JOURNAL ARTICLES
77
JOURNAL CLUB DR.PRAVEEN NAGULA
-
Upload
praveen-nagula -
Category
Education
-
view
159 -
download
0
Transcript of JOURNAL ARTICLES

JOURNAL CLUB
DRPRAVEEN NAGULA
Contents
1Valvular Heart Disease In India
2ESH PRACTICE GUIDELINES for ABPM
3BAT (BAROREFLEX ACTIVATION THERAPY)
4ECG Challenge
5PREVAIL Trial
6Update on PCSK9 Inhibitors
7Abstracts
2
Indian Heart JournalJuly 2014 3
Background
Diseases of the heart valves constitute a major cause of
cardiovascular morbidity and mortality worldwide with rheumatic
heart disease (RHD) being the dominant form of valvular heart
disease (VHD) in developing nations
The current study was undertaken at a tertiary care cardiac center with
the objective of establishing the incidence and patterns of VHD by
Echocardiography (Echo)
4
Among the 136098 first-time Echocardiograms performed
between January 2010 and December 2012 an exclusion
criterion of trivial and functional regurgitant lesionsyielded a
total of 13289 cases of organic valvular heart disease as the
study cohort
5
6
In RHD the order of involvement of valves was mitral (602)
followed by aortic tricuspid and pulmonary valves
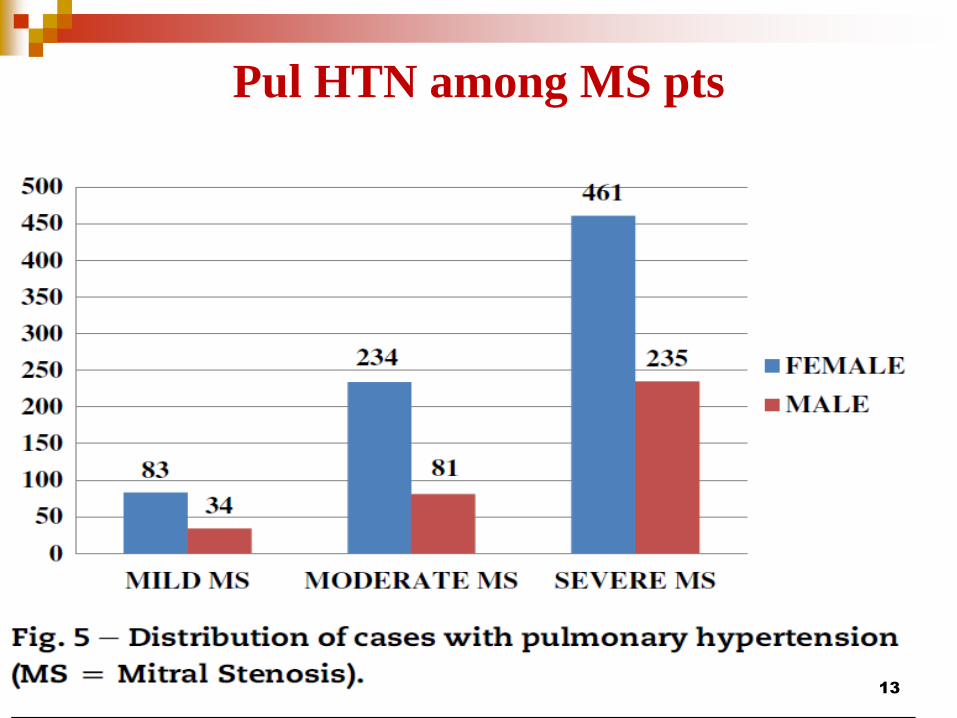
Mitral stenosis predominantly seen in females was almost
exclusively of rheumatic etiology (974)
The predominant form of isolated MR was rheumatic (411)
followed closely by myxomatous or mitral valve prolapse (408)
Isolated AS more common in males was the third most common
valve lesion seen in 73 of cases Degenerative calcification was
the commonest cause of isolated AS (650) followed by bicuspid
aortic valve (BAV) (339) and RHD (11)7
Multiple valves were involved in more than a third of all
cases (368) The order of involvement was
MS MR gt MS AR gt MR AR gt AS AR gt MR AS
gt MS AS
Overall 97 of cases had organic tricuspid valve disease
8
9
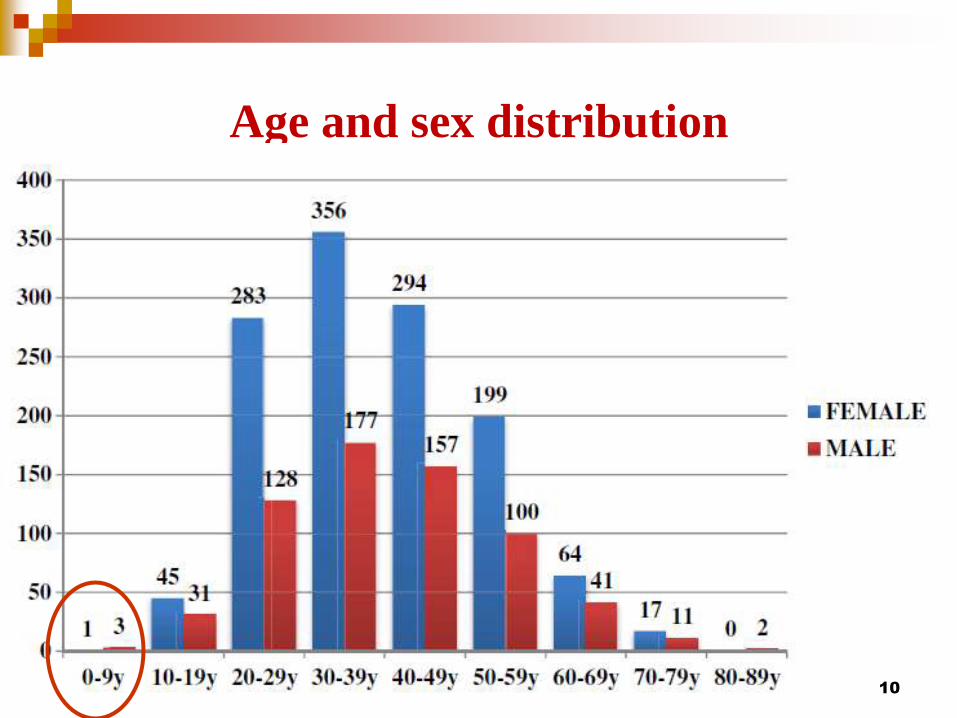
Age and sex distribution
10
11
Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Contents
1Valvular Heart Disease In India
2ESH PRACTICE GUIDELINES for ABPM
3BAT (BAROREFLEX ACTIVATION THERAPY)
4ECG Challenge
5PREVAIL Trial
6Update on PCSK9 Inhibitors
7Abstracts
2
Indian Heart JournalJuly 2014 3
Background
Diseases of the heart valves constitute a major cause of
cardiovascular morbidity and mortality worldwide with rheumatic
heart disease (RHD) being the dominant form of valvular heart
disease (VHD) in developing nations
The current study was undertaken at a tertiary care cardiac center with
the objective of establishing the incidence and patterns of VHD by
Echocardiography (Echo)
4
Among the 136098 first-time Echocardiograms performed
between January 2010 and December 2012 an exclusion
criterion of trivial and functional regurgitant lesionsyielded a
total of 13289 cases of organic valvular heart disease as the
study cohort
5
6
In RHD the order of involvement of valves was mitral (602)
followed by aortic tricuspid and pulmonary valves
Mitral stenosis predominantly seen in females was almost
exclusively of rheumatic etiology (974)
The predominant form of isolated MR was rheumatic (411)
followed closely by myxomatous or mitral valve prolapse (408)
Isolated AS more common in males was the third most common
valve lesion seen in 73 of cases Degenerative calcification was
the commonest cause of isolated AS (650) followed by bicuspid
aortic valve (BAV) (339) and RHD (11)7
Multiple valves were involved in more than a third of all
cases (368) The order of involvement was
MS MR gt MS AR gt MR AR gt AS AR gt MR AS
gt MS AS
Overall 97 of cases had organic tricuspid valve disease
8
9
Age and sex distribution
10
11
Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
Indian Heart JournalJuly 2014 3
Background
Diseases of the heart valves constitute a major cause of
cardiovascular morbidity and mortality worldwide with rheumatic
heart disease (RHD) being the dominant form of valvular heart
disease (VHD) in developing nations
The current study was undertaken at a tertiary care cardiac center with
the objective of establishing the incidence and patterns of VHD by
Echocardiography (Echo)
4
Among the 136098 first-time Echocardiograms performed
between January 2010 and December 2012 an exclusion
criterion of trivial and functional regurgitant lesionsyielded a
total of 13289 cases of organic valvular heart disease as the
study cohort
5
6
In RHD the order of involvement of valves was mitral (602)
followed by aortic tricuspid and pulmonary valves
Mitral stenosis predominantly seen in females was almost
exclusively of rheumatic etiology (974)
The predominant form of isolated MR was rheumatic (411)
followed closely by myxomatous or mitral valve prolapse (408)
Isolated AS more common in males was the third most common
valve lesion seen in 73 of cases Degenerative calcification was
the commonest cause of isolated AS (650) followed by bicuspid
aortic valve (BAV) (339) and RHD (11)7
Multiple valves were involved in more than a third of all
cases (368) The order of involvement was
MS MR gt MS AR gt MR AR gt AS AR gt MR AS
gt MS AS
Overall 97 of cases had organic tricuspid valve disease
8
9
Age and sex distribution
10
11
Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
Background
Diseases of the heart valves constitute a major cause of
cardiovascular morbidity and mortality worldwide with rheumatic
heart disease (RHD) being the dominant form of valvular heart
disease (VHD) in developing nations
The current study was undertaken at a tertiary care cardiac center with
the objective of establishing the incidence and patterns of VHD by
Echocardiography (Echo)
4
Among the 136098 first-time Echocardiograms performed
between January 2010 and December 2012 an exclusion
criterion of trivial and functional regurgitant lesionsyielded a
total of 13289 cases of organic valvular heart disease as the
study cohort
5
6
In RHD the order of involvement of valves was mitral (602)
followed by aortic tricuspid and pulmonary valves
Mitral stenosis predominantly seen in females was almost
exclusively of rheumatic etiology (974)
The predominant form of isolated MR was rheumatic (411)
followed closely by myxomatous or mitral valve prolapse (408)
Isolated AS more common in males was the third most common
valve lesion seen in 73 of cases Degenerative calcification was
the commonest cause of isolated AS (650) followed by bicuspid
aortic valve (BAV) (339) and RHD (11)7
Multiple valves were involved in more than a third of all
cases (368) The order of involvement was
MS MR gt MS AR gt MR AR gt AS AR gt MR AS
gt MS AS
Overall 97 of cases had organic tricuspid valve disease
8
9
Age and sex distribution
10
11
Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Among the 136098 first-time Echocardiograms performed
between January 2010 and December 2012 an exclusion
criterion of trivial and functional regurgitant lesionsyielded a
total of 13289 cases of organic valvular heart disease as the
study cohort
5
6
In RHD the order of involvement of valves was mitral (602)
followed by aortic tricuspid and pulmonary valves
Mitral stenosis predominantly seen in females was almost
exclusively of rheumatic etiology (974)
The predominant form of isolated MR was rheumatic (411)
followed closely by myxomatous or mitral valve prolapse (408)
Isolated AS more common in males was the third most common
valve lesion seen in 73 of cases Degenerative calcification was
the commonest cause of isolated AS (650) followed by bicuspid
aortic valve (BAV) (339) and RHD (11)7
Multiple valves were involved in more than a third of all
cases (368) The order of involvement was
MS MR gt MS AR gt MR AR gt AS AR gt MR AS
gt MS AS
Overall 97 of cases had organic tricuspid valve disease
8
9
Age and sex distribution
10
11
Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

6
In RHD the order of involvement of valves was mitral (602)
followed by aortic tricuspid and pulmonary valves
Mitral stenosis predominantly seen in females was almost
exclusively of rheumatic etiology (974)
The predominant form of isolated MR was rheumatic (411)
followed closely by myxomatous or mitral valve prolapse (408)
Isolated AS more common in males was the third most common
valve lesion seen in 73 of cases Degenerative calcification was
the commonest cause of isolated AS (650) followed by bicuspid
aortic valve (BAV) (339) and RHD (11)7
Multiple valves were involved in more than a third of all
cases (368) The order of involvement was
MS MR gt MS AR gt MR AR gt AS AR gt MR AS
gt MS AS
Overall 97 of cases had organic tricuspid valve disease
8
9
Age and sex distribution
10
11
Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

In RHD the order of involvement of valves was mitral (602)
followed by aortic tricuspid and pulmonary valves
Mitral stenosis predominantly seen in females was almost
exclusively of rheumatic etiology (974)
The predominant form of isolated MR was rheumatic (411)
followed closely by myxomatous or mitral valve prolapse (408)
Isolated AS more common in males was the third most common
valve lesion seen in 73 of cases Degenerative calcification was
the commonest cause of isolated AS (650) followed by bicuspid
aortic valve (BAV) (339) and RHD (11)7
Multiple valves were involved in more than a third of all
cases (368) The order of involvement was
MS MR gt MS AR gt MR AR gt AS AR gt MR AS
gt MS AS
Overall 97 of cases had organic tricuspid valve disease
8
9
Age and sex distribution
10
11
Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Multiple valves were involved in more than a third of all
cases (368) The order of involvement was
MS MR gt MS AR gt MR AR gt AS AR gt MR AS
gt MS AS
Overall 97 of cases had organic tricuspid valve disease
8
9
Age and sex distribution
10
11
Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

9
Age and sex distribution
10
11
Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
Age and sex distribution
10
11
Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

11
Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Mitral stenosis
12
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
Pul HTN among MS pts
13
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
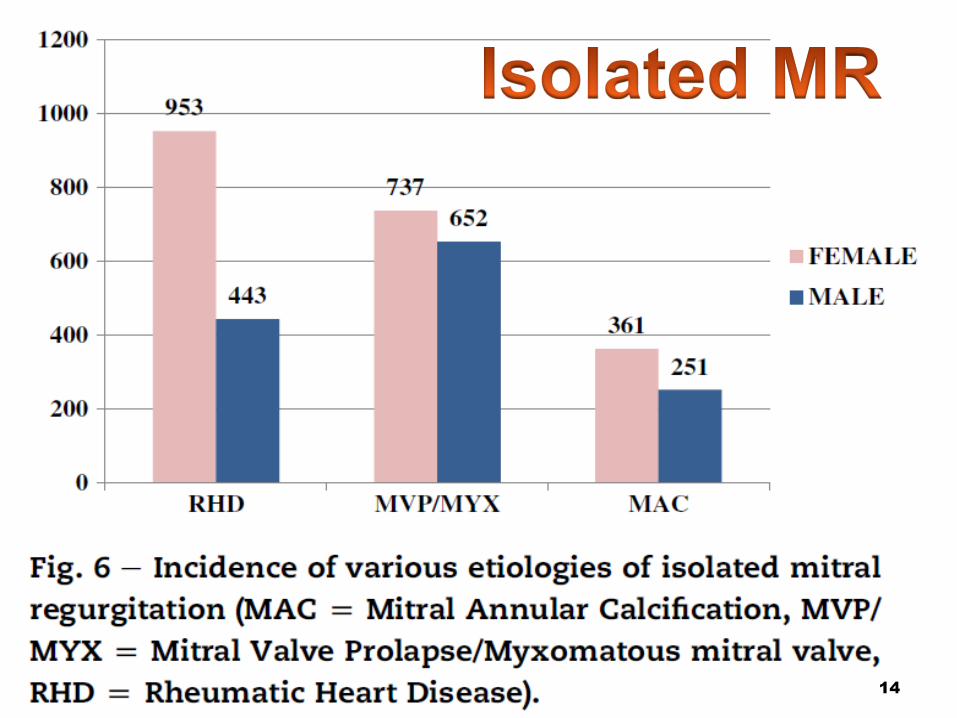
14
15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

15
Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Most common is MS+MR (AS +MR ndash Euro Heart Survey )
Least combination was that of MS +AS
Multivalvular disease was seen more in Females (121)
Lesion combinations involving MS were common in females
while all AS combinations were in males
MR+AR gt MS + AR - paediatric age groups (reverse in Adults)
In RHDthe combinations were hellip
VALVE LESION
COMBINATION
PROPORTION OF
CASES
MS +MR (466)
MS +AR (265)
MR +AR (233)
AS +AR (24)
MR +AS (09)
MS+AS (03) 16
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
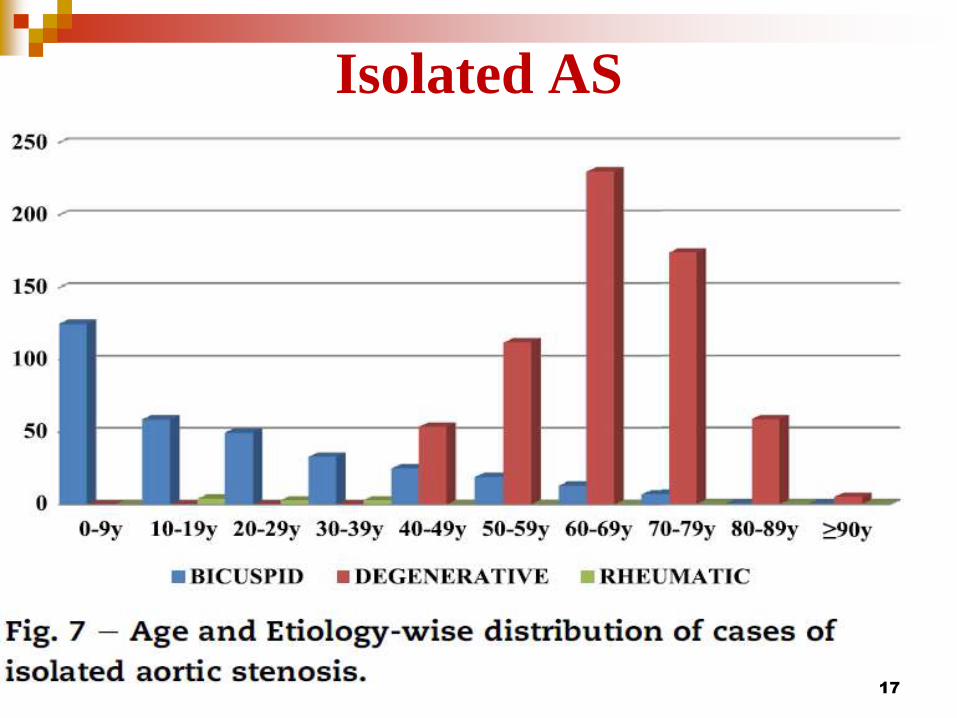
Isolated AS
17
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
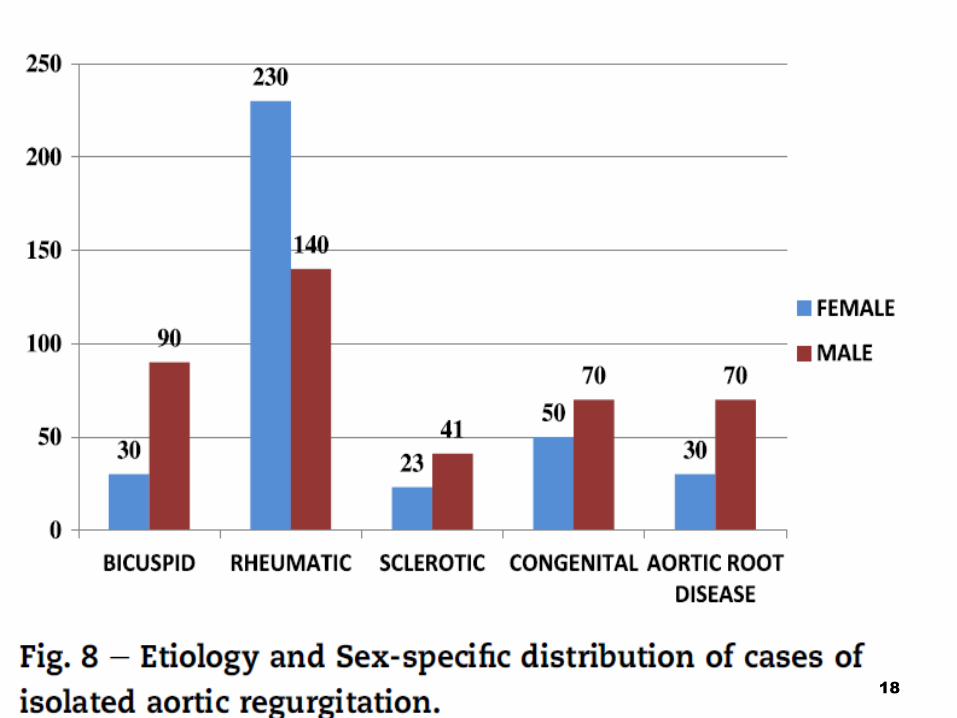
18
19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

19
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
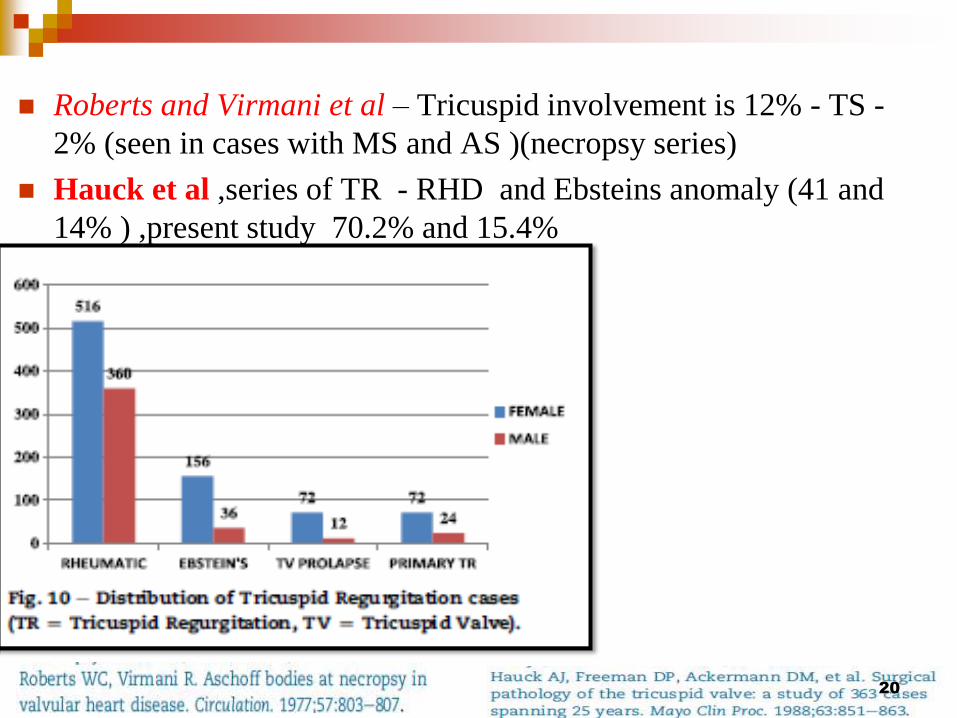
Roberts and Virmani et al ndash Tricuspid involvement is 12 - TS -
2 (seen in cases with MS and AS )(necropsy series)
Hauck et al series of TR - RHD and Ebsteins anomaly (41 and
14 ) present study 702 and 154
20
Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Conclusion
RHD contributed most to the burden of VHD in the present
study with calcific degeneration myxomatous disease and BAV
being the other major forms of VHD
Multiple valves were affected in more than a third of all cases
21
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
EUROPEAN SOCIETY OF HYPERTENSION PRACTICE GUIDELINES FOR AMBULATORY BLOOD PRESSURE MONITORING
GParati et alJ Hypertension 2014321359-1366
Consensus document 22
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
Introduction
Blood Pressure (BP) varies widely through a 24 hr period
Ambulatory blood pressure monitoring (ABPM) involves
measuring BP at regular intervals(usually every 20-30 min)over a
24 hr period while patients undergo normal daily activities
including sleep
Accuracy validated over all ages
23
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
How came the idea of ABPM
Blood pressure is a highly dynamic parameter with continuous
fluctuations having both short term and long term variability
Short term variability within 24 hrs can be readily assessed by
ABPM
Long term variability- BP measurements over daysweeksor
months with repeated measurements of officeHBPMABPM
Short term variability can be considered for risk stratification
Not a parameter for routine use in clinical practice
24
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
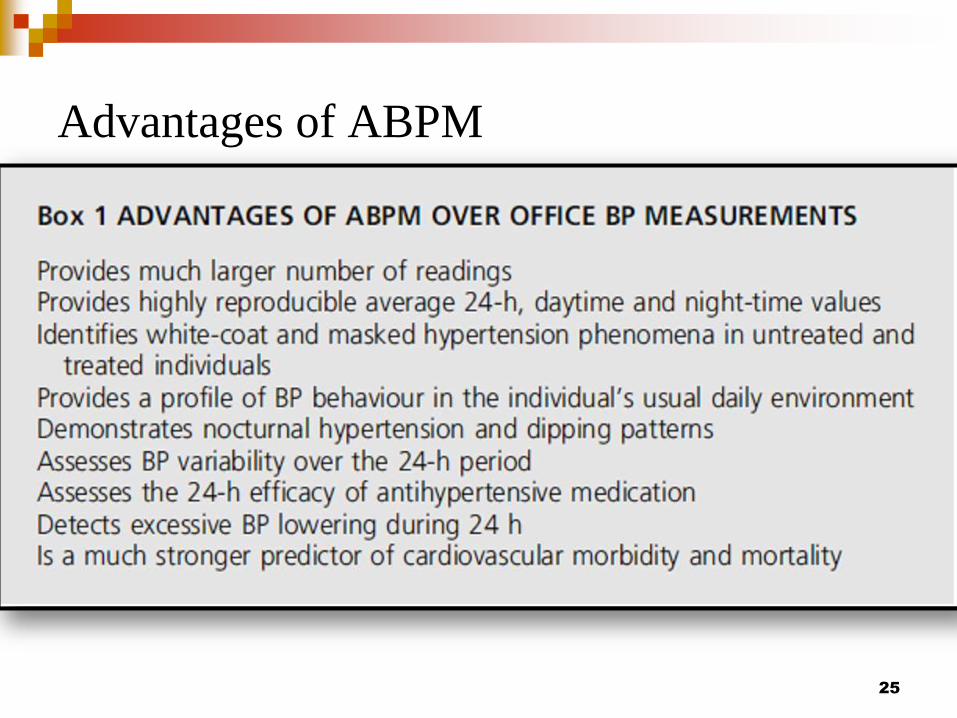
Advantages of ABPM
25
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
Why these guidelines
ESH 2013 ABPM position paper
Evidence from over 600 papers34 international experts in
HTN(Milan2011)
Reference source for ABPM(obviously)
Main conclusions that are directly relevant to clinical practice
are presented and updated
26
Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Questions addressed hellip
Which patients should have ABPM
How to apply and interpret ABPM in daily practice
How to introduce an ABPM serivce in routine clinical
practice
27
Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Indications
1white coat HTN in untreated patients (most well established
indication)
2identify varying 24 hr BP profiles
3identify masked HTN
4assessment of treatment efficacy
28
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
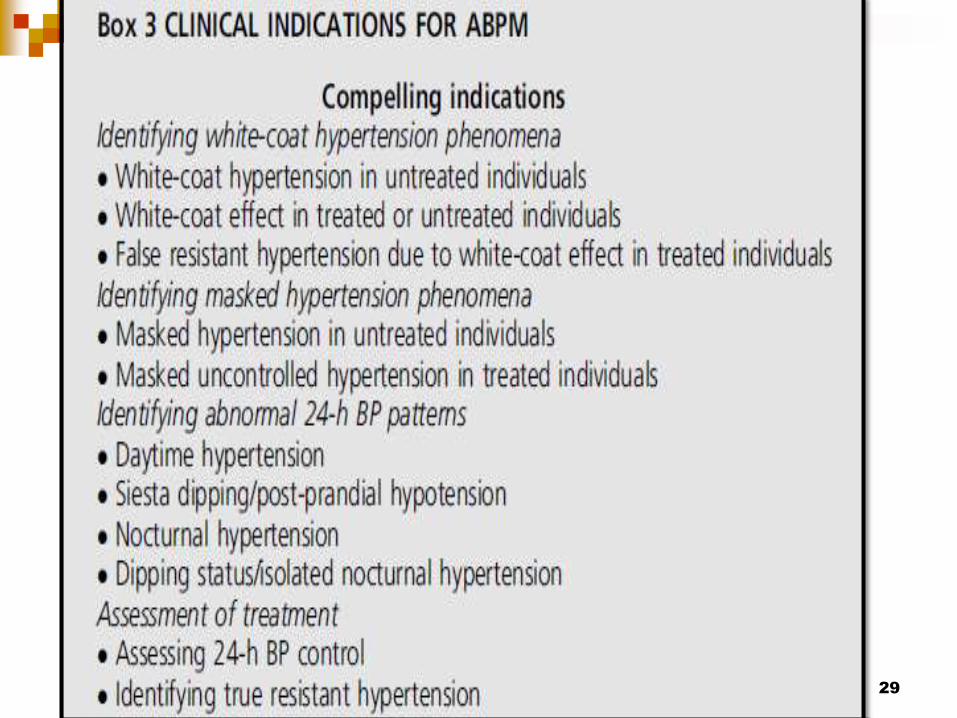
29
30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

30
Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Definition of white coat hypertension
31
Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Masked HTN Masked uncontrolled HTN
32
33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

33
Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Fall of Nocturnal
SBPDBP
Ratio of
nightday
SBPDBP
Remarks
DIPPING gt10 lt20 gt08 lt 09 Normal
REDUCED
DIPPING1-10 gt09 lt 10 Increased CV risk
NON DIPPING
RAISINGIncrease in BP ge1 Increased CV risk
EXTREME
DIPPINGgt20 lt08 debatable
NOCTURNAL
HTNgt12070mm Hg
34
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
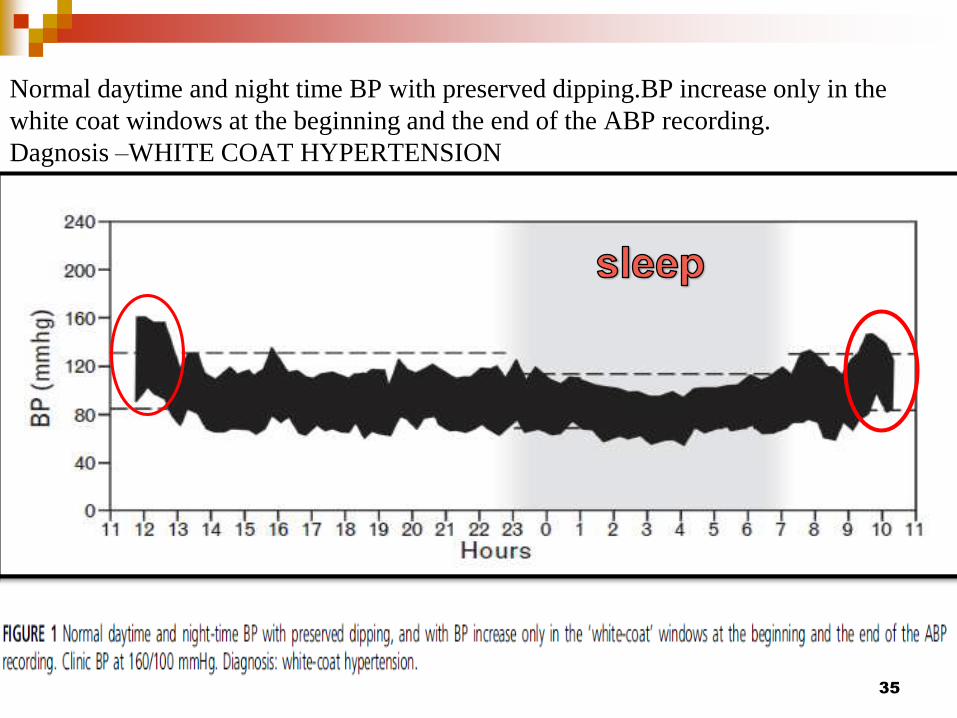
Normal daytime and night time BP with preserved dippingBP increase only in the
white coat windows at the beginning and the end of the ABP recording
Dagnosis ndashWHITE COAT HYPERTENSION
35
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
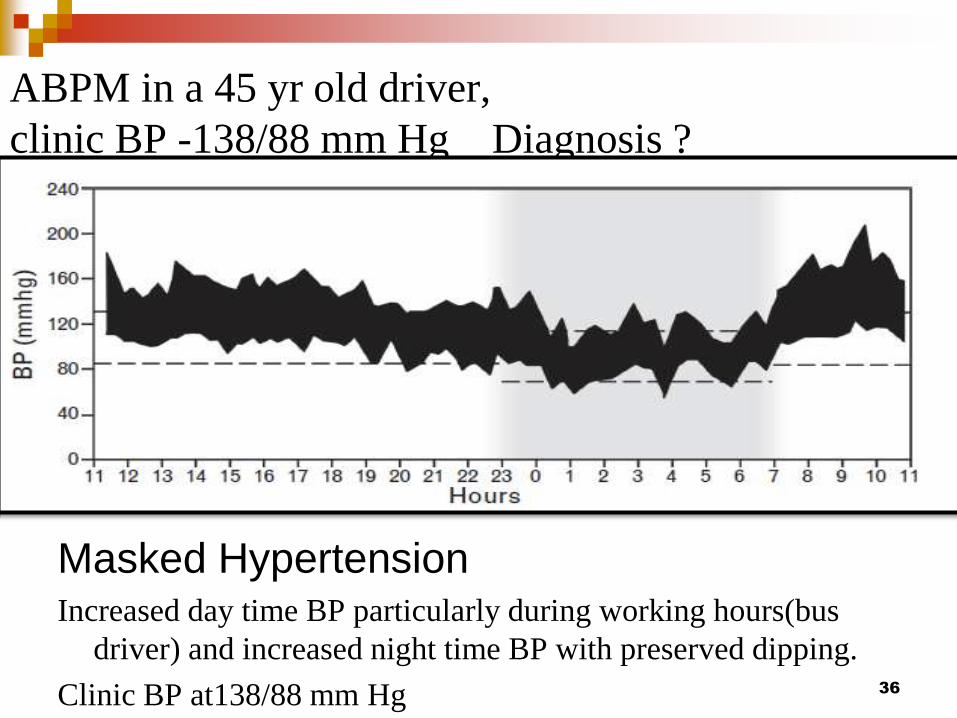
ABPM in a 45 yr old driver
clinic BP -13888 mm Hg Diagnosis
Masked HypertensionIncreased day time BP particularly during working hours(bus
driver) and increased night time BP with preserved dipping
Clinic BP at13888 mm Hg 36
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
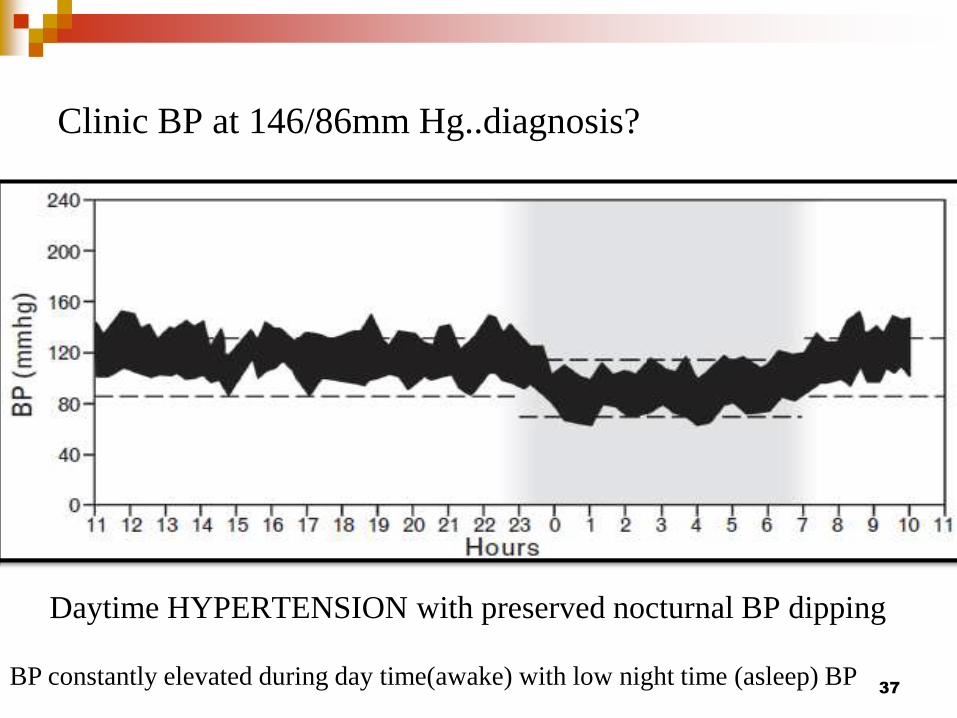
Clinic BP at 14686mm Hgdiagnosis
Daytime HYPERTENSION with preserved nocturnal BP dipping
BP constantly elevated during day time(awake) with low night time (asleep) BP37
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
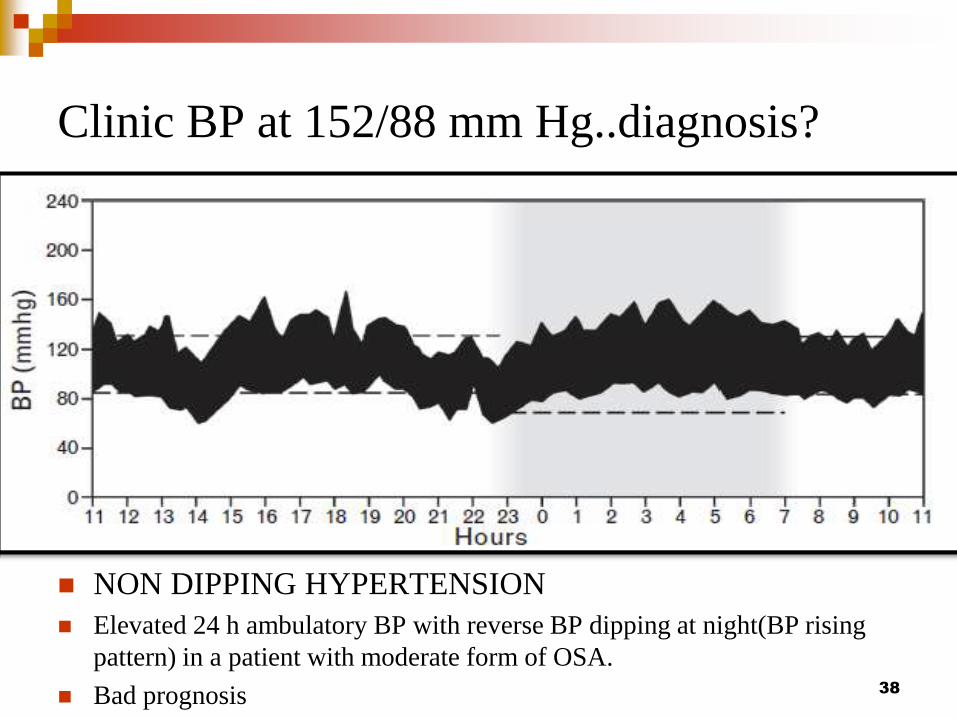
Clinic BP at 15288 mm Hgdiagnosis
NON DIPPING HYPERTENSION
Elevated 24 h ambulatory BP with reverse BP dipping at night(BP rising
pattern) in a patient with moderate form of OSA
Bad prognosis 38
39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

39
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
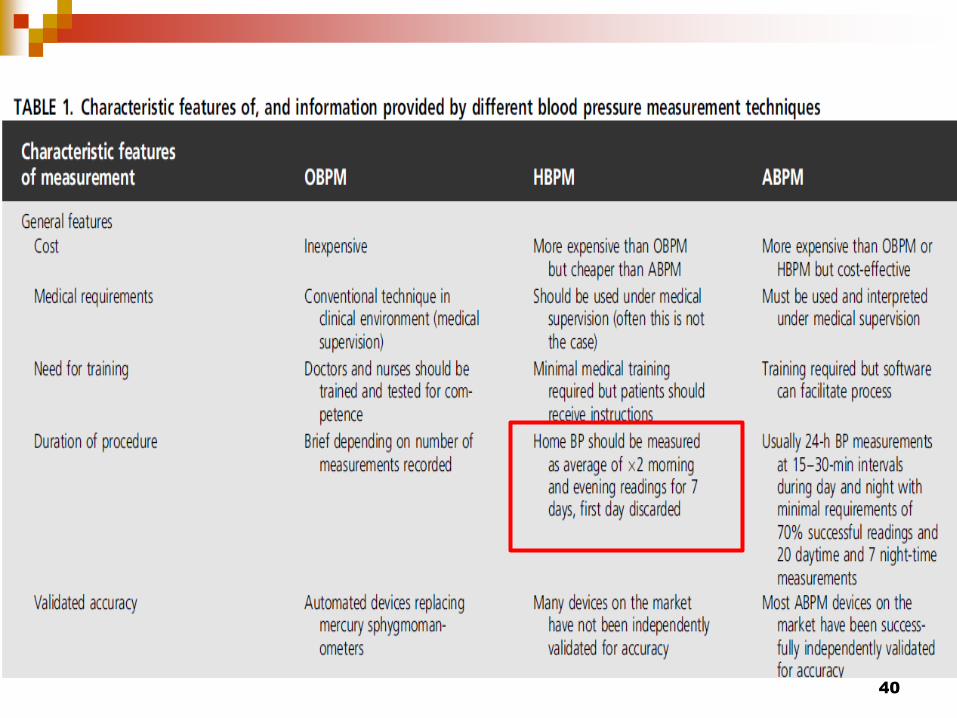
40
41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

41
42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

42
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
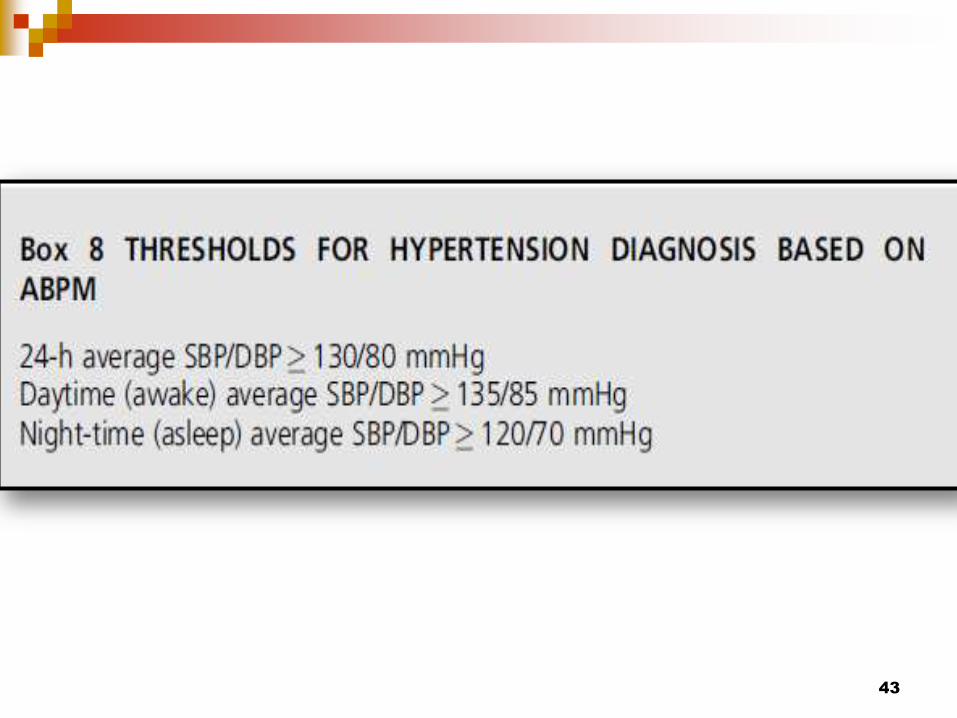
43
44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

44
45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

45
46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

46
Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Welch Allyn ABPM 6100 Demonstrationmp4
Wearing a 24 hour blood pressure
monitor[12]mp4
47
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
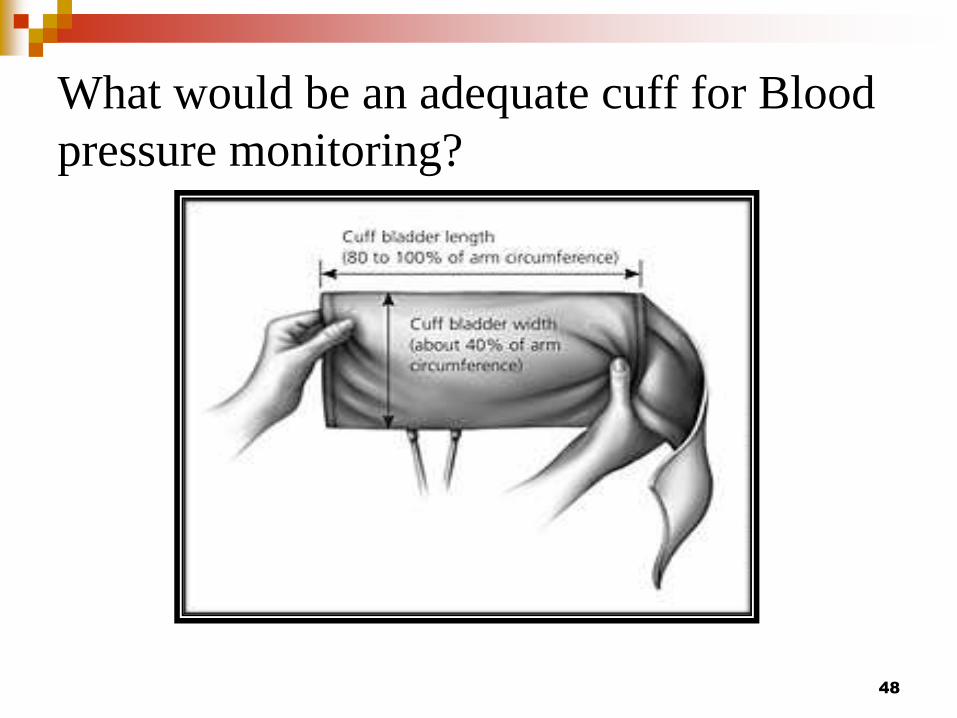
What would be an adequate cuff for Blood
pressure monitoring
48
BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

BP cuff sizes in children
49
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
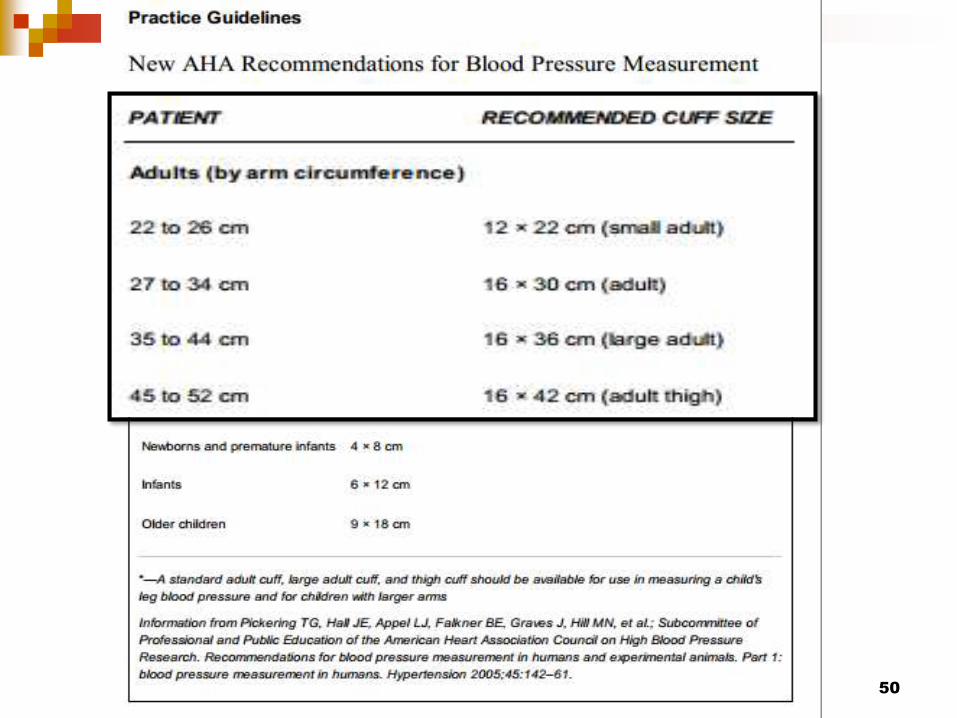
50
BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

BAROREFLEX ACTIVATION THERAPY
Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Baroreflex activation therapy
52
53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

53
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
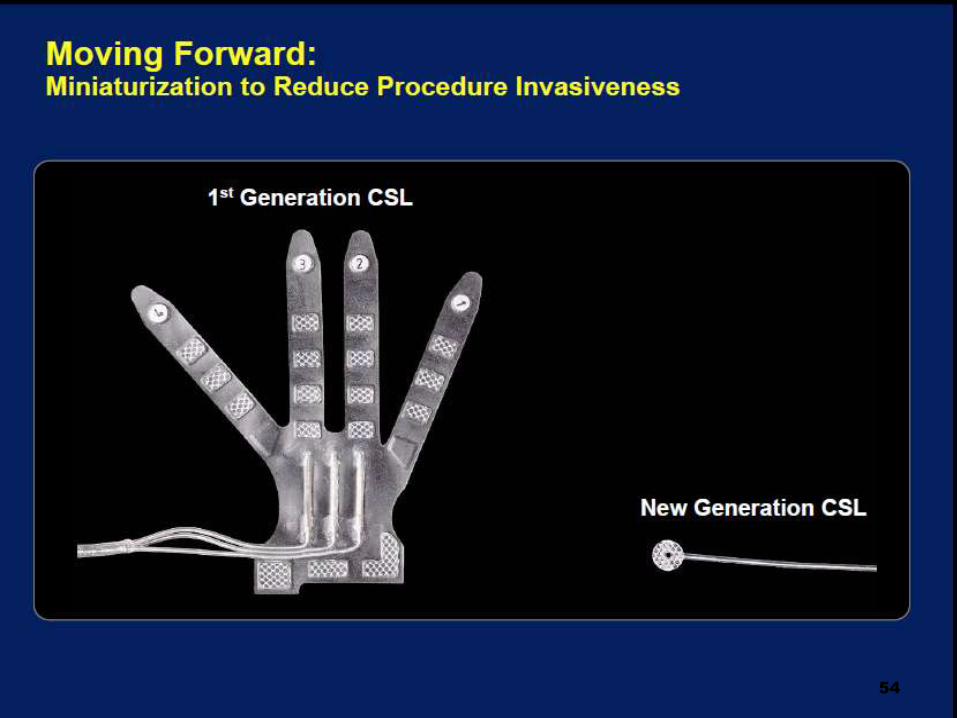
54
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
Barostim neo videomp4
55
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
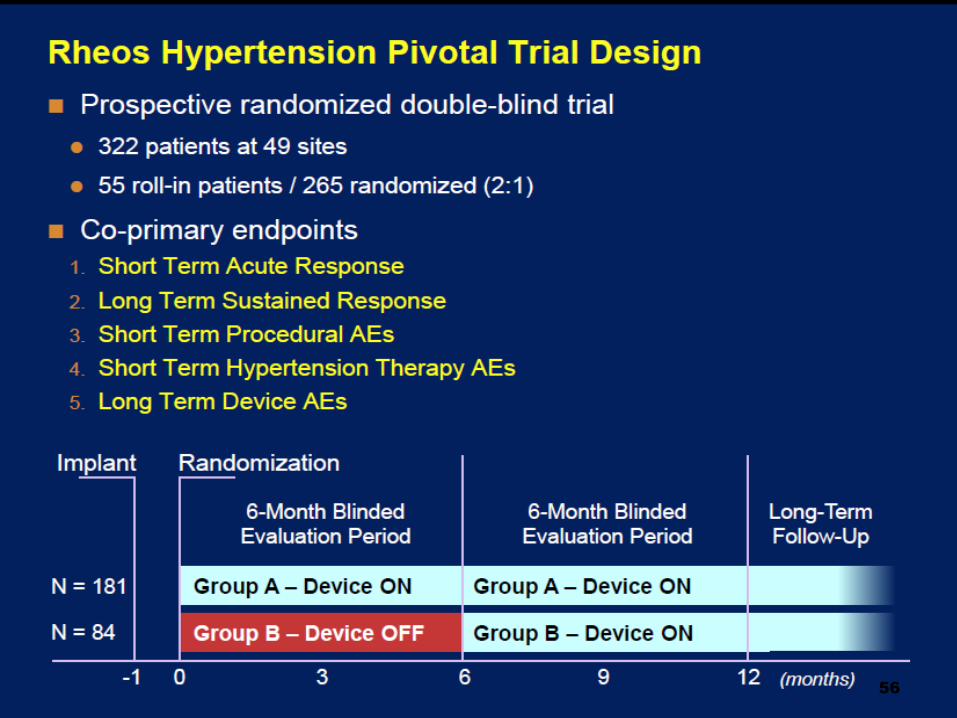
56
57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

57
58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

58
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
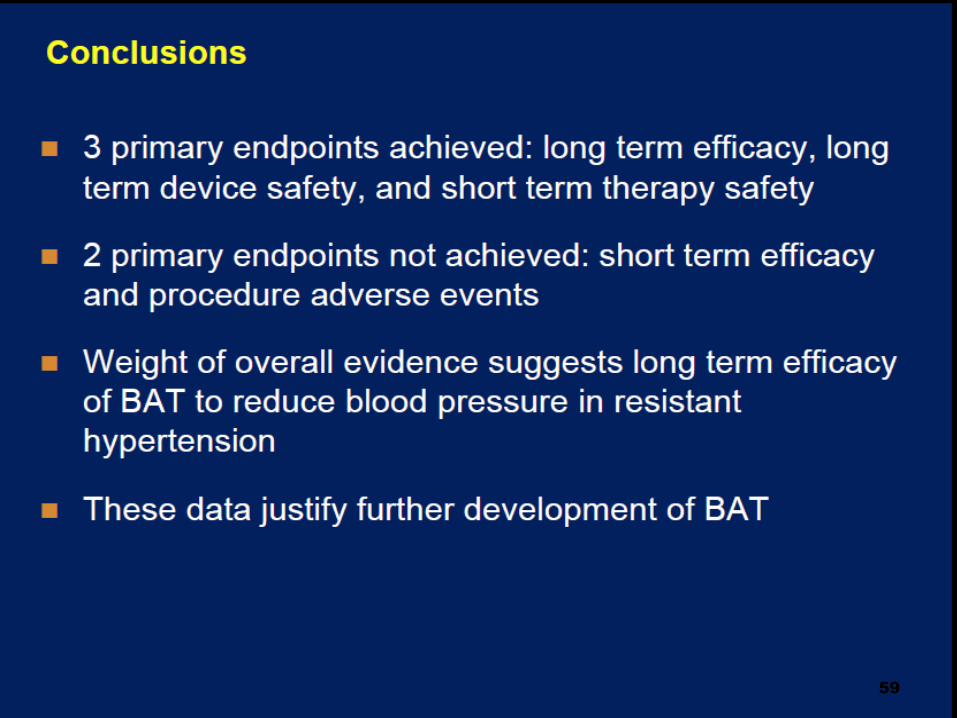
59
ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

ECG CHALLENGE
61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

61
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
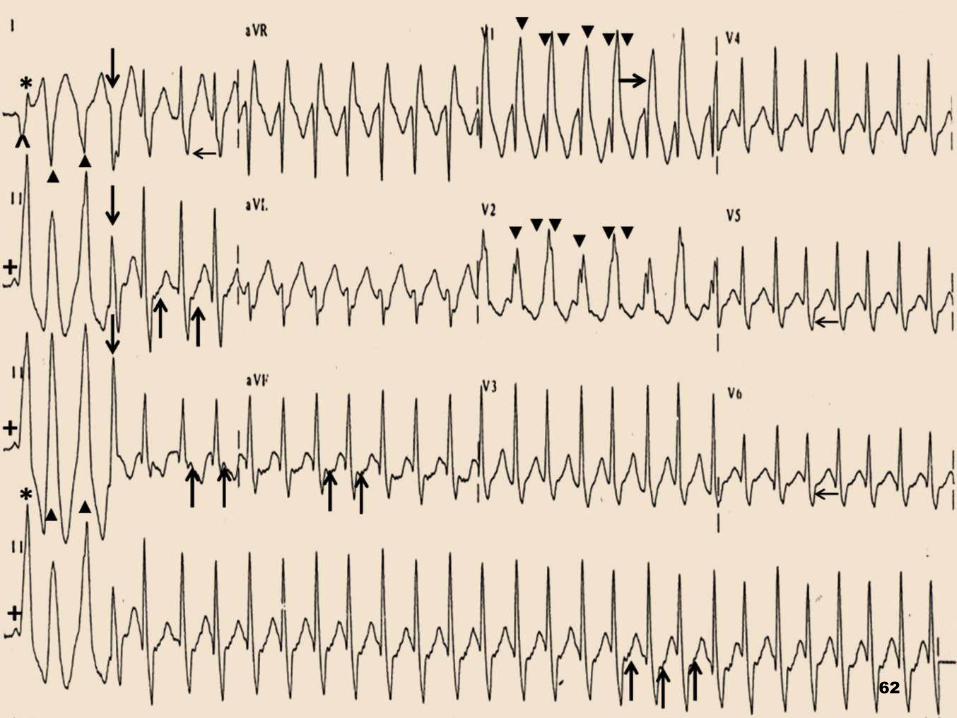
62
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
Supraventricular tachycardia
WPW syndromeLeft lateral pathway
AVRT orthodromic
QRS alternans
63
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
64
65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

65
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
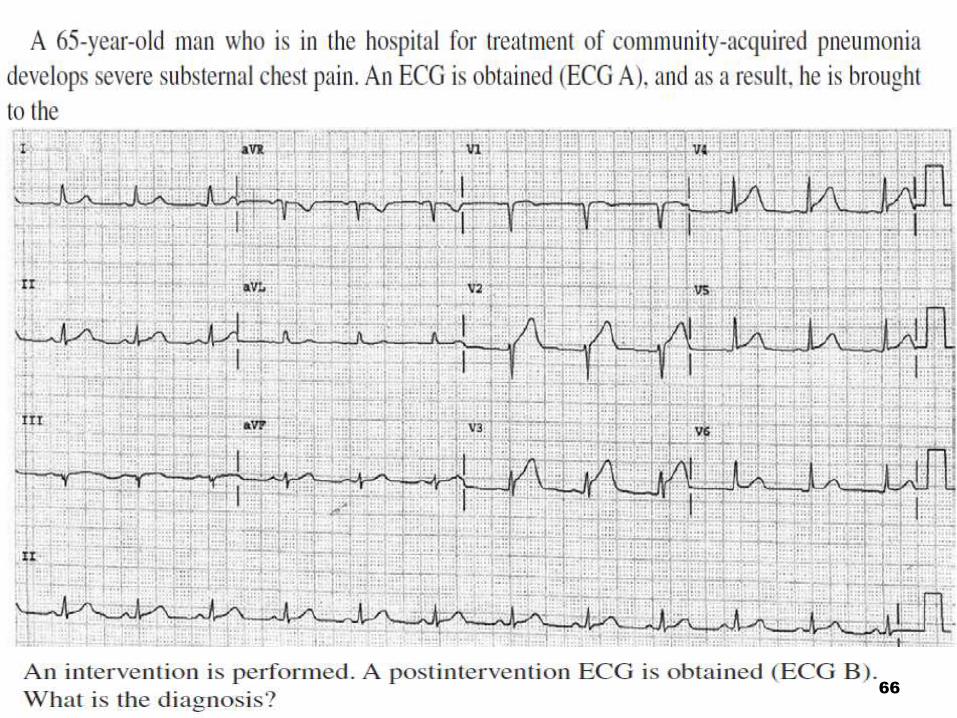
66
67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

67
Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

Acute evolving anterior transmural MI
Post Thrombolysis ndash AIVR
68
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
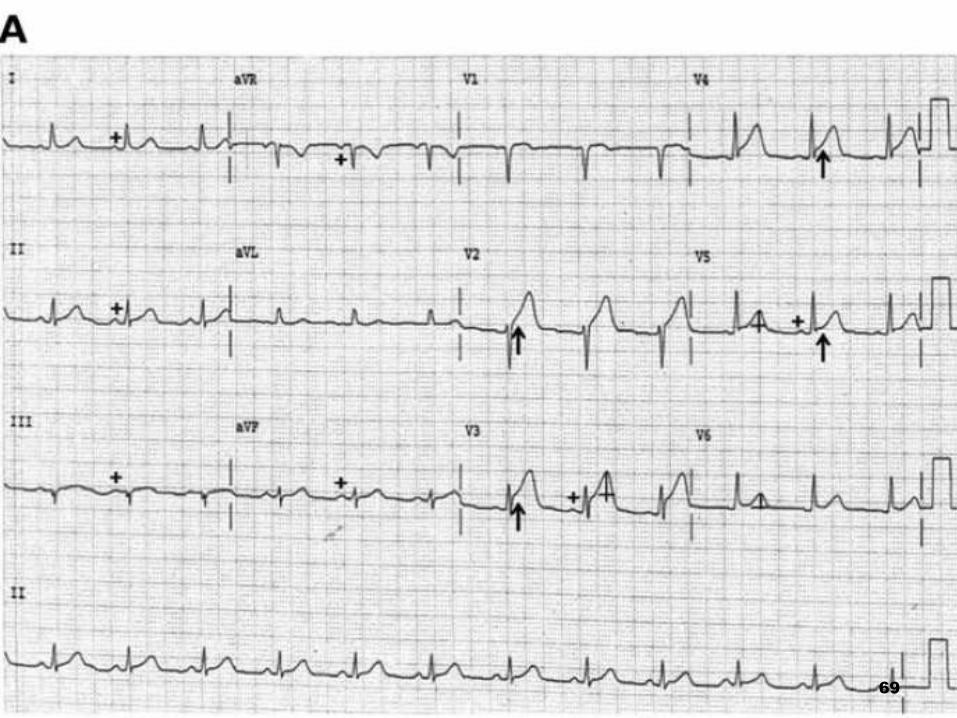
69
70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

70
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
71
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
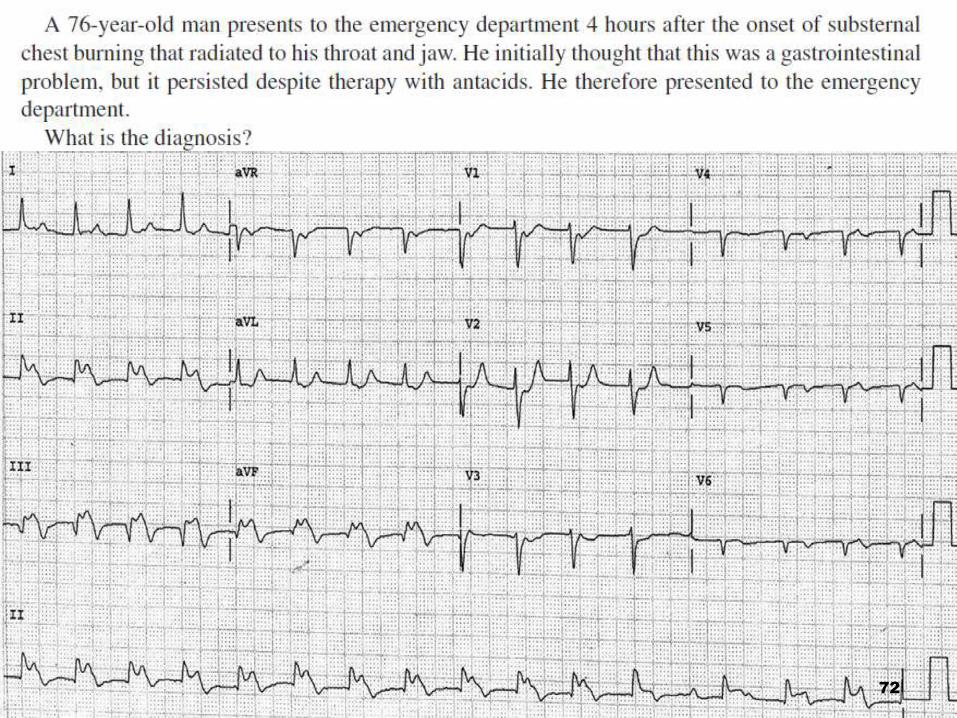
72
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
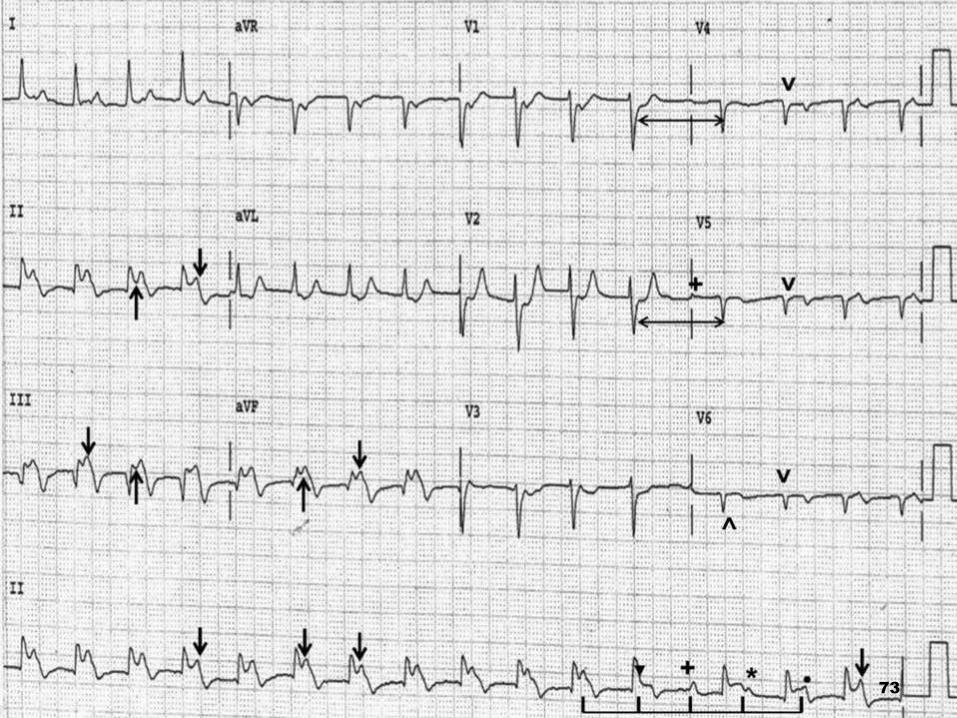
73
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
Acute inferior ST segment elevation myocardial
infarction
Second degree AV block(Mobitz type I)
74
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77
What is pardeersquos sign
75
ST elevation as a sign of coronary
obstruction
1920
76
77

ST elevation as a sign of coronary
obstruction
1920
76
77

77