes practitioners in all areas ofhand rehabilitation—theoretical thinkers, practition-ers, and trained researchers—and we thus have theexpertise to collaborate as members of review teams.
Mike25 places a burden of responsibility on allhealth care professionals and at the same time allevi-ates a sense of despair we may feel because we stillseem to have so far to go. In her paper entitled “Out-come Research and the Quality of Health Care: TheBeacon of an Ethics of Health Care,” she proposestwo imperatives for the ethics of evidence. The first is“to create, disseminate, and use the best possible sci-entific evidence as a basis for every phase of medicaldecision making.” The second is “to increase theawareness of, and come to terms with, the extent andultimately irreducible nature of uncertainty.”
We need to accept that we can never provide evi-dence for every detail of our practice. Science canhelp us with the first imperative, and with awarenessof both imperatives we may have the patience andpersistence to make the best choices for each individ-ual patient.
Scientific evidence cannot replace the excitement atherapist feels when a splint is completed; when itmeets the requirements of the patient, the needs of theinjured tissues, and other demands of care; and whenits appearance and fit and its smart and skillful con-struction are just right. Seeking to demonstrate theevidence for such a masterpiece should enrich andsatisfy every clinician, providing the opportunity tocombine technical expertise and scientific evidence. Itwill make the entire splint treatment “just right.”
Acknowledgments
The author thanks Kenneth Ottenbacher, PhD, for criticalcomments on the paper, and Elaine Ewing Fess, MS, OTR,FAOTA, CHT, for critical comments and references ofsplint examples.
REFERENCES
1. Sackett DL, Richardson WS, Rosenberg W, Haynes RB.Evidence-based Medicine: How to Practice and Teach EBM.New York: Churchill Livingstone, 1997, chapter 1.
2. Bury T, Mead J. Evidence-based Health Care: A PracticalGuide for Therapists. Woburn, Mass.: Butterworth-Heinemann, 1998:4–42.
3. Urbaniak JR Physician accountability: winning the public trust[presidential address]. J Hand Surg. 1993;18A(3):379–87.
4. Deyo RA. Using outcomes to improve quality of research andquality of care. In: Geyman JP, Deyo RA, Ramsey SD (eds).Evidence-based Clinical Practice: Concepts and Approaches.Woburn, Mass.: Butterworth-Heinemann, 2000:65–72.
5. Kane RL. Understanding Healthcare Outcomes Research.Gaithersburg, Md.: Aspen, 1997:1–15.
6. Tarlov AR, Ware JE, Greenfield S, Nelson EC, Perrin B, ZubkoffM. The medical outcome study. JAMA. 1989;262(7):925–30.
7. MacDermid JC. The outcome issue [editorial]. J Hand Ther.2001;14(2):61–2.
8. MacDermid JC, Richards RS, Roth JH. Distal radius fracture: aprospective outcome study of 275 patients. J Hand Ther. 2001;14(2):154–69.
9. Katz JN, Keller RB, Augusta ME, et al. Maine carpal tunnelstudy: outcomes of operative and nonoperative therapy forcarpal tunnel syndrome in a community-based cohort. J HandSurg. 1998;23A:697–710.
10. Edinburg M, Widgerow AD, Biddulph SL. Early postoperativemobilization of flexor tendon injuries using a modification ofthe Kleinert technique. J Hand Surg. 1987;12A:34–8.
11. Levine DW, Simmons BP, Koris MJ, et al. A self-administeredquestionnaire for the assessment of severity of symptoms andfunctional status in carpal tunnel syndrome. J Bone Joint Surg.1993;75A:1585–92.
12. Weiss ND, Gordon L, Bloom T, So Y, Rempel DM. Position of thewrist associated with the lowest carpal tunnel pressure: implica-tions for splint design. J Bone Joint Surg. 1995;77A(11):1695–9.
13. Burke DT, McHale Burke M, Stewart GW, Cambre A.Splinting for carpal tunnel syndrome: in search of the optimalangle. Arch Phys Med Rehabil. 1994;75:1241–4.
14. Helewa A, Walker J. Critical Evaluation of Research inPhysical Rehabilitation: Toward Evidence-based Practice.Philadelphia, Pa.: Saunders, 2000:80, 125–41.
15. Strickland JW, Glocovac SV. Digital function following flexortendon repair in zone II: a comparison of immobilization andcontrolled passive motion techniques. J Hand Surg. 1980;5(6):537–43.
16. Stegink Jansen CW, Minerbo G. A comparison between earlydynamically controlled mobilization and immobilization after
142 JOURNAL OF HAND THERAPY

flexor tendon repair in zone 2 of the hand: preliminary results.J Hand Ther. 1990;3(1):20–5.
17. Sackett DL, Richardson WS, Rosenberg W, Haynes RB.Evidence-Based Medicine: How to Practice & Teach EBM. 2nded. New York: Churchill Livingstone, 2000:1–12.
18. Sackett DL. Rules of evidence and clinical recommendationson the use of antithrombotic agents. Chest. 1989;95(2):2S–4S.
19. Pinsky EL, Deyo RA. Clinical guidelines: a strategy for translat-ing evidence into practice. In: Geyman JP, Deyo RA, Ramsey SD(eds). Evidence-Based Clinical Practice: Concepts & Approaches.Woburn, Mass.: Butterworth-Heinemann, 2000:65–72.
20. Chalmers I, Enkin M, Keirse MJNC (eds). Effective Care inPregnancy and Childbirth. Oxford, UK: Oxford UniversityPress, 1989.
21. Clancy CM, Eisenberg JM. Outcomes research at the Agencyfor Health Care Policy and Research. DMCO. 1997;1:72–80.
22. American College of Physicians– American Society of InternalMedicine. ACP Journal Club. Haynes RB (ed). Philadelphia,Pa.: ACP-ASIM, 1994–present. Available at: http://www.acpjc.org/.
23. Lacasse Y, Wong E, Guyatt GH, King D, Cook DJ, GoldsteinRS. Meta-analysis of respiratory rehabilitation in chronic pul-monary disease. Lancet. 1996;348:1115–9.
24. Struijs PA, Smidt N, Arola H, Dijk v VA, Buchbinder R,Assendelft WJ. Orthotic devices for the treatment of tenniselbow (Cochrane Review). Cochrane Database Syst Rev.2002;(1):CD001821.
25. Mike V. Outcomes research and the quality of healthcare: the bea-con of an ethics of evidence. Eval Health Prof. 1999;22(1):3–32.
26. Gelberman RH, Woo SL-Y, Lothringer K, van de Berg JS,Akeson WH. Effects of early intermittent mobilization on heal-ing canine flexor tendons. J Hand Surg. 1982;7(2):170–5.
27. Gelberman RH, Siegel DB, Woo SL-Y, Amiel D, Takai S, Lee D.Healing of digital flexore tendons: importance of the intervalfrom injury to repair. J Bone Joint Surg. 1991;73A(1):66–75.
28. Rizzo F, Hamilton BB, Keagy RD. Orthotic research evaluationframe work. Arch Phys Med Rehab. 1975;56:304–8.
29. Boozer JA, Sanson MS, Soutas-Little RW, Coale EH, Pierce TD,Swanson AB. Comparison of the biomechanical motions andforces involved in high-profile versus low-profile dynamicsplinting. J Hand Ther. 1994;7:171–82.
30. Citron ND, Foster A. Dynamic splinting following flexor ten-don repair. J Hand Surg. 1987;12B(1):96–100.
31. Bunnell S: Surgery of the Hand, 2nd ed. Philadelphia, Pa.Lippincott, 1948:626–30.
32. Duran RJ, Houser RG: Controlled passive motion followingflexor tendon repair in zones 2 and 3. In: American Academyof Orthopedic Surgeons. Symposium on Tendon Surgery inthe Hand. St Louis, Mo.: Mosby, 1975:105–14.
33. Silfverskiold KL, May EJ, Tornwall AH. Flexor digitorum pro-fundus excursions during controlled motion after flexor ten-don repair in zone II: a prospective clinical study. J Hand Surg.1992;17A:122–31.
34. Lister GD, Kleinert HE, Kutz JE, Atasoy E. Primary flexor ten-don repair followed by immediate controlled mobilization. JHand Surg. 1977;2(6):441–51.
35. Silfverskiold KL, May EJ. Flexor tendon repair in zone II with anew suture technique and an early mobilization program com-bining passive and active flexion. J Hand Surg. 1994;19A:53–60.
36. May EJ, KL Silfverskiold. Controlled mobilization after flexortendon repair in zone II: a prospective comparison of threemethods. J Hand Surg. 1992;17A:942–52.
37. American Society of Hand Therapists. Clinical AssessmentRecommendations. 2nd ed. Chicago, Ill.: ASHT, 1992.
April–June 2002 143

WHY PLASTER OF PARIS?
Plaster of Paris, a highly compliant material, isoften overlooked in the splinting of hand patients.This article enumerates the advantages of plaster ofParis and illustrates its application in specific clinicalsituations. This information is intended to encouragetherapists to introduce plaster of Paris more readilyinto their treatment armamentarium as a means ofaccomplishing tissue change.
The current primary treatment to mobilize stiffjoints and adherent soft tissue is the application ofintermittent force via mobilization splinting. The sus-tained positioning of joints and soft tissue with plas-ter of Paris provides a gentler and more precisemeans of tissue remodeling than does dynamic orstatic progressive splinting. The only possibleresponse to continual positioning in a plaster of Pariscast is plastic deformation, a permanent change in tis-sue length due to the realignment of collagen fibers.
Removable splints create an elastic response in thetissues such that, on removal of the splint, the tissuereturns to the previous position. The idea of mobiliz-ing tissue by immobilizing it seems contradictory.One must grasp the concept of positioning tissue andwaiting until it has time to adapt to a new length andshape. Bell1 agrees that we must abandon the tradi-tional concept of applying force, and think instead of
the ability to position joints to positively influencethe dynamic remodeling properties of soft tissue.
Because we know that prolonged periods of immo-bility have negative effects,2–14 many cliniciansassume that short-term immobilization of joints andsoft tissue is to be avoided. The risk of losing motion(even temporarily) is so intolerable that plaster ofParis casting is avoided unless it is the last resort forgaining motion. Immobilization of uninjured jointsmust be prolonged, and the extremity kept immobilefor the negative effects of immobilization to stiffenuninjured joints. A loss of motion in one directionusually occurs with plaster of Paris splinting or cast-ing, but clinical experience has proved this to be tem-porary. The unspoken assumption—that all jointsshould be allowed to move in all directions whenregaining motion in the hand—must be abandoned ifefficiency and precision in joint and soft tissue mobi-lization are to occur.
If joint tightness or tissue adherence is present in arecently injured hand, tissue elongation can beregained and motion restored by a brief period of cast-ing. The clinical goal is quickly converted from gain-ing motion to maintaining motion. Thereafter, inter-mittent splinting can maintain the gains. In contrast, ifintermittent splinting and manual mobilization tech-niques are the first choice, many hours of tissue elon-gation are needed to effect permanent tissue change.
Joint stiffness and tissue adherence that are matureand resistant to intermittent mobilization splintingand manual mobilization also respond to positioningwith plaster of Paris casting. In some chronically stiff
Plaster of Paris: The Forgotten Hand Splinting Material
Judy C. Colditz, OTR/L, CHT, FAOTAHandLab, a division of RHRC, Inc.Raleigh, North Carolina
ABSTRACT: This article examines the concept of tissue adapta-tion in response to the application of plaster of Paris splints andcasts. A review of the history of plaster of Paris and its composi-tion, its working properties, and precautions for its use introducesthe reader to this oft-forgotten material. Four designs are describedfor plaster of Paris application—circumferential padded casts, dig-ital unpadded casts, plaster slabs, and contour molds. The discus-sion of clinical application of plaster of Paris covers joint tightness,arthritis, contracted joints due to spasticity, muscle-tendon tight-ness, skin tightness, skin and joint tightness, and edema reduction.In addition, a new application called casting motion to mobilizestiffness (CMMS), developed by the author, is discussed. The useof plaster of Paris to improve postoperative flexor tendon glide isalso discussed. This review article intends to stimulate the readerto use plaster of Paris splinting or casting more frequently to solveclinical problems. J HAND THER. 2002;15:144–157.
144 JOURNAL OF HAND THERAPY
Correspondence and reprint requests to Judy C. Colditz, OTR/L,CHT, FAOTA, HandLab (a division of RHRC, Inc.), 2615 LondonDrive, Raleigh, NC 27608; e-mail: <[email protected]>.

hands, constrained motion in a cast can direct activemotion to the stiff joints, so that they regain both softtissue glide and joint motion. Because the cast is notremovable and all motion is directed repeatedly to thesame tissue, dramatic change occurs without theapplication of external force.
Kolumban15 offers the only study to date that com-pares the effectiveness of serial plaster of Paris cast-ing with the the effectiveness of mobilization splint-ing. In his study with leprosy patients, casting wasclearly superior to dynamic splinting and resulted infewer pressure areas.16 Unfortunately, no compara-tive studies of patients with joint stiffness due totrauma are available. Since the primary benefit ofplaster of Paris is a more rapid change in the qualityof the soft tissue, photographs do not adequatelyconvey this progress. No objective means of quanti-fying these changes currently exist. Direct palpationis the only means of demonstrating the quality ofchange in soft tissue.
Since plaster of Paris casting is frequently used as ameans of mobilization ”splinting,” the words splintand cast become confusing in this context. In this arti-cle, splint is used when the piece is removable(regardless of the material from which it is made) andcast is used when the design (usually made of plasterof Paris) cannot be removed by the patient.
HISTORY
Archives provide numerous reports of various sub-stances being applied to splinted body parts to stiff-en the part for fracture immobilization. It was notuntil 1852 that a technique was developed for apply-ing plaster of Paris directly to an extremity. (It iscalled plaster of Paris because it was first preparedfrom the gypsum mined in Paris, France.) In 1852, aDutch army surgeon, Antonius Mathysen, treatedbattle wounds in the Crimean War with cotton band-ages filled with dry plaster of Paris.17
This somewhat awkward means of plaster applica-tion continued until 1927, when binder ingredients(starches, gums, and resins) were added to improvethe adherence of the plaster to the gauze. These addi-tives made the application of a cast less messy andmore consistent. Later, other additives were incorpo-rated to change the physical properties of plaster ofParis, such as the setting time, which allowed stan-dardized production.18,19
In the first half of the 1900s, plaster of Paris was themost readily available material both for immobiliza-tion of acute injuries and intermittent immobilizationor mobilization splinting. Serial plaster splinting orcasting was used to mobilize stiffened joints due totrauma20 and contractures due to arthritis.19
Bunnell20–22 incorporated outriggers into plaster ofParis splints to provide dynamic mobilization. Brand’swork23 in India with leprosy patients introduced the
use of plaster of Paris for serial positioning of joints,especially the small interphalangeal (IP) joints.
In the 1970s, low-temperature thermoplastic mate-rials became available. These materials, which couldbe quickly molded on the patient and easily altered,revolutionized mobilization splinting of the hand. Atabout the same time, lighter-weight and water-resist-ant synthetic casting materials replaced the tradition-al plaster of Paris casting materials used for acuteinjuries. As a result of these two developments, plas-ter of Paris came to be used less frequently by bothphysicians and therapists. The infrequency withwhich plaster of Paris is currently used in hand ther-apy is reflected by the very brief mention of its use inrecent hand splinting texts.24–27
COMPOSITION
Plaster of Paris is derived from gypsum (calciumsulfate dihydrate), a naturally occurring rocklike sub-stance found in rock salts. When gypsum is heated to128° C, most of the water is driven off, resulting in apowdery substance commonly known as plaster ofParis. When water is added to the dry plaster ofParis, the water molecules incorporate themselvesinto the crystalline lattice of the calcium sulfate dihy-drate, thus giving up most of their kinetic energy inthe form of heat. This hydration process converts theweak and powdery plaster of Paris into a homoge-neous, rock-hard mass.18,19,28
The time required for the plaster to set up varies,depending on the additives.29 Manufacturers clearlylabel their products with the set-up time. Plaster ofParis with minimal additives is called gypsona.When plaster of Paris is used for hand mobilization,gypsona impregnated into leno-weave gauze (a non-raveling, closely woven gauze) is highly recommend-ed (Gypsona Gauze Type-Leno, Smith & Nephew,Inc., Germantown, Wisconsin).
Gypsona has a creamier consistency than the plas-ter of Paris with additives, although the latter is moredurable and water-resistant.29 For removal, a castmade of gypsona may first be softened by soaking.
ADVANTAGES ANDDISADVANTAGES
The advantages of plaster of Paris as a splintingmaterial are 1) its ability to intimately conform1,23,30;2) the decreased possibility of pressure areas, becauseof the increased conformity16,23; 3) the lesser sheer-force (the movement of the splint or cast on the skin)1;4) its porosity, which allows absorption of perspirationand prevents skin maceration23,30; 5) its retention ofbody heat, which provides a gentle, neutralwarmth31–34; 6) its reasonable cost23,30,35; and 7) its usein the construction of comfortable, nonremovablecasts to facilitate tissue response.
April–June 2002 145

No thermoplastic material, regardless of its mold-ing properties, can mimic the ability of plaster ofParis to conform. Synthetic casting materials aremuch stiffer than plaster of Paris,36–38 although theyare stronger.37,38 Strength is a consideration only inweight-bearing casts and large casts over joints influ-enced by spastic muscles.
Thermoplastic splints and plaster of Paris casts areestimated by the author to have similar material costsper application, but the time cost for construction ofa mobilization splint is much greater than for a plas-ter of Paris cast. Synthetic casting materials are about2 to 2.5 times more costly than plaster of Paris.36–38
Disadvantages of plaster of Paris are 1) the skillrequired for precise application and safe removal ofcasts made from it; 2) the sensitivity of hardenedplaster of Paris to water exposure, which may causeinconvenience in the performance of activities ofdaily living; and 3) its heavier weight in comparisonwith thermoplastic splinting materials. Because theperiod when a cast is worn full time is relativelybrief, the weight of the cast is rarely a problem.Besides, the cast will not be unnecessarily heavy if itis skillfully constructed and applied.
PRECAUTIONS
Care must be taken in the application of plaster ofParis to prevent inaccurate positioning or stabiliza-tion, with inappropriately displaced pressure.Pressure areas and circulatory constriction are possi-ble, although these complications are far more com-mon when plaster of Paris is applied to an acutelyinjured hand. Patients with asensate areas are mostvulnerable to complications from inappropriate pres-sure.
The primary concern in the application of plaster ofParis is avoidance of excessive heat from the exother-mic process, which can cause second- or third-degreeburns.18,39–41 Therapists should be fully aware of themultiple factors that influence the exothermic processin plaster of Paris.
The greatest influence on the exothermic process isthe speed of the setting time: The faster the settingtime, the greater the exothermic process.17,40,42 Thesecond most important influence is the thickness ofthe plaster of Paris, with a thicker cast or splint gen-erating more heat.17,40,42 Third, increased tempera-ture of the dipping water also increases the heat gen-erated.19,40,42
Wrapping material over the setting plaster of Parisor covering the cast or splint with pillows preventsthe heat from dissipating and significantly increasesthe internal temperature.40–42 As the cast or splint issetting, the patient should be instructed to avoid cov-ering it until it is completely cool and dry.
Other factors that affect the heat generated by theexothermic process are the humidity and tempera-
ture of the room40 and whether the immersion waterhas had previous plaster of Paris dipped in it.40,42
The thickness of the padding is an insignificant fac-tor in temperature alteration.40 Recommended tem-peratures for the dipping water vary greatly in theliterature.19,28,40,42,43 For each type of plaster of Parisused, therapists should follow the manufacturer’swritten recommendation for immersion water tem-perature.
During cast removal, vibration from the oscillatingsaw blade generates heat. If the cast saw blade is heldin one position, the heat generated by it may burn thepatient. To prevent this, the saw technique mustincorporate an up-and-down movement of theblade.17,44,45
If pressure on the blade is maintained after it hascut through the plaster, a friction burn or abrasion tothe skin will result. Practice is required to developskill in cast removal, so that saw movements are keptsecurely in control and the pressure is released assoon as the blade pierces through the plaster.
As discussed later, plaster of Paris can be applieddirectly to the skin. Contact dermatitis, although rare,should be considered whenever an unpadded cast orsplint is applied.43,46,47
SPLINT AND CAST DESIGNS
Plaster application to the hand has three basicdesigns—circumferential casts (padded over thehand, unpadded over the digit), padded slabs, andisolated contour molds.
Circumferential Padded Cast
Padded casts have a layer of tubular stockinetteapplied directly to the skin, over which cast paddingis applied prior to the application of plaster of Paris.The use of cotton cast padding (Webril undercastpadding, North Coast Medical, Inc., Morgan Hill,California) rather than synthetic padding is recom-mended. Synthetic padding will narrow as tension isapplied, whereas the cotton will shred apart beforeexcessive tension is applied, preventing the possibil-ity of excessively tight application. Synthetic paddingalso usually has more cushion, making the applica-tion of intimately molded plaster of Paris over thepadding more difficult.
A wet roll of plaster of Paris is quickly wrappedaround the padded part, overlapping by 25% to 50%,with four to six layers applied for a non-weight-bear-ing circumferential cast.18,44 As soon as a completeroll of plaster of Paris has been applied, the layers aresmoothed together until it becomes one mass. Oncethe set point is reached, joints cannot be repositionedor the contour changed. Any attempted remoldingwill hinder the interlocking of calcium sulfate crys-tals and weaken the cast or splint.28
146 JOURNAL OF HAND THERAPY

Circumferential casts require removal by cuttingdown two sides with an oscillating cast saw. If thepadding and stockinette are cut on one side only, thecircumferential cast becomes a hinged removable cast(called a bivalved cast). The addition of circumferen-tial hook-and-loop straps allows periodic reapplica-tion of the cast during weaning periods.
Digital Unpadded Casts
Because of the tubular shape of the digits, digitalcasts can be applied directly to the skin and easilyremoved by soaking in water or cutting with scissors.(Cast saws are never used on unpadded casts.) Theplaster of Paris adheres slightly to the underlying skin,forming perfect contact for pressure distribution.Multiple layers of 1-inch-wide plaster of Paris stripsare wrapped around the digit and smoothed togetherwhile the joints are gently positioned. Bell-Krotoskiprovides detailed descriptions of this technique.1,16
Plaster Slabs
Plaster slabs are lengths of multiple layers of plas-ter of Paris applied to one or both sides of the extrem-ity. Prior to application, a wet slab is placed on stripsof padding material and smoothed out so that theplaster of Paris layers meld together and adhere tothe padding. The slab is then held in place on theextremity with an elastic bandage or gauze wrap.When two slabs are used, one may be applied andallowed to harden slightly before the second isapplied. The slabs can be removed and reapplied bythe patient (Figure 1).
Contour Molds
Contoured plaster of Paris molds are used to applypositive pressure to scars and, secondarily, to assist inrepositioning joints. Since the plaster of Paris contourswell and does not cause maceration, it is the ideal
April–June 2002 147
FIGURE 1. Plaster of Paris slabs are used to serially position the wrist. Topleft, Multiple layers of plaster of Paris are prepared. Top right, Slabs areimmersed in water and then smoothed out over layers of cast padding. Left, Avolar slab is applied and wrapped in place, and the wrist is held in extensionwhile the plaster of Paris hardens. Above, After identical application of a dor-sal slab, both slabs can be removed and reapplied.

material for application directly over scars, especiallyif the skin needs to be held at length while the positivepressure is applied. The plaster of Paris may beapplied directly to the skin, or one layer of paddingmay be applied underneath. One layer of wet plasterof Paris is applied at a time and is smoothed in place,until the desired size and shape are achieved. To pre-vent friction of the mold on the hand, the mold isapplied with an elastic or self-adherent elastic wraprather than with straps.
Regardless of the design, the most importantaspect of successful use of plaster of Paris is the meld-ing of the layers together, to make a strong and well-molded contour.
CLINICAL APPLICATIONS
Joint Tightness
The periarticular structures of the human jointadaptively shorten under any circumstance in whichthe joint is not carried through the full range ofmotion. If trauma creates scar within the periarticularstructures, the resistance to full motion becomes evengreater. Joint tightness is currently the most commonclinical problem treated with plaster of Paris castingor splinting.
Serial Digital Casting
Serial digital casts are frequently used to decreaseIP flexion contractures. This technique was devel-oped by Brand23 and Kolumban48 in work with lep-rosy patients in India, and it is detailed by Bell-Krotoski1,16 and others.49 Kolumban’s work48 has val-idated the superiority of serial casting for increasingjoint motion in patients with leprosy, compared withboth traditional physical therapy techniques anddynamic splinting.
Both recently injured joints and chronically stiffjoints respond to serial casting. Those who hesitate toapply serial casting for a brief period early in thetreatment of proximal interphalangeal (PIP) jointproblems are missing a valuable opportunity. A fewdays of serial casting will significantly decrease jointedema while enabling the joint to regain the weakermotion of extension.
In many cases, reducing joint edema is as crucial tothe resumption of normal joint motion as is decreas-ing the resistance of the periarticular structures. Abulbous, somewhat fluctuant PIP joint with inflam-mation localized to one or more collateral ligaments isan ideal candidate for a short period of serial castingearly in rehabilitation.
Concerns are often expressed that the circumferen-tial pressure of the cast on a digit may cause ischemiadue to increased swelling. Since the cast is neverapplied in the acute inflammatory stage and since thepressure of the hardened cast is static, the common
response of the digit is decreased edema. The rest thatthe cast provides to the joint contributes to dimin-ished inflammation, which also reduces edema.
Both edematous PIP joints and contracted PIPjoints may gain greater flexion as a result of theextension mobilization casting. In an edematousjoint, greater flexion results from increased room tomove into a closed pack position. In a contractedjoint, the elongation of scar impeding volar platemovement allows the volar plate to more readily foldout of the way during flexion.
An additional advantage of plaster of Paris digitalcasting is the ability to mobilize adjacent joints inopposite directions. In a fixed boutonniere deformity,the DIP joint can be mobilized into flexion and the castallowed to harden. The PIP joint is then cast towardextension with the application of additional plaster ofParis. Conversely, fixed swan neck deformities can begently altered by first mobilizing the DIP joint intoextension and then the PIP joint into flexion.1 Digitalcasts may also be used to mobilize an isolated tightjoint while a thermoplastic splint with outriggers isapplied to elongate a tight muscle–tendon unit.1
Serial Plaster of Paris Slabs
Plaster of Paris slabs are particularly useful forregaining wrist extension after distal radius frac-ture.43 Immediately following mobilization of thewrist in therapy, the wrist is positioned in easy max-imum extension and a volar slab is applied. A dorsalplaster of Paris slab is then applied to hold the wristsecurely against the volar mold. When appliedtogether, these two molds sandwich the wrist andhold it in maximum extension (Figure 1). The patientwears this for prolonged sessions during the day,and sleeps in it. After waking, the patient starts withthe wrist at its maximum extension, rather thanworking to regain the maximum achieved the previ-ous day. When the patient can actively lift the wristout of the volar slab, a new one is molded.
Arthritis
Prior to the development of anti-inflammatorydrugs, plaster of Paris immobilization splints or castswere used to decrease synovial inflammation andreduce pain in patients with inflammatory arthritis.When inflammation subsided, serial plaster of Parissplints or casts were then applied to regain motion inthe stiffened joints.19 Since the advent of anti-inflam-matory drugs, immobilization splinting for control ofsynovial inflammation is rarely used in the UnitedStates. The use of night resting splints19 has contin-ued, but these splints are now made from thermo-plastic materials for ease of construction and greaterdurability.
There remains a large realm of appropriate appli-cation of plaster of Paris to minimize and in some
148 JOURNAL OF HAND THERAPY

cases reduce hand joint deformities resulting fromarthritis and other connective tissue disorders. Asjoint deformities or instability begins, the balance ofthe forces crossing the joints of the hand is altered.Deformities are likely to progress if there is no exter-nal influence in the opposite direction. Gentle, slowrepositioning of the joints via serial plaster of Parissplinting or casting allows the soft tissues to resumetheir previous length. This is the ideal way to mobi-lize such joints comfortably.
It is only when forceful serial casting is applied thatconcern for cartilage neurosis via sustained pressure isa consideration. Since rheumatoid arthritis is a colla-gen disorder that increases the laxity of the supportingstructures of the joints, fear of stiffness from a reason-able period of immobilization from serial splinting orcasting is unfounded.
Serial casting to reduce digital deformities, such asboutonniere and swan neck deformities, may beapproached as in the hand with trauma, so long asx-rays show an absence of a fused joint. Even anobstinate joint with a pseudarthrosis can sometimesbe slightly repositioned so that the deformed positionis more functional. Therapists will do no harm if theydiscard any idea of force application in theirapproach to patients with such deformities, andapply plaster of Paris to gently reposition the tissue.
In a patient with severe contractures due to sclero-derma, the possibility of regaining joint motion isobliterated by the nature of the disease. Patients withseverely contracted PIP joints have ischemia of thetaut dorsal skin, and dorsal ulcers are frequentlypresent. These ulcers are hard to heal, because theposition of the severely contracted joint places con-tinual tension on the dorsal skin, and the prominentapex of the flexed PIP joint is prone to abrasion. Acarefully applied serial digital cast (with a thin layerof cast padding over the PIP prominence) will protectan ulcer from pressure or fiction and can slowlyrelieve some of the tension on the dorsal skin, allow-ing the ulcer to heal. Care must be taken that the castis not tight enough to constrict even further thealready diminished blood flow of the finger.
Contracted Joints Due to Spasticity
Inhibitive casting is used as a treatment technique inpatients with cerebral palsy and head injuries, todecrease spasticity and improve joint contrac-tures.31–34,50–53 Although reports of the use of plaster ofParis inhibitive casting are limited to single case stud-ies or general observation, a significant change in qual-ity of movement and amount of joint motion is consis-tently reported.31,33,34 The extremity is cast in a func-tional tone-inhibiting posture that theoreticallyreduces cutaneous input and spasticity by providingneutral warmth and even cutaneous pressure.31–34 Theprolonged positioning also results in muscle lengthen-
ing.31 After initial progress has been noted, the cast isbivalved and worn for limited periods during day. Asone would expect, these patients need long-term cast-ing to retain the gains that have been made.31,33
Most casting of these patients is used to mobilizelarge joints such as the elbow or knee. Both circumfer-ential serial casts and drop-out casts are used. Drop-out casts are circumferential around either the proxi-mal or the distal bone, but the other bone is allowed tomove only in the direction away from the contractedposition. This allows active muscle contraction of thedesired (and weaker) muscle into a greater range ofjoint motion, but it prevents the joint and muscle fromresting in the fully contracted position.32,54,55
This concept of controlling the direction and extentof joint motion has been used by the author to devel-op a new approach to mobilization of the stiff hand—casting motion to mobilize stiffness (CMMS)—whichis discussed below.
Muscle–Tendon Tightness
Tightness of the muscle–tendon unit of either theextrinsic flexors or the extensors is remedied by seri-al positioning of all the joints crossed by the muscle,to regain maximum length.43 Since each joint beingpositioned requires three points of pressure to beaccurately immobilized,56 the multiple joints of thehand and wrist can best be serially positioned usingvolar and dorsal plaster of Paris slabs. If only onecomponent is used, stability of the splint on the handis dependent on the strapping or wrapping, whichover time allows movement of the hand joints in thesplint.57 When plaster of Paris slabs are used bothdorsally and volarly, only one position is availablefor all the joints, and this position is sustained.
This slab technique also provides a safe means ofrepositioning an acutely injured hand while provid-ing gentle compression to minimize edema. Thevolar slab is molded to position the wrist and hand inthe desired position. When the volar slab starts toharden, the dorsal slab is molded. An additionalsmaller slab is molded to hold the thumb (Figure 2).
Skin Tightness
Because both burns and skin grafts provide a largebed of contractile scar, maintenance of skin length inall directions is needed to avert loss of joint motion.Plaster of Paris conformed over an area can comfort-ably position numerous joints accurately and alsoprovide perfectly distributed pressure with a breath-able material.
Plaster of Paris seems to be the ideal material in suchcircumstances, rather than being used only for patientswho are noncompliant, as advocated by some.58,59 Thetissue response with plaster of Paris—the reduction ofsubtle edema, the flattening and softening of the tissue,and its increased mobility in response to gentle pres-
April–June 2002 149

sure59—is always superior to the tissue response withthermoplastic splints. The straps of thermoplasticsplints can never stabilize a splint as accurately as cancircumferential application of plaster of Paris or con-tour molds held in place with wraps.
The prolonged splinting or casting needed bypatients with extensive burn or skin injuries is a chal-lenge. The immobilization imposed by any type ofsplint or cast, whether made of thermoplastic materi-al or of plaster of Paris, is difficult to balance with theneed for joint movement. Plaster of Paris can easilybe applied in a design that allows for splint removal.Bivalved casts, splints, or molded supports wrappedin place with self-adherent wrap or overlappingmolded plaster of Paris slabs can provide well-distributed pressure but also can be removed for skinhygiene and exercise.
Because skin scars can cover any plane of motionand any number of joints, multiple joints often need
to be positioned. When thermoplastic materials areused, all joints must be simultaneously positionedwhile the thermoplastic material is cooling. Withplaster of Paris, one joint can be precisely positionedand the plaster of Paris allowed to harden. Thenadditional plaster of Paris can be added for carefulpositioning of the adjacent joint. By use of plaster ofParis, a contracted hand can be slowly coaxed into amore functional position.59 If motion is lacking inboth directions, Rivers59 suggests using alternatingflexion and extension casts to prevent significant lossof motion in either direction.
Plaster of Paris is well tolerated over open wounds.One study of split thickness skin grafts to the lowerextremity showed that in patients who received castsimmediately after surgery, wound closure was morerapid, graft acceptance was better (72% vs. 100%),and fewer therapy treatments were required than inan uncasted group.35 Since plaster of Paris decreasesfriction of the splint or cast on the wound andabsorbs wound drainage, it allows unimpededwound healing. Wounds with unhealed areas andimmature scars intolerant of friction (such as burnwounds that easily blister) are ideal candidates forthe gentle pressure that plaster of Paris provides.Such wounds are tolerant of plaster of Paris alsobecause collection of perspiration and moisture–anegative aspect of thermoplastic splinting material—is avoided.
Skin and Joint Tightness
If joint tightness accompanies skin shortness due toscarring, plaster of Paris provides direct pressure tothe scar while joints are mobilized with repeatedrepositioning. In the author’s opinion, the concurrentpresence of skin and joint tightness is an absoluteindication for the use of serial casting. This is espe-
150 JOURNAL OF HAND THERAPY
FIGURE 2. Dorsal and volar plaster of Paris slabs with a smallthumb slab can slowly and safely reposition joints in the acutelyinjured hand while providing conformed compression to reduceedema.
FIGURE 3. Left, Following severe crush injury,the long finger stump is contracted and the first webspace is tight. Middle, A serial cast is applied (dor-sal view). Right, Extension of long finger stumpand elongation of first web are regained.

cially true in the thumb, where the many directionsof motion and planes of skin movement make mobi-lization difficult. In multiple tissue injuries with skininjury—such as explosion injuries to the palm, skinloss in the first web, and severe crush injuries to thepalm—plaster of Paris is likely to be more useful thanthermoplastic materials (Figure 3).
Edema Reduction
Traditional hand therapy techniques for edemareduction are elevation, active motion, and compres-sion with either elastic gloves or wraps or the appli-cation of massage. Recent increased awareness of theanatomy and physiology of the lymphatic system hascaused many hand therapists to adopt gentlerapproaches when using these techniques, since wehave learned that excessive pressure can preventlymph fluid from entering the initial lymphatics.60,61
Active finger movement while in a wrist cast causesthe skin on the palmar and dorsal surface of the handto move. The soft constraint of the padded plaster ofParis around the metacarpal area provides a lightmassage to the skin that facilitates lymphatic flow.Since the cast retains its original size and shape, thereis no danger of a constrictive force, such as that seenwith proximal compressive wraps.
This response was highlighted by a dramaticreduction in edema in a patient with a severe crushinjury. A small cast was applied around the ampu-tated thumb stump to contour the palmar scar andprovide maximum abduction of the first metacarpal.The presence of the thin padded cast over themetacarpal area resulted in a dramatic reduction ofedema (Figure 4). Use of such a thin cast over themetacarpal area and around the base of the thumbmay in some cases be a preferable edema reductiontechnique in the severely injured hand.
Joint Tightness, Soft Tissue Adherence,Chronic Edema, and Altered Pattern ofMotion in the Chronically Stiff Hand
Casting motion to mobilize stiffness (CMMS) is atechnique developed by the author that uses plasterof Paris casting to selectively immobilize proximaljoints in an ideal position while constraining distaljoints so that they move in a desired direction andrange.62,63 Only active motion is used to gain bothactive and passive joint motion. No passive force isapplied to any joint during the casting. The hand issimply positioned so that the muscle and joint move-ment needed is the only motion that can occurrepeatedly over a long period of time (Figure 5).
In the chronically stiff hand, generalized joint stiff-ness results in joint tightness with a hard end-feel andconstraint of soft tissue movement. Since the cast redi-rects the muscle–tendon excursion constantly to thejoints where it is most needed, cyclic active motionmobilizes the tissue in both directions.64 The activemotion re-establishes the normal collagen cross-link-ing.65–67 Mobilization splinting, on the other hand,moves the tissues in only one direction. Additionalnegative effects of mobilization splinting are constric-tion that contributes to edema, immobilization thatprevents pumping of the venous and lymphatic sys-tem, and the possibility of excessive force, all of whichprolong the inflammatory response.68,69 These factorsand the intermittent nature of mobilization splintingoften make mobilization splinting ineffective in thechronically stiff hand.
The advantages of using active motion to mobilizestiffness in the CMMS technique far outweighs anynegative effects of temporary immobilization of prox-imal joints. The movement of the stiffest joints main-tains lubrication within the collagen cell matrix, pre-vents abnormal cross-link formation, facilitates lym-
April–June 2002 151
FIGURE 4. Left, Patient following severe crush injury with multiple fractures, tendonlacerations, amputations, and open wounds has thin circumferential cast applied to moldpalmar scar and position thumb stump.(Dorsal view; Cast padding is taped between fin-gers) Middle, Pitting edema is present prior to casting. Right, After a few days of castingedema is significantly reduced.

phatic flow, strengthens muscles, and re-establishesindependent glide of tissue layers. Although continu-ous passive motion has proved to be effective in thetreatment of acute joint injuries,70–72 neither laborato-ry nor clinical studies have demonstrated its useful-ness for reducing stiffness once it is present.71,73
Abnormal patterns of motion are established as aresult of the lack of tissue mobility (Figure 6, left). Thepatient repeatedly moves the loosest joints, whichencourages the somatosensory cortex to memorizethis aberrant pattern. Therefore, regaining motion inthe stiff hand is both a complex mechanical and cere-bral issue.
The mechanical problems are shown by the pres-ence of deviate patterns of motion. The most com-mon patterns are the dominant intrinsic flexion pat-tern, in which the metacarpophalangeal (MCP) jointsflex before the IP joints, reinforcing the stiffness in theIP joints; and the dominant extrinsic flexion patternwith stiff MCP joints, in which the IP joints flex fullybefore MCP joints. Almost all patterns of motion willcause a loss of the normal reciprocal balance of ten-odesis, in which finger flexion occurs concurrent towrist extension. A vicious cycle is establishedbecause the tissue stiffness prevents the normal pat-tern of motion, and without the normal pattern ofmotion the stiffness cannot be resolved.
152 JOURNAL OF HAND THERAPY
FIGURE 5. Child with severe lawn mower injury at the wrist is fitted with a cast to support the wrist and position the fingers in slightflexion to facilitate maximum tendon glide after flexor tenolysis.
FIGURE 6. Left, Active finger flexion of patient with multiple wrist injuries and 4-month chronic open wound shows abnormal pos-ture and limited motion. Right, Cast with dorsal hood over the fingers immediately re-establishes pinch.
FIGURE 7. Patient with diminished finger flexion followingdistal radius fracture is fitted with a cast with the MCP joints inextension to allow active IP flexion to mobilize the interosseousmuscles.

Depending on the dominant pattern of motion, theCMMS cast blocks and stabilizes the proximal joints.For example, a hand with the dominant intrinsic flex-ion pattern is cast with MCP flexion blocked. If pro-fundus glide is poor, a dorsal hood is added to posi-tion the distal interphalangeal (DIP) joints in relative-ly greater flexion than the PIP joints, ensuring thatthe most likely muscle movement will be that of thethe flexor digitorum profundus. In hands withextremely limited motion, supporting the wrist inextension and placing a hood over the fingers imme-diately positions the fingers so that pinch is possible(Figure 6, right). This quickly converts a nonfunction-al hand to an assisting hand while digital motion isbeing regained.
Arbuckle and McGrouther74 validated the use ofthe dorsal hood to position the IP joints in greaterflexion than the MCP joints. They showed that thenormal pattern of digital flexion is initiated with IPflexion prior to any significant MCP flexion (hookposition). One must be cautioned against blockingthe MCP joints in full extension in the very stiff hand,since tight interosseous muscles may provide toomuch resistance to active IP flexion in the initialstages of mobilization. When reasonable profundusglide is regained, the cast position is changed to fullMCP extension so that IP flexion can mobilize thetight interosseous muscles (Figure 7).
A second example is the hand with stiff MCP jointsbut flexible IP joints. The dorsal hood extends onlyover the proximal phalanges (Figure 8). The patientworks on pulling the proximal phalanx away fromthe dorsal hood using primarily intrinsic muscles(minimal IP flexion) (Figure 8, middle). When agreater range of MCP flexion is gained, a new dorsal
hood is applied to allow this active motion to occur ina greater range of flexion.
Although casting or other immobilization of the IPjoints might be considered to transmit all flexor forceto the resistant MCP joints, the author has not foundthis necessary, even with joints with a significanthard end-feel. At no time is any force applied to anyjoint with the plaster of Paris cast, nor are joints heldat the absolute end-range of motion. The joints aresimply positioned within the cast to optimize activemotion.
Third, if isolated joints are stiff, the cast restrains allproximal (or other) joint movement. Movement occursonly at the site of the greatest stiffness (Figure 9). Thisis particularly helpful with PIP joint stiffness in whichboth flexion and extension are lacking. This is the onlymobilization technique by which motion can begained in both directions at the same time.
The neurologic consequences resulting from thealtered pattern of motion create an additional consid-eration in the rehabilitation process. Since stiffnessproduces an abnormal pattern of motion, the motorcortex learns this pattern of motion as the new “nor-mal.” Neuroscience research shows that animals andhuman beings trained in movement combinationsmagnify the cortical representations of the motorareas used predominantly and that lack of usedecreases the corresponding cortical area.75–77
For motor cortex repatterning to occur, repeatedmotion in the desired pattern is needed over a periodof time.78,79 With removable splints, a patient revertsto the aberrant pattern of motion each time the splintis removed, and repatterning of the cortex is defeat-ed. This explains why mobilization splinting so oftenfails to reduce resistance in the very stiff hand or
April–June 2002 153
FIGURE 8. Patient with hard end-feel stiffness of MCP joints following MCP joint dislocations:. Left, Limited active MCP flexion.Middle, Cast that dictates active MCP flexion in end range. Right, Active flexion after casting.

joint. For progress to occur and be maintained, thepatient must wear the CMMS cast for a significantperiod of time and wean slowly. Since original corti-cal connection patterns persist and can easily be re-activated,78 a few weeks in a cast can convert the pat-tern of motion even if the stiffness has been of longduration.
In the chronically stiff hand, mild pitting edemaaccompanies atrophic, shiny skin and diminished orabsent joint creases. The tissues are firm to palpationand have decreased mobility. The excess fibrosisfrom the prolonged immobility and the presence ofhigh-protein edema impede the flow of lymphaticfluid.60,80,81 Because of the limited active motion, thelymphatic system becomes stagnant. Since the singlemost effective stimulator of the lymphatic system isactive motion,12,60,61,80,82,83 CMMS casting effectivelyfacilitates lymphatic pumping by encouraging activemotion. No other mobilization technique providesthis stimulus so consistently.
Since the initial lymphatics in the skin are easily col-lapsed by excessive pressure,61,84 light pressure isrequired to facilitate lymphatic flow. The cast provideslight pressure to the hand, while movement of thehand within the padded casts provides a facilitatorypseudo-massage to the skin. There is also a direct rela-tionship between ambient temperature and the per-meability of the initial lymphatics.85,86 The insulationof the cast provides neutral warmth, retaining thebody heat. In addition to effecting lymphatic flow, theneutral warmth may assist in general tissue relaxationand facilitate tissue elongation.31,32
Dramatic results have been seen in numerouspatients with chronically stiff hands due to a widevariety of conditions. Each case is unique, and thecast design must be specific to the altered pattern of
motion. The cast must be precisely applied with accu-rate molding to ensure well-distributed pressure.Most therapists are uncomfortable with the tempo-rary loss of motion in some joints and are likely towean a patient out of the cast too early, so that a peri-od of recasting is often required. Therapists must letgo of previous assumptions that motion must begained in all directions simultaneously.
The CMMS technique should not be used onpatients who are claustrophobic or have acuteinjuries or in a patient whose anatomy is so alteredthat a balance of motion cannot be regained when theCMMS casting is discontinued.
Postoperative Mobilization of Flexor Tendon Glide
In unusual circumstances, following flexor tenoly-sis or flexor tendon repair, the application of a plas-ter of Paris cast to stabilize the wrist and allow onlyfinger flexion may be the optimal postoperative ap-proach. If a patient has had limited flexor tendonglide for a period of time, the unimpeded intrinsicmuscles will always be dominant. Placing the handin a cast in which only flexor glide is possible assiststhe patient with accurate muscle pull-through. Inflexor tenolysis, the cast may be applied early aftersurgery.
Limited proximal excursion of the flexor tendonsmeans that the muscles have never been allowed tomaximally contract. Placing the hand in a cast with adorsal hood over the fingers allows the patient towork in the end range of active finger flexion, whichalso allows effective muscle strengthening. When thismotion is regained, extension can be incorporatedinto the exercise program. Stretching and intermit-tent splinting can help the patient regain the exten-
154 JOURNAL OF HAND THERAPY
FIGURE 9. Left, 13-year-old patient with unusual pattern of hyperflexion of both the metacarpophalangeal and distal interphalangealjoints with limited proximal interphalangeal (PIP) joint flexion following proximal phalanx fracture. Middle, Cast to prevent motionat all joints but the PIP joint. Right, Final flexion.

sion, since it was dominant prior to the tenolysis.This treatment approach has been particularly usefulwith children and with mentally retarded adults whohave difficulty appreciating the correct motion.
In patients who have had flexor tendon repairs andare in unusual circumstances (such as incarceration)and in patients who have limited comprehension, thehand is placed in a cast with a dorsal hood after3 weeks of immobilization. The dorsal hood protectsthe hand from forced extension but allows activeflexion while stabilizing the wrist. At 6 weeks, whenthe tendon can withstand passive extension, the castis removed and the patient works on regainingextension while maintaining flexion.
Some therapists have expressed concern that thedorsal hood would create IP flexion contractures.Since the joints are moving actively and edema isminimal, this concern has appears to be unfounded.
This type of cast application allows simplificationof the postoperative regimen. The motion with thegreatest deficit is the primary focus. Until adequategains are made in that direction of motion, motion inthe other direction is ignored. Casting can be thoughtof as a jump-start for the greatest deficiency. The fewweeks of casting are, realistically, a very short periodrelative to the maturation process of the healing scar.
CONCLUSION
This article reviews the characteristics of plaster ofParis and re-introduces the concept of tissue adapta-tion in response to the application of plaster of Parissplints and casts. Clinical examples of the use of plas-ter of Paris are discussed, and a variety of applica-tions in cases with specific diagnoses are described.
It is hoped that the reader will question previousassumptions about temporary immobilization ofuninjured joints, concurrent goals of gaining motionin all directions, and methods of edema reduction.Such questions should lead the reader to use plasterof Paris splinting or casting more often to solve clini-cal problems. Therapists who lack plaster of Parishandling skills should seek the assistance of a skilledpractitioner and should apply and remove numerouscasts before using these treatment techniques withpatients.
REFERENCES
1. Bell JA. Plaster casting in the remodeling of soft tissue. In: FessEE, Philips CA (eds). Hand Splinting: Principles and Methods.2nd ed. St Louis: CV Mosby, 1987.
2. Akeson WH, Amiel D, Mechanic GL, Woo SLY, Harwood FL,Hamer ML. Collagen cross-linking alterations in joint contrac-tures: changes in the reducible cross-links in periarticular con-nective tissue collagen after nine weeks of immobilization.Connect Tissue Res. 1977;5:15–9.
3. Akeson WH, Amiel D, Abel MF, Garfin SR, Woo SL-Y. Effects ofimmobilization on joints. Clin Orthop Rel Res. 1987;219:28–37.
4. Akeson WH. An experimental study of joint stiffness. J Bone
Joint Surg. 1961;43A:1022–34.5. Amiel D, Woo SL-Y, Harwood FL, Akeson WH. The effect of
immobilization on collagen turnover in connective tissue: abiochemical-biomechanical correlation. Acta Orthop Scand.1982;53:325–32.
6. Booth WF. Time course of muscular atrophy during immobi-lization of hind limbs in rats. J Hand Surg.977;43A:656–61.
7. Bray RC, Shrive NG, Frank CB, Chimich DD. The early effectsof joint immobilization on medial collateral ligament healingin an ACL-deficient knee: a gross anatomic and biomechanicalinvestigation in the adult rabbit. J Orthop Res. 1992;10:157–66.
8. Grauer D, Kabo JM, Dorey FJ, Meals RA. The effects of inter-mittent passive exercise on joint stiffness following periarticu-lar fracture in rabbits. Clin Orthop Rel Res. 1987;220:259–65.
9. Kasperczyk WJ, Bosch U, Oestern HJ, Tscherne H. Influence ofimmobilization on autograft healing in the knee joint. ArchOrthop Trauma Surg. 1991;110:158–61.
10. Liepert J, Tegenthoff M, Malin J-P. Changes of cortical motorarea size during immobilization. Electroencephalogr ClinNeurophysiol. 1995;97:382–86.
11. Muneta T, Yamamoto H, Takakuda K, Sakai H, Furuya K.Effects of postoperative immobilization on the reconstructedanterior cruciate ligament. Am J Sports Med. 1993;21:305–13.
12. Namba RS, Kabo JM, Dorey FJ, Meals RA. Continuous passivemotion versus immobilization. Clin Orthop Rel Res. 1991;267:218–23.
13. Woo SL-Y, Gomez MA, Sites TJ. The biomechanical and mor-phological changes in the medial collateral ligament of the rab-bit after immobilization and remobilization. J Bone JointSurg.1987;69A:1200–11.
14. Woo SL-Y, Matthews P, Akeson WH, Amiel D, Convery FR.Connective tissue response to immobility: correlative study ofbiomechanical measurements of normal and immobilized rab-bit knees. Arthritis Rheum. 1975;18:257–64.
15. Kolumban S. The use of dynamic and static splints in straight-ening contracted proximal interphalangeal joints in leprosypatients: a comparative study. Presented at: 47th AnnualConference of the American Physical Therapy Association,1960.
16. Bell-Krotoski JA. Plaster cylinder casting for contractures ofthe interphalangeal joints. In: Mackin EJ, Callahan AD, SkirvenTM, Schneider LH, Osterman AL (eds). Hunter, Mackin &Callahan’s Rehabilitation of the Hand. 5th ed. St. Louis, Mo.:Mosby, 2002:1839–45.
17. Salib P. Plaster Casting. New York: Appleton-Century-Crofts,1975.
18. Woo K. Techniques in Surgical Casting and Splinting.Philadelphia, Pa.: Lea & Febiger, 1987.
19. Rotstein J. Simple Splinting: The Use of Light Splints andRelated Conservative Therapy in Joint Diseases. Philadelphia,Pa.: Saunders, 1965.
20. Bunnell S. Surgery of the Hand. 2nd ed. Philadelphia, Pa.:Lippincott, 1948.
21. Beasley RW. The addition of dynamic splinting to hand casts.Plast Reconstr Surg. 1969;44:507.
22. Bunnell S. Active splinting of the hand. J Bone Joint Surg.1946;28:732–6.
23. Brand PW. The reconstruction of the hand in leprosy. Ann RColl Surg Engl. 1952;11:350.
24. Wilton J. Hand Splinting. London, UK: Saunders, 1997.25. Salter MI, Cheshire L. Hand Therapy, Principles and Practice.
Oxford, UK: Butterworth-Heinemann, 2000.26. Van Lede P, Van Veldhoven G. Therapeutic Hand Splints: A
Rationale Approach. Antwerp, Belgium: Provan bvba, 1998.27. McKee P, Morgan L. Orthotics in Rehabilitation. Philadelphia,
Pa.: F.A. Davis, 1998.28. Bleck E, Duckworth N, Hunter N. Atlas of Plaster Casting
Techniques. Chicago, Ill.: Year Book, 1974.29. Lewis R. Handbook of Traction, Casting, and Splinting
Techniques. Philadelphia, Pa.: Lippincott, 1977.30. Flatt AE. The Care of the Arthritic Hand. 5th ed. St. Louis, Mo.:
April–June 2002 155

Quality Medical Publishing, 1995.31. Law M, Cadman D, Rosenbaum P, Walter S, Russell D,
DeMatteo C. Neurodevelopmental therapy and upper-extrem-ity inhibitive casting for children with cerebral palsy. Dev MedChild Neurol. 1991;33:379–87.
32. King TI. Plaster splinting as a means of reducing elbow flexorspasticity: a case study. Am J Occup Ther. 1982;36:671–3.
33. Katz RT. Management of spasticity. Am J Phys Med Rehabil.1988;67:108–16.
34. Barnard P, Dill H, Eldredge P, Held JM, Judd DL, Nalette E.Reduction of hypertonicity by early casting in a comatosehead-injured individual: a case report. Phys Ther. 1984;64:1540–2.
35. Ricks NR, Meagher DPJ. The benefits of plaster casting forlower-extremity burns after grafting in children. J Burn CareRehabil. 1992;13:465–8.
36. Wytch R, Ashcroft G, Ledingham WM. Modern splintingbandages. J Bone Joint Surg. 1991;73B:88–91.
37. Marshall PD, Dibble AK, Walters TH, Lewis D. When should asynthetic casting material be used in preference to plaster-of-Paris? A cost analysis and guidance for casting departments.Injury. 1992;23:542–4.
38. Rowley DI, Pratt D, Powell ES, Norris SH, Duckworth T. Thecomparative properties of plaster of Paris and plaster of Parissubstitutes. Arch Orthop Trauma Surg. 1985;103:402–7.
39. Hedeboe J, Larsen FM, Lucht U, Christensen ST. Heat genera-tion in plaster-of-Paris and resulting hand burns. Burns InclTherm Inj. 1982;9:46–8.
40. Gannaway JK, Hunter JR. Thermal effects of casting materials.Clin Orthop. 1983:181;191–5.
41. Becker DJ. Danger of burns from fresh plaster splints sur-rounded by too much cotton. Plast Reconstr Surg. 1978;62:436–7.
42. Lavalette R, Pope MH, Dickstein H. Setting temperatures ofplaster casts: the influence of technical variables. J Bone JointSurg. 1982;64A:907–11.
43. Tribuzi S. Serial plaster splinting. Mackin EJ, Callahan AD,Skirven TM, Schneider LH, Osterman AL (eds). Hunter,Mackin & Callahan’s Rehabilitation of the Hand. 5th ed. St.Louis, Mo.: Mosby, 2002:1828–38.
44. Parsons TA. Basic casting techniques. Aust Fam Phys. 1991;20:254–70.
45. Williams J. Plaster of Paris: A Manual of Basic CastingTechniques. Auckland, NZ: Joan Williams/Smith & NephewNZ, 1990.
46. Lovell C, Staniforth P. Contact allergy to benzalkonium chlo-ride in plaster of Paris. Contact Dermatitis. 1981;7:343–4.
47. Staniforth P. Allergy to benzalkonium chloride in plaster ofParis after sensitization to centrimede: a case report. J BoneJoint Surg. 1980;62B:500–1.
48. Kolumban S. The role of static and dynamic splints, physio-therapy, techniques and time in straightening contractures ofthe interphalangeal joints. Lepr India. 1969;41:323–8.
49. Colditz JC, Schneider AM. Modification of the digital serialplaster casting technique. J Hand Ther. 1995;8:215–6.
50. Garland DE, Keenan MA. Orthopedic strategies in the man-agement of the adult head-injured patient. Phys Ther.1983;63:2004–9.
51. Mills VM. Electromyographic results of inhibitory splinting.Phys Ther. 1984;64:190–3.
52. Conine TA, Sullivan T, Mackie T, Goodman M. Effect of serialcasting for the prevention of equinus in patients with acutehead injury. Arch Phys Med Rehabil. 1990;71:310–2.
53. Goya-Eppenstein P, Hill J, Philips CA, Philip M, Seifert T,Yasukawa A. Casting protocols for the upper and lowerextremities. Gaithersburg, Md.: Aspen, 1999.
54. Booth BJ, Doyle M, Montgomery J. Serial casting for the man-agement of spasticity in the head-injured adult. Phys Ther.1983;63:1960–6.
55. Cherry D, Weigand G. Plaster drop-out casts as a dynamicmeans to reduce muscle contracture. Phys Ther. 1981;61:
1601–3.56. Colditz JC. Efficient mechanics of PIP mobilisation splinting.
Br J Hand Ther. 2000;5:65–71.57. Taams KO, Ash GJ, Johannes S. Maintaining the safe position
in a palmar splint: the “double-T” plaster splint. J Hand Surg.1996;21B:396–9.
58. Ridgway CL, Daugherty MB, Warden GD. Serial casting as atechnique to correct burn scar contractures: a case report. JBurn Care Rehabil. 1991;12:67–72.
59. Rivers E. Management of hypertrophic scarring. In: Fisher S,Helm P (eds). Comprehensive Rehabilitation of Burns.Baltimore, Md.: Williams & Wilkins, 1984:177.
60. Mortimer PS. Therapy approaches for lymphedema.Angiology. 1997;48:87–90.
61. Ryan TJ, Mortimer PS, Jones RL. Lymphatics of the skin. Int JDermatol. 1986;25:411–9.
62. Colditz JC. Preliminary report of a new technique for castingmotion to mobilize stiffness [abstract]. J Hand Ther. 2000;13:72.
63. Colditz JC. Therapist’s management of the stiff hand. In:Mackin EJ, Callahan AD, Skirven TM, Schneider LH,Osterman AL (eds). Hunter, Mackin & Callahan’s Rehabilita-tion of the Hand. 5th ed. St. Louis, Mo.: Mosby, 2002:1021–49.
64. Weisman G, Pope MH, John RJ. Cyclic loading in knee liga-ments. Am J Sports Med. 1980;8:24–30.
65. Akeson WH, Amiel D, Woo SL. Immobility effects on synovialjoints: the pathomechanics of joint contracture. Biorheology.1980;17:95–110.
66. Donatelli R, Owens-Burkhart H. Effects of immobilization onthe extensibility of periarticular connective tissue. J OrthopSports Phys Ther. 1981;3:67–72.
67. Noyes FR. Functional properties of knee ligaments and alter-ations induced by immobilization. Clinical Orthop Rel Res.1977;123:210–41.
68. Brand PW, Hollister AM. Clinical Mechanics of the Hand. 3rded. St. Louis, Mo.: Mosby, 1999.
69. Merritt WH. Written on behalf of the stiff finger. J Hand Ther.1998;11:74–9.
70. O’Driscoll SW, Kumar A, Salter RB. The effect of the volume ofeffusion, joint position and continuous passive motion onintraarticular pressure in the rabbit knee. J Rheum. 1983;10:360–3.
71. Salter RB. The biologic concept of continuous passive motionof synovial joints: the first 18 years of basic research and itsclinical application. Clin Orthop Rel Res. 1989;242:12–25.
72. Van Royen BJ, O’Driscoll SW, Dhert WJA, Salter RB. A com-parison of the effects of immobilization and continuous pas-sive motion on surgical wound healing in mature rabbits. PlastReconstr Surg. 1986;78:360–6.
73. Meals RA. Post-traumatic limb swelling and joint stiffness arenot causally related experimental observations in rabbits. ClinOrthop. 1993;(287):292–303.
74. Arbuckle JD, McGrouther DA. Measurement of the arc of dig-ital flexion and joint movement ranges. J Hand Surg. 1995;20B:836–40.
75. Liepert J, Bauder H, Miltner WHR, Taub E, Weiller C.Treatment-induced cortical reorganization after stroke inhumans. Stroke. 2000;31:1210–6.
76. Byl NN, Merzenich M, Jenkins WM. A primate genesis modelof focal dystonia and repetitive strain injury, part I: Learning-induced dedifferentiation of the representation of the hand inthe primary somatosensory cortex in adult monkeys.Neurology. 1996;47:508–20.
77. Pascual-Leone A, Cammarota A, Wassermann EM, Brasil-NetoJ, Cohen L, Hallett M. Modulation of motor cortical outputs tothe reading hand of Braille readers. Ann Neurol. 2000;34:33–7.
78. Kaas JH. Plasticity of sensory and motor maps in adult mam-mals. Ann Rev Neurosci. 1991;14:137–67.
79. Merzenich M, Kaas J, Wall J, Nelson R, Sur M, Felleman D.Progression of change following median nerve section in thecortical representation of the hand in areas 3b and 1 in adultowl and squirrel monkeys. Neuroscience. 1983;10:639–65.
156 JOURNAL OF HAND THERAPY

80. Casley-Smith JR, Casley-Smith JR. High-protein oedemas andthe benzo-pyrones. Sydney, Aust.: Lippincott, 1986.
81. Casley-Smith JR, Gaffney RM. Excess plasma proteins as acause of chronic inflammation and lymphoedema: quantita-tive electron microscopy. J Pathol. 1981;133:243–72.
82. Junquerira LC, Carneiro J, Kelley RO. Basic Histology. 8th ed.Norwalk, Conn.: Appleton & Lange, 1995.
83. Leduc O, Peeters A, Bourgeious P. Bandages: scintigraphic
demonstration of its efficacy on colloidal protein reabsorptionduring muscle activity. Prog Lymphol. 1990;12:421–3.
84. Miller GE, Seale J. Lympathic clearance during compressiveloading. Lymphology. 1981;14:161–6.
85. Xujian S. Effect of massage and temperature on the permeabil-ity of initial lymphatics. Lymphology. 1990;23:48–50.
86. Ohkuma M. Skin and lymphatic system. Prog Lymphol. 1990;12:45–50.
April–June 2002 157

In the treatment of stiff joints, hand therapists havetraditionally used splints that position a joint at itsavailable end range in preference to manual stretchingtechniques. This practice is supported by the observa-tion of Brand that “every bit of tissue elongationaccomplished by stretch will shorten again when theforce is relaxed”1 and by similar findings of Frank etal. that “ligaments return to pre-stretch length.”2
Many splints are designed to increase permanenttissue elongation and hence improve passive rangeof motion (PROM), but the question of “which is thesplint of choice” in each case has customarily beendecided subjectively on the basis of a therapist’s clin-ical experience in the treatment of similar cases. Theliterature provides no objective guidelines to deter-mine the splint of choice.
Although this paper cannot offer research data toanswer this question, its purpose is to present anobjective decision-making scheme based on clinicalassessment of tissue compliance, for use in planninga splinting program for patients with joint stiffness.The scheme was devised to be consistent with theknown biology of joint stiffness and with my clinicalexperience.
TISSUE CHARACTER OF THE STIFF JOINT, AND COLLAGENRESPONSES TO LOADING
In 1966, Peacock3 demonstrated on a canine modelthat joint stiffness was the by-product of a period ofimmobilization following trauma. He also showedthat the primary tissue involved in joint stiffness was
the periarticular connective tissue—specifically, theligament and capsule that were placed in a shortenedposition during the period of immobilization. Otherinvestigators, such as Akeson et al.,4 have confirmedPeacock’s adaptive shortening concept, observingthat “soft-tissue (periarticular connective tissue)resistance may be in fact primarily responsible forclinical joint stiffness.”
In 1976, Arem and Madden5 published a seminalreport on the remodeling of scar in mice. They demon-strated (at autopsy) elongation of the scar substancethat had been subjected to prolonged, gentle stress. In1984, Light et al.6 reported that low-load prolongedstretch was more effective than high-load brief stretchin the treatment of stiff knees in human subjects.
Extrapolating from Light’s data, Flowers postulat-ed that the amount of increased range of motion inthese knees was proportional to the length of time thejoints were held in the end-range position. This wasthe inspiration for the term TERT (total end-rangetime). In 1994, Flowers and LaStayo7 published datato support the TERT principle, derived from a studyof 20 proximal interphalangeal (PIP) flexion contrac-tures in 15 patients. Their conclusion was thatincrease in PROM in stiff joints is directly propor-tional to the time the joint is held at the end range.
Not only did the Flowers and LaStayo paper estab-lish the TERT principle, it also supported an often-referenced Brand concept that previously had notbeen substantiated by data—namely, that it is betternot to use the word “stretch” for what should belong-term growth. If we want to restore normallength to a tissue that has shortened after disuse, weneed to reverse the process and apply the stimulus ofactivity or, better, hold the tissue in a moderatelylengthened position for a significant time. Then itwill grow.8
A Proposed Decision Hierarchy for Splintingthe Stiff Joint, with an Emphasis on
Force Application Parameters
Kenneth R. Flowers, PT, CHTPresident, Current Clinical Concepts, Inc.,San Francisco, California;Adjunct faculty,University of California San Francisco
158 JOURNAL OF HAND THERAPY
Correspondence and reprint requests to Kenneth R. Flowers, PT,CHT, 875 La Playa #278, San Francisco, CA 94121; e-mail: <[email protected]>.

FORCE APPLICATION THROUGHSPLINTING
Flowers and LaStayo7 suggested that TERT couldbe used to quantify the dosage of stress provided bysplints when a low-load prolonged stretch protocol isused. In 1994, McClure et al.9 published an algorithmfor the use of the TERT principle in clinical splintingof the stiff joint. However, a prescription for a dosagecontains not only the element of time but also the ele-ment of intensity. The McClure TERT algorithm doesnot address the variable of intensity expressed byforce or over-pressure. Indeed, no published datawere found that adequately address the issue of over-pressure in the splinting of stiff joints.
Many experienced therapists suspect that theapplication of a greater force will result in greatergains in PROM, much as longer application timeresults in greater gains in PROM as stated in theTERT principle. The decision hierarchy for splintingthe stiff joint proposed in this article extends thequantification of the collagen responses noted in theTERT principle to include the element of force, tosuggest a splinting prescription that is based on timeand intensity.
The clinical guideline that I have developed isbased on assessment of tissue compliance or the con-verse, stiffness. The basis for tissue compliance canbe found in the biomechanical principle of thestress–strain curve (Figure 1).
Tissue compliance has been clinically assessed invarious ways, using procedures with varyingdegrees of assessment reliability. A method forassessing stiffness that has been popularized by man-ual therapists and described by Cyriax10 is based onthe concept of end-feel. Using this method, the thera-pist passively carries the joint to its available endrange and manually applies a gentle over-pressure.The end-feel is that sensation imparted to the thera-pist’s hands as the restricted range is encountered.Based on “how it feels,” the therapist determines theend-feel and assesses the stiffness.
In my opinion, this method is highly subjective.McClure et al.11 reported poor inter-rater agreementin a controlled study in which experienced orthope-dic therapists tested the play of the joint in a humanknee model. The kappa values were only 0.38 whenthe knees were in 30° of flexion and 0.00 when theknees were fully extended. A more reliable methodof assessing the compliance of a joint would be use-ful to clinicians who treat joint stiffness.
Another, more objective method of assessing compliance or stiffness has long been advocated byBrand.12 This is the use of a torque angle curve (TAC). A TAC is constructed by passively moving a joint through its available range and recording aseries of goniometric readings at intervals, with
increasing force (torque) being applied to the joint—e.g., 20° at 200 g. This series of readings is plotted ongraft paper, and a smooth line is drawn connectingthe points. This smooth line is the TAC and is in actu-ality a form of a tension–elongation curve, as previ-ously described. The TAC is analyzed by applyingthe basic geometric tool of determining the slope ofthe curve, where the slope is defined as the rise overthe run. The interpretation of the TAC with regard totissue compliance or stiffness is as follows: The moregentle the slope, the more compliant the tissue; thesharper the slope, the stiffer the tissue.
No definitive data are available to validate theBrand TAC measurement. In 1985, in an attempt tosubstantiate Brand’s concept, Flowers and Pheasant13
reported the results of a study involving healthyphysical therapy students who each allowed the PIPjoint of their nondominant ring finger to be immobi-lized in a plastic cast in full extension. The period ofimmobilization varied from a minimum of 1 week forone group to a maximum of 6 weeks for anothergroup. Immediately following cast removal, theimmobilized hand of each subject was placed in awhirlpool bath for 20 minutes, and the subject wasencouraged to do AROM exercises. At the end of the20 minutes, PIP joint flexion was measured.
The investigators were hoping to plot TACs for eachgroup, anticipating sharper curves for the stiffer joints.Unfortunately, every subject had regained full flexionat the end of the 20-minute whirlpool session. Becauseno significant joint stiffness resulted from this methodof immobilizing uninjured joints, the study was notable to validate Brand’s theory of assessing joint stiff-ness through the use of TACs.
Over time, I have not found the TAC analysismethod to be clinically effective in my practice, and Ihave abandoned its use. I cannot say for certain whyI have not had success with it, because the rationalehas great appeal; perhaps my technique was poor.
April–June 2002 159
FIGURE 1. Tension-elongation or torque angle curve (TAC).Line ABCD is the curve for normal tissue, characterized by thelong “toe” section (AB) and steep slope of the terminal section(CD). Line AF is the curve for stiff, noncompliant tissue, char-acterized by a steep slope. Line AE is the curve for compliant tis-sue, characterized by a gentle slope.

In their 1978 textbook, Management of Acute HandInjuries, Weeks and Wray14 describe a clinical methodof assessing joint PROM using a defined force over adefined period of time. First, the joint is passivelytaken to its end range with a given force application.Next, the load is increased to a given amount andmaintained for a sustained period, such as 10 minutes,after which the PROM reading is repeated. The gain,or lack of gain, in PROM is used as an indicator of thelikelihood of success of further therapy, presumablythrough end-range splinting.
In fact, Weeks and Wray advocate the use of this testto determine whether to “operate, rehabilitate, orrate.” However, this measure does not attempt toquantify the potential of the stiff collagen tissue torespond to interventions aimed at elongating the tis-sue. It is important for a therapist to assess this poten-tial for change so that a splint design can be chosenand tailored not only to the degree of stiffness but alsoto the responsiveness of the stiffness.
The Weeks method of testing, which I have foryears referred to as simply “the Weeks test,” unlikethe Brand TAC method, does not look at the slope ofthe curve generated in the initial maneuver—whenthe joint is taken to its available end range in a single,gentle passive motion—but rather at the amount ofcreep shown in response to a sustained force overtime. Both the Weeks method and the Brand TACmethod were proposed to assess the same character-istic of the stiff joint—namely, its potential compli-ance—but they do so by looking at different charac-teristics of the joint’s response to passive force.
The Decision Hierarchy
The proposed decision hierarchy for splinting thestiff joint makes use of a modified Weeks test (MWT).The objective of the MWT is to provide clinicianswith a basis on which they can proactively formulate
a plan of splinting after determining whether jointstiffness is a significant problem. The numeric resultof the MWT is used as the guideline for splint selec-tion.
Before performing the MWT in a specific case, thetherapist must make an initial determination ofwhether joint stiffness is a significant problem. Thisfirst determination is typically done during thepatient’s initial evaluation, but the MWT is typicallynot performed until the patient’s next visit, becauseof time constraints on the initial visit.
The patient is instructed not to do any exercise orwear any splint on the day the MWT is to be per-formed. The objective of this instruction is to have thepatient present to the therapist with a joint that hasnot been stressed. Before any modality of treatmentor exercise is applied, the joint is measured passivelyusing standard goniometric technique. This firstPROM measurement is called the “cold reading.”
After the cold reading has been taken, the patientplaces the involved extremity in a thermal modality,preferably one in which motion is facilitated, such aswhirlpool bath or fluidotherapy rather than a con-stricting hot pack. The patient is instructed to active-ly exercise in the modality for 20 minutes. Immedi-ately following the thermal exercise period, thepatient is asked to manually position the involvedjoint at its available end range, apply a tolerable over-pressure, and maintain that force for 10 minutes.
Immediately on completion of the 10-minute over-pressure session, a second ROM reading is taken.This second reading is called the “preconditionedreading,” because it is presumed that, as a result ofthe exercise period and manual stretching, the jointhas met the definition of preconditioning describedin Fung’s Biomechanics: Mechanical Properties of LivingTissue.15 Preconditioning is the biophysical term forthe joint when it is “all stretched out” and is notgoing to yield to further force without undergoingdamage, such as microtrauma.
At this point, the two PROM readings are com-pared to establish the gain in PROM. As in the origi-nal test described by Weeks and Wray, the gain is theindicator of the compliance or stiffness and is used toguide the therapist in selecting the treatment ofchoice—in this case, to define “the splint parametersof choice.”
I have adopted the following guidelines in my clin-ical practice to decide the splint parameters of choice,no matter which extremity joint is being evaluated:
■ If the MWT results in a gain of (approximately)20°, I opt not to splint the patient but to relyinstead on an exercise program alone.
■ If the gain is of (approximately) 15°, I consider thejoint slightly stiff and go with the least stressfulend-range splint, a static splint which by defini-tion provides no over-pressure.
160 JOURNAL OF HAND THERAPY
Key Concepts
■ Elastic recovery of ligamentous length follows stretch
■ Trauma and immobilization result inadaptive shortening and stiffness
■ Gentle prolonged stress promotes tissue lengthening
■ Tissue compliance or stiffness is predictedwith the modified Weeks test
■ Dosage of force application is determined with the splinting decision hierarchy
■ Patient response is monitored to assess safety and effectiveness of splint program

■ If the gain is (approximately) 10°, the joint is sig-nificantly stiff and in need of some over-pressureto increase the stress delivery. This joint probablyrequires a dynamic splint. All experienced thera-pists know that there is, clearly, considerable vari-ation as to “how much tension” should be em-ployed in the use of dynamic splints. I am notaware of any objective guidelines for directingthis decision, except to respect the patient’s pain.
■ If the gain is on the order of 5° or less, the joint isvery stiff and will require the most aggressiveintervention. In my scheme, this indicates a staticprogressive splint that delivers unremitting over-pressure at the very end of the stress–strain curve.
These guidelines are summarized in Table 1.Clinical scientific validation of these procedures is
still in progress. This system is based on actualdegrees of change in PROM, but a similar approachusing percentage change might be as appropriate orbetter. This question would make excellent fodder forinvestigation.
Case Presentation
The following case presentation illustrates how theMWT was applied clinically. The patient was a 35-year-old secretary. On June 1, she fell while playingvolleyball and sustained a supracondylar fracture ofthe humerus of her nondominant arm. The fracturewas initially managed by K-wire percutaneous pin-ning and plaster immobilization for 28 days.
Following pin removal, the patient presented fortherapy on July 2. At the initial therapy evaluation, itwas found that a flexion contracture was a significantclinical problem and that the patient would probablyrequire splinting to regain functional ROM.
On July 3, the patient returned to the clinic for theMWT, which was performed in the following manner:
■ Passive ROM of elbow extension was measuredand found to be 60°.
■ The patient ‘s arm was immersed in a whirlpoolbath at 105° F for 20 minutes. The patient wasinstructed to actively flex and extend her elbowwithin her limits of pain throughout the whirlpoolsession.
■ At the end of the whirlpool session, the patientwas positioned with her arm resting on a tablepadded with a folded towel and was shown howto manually use her uninvolved arm to apply con-tinuous over-pressure into extension up to herpain tolerance. She used a palm-to-palm methodto grip her involved hand with her uninvolvedhand. Her involved forearm was supinated.
■ On termination of this manual stretching session,a second measurement of the PROM of extensionwas performed. The reading was 51°.
■ The change in PROM between the cold reading(the first reading) and the preconditioned reading(the second reading) was 9°.
■ On the basis of this MWT result, a dynamic elbowextension splint was fabricated and fitted.
■ The patient wore the splint for 30 minutes thatday in the clinic to test for tolerance to the splint.
■ A home-wearing schedule was established todeliver an initial TERT dosage of one hour a day.
■ A follow-up visit was scheduled for July 5, toassess reactivity and effectiveness.
DISCUSSION
In clinical practice, the MWT and its interpretationare user-friendly, in that they are straightforward toperform and both time- and cost-effective. When apatient appears to be reaching a plateau in PROMgains, repetition of the MWT is often helpful fordeciding whether to go up the hierarchy ladder to amore aggressive splint.
Prudent application of stress to overcome stiffnessrequires considerations beyond the initial choice ofsplint as aided by the MWT. The viscoelastic behav-ior of stress relaxation must be borne in mind in theuse of static progressive splints. The definition ofstress relaxation is that if a tissue is placed under ten-sion and the length of the tissue is held constant, aftera short time (perhaps 15 to 20 minutes), the amountof tension required to maintain that length decreasesas the tissue “relaxes.”15 However, this phenomenoncannot be repeated many times in rapid succession,because once the relaxation has occurred, the tissuelength is maintained by the elastic restraints withinthe tissue components, such as covalent cross-links.16
The potential for adverse response to stress deliv-ery must always be foremost in the therapist’s mind,The therapist is obligated to monitor the patient forany possible adverse reaction to the any low-loadprolonged stress therapy.
Typically, hand therapists monitor pain, swelling,ROM, and grip/pinch performance to assess adversereactions. It is intuitively obvious that any adversereaction calls for a diminution of the stress dosage. Inmany instances, the stiffness analysis of the MWT willindicate that a certain level of stress is needed, but the
April–June 2002 161
TABLE 1. Guidelines for Interpretation of the Modified Weeks Test
PROM Increase Splinting
About 20° No splint
About 15° Static splint
About 10° Dynamic splint
About 0°–5° Static progressive splint

patient will be unable to tolerate that level of stress. Insuch cases, the therapist must default to a lower levelof stress that can be tolerated by the patient andshould increase the stress only as tolerated.
The proposed splinting decision hierarchy for thestiff joint described here should not mitigate againstor override a dosage consideration that is based onthe TERT principle. The two measures of dose arecomplementary, not mutually exclusive. However,increased over-pressure should not be substitutedfor long TERT doses. Over-pressure is the interven-tion of last resort, because tissues are often too irrita-ble to tolerate significant over-pressure. So TERTtrumps over-pressure, but both may be required.
The face validity of a model of testing or treatmentoften comes from the clinic before research data arereported to substantiate its use. The vision of Brand,which was later substantiated by the TERT paper, is anexample. Clinicians can be stimulated to try theseuntested hypotheses in their own clinical practice.Scientific validation can come later in the form of con-trolled studies that grow out of clinical impressions.
The decision hierarchy presented here is purelytheoretic; it has not been substantiated by dataobtained under controlled conditions. We need datato support clinical impressions such as these.Concepts related to this topic would make fertileground for scientific investigation.
The MWT method is clearly only a model forassessing specific characteristics of joint stiffness andthe application of forces in splint selection. It isbeyond the scope of this paper to discuss the manyother nuances of splinting, such as choice of materi-als and fabrication.
CONCLUSIONS
■ To date, selection of the proper splint for manag-ing joint stiffness has been empirical.
■ To date, clinical methods of assessing joint stiff-ness or compliance have not been shown to bevalid or reliable.
■ This paper proposes a new method of assessingjoint stiffness or compliance called the MWT.
■ Guidelines are proposed for interpreting theMWT in the selection of the proper splint to man-age joint stiffness.
■ Data to substantiate the proposed model are lack-ing.
REFERENCES
1. Brand P. Hand rehabilitation: management by objectives. In:Hunter JM, Schneider LC, Mackin EJ, Callahan AD (eds).Rehabilitation of the Hand. 2nd ed. St. Louis, Mo.: Mosby,1984.
2. Frank C, Amiel D, Woo S. Normal ligament properties and lig-ament healing. Clin Orthop. 1985;196:15–24.
3. Peacock EE. Some biomechanical and biophysical aspects ofjoint stiffness. Ann Surg. 1966;164:1–12.
4. Akeson W, Amiel D, Woo S. Immobility effects on synovialjoints: the pathomechanics of joint contracture. Biorheology.1980;17:95–110.
5. Arem A, Madden J. Effects of stress on healing wounds: inter-mittent noncyclical tension. J Surg Res. 1976;20:93–102.
6. Light K, Nuzik S, Personius W. Low-load prolonged stretch vs.high-load brief stretch in treating knee contractures. PhysTher. 1984; 64: 330-333.
7. Flowers KR, LaStayo P. Effects of total end-range time onimproving passive range of motion. J Hand Ther. 1994;7(3):150–7.
8. Brand P. Clinical Mechanics of the Hand,. St. Louis, MO:Mosby, 1985; 62-67.
9. McClure PW, Blackburn LG, Dusold C. The use of splints in thetreatment of joint stiffness: biological rationale and an algorithmfor making clinical decisions. Phys Ther. 1994;74(12):1101–7.
10. Cyriax J. Textbook of Orthopedic Medicine, Vol 1: Diagnosis ofSoft Tissue Lesions. 6th ed. Baltimore, Md.: Williams &Wilkins, 1975.
11. McClure PW, Rothstein JM, Riddle DL. Intertester Reliabilityof Clinical Judgements of Medial Knee Ligament Integrity.Phys Ther. 1989; 69, # 4: 268-275.
12. Brand P. Clinical Mechanics of the Hand. St. Louis, Mo.:Mosby, 1985:62–7.
13. Flowers K, Pheasant S. The use of torque angle curves in theassessment of digital joint stiffness. J Hand Ther. 1985;1:69–75.
14. Weeks PM, Wray RC. Management of Acute Hand Injuries.2nd ed. St. Louis, Mo.: Mosby, 1978:434–8.
15. Fung Y. Biomechanics, Mechanical Properties of Living Tissue.New York: Springer-Verlag, 1981:211.
16. Peacock EE. Wound Repair. 3rd ed. Philadelphia, Pa.:Saunders, 1984:84–6.
162 JOURNAL OF HAND THERAPY

Static progressive splinting is a time-honored con-cept—not a new one. For more than 20 years, clini-cians have recognized the effectiveness of static pro-gressive splints to improve passive range of motion(PROM). Initially, clinicians used low-technology,grossly adjustable approaches to static progressivesplinting. Splint designers then sought a means toimprove the technique with components that offerinfinitely adjustable joint torque control and are easyto apply, lightweight, low-profile, and reasonablypriced.
Recognizing the power of static positioning, Flatt,in the 1994 edition of The Care of Congenital HandAnomalies,1 wrote, “Static splinting yields betterresults than dynamic forms” to increase PROM.(Here dynamic means “elastic/spring traction”splints.) Discussing rehabilitation of the elbow, notedsurgeons Nirschl and Morrey2 oppose the use ofdynamic splinting to gain motion.
In spite of such statements in the literature and theclinical success of static progressive splints,3–10 someclinicians still use dynamic or elastic forms exclusive-ly. With the number of clinicians who understand the
principles and benefits of static progressive splintingreaching a critical mass, this splinting approach hasthe potential to become the technique of choice forincreasing PROM. Static progressive splinting canachieve gains in PROM when other therapeutic andsplinting approaches fail.11
This article defines static progressive splinting anddescribes its advantages for improving PROM. It alsoclarifies the indications and contraindications for thissplinting approach and explains the unique mechan-ics of static progressive splinting. Regimen guide-lines for various aspects of static progressive splint-ing are provided, and many splint designs incorpo-rating the static progressive approach are illustrated.
DEFINITION OF STATICPROGRESSIVE SPLINTING
Static progressive splinting is the use of inelasticcomponents—such as hook and loop tapes, staticline, progressive hinges, turnbuckles, screws, andgears—to apply torque to a joint in order to staticallyposition it as close to end range as possible and thusincrease PROM (Figure 1).12–16 These componentsallow progressive changes in joint position as PROMchanges, without changes in the structure of thesplint. The variation in the gradability of the variousforce generators demands special attention, andTable 1 compares component gradability.
Karen Schultz-Johnson, MS, OTR, FAOTA, CHTDirector, Rocky Mountain Hand TherapyEdwards, Colorado;Adjunct FacultyRocky Mountain University of Health ProfessionsProvo, Utah
ABSTRACT: Static progressive splinting is the use of inelasticcomponents to apply torque to a joint in order to statically posi-tion it as close to end range as possible. It maximizes total end-range time, thus increasing passive range of motion. As tissuelengthens in response to this carefully applied stress, the clinicianor wearer adjusts the joint position to progress tissue at the newmaximum tolerable length. Static progressive splinting combinesprecision in joint position and torque application with patient-controlled stress to create an approach powerful enough to suc-ceed when no other treatment approach does. This article discuss-es static progressive splinting indications, contraindications, andadvantages as well as guidelines for a splinting regimen. It offersmany examples of static progressive splinting and makes clearthat this approach can be used with any mobilizing splint design.The unique mechanics of this splinting approach are described,and the various methods of achieving static progressive splintingare compared. Offering high levels of patient satisfaction andcompliance, static progressive splinting has come to the forefrontof clinical practice.J HAND THER. 2002;15:163–178.
Static Progressive Splinting
April–June 2002 163
The author has a financial interest in one or more products men-tioned in this article.Correspondence and reprint requests to Karen Schultz-Johnson,MS, OTR, FAOTA, CHT, Director, Rocky Mountain HandTherapy, P.O. Box 2145, Edwards, CO 81632; e-mail: <[email protected]>.

Static progressive splints may require adjustmentof the line or angle of pull as PROM progresses.When applied correctly, the static progressive splintholds shortened tissue at its maximum tolerablelength and does not stress beyond it12 (Figure 2). Astissue lengthens in response to this carefully appliedstress, the clinician or wearer adjusts the joint posi-tion to progress tissue at the new maximum tolerablelength. The process continues until the patientachieves desired tissue length and range of motion.
Clinicians apply other splinting approaches toincrease PROM. One such approach, the elastic trac-tion splint, uses self-adjusting resilient or elastic com-ponents such as spring wire, rubber bands, andsprings that create “a mobilizing force on a segment,resulting in passive or passive-assisted motion of a
joint or successive joints.”17 Such splints allow active-resisted motion in the direction opposite their line ofpull. The generated tension continues as long as theelastic component can contract, even when the short-ened tissue reaches the end of its elastic limit.
Clinicians often use the term “dynamic” for this typeof splint, because it has moving parts and resilientcomponents. However, the term “dynamic” is alsoused to describe a mobilizing splint—one that exertsforces on the involved joint or tissue to affect a changein joint motion.18 For purposes of clarity, this articleuses the term “elastic traction” to describe this type ofsplint. Although the combination of elastic compo-nents with inelastic components does increase controlover the force generated, it is not the same as static pro-gressive splinting. Figure 3 illustrates this concept.
Serial static splints are yet another splintingapproach to increasing PROM at a joint. A serial stat-ic splint positions the restricted tissue at maximumtolerable length. To accommodate increases in tissuelength and progress to a greater range of motion(ROM), the clinician must remold the splint to placethe tissue at the increasing maximum tolerablelength.16
INDICATIONS FOR STATIC PROGRESSIVE SPLINTING
The clinician applies a static progressive splint todecrease stiffness at a joint. Stiffness—the loss ofPROM at a joint, coupled with the need for increasesin muscular effort to achieve end range—continuesto be a common reason that patients attend clinics forupper extremity therapy. In her 1999 keynote addressat the American Association of Hand Surgeons semi-nar on joint stiffness, Maureen Hardy noted that,while hand specialists have made great strides inhand surgery and rehabilitation, joint stiffness con-tinues to be a challenge.
THE BIOLOGIC BASIS OF STATICPROGRESSIVE SPLINTING
The biological basis for using static progressivesplints to increase PROM lies in the ability of low-load prolonged stress to reorganize tissue in a man-ner conducive to motion and function. Loss of jointflexibility has two major sources—scar formation andadaptive shortening.19 Both create formidable barri-ers to motion.
Scar limits motion by several mechanisms. First, itssheer bulk may create physical blocks to motion.Second, it can limit the excursion of tissue when itspot-welds a moving structure to a nonmoving one.Finally, because scar consistently reorganizes in adenser form, the resulting tissue becomes progres-sively more resistant to lengthening and has lessviscoelasticity.19
164 JOURNAL OF HAND THERAPY
FIGURE 1. Static progressive splinting is the use of inelasticcomponents, such as hook-and-loop tape, static line, progressivehinges, turnbuckles, screws, and gears, to apply torque to a jointto increase passive range of motion.
TABLE 1. Gradability of Static Progressive ForceGenerators, from Most to Least Gradable
Infinitely adjustable:■ Can change the joint position by a fraction of a degree
and torque by a fraction of a gram■ Types of static progressive splinting components—
turnbuckles, screws, gears, and MERiT components (UE TECH, Edwards, Colorado)
Potentially infinitely adjustable:■ Progressive hinges have a continuous arc of motion and
position the joint at any degree of range of motion(ROM)■ Physically difficult to progress joint ROM and torque
exactly as desired
Grossly adjustable:■ Offer approximate adjustment in ROM■ Types of static progressive splinting components—
hook-and-loop tape, incremental hinges (change joint position to 10° to 30° increments)
NOTE: The higher the level of gradability, the more the patient cantake advantage of small changes in tissue length and excursion byrepositioning the joint at the new end range.

Adaptive shortening decreases the length of a tis-sue when the tissue is placed in a slack position. Thiscan occur quickly in the presence of inflammation, orit may occur over several weeks or months. Theshortened tissue restricts joint motion.
To reverse the motion-robbing effects of scar andadaptive shortening, a clinician faces the challenge ofchanging the length and density of the scar, scaradhesions, and adaptively shortened tissue. Toachieve these desired changes, the clinician controlsthe environmental demands on the tissue and appliesthe mechanical stimulus of stress. Living tissue,including scar, will reorganize and change inresponse to stress. The stress stimulus of tension trig-gers an increase in the length of the tissue.20
Clinical experience and the orthodontic and ortho-pedic literature support the use of low-load pro-longed stress over any other combination of load and
stress for achieving permanent increases in tissuelength and, therefore, in PROM.20–24 Although themechanism of action is unknown, low-load pro-longed stress appears to work by providing amechanical stimulus that causes scar to biologicallyremodel into a form conducive to motion. The scien-tific community has not yet quantified the exactamount of stress required to stimulate change in tis-sue length. However, in this author’s experience, theamount of stress required increases as the maturationof the scar progresses. Studies by Akeson et al.25 andby Frank et al.26 indicate that scar contracts andbecomes denser as it matures.
Although the clinician has many devices in thetherapy toolbox to control environmental demandson tissue and apply optimal stress, splinting is themost powerful. Splinting maintains tissue changesand elongation that have been gained during thera-
April–June 2002 165
FIGURE 3. Static progressive force generators use entirely inelastic components and do not combine elastic and inelastic components.Left, The flexion glove uses elastic traction, in the form of rubber bands attached to the glove, to flex the finger joints. (Photograph cour-tesy of Alimed, Inc.) Middle, This glove still uses rubber band elastic traction, but the rubber bands are attached to hook tape to trac-tion the finger joints into flexion. The inelastic tape allows some variation in the amount of force the elastic traction generates. However,the combination still creates elastic traction. (Photograph courtesy of Alimed, Inc.) Right, This glove uses static progressive traction, inthe form of inelastic splint line attached to hook tape, to traction the finger joints into flexion. This embodies true static progressive trac-tion, in which static force generators replace all elastic ones. (Photograph © Karen Schultz-Johnson.)
FIGURE 2. Static progressive splints allow adjustable tension and changes in joint position at any time. They establish a static tensionthat places tissue at maximum length but does not stress beyond it. As tissue remodels into a longer form, the patient or clinician can imme-diately adjust the splint to capture this increased tissue length and thus increase passive range of motion. (Artwork © Karen Schultz-Johnson.)

py, through a patient’s home program, and by func-tional use of the hand. Using low tension, it positionsthe joint at end range over long periods of time.
All forms of mobilizing splints base their effective-ness on the principle of stress application. A staticprogressive splint delivers the type of stress that tis-sue requires to overcome these barriers and toachieve desired increases in PROM.
Typically, the clinician employs experience and datafrom repeated evaluation to determine optimal stressloads. The clinician considers the effects of these threevariables—intensity, duration, and frequency—asthey mediate total stress delivery.19 Research has sup-ported the hypothesis that the longer tissue remains atmaximum tolerable length, the more it increases inlength.19,21 Thus, the key elements in increasing PROMare high time doses of low-load stress adequate to positionthe shortened tissue at or near the end of its currently avail-able length.
ADVANTAGES OF STATICPROGRESSIVE SPLINTING
Force and Range-of-Motion Adjustment
The ideal amount of torque exerted on a joint willbe the minimum necessary to achieve the goal pointin the PROM—that is, the maximum tolerable endrange. Of course, a relationship exists between thegoal PROM and the amount of force required toattain the goal. In the past, when elastic traction orgross static progressive methods were used, achiev-ing this exact relationship was one of the most diffi-cult aspects of splint fabrication and was oftenimpossible. With the advent of static progressivecomponents that offer infinitely variable tension, thisgoal is now easily achieved.
Elastic tension is not readily or precisely adjustable.It is difficult, and in some cases impossible, to establisha tolerable elastic tension that places tissue at maxi-mum length but does not stress beyond it. The elastic
component that can generate the amount of forceneeded to remodel mature scar may continue to short-en tissue to the point where it tractions the jointbeyond its currently available end range.
Although this amount of tension might initiallyappear desirable, and might appear to be the logicalsolution to the problem of lengthening tissue, in fact itis not. Stressing tissue beyond its available lengthcauses pain and ultimately creates micro-tears andincreased scar formation (Figure 4). Edema, heat, ery-thema, pain, and stiffness indicate that micro-traumahas occurred. The micro-tears, in turn, undergo thenormal phases of wound healing—inflammation,fibroplasia, and maturation. As the scar matures, itcontracts and further limits PROM.
Although serial static splints create constant ten-sion and joint positioning, the patient cannot movefrom the end range established by the clinician. Thesplint holds tissue at its current maximum length,and this tissue length remains the same until the cli-nician progresses the splint.
Force Control
Static progressive splints introduced an importantconcept into splinting regimens: patient-controlledforce. While a clinician may initially balk at giving thiscontrol to a patient, clinical experience has shown theeffectiveness of empowering the patient in this way.One need only imagine being placed in a splint withtension pre-set by a clinician who cannot know thephysical experience of that level of tension, especiallyover long periods of time, to appreciate the benefits ofpatient-controlled tension. The clinician can make aneducated guess about force adjustment. However,only the wearer can truly set the precisely correct load.
Static progressive splints have the advantage ofallowing the patient to instantly progress the splintrather than waiting for the therapist to do so. Thisresults in rapid gains in PROM as the patient takesimmediate advantage of incremental PROM increas-
166 JOURNAL OF HAND THERAPY
FIGURE 4. Elastic tension splints. An elastic component that can generate the amount of force needed to remodel mature scar may con-tinue to shorten to the point where it tractions the joint beyond its current available end range. This over-pressure may initially appear tobe a desirable and logical means of lengthening tissue, but it may cause further damage. Stressing tissue beyond its available length causespain and ultimately creates microtears and increased scar formation. As this new scar matures, it contracts and further limits passive rangeof motion. (Artwork © Karen Schultz-Johnson.)

es. The patient remains at end range until the patientor clinician re-adjusts the splint to optimize the com-bination of range of motion and tension. The value ofempowering the patient to adjust the splint cannot beoverstated.
The patient who has cognitive problems or wholacks kinesthetic feedback will not be a good candi-date for adjusting the splint tension independently.(Guidelines for clinician-controlled tension appearunder Static Progressive Splinting Regimen, below.)When allowing a patient to set the torque, the clini-cian must assume responsibility for providing thepatient with clear guidelines.
In contrast, elastic traction deprives both the clini-cian and the patient of control over force, becausesprings and elastics deform over time. Even when theclinician thinks that the splint tension has been set,patients will change the type of rubber band or itslength or will deform the spring in an attempt to con-trol splint tension. Ultimately, the patient exerts finalcontrol over a splint that exerts too much or too littletension: The patient simply removes it.
With an elastic traction splint, the patient can alsopull against the force and shorten the tissue on anintermittent basis. This thwarts the entire purpose ofthe splint—that is, to hold the tissue at its maximumlength for long periods of time.27
Splint Tolerance, Compliance, and Time Dosage
Because a static progressive splint positions the jointprecisely at end range with the appropriate amount offorce, and because the patient can increase and de-crease the tension, the static progressive splint maxi-mizes splint tolerance. This fosters compliance in theform of consistent and multiple-hour splint wear. Thetotal end-range time directly affects the speed andamount of PROM gain.21 Thus, the dosage of splintingthat a patient receives is critical to achieving optimaloutcome—the reorganization of tissue in a longerform, which in turn provides increased PROM.
With good splint tolerance comes the possibility ofsplint wear during sleep. This reduces or eliminatesthe need for daytime splint wear when the splintwould interfere with functional use of the hand andexercise. By wearing the splint at night, the patientreceives approximately 8 hours of therapy during a period when little is usually accomplished thera-peutically.
Application by Joint End-feel
A common misconception is that clinicians shoulduse static progressive splinting exclusively with hardend-feel joints and elastic tension splints exclusivelywith soft end-feel joints. (See Splint IndicationsAlgorithm: Applying Static Progressive Splints,below, for definitions of soft and hard end-feel joints.)
While many clinicians have found that static pro-gressive splints demonstrate a high level of effective-ness with hard end-feel joints,27,28 they also find thatstatic progressive splints often improve the PROM ofsoft end-feel joints faster than elastic tension splints.Clinical experience has shown that elastic tractionsplints often fail to improve the PROM of hard end-feel joints. This may be because of the splint tolerancefactors described above and the inability of a patientwith a hard end-feel joint to wear such a splint longenough to experience adequate total end-range time toachieve tissue remodeling.
Removability
The patient can remove a static progressive splintfor periods of exercise. Although serial casts maxi-mize compliance, distribute pressure, and also helpcontrol edema, they deprive the splinted joints ofactive range of motion (AROM). AROM encouragesfunctional organization of scar tissue and facilitateslengthening of adhesions in both directions.29 Motionpromotes nourishment of cartilage30,31 and helpspump high protein edema into the lymphatics.32 Bashand Spur state, “Serial casting immobilizes the arm,interferes with the performance of home exercise andactivities of daily living, and may cause stiffness inthe opposite direction.”4 Static progressive splintsoffer most of the benefits of serial static splints whilepermitting AROM.
Efficacy, Efficiency, and Cost Effectiveness
In this era of managed care, minimizing treatmentcosts and speeding the injured worker back to gain-ful employment are more important than ever before.The static progressive approach to splinting PROMlimitations helps the clinician meet the managed carechallenge. The speed with which static progressivesplinting succeeds in conjunction with the option forpatient-controlled tension results in a reduction inthe number of treatment sessions. Bonutti et al.33
demonstrated that static progressive splintingimproved PROM in cases in which no other treat-ment approach was successful. Such proven efficacydemands that clinicians seriously consider this treat-ment approach.
Static progressive splints represent a potential costsavings in comparison with serial static splints. Staticprogressive splints accommodate increases in jointmobility without the need to remold the splint toprogress PROM, saving the time for remolding orrefabrication that serial static splints require. Eachtime clinicians fabricate circumferential casts, theymust use consumable materials, necessitating addi-tional expense. Many static progressive componentsare reusable, minimizing materials expense.
Physicians and therapists have described patientswith contractures who were scheduled for surgical
April–June 2002 167

release prior to application of static progressivesplints. Because of the success of static progressivesplinting, surgery was cancelled. When comparingthe cost of static progressive splinting with the costsof surgical release of a joint, the effectiveness and fis-cal efficiency of the splinting become apparent. Staticprogressive splinting has provided improvements inPROM similar to or better than those gained by sur-gery, without the risks.
THE SPLINT INDICATIONS ALGORITHM: APPLYING STATICPROGRESSIVE SPLINTS
When evaluation reveals PROM loss, the clinicianuses decision-making techniques to identify theapproach to motion restoration that best suits thepatient’s many needs and characteristics. The clini-cian’s knowledge of the status of tissues relevant tothe stage of wound healing forms the basis for thedecision. Application of an appropriate splint alwaysrequires consideration of diagnosis, surgical proce-dure, the patient’s temperament, and the patient’sgeneral health.
Frequently, the clinician will choose a splint as partof the treatment plan. As a foundation for making thechoice between the various splinting approaches, cli-nicians have developed various algorithms thatmatch the type of splint with the phase of woundhealing. Figure 5 shows one such algorithm andserves as a guideline only.
The algorithm features the three phases of woundhealing—inflammation (acute), fibroplasia (prolifera-tive), and maturation (chronic):
The inflammatory phase of healing begins withinhours of trauma and continues for at least 3 days,although it may persist for days or weeks, especiallyin complex injuries, and can be renewed in responseto even a relatively minor trauma. . . . Local vasodila-tion permits the leakage of blood and plasma into theinjured area, creating increased edema, heat, redness,and pain, the classic signs of inflammation. Inflam-matory cells invade the wound but do not immedi-ately begin to form collagen.33
Fibroplasia begins 3 to 4 days after injury. Capillaryin-growth supplies nutrition to the area, and myofi-broblasts stimulate wound contraction. The presenceof inflammatory cells and products leads to fibroblastrecruitment and activity. Soon outnumbering othertypes of cells in the wound, the fibroblasts synthesizecollagen rapidly. At this phase, tissue inter-cellularbonds are fragile, making the wound susceptible torupture if it is exposed to excessive tension.
Approximately 3 weeks after injury, the size andcollagen content of the scar stabilizes. The woundactively turns over collagen, destroying old fibersand placing them with new ones. 33 At this point, thewound transitions to the maturation phase, when the
dynamic turnover of collagen provides for differenti-ation of scar to accommodate to the tissue type andthe stresses under which the tissue is placed. Themost active period of this phase lasts from 3 weeks to6 months. Remodeling continues for many moremonths at an ever-decreasing rate.33
At the beginning of the inflammatory phase, staticor serial static splints may provide the only appro-priate splinting approach. As the inflammatoryphase progresses toward its end, the clinician mayapply a static progressive splint to begin a gentle,controlled approach to increase PROM.
Not all patients will be able to tolerate passivetorque in the late inflammatory phase, and it shouldbe avoided with patients in some diagnostic cate-gories. For example, patient-controlled passive exten-sion is contraindicated for the patient who under-went a zone II flexor tendon repair 4 days previous-ly. However, a patient may be able to benefit from astatic progressive splint 4 days after metacarpo-phalangeal (MCP) capsulotomy. As stated above, theclinician considers multiple factors before applying asplint.
In the past, some clinicians delayed using staticprogressive splinting until the later phases of woundhealing, because they considered it a high-load gen-erator. This is a misconception. A static progressiveforce generator has a wide range of load application,from extremely low to extremely high. With the infi-nitely adjustable static progressive force generators,such as those incorporating gears and screws, therange of force—from low to high—is much morediverse than that achievable with a rubber band orspring. This makes static progressive splinting poten-tially applicable at the end of the inflammatory phaseand during the fibroplasia phase, even when tissue isat the lower ranges of tensile strength.
Thus, the clinician can employ a static progressiveapproach before considering elastic traction. It is upto the clinician to establish the correct amount of ten-sion or load for the given tissue. In addition, the cli-nician must set up the splint appropriately and teachthe patient how to use it.
During the late fibroplasia stage and the early matu-ration phase, the joint with limited PROM will oftenhave a compliant feel when the clinician applies pas-sive force to achieve end range. This compliant feel isoften called a “soft end-feel.”34 When applying mod-erate passive force to this type of joint, the therapistwill have the sense that the joint the joint rapidlyincreases its passive motion arc. Elastic traction splintsand serial static splints will ultimately provide thedesired result of increased PROM. However, clinicaluse suggests that static progressive splints increase therange of motion more rapidly than other splintingapproaches for this soft end-feel type of limitation.
Scar becomes denser in the maturation phase. Atthis point in the healing continuum, the tissue
168 JOURNAL OF HAND THERAPY

requires longer periods of end-range positioning andhigher loads in order to remodel. Some joints feelextremely limited and unyielding when the clinicianapplies passive force to achieve end range. Thesejoints are said to have a “hard end-feel.”34
In contrast to other splints, static progressive splintsare extremely effective with these types of joint range-of-motion problems. Static progressive splints cangenerate the appropriate forces and joint position in away that patients can tolerate for adequate forcedosage. Clinical experience and research33 have shownthat static progressive splints can make improvementsin hard end-feel joints when no other therapeuticintervention other than surgery can.
CONTRAINDICATIONS TO STATICPROGRESSIVE SPLINTING
Just as it is important to know indications for a stat-ic progressive splint, it is important to know its contra-indications. These contraindications are the same asthose for any type of mobilizing splint. They are:■ Joint instability■ Avascular necrosis ■ Acute inflammation*■ Infection ■ Unstable fractures■ Marked demineralization■ Myositis ossificans■ Heterotopic ossification■ Exostosis formation■ Loose body in joint■ Stress across healing structures that lack adequate
blood supply or that lack tensile strength to with-stand tensile stress
The clinician must carefully consider the appropri-ateness of applying a static progressive splint when apatient’s status includes of sensory loss or cognitiveimpairment, or both. The patient with compromisedsensation or cognition requires a splint design thatensures skin integrity while minimizing the risk ofvascular compromise and shear.
The patient with spasticity may benefit from a staticprogressive splint. However, because patients withhypertonic muscles often have sensory or cognitiveimpairment as well, the clinician must carefully con-sider the appropriateness of this splinting approachfor them. In addition, a patient with spasticity may bedependent on caregivers to don and doff a splint. Thisdependency may compromise splint effectiveness ifthe caregivers do not have adequate training in apply-ing and adjusting the splint. Splinting of patients withhypertonic muscles always requires a great deal ofassessment and clinical problem solving.
Three special diagnostic categories require specialcomment. They are:■ Dupuytren’s contracture ■ Motion loss due to tissue irradiation ■ Diseases creating fibrotic tissue
These diagnoses are contraindications to the appli-cation of not only static progressive splints but alsoany type of mobilizing splint.
Dupuytren’s contracture will not respond to low-load prolonged stress.35,36 Because of the nature ofDupuytren’s tissue, with its constituent myofibro-blasts, it will not remodel in the same way as normaltissue or scar. A patient with Dupuytren’s contrac-ture will respond to splinting only after surgery,because the surgery removes the unresponsive tissueand replaces it with scar. Scar tissue will respond tothe stresses that splinting imparts.
Irradiated tissue will usually not respond to low-load prolonged stress. Irradiated tissue is mostlyfibrotic and does not possess the same viscoelasticproperties as normal connective tissue. It lacks thenumber and type of live cells required to respond tothe mechanical stimulus and to reorganize.
April–June 2002 169
*The contraindication to static progressive splinting in the pres-ence of acute inflammation is diagnosis dependent and does notapply across the board. (See discussion of splinting during theinflammatory phase, under “Splint Indications Algorithm—Applying Static Progressive Splints.”)
FIGURE 5. As a foundation for making the choicebetween the various splinting approaches, clinicianshave developed various algorithms that match thetype of splint with the phase of wound healing.

Some types of pathology create fibrotic tissue.Powerful enough to sublux joints, the fibrotic tissuecontracts, creating deformity. Scleroderma may beone such entity. The clinician using a splint toincrease PROM in a patient with scleroderma mustuse great care and monitor the hand closely. Clinicalexperience suggests that fibrotic tissue does notrespond to splinting.
Whenever a clinician applies a splint, especiallywhen there is any doubt about splint appropriatenessor tolerance, the clinician must rigorously check forthe following signs and symptoms, which indicate aproblem with the splint: ■ Pain■ Heat■ Redness■ Edema■ Decreased range of motion■ Decreased strength ■ Decreased sensation
If any of these signs and symptoms are present, theclinician must thoroughly check the splint for fit andpressure distribution. It is especially important torethink the rationale for splint application to be cer-tain of its appropriateness.
STATIC PROGRESSIVE SPLINTING REGIMEN
The clinician is responsible for establishing anappropriate splinting regimen for each patient. Whendesigning a splint and instructing the patient in itsuse, the clinician must consider many issues, whichinclude (but are not limited to) acuteness of injury,time since surgery, wound status, stage of woundhealing, edema, pain, sensation, general health sta-tus, cognitive status, and motivation.12 Static pro-gressive splinting generally follows the same regi-men guidelines as any other type of splinting.
The patient may initially wear the splint for a brieftrial period (the clinician sets the duration) to deter-mine tolerance. During this trial period, the clinicianacquires feedback regarding appropriate fit, line ofpull, tension, and other important variables. Once thepatient can tolerate the splint for the trial period, theclinician may instruct the patient to wear the splintfor longer periods of time.
When designing the splinting regimen, the clinicianshould keep this basic principle in mind: The moretime the tissues spend at end range, the more quicklyPROM will improve.21 The clinician adapts this princi-ple for each patient. A range of splinting periods maybe used to treat a given patient successfully.
In this author’s clinical experience, a patient with acontracture that has a soft, springy end-feel can wearthe splint for 3 to 4 hours a day and obtain rapid, excel-
lent results. At the other extreme, a patient with a well-established hard end-feel contracture, who is compli-ant and well aware of splint precautions, may be ableto wear the splint 23.5 hours a day, removing it onlyfor hygiene. This approach has successfully improvedPROM when no other splinting approach did. Asmentioned earlier, a patient may also be able to wear astatic progressive splint during sleep, and thus obtain8 hours of end-range time that does not take awayfrom function and movement during the day.
Gains at a joint of 5° to 10° per week indicate splintsuccess. The splint wear schedule may require someexperimentation before the clinician and patient dis-cover the optimal one. Close monitoring of skin sta-tus, PROM, patient awareness of splint precautions,and patient acceptance of the splint, among other fac-tors, will help the clinician establish an ideal splint-ing regimen.
Static progressive splints offer the option of havingthe patient set the splint tension. Clinicians who haveno experience with patient-controlled tension may ini-tially feel apprehensive about allowing a patient toadjust a splint independently. A careful assessment ofwhether the patient can make healthy judgmentsabout splint tension and joint position will allay thisconcern. However, it should be kept in mind thatpatients wearing elastic traction splints self-adjust ten-sion by changing or shortening rubber bands, by mov-ing the hand in the splint, and by removing the splint.In this author’s experience, even patients from difficultpopulations—such as children, patients with languagebarriers, and patients with minimal education—canlearn to adjust splints properly. The responsibility lieswith the clinician to provide instructions in a way thatthe patient can comprehend.
Using simple, everyday language, the clinicianexplains the concept of low-load prolonged stress topatients. Illustration with examples that people canrelate to—such as braces straightening the teeth orpointy shoes deforming the foot—brings the concepthome. Making it clear that splints have the capacityto modify the tissue that restricts patients’ move-ment, the clinician instructs patients to position eachjoint so that they experience a mild to moderatestretch sensation at the joint or in the tissue adjacentto the joint. Patients must understand that gentlestress will give them the results they seek.
Although wearing a splint may not be easy, it mustbe pain free. Clinicians will find it very helpful tomake it clear to their patients that they will alwaysexperience stretch before pain. This will help themwith proper tension adjustment. Patients must alsounderstand that the use of too much tension will notincrease PROM faster. Rather, high force will re-injurethe tissue, producing more scar and increasing thetime before the joint moves as they would like. Seldomdoes a patient ignore these warnings when the clini-cian states the precautions clearly and emphatically.
170 JOURNAL OF HAND THERAPY

The patient without the cognitive skills or kines-thetic feedback to guide the splint tension presents aspecial challenge. In such a case, if the clinicianjudges a static progressive splint to be the splint ofchoice, she or he must establish the splint tension.Using range-of-motion evaluation, edema and tem-perature assessment, observation of color, and anunderstanding of the type and duration of thepathology to guide the decision, the clinician deter-mines joint position in the splint.
As a general guideline, the splint might position thejoint approximately 5° beyond readily available endrange. “Readily available range” means the range ofmotion that is easily achieved without dramaticallyincreasing joint torque. On a torque-angle ROM graph,this point occurs just before the line begins to curvesharply upward. Clinical experience has shown thatmany patients will be able to tolerate such a positionand still enjoy steady gains in PROM from splinting.
Another option is to position the joint by “feel.”The clinician applies torque to the target joint untilshe or he feels slight resistance. Using a light to mod-erate force, the clinician should set the splint to main-tain this desired position. Over time, the joint will“communicate” its needs and tolerances, and theposition will be adjusted. Every case is different, ofcourse, and only the clinician managing the individ-ual patient can determine the optimal joint position.
SPLINT DESIGN
The following pages present a wide range of staticprogressive splint designs that address PROM prob-lems at each joint of the upper extremity. It is alwayshelpful to remember that the optimal splint designresults when the clinician first asks “What does thishand need?” rather than “What splint goes with thisdiagnosis?”12 It is a common misconception that stat-ic progressive splinting can only be used with certainsplint designs (Figure 6). Let the splints illustratedhere stimulate ideas for unique designs to match eachpatient’s needs.
Although the nature of the PROM limitation con-trols most of the decision-making process with regardto the type and design of a static progressive splint,several other issues also come to the forefront. Theseare:■ Ease of splint construction■ Cost■ Weight■ Bulk■ Stability on the arm■ Material tolerance■ “Gadget tolerance”■ Compliance
When considering the ease of splint construction,the clinician must determine whether he or she hasthe skills and the time to make a given splint. Evenwhen using a prefabricated or rental splint, the clini-cian will need to be able to modify and fit the splintproperly to achieve optimal results with it.
Certainly, splint cost is a critical factor. The clini-cian and patient must decide together if a custom-fabricated, prefabricated, or rental splint best suitsthe specific financial situation.
The treatment team must also match the weightand bulk of a splint to the patient’s body and func-tion. Some patients may fail to tolerate certain mate-rials and will require alternative materials, padding,or liners.
While many patients are fascinated by the work-ings of a splint, others are undone by them. Thus, thepatient’s “gadget tolerance” comes into play. The cli-nician must evaluate each patient’s ability to toleratethe design and complexity of a splint.
The clinician’s careful consideration of each ofthese factors often determines the final factor—patient compliance with the splinting regimen. Ajudgment error in any of these factors will oftenresult in a patient’s failure to commit to the splintingregimen. Compliance failure will significantly com-promise ultimate outcome.
April–June 2002 171
FIGURE 6. It is a common misconception that static progressive splinting can be used only with certain splint designs. This wristextension splint uses the same base and components; only the force generator changes. Left, Elastic tension wrist extension splint.(Photograph © Karen Schultz-Johnson.). Right, Static progressive wrist extension splint. (Photograph © UE TECH.)

Considering the Amount of Torque withStatic Progressive Splinting
For many years, clinicians have cited a certainnumber of grams as the maximum torque to mobilizea joint. This guideline is based on the limitations ofskin under a conventionally sized finger sling madeof relatively soft material and not on the fragility of thetarget tissue.37
It is critical to understand that when mobilizingsplints are used, the skin, not the contracted tissue orscar, is usually the “weak link” in the system. Withimproved pressure distribution, the splint acting onwell-established contractures with fully healed tissuewill be able to generate more torque without tissuedamage. For this reason many of the splints picturedin this article feature rigid loops, because these dis-tribute pressure better.38
It appears that the longer the joint contracture hasexisted, the more force is required to achieve thePROM goals. As described above, scar becomesdenser as it matures and seems to require morecumulative mechanical force to alter its structure. Inaddition, larger joints require more torque thansmaller ones. Thus, the appropriate amount of torquewill vary with the stage of healing, the size of thejoint and the ability of the splint to distribute pres-sure along the skin surface.
To provide the optimum amount of torque, eachsplinted joint will require its own individual staticprogressive component. The example of two adja-cent MCP joints with extension contractures willhelp illustrate the reasons for this. Assessment oftwo such stiff joints will almost always reveal thatthey do not have the same PROM in flexion, that theamount of torque required to position each joint atend range differs, and that the PROM of each pro-gresses at a different rate. To avoid overstressing thestiffer joint, the tension the component generateswill need to be lighter. With the lighter force, the lessstiff joint will not receive the correct amount of ten-sion and may not benefit from the splint. With twoseparate static progressive components, however,each joint will receive the correct amount of torqueand can progress at to its own unique rate. In a likefashion, the therapist designing an elastic tractionsplint uses a separate rubber band or spring for eachjoint. An exception to this “one-joint, one-compo-nent” rule is when the tissue restricting motion is notspecific to the joint structure but rather the extrinsicsoft tissue affecting a joint series—for example, theMCP and interphalangeal (IP) joints of the thumb—such as with extrinsic extensor tightness.
Another exception is the final-flexion splint. Theunique design of this splint distributes the torque ofone static progressive component to position eachjoint at maximum tolerable end range.
Combining Static Progressive Splintingwith Other Splinting Approaches
Clinicians sometimes confront the challenge of ajoint with limited PROM paired with the need forperiarticular structures to undergo AROM. WhenAROM is essential and PROM is limited, a clinicianshould consider combining static and elastic tractionapproaches (Figure 7). The problems clinicians oftenface after flexor tenolysis exemplify this situation. Insuch a case, the patient may have PIP flexion con-tracture. The clinician must work to improve IPPROM in extension while focusing on active motionto allow free excursion of the tendon.
The splint shown in Figure 7 illustrates how thepatient can benefit from both approaches in onesplint—specifically, elastic traction for extension of thePIP joint, which allows active motion when the patientpulls against the traction (Figure 7, left), and static pro-gressive extension to hold the PIP joint at maximumtolerable end range (Figure 7, right). Clinicians mayfind that their patients can wear this splint in elastictraction mode during the day and in static progressivemode at night during sleep, when the tendon does nothave the opportunity to move.* Clinicians may alsoinstruct their patients to alternate between elastic andstatic progressive traction during the day.
A splint design may also combine the serial staticand static progressive or static and static progressiveapproaches. Bell-Krotoski describes the combinationof PIP joint serial casting with a mobilizing splint toincrease MCP joint flexion to reverse the joint con-tractures often seen with combined median and ulnarnerve lesions.39 The splint shown in Figure 8 illus-trates the use, in one splint, of serial casts for PIP jointextension with static progressive MP joint extensionfor a patient with extrinsic flexor tightness. An alter-native design for the same problem, the splint shownin Figure 9 puts a static finger extension platformtogether with static progressive MP joint extension.
The splint shown in Figure 10 effectively combinedstatic IP extension with static progressive flexion aftermetacarpal fracture, when the patient lacked MCPjoint flexion and IP joint extension. Figure 11 shows astatic splint base positioning the thumb metacarpal inmaximum flexion while the MP joint undergoes staticprogressive traction to increase passive flexion.
The clinician can use multiple types of static pro-gressive traction in one splint. The splint shown inFigure 12 makes use of a MERiT component (UETECH, Edwards, Colorado) to traction the wrist into
172 JOURNAL OF HAND THERAPY
*A clinician may instruct a post-tenolysis patient to set an alarmand get up once or twice a night to remove the finger sling of asplint set in static progressive mode, and actively move the finger.Although this may seem a difficult request, the results will justifythe effort. The patient–clinician team can determine the durationof this nighttime regimen.

April–June 2002 173
FIGURE 8. The use of serial casts for proximal interphalangealextension with static progressive metacarpophalangeal extensionin a single splint, for a patient with extrinsic flexor tightness.(Photograph © Karen Schultz-Johnson.)
FIGURE 9. An alternative design for extrinsic flexor tightness,this splint combines a static finger extension platform with staticprogressive metacarpophalangeal extension. (Photograph © KarenSchultz-Johnson.)
FIGURE 10 (near right andmiddle right). Combining staticsplints with static progressivesplints. Near right, This splintcombines a serial cast for distalinterphalangeal extension withstatic progressive proximal inter-phalangeal flexion. (Photograph© Karen Schultz-Johnson.) Middleright, This design effectively com-bines a static interphalangeal (IP)joint extension splint with staticprogressive metacarpophalangeal(MCP) joint flexion followingmetacarpal fracture, when thepatient lacked MCP joint flexionand IP joint extension. (Photograph© Karen Schultz-Johnson.)
FIGURE 11 (above right). A static splint base posi-tions the thumb metacarpal joint in maximum flexionwhile the metacarpophalangeal joint undergoes static pro-gressive traction to increase passive flexion. (Photograph© Karen Schultz-Johnson.)
FIGURE 12 (left). This splint shows a MERiT component thattractions the wrist into ulnar deviation while hook-and-loop tapeexerts pull on composite thumb metacarpophalangeal/inter-phalangeal joint flexion. The indication for this splint was limitedthumb flexion following deQuervain’s release when the extrinsicextensors of the thumb became adherent. (Photograph © KarenSchultz-Johnson.)
FIGURE 7. This splint shows how the patient can receive the benefits of both elastic traction and static progressive splinting approach-es in one splint with interchangeable force components. Left, Elastic traction for extension of the proximal interphalangeal (PIP) jointallows active motion when the patient pulls against the traction. Right, Static progressive extension holds the PIP joint at maximumtolerable end range.

ulnar deviation while hook-and-loop tape exerts pullon composite thumb MCP/IP joint flexion. The indi-cation for this splint was limited thumb flexion incombination with wrist ulnar deviation followingdeQuervain’s release, when the thumb extrinsicextensors became adherent. The hook-and-loop tapekept the splint lighter and was adequate for thepatient to create the gradations of force required tolengthen the adhesions.
Using creativity and expertise, the clinician hasmany options and splinting combinations availableto treat a patient’s PROM problems.
The clinician can use a static progressive approachwith any joint in the upper extremity. Splints canwork to improve either flexion or extension of a sin-gle distal interphalangeal (DIP), PIP, or MCP joint(Figures 13 to 16) or a combination of the finger joints(Figure 17). As described above, a single splint maybe designed to increase flexion at one joint and exten-sion at another (see Figure 10).
Some clever splint designs facilitate motion inalternating directions, such as flexion and extension(Figure 18) or pronation and supination (Figure 19).In another example, when a patient complained thatshe had too many splints to wear for her multiplePROM limitations after a serious motor vehicle acci-dent, her therapist designed a splint that combinedfinger DIP/PIP joint flexion, MCP joint extension,wrist extension, and forearm rotation. Unfortunately,the splint failed the “gadget tolerance” test, and thepatient declined to wear it. Common goals of splintsinclude increasing wrist flexion (Figure 20) or exten-sion (Figure 21), the span of the thumb web, elbowflexion (Figure 22) or extension, and shoulder abduc-tion and external rotation (Figure 23).
SUMMARY
Clinical experience and research have supported theefficacy of static progressive splinting to improvePROM quickly and efficiently. Many clinicians, whenfaced with PROM limitations in a patient, find thatstatic progressive splinting is the technique of choice.This article reviews the literature, the benefits ofpatient-controlled tension, and splint mechanics tosupport the advantages of this splinting approach. Thecombined benefits of achieving precise torque andjoint position with patient-controlled tension result inhigh splint tolerance, compliance, and patient satisfac-tion. The static progressive approach creates a highlyeffective means to deliver an adequate dose of totalend-range time. Maximizing total end-range time willmake it possible to achieve treatment goals.
The classification of static progressive splinting asonly a high-force generator is a misconception. A stat-ic progressive force generator has a wide range of loadapplications, from extremely low to extremely high.Any tissue that can tolerate elastic traction can toleratestatic progressive traction. The principle “always useelastic splinting with soft end-feel joints and static pro-gressive splinting with hard end-feel joints” is incor-rect. While it is true that only static (i.e., static progres-sive, serial static) splinting approaches will successful-ly improve many hard end-feel joints, static progres-sive splints will also resolve soft end-feel contractureswith great speed. Thus, while specific diagnoses orpatient characteristics may dictate specific approachesto splinting joints with PROM limitations, anysplintable joint limitation will respond to static pro-gressive splinting.
174 JOURNAL OF HAND THERAPY
FIGURE 15. Static progressive splint to increase proximalinterphalangeal joint extension. (Photograph courtesy of theRehabilitation Division of Smith & Nephew, Inc.).
FIGURE 16. Static progressive splint to increase metacarpo-phalangeal joint flexion. (Photograph © Karen Schultz-Johnson.)
FIGURE 13 (left). Static progressive splint to increase distalinterphalangeal joint flexion. (Photograph courtesy of PamSchindeler-Grasse and Pattie Paynter.)
FIGURE 14 (right). Static progressive splint to increase proxi-mal interphalangeal joint flexion. (Photograph © Karen Schultz-Johnson.)

April–June 2002 175
FIGURE 17. Static progressive splints that simultaneously flex more than one finger joint at a time. Left, This design, called a final flexion splint, uses a MERiT component. (Photograph © UE TECH.) Middle, This splint uses a unique design with hook-and-loop tape.(Photograph courtesy of AliMed, Inc.) Right, Splint to increase proximal and distal interphalangeal joint flexion. (Photograph © Karen Schultz-Johnson.)
FIGURE 18. Some clever splint designs facilitate motion in alternat-ing directions, such as flexion (above) and extension (right), hereillustrated at the elbow. (Photograph © UE TECH.)

176 JOURNAL OF HAND THERAPY
FIGURE 21. Left, Static progressive splint to increase wrist extension using a progressive hinge. (Photograph courtesy of theRehabilitation Division of Smith & Nephew, Inc.) Right, Static progressive splint to increase wrist extension using a DigiTECH out-rigger. (Photograph © UE TECH.)
FIGURE 20. Static progressive splint to increase wrist flexion. (Photograph© UE TECH.)
FIGURE 19. Another splint design that facilitates motion in alternating directions, here illustrated at the forearm for supination (left)and pronation (right). (Artwork © UE TECH.)

April–June 2002 177
FIGURE 22. Above, Static progressive hinge splint to increase elbow flex-ion (Photograph courtesy of Alimed, Inc.) Right, Static progressive splint toincrease elbow flexion. (Photograph reprinted, with permission, from BashDS, Spur ME. An alternative to turnbuckle splinting for elbow flexion. JHand Ther. 2000;13[3]:237–40.)
FIGURE 23. Static progressive splint toincrease shoulder abduction and externalrotation. (Photograph courtesy of JointActive Systems, Inc.)

The clinician can apply static progressive splints toany joint or group of joints in the upper extremity.Static progressive splint designs run the gamut of asplint maker’s imagination; they are not limited tocertain patterns or specific applications. A cliniciancan use static progressive force generators in place ofelastic components in any existing splint design.
Clinicians report cases of PROM that improved withstatic progressive splinting when no other approachworked. Because of their successes with static progres-sive splinting, clinicians have reported the cancellationof scheduled patient joint capsulotomies.
Nothing can be more gratifying than making a pos-itive difference in people’s lives. The static progres-sive approach to splinting gives clinicians the powerto do that for their patients.
REFERENCES
1. Flatt AE. The Care of Congenital Hand Anomalies. St. Louis,Mo.: Quality Medical Publishing, 1994:204.
2. Nirschl RP, Morrey BF. Rehabilitation. In: Morrey BF (ed). TheElbow and Its Disorders. 2nd ed. Philadelphia, Pa.: Saunders,1993:177–8.
3. Mullen TM. Static progressive splint to increase wrist exten-sion or flexion. J Hand Ther. 2000;13:313–4.
4. Bash DS, Spur ME. An alternative to turnbuckle splinting forelbow flexion. J Hand Ther. 2000;13:237–40.
5. Blackmore S. Splinting for elbow injuries and contractures. In:Skirven T, Raphael J. Contractures and splinting. Atlas of theHand Clinics. Philadelphia, Pa.: Saunders, 2001;6(1):21–50.
6. Colello-Abraham K. Splinting for the forearm contracture. In:Skirven T, Raphael J. Contractures and splinting. Atlas of theHand Clinics. Philadelphia, Pa.: Saunders, 2001;6(1):61–76.
7. Lucas S. Splinting the stiff wrist. In: Skirven T, Raphael J.Contractures and splinting. Atlas of the Hand Clinics.Philadelphia, Pa.: Saunders, 2001;6(1):77–106.
8. Moscony A. Splinting for extension contractures of the digit.In: Skirven T, Raphael J. Contractures and splinting. Atlas ofthe Hand Clinics. Philadelphia, Pa.: Saunders, 2001;6(1):117–34
9. Hobson L. Splinting for the proximal interphalangeal jointflexion contractures. In: Skirven T, Raphael J. Contractures andsplinting. Atlas of the Hand Clinics. Philadelphia, Pa.:Saunders, 2001;6(1):135–58.
10. Schindeler-Grasse P, Paynter P. Splinting for thumb contrac-tures. In: Skirven T, Raphael J. Contractures and splinting. Atlasof the Hand Clinics. Philadelphia, Pa.: Saunders, 2001;6(1):165–88.
11. Bonutti PM, Windau JE, Ables BA, Miller BG. Static progres-sive stretch to re-establish elbow range of motion. Clin OrthopRel Res. 1994;303:128–34.
12. Schultz-Johnson KS. Splinting: a problem-solving approach. In:Stanley BG, Tribuzi SM (eds). Concepts in Hand Rehabilitation.Philadelphia, Pa.: Davis, 1992:238–71.
13. McKee P, Morgan L. Orthotics in Rehabilitation. Philadelphia,Pa.: Davis, 1992:238–71.
14. Coppard BM. Lynn P. Introduction to splinting. In: CoppardBM, Lohman H (eds). Introduction to Splinting: A Clinical-rea-soning and Problem-solving Approach. 2nd ed. St. Louis, Mo.:Mosby, 2001:9.
15. Wilwerding-Peck J. Mobilization splints. In: Coppard BM,Lohman H (eds). Introduction to Splinting: A Clinical-reason-ing and Problem-solving Approach. 2nd ed. St. Louis, Mo.:Mosby, 2001:261–2.
16. Hogan L, Uditsky T. Pediatric Splinting: Selection, Fabrication,and Clinical Application of Upper Extremity Splints. SanAntonio, Tex.: Therapy Skill Builders, 1998:18.
17. Fess EE, Philips C. Hand Splinting: Principles and Methods. 2nded. St. Louis, Mo.: Mosby, 1987:86.
18. Bailey JM, Cannon NM, Fess EE, et al. (eds). Splint Classi-fication System. Chicago, Ill.: American Society of HandTherapists, 1992:5.
19. Flowers KR, Michlovitz SL. Assessment and management ofloss of motion in orthopedic dysfunction. In: PostgraduateAdvances in Physical Therapy. Alexandria, Va.: AmericanPhysical Therapy Association, 1988.
20. Arem A, Madden J. Effects of stress on healing wounds: inter-mittent noncyclical tension. J Surg Res. 1976;20:93–102.
21. Flowers KR, LaStayo P. Effect of total end-range time onimproving passive range of motion. J Hand Ther.1994;7(3):150–7.
22. Light K, Nuzik S, Personius W, et al. Low-load prolongedstretch versus high-load brrief stretch in treating knee contrac-tures. Phys Ther. 1984;64:330–3.
23. Hotchkiss RM. Application of hinged external fixator forelbow limitations. ASSH meeting, Snowmass, Colorado,March 1995.
24. Hotchkiss RM. Design rationale. Literature accompanyingElbow Compass Hinge.
25. Akeson WH, Ameil D, Woo SL-Y. Immobility effects on syn-ovial joints: the pathomechanics of joint contracture. Bio-rheology. 1980;17:95–110.
26. Frank C, Ameil D, Woo SL-Y, Akeson WH. Normal ligamentproperties and ligament healing. Clin Orthop Rel Res.Philadelphia, Pa.: Lippincott, 1985;196:15–24.
27. Bell-Krotoski JA. Plaster casting for the remodeling of soft tis-sue. In: Fess EE, Philips C. Hand Splinting: Principles andMethods. 2nd ed. St. Louis, Mo.: Mosby, 1987:453–4.
28. Fess EE, Philips C. Hand Splinting: Principles and Methods. 2nded. St. Louis, Mo.: Mosby, 1987:297.
29. Brand PW, Hollister AM. Clinical Mechanics of the Hand. 3rded. St. Louis, Mo.: Mosby, 1999:268.
30. Salter RB, Simmonds DF, Malcolm BS, et al. The biological effectof continuous passive motin on the healing of full thicknessdefects in articular cartilage. J Bone Joint Surg. 1980;62A:1232–51.
31. Dimick MP. Continuous passive motion for the upper extremi-ty. In: Hunter JM, Schneider LH, Mackin EJ, Callahan AD (eds).Rehabilitation of the Hand: Surgery and Therapy. 3rd ed. St.Louis, Mo.: Mosby, 1990:195–220.
32. Artzberger S. Manual Edema Mobilization Manual. 2001.33. Stewart KM. Therapist’s management of the complex injury. In:
Hunter JM, Mackin EJ, Callahan AD (eds). Rehabilitation of theHand: Surgery and Therapy. 4th ed. St. Louis, Mo.: Mosby,1995:1058.
34. Cyriax J. Textbook of Orthopedic Medicine, vol. 1: Diagnosis ofSoft Tissue Lesions. 8th ed. Philadelphia, Pa.: Bailliere Tindall,1982:53.
35. Abbot K, Kenney J, Burke F, et al. A review of attitudes to splin-tage in Dupuytren’s contracture. J Hand Surg. 1987;12B:326–8.
36. Sampson S, Badalamente M. Hurtst L, et al. The use of a passivemotion machine: the postoperative rehabilitation of Duputren’sdisease. J Hand Surg. 1992;17A:333–8.
37. Brand PW. Splinting to increase PROM [question-and-answerperiod following lecture]. The Insensitive Hand: Biomechanicsof Deformity Symposium at G. W. Long Hansen’s DiseaseCenter, 1988.
38. Brand PW, Hollister AM. Clinical Mechanics of the Hand. 3rded. St. Louis, Mo.: Mosby, 1999:223–7.
39. Bell-Krotoski JA. Plaster casting for the remodeling of soft tis-sue. In: Fess EE, Philips C. Hand Splinting: Principles andMethods. 2nd ed. St. Louis, Mo.: Mosby, 1987:449–66.
178 JOURNAL OF HAND THERAPY

Lateral epicondylitis is a common problem, itsprevalence ranging from 1% to 3% of the generalpopulation, increasing to 19% of men in the fifthdecade of life.1 Since its introduction in 1971, the fore-arm support band (also known as the “tennis elbowband” or “counterforce brace”) has been widelyincorporated into the treatment regimens of manypatients with lateral epicondylitis.2 Application ofthis orthotic to the forearm has been hypothesized todecrease the tension of the extensor carpi radialis bre-vis (ECRB) origin on the lateral epicondyle withactivity.
Since tendinosis of the ECRB origin at the lateralepicondyle is thought to be the pathologic lesion oftennis elbow, symptomatic relief would intuitivelybe expected if tension were reduced at the origin ofthe ECRB. Conservative therapy usually focuses onstretching and strengthening exercises with concomi-tant activity modifications, generally with a high clin-ical success rate. In more difficult cases that are notresponsive to these modalities, however, treatmentsuccess is unpredictable.
Standard tennis elbow braces, specialized tenniselbow braces (e.g., Aircast braces, Aircast, Inc.,Summit, New Jersey), corticosteroid injections, andwrist extension braces have been proposed as contin-ued conservative treatment of lateral epicondylitisrefractory to initial therapeutics. Each of these treat-ment modalities lacks definitive evidence to supportor refute its use in the treatment of lateral epicondyli-tis.3–6 An attempted meta-analysis of the literature onlateral epicondylitis treatment methods, performedby Labelle et al.,7 found insufficient evidence to sup-port any particular treatment. This analysis conclud-ed that the most important factor in treatment of lat-eral epicondylitis is the natural evolution of the dis-ease and the placebo effect of its treatment.
An electromyographic study of the forearm exten-sors with the application of both standard and Aircasttennis elbow bands showed reduced electromyo-graphic activity with both bands; statistically signifi-cant reduction was shown only with use of the Aircastband.6 This study did not control for the force at whichthe two bands were applied, stating that the bandswere applied “snugly without pinching the skin,” thusrendering the results difficult to interpret. Jansen et al.5
reported an additional electromyographic study eval-uating the effect of various wrist orthoses on the wrist
Nicholas J. Meyer, MDDepartment of Orthopaedic SurgeryMedical College of WisconsinMilwaukee, Wisconsin
William Pennington, MDDepartment of Orthopaedic SurgeryMedical College of Wisconsin
Barb Haines, OTR, CHTDepartment of Orthopaedic SurgeryMedical College of Wisconsin
Roger Daley, MD, PhDDepartment of Orthopaedic SurgeryMedical College of Wisconsin
ABSTRACT: The forearm support band is hypothesized toreduce force, and thus inflammation, at the extensor carpi radialisbrevis (ECRB) origin. Very little published evidence supports anactual effect on the forces at the ECRB origin, however. Theauthors describe a cadaveric study in which forces at the ECRBorigin were measured while various pressures were applied to theforearm support band and the ECRB tendon was loaded distally.The results reveal an increased effect with increased band pres-sure and a decreased relative effect with increased force applieddistally. For clinical correlation, application pressure was alsomeasured in nine patients using a counterforce brace. While fur-ther clinical evaluation is necessary to determine the most appro-priate clinical indications for use of a forearm support band, theseresults suggest that the forearm support band may be most effec-tive when applied at a force of 40 to 50 mmHg and used duringlight-duty activities. J HAND THER. 2002;15:179–184.
The Effect of the Forearm Support Band on Forces at the Origin of the
Extensor Carpi Radialis Brevis: A Cadaveric Study and Review of Literature
April–June 2002 179
Correspondence and reprint requests to Nicholas J. Meyer, MD,Department of Orthopaedic Surgery, Medical College ofWisconsin, 9200 W Wisconsin Avenue, Milwaukee, WI 53226; e-mail: <[email protected]>.

extensor muscles. This study demonstrated elec-tromyographic changes in the wrist extensors exclu-sively during lifting activities. No electromyographicdifference was noted with gripping activities.5
Regardless, no studies have shown that electromyo-graphic changes translate to clinical improvement inpatients with lateral epicondylitis.
The clinical effect of the tennis elbow band has alsobeen controversial. A study measuring pain-free gripstrength and pain scores in patients with lateral epi-condylitis without brace treatment, with a tenniselbow brace, and a placebo brace showed no changein acute pain or strength.8 This study acknowledged,however, that the brace may be effective for extend-ed periods, but this was not studied. Another studyshowed an increase in wrist extensor strength duringrapid repetition activities with application of thebrace in asymptomatic persons.9
In light of this review of the literature, the purposeof our study was to develop a cadaveric model usinga forearm support band, with the goal of measuringthe percentage force reduction at the ECRB originwith application of a forearm support band at vari-ous pressures. This model would allow us to deter-mine whether an actual mechanical effect exists. Toaccurately correlate this cadaveric study with a clini-cal scenario, the pressure at which patients routinelyapply the forearm support band was also measured.An attempt was made to duplicate these pressures inthe cadaveric model.
METHODS
Five cadaver arms transected at the mid-humeruswere mounted to a support frame in neutral supina-tion/pronation, neutral wrist extension/flexion, and90° elbow flexion, using Steinman pins through thedistal ulna and proximal humerus. The ECRB tendonwas isolated distal to the intersection of the extensorpollicis brevis and abductor pollicis longus through a3-cm longitudinal incision. A #5 suture was placed
through and around the tendon at this point andpassed through a low-friction pulley for applicationof weight. The ECRB origin was isolated through a5-cm incision over the lateral epicondyle. A #5 suturewas passed deep to and through the ECRB tendonorigin and was subsequently connected to a customforce transducer. A blood pressure cuff measuring5-cm in width was applied to the forearm and cen-tered 5-cm distal to the lateral epicondyle (Figure 1).
The force transducer was initially calibrated with noweight applied to the tendon and the cuff deflated. Forthe first trial, 5 lb was applied to the tendon distallyand the force at the ECRB origin recorded. The weightwas removed, the cuff was inflated to 50 mmHg, theweight re-applied, and the force again measured at theECRB origin. This sequence was repeated through fivecycles. Similarly, the entire sequence and five trialswere repeated with cuff pressures of 50, 100, 150, and200 mmHg and loads of 5, 10, and 15 lb being appliedsequentially to the tendon distally.
The recorded data consisted of voltage as measuredby the force transducer attached to the ECRB origin,cuff pressure, and weight applied to the distal tendon.The voltage was recorded for all trials with 0, 5, 10,and 15 lb applied as well as with 0, 50, 100, 150, and200 mmHg cuff pressure. Absolute force at the ECRBorigin was not calculated; however, force as a percent-age of control (no cuff pressure) was measured andrecorded. Standard deviation was calculated in stan-dard fashion. A Student t test was used to calculatep values for the comparison with force reductions at50 mmHg cuff pressure.
To determine the force at which an average patientapplies the tennis elbow brace, nine patients currentlybeing treated for lateral epicondylitis were studied. Apediatric blood pressure cuff measuring approximate-ly 5 cm in width was insufflated with a small amountof air, inserted into the pocket of an Aircast forearmsplint, and applied by the patient in normal fashion tothe same level of tightness that the patient normally
180 JOURNAL OF HAND THERAPY
FIGURE 1. Experimental set-up. Schematic of cadaver modelshowing the ECRB tendon loaded by a fixed weight distally (0, 5,10, or 15 lb), the origin monitored by a strain gauge, and theforearm support band cuff pressure regulated.
FIGURE 2. Force reduction trends related to cuff pressure andforce applied distally. The percentage force reduction with appli-cation of the forearm cuff reveals a trend as cuff pressure increas-es and as additional weight is applied distally. This was statisti-cally significant for the 5- and 15-lb trials, but not for the 10-lbtrial.Vertical hatching indicates 50 mmHg pressure; white, 100mmHg; horizontal hatching, 150 mmHg; black, 200 mmHg.

applies the counterforce brace. This pressure wasrecorded, the patient performed maximal grip, and theresulting cuff pressure and grip force were recorded.This was applied and re-applied three times, and theaverage application pressure and grip force wererecorded for each patient.
RESULTS
Four of the cadaver arms were used for experimen-tation. One arm showed abnormal adhesions of thetendon distally and produced inconsistent results.This trial was discarded from statistical analysis. Atrend was observed for the trials and is graphicallyrepresented in Figure 2. As cuff pressure was increas-ed, the percentage force reduction also increased. Inaddition, with increasing loads to the tendon distally,the percentage force reduction decreased (that is, thepercentage effect was less with higher loads).
Table 1 shows the percentage change in force com-pared with control values (no cuff pressure) for eachamount of pressure and force applied distal to thecuff. Standard deviation and p values derived fromcomparison with findings at 50 mmHg pressure arealso included.
Statistically significant differences were noted in alltrials with 5 and 15 lb applied to the ECRB distally, butnot with 10 lb applied. However, the trend appearedto fit as expected between the 5- and 15-lb trials.Review of the raw data revealed that one specimen inthe 10-lb trial had statistically significant deviationfrom the other specimens in its group, but this was notfound in the 5- or 15-lb trial. Thus, the specimen could
not be excluded from statistical analysis on the basis ofthis deviation (at the 10-lb trial) alone. Given the limit-ed number of specimens used in the trials, theachievement of statistical significance for all trials isdifficult. More important, however, these trials didshow a consistent and logical trend.
Clinical measurement of forearm band pressure innine patients familiar with the use of the bandshowed high variability in resting pressure of appli-cation. The average force at which the cuff wasapplied was 45 ± 25 mmHg (range, 21–101 mmHg).This pressure rose to 86 ± 39 mmHg (range, 42–150 mmHg) during maximal grip and was independ-ent of grip force produced (Figure 3).
DISCUSSION
Many authors agree on a common theoretic mecha-nism of action for the counterforce forearm band.Presumably by inhibiting muscle expansion, the banddecreases the magnitude of muscle contraction andthereby reduces tension at the musculotendinous unitproximal to the band.5,6,10,11 Other authors proposeadditional benefits of minimizing exaggerated tendonmovement,12 decreasing the force contribution bymuscle fibers proximal to the band,6 dispersing stressaway from the pathologic area by “broadening” thearea of the common extensor muscle origin, or direct-ing potential stress overloads to healthy tissues andpossibly the band itself.13 Nirschl14 agrees that tensionat the musculotendinous unit proximal to the band isreduced, but suggests that the brace acts by supplyingthe extensor muscle mass with a second origin distal tothe radial head, thereby decreasing the fulcrum effectthat occurs at the attachment to the lateral epicondyle.
Since our model is a purely passive system (withno active muscle activity), we cannot comment onany electromyographic effect or reduction in muscleactivity. However, our study does support Nirschl’s
April–June 2002 181
FIGURE 3. Cuff pressure during rest and grip, as related togrip force. Among the nine patients experienced in the use of thetennis elbow band, the average force at which the cuff wasapplied was 45 ± 25 mmHg (range, 21–101 mmHg). This pres-sure rose to 86 ± 39 mmHg during maximal grip and was inde-pendent of grip force. Black indicates resting pressure; white,gripping pressure.
TABLE 1. Percentage Force Reduction Related to Cuff Pressure and Force Applied Distally
Cuff Force Pressure Reduction SD SE p
(mmHg) (%) Value*
At 5-lb applied force:
50 13 7 1.8 –100 24 11 2.8 0.02 150 32 14 3.5 0.02 200 38 22 5.5 0.04
At 10-lb applied force:
50 10 8 2.0 – 100 14 11 2.8 0.21 150 19 11 2.8 0.05 200 28 19 4.8 0.06
At 15-lb applied force:
50 6 5 1.3 – 100 13 7 1.8 0.01 150 17 8 2.0 0.01 200 25 11 2.8 0.01
NOTE: Data show the percentage force reduction achieved with 50,100, 150, and 200 mmHg pressure applied to the forearm cuff withapplied weights (force) of 5, 10, and 15 lb. *The p value for each series is derived from comparison with find-ings at 50 mmHg.
and standard deviation?

theory that the origin of the ECRB is broadened andtransported distal to the ECRB origin, as evidencedby the reduction of force in this model.
Electromyographic activity and muscle strengthusing the forearm support band have been tested insubjects with and without lateral epicondyle pathol-ogy. The armband has been shown to both increaseand decrease wrist extensor strength in several con-tradictory studies. Wadsworth et al.13 proposed thatthe effects of the armband in patients who havepathology may differ from those in patients withoutpathology. In those without pathology, the armbandmay decrease strength by mechanically limiting max-imal contraction. In those with pathology, it mayincrease strength by lessening pain and thus permit-ting a more forceful contraction.
Groppel and Nirschl12 performed a biomechanicalanalysis of banded and unbanded tennis players usingthree-dimensional cinematography and electromyo-graphic techniques in normal subjects. Banding result-ed in lower electromyographic activity of the extensorcarpi ulnaris and extensor carpi radialis during serveand backhand strokes than in the unbanded controls.Priest15 found that the backhand stroke produced lat-eral epicondylar symptoms twice as frequently as theserve in patients with tennis elbow, and Nirschl14
reported that the backhand initiates tennis elbow in90% of affected tennis players. These findings suggestthat tennis elbow is aggravated by both passive stretchat the ECRB origin (e.g., extremes of wrist flexion withserving) and active firing of the extensors (e.g., use ofthe backhand stroke).
Adding to the problem of contradictory informationabout the mechanism of forearm support bands, thereare several designs of these bands on the market.These designs range from a simple adjustable strap toa band with a small balloon (Aircast, New Jersey) thatconcentrates pressure over the extensor wad.
Snyder-Mackler and Epler6 studied the effects ofboth standard and Aircast bands on electromyo-graphic activity of the extensor digitorum communis(EDC) and ECRB proximal to the band, comparedwith control values in normal subjects. They foundthat, the Aircast band caused a significant reductionin electromyographic activity of the ECRB and EDC,compared with control values and findings for thestandard band. The standard band also caused areduction in electromyographic activity, but this wasnot statistically significant. Interestingly, the decreasein electromyographic activity due to the bands wasmore marked in the EDC than in the ECRB. Oncemore, whether reduced electromyographic activitycorrelates to clinical improvement remains to beseen.
Regarding the clinical effect of the forearm supportband, the literature again lacks definitive results.Froimson2 first introduced the concept of a formalforearm support band to clinical use. In his series of
40 patients, 23 of 28 patients treated with the forearmband plus steroid injection were relieved of pain, aswere 10 of 12 patients treated with the forearm bandalone. A shortcoming of this series is the absence of acomparison control group with findings that woulddefinitively support use of the band.
Along with the forearm support band, numerousother nonsurgical treatment modalities exist for lateralepicondylitis. Topical diclofenac has been shown tohave a short-term effect on elbow pain related to later-al epicondylitis, but its result and long-term effectslack consistency.16 Oral diclofenac and other non-steroidal anti-inflammatory drugs have been reportedto improve pain, but these carry the risk of side effectsranging from gastrointestinal upset and ulceration torenal damage, which may outweigh the benefitsderived from their use.7
Although our study suggests a mechanical benefit,the review of literature has shown that recommenda-tions regarding the timing and duration of applica-tion vary. Froimson2 directs patients to use the bandonly during painful activities and to remove it duringperiods of inactivity. In acute cases, the forearm bandmay be used in conjunction with local anesthetic andsteroid injections. Finally, Froimson recommendsusing the band during activity for at least 1 year afterpain relief is achieved, to avoid recurrence. Priest15
recommends that moderately symptomatic patientswear the band during any activity and that highlysymptomatic patients wear it at all times except atnight.
Other authors also recommend use of the forearmband in the acute phase of treatment, during thestrengthening exercise program, but they suggestthat patients be weaned from its use over the remain-der of the rehabilitative program.11 These authorsalso suggest limiting forearm band use to the early,less acute, or less painful cases in which splinting orcorticosteroid injection is not thought to be necessary.Others have suggested that counterforce bracing beimplemented when symptoms have resolved, such aswhen there is no pain with daily activity, no referredpain, and full range of motion.10 Counterforce brac-ing is felt to be a supplement to, and not a replace-ment for, muscular strengthening exercises.
Perhaps the most difficult measure to quantify isthe tension at which the forearm band is applied.Most authors do not address this issue sufficiently intheir discussions and studies and instead simplyreport applying the brace so that it feels “comfort-able.” For example, they describe the tension atwhich the forearm band has been applied in the fol-lowing ways: “. . . tension is adjusted to a comfortabledegree with the muscles relaxed so that maximumcontraction of the wrist and finger flexors and exten-sors is inhibited by the band . . .”2; “. . . secure it . . . sothat a subject felt comfortable when relaxed butnoticed tension when contracting his/her forearm
182 JOURNAL OF HAND THERAPY

muscles . . .”13; “. . . wrapped snugly about the bulki-est portion of the upper forearm. . .”15; and “. . . snug-ly without pinching the skin . . . .”6
Obviously, much discrepancy and little objectivedata exist regarding the optimal pressure of applica-tion.
The positioning of the forearm band is, similarly,not adequately addressed in the literature. Oneauthor recommends applying and adjusting the bandwith the forearm pronated,10 while most recommendapplication with the forearm in neutral position.Most agree that the band should be placed approxi-mately 2 cm distal to the lateral epicondyle.6,13
Potential side effects of use of the forearm bandinclude venous congestion and edema.2 Enzenauerand Nordstrom17 reported a case of transient anteriorinterosseous nerve syndrome following treatmentwith a forearm band. In this case, the patient hadapplied the band firmly and “overzealously.” After 1week of wearing the forearm band, the patient devel-oped deep forearm pain associated with weakness ofthe hand. Normal function returned 48 hours afterthe forearm band was discontinued.
The results of our study, if applied in the clinicalsetting, address several of the vague and ambiguouspoints mentioned previously. First, the forearm sup-port band in this model decreases the forces at theECRB origin, suggesting that the band does, at leastin part, create a second “origin” for the ECRB distalto the lateral epicondyle. Second, the band reduces alarger percentage of the force in lower-force activities(13%–38% reduction) than in higher-force activities(6%–25% reduction) (see Table 1). This suggests thata successful clinical effect may be more likely inlower-demand, repetitive activities but that use of theband has an effect, albeit diminishing, in higher-demand activities. This effect may be analogous tothe disease process itself: If the forces experienced atthe ECRB origin are “overloading” the area by 10% to20%, the support band may diminish the forcesenough to allow the tissues to recover.
Regarding the clinical use of the forearm supportband, patients do not consistently apply the band to auniform tension. In fact, since they are not taught toapply the band to a goal tension, and there is no regu-lator on the band itself, it is almost impossible to applythe band to a consistent pressure. In our series of ninepatients, the pressure ranged from 21 to 101 mmHg atrest and rose during gripping to 42 to 150 mmHg.
The largest excursion in pressure was observedwhen the band was applied at 40 to 50 mmHg, caus-ing a rise to approximately 100 to 140 mmHg (seeFigure 3). While this requires, and is the subject of, fur-ther investigation, it would suggest that an applicationpressure of 40 to 50 mmHg would offer the optimalmechanical benefit (Figure 4). This resting pressurewould be below diastolic blood pressure, minimizingedema. In our model, however, the rise in pressure
during activity would create a 24% to 32% force reduc-tion during low-demand activities.
In short, this model suggests a mechanical basis forthe forearm support band, since it decreases the forceat the ECRB origin dependent on pressure of appli-cation (increased effect with increased pressure) andload applied to the ECRB tendon distally (decreasedeffect with increased loads). While this study hasmany limitations inherent in cadaveric models (e.g.,no true clinical effect measured, a purely passivemodel, cadaveric vs. in vivo testing), the findingsappear logical and applicable. However, furtherstudy is required to determine the optimal period ofapplication, pressure of application, and position ofapplication to attain the desired effect. Study of clin-ical efficacy is also required.
CONCLUSIONS
■ The forearm support band appears to provide amechanical inhibition of force transference to theECRB origin during activities that load the ECRBtendon distally.
■ The force reduction caused by the forearm sup-port band is proportional to the pressure of appli-cation.
■ The force reduction caused by the forearm sup-port band in inversely proportional to the loadapplied to the ECRB tendon distally.
■ Patients with lateral epicondylitis who have beenusing the forearm support band apply the brace tohighly variable pressures (from 20 to 100 mmHg).
■ Further study is necessary to determine an idealpressure of application, period of application, andtrue effect on symptoms related to lateral epi-condylitis.
April–June 2002 183
FIGURE 4. Pressure difference from rest to grip. The dataobtained from the clinical trials show a peak pressure effect at 40to 50 mmHg resting pressure. In this range, the pressure risesmaximally during grip, independent of grip strength. This sug-gests an optimal pressure of application in the 40 to 50 mmHgrange. Circles connected by a solid line indicate pressure differ-ence; squares connected by a staggered line indicate grip strength.

Acknowledgments
The authors thank Linda McGrady and the staff of theBiomechanics Lab at the Medical College of Wisconsin fortheir assistance in obtaining and analyzing the raw data.
REFERENCES
1. Allander J. Prevalence incidence and remission rates of somecommon rheumatic diseases and syndromes. Scand JRheumatol. 1974;3:145–53.
2. Froimson AI. Treatment of tennis elbow with forearm supportband. J Bone Joint Surg. 1971;53(A):183–4.
3. Assendelft WJ, Hay EM, Adshead R, Bouter LM. Corti-costeroid injections for lateral epicondylitis: a systematicoverview. Br J Gen Pract. 1996;46:209–16.
4. Boyer MI, Hastings H. Lateral tennis elbow: “Is there any sci-ence out there?” J Shoulder Elbow Surg. 1999;8(5):481–91.
5. Jansen CW, Olson SL, Hasson SM. The effect of use of a wristorthosis during functional activities on surface electromyogra-phy of the wrist extensors in normal subjects. J Hand Ther.1997;10:283–9.
6. Snyder-Mackler L, Epler M. Effect of standard and Aircast ten-nis elbow bands on integrated electromyography of forearmextensor musculature proximal to the bands. Am J Sports Med.1989;17:278–81.
7. Labelle H, Guibert R, Joncas J, Newman N, Fallaha M, RivardCH. Lack of scientific evidence for the treatment of lateral epi-
condylitis of the elbow: an attempted meta-analysis. J BoneJoint Surg. 1992;74(B):646–51.
8. Wuori JL, Overend TJ, Kramer JF, MacDermid J. Strength andpain measures associated with lateral epicondylitis bracing.Arch Phys Med Rehabil. 1998;79:832–7.
9. Stonecipher DR, Catlin PA. The effect of a forearm strap on wristextensor strength. J Orthop Sports Phys Ther. 1984;6(3): 184–9.
10. Galloway M, DeMaio M, Mangine R. Rehabilitative techniquesin the treatment of medial and lateral epicondylitis. Ortho-pedics. 1992;15(9):1089–96.
11. Gellman H. Tennis elbow (lateral epicondylitis). Orthop ClinNorth Am. 1992;23:75–82.
12. Groppel JL, Nirschl RP. A mechanical and electromyographi-cal analysis of the effects of various joint counterforce braceson the tennis player. Am J Sports Med. 1986;14:195–200.
13. Wadsworth CT, Nielsen, DH, Burns LT, Krull JD, ThompsonCG. Effect of the counterforce armband on wrist extension andgrip strength and pain in subjects with tennis elbow. J OrthopSports Phys Ther. 1989;11:192–7.
14. Nirschl RP. Tennis elbow. Orthop Clin North Am. 1973;4:787–800.
15. Priest JD. Tennis elbow: the syndrome and a study of averageplayers. Minn Med. 1976;59:367–71.
16. Burham R, Gregg R, Healy P, Steadward R. The effectivenessof topical diclofenac for lateral epicondylitis. Clin J SportsMed. 1998;8(2):78–81.
17. Enzenauer RJ, Nordstrom DM. Anterior interosseous nervesyndrome associated with forearm band treatment of lateralepicondylitis. Orthopedics. 1991;14:788–90.
184 JOURNAL OF HAND THERAPY

Rheumatoid arthritis (RA) is the most commonchronic inflammatory disease of joints characterizedby remissions and exacerbation.1 After several yearsof persistent synovitis in chronic arthritis, jointdestruction, instability, and deformity ensue. Thehand function and activities of daily living of thesepatients with rheumatoid arthritis showed deteriora-tion in a 5-year follow-up study.2 The disease oftenbegins in the hand, and upper extremity function canbe seriously impaired with progression of the dis-ease. The incidence of deformities at the interpha-langeal joints and the wrist ranges from 63% to 85%.3
One of the most common hand deformities is flex-ion contracture of the proximal interphalangeal (PIP)joint. The PIP joint and its motion are among themost important factors in hand function.4 The PIPjoint is the epicenter of the hand and is responsiblefor 85% of total encompassment when an object isgrasped.4,5
As a result of chronic inflammation, shortening ofthe volar plate, with its proximal lateral check-reinextensors, and of the collateral ligaments may devel-op, causing flexion deformity at the PIP joint. Tendonadhesions at the palmar skin, flexor tendons, or
sheaths may be associated components of flexioncontracture. If the PIP joint cannot fully extend, thenextension in preparation for grasp is limited, andlarge objects cannot be gripped. Lack of PIP exten-sion can also hinder other functional activities.4
Provision of static resting hand splints has beenfound to be effective in the early stage of disease, torest the inflamed joint and provide pain relief,6–9 butvery few studies have reported the clinical value ofthese resting splints in the prevention or correction offinger deformities in patients with rheumatoid arthri-tis.10,11 Most occupational therapists are reluctant toprescribe corrective or dynamic splints for patientswith rheumatoid arthritis, for fear that the stretchingforce might create further damage to the joints andthus cause pain and discomfort.12,13 Fairleigh andHacking10 reported the clinical application of dynam-ic splints in patients who underwent arthroplasty.Palchik et al.11 also reported the application ofdynamic splints in the early management of bouton-niere deformity, but their sample size was too smallto generalize the results.
Previous studies reported that the uses of elasticsplints and traction have been proved to be effectivein preventing and correcting finger deformi-ties.4,5,14–16 Wu17 found that static inelastic correctivesplints for flexion contracture of the PIP joint mightbe more effective than dynamic or elastic splints withrubber band or coil-spring elements. Li18 conducted a
April–June 2002 185
Correspondence and reprint requests to: Cecilia W.P. Li-Tsang,PhD, Associate Professor, Department of Rehabilitation Sciences,The Hong Kong Polytechnic University, Hung Hom, Kln.,HongKong; e-mail: <[email protected]>.
Cecilia W. P. Li-Tsang, OT(C), MPhil, PhDAssociate Professor, Department of Rehabilitation SciencesThe Hong Kong Polytechnic UniversityHong Kong
Leung Kim Hung, MBBS, FRCSProfessor, Department of Orthopaedics and TraumatologyThe Chinese University of Hong KongHong Kong
Arthur F. T. Mak, MSc, PhDChair and Professor, Rehabilitation Engineering CentreThe Hong Kong Polytechnic University
ABSTRACT: This paper reports a matched-pair experimentalstudy to investigate the effect of corrective splinting on flexioncontracture of rheumatoid fingers. Twenty-four patients withrheumatoid arthritis and finger flexion contracture participated inthe study. After a 6-week baseline measurement of hand func-tion—including measurement of grip strength and range ofmotion and administration of the Jebsen Hand Function Test—thepatients were randomly placed into two groups. Patients in thefirst group were given dynamic (Capener) splints, and those in thesecond group were given static (belly gutter) splints. Hand func-tion was re-assessed 6 weeks after the splinting program. Resultsindicated significant improvement in both groups, not only in thecorrection of the finger flexion contracture (p < 0.0005) but also ingrip strength (p = 0.001) and hand function (p < 0.0005). Patientswith dynamic finger extension splints did not differ from thosewith static splints in extension gains, but they did have better flex-ion than patients with static splints. Both types of splints can berecommended for flexion contracture of rheumatoid fingers,depending on patients’ preferences and comfort. J HAND THER. 2002;15:185–191.
The Effect of Corrective Splinting on FlexionContracture of Rheumatoid Fingers

biomechanical analysis of finger splints and foundthat the dynamic (Capener) splint is more effectivethan the static (belly gutter) splint in correcting flex-ion contracture at the PIP joint. Most of these studieswere conducted on joint contracture caused by trau-matic injury, not by chronic disease.
Therapists have been concerned that the loadingforce of these corrective splints might cause pain andfurther damage to inflamed joints. However, if thecorrective force is monitored closely and maintainedwithin the pain threshold of each patient, would suchsplinting be equally effective for patients withrheumatoid arthritis?
This study examined the effects of the early appli-cation of corrective splinting on flexion contracture ofrheumatoid fingers and compare the effects of twodifferent types of corrective splints—a static splintand a dynamic splint—on the hand function ofpatients with rheumatoid arthritis. There were threehypotheses. The first hypothesis was that the handperformance of patients with rheumatoid arthritis, asmeasured by ROM, strength, and dexterity, wouldnot change over a baseline period of 6 weeks. Thesecond hypothesis was that treatment with a splint ofthe PIP joint would change hand performance over aperiod of 6 weeks. The third hypothesis was that thetype of splint used would affect the hand perform-ance after a 6-week period of splint use.
RESEARCH DESIGN
The study was designed to compare the effective-ness of two types of corrective splinting on flexioncontracture of rheumatoid fingers, using a matched-pairs control group design (Figure 1). Patients withsimilar functional levels, age, sex, and affected fin-gers were paired into the two groups for comparisonof the effect. This helped minimize the discrepancy inhand function assessments due to variation in sever-ity of the disease processes.
METHODS
Patients
A total of 30 patients (22 women and 2 men) wererecruited from three outpatient rheumatology clinicsand selected for the study. Twenty-four patients com-pleted the study in 12 weeks, but the remaining sixpatients could not continue the program because ofthe exacerbation of their disease. All the patients wereright-hand dominant. Patients were housewives(45.8%), clerical staff (25%), students (16.7%) and otherprofessionals (12.5%), who had demands of light tomoderate manual tasks during their daily routines.The average age was 37.08 years (SD, 16.34 years).
Inclusion criteria were that the patients werebetween 15 and 65 years of age and had diagnoses ofrheumatoid arthritis with finger flexion contractureless than 45°. Patients with fixed, permanent defor-mities or with articular damage on the PIP jointswere excluded from the study. Patients with PIPjoints with differences in passive range of motion lessthan 10° were also excluded from the study.
On the basis of their degree of impairment, 17patients were rated functional class II and 7 wererated functional class III.19 There were even distribu-tions of sex, hand dominance, affected hands, andaffected fingers in both groups (Table 1). The groupsshowed no significant differences in the degree offlexion contracture on affected fingers (p = 0.631),active flexion (p = 0.524), grip strengths (p > 0.05), andJebsen Hand Function Test (JHFT) results (p = 0.921)(Table 2). The initial mean degree of flexion contrac-ture was 34.2° (SD, 11.6°) among the 24 patients.
186 JOURNAL OF HAND THERAPY
TABLE 1. Distribution of Sex, Age, Year of Onset,Affected Hand and Affected Fingers of Two Groups
Characteristics Group 1 Group 2 Total(n=12) (n=12) (n=24)
Functional class:II 8 9 17 III 4 3 7
Mean year of onset (SD) 6.5 5.5 6.0 (2.5) (2.0) (2.0)
Mean age in years (SD) 34.25 37.17 35.71 (16.18) (17.02) (16.24)
Sex distribution: Female 11 11 22 Male 1 1 2
Affected hand: Right 10 9 19 Left 2 3 5
Affected finger: Index 5 5 10 Middle 6 6 12 Ring 1 1 2
FIGURE 1. Pretest–posttest control group study design. Key:X1 indicates patients with rheumatoid arthritis in group 1; Y1,patients with rheumatoid arthritis in group 2; X2, same group ofpatients in group 1 after 6 weeks; Y2, same group of patients ingroup 2 after 6 weeks; A, splint intervention–dynamic fingerextension splint (Capener splint); B, splint intervention–staticfinger extension splint (belly gutter splint); X3, group 1 patientsafter 6 weeks of splint intervention; Y3, group 2 patients after 6weeks of splint intervention.

Procedures
All patients were informed of the study and toldthat they could terminate the study at any time.Written consent was obtained from each patient priorto assessment. Two envelopes were prepared, onewith a “1” and one with a “2” labeled inside . Eachpatient was asked to draw one of the two envelopesand was then assigned to group 1 or group 2,depending on the number labeled inside the drawnenvelope. A qualified therapist who was blinded tothe study conducted the hand function assessmentsbefore and after treatment. The investigator providedthe intervention program for all patients in the study.
Measurements
The hand function assessment included assessmentof joint range of motion, assessment of grip strength,and administration of the Jebsen Hand Function Test(JHFT).
For each patient in both groups, the active range ofmotion of the affected finger joints, including themetacarpophalangeal (MCP), PIP, and distal interpha-langeal (DIP) joints, was measured using a fingergoniometer. According to Fess20 and Hunter et al.,21
the finger goniometer is a reliable and valid assess-ment tool in the measurement of joint range of motion.
A Jamar dynamometer and a pinch gauge wereused to assess power grip, pinch grip, chuck grip,and lateral pinch grip of the affected hand of eachpatient. Both instruments were found to be reliabletools for measurement of various hand grips.20,21
It has been suggested that the Jebsen HandFunction Test (JHFT) is a useful adjunct to evaluationof the hand in rheumatoid arthritis.22 Therefore, eachpatient was asked to complete the seven subtests ofthe JHFT, included writing, turning cards, picking upsmall objects, simulating feeding, stacking chesspieces, picking up light cans, and picking up heavycans. The JHFT has proved to have high reliability inmeasurement of hand function.22,23
The patients used regular medication and therapyservices, except splinting intervention, on both hands.Patients in group 1 each received a custom-madedynamic (Capener) splint with coil length, width, andcircumferences adjusted to suit the individual patient.The patient was instructed to apply the dynamic splintfour times a day. The duration of wear depended onthe tolerance of each patient, with a minimum of 6hours a day. Patients were also instructed to exercisethe joint during the period of wear.
Each patient in group 2 received a custom-madestatic finger extension (belly gutter) splint, which wasto be worn at rest a minimum of 6 hours per day.Patients were also reminded to exercise and mobilizethe PIP joint during the day when the splint was off.
The investigator explained the mechanisms of thesplints and the wearing procedures to all patients. If
they felt any pain or discomfort on the joint afterwearing the splint, they should report this to theinvestigator. The investigator also examined theaffected PIP joint regularly to adjust the loading forceand to ensure that the loading force would not causeany joint damage. Each patient was asked to use adiary to record the splint-wearing regimen and dura-tion. After the 6-week intervention period, therecorded splint-wearing time among the patients wasbetween 5.5 and 8 hours, with a mean value of 6.75hours (SD, 1.25 hours). There was no significant dif-ference between two groups in the length of wear(p > 0.01).
DATA ANALYSIS
Three analyses were performed. First, a paired-sample t-test was conducted to compare the initialassessment score and the pretest score, to indicate thestability of the hand performance of the patientswithout any intervention. Second, the paired samplet-test was used to analyze the pretest and post-testscores to determine whether there were significantdifferences before and after intervention, regardlessof the splint design. Third, an independent t-test wasused to determine whether there was a difference inthe hand function scores between patients ingroup A, who used the dynamic splint, and those ingroup B, who used the static splint.
RESULTS
Baseline Hand Function Performance of Patients
A baseline comparison was conducted at the initialassessment and at 6 weeks (Table 3), when all patientsreceived regular medication and other therapy servic-es. Dosage and types of medication depended on themedical conditions of individual patients but
April–June 2002 187
TABLE 2. Hand Function Performance of Group 1(Dynamic Splint) and Group 2 (Static Splint)
Mean (SD)Measure Group 1 Group 2
p
(n=12) (n=12)Value
PIP joint extension (°) 37.08 (11.57) 31.25 (11.31) 0.631
PIP joint flexion (°) 88.75 (7.42) 86.5 (9.03) 0.524
Power grip (kg) 10.08 (4.67) 12.38 (10.78) 0.096
Pinch grip (kg) 2.43 (1.47) 2.45 (1.75) 0.739
Lateral grip (kg) 3.10 ( 1.44) 3.30 (1.50) 0.613
Chuck grip (kg) 3.08 ( 1.84) 3.45 (2.09) 0.350
JHFT score (sec) 53.49 (12.79) 53.48 (13.21) 0.921
ABBREVIATION: JHFT indicates Jebsen Hand Function Test* p < 0.05.

remained the same throughout the 12-week period ofstudy. Weekly attendance at a physiotherapy unit formobilization and pain relief therapy was also requiredthroughout the 12-week period to ensure consistencyin intervention protocol before and after splint inter-vention. This served as a control period prior to theadministration of splinting.
No statistically significant differences existed in theactive range of motion of the affected PIP joints(p = 1.000 for PIP extension and p = 0.158 for PIP flex-ion) and the hand function test scores (p = 0.108)among the 24 patients. There were also no statistical-ly significant differences in power grip (p = 0.41),pinch grip (p = 0.334), chuck grip (p = 0.268), and lat-eral pinch (p = 0.083) during this baseline period,when no patients had any splint intervention.
The Effect of Corrective Splinting on Hand Function
All patients were assessed before and after the splintintervention program (Table 4). Results showed sig-nificant improvements for all patients in correction offlexion contracture at the PIP joints (p < 0.0005) afterthe splint intervention. The mean difference among allpatients was 18.75° of improvement. In terms of gripstrength, improvements in power grip (p = 0.001),
pinch grip (p = 0.002), chuck grip (p < 0.0005), and lat-eral pinch grip (p < 0.0005) after splint interventionwere noted. A significant difference was also notedbetween the hand function scores (as measured by theJHFT) for all patients before and after the splint inter-vention program (p < 0.0005).
As mentioned earlier, the significant improvementin correction of flexion contracture for all patientsshowed that corrective splinting is effective in cor-
188 JOURNAL OF HAND THERAPY
TABLE 3. Hand Performance Measures for the Two Groups Combined (n = 24) Six Weeks after Initial Assessment
Mean (SD)
Initial assessment Pretest t Value Df p Value
PIP joint extension 34.2 (11.6) 34.2 (11.6) 0.00 23 1.000
PIP joint flexion 87.6 (8.2) 89.0 (7.7) –1.46 23 0.158
Power grip 11.23(8.21) 11.05 (7.94) 0.84 23 0.410
Pinch grip 2.44(1.6) 2.56 (1.72) –0.94 23 0.334
Chuck grip 3.24(1.9) 3.16 (1.9) 0.74 23 0.268
Lateral grip 3.20(1.4) 3.35 (1.5) –1.82 23 0.083
JHFT score 53.49 (12.7) 52.27+10.8 1.71 23 0.108
ABBREVIATION: JHFT indicates Jebsen Hand Function Test*p < 0.05
TABLE 4. Hand Performance Measures for the Two Groups Combined (n = 24) Pre- and Post-intervention
Mean (SD)
Pretest Posttest t Value Df p Value
PIP joint extension 34.17 (11.6) 15.42 (10.52) 13.84 23 <0.0005*
PIP joint flexion 88.95 (7.66) 95.00 (8.72) –6.36 23 <0.0005*
Power grip 11.05 (7.94) 12.08 (8.50) –3.61 23 0.001*
Pinch grip 2.56 (1.72) 2.86 (1.61) –3.45 23 0.002*
Chuck grip 3.20 (1.93) 3.73 (2.05) –4.12 23 <0.0005*
Lateral grip 3.36 (1.50) 3.82 (1.62) –4.67 23 <0.0005*
JHFT score 52.10 (10.90) 47.32 (10.17) 5.21 23 <0.0005*
ABBREVIATION: JHFT indicates Jebsen Hand Function Test*p < 0.05
FIGURE 2. Mean hand function values before and after splintingintervention in group 1 (dynamic splint) and group 2 (static splint).Black columns show pre-splint values; hatched columns, post-splintvalues.

rection of PIP joint flexion contracture. There was nostatistically significant difference between the twogroups in active extension of the PIP joint (p > 0.05)(Figure 2), but a significant difference in active flex-ion was noted between patients in the dynamic splintprogram and those in the static splint program(p = 0.032) (Figure 3 and Table 5).
The null hypothesis, that static and dynamic splintspromoted the same strength, had to be accepted. Nosignificant difference was noted between the dynam-ic splinting group and the static splinting group inpower grip, pinch grip, chuck grip, or lateral pinchgrip (p > 0.05).
DISCUSSION
Most research studies have focused on the effectsof resting splints for patients with rheumatoid arthri-tis in relieving pain, resting the joints, and preventingdeformities.7,9,11–13,24 Other researchers have reportedsuccess in the use of corrective splinting in the man-agement of PIP joint flexion contracture.4,15–17
Nevertheless, very few researchers have studied theapplication of corrective splinting to overcome jointflexion contracture in patients with rheumatoidarthritis.10
This study examined the effects of corrective splint-ing in the management of PIP joint flexion contrac-ture using a pain-controlled model. Patients selectedfor this study were fully aware of the pain-controlledmechanisms and were asked to wear their splintswithin their limits of pain during the 6 weeks of inter-vention.
There was no significant difference between theinitial and 6-week assessments, showing that the reg-ular medication and therapy services did not havedirect effect on the correction of PIP flexion contrac-ture. This indicated that the patients’ conditions werequite stable and that any later changes could be dueto splint intervention. After the 6-week splint inter-vention, improvements in the correction of flexion
contracture at the affected PIP joint were observed(p < 0.001). The results were supported by those ofprevious studies by Wu17 and Li,18 showing that, inpatients with rheumatoid arthritis, static and dynam-ic corrective splinting regimens could reduce flexioncontracture of the PIP joint equally well.
The major consideration in application of the cor-rective splints was whether signs of active synovitiswere present. Of the 30 patients selected for thisstudy, 6 were found to have active synovitis duringthe 6-week control period. These patients were with-drawn from the study because of deterioration due tothe disease process, and they were asked to increasethe dosage of medication. The pain and diseaseaggravation had no direct correlation with the splintintervention program.
The remaining 24 patients did not report increasedpain during or after the splinting program. Therewere no signs of inflammation on the affected PIPjoints. The flexion contractures were caused mainlyby chronic edema and stiffness, which are commonamong patients with rheumatoid arthritis.
Findings from this study conflicted with those ofthe biomechanical analysis in Li’s study,18 whichshowed that the Capener splint could generate a bet-ter torque force for optimal correction of flexion con-tracture at the PIP joint by providing adjustment ofcore circumferences, strength, and length. In the bio-mechanical analysis, the force generated by thedynamic finger extension splint (the Capener splint)is proportional to the deflection angle of the joint.The bilateral coil at both sides of the PIP joints helpsprovide the continuous torque force to extend the fin-ger. The force can be adjusted (by modifying thedimensions of the coil) to provide the best stretchingforce tolerable by the patient. It is extremely impor-tant to monitor this force, especially for patients withrheumatoid arthritis.
April–June 2002 189
TABLE 5. Hand Function Performance of Group 1(Dynamic Splint) and Group 2 (Static Splint) after
Post-splint Intervention
Mean (SD)
Group 1 Group 2 p (n=12) (n=12) Value
PIP joint extension ((°) 13.33 (9.37) 17.5 (11.58) 0.343
PIP joint flexion (°) 98.75 (6.44) 91.25 (9.32) 0.032*
Power grip (kg) 11.25 (5.04) 12.91 (11.14) 0.644
Pinch grip (kg) 2.92 (1.80) 2.80 (1.47) 0.964
Lateral grip (kg) 3.73 (1.81) 3.92 (1.49) 0.779
Chuck grip (kg) 3.75 (2.13) 3.70 (2.08) 0.962
JHFT (sec.) 47.11 (10.20) 47.53 (10.59) 0.922
ABBREVIATION: JHFT indicates Jebsen Hand Function Test* p < 0.05.
FIGURE 3. Mean proximal interphalangeal joint flexion val-ues before and after splint intervention. Black columns showpre-splint values; hatched columns, post-splint values.

The other factor to consider is the duration of splintwear. It remained difficult for the investigator to doc-ument exactly the duration of splint wear for indi-vidual patients. However, in group 2, most patientspreferred to wear the static splint during night rest(i.e., around 8 hours of wear), but most patients ingroup 1 could not recall how long they wore thedynamic splint.
Group variance was greater among patients wear-ing the dynamic splint. This might contribute to thelack of significant differences between the twogroups in the correction of flexion contracture of thePIP joints, even though there was strong evidencefrom the biomechanical analysis that the dynamicsplint creates a better corrective force than the staticsplint does. The data suggest support for the biome-chanical model, because the clinical observationsshowed that the patients in group 1 regained morethan 20° active extension, whereas the patients ingroup 2 showed an improvement of only about 15°extension.
According to feedback from the patients, thedynamic splint was easy to apply and remove, whichinclined patients to put it on more regularly betweendaily activities. On the static splint, in contrast, thestrap of hook-and-look tape across the joint had to beadjusted every time the splint was put on, andpatients reported some difficulties in adjusting it tothe right tension. The generated forces thus variedwith each application of the static splint, dependingon the tension of the strap.
Although there was no difference in extension cor-rection between the two splints, a significant differ-ence existed in the flexion resulting from the splint-ing. It was interesting to find out that improvementin active flexion of the PIP joint was significantlygreater in group 1 than in group 2. This may bebecause of soft tissue contracture at the joint causingPIP joint extension contracture, with active flexionlimited as a result.
Extension contracture may be due to adhesion ofthe central extensor tendon, articular surface dam-age, or damage at the volar plate in particular.11,16
Hunter et al.21 also emphasize that active mobiliza-tion of the joint is useful to correct the contracture.
In this study, patients in group 1 showed betterimprovement than those in group 2. This may beexplained by the fact that the Capener splint encour-aged both active flexion and extension during thesplint program, whereas the static belly gutter splintcould not perform both functions.
Both groups of patients showed a significantimprovement in grip strength after the splint inter-vention program. It is possible that the soft tissuecontracture is due to shortening of collateral liga-ments or other factors, as described previously.4,25
Once the contracture has developed, the finger has afaulty position of grip. The flexor and extensor ten-
don excursions are changed, and the mechanicaladvantage is decreased. Therefore, the grip strengthsare affected.13 Once the soft tissue contracture hasbeen dealt with, the joint is in good alignment andthe tendon excursion is working at its most mechan-ically advantageous position, so the grip strength isstronger.
Patients in both groups also reported improvementin daily functional hand tasks, although the actualimprovement in functional daily activities was notdocumented.
Functionally, the PIP joint is responsible for 85% oftotal encompassment in the grasping of an object. If aPIP joint is limited in active movement, then activi-ties involving handling and maintaining grip onmedium to small objects becomes difficult. Results ofthe JHFT clearly showed that impairment of even asingle joint would affect hand function in a patientwith rheumatoid arthritis.
Therapists have to monitor the resistive correctiveforce very carefully when treating patients withrheumatoid arthritis.15–18 Both objective measure-ments, with regard to defining the coil strengths, andsubjective impressions of patients should be takeninto consideration. The position of application of cor-rective force, the torque generated at the PIP jointcausing joint compression, the contact pressure, thecosmesis, and the material properties of the splint arethe key factors to consider in the management of flex-ion contracture in patients with rheumatoid arthritis.We cannot substantiate any negative effects of theapplication of the dynamic Capener splint to increasemotion in our patients with rheumatoid arthritis.
CONCLUSION
Twenty-four patients with rheumatoid arthritiswere investigated to determine the effect of correc-tive splinting on flexion contracture of the rheuma-toid finger. Two types of corrective splints, one static(belly gutter splint) and one dynamic (Capenersplint), were selected for comparison of the effect onhand function. A matched-pair controlled groupdesign was adopted for the study, and after a base-line period of 6 weeks, patients were divided intotwo groups, which each used a different splint pro-gram.
After 6 weeks of splint use, a post-splint assess-ment was performed. All patients showed significantimprovement in their hand function after the splint-ing program, compared with function assessed atbaseline. Thus, a splinting program is effective in cor-recting flexion contracture of the joint and improvinggrip strength and hand function.
There was no significant difference in the percent-age improvement in grip strength between the staticsplint group and the dynamic splint group.Improvement in PIP flexion was significantly greater
190 JOURNAL OF HAND THERAPY

with the dynamic splint than with the static splint,but no differences were found between the other out-come measures.
This is a clinical study to investigate the effective-ness of corrective splinting on flexion contracture inthe rheumatoid hand. Information gained from thisstudy has helped us develop further research into thebiomechanical and clinical aspects of splinting inter-vention for patients with rheumatoid arthritis.Dynamic splints are effective in the correction of softtissue contracture of the PIP joint in patients withrheumatoid arthritis.
This study does not confirm the hypothesized neg-ative effects of dynamic splinting. The dynamic splintis reported to be better in the correction of flexion con-tracture of the PIP joint, although this finding is notstatistically proved. However, biomechanical analysisshowed that dynamic splinting is more effective thanstatic splinting in correcting flexion contracture of thePIP joint.18 Moreover, active flexion showed signifi-cant improvement with the dynamic finger extensionsplint, compared with the static splint. This indicatedthat therapy should focus not only on regaining lostfinger extension but also on increasing joint mobilityin both flexion and extension.
Although no significant difference was shownbetween the dynamic splint and the static splint inthe regaining of active extension of the PIP joint, thedynamic splint was not associated with a negative oradverse effect noted in other reports.11,24 Patients didnot complain of pain, fatigue, or over-stretching afterwearing the dynamic splint.
The clinical findings in this study did not confirmdeductions made from the biomechanical findings.18
There may be factors that researchers neglected dur-ing the clinical study, such as the total duration ofwearing time, which was not monitored properly inthis study. The methods of splint fabrication need tobe taken into special consideration as well. Specialcare should also be taken not to overstretch the deli-cate tissues around the joints. In addition, the elastic-ity of the coils should be checked frequently, since itis important to control the amount of corrective forceon the joint generated by the coil spring.
Further studies should examine the effect of splint-ing and the generation of corrective force in greaterdepth. Biomechanical analyses of different designsshould also be conducted.
Acknowledgments
The author thanks Professor P. C. Leung, Dr. W. S. Wong,Mr. Simon Wong, and Mr. Hercy Li for their great supportin completing the project. She also thanks the occupationaltherapy students, Mr. Edward Chan, Ms. Meaki Chan, Ms.Sanny Cheng, and Ms. Rosanna Kay, for their help in col-lecting data for the project.
REFERENCES
1. Melvin JL. Rheumatic Diseases in the Adult and Child:Occupational Therapy and Rehabilitation. 3rd ed.Philadelphia, Pa.: Davis, 1989.
2. Dellhag B, Bjelle A. A five-year follow-up of hand function andactivities of daily living in rheumatoid arthritis patients.Arthritis Care Res. 1999;12(1):33–41.
3. Dieppe PA, Dopherty M, MacFarlane DG, Maddison PJ.Rheumatological Medicine. Edinburgh, UK: ChurchillLivingstone, 1985.
4. Prosser R. Splinting in the management of proximal interpha-langeal joint flexion contracture. J Hand Ther. 1996;9:378–86.
5. Curtis RM. Management of the stiff hand. In: Hunter JM,Schnedier LH, Mackin EJ, Callahan AD (eds). Rehabilitation ofthe Hand. 3rd ed. St. Louis, Mo.: Mosby, 1990:321–7.
6. Estes JP, Bochenek C, Fasler P. Osteoarthritis of the fingers. JHand Ther. 2000;13(2):108–23.
7. Feinberg JR, Brandt KD. Use of resting splints by patients withrheumatoid arthritis. Am J Occup Ther. 1981;35:173–8.
8. Feinberg JR, Trombly CA. Arthritis. In: Trombly CA (ed).Occupational Therapy for Physical Dysfunction. 4th ed.Baltimore, Md.: Williams & Wilkins, 1994:815–30.
9. Janssen M, Phiferons, Dijkmans BAC. The prevention of handdeformities with resting splints in rheumatoid arthritispatients: a randomized single blind one-year follow-up study.Arthritis Rheumatol. 1990;33:123–6.
10. Fairleigh A, Hacking S. Post-operative metacarpophalangealarthroplasty dynamic splint for patients with rheumatoidarthritis. Can J Occup Ther. 1988;55(3):141–6.
11. Palchik NS, Mitchell DM, Gilbert NL, Schulz AJ, Dedrick RF,Palella TD. Nonsurgical management of the boutonnieredeformity. Arthritis Care Res. 1990;3(4):227–32.
12. Hanten DW. The splinting controversy in rheumatoid arthritis.Occupational Therapy in Practice. Special Interests SectionNewsletter. 1982;5(4):118–22.
13. Hittle JM, Pedretti LW, Kasch MC. Rheumatoid arthritis. In:Pedretti LW (ed). Practice Skills for Physical Dysfunction. 4thed. St. Louis, Mo.: Mosby, 1996:639–60.
14. Brand P, Hollister A. Clinical Mechanics of the Hand. 2nd ed.St. Louis, Mo.: Mosby, 1995.
15. Colditz JC. Spring wire splinting of the proximal interpha-langeal joint. In: Hunter JM, Schneider LH, Mackin EJ,Callahan AD (eds). Rehabilitation of the Hand. 2nd ed. St.Louis, Mo.: Mosby, 1984:862–74.
16. Fess EE. Force magnitude of commercial spring-coil andspring-wire splints designed to extend the proximal interpha-langeal joint. J Hand Ther. 1988;1:86–90.
17. Wu SH. A belly gutter splint for proximal interphalangeal jointflexion contracture. Am J Occup Ther. 1990;45:839–43.
18. Li C. Force analysis of the belly gutter and Capener splint. JHand Ther. 1999;12(4):337–43.
19. Steinbrocker O, Traeger CG, Batterman RC. Therapeutic crite-ria in rheumatoid arthritis. JAMA. 1949:140-659.
20. Fess EE, Philips CA. Hand Splinting: Principles and Methods.2nd ed. St. Louis, Mo.: Mosby, 1987.
21. Hunter JM, Mackin EJ, Callahan, AD. Rehabilitation of theHand. 4th ed. St. Louis, Mo.: Mosby, 1995.
22. Sharma S, Schumacher R Jr, McLellan AT. Evaluation of theJebsen Hand Function Test for use in patients with rheumatoidarthritis. Arthritis Care Res. 1994;7(1):16–9.
23. Jebsen R, Taylor N, Trieschmann R, Trotter M, Howard L. Anobjective and standardized test of hand function. Arch PhysMed Rehabil. 1969;50:311–9.
24. Rennie HJ. Evaluation of the effectiveness of a metacarpopha-langeal ulnar deviation orthosis. J Hand Ther. 1996;9:371–7.
25. Wilson R. Rheumatoid arthritis of the hand. Orthop Clin NorthAm. 1986;17:313–43.
April–June 2002 191

192 JOURNAL OF HAND THERAPY
Splint making involves the application of sciencecombined with the art of healing and the art of creat-ing objects that can be appreciated for their utilityand beauty by patients, prescribing physicians, andtherapists alike. “Minimalistic art” describes thoseworks of art, like certain paintings or buildings,whose full meaning is expressed in the least possiblestructure. The less structure, the more clearly anintended effect can prevail.
The concept of minimalistic design is also impor-tant in the creation of tools used in daily living, suchas corkscrews, and tools used in patient treatment,such as splints. In a splint as in a work of art, it isoften true that the less structure there is, the greaterthe effectiveness of the splint and the patient’s appre-ciation of it.
Minimalistic splint design is an approach that antici-pates and answers many questions that arise in splintmaking prior to fabrication of a splint, in order toachieve optimal effectiveness of the splint with theleast amount of structure. It takes into considerationthe many different aspects of making splints in themost structurally efficient way, including technicaland financial possibilities and constraints. Instead ofcorrecting design shortcomings on the go, during con-struction, the therapist uses the minimalistic-designsplinting algorithm proactively to revise the originaldesign and create a new prototype. A minimalistic-design splint is rarely the fruit of a first attempt.
Published reports rarely address the issue ofwhether a proposed splint design achieves its goals
with the least possible structure. Too often, improve-ments simply add more structures. Who does notremember a disastrous splinting experience, when asplint did not fit the patient’s hand and an endlessseries of small and ineffective alterations began, whichultimately did little to improve the product?
The purpose of this paper is to present, in a per-sonal style, a rationale for minimalistic splint design.The basic principle of minimalistic design is illustrat-ed by the objects shown in Figure 1, but it is appliedhere specifically to the making of effective splints.
BACKGROUND
Until the end of the 1960s, it was common knowl-edge that splint makers working with patients withspasticity generally wished that the patients wouldeither be under strong relaxation medication or betotally insensitive to pain. The splints they madewere rarely masterpieces, although it was not yetclear what masterpieces were supposed to look like.Often, the shape of a splint did not match the handwell, let alone achieve its therapeutic goal.
Around the same time, the first hand splintingbrochures and manuals addressed to occupationaltherapists were published.1 Promoting the use of thenewly invented low-temperature thermoplastics,which could be molded directly to the patient, theyprovided various patterns, described working tech-niques, and included pictures of the finished products.
My first personal attempts at splint making, datingfrom this period, were not very exciting. It was notthat the end results were failing, but I could read frommany patients’ faces a somewhat doubtful apprecia-tion. What was wrong? On self-evaluation, I realizedthat I was clueless about splint design and construc-
Paul Van Lede, OT, MSRucaplein, AntwerpBelgium
ABSTRACT: Theoretic clinical reasoning is becoming increasing-ly important in splint construction. The purpose of this paper is topresent an algorithm of decision steps that will help therapistsconsider all aspects of splint making proactively, so that they cantake the necessary steps to be successful. A decision flowchart ispresented and discussed in detail. An extra dimension of splintdesign is emphasized—namely, frugality in structure, technique,and cost. The paper concludes that the use of a comprehensivedecision algorithm provides the basis for successful working tech-nique and that the ability to create minimal-design splints is morea state of mind than a technical skill. J HAND THER. 2002;15:192–201.
Minimalistic Splint Design:A Rationale Told in a Personal Style
The author has a financial interest in one or more products men-tioned in this article.Correspondence and reprint requests to Paul Van Lede, OT, MS,Rucaplein, 556 B2610 Antwerp, Belgium; e-mail: <[email protected]>.

tion and that none of the existing handouts addressedthese issues.
From orthotic study books (addressed to ortho-tists), I learned that splint making necessarily beginswith physics (read “mechanics”) and must be fol-lowed by a thorough study of materials—in otherwords, the one thing that I hated most as a studentand the other that no manufacturer seemed eager topublish.
What was it, then, that motivated me to makesplints? First, as an occupational therapist, I was in aposition to learn my patients’ functional splintingneeds as no one else could. Second, I could appreci-ate what kind of splint was likely to meet theseneeds. And third, I was backed and encouraged by aprescribing physician who discovered a new andvery interesting therapy modality.
So, I thought, no problem: All that’s needed is toorder some more of these expensive thermoplastics,heat up some water in a small frying pan, get adecent pair of scissors, grab some more stuff from theOT department, and get going, training on a trainee’shand. But it soon became apparent that not all splintpatterns found in the literature were the products ofgenius design minds. Some splints could be fabricat-ed much more easily and were more attractive thanothers. But something was missing. Was it just that I found copying boring? Or could these designs bedone better with more creativity?
After a couple of months (or years?), the questionsno longer troubled me. I had learned in practice whatthe splinting manual never suggested—namely, thatsplinting design, fabrication, and management are arational process that can (and must) be clearly andproactively structured; that by following an algorith-mic sequence we can achieve both simplicity ofdesign and optimal effectiveness. I had learned that,if we use the algorithm, our splints are more likely tobe fully effective, cosmetically acceptable, and wornby our patients without reservations.
THE SPLINTING ALGORITHM
What Is an Algorithm?
An algorithm is a list of decisions that are made ina predetermined order to find an answer to a ques-tion.2 The splinting algorithm (Figure 2), if followedwith care, can guarantee good splint function andenable the splint maker to avoid bungling. Use of thealgorithm is helpful for those who make splints onlyoccasionally and for advanced splint makers whoface unusual splinting challenges.
Improvisation is not good enough in splinting, andpatients do not accept poor standards. Splints, unlikeplaster casts, can be removed, and a dissatisfied patientwill discard a bad splint and quit the therapy. For thisreason, therapists are obligated to design splints that atleast look and feel attractive enough to be worn.
The splinting algorithm is also designed to definethe technical and financial feasibility of a splint. Whenthe algorithm is used, design starts from scratch, notwith reference to a “recipe” book. The algorithm takesthe form of a flowchart that outlines sequential prob-lem-solving steps to create a perfectly fitting splintthat fulfills the therapeutic requirements.
April–June 2002 193
FIGURE 1. Minimal-design table, consisting of three prefabri-cated parts—the base, the table top, and the foot, to be assembledby clicking the components in place. The design is efficient, neat,easy, inexpensive, and without any excess.
FIGURE 2. Bird’s-eye overview of the algorithmic sequences.Details appear in Figures 3, 4, and 15.

In a clinical situation, the algorithm begins with aprescription that clearly and fully specifies the thera-peutic aims and goals of the desired splint. Usingthese data, the splint maker compiles the theoreticmechanical inputs that are necessary to draft a proto-type. The prototype is further refined according totechnical considerations based on the patient’s per-sonality, the splint maker’s technical expertise, andthe availability of materials.
The Splint Prescription
Besides the diagnosis, or identification of thepathology, the prescription should mention clearlyand in detail the anatomic boundaries and therapeu-tic goals of the splint (Figure 3).
Therapists often complain that splint prescriptionslack the information they require. It is then the thera-pist’s responsibility to fill in the first part of the flow-chart using the following guidelines.
This first part of the algorithm is based on the orig-inal ASHT splint classification system, issued in 1992and designed to be used as aid to the prescription.2
Anatomic Boundaries
The anatomic boundaries are determined by thesegments that need to be splinted. A segment mayconsist of either two articulated bones (basically, ajoint) or just a bone—hence the need to consider artic-ulation splints vs. non-articulation splints.
It is commonly assumed that splints should em-brace the whole segment without covering adjacentsegments that are not specified in the prescription,unless the coverage of the adjacent segments is nec-essary to improve stability of the splint.
The primary focus is the segment that is the target ofthe splint’s action, usually where the pathologic tis-sues are located or at least where the pathologic actionis concentrated—e.g., an inflamed metacarpophalan-geal (MCP) joint that needs to be immobilized by a
splint reaching from the proximal extremity of themetacarpal to the distal extremity of the first phalanx,or a muscle contracture of the flexor digitorum super-ficialis that must be treated by mobilization of thewrist, the MCP joint, and the interphalangeal (IP) joint.
The secondary focus is not the target tissue of thesplint’s action but is, rather, a segment that facilitatesor hinders the completion or achievement of the pri-mary focus. There may be more than one secondaryfocus. The secondary focus is not directly involved inthe pathology. For example, MCP joint flexionremoves a barrier against PIP joint extension byrelaxing the long flexor muscles; the MCP joint isthus a secondary focus. From biomechanics, we learnfurther that dorsal splints are allowed to reach andeven partially cover adjacent joints to increase thelever arms, whereas volar splints have to leave clearthe bulk of soft tissues that could impede jointmotion.3
Therapeutic Goals
There is a limitation to what can be achieved by theapplication of splints, since splints are only simplemechanical tools. Splints can be used to mobilize,immobilize, restrict mobilization, compress, or shielda target tissue. Each goal suggests a particular splintdesign.
Immobilization means that no mobility is allowed andusually concerns all planes of motion.2 The position ofthe hand in which immobilization is carried out is dic-tated by the prescription. A painful wrist, for example,is immobilized in a neutral, relaxed position.
Mobilization is when a joint is brought into a newposition and possibly held in this position, as when adrop hand is positioned in a functional position. Themobilization modality is static when the positioningtakes place with the donning of the splint. It impliesthat the splint can be made of a single piece of materi-al. The mobilization is dynamic when back and for-ward motions are allowed, which require the deviceto contain two movable parts.
With simple dynamic splints, the motion in onedirection is achieved actively by the patient, whereasthe return is accomplished passively by the splint. Asa result, the splint possesses a source of energy—hence the term “dynamic.”
Mobilization can further be described as position-ing, when no changes in position are expected overtime, or correcting, when gradual motion improve-ment is expected. The rigidity of the splint materialand, even more, of the splint design determines thesturdiness of the splint.
Mobilization stops can be placed either across themotion path or over a motion plane. Range of motionrestriction is when, for example, a blocking hinge isused. Such splints should be called mobile instead ofdynamic, since there is no source of energy.
194 JOURNAL OF HAND THERAPY
FIGURE 3. First part of the flowchart: the splint prescription.At least one item from each level must be found in the medicalprescription.

Plane restriction is when bilateral hinges are used toguide the joint in a determined path of motion, such asin an ulnar drift splint designed to allow only flexionand extension of the MCP joints. To minimize thesplint design, a single hinge is used. The single hingemandates a large contact surface to avoid torsion.
Compression (of soft tissue) has several therapeuticindications and is used, for example, for immobiliza-tion of long bone fractures (functional fracture brac-ing), deep-wound healing (burns), and neurologicinhibition (cerebral palsy). Shielding from externalforces and thermal isolation are other possible thera-peutic actions, but since there is no force application,these devices can no longer be termed (therapeutic)tools. Shin pads for football players and breast shieldsfor slalom skiers are examples of such devices.
To complete the prescription, the direction of mobi-lization (e.g., flexion vs. extension, abduction vs.adduction), the intensity of the action (e.g., magnitudeof torque, pressure, and traction), and the wearing reg-imen need to be described. The intensity of action andthe wearing regimen do not influence the splint designand so will appear at the end of the algorithm, whenthe wearing protocol is worked out by the therapist. Inmy opinion, it is also the responsibility of the splintmaker, rather than the prescribing physician, to workthrough the next steps of the algorithm, including thefinal design of the splint and the choice of materials.
Mechanical Considerations
We now consider the mechanical issues, which aredictated by physical laws (Figure 4). Only two toolscan be considered—levers and coaptation circuits.Any splint design will adhere closely to the mechan-ical rules that govern their operation—no more, noless. Ignoring or neglecting these rules will inevitablyresult in malfunction or non-function of the splint.
Lever-based Splints
Levers are defined as rigid bars that pivot on a fixedpoint and are used to transmit forces called power andload. Splints are used as levers either to lift up loads orto increase a movement path (muscle weakness).
Ideally, the splint pivot is located at the level of thejoint axis, and the power arm is anchored around theproximal anatomic segment. The distal anatomic seg-ment is the load to be mobilized.
In designing a splint, the therapist does not need tobe able to discern the various lever categories somuch as identify the various areas where the splintwill be in contact with the anatomic segments. Thisstep is crucial in any splint design; it is also very sim-ple. To identify these areas, it suffices to sketch thepathologic starting position and indicate the areas ofcontact according to the desired mobilization(Figure 5, top). A common mistake in many splintsmay originate in a missing point of support to com-plete the lever4,5 (Figure 5, bottom).
Next, it must be decided how the three points ofcontact (or multiple of three) are to be connected toeach other—on the bottom (Figure 6, left), on the top(Figure 6, middle), or on the sides (Figure 6, right).
Minimalistic design avoids the covering of areaswhere no contact is needed—hence, the idea to createwindows for aeration and lighter construction. Agood example of a minimalistic-design three-pointsplint is the swan neck splint made by The SilverRing Company (Charlottesville, Virginia).
The decision for a volar-based rather than dorsal-based splint is usually not intentional but dictated byhabits, precut patterns, or the need for accessories(such as outriggers) on dynamic splints. Mechanicalissues should, however, dictate this choice. Volar-based splints push the joint; dorsal-based splints pullit in extension. Since pulling, pushing, and shiftinghave specific effects on the skin and the underlyingtissues, the mechanics are not equally favorable.
Volar splints have a bed-like construction that isvery comfortable for resting. Consequently, resting
April–June 2002 195
FIGURE 5. Top, The drawing of a pathologic starting position,it is easy to determine the areas of pressure that are needed forextension of a whole finger. Bottom, Possible consequences of amissing point of support.
FIGURE 4. The second part of the flowchart: mechanical con-siderations. Working from top to bottom, at least one item fromeach level must be selected according to results of the structuralanalysis.

splints should always be volar (Figure 7). Doesn’tthat make sense? Yet volar splints are not so efficientfor extending resisting joints (stiff joints or hyperton-ic muscles), because of the relatively high friction thatoccurs between the skin and the splint surface at bothsplint extremities. The more pressure is applied andsoft padding is used, the higher the friction and theless efficient the splint action becomes. For thosecases, then, a volar design should not be used. Couldthe friction be reduced if padding were avoided andlubricant used instead? Not sufficiently!
With dorsal splints, straps on the extremity pull(rather than push) the joints into extension (Figure 8).This action is much more efficient, and no frictionbuilds up, only pressure. Pressure can easily be dis-persed over large surfaces, softened by padding. Canpadding be used in dorsal splints? Absolutely, aslong as it is not used to disguise a faulty design.
With dorsal connections, splints correcting multiplejoints do not have to contour each joint precisely, sincethe straps, not the splint material, take up the forces.
Lateral-connection splints can be designed with orwithout fixation straps. With a strap, the splint resem-bles a crowbar, making tilting very easy (Figure 9, left)That is why lateral-connection splints are indicated tomobilize “big” joints, such as the wrist and the elbow.They are also very practical for mobilizing joints out ofawkward positions, as with longstanding hypertonic-ity that results in strong muscle contractures.
A lateral-connection splint without straps can beconsidered a true minimalistic design (Figure 9, right).However, since such a splint has no opening strap, thepatient should have sufficient joint range of motion tosneak into the splint, which is not always easy or fea-
sible. Examples are the swan neck splint mentionedearlier and spiral wrist splints.
A nice feature of lateral-connection splints is thathinges can be incorporated that perfectly match thejoint axis. Try to do this with either a volar or a dor-sal splint and you will see both a huge motion dis-crepancy and plenty of excess material to be trimmedof the volar splint to allow full range of motion.
The design of circumferential splints results from athree-point analysis when joint motion is allowed innone of the motion planes. The analysis reveals threegirdles around the points of contact. One girdle sur-rounds the pivot, and two girdles surround bothextremities. Connecting the girdles results in a cir-cumferential design (Figure 10). These splints areknown to be extremely stable and very comfortablesince the stability is neither due to the material stiff-ness nor the thickness.
Circuit-based Splints
A coaptation system2 is a closed circuit, usually ofsoft elastic material, that holds one or more joints in aflexed position (Figure 11, left). Such splints are partic-ularly efficient for increasing joint flexion, as in stifffingers. The standard example is the flexion glove.
The smaller the circuit, the more flexion is obtained.The art of the therapist is demonstrated in designingthe circuit so that the target joint of a digit, the primaryfocus, benefits the most. Because the proximal seg-ments of digits are longer than the distal segments, theproximal segments in a circuit are more compressedand flexed. For this reason, the therapeutic action isdirected in a proximal-to-distal direction. Once the
196 JOURNAL OF HAND THERAPY
FIGURE 6. Biomechanical possibilities to connect points of support on the bottom (left), on the top (middle), or on the sides (right).
FIGURE 7 (left). A volar splint is comfortable while resting.FIGURE 8 (right). A dorsal splint is efficient in the application of traction.

proximal joint has reached its end position, it isremoved from the circuit to allow tightening of the cir-cuit. The joint distal to it now becomes the most prox-imal joint to benefit from the splint action.
To avoid excessive bulk and favor the minimalisticdesign of a circuit, a shortcut that follows the radius
of the theoretic circle is allowed (Figure 11, right).With a stiff extended digit, however, a shortcut coap-tation design will need an outrigger on the volaraspect, which makes the splint voluminous. Onlyafter the digit is semi-flexed can the outrigger beremoved and the splint become less cumbersome.
April–June 2002 197
FIGURE 10. Circumferential design offers goodtotal immobilization.
FIGURE 9. Left, A lateral-connection splint with strap provides easy leverage. Right, These two splints show that a lateral-connectionsplint without a strap is the minimalistic design.
FIGURE 11. Coaptation circuit(far left). A shortcut, using onlypart of the coaptation circuit, isallowed along the radius only(left).

Because postoperative splints sometimes have to becombined with other medical devices, such asBaxters, external fixation devices, and plaster of Pariscasts, they may end up bulky and not minimalistical-ly designed at all. Functional splints, on the contrary,have to comply with work situations and be discrete,so minimalistic designs are paramount.
Mode of Force Application
All medical requirements except the treatmentmodality have now been translated into mechanicalsplint requirements. The treatment modality can beeither static or dynamic.
Dynamics, in the sense of splint making, is thestudy of splint motion in harmony with joint motion.It addresses the motion path of the participatingbony elements (osteokinematics) and motion withinthe joint (arthrokinematics) as well as the appliedenergy (kinetics).
The natural biomechanics of the hand are complexand hard to mimic, especially when we realize thatall sound joint motions have rotational motion paths.Consequently, dynamic splints should movethroughout the entire range of motion. Splints thathave rigid outriggers and rubber bands that movelinearly cannot do this. Here is where true artistrywill shine! The fabrication of dynamic splints withhinges, let alone the inclusion of a source of energy toobtain a minimalistic design, is not a beginner’s cupof tea.
Why can we not keep it simple and remain contentwith outriggers and rubber bands?
Let’s consider the patient, again, and the situationin which the splint is to be used. In the postoperativetreatment phase, patients usually do not argue aboutthe splint bulk, given that other horrors are probablyhounding their subconscious at this time. Duringearly postoperative care, the accuracy of the splintdesign and the applied force are of much moreimportance than aesthetics and discretion. The splint
maker is allowed to opt for an easily adjustable andusable dynamic system even at the expense of a sleekand slim design. Full range of motion is not an issueyet, and patient’s motions are slow, without a func-tional goal. Thus, splints with outriggers and rubberbands, although not minimalistically designed, areacceptable.
This does not mean that any profile is tolerable. Thepatient is entitled to sleep at night and must be able tomove comfortably through doorways. (Given the con-straints imposed by some exaggerated, high-profilesplints, this common-sense view is not as obvious as itseems.) The minimalistic profile of a dynamic splintwith outrigger is dictated by the angle of pull of therubber band (short vs. long outrigger) (Figure 12) andby the length of the rubber band (determined by theelasticity modulus) (Figure 13).4 The profile does notshow the splint maker’s skill as some like to believe.
What I call a vertical profile (usually termed a highprofile, although it is not necessarily high) is actually apreferred minimalistic design option. It is efficient andeasy to make, although it is sometimes less appealingcosmetically because of its bulk. Horizontal-profilesplints (sometimes genuinely low profile, sometimesnot) are less cumbersome to wear but more difficult tomake, because pulleys need to be added to redirect therubber band from horizontal to vertical. They are alsolikely to be more expensive.
When simple eyelets replace rotational pulleys (tosave money) and fishing line replaces part of the rub-ber band (to reduce drag), the elastic modulus increas-es dramatically, making it necessary to lengthen therubber band—and lose the original minimalisticdesign.
In addition, the therapist needs to consider carefullythe amount of force provided by the elastic modulus of
198 JOURNAL OF HAND THERAPY
FIGURE 12. The angle of pull determines the length of the out-rigger (and vice versa).
FIGURE 13. With vertical profile splints, the length of the rub-ber band determines the height of the outrigger.

the dynamic splint. Elastic modulus is like the horse-power in a car. If it is too weak, driving uphill can betedious and time-consuming, but if it is too strong, thecar will swerve out of control on the first curve!
In the rehabilitation phase, the accuracy of the trac-tion force is important, but even more important, andultimately decisive, is the user-friendliness of thesplint. This benefits the patient directly, but it alsoimproves the likelihood that the splint will be includ-ed in the total package of care, in the event that sever-al therapists, or clinicians from more than one disci-pline, are involved in the care of the patient. An exam-ple of this is a splint fabricated for a burn patient, inwhich the splint maker—as well as nursing and med-ical personnel—is active in the care of the patient.
In functional situations, the patient is king. Patientsdecide for themselves whether splints are worn ornot, when they are worn, for how long, and howoften. A splint can be called functional only when it pro-vides more benefit than inconvenience.
Except for functional splints that are designed for aparticular function, these splints should allow mostactivities of daily living, such as grabbing keys out of anarrow pocket, writing and typing, driving a car, andriding a bike. Outriggers are always too bulky andcumbersome, and exposed rubber bands are frail. Thequest is for a “no-profile” design (Figure 14), with coilsprings or maybe, in the near future, electronic devices.
For patients with long-term or permanent handi-caps, specific functions may require long-lastingsplint materials, such as high-temperature thermo-plastics, and special accessories, such as polycentrichinges, but these are often beyond the technical scopeof therapists.
Technical Considerations
According to the flowchart (Figure 15), the proto-type is now ready to be refined according to theanatomic shape and biomechanics specific to thepatient. Good knowledge of the technical side of var-ious splinting materials and accessories surely willhelp the therapist finalize the splint.
The time has come that we as therapists not onlyconsider the biomechanics of a splint design, but alsoconsider aesthetics, styling, colors, fancy decorationfor kids (Figure 16)—in short, everything fun or aes-thetically pleasing that helps increase a patient’s com-pliance in use of the splint. A splint should reflect thepatient’s taste, of course, not the splint maker’s.
A simple finishing touch, such as realigning aswiveled edge or polishing the splint surface, is alsopart of minimalistic design and takes only seconds todo. The glitter of poster splints is often just such atouch. It is not a matter of the splint maker beingexceptional, just taking a little more time on the fin-ishing.
The algorithm thus far has described decisions madewithout reference to the personal skill of an individualtherapist. Now comes the time when we have to makefinal decisions based on our preferences and skills andthe splint’s feasibility. How the splint is supposed to
April–June 2002 199
FIGURE 15. Third part of the flowchart: technical considera-tions. Materials and accessories are selected according to thepatient’s needs and taste as well as availability. NOTE:Kinematic parts provide positioning and angular control;kinetic parts provide forces.7 LTTP indicates low-temperaturethermoplastic; HTTP, high-temperature thermoplastic.
FIGURE 14. “No-profile” splints. Left, median nerve splint. Right, Granger-design splint with a short sling attachment.6

look is known; the question is whether we are the rightperson to fabricate it. How have we been trained? Inwhat part of the world are we living? What materialsare available, and who is going to pay the bill?
Sometimes the choice of material is dictated by theprescription (thermoplastic splinting material vs.Neoprene, for example), but it is never dictated bybrand name. This would not make sense, since somebrands are offered in a limited number of countriesand identical materials may be distributed under dif-ferent names.
The better therapists know the properties of splint-ing materials, the more judicious the choices they willmake and the more perfectly their splints will be fab-ricated, without needing corrections or reinforce-ments. We want to use thin material for finger orthumb splints and thick material for elbow splints,perforated material for circumferential immobiliza-tion splints, but non-perforated for lateral connectionsplints. This is also minimalistic splint design!
These early years of the new millennium are notlikely to bring us new splinting materials that aremore convenient than low-temperature thermoplas-tics. Forty years after their introduction, low-temper-ature thermoplastics are available with a wide vari-ety of properties, marketed by many manufacturers,and distributed all over the world.
If the greatest advancements in the near future arenot expected to occur because of changes in materials,then the question is what other factors have con-
tributed, or will contribute, to advancements in splint-ing. How much have we improved our skills in shap-ing thermoplastics, and how much knowledge havewe gained from experts other than therapists?Mechanical, chemical, and orthotic engineers are thepeople we should consult initially. The issue is notlimited to the conformability, drape, and resistance tostretch of thermoplastics. Other, fine-tuning features,which are less often specified, are worth consideringin the fabrication of a minimalistic-design splint.
Elasticity, for example—usually called “memo-ry”—is not only a matter of material re-usability.Elasticity is primarily the ability of the material tostretch evenly and retract excess material, avoidingthe need for the therapist to fold the material, asshown in the elbow splint in Figure 17. 3
Many splint makers think some thermoplastics arejust pliable, not very stretchable, which is of courseincorrect. It is by stretching, not folding, that a two-dimensional sheet is magically transformed into athree-dimensional splint. The result is a neat shape,free of fringes and extra reinforcements.
Another unusual feature of splinting materials isadhesion. Although many tedious stories circulateabout the accidental bonding of untreated plastics,many splint makers have learned to use the exquisiteproperties of the sticky materials. Neatly bondedstraps and hinges, instead of rivets, may also be partof a minimalistic design.
As for the fabrication of accessories, such as hinges,outrigger systems, and pulleys, the question iswhether we are content with what is available or,instead, have the ability, time, and desire to custom-make them. Minimalistic-design splinting often favorscustom fabrication.
Prefabricated kits are convenient to use but not nec-essarily the best choice. Because prefabricated designsaddress as many pathologic conditions and sizes as
200 JOURNAL OF HAND THERAPY
FIGURE 16. A special design for a special person.
FIGURE 17. With a splinting material that lacks elasticity, foldsare inevitable. With elastic products, folds are easily avoided, asshown in the lower splint.

possible, the splints have many features that may notbe relevant for a particular patient. Pathologic condi-tions with identical target joints, and identical primaryfoci for splinting, do not necessarily call for identicalsplint designs, either. For instance, most therapistschoose a dynamic splint design with outrigger to assistMCP extension for treatment of postoperative arthro-plasty, but flexible outriggers without rubber bandsare the right choice for a patient with a radial nervepalsy, because they are more functional. Prefabricatedkits are intended for splint makers who have limitedtechnical skills or time.
CONCLUSIONS
Because splint making is a rational activity, it hasbeen possible to draw up a detailed flowchart thatincludes all the features that need to be considered,ensuring that all the steps necessary for success willbe taken. If all the decision steps of the flowchart arefollowed correctly, no omissions will occur and thesplint maker will not have to make corrections, losingprecious time and ruining the design.
The flowchart presented in this paper is notunique, and many splint makers have developedtheir own, but most of these do not have minimalis-tic design as a goal. Minimalistic design is an extradimension that results not only from a straightfor-ward thinking but also from an emphasis on simplic-ity and economy.
Minimalistic splint design can be learned easily.The desire to refine the splint design and the designprocess over and over again is a state of mind.
A minimalistic design emerges as we continue toquestion whether our splint fabrication is following a
minimalistic approach. Does the design directlyaddress all the splinting requirements before thesplint is fabricated? Does it address technical andfinancial possibilities and limitations in the moststructurally efficient ways?
Minimalistic splint designs are never created over-night. They grow, rather, out of a constant search toimprove a basically sound concept. Are we preparedto reconsider the quality of our work and our habitscontinually?
Acknowledgments
The splinting algorithm was created with Griet vanVeldhoven, OT, orthopedic engineer, as the basis of theworking method elaborated in the second volume of ourbook Therapeutic Hand Splints: A Rational Approach andPractical Applications (Antwerp, Belgium: Provan, in press). The author thanks Caroline W. Stegink Jansen, PT, PhD, forher endless support and encouragement in designing thispaper and making it readable.
REFERENCES
1. Malick MH. Manual on Static Hand Splinting. Pittsburgh, Pa.:Harmarville Rehabilitation Center, 1968.
2. Bailey JM, Cannon NM, Fess EE, et al. (eds). Splint Classi-fication System. Chicago, Ill.: American Society of HandTherapists, 1992.
3. Van Lede P, van Veldhoven G. Therapeutic Hand Splints: ARational Approach. Vol 1: Mechanical and Biomechanical Con-siderations. Antwerp, Belgium: Provan, 1998.
4. Fess EE, Philips CA; Hand Splinting: Principles and Methods.St. Louis, Mo: Mosby 1987.
5. Brand PW, Hollister A. Clinical Mechanics of the Hand. 2nded. St. Louis, Mo.: Mosby, 1993.
6. Crochetière W, Granger CV, Ireland J. The Granger orthosis forradial nerve palsy. Orthot Prosthet. 1975;29(4):27–31.
7. Craik RL, Oatis CA. Gait Analysis: Theory and Practice. St.Louis, Mo.: Mosby, 1995:455,160.
April–June 2002 201

Splinting Materials Old and New
For this special issue on splinting, the Practice Forum presents two splinting ideas. The first arti-cle features an ancient material largely unknown in western clinics, and the second utilizes a newmaterial. Our ancient idea comes from Uganda and demonstrates the creativity borne of necessity,beautifully illustrating the spirit that has made splinting such an important contribution to reha-bilitation of the hand. Our second article is a new variation on a popular theme, static progressivesplinting. For readers interested in the theory of static progressive splinting, two scientific articlesin this issue discuss the concept in detail—”A Proposed Decision Hierarchy for Splinting the StiffJoint, with an Emphasis on Force Application Parameters” (p. 158), by Ken Flowers, and “StaticProgressive Splinting” (p. 163), by Karen Schultz-Johnson.—PEGGY FILLION, OTR, CHT
PRACTICE FORUM
202 JOURNAL OF HAND THERAPY
ORIGINS AND APPLICATION OF BARK CLOTH IN UPPER EXTREMITY SPLINTING
Gail N. Groth, MHS, OTR, CHTRehab in MotionWatertown, Wisconsin
Julius Kamwesiga, OTProgram in Occupational TherapyMakerere UniversityKampala, Uganda
No thermoplastics in the supply cabinet? Just graba length of bark cloth, and go to it! Therapists inUganda have been using bark cloth for decades,maybe centuries.
In Third World countries, therapists have learnedcreative solutions to the problems they encounter.Their creativity is fostered by necessity, since westerntechnologies, if available, are rarely affordable.Furthermore, western solutions often infringe onlocal culture and tradition.
While familiar with the properties of low-tempera-ture thermoplastics, the professors at the MakerereUniversity in Kampala, Uganda, recognize theimpracticality of training their students in the use of
the material. It is cost-prohibitive and can beobtained only through infrequent donations. The cre-ative solution is to teach students to fabricate custom-made removable splints out of bark cloth.
Bark cloth (Figure 1) is harvested from a species offig tree, Ficus natalensis, known locally as the mutubaor banyan tree. The tree grows best in low-lying wet-lands found throughout Uganda. This species of figtree is one of few that can withstand the completeremoval of its bark and then grow it back again. Localworkers use a sharp knife to peel the bark away fromthe tree trunk. They begin just above ground leveland stop debarking just below the level of the firstbranch.
The bark is processed through a series of steps,which take two to five days to complete. The bark islaid on top of a felled tree and beaten with woodenmallets to make it more malleable. A series of wet-tings and dryings then transforms it into a fibrous,cloth-like material. A dye made from roots is applied,turning the bark cloth a beautiful burnt umber color.
Bark cloth is traditionally used for burial shroudsand for women’s clothing. It is also used to honorroyals in the Bagandan tribe. Often, it is embroideredwith bright colors and made into wall hangings,coasters, and placemats that are sold at the market-places. It is produced primarily in Uganda, but it isalso made in southern Sudan and western Kenya.
Therapists have found that bark cloth splints pro-vide sufficient immobilization, protection, and posi-tioning for a variety of clinical conditions. Ugandanoccupational therapy professors at MakerereUniversity, in Kampala, provide the followinginstructions for making a bark cloth splint.
Gail Groth was the recipient of the 2001 Vargas InternationalHand Therapist Teaching Fellowship from the AmericanAssociation of Hand Surgeons. This enabled her to volunteer atthe Mulago Hospital in Kampala, Uganda, in May 2001.Correspondence and reprint requests to Gail Groth, MHS, OTR,CHT, 1406 Beacon Drive, Watertown, WI 53098; e-mail: <[email protected]>.

April–June 2002 203
Fabrication of a Volar Wrist Splint
Preparation
1. Rip the bark cloth into small pieces, approxi-mately 2 square inches each (Figure 2).
2. Make a flour paste by mixing approximately onepart warm water with four parts flour.
3. Position the patient so that he or she is seatedwith the elbow on a table, forearm supinated,wrist in desired position, fingers relaxed.
4. Cut two small holes in a thin plastic bag and placethe holes over the patient’s thumb and fingers.
5. Crumble pieces of newspaper into three or fourballs.
Construction
1. Finger-paint the back of a piece of bark cloth withthe flour paste (Figure 3). Cover the surface entire-ly, but not so thickly that the paste drips off.
2. Lay the piece of cloth on top of the plastic, justproximal to the distal palmar crease (Figure 4).Using broad and sweeping motions, press andsmooth the piece onto the plastic.
3. Repeat this process, working distally to proximal-ly. Place each new piece so that it overlaps approx-imately one third of the previous piece. CAUTION:If you overlap too much, the splint will take toolong to dry. If you don’t overlap enough, thesplint will lose strength—and it will lose its shapewhen removed from the patient’s arm for drying.
FIGURE 1. Bark cloth, made from a species of fig trees (ficus natalensis). FIGURE 2. A small piece of ripped bark cloth.
FIGURE 3. Finger-painting flour paste onto the cloth. FIGURE 4. Layering the cloth pieces onto the arm.

204 JOURNAL OF HAND THERAPY
4. Gently smooth each new piece as it is added.
5. Wrap the bark cloth pieces around three quartersof the forearm diameter. Extend the bark clothpieces down two-thirds the length of the forearm.
6. When one layer is complete, gently pry the barkcloth off the patient, leaving the plastic bag intact.
7. Gently insert the newspaper balls into the splintto protect the forearm mold.
8. Allow the splint to dry for 1 to 2 days.
9. Remove the newspaper and plastic bag when theupper surface of the bark cloth feels dry.
10. Reinsert a smaller amount of newspaper, andallow the splint to dry overnight.
11. Repeat steps 1 to 10 until the desired rigidity isobtained. Typically, three layers are sufficient formost splinting purposes.
Finishing
1. Trim all edges, and cut three slits (each approxi-mately 1 inch long) on both sides of the splint, forstraps.
2. Varnish all surfaces with a clear polyurethane orsimilar product.
3. Thread the strapping material through a slit andsew the shorter end onto the longer strap.
4. Thread the same strapping material through theopposite slit, fold it back on itself, and lightlymark the area for closure with a pencil.
5. Sew Velcro hook-and-loop tape onto the strap-ping material.
6. Repeat steps 3 to 5 for the remaining straps.
A completed splint is shown in Figure 5.
Advantages of Bark Cloth Splints
Because it is a traditional product of the Ugandanpeople, bark cloth is easily obtained, even in the mostremote parts of the country.
Bark cloth costs very little. It is sold in large strips atthe marketplaces. The strips vary in size, but a typicalpiece is approximately 2 x 3 yards. This is enough forsix to eight splints and costs 5,000 shillings (about $3).
Custom-made splints are renowned for their superi-or fit and comfort. Bark cloth splints in particular canbe very light in weight and thin (much like 3/16 Orofit)but have high rigidity. The thickness and durability ofa bark cloth splint is easily adjusted with variation inthe number of layers of cloth applied.
Finally, bark cloth splints have proved to bedurable and able to withstand heavy use.
Disadvantages of Bark Cloth Splints
Bark cloth is traditionally used to shroud the dead.Splinting an injured extremity with a burial shroudmay have a negative effect on compliance.
Allowing for drying time, it may take from 2 to 6days to complete a bark cloth splint. This protractedtime is prohibitive for postoperative patients and fortraveling therapists who move from village to vil-lage, staying in each for only a day.
Bark cloth is not suitable for all splints. It is best usedwith medium to small (non-weight-bearing) splints. Itis unsuitable for large splints, such as long-arm splints,and splints designed to remediate hypertonicity.
Once formed, bark cloth splints cannot be adjustedin size. Therefore, they would not be appropriate foredematous body parts or for parts of the body inwhich significant muscular atrophy is anticipated.
Finally, it is somehow difficult to fix the straps on abark cloth splint, and to some patients, the splint maynot be appealing cosmetically.
FIGURE 5. The completedbark cloth splint.

INTRODUCTION TO A NEW METHOD FOR INELASTIC MOBILIZATION
Nelson Vazquez, OTR/L, CHTKessler Rehabilitation CentersMiami, Florida
Clinicians using inelastic traction (also known asstatic progressive splinting) will be interested in thisnew technique for applying inelastic mobilizationforces with a low-profile component called ClikStrips,a part of the Vazquez Inelastic Mobilization System.
King1 suggested that an inelastic mobilizationmechanism should apply low-load prolonged stressto contracted tissue with consecutive, advancing iso-metric settings. ClikStrips have measurable, repeat-able, consecutive advancing isometric settings at1.4-mm intervals. Keep in mind that there are cur-rently no published data that define a precise forceapplication (in grams or newtons) for the biological-ly safe and effective use of inelastic traction deviceslike this one, which is now under preliminary scien-tific investigation.
The purpose of this clinical paper is to present asimple and inexpensive technique for applyinginelastic traction forces to essentially any static pro-gressive splint design.
Materials and Methods
Materials and Tools (Figures 1 and 2)
■ ClikStrips component■ 1/16-inch-thick Reveals (low-temperature
thermoplastic) thermoplastic■ Reveals Tube, medium size■ 25-lb test monofilament for wrist and digits,
50 lb. for elbow■ Line connectors■ Finger sling■ Hook-and-loop straps (e.g., Velcro)■ Solvent■ Liquid adhesive (like super glue)■ Heat pan■ Heat gun■ Scissors■ Hole punch■ Crimp tool
ClikStrips and Reveals materials are available fromWFR Corporation, Wyckoff, New Jersey (www.
reveals.com); all other materials and tools are avail-able from WFR or any other national supply compa-ny that serves hand therapists.
ClikStrips are made of a translucent semi-crys-talline thermoplastic material, polyamide-nylon 6/6.The material has a high resistance to wear, heat, andchemicals, including solvents. It has a melting pointof 490° F and a locking strength of 50 lb.
The ClikStrips component consists of two parts, theStrip and the Lockclip. The Strip (Figure 3) is 16 mmlong and 0.7 mm wide. Its volar surface consists of a
April–June 2002 205
FIGURE 1. Materials used in fabrication of the splint.
FIGURE 2. Tools.
The author has a financial interest in one or more products men-tioned in this article.Correspondence and reprint requests to Nelson Vazquez, OTR/L,CHT, Kessler Rehabilitation Centers, 401 SW 42nd Avenue, Suite301, Miami, FL 33155; e-mail: <[email protected]>.
FIGURE 3. The ClikStrips Strip has seven isometric advance-ments per centimeter (18 per inch).

series of ridged stops at 1.4166-mm intervals. Thereare approximately seven ridges or advancements percentimeter (approximately 18 per inch). The Strip isinserted into the Lockclip to engage the inelasticmobilization (Figure 4).
The Lockclip (Figure 5) has an entrance with anarch projecting from it, called the upright. Theentrance tunnels toward the smaller opening, theexit. At the upper rim of the exit is the angled clip,which is controlled superiorly by the release tab.
Method
The low-profile ClikStrips allow creative liberty inhand and wrist splint designs. Figure 6 shows a com-pleted hand-based splint design using a ClikStripscomponent. The patient had a plated fifth metacarpalfracture with a resultant metacarpophalangeal jointextension contracture. (With the Lockclip properlybonded, the elbow can also be statically mobilized.)
1. Splint base. The splint base is 1/16-inch-thickReveals thermoplastic formed circumferentiallyto minimize distal migration.
2. Outrigger. Solvent is brushed on a 1/2 inch of a2-inch-long contour tube 7 mm in diameter, andthen dry-heated with a heat gun. The softenedportion is folded to 90° for bonding to the distalborder of the splint base just opposite theinvolved digit. (The placement site is spot-heatedfor 1 or 2 seconds after the solvent is applied).
While the material is still moldable, a crimp tool isused to form a horizontal hinge (slightly angledtoward the scaphoid) at the base of the outrigger(Figure 7). The outrigger should fold toward thescaphoid to follow the anatomic flexion of themetacarpophalangeal joint. The remainder of theoutrigger, distal to the hinge, is dipped into theheated water in the splint pan and, once transpar-ent, is molded into a cobra-like hook. Before itcools, the tip of the outrigger is flattened by a sus-tained pinch.
When the outrigger has cooled, one hole is madewith the hole punch at the curve facing the prox-imal phalanx (for a 90° traction alignment of thesling relative to the proximal phalanx), and a sec-ond hole is made through the flattened tip. Thehinged outrigger will move with the proximalphalanx as range of motion increases.
3. Finger sling. A line connector is slipped onto a4-inch length of 25-lb. test monofilament.Approximately 1 inch of the monofilament isslipped through one portal of the finger sling ofchoice, then threaded through the line connector.
206 JOURNAL OF HAND THERAPY
FIGURE 5. Diagram of the Lockclip, showing the entrance andexit for the strip as well as the upright, the angled clip, and therelease tab.
FIGURE 4. The ClikStrips Strip inserted into the Lockclip.
FIGURE 6. A completed hand-based splint using ClikStrips. a,Strip component. b, Lockclip. c, Reveals Tube bonded to base. d,Crimped hinge. e, Punched hole for sling attachment. f, Punchedhole for strip attachment. g, Punched hole in the strip.

The line connector is firmly compressed at bothends, with the crimp tool, to form a small closedmonofilament loop around the portal. This isrepeated with the second portal of the sling.
With the outrigger positioned parallel to theproximal phalanx, a monofilament from one ofthe portals is passed through the first punchedhole of the outrigger. A line connector is used tojoin the monofilaments of both portals, and iscrimped to form a closed loop connecting thesling to the outrigger (Figure 8).
The crimped hinge axis of the outrigger will notmimic flexion of the MCP joint axis; therefore, asmotion improves, an additional hole may bepunched and the sling monofilament re-attachedto it to maintain the optimal 90° angle of pull.
4. ClikStrips Lockclip. For the placement of theLockclip, a mark is made at the proximal edge ofthe splint base in alignment with the scaphoid rel-ative to the affected digit. A 1.5-cm square of 1/16-inch-thick Reveals thermoplastic is brushed withsolvent on both sides, as is the mark on the splintbase. The square piece is dry heated with a heat-gun until transparent (Figure 9), and the markedarea on the splint base is dry-heated for 1 to 2 sec-onds. The square piece is placed over the markedspot, ensuring a unified bond. Immediately, onedrop of liquid adhesive is placed on the bottom ofthe ClikStrips Lockclip (Figure 10). If more thanone drop of adhesive is used, the excess will over-flow into the tunnel and hinder the ease withwhich the Strip moves through it.
The Lockclip is firmly embedded into the stilltransparent 1/16-inch-thick Reveals thermoplastic,
April–June 2002 207
FIGURE 7. A crimp tool is firmly compressed to form a thinhinge.
FIGURE 9. Reveals thermoplastic is dry-heated on both sidesuntil transparent.
FIGURE 10. One small drop of liquid adhesive is placed onthe bottom of the Lockclip.
FIGURE 8. Positioning of the outrigger in relation to the fin-ger. a, Cobra-shaped outrigger with hinged base and flattenedtip. b, Finger sling. c, Finger sling portal. d, Finger sling mono-filament connection to first punched hole of outrigger.

with the entrance directly facing the outrigger(Figure 11). It is imperative to use 1/16-inch-thickelastic thermoplastic material, so that the materi-al will not encroach into the Lockclip’s tunnelonce the clip has been embedded. Because of the100% memory and 2% shrinkage of the Revealsthermoplastic, it firmly hugs the circumferenceof the Lockclip base as it cools and hardens, pro-viding an excellent bond.
5. ClikStrips Strip. The splint is secured to thepatient’s hand with hook-and-loop straps, andthe finger sling is placed over the proximal pha-
lanx to position the hinged outrigger at its start-ing point. With the ridges facing upward, theStrip is sized by slipping the unridged tipthrough the Lockclip and pushing it throughthree or four audible clicks. The Strip is then cut1 to 11/2 inches from the outrigger, and a smallhole is punched near the cut edge (Figure 12).
A 3-inch length of monofilament is cut andwoven through the second hole of the outriggerand then through the hole in the Strip, to form aloop. Each end of the monofilament is passedinto a line connector and crimped.
6. Implementation. With the components in placeand the splint base properly secured with hook-and-loop straps, the Strip is pushed through theLockclip until the slack of the components is elim-inated. The unridged proximal end of the Strip isfirmly pinched and the Strip pulled through theLockclip one click at a time, until the appropriateforce (which does not exceed safe end range) isestablished. The indentation of the ridge immedi-ately proximal to the angled clip is marked with apen as a baseline and then marked subsequentlyas progress is made.
It is very important that the patient understandsthe concept of incremental increases to preventdamage to tissues. The inherent feedback fromeach advancing visible ridge may, at times, temptan enthusiastic patient to be too aggressive inadvancing the Strip before the tissue is able to tol-erate the tension. For this reason it is suggestedthat the therapist perform the advancements, atleast initially.
To disengage the Strip and release the isometrictraction, the patient, using the uninvolved hand,places the tip (not the pulp) of the thumb againstthe upright and the tip (not the pulp) of the indexfinger on the release tab, and firmly pinches.While the pinch is maintained, the involved digitis actively extended, causing the Strip to slide outof the Lockclip in a distal direction.
For any mobilization technique, it is the clinicianwho determines the appropriate force and durationof force for a particular tissue restriction.2 Accordingto Flowers and LaStayo,3 increases in the passiverange of motion of a contracted joint are directly pro-portional to the time the joint is maintained at endrange. The tension itself is progressively altered tocoincide with and maintain the matrix turnover rate4;however, because of variances in tissue response andin the severity of injuries, no specific time can be gen-erally established for the duration of splint applica-tion to gain motion.2
208 JOURNAL OF HAND THERAPY
FIGURE 12. Sizing and attachment of the ClikStrips Strip. a,Sized ClikStrips Strip with punched hole and monofilamentattachment to flattened tip of outrigger. b, Unridged proximalend. c, Baseline tracking mark on strip indicates start of traction.
FIGURE 11. The Lockclip is compressed into the 1/16-inch-thickReveals thermoplastic and held for 30 seconds.

Conclusion
The ClikStrips inherent measuring device withinits ridged traction line allows for precise control inmobilization of stiff tissue. Each increment has a dis-tinct, unmistakable, audible click per advancement toassure limited progression. It is versatile, cost-effec-tive and relatively simple to apply. Its opaque hueblends well with Reveals and, along with its low pro-file, makes it cosmetically acceptable. Patient com-pliance is excellent in that they have visible, direct,measurable feedback of their improvement.
With modification, this component can be fabricat-ed with materials found at some hardware stores. It
is also available commercially, without need formodification, from WFR Corporation (Wyckoff, NewJersey; www.reveals.com).
References
1. King JW. Static progressive splints. J Hand Ther. 1992;5:36–7.2. Colditz JC. Therapists’ management of the stiff hand. In:
Hunter JM, Mackin EJ, Callahan AD (eds). Rehabilitation ofthe Hand: Surgery and Therapy. 4th ed. St. Louis, Mo.: Mosby,1994:1141–59.
3. Flowers KR, LaStayo P. Effect of total end range time oimproving passive range of motion. J Hand Ther. 1994;3:150–7.
4. Fess EE, McCollum M. The influence of splinting on healingtissues. J Hand Ther. 1998;2:157–161.
April–June 2002 209