Journal of Early Intervention - Scott Memorial...
20
http://jei.sagepub.com/ Intervention Journal of Early http://jei.sagepub.com/content/29/4/287 The online version of this article can be found at: DOI: 10.1177/105381510702900402 2007 29: 287 Journal of Early Intervention Philippa H. Campbell and L. Brook Sawyer Participation-Based Services Supporting Learning Opportunities in Natural Settings Through Published by: http://www.sagepublications.com On behalf of: Division for Early Childhood of the Council for Exceptional Children can be found at: Journal of Early Intervention Additional services and information for http://jei.sagepub.com/cgi/alerts Email Alerts: http://jei.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://jei.sagepub.com/content/29/4/287.refs.html Citations: by Philippa Campbell on October 20, 2010 jei.sagepub.com Downloaded from
Transcript of Journal of Early Intervention - Scott Memorial...

http://jei.sagepub.com/
InterventionJournal of Early
http://jei.sagepub.com/content/29/4/287The online version of this article can be found at:
DOI: 10.1177/105381510702900402
2007 29: 287Journal of Early InterventionPhilippa H. Campbell and L. Brook Sawyer
Participation-Based ServicesSupporting Learning Opportunities in Natural Settings Through
Published by:
http://www.sagepublications.com
On behalf of:
Division for Early Childhood of the Council for Exceptional Children
can be found at:Journal of Early InterventionAdditional services and information for
http://jei.sagepub.com/cgi/alertsEmail Alerts:
http://jei.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://jei.sagepub.com/content/29/4/287.refs.htmlCitations:
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

287
REGULAR ARTICLE
Supporting Learning Opportunities inNatural Settings ThroughParticipation-Based Services
PHILIPPA H. CAMPBELL AND L. BROOK SAWYERThomas Jefferson University
Recommended early intervention practices emphasize family-centered approaches provided withinnatural settings through interventionist interactions with caregivers. We defined this approach asparticipation-based and used the Home Visiting Observation Form (HVOF) and the NaturalEnvironments Rating Scale (NERS) to describe 50 home visits and to examine the extent to whichparticipation-based services could be identified and distinguished from traditional services. Aminority of the sample visits were described as participation-based although participation-basedservices were clearly distinguishable from traditionally provided services. Interventionists usingparticipation-based approaches interacted with the caregiver-child dyad and caregivers wereactively involved with their children during the session. Results from the study suggest the NERScan be used to describe characteristics of participation-based services and holds promise asa measure that might be used by interventionists, their supervisors, or by researchers to measureintervention fidelity during home visits.
Home visits have become a primary methodfor early intervention birth to 3 service pro-vision. The home as a location for earlyintervention services evolved as states ad-dressed the Part C natural environments
requirement and defined natural environ-ments as a location where services occur.
Although IDEA regulations broadly definenatural environments as &dquo;those settings thatare natural or normal for the child’s age peerswho have no disabilities&dquo; (34 CFR 303.18),homes came to be viewed as the defaultnatural environment for Part C. In 1993,47% of infant-toddlers received early inter-vention services in the home. By 1997, this
percent had increased to 59% and by 2004, to83% (U.S. Department of Education, Officeof Special Education Programs, 2003; 2004).
Even though a majority of infants andtoddlers receive their early interventionservices at home, concerns have been ex-
pressed about the extent to which thoseservices are any different than what thera-
pists, teachers, or other early interventionspecialists traditionally have provided in
a center or clinic (McWilliam, 2000). Tradi-tional service models generally are child-
focused, oriented to children’s developmentalor physical needs, and include the followingcomponents: a) areas of concern, generallyexpressed as developmental skill outcomes orgoals; b) planned methods, strategies, or
approaches to be used to address the areasof concern; and c) progress monitoring ormeasurement. In traditional services, theinterventionist plans activities that provide
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

288
a context in which the child can learn or
practice targeted skills and works directlywith the child to provide learning opportu-nities. Home programs might be designed forcaregivers to work on targeted outcomes
between intervention visits (Dunst, Trivette,Humphries, Raab, & Roper, 2001).
Alternatives to the traditional approachhave been offered and attempts have beenmade to rethink and define practice innatural environments (Chai, Zhang, & Bis-
berg, 2006). A conceptual model for imple-mentation of intervention in natural settings(e.g., home and community) has been de-scribed by Stremel and Campbell (2007) whodefined nine components of practice innatural settings by summarizing recom-
mended practices reported in the literature.The identified components are broad-basedand include practices such as interaction withfamilies, assessment, intervention, and prog-ress monitoring, all of which should be
present when practitioners work with infantsand toddlers and their families. The beha-viors and practices of early interventionistswhen providing intervention in natural set-
tings has been described and labeled as
participation-based, given that a primarypurpose of intervention in natural settings isto promote children’s participatory learningopportunities and to teach caregivers to useeffective strategies in their interactions withtheir children (Campbell, 2004).One assumption underlying the participa-
tion-based approach is that services will be
incorporated into a family’s daily routinesand activities. The importance of providingearly intervention services within activitiesand routines has been emphasized throughthe development of specific curricula or
procedures such as routines-based interven-tion (McWilliam & Scott, 2001), familyguided routines-based intervention (Cripe,Hanline, & Daley, 1997; Woods, Kashinath,& Goldstein, 2004), activity-based interven-tion (Pretti-Frontczak & Bricker, 2004; Val-vano, 2004), learning opportunities (e.g.,Dunst, 2000, 2001; Dunst & Bruder, 1999;Dunst, Bruder, Trivette, Raab, & McLean,2001; Dunst, Hamby, Trivette, Raab, &
Bruder, 2000; Dunst, Herter, & Shields.
2000), or the more recently labeled modelof early intervention in natural environments(EINE; McWilliam, 2005). Although each ofthese approaches define key features some-what differently, they share a common focuson both the identification and use ofactivities and routines as contexts for teach-
ing and learning and on an interventionistrole of supporting and teaching families
(Chai et al., 2006; Edelman, 2004). Whilemany of the approaches include specificforms for interventionists to use to planinterventions (e.g., Dunst, Bruder, Trivette,Hamby, et al., 2001; McWilliam, 2005;Woods, 2005) or suggest general home
visiting strategies (Axtmann & Dettwiler,2005; Klass, 2003: Wasik, Bryant, & Lyons,1990), to date, none of these advocated
approaches clearly delineate exactly what aninterventionist should do when visiting a childand family in their home or other naturalsetting. In the absence of descriptions ofwhat interventionists should do, it is difficultto either examine intervention fidelity or itsrelationship to child and family outcomes.
Describing Home VisitsThe Home Visit Observation Form (HVOF;McBride & Peterson, 1997) was designed todescribe and quantify what early interven-tionists do during home visits. The formrecords interaction partners (who is in the
interaction), content of the interaction (whatis occurring during the visit), and the role ofthe home interventionist. In the initial use ofthis scale, the authors asserted that if family-centered services were being provided, a mi-nority of the interactions would be betweenonly the interventionist and child, the visitcontent would reflect a variety of areas witha minority of time spent solely on children’sskill development, and a minority of timewould be spent by the interventionist in directteaching of the child. When used with a samplethat consisted of 15 early interventionists and28 children/families, with data collected acrossthree home visits for each interventionist/
child/family triad, results showed the visits didnot reflect the principles identified by the
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

289
authors as reflective of a family-centeredapproach. Primarily, providers interactedwith children and the content of a major-ity of the visits focused almost entirely onchild development. The providers spent morethan half their time in direct teaching withchildren.Two additional studies of early interven-
tion home visits have been conducted andboth have used modifications of the originalHVOF. Early intervention home visits werecompared with visits made by two types ofEarly Head Start workers (i.e., child de-
velopment specialists and family develop-ment specialists; Peterson, Luze, Eshbaugh,Jeon, & Kantz, 2007). In the early interven-tion provider group (n = 15), almost half ofthe interactions involved only the interven-tionist and child, with content focused almostexclusively on the child’s development. Theinterventionists spent more than half theirtime instructing the child. Results were
similar in a second study where three visitsof 83 early interventionists who had and hadnot received relationship-based training werecompared using a modification of the orig-inal HVOF. In this study, a fourth categorywas added to the HVOF to describe the roleof the caregiver (Wilcox & Lamorey, 2004;Wilcox, Campbell, & Lamorey, 2006). Amajority of interactions for both groups ofearly interventionists were classified as in-
cluding the interventionist-caregiver-child.The primary caregiver’s role, however, wasto watch or not interact with the child or
interventionist; caregivers interacted withchildren less than 20% of the visit time.Interventionists spent over half of their time
directing the child.
A Framework for Participation-BasedHome Visits
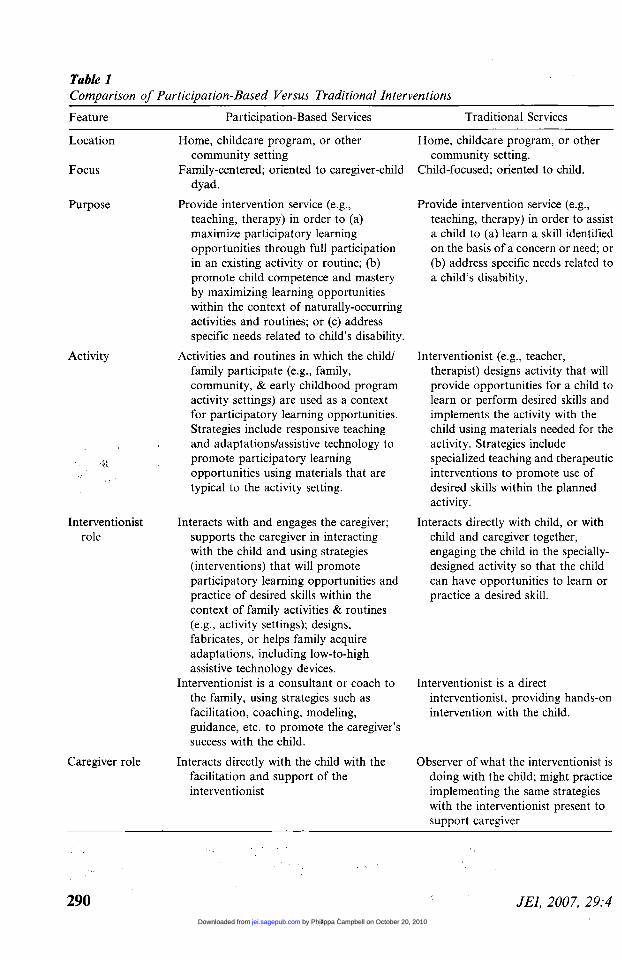
Using reports from the literature, features oftraditional and participation-based serviceswere contrasted using six dimensions: loca-tion, focus, purpose, activity, role of the
interventionist, and role of the caregiver. Asshown in Table 1, the location where servicesare provided is not a distinguishing featurebetween these two types of service provision
approaches. There are, however, criticaldifferences in the focus of each approach,although early interventionists might trans-late these concepts differently in practice. Forexample, early interventionists report that
they are focusing on the family and doingwhat the family wants them to do when theycome into a home and provide direct one-on-one services to children (Hanson & Bruder,2001). Furthermore, practitioners’ under-
standing of working with families oftenmeans that families should &dquo;get down onthe floor&dquo; and watch what practitioners dowhen they are working with children so thecaregiver will be able to follow-throughbetween sessions (Campbell & Halbert,2002). Because terms such as family-centeredor natural environments mean different thingsto different individuals, we further definedthe focus of services by purpose, activity, androle dimensions.
Broadly speaking, the purpose of both
participation-based and traditional services isto provide intervention for a child. The
intervention is translated differently, howev-er, in the activities used for intervention andin the roles of the interventionist and
caregiver. In participation-based services,the interventionist uses naturally occurringroutines (e.g., mealtimes) or activities (e.g.,playing on a playground; riding in the car;shopping) to provide children’s learningopportunities. In traditional services, an
interventionist designs activities to providespecific learning opportunities (e.g., playingwith particular toys to encourage manipula-tion). When interventionists create activitiesto provide specific learning opportunities,they generally select materials needed to
engage in the activity, which might result ininterventionists bringing special materialsinto the home (Washington, Schwartz, &
Swinth, 1994). In participation-based ser-
vices, the caregiver interacts directly with thechild while the interventionist supports,teaches, or coaches. In traditional services,the interventionist interacts directly with thechild and the caregiver is either not present orobserves (mostly passively) what the inter-ventionist is doing.
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from
290
Table 1
Comparison of Participation-Based Versus Traditional Interventions
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

291
Given the promise of the HVOF measurefor describing what occurs during home visitsand a framework for distinguishing partici-pation-based versus traditional home visitingapproaches, the present study had two majorpurposes: (a) to describe characteristics of
early intervention home visits and (b) to
determine the extent to which participation-based and traditional services could be
distinguished by key characteristics usingthe HVOF and an investigator-developedrating scale. We hypothesized that earlyinterventionists could be working withina natural setting (e.g., the home) but beproviding either the same type of service (i.e.,traditional) as would be provided in anothersetting (i.e., clinic or center) or a type ofservice where family activities and routinesprovided a context for intervention (i.e.,participation-based). Because traditional ser-vices are reported in the literature as a pre-dominant service model, we hypothesizedthat a majority of the visits would beclassified as traditional and that interven-tionist characteristics such as discipline, yearsof experience, or number of children/familieswith whom an interventionist was working(e.g., caseload) would not be related to thetype of service provided.
METHOD
ParticipantsThe sample of convenience for the presentstudy was 50 early interventionists froma variety of disciplines (e.g., teachers and
therapists) who provided Part C services ina northeastern state. All participants sub-mitted to the investigators a videotape thatshowed a typical intervention activity witha child and family they served. Table 2 showsthe demographic information for the studysample. A majority of the interventionistswere female and Caucasian, although indi-viduals with other ethnic backgrounds madeup 28% of the sample. Teachers (27%)constituted the largest percent of interven-tionists ; occupational therapists, physicaltherapists, and speech-language pathologistscomprised 15% to 24% of the study sample.
Interventionists had an average age of36.5 years and averaged more than 8 yearsexperience in their disciplines (range < to
24 years) and 3 years of experience in earlyintervention (range < I to 17 years).
The majority of children served by theseinterventionists were male. Approximatelytwo-third were Caucasian, one-fifth were
African American, and the remaining chil-dren were Latino. Almost half of the childrenwere between 12 and 24 months of age; theremainder were between 25 and 36 months.No children included in the sample wereyounger than 12 months. Approximatelyone-third of the children had speech delaysonly, one-third had motor disabilities, andthe remaining were classified as havingmultiple disabilities (e.g., blind with physicaldisability), developmental delay, pervasivedevelopmental disorder or autism, or otherconcerns (e.g., nutritional problems).
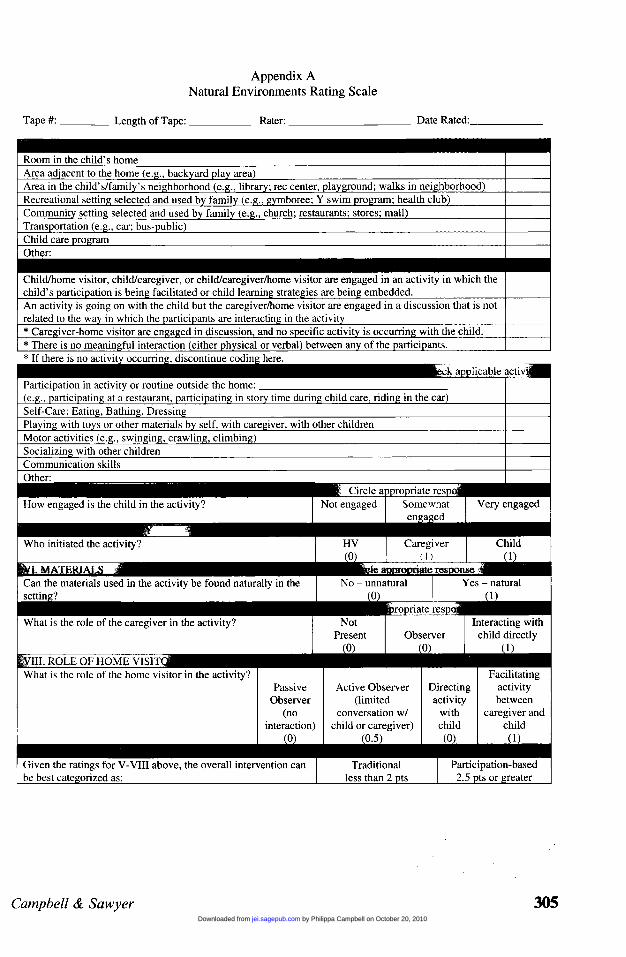
MeasuresWe rated each of the 50 videotapes with twoscales to describe what occurred during thehome visits. Each tape was rated first withthe Natural Environments Rating Scale
(NERS; Campbell & Sawyer, 2004; Appen-dix A) and then with a modified version ofthe Home Visit Observation Form-Modified(HVOF-M; Wilcox & Lamorey, 2004).
Natural Environments Rating Scale
(NERS). We developed the NERS to
summarize home visit activities focused onchild learning. Ratings were made followingviewing of a videotaped visit between aninterventionist and the family/child. The firstNERS category rated was setting. Settingwas noted to identify situations where inter-ventionists worked with families and childrenin settings outside the home. More than onesetting could be represented on the tape andcounted. Because the NERS was designed tobe used to rate implementation of child-focused interventions, activity was used toidentify broadly the situation(s) occurring onthe tape. If the focus of the visit was not ona child-focused activity (e.g., interventionistand caregiver were having a discussion), useof the NERS was discontinued. When the
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

292
Table 2
Early Interventionist Characteristics
Note. OT = occupational therapist; PT = physical therapist; SLP = speech and language pathologist.
rater determined the session included a child-focused intervention, six additional cate-
gories were rated on the NERS: (a) type ofactivity; (b) engagement of child; (c) leader ofactivity; (d) materials; (e) role of caregiver;and (f) role of home visitor (see Appendix).Type of activity further specified the pur-pose(s) of the intervention activity (e.g.,socialization, motor skills). More than onetype of activity could be represented on thetape and counted. Engagement of child wasrated on a 3-point scale ranging from notengaged ( 1 ) to very engaged (3) .The characterization of the session as
traditional or participation-based resultedfrom scores obtained on the remaining fourcategories: leader of activity, materials, role
of caregiver, and role of home visitor. Thesefour categories were used to represent dimen-sions that differentiated the two types of
services. Leader of the activity referred to
whether the activity was a child-directed oradult-directed activity and identified the
adult (e.g., interventionist or caregiver) whowas directing the activity. Because activitiesthat are planned and directed by an earlyinterventionist might be de-contextualizedfrom the child’s activities and routines and
require use of specialized materials (e.g.,particular toys or therapy equipment), werated whether the materials used during theactivity would be naturally available in thesetting. The last two categories identifiedroles for the interventionist (i.e., observing,
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

293
directing, or facilitating) and the caregiver(i.e., not present, observing, or directlyinvolved).
The four categories were scored by assign-ing a value of 7 to each characteristic ofa participation-based visit (see Appendix Afor coding values). In the role of the in-
terventionist, however, a midpoint value of0.5 was assigned to the category of activeobserver because active observer includessome interaction with the caregiver but notthe extent of interaction required to be codedas facilitator, a role that is a characteristic ofa participation-based approach. Videotapeswith values totaling 2 points or less were
coded as traditional, and those with scores of2.5 points or greater were labeled as partic-ipation-based. In the present study, the
primary purpose of the NERS was to
differentiate between traditional or partici-pation-based approaches based on the fouron key dimensions. These two approacheswere viewed as dichotomous, rather thancontinuous. Characterizations of activities
viewed on the videotapes as participation-based or traditional were based on ratingsassociated with four inter-related categories:leader of activity, materials, role of caregiver,and role of home visitor.Home Visit Observation Form-Modified
(HVOF-M). The original HVOF form
(McBride & Peterson, 1997) was designedto be completed by a rater who is presentduring the entire home visit. The originalform contained three major coding cate-
gories : interaction partners, content of theinteraction, and role of the home visitor. Inthis study, a modified version of the HVOFwas used (i.e., HVOF-M). The HVOF-M isan observational coding instrument, which isscored while viewing a videotape of a homevisit. For the modified version, a fourth
category was included, with codes that
specified the role of the caregiver (Wilcox &
Lamorey, 2004). Each of the four categoriesincluded multiple codes to allow recording ofa wide variety of situations. For example,interaction partners included various combi-nations of child, parent, home visitor, andother participants. Content of the interaction
included such activities as discussion ofvarious topics (e.g., child’s progress, child’sservices, family issues), explanations byinterventionists to parents about goals andactivities, and play with the child (i.e., child-focused activity). Role of the home visitor
generally consisted of home visitor workingdirectly with the child, supporting the
family’s actions with the child, or havinga discussion with the family. Role of theparent included such actions as working withthe child, watching the interventionist workwith the child, or engaging in discussion withthe home visitor. (The HVOF-M can beobtained from the first author upon request).
Procedures
Early intervention service providers complet-ed a two-session self study professionaldevelopment workshop where they learnedabout providing intervention within naturalenvironments. Providers were given writtenmaterials, such as an assessment of familyroutines and activities, to use in their workwith children and families. They subsequent-ly attended a second session where theysubmitted written materials and a videotapeof themselves implementing a &dquo;typical&dquo; ac-tivity in the context of a home visit with a self-selected family. Interventionists were askedto obtain and submit a videotape that wasfocused on an intervention activity witha child (versus a family discussion) of
approximately 20 min in length. Submittedvideotapes varied in length from 5 to 80 min(M = 22.5; SD - 15.6). Shorter tapesgenerally consisted of one specific child-focused activity (e.g., practicing using hand-over-hand feeding technique), whereas longertapes contained multiple child-focused activ-ities or contained a child-focused activityand other components, such as family dis-cussion.
Scoring the Natural Environments RatingScale (NERS). A staff researcher watchedeach videotape in its entirety and then ratedthe setting and activity categories of the
NERS. If the tape contained a child-focused
activity (or activities), then the remainingNERS categories (i.e., type of activity, child
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

294
engagement, leader of activity, materials, roleof caregiver, and role of home visitor) wererated based on the activities. Descriptiveanalyses (i.e., frequency counts, percentages)were conducted for seven of the eight NERScategories for each of the service classifica-tions (i.e., participation-based or traditional).The excluded category was activity becausethis category was used to verify that an
activity involving the child was occurring andthat the NERS could be used to rate the
videotaped visit.Approximately 20% (11 of 50) of the
videotapes were randomly selected and codedby a second staff researcher to determineinterobserver agreement. The number of
NERS categories for which the two codersdemonstrated agreement was summed, di-vided by the total number of categories, andmultiplied by 100. We calculated interrater
agreement for all eight categories and for thefour categories that were used to determinewhether the videotape activity was participa-tion-based or traditional. Overall, the twoobservers demonstrated a mean percentagreement of 86% for the eight categoriesand 89% agreement for the four categories.
Scoring the Home Visiting Observation
Form-Modified (HVOF-M). Each of the
four HVOF-M categories were rated usingcodes representing each category at 30 secintervals Within each of the four codingcategories, if more than one rating could beapplied during a 30-sec interval, the behaviorthat occurred for the predominant amount oftime was rated. For example, if the in-terventionist was providing sensitive direc-tion for 20 sec (of the 30-sec interval) andwas providing sensitive facilitation for 10 sec,the role of the interventionist was scored assensitive direction for that interval. Because
length of the videotapes varied, we calculatedthe percent of intervals in which each codeoccurred. For example, 75% in sensitivedirection represented a situation where theinterventionist was coded as providing sensi-tive direction during 75% of the ratingintervals.
Coding began when the videotaped child-focused activity started; if the videotape
began with the camera being set-up or othernon-child focused intervention, we delayedcoding until the intervention activity started.Coding continued until the end of the
videotape or until 40 intervals (i.e., 20 min)elapsed. Twenty min was judged as sufficientduration for filming one or two child-focusedactivities; videotapes longer than 20 min
generally contained periods of nonchild-focused activities (e.g., family discussion,camera set-up). Tapes under 20 min includedone child-focused activity generally occurringwith an infant or younger child. Thirtypercent of the tapes were analyzed for 40intervals (20 min), 28% for 30-39 intervals(15-19.5 min), 22% for 20-29 intervals (10-14.5 min), and 20% for fewer than 20intervals (5-9.5 min).
Additional codes were used to representissues related to technical problems or lack ofinteraction. A code of technical problem wasused to define problems with videotaping(e.g., the camera was pointing toward thefloor for the majority of the interval). Anyintervals in which the primary code was
technical problem were dropped before per-cent interval data were calculated. A second
code, no interaction, was used across all
categories and this code reflected no interac-tions occurring among any of the partici-pants during the interval. In categories ofrole of the home visitor or role of the
caregiver, an additional code was used to
reflect no interaction of the specific individualbeing rated (e.g., no interaction of the homevisitor with either the child or caregiverbecause the home visitor was engaged inanother activity such as writing notes). Allcodes were used to rate each videotape.Similar codes were combined within each
category to reduce the number of codes usedin the analyses (see Table 3). For example,intervals coded as no interaction were com-bined intervals coded as transition, a codeused to rate transitions between activities.
Descriptive analyses (i.e., means, ranges,standard deviations) were computed for thecombined codes for the HVOF.
Approximately 30% (16 of 50) of the
videotapes were coded by a second research
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

295
Table 3Final Rating Categories for the Modified HVOF1
Note. HVOF = Home Visiting Observation Form; ~ = Table 3 represents the collapsed codes for the modified HVOF.For information on the complete list of codes, contact Philippa Campbell at [email protected]
assistant to determine interobserver agree-ment rates. Agreement rates were calculatedfor each category and for the overall
videotape. The number of intervals for whichthe coders demonstrated agreement on a cat-
egory was summed, divided by the totalnumber of intervals, and multiplied by 100.Overall, the two observers demonstratedmean percent agreement of 92% (99% forinteraction partners, 93% for content of
interaction, 85% for role of home visitor,and 94% for role of parent).
Comparison across traditional and partici-pation-based groups. Independent samples,two-tailed, t-tests were conducted to compareintervention visits rated on the NERS scale
as traditional or participation-based acrossthe combined codes on the HVOF. We
calculated standardized difference effect sizesbased on the mean percent interval data foreach group and the standard deviation of thetraditional group, where d = .20, d = .50,and d= .80 are considered small, medium,and large effect sizes, respectively (Rosenthal& Rosnow, 1991).
RESULTS
Characteristics of Home Visits Rated bythe NERSBased on NERS ratings, 35 (70%) of the 50videotaped visits were coded as traditional,
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

296
Table 4Natural Environments Rating Scale (NERS)
while 15 (30%) were coded as participation-based. Table 4 shows the percentages foundfor each NERS category across the two
groups. Overall, most of the visits occurredin a room in the child’s home although 27%of the participation-based services occurredin an area in the family’s neighborhood suchas a park, playground, or store. A range ofactivities (e.g., playing with toys, physicalmotor activities) were represented in both
types of visits. Children were rated as notengaged in less than 10°Io of visits in both
categories, and children in participation-based services were more frequently ratedas very engaged when compared to childrenreceiving traditional services.
To investigate whether the visits classifiedas traditional or participation-based differedin categories of setting, type of activity, andengagement, chi-square tests were used. Onlyone statistically significant difference was
found: participation-based home visits weremore likely to be provided in the child’s
neighborhood than were the traditional visits(X2= (1, N=75) = 10.15, p <.O1). Phi, whichindicates the strength of the associationbetween two variables, was .45 (medium tolarge effect).
Differences were found for each of thefour dimensions used to determine whether
I
the home visit activity session was rated astraditional or participation-based. For visits
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

297
coded as traditional, the interventionist waspredominantly the leader and director of theactivity, with the caregiver most often actingas an observer. In the visits coded as
participation-based, either the caregiver orthe child was the activity leader. The
caregiver directly interacted with the child,and the most frequent role of the interven-tionist was as a facilitator. In both groups,materials were almost exclusively natural tothe environment.
Characteristics of Home Visits Rated bythe HVOFTable 5 shows the means and standarddeviations of the traditional (n = 35), andparticipation-based groups (n = 15) for thecombined codes associated with the fourHVOF categories. These data are reportedas percentages of intervals for each code. Theresults of independent-samples, two-tailed t-
tests comparing the traditional and partici-pation-based groups for each category alsoare illustrated in Table 5. Although the
percentage of intervals rated as no interac-tionltransition (i.e., no interactions amongcaregiver, home visitor, or child) were smallin both the traditional and participation-based videotapes, the videotapes rated as
participation-based included a greater per-centage of no interactionltransition intervalsand this difference was statistically signifi-cant across each of the four rating categories.
Interaction partners. Overall, a majorityof interactions for both groups consisted ofinteractions between the interventionist-care-
giver-child. Interactions between only thechild and the interventionist were more
frequent, however, in the traditional groupand these differences were significant (t (47.5)=3.33, p - .002). According to Cohen’s
(1988) guidelines, the standardized differenceeffect size (d = .65) is considered a mediumeffect.
Interactions between the caregiver and thechild alone (e.g., no interventionist interac-tion) occurred less frequently in traditionalthan in participation-based groups (2.39%versus 17.46% of intervals). This differencewas not statistically significant (t (14.49) =
-1.84) but the effect size was large(d=-2.39). Very few of the intervals in eithergroup were coded with interactions betweenother combinations of participants (e.g.,other adult and child or caregiver and
sibling).Content. For both groups, most interac-
tions involved some type of play activity.This finding was not unexpected due to thesample inclusion criteria of a visit that wasintervention-based; play is the content codein the modified HVOF used to code any
activity related to the child. The percentageof intervals that focused on a discussionbetween the parent and interventionistsabout the child’s needs were similar across
traditional and participation-based groups.Slightly more participation-based intervalsincluded an interventionist providing an
explanation of a topic to the caregiver.Neither group frequently engaged in discus-sion of other sorts (i.e., discussion aboutother family members, services, administra-tive issues, or general talk). Nor did eithergroup often display content about &dquo;other&dquo;areas (e.g., child crying and interactioncenters on calming child).
Role of the home visitorlinterventionist.
Statistically significant and noteworthy dif-ferences between the traditional and the
participation-based groups occurred for sixof eight role categories. Interventionists in
the traditional group more often displayedbehavior related to interacting with childrenin an adult-directed activity. These includedproviding both sensitive direction, where theinterventionist initiates an activity that is
well-paced and involves opportunities for thechild to make choices, and sensitive facilita-tion, where the interventionist joins intochild-initiated play and actively engages inand facilitates a child-initiated play activity.The effect size for both of these codes was
large according to Cohen’s (1998) guidelines(d = .99 and d = .82, respectively). Interven-tionists in the traditional group more often
provided insensitive interactions, a codingcategory that combined insensitive facilitation(e.g., the interventionist is passive and mainlyobserves the child engaged in child-initiated
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

298
Table 5Home Visit Observation Form (HVOF) Ratings
Note. 1 = Degrees of freedom vary because statistical adjustments for unequal means and variances were invoked.
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

299
Table 6
Percent of Intervals for Role of Caregiver and Role of Interventionist by NERS Rating Category
Note. NERS = Natural Environments Rating Scale; HVOF = Home Visiting Observation Form.
play) and insensitive direction (e.g., the in-
terventionist directs the activity and the childis provided little choice or opportunity torespond). Differences between the groupswere statistically significant (t (42.6) = 2.09,p = .04) with a medium effect size (d = .47).
As shown in Table 5, intervals where theinterventionist supported (through modelingor verbal support) the interaction betweenthe child and caregiver were more frequent inthe participation-based group. Similarly,interventionists in the participation-basedgroup more often observed the caregiverinteracting with the child. The remainingtwo roles for interventionists were not
statistically different between groups. Partic-ipation-based interventionists slightly moreoften engaged in conversation with caregiversthan did traditional providers. Videotapesrarely showed providers engaging in &dquo;other&dquo;roles (e.g., soothing crying child, wipingchild’s nose).
Role of the caregiver. Statistically signif-icant and noteworthy differences emerged infour of six categories associated with care-giver roles. Caregivers in the traditional
group most frequently watched the interven-tionist and child interact. Caregivers in thetraditional group also showed a higher per-centage of intervals as not being involved inthe interaction. Both effect sizes for these
categories were medium to large (d = .89 and.74, respectively) For the participation-based
group, the predominant caregiver role was tointeract with the child (58.2% of intervals).The two groups showed roughly even per-centages of intervals for caregivers (a)engaging in conversation with the interven-tionist and (b) engaging in other interactions(e.g., interacting with a sibling child or
another adult).
Differentiating Traditional andParticipation-Based ServicesAlthough the number of visits that were
rated as participation-based was smaller thanthose rated as traditional, the NERS codingcategories differentiated between the two
approaches. Of the four categories that
comprised the NERS, only the role of thehome visitor and role of the caregiver overlapwith categories on the HVOF. Neither theuse of materials that would be easily avail-able in the home nor ratings of who serves asthe leader of the intervention activity are
included on the HVOF. To compare the
NERS and the HVOF, a matrix was con-structed comparing caregiver and interven-tionist roles for traditional and participation-based services. As shown in Table 6, mean
percentages of intervals for each of the
caregiver and interventionist roles alignedwith the types of roles expected in traditionaland participation-based services. Additional-ly, interventionist characteristics for the twotypes of service categories (see Table 2) were
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from
300
compared using independent t-tests and, asexpected, no statistically significant differ-ences for total years of experience (t(38) =.620, p = ns), total years of experience in EI(t(40)= .238, p = ns), or hours per week thatthe interventionist worked in early interven-tion ( t(38)= .293, p = ns) were found. Chi-square analyses showed no differences be-tween the two groups based on the disciplineof the interventionist (X2(4, N= 41) = 2.36 p= ns).
DISCUSSION
Characteristics of home visits that includeda child-focused intervention activity (asopposed to primarily discussion between theinterventionist and caregiver) were rated
using two different scales to describe char-acteristics of visits and to explore the extentto which different types of service approachescould be distinguished based on these char-acteristics. The Natural Environments RatingScale (NERS) was constructed and itseffectiveness in distinguishing the two typesof services was explored.
The extant literature suggests that earlyintervention services have been providedmost frequently through a traditional modelwhere an interventionist-directed activity isused to provide opportunities for a child tolearn or practice new skills (e.g. Dunst,Trivette et al., 2001). Findings in this studyare consistent with earlier studies. A majority(70%) of the activities videotaped by inter-ventionists in our sample and submitted as&dquo;typical&dquo; were rated as traditional. Ourtraditional services descriptions are compa-rable to descriptions of early interventionhome visits described in previous studies
(McBride & Peterson, 1997; Wilcox &
Lamorey, 2004). In each of these studies,early interventionists were most likely to bedirecting activities with children while care-givers played primary roles as observers. Inthe traditional-rated videotapes in the pres-ent study, the interventionist primarily di-rected the child-focused activity although ina small percentage of instances, intervention-ists used facilitation rather than direction by
joining and following the child’s lead withinthe activity. The HVOF-M codes of directionand facilitation relate specifically to interven-tionist use of these strategies when interact-ing with children. In the present studysample, these strategies were used more
frequently when traditional services were
provided because interventionists had moredirect interaction with children than in
participation-based services. The differencesin the use of direction and facilitation in
videotapes rated as traditional were statisti-cally significant and noteworthy when com-pared to participation-based services.
In all videotapes, the primary interactionpartners were most often a triad of the
caregiver-child-interventionist, but almosta quarter of the coded interactions fortraditional services involved only the inter-ventionist-child (i.e., the caregiver was eithernot present or was present in the room butwas not part of the interaction even in anobserver role). What the caregiver was doingduring the session was reflected under therole of the caregiver category. For the
traditional services group, the caregivers’primary roles were watching and not presentin the interaction. There were statisticallysignificant and noteworthy differences be-tween the traditional and participation-basedgroup across both of these coding categories.A total of 30% of the home visits in our
sample were rated as participation-based. Inthese visits, either the caregiver or the childwas the leader of the activity and theinterventionist supported or actively ob-served the caregiver-child interaction. Theuse of supportive interaction and observationin participation-based services differed sig-nificantly when compared with traditionalservices. The primary interaction partnerswere a triad of the caregiver-child-interven-tionist, but in participation-based services,the caregiver’s primary role was interactingwith the child and this difference was
statistically significant when compared withtraditional services where the caregivers’ rolewas most frequently as an observer. For
categories related to the role of the in-
terventionist and the role of the caregiver,
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from

301
the interactions that typified both participa-tion-based and traditional services were
distinctly different. Participation-based ser-vices reflected use of natural environments asa context for learning opportunities anda primary interventionist role of supportingcaregiver-child interactions.
Based on the findings of this study and thefew others that have examined systematicallywhat occurs during early intervention visits(McBride & Peterson, 1997; Peterson et al.,2007; Wilcox & Lamorey, 2004), it seems clearthat despite a decade or more of emphasis onfamily-centered approaches, use of naturalsettings, and the importance of caregiver-childinteraction, many interventionists are not
applying these concepts within early interven-tion services. The typically used traditionalapproach seems to be in direct opposition torecommended practices. Recommended prac-tices suggest that intervention should be
provided so that providers teach caregivershow to use the activities and routines innatural settings as opportunities for learning(Sandall, Hemmeter, Smith, & McLean, 2005;Stremel & Campbell, 2007.)
In the present study, the NERS andHVOF-M both were able to distinguish thetwo approaches to service delivery. This
finding is noteworthy because the HVOF-Mis a research-based tool that rates four
categories in 30-second intervals and requiressignificant resources for its use. In contrast,the NERS, designed for use with interven-tion-based activities, uses global ratings thatare made following the conclusion of anintervention activity. The HVOF, however,takes a broader perspective of early inter-vention visits and its use is not restricted toactivities with a child intervention focus.
Three major limitations present in this
study should be acknowledged. First, the
sample was a convenience sample of inter-ventionists who were asked to obtain andsubmit a videotape as part of a professionaldevelopment workshop. Interventionists se-lected both the family and the activity theytaped. Neither the families nor the childrenmight have been representative of the inter-ventionist’s caseload or the population of
children in the early intervention system inthe targeted state or in the United States. Forexample, no children under the age of
12 months were included in the sample.Further, although interventionists were
asked to tape an activity (of their choice) of20 min or longer, the length of the activitiesvaried considerably and many were shorterthan 20 min. Although we reported percentinterval data as a way to represent theoccurrence of HVOF coding categoriesacross videotaped activities of varyinglengths, large within-group variability on
the HVOF coding categories was evident.Second, the way in which the taping was
conducted was determined by the interven-tionist and the strategies used to obtain thevideotape varied. In some instances, thecamera was left on, but unattended. Alter-
natively, an individual not usually present atthe home visit did the recording. In otherinstances, a family member (but not the
primary caregiver) took responsibility for
videotaping. The different strategies used tofilm the videotape might have influenced theinteractions that were recorded.
Interventionists submitted only one video-taped example of an intervention activitywith one child/family. Other studies
(McBride & Peterson, 1997; Peterson et al.,2007; Wilcox & Lamorey, 2004) have in-
cluded three or more samples of the sameinterventionist with the same family/child inorder to obtain a more stable and represen-tative picture of interactions. Given thatcertain features of typical visits are likely tovary from visit to visit or that a particularvisit might be influenced by circumstancessuch as family crisis, child progress, child
engagement, or other features, our visits werelikely not more than a one-time view ofa particular child/family and are not likely tohave been representative of interventionistpractices with either the selected child/familyor across children/families with whom anindividual interventionist was working. Toobtain an accurate view of individual in-
terventionist practices, samples would needto include more than one videotaped visitwith more than one family/child.
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from
302
Implications for PracticeDespite noted limitations, distinguishing twotypes of service approaches might be usefulwithin the field of early intervention. Oper-ationalizing practice so interventionists knowwhat they should or should not do duringintervention visits might assist them to trans-late recommended practice principles intotheir interactions with children and families.The NERS, developed as a way to rate theoccurrence of literature-based recommended
practices, might be used by researchers asa measure of fidelity of implementation ofrecommended practices during home visits.Supervisors might use the NERS to identifypractices being used by their staff and to
guide them to better practice. The NERS alsomight be used by early interventionists toidentify the strengths of their interventionand areas that need to be improved. Withthis type of information, interventionists andsupervisors might be able to identify specificareas for professional development. Addi-tionally, interventionists or their supervisorsmight learn that early intervention visitsreflect recommended practices under some,but not under all circumstances. For exam-
ple, interventionists might face challengesimplementing recommended practices withfamilies with particular characteristics, chil-dren with specific types of disabilities, or incertain types of natural settings, such as childcare programs.
Early interventionists have been exposedto a variety of different terms and models ofearly intervention, each of which are basedon recommended practices and family-cen-tered approaches. Two primary componentsof recommended practices are the provider-caregiver-child relationship and the use ofactivities and routines (e.g., activity settings)as sources for both intentional and incidentalchild learning opportunities. The current
recommended models or approaches eachemphasize different aspects of a family-cen-tered approach and no one model or
approach equally addresses all componentsof recommended practice (Stremel & Camp-bell, 2007). For example, coaching (Hanft,Rush, & Shelden, 2004) promotes strategies
for interacting with families, while familyguided routines-based intervention (Woods,2005) provides strategies for identifyingfamily routines and developing routines-based intervention plans.
Despite recommended practices and theirtranslation into various models or ap-
proaches, few families and children appearto be receiving optimal services (e.g., Bruder,2000; Hanson & Bruder, 2001; Dunst, Bruder,Trivette, Hamby et al., 2001). Findings fromthe present study and those conducted byothers related to what interventionists do
during visits illustrate that typical interven-tionist practices often do not match those thatare recommended (McBride & Peterson, 1997;Wilcox & Lamorey, 2004). These studies covera 10-year time span, from 1997 through thepresent, a time period during which homeshave become the primary location for pro-viding early intervention services and signifi-cant time and resources have been directed to
offering professional development in areas
such as provider-caregiver-child interactionsand working within the context of naturalsettings.
Conceptually based models describinggeneral characteristics of early interventionpractice have been prolific in the earlyintervention field as researchers, developers,policymakers, providers, and families havestruggled for over a decade to define andimplement effective practice. Perhaps shiftingfocus to specific features of participation-based services and the contrast of this type ofservice with more traditional services willallow interventionists not only to focus ontheir day-to-day interactions with childrenand families but also to optimize theseinteractions so recommended practices are
regularly used during home visits.
REFERENCES
Axtmann, A., & Dettwiler, A. (2005). The visit:
Observation, reflection, synthesis for trainingand relationship building. Baltimore: Brookes.
Bruder, M. B. (2000). Family-centered earlyintervention: Clarifying our values for thenew millennium. Topics in Early ChildhoodSpecial Education, 20, 105-115.
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from
303
Campbell, P. H. (2004). Participation-based services:Promoting children’s participation in natural
settings. Young Exceptional Children, 8, 20-29.
Campbell, P. H., & Halbert, J. (2002). Betweenresearch and practice: Provider perspectivesabout early intervention. Topics in EarlyChildhood Special Education, 22, 213-226.
Campbell, P. H., & Sawyer, L. Brook (2004).Natural Environments Rating Scale. Availablefrom Child & Family Studies Research
Programs, Thomas Jefferson University, Phi-ladelphia, PA.
Chai, A. Y., Zhang, C., & Bisberg (2006).Rethinking natural environment practice: Im-plications from examining various interpreta-tions and approaches. Early Childhood Edu-cation Journal, 34, 203-208.
Code of Federal Regulations, 34 CFR 303.18, July1, 1999.
Cohen, J. (1988). Statistical power analysis for thebehavioral sciences (2nd ed.). Hillsdale, NJ:Lawrence Earlbaum Associates.
Cripe, J. W., Hanline, M. F., & Daley, S. E.
(1997). Family-guided routines for early in-tervention services. Young Exceptional Chil-dren, 1, 18-26.
Dunst, C. J. (2000). Everyday children’s learningopportunities: Characteristics and conse-
quences. Children’s Learning OpportunitiesReport, 2(1), 1-2.
Dunst, C. J. (2001). Participation of youngchildren with disabilities in community learn-ing activities. In M. J. Guralnick (Ed.). Earlychildhood inclusion: Focus on change (pp. 307-333). Baltimore: Brookes.
Dunst, C. J., & Bruder, M. B. ( 1999). Family andcommunity activity settings, natural learningenvironments, and children’s learning oppor-tunities. Children’s Learning Opportunity Re-port, 1(2), 1-2.
Dunst, C. J., Bruder, M. B., Trivette, C. M.,Hamby, D., Raab, M., & McLean, M. (2001).Characteristics and consequences of everydaynatural learning opportunities. Topics in EarlyChildhood Special Education, 21, 68-92.
Dunst, C. J., Bruder, M. B., Trivette, Raab, M., &McLean, M. (2001). Natural learning oppor-tunities for infants, toddlers, and preschoo-lers. Young Exceptional Children, 4, 18-25.
Dunst, C. J., Hamby, D., Trivette, C. M., Raab,M. , & Bruder, M. B. (2000). Everyday familyand community life and children’s naturallyoccurring learning opportunities. Journal ofEarly Intervention, 23, 151-164.
Dunst, C. J., Herter, S., & Shields, H. (2000).Interest-based natural learning opportunities.
Young Exceptional Children Monograph Se-ries, 2, 37-48.
Dunst, C. J., Trivette, C. M., Humphries, T.,Raab, M., & Roper, N. (2001). Contrastingapproaches to natural learning environmentinterventions. Infants and Young Children, 14,48-63.
Edelman, L. (2004). Principles and strategies for
family-centered home based visits. Resources andConnections, 3(1), 1-6. Retrieved June 30, 2007,from http://www.earlychildhoodconnections.org/files/home based services.pdf
Hanft, B., Rush, D., & Shelden, M. (2004).Coaching families and colleagues in earlychildhood. Baltimore: Brookes.
Hanson, M. J., & Bruder, M. B. (2001). Earlyintervention: Promises to keep. Infants andYoung Children, 13(3), 47-58.
Klass, C. S. (2003). The home visitor’s guidebook:Promoting optimal caregiver and child devel-opment (2nd ed.). Baltimore: Brookes.
McBride, S., & Peterson, C. (1997). Home-basedintervention with families of children withdisabilities: Who is doing what? Topics inEarly Childhood Special Education, 17,209-233.
McWilliam, R. A. (2000). Its only natural — to
have early intervention in the environmentswhere it is needed. Young Exceptional Chil-dren Monograph Series, 2, 17-26.
McWilliam, R. A. (2005). Early intervention innatural environments. Retrieved August 22,2005, from Vanderbilt University Web site:
http://www.vanderbiltchildrens.com/interior.php?mid=1218
Mc William, R. A., & Scott, S. (2001). A supportapproach to early intervention: A three-partframework. Infants and Young Children, 13(4),55-66.
Peterson, C. A., Luze, G. J., Eshbaugh, E. M.,Jeon, H-J., & Kantz, K. R. (2007). Enhancingparent-child interactions through home visit-ing : Promising practice or unfulfilled promise.Journal of Early Intervention, 29, 119-140.
Pretti-Frontczak, K., & Bricker, D. (2004). Anactivity-based approach to early intervention
(3rd ed.). Baltimore: Brookes.
Rosenthal, R., & Rosnow, R. L. (1991). Essentialsof behavioral research: Methods and data
analysis (2nd ed.). New York: McGraw-Hill.
Sandall, S., Hemmeter, M. L., Smith, B., &
McLean, M. (2005). DEC recommendedpractices: A comprehensive guide for practicalapplication in early interventionlearly childhoodspecial education. Longmont, CO: SoprisWest.
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from
304
Stremel, K., & Campbell, P. H. (2007). Imple-mentation of early intervention within naturalenvironments. Early Childhood Services: AnInterdisciplinary Journal of Effectiveness, 1(2),83-105.
U.S. Department of Education, Office of SpecialEducation Programs. (2003). Data analysissystem (DANS) percentage of Part C infantsand toddlers served in the home and in
programs for typically developing children,1994, 1997, 2000. Retrieved on August1, 2005 from http://www.ideadata.org/PartCDataMeeting2003.asp.
U.S. Department of Education, Office of SpecialEducation Programs. (2004). IDEA Part Cprogram settings (2004). Retrieved on Decem-ber 1, 2006 from https://www.ideadata.org/arc_toc7.asp#partcEIS.
Valvano, J. (2004). Activity-focused motor inter-ventions for children with neurological con-ditions. Physical and Occupational Therapy inPediatrics, 24(12), 79-107.
Washington, K., Schwartz, I., & Swinth, Y.
(1994). Physical and occupational therapistsin naturalistic early childhood settings: Chal-lenges and strategies for training. Topics in
Early Childhood Special Education, 14,333-349.
Wasik, B. H., Bryant, D., & Lyons, C. M. (1990).Home visiting: Procedures for helping families.Thousand Oaks, CA: Sage.
Wilcox, M. J., & Lamorey, S. (October 1, 2004).Relationship-based practice in early interven-tion settings: The experimental investigation ofimpact and effectiveness: Final report. U. S
Department of Education, Field-Initiated Re-search R305T00049.
Wilcox, M. J., Campbell, P. H., & Lamorey, S.
(2006, February). Home visiting in earlyintervention: What happens and what does itmean for families and children? Paper pre-sented at the CRIEI Conference, San Diego,California.
Woods, J. (2005). Family guided routines-basedintervention. Retrieved August 15, 2005, fromFlorida State University, Family-GuidedRoutines- Based Intervention Project Website: http://fgrbi.fsu.edu
Woods, J., Kashinath, S., & Goldstein, H. (2004).Effects of embedding caregiver-implementedteaching strategies in daily routines on chil-dren’s communication outcomes. Journal ofEarly Intervention, 26, 195-193.
Address correspondence to Philippa Campbell, 5thfloor, Edison, 130 S. 9th St., Philadelphia, PA19107. E-mail: pipcamp@aol. com. or [email protected]
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from
305
Appendix ANatural Environments Rating Scale
by Philippa Campbell on October 20, 2010jei.sagepub.comDownloaded from